
Case by Dr. Eytan Raz
To see a World in a Grain of Sand…
In this application, To see a World in a Grain of Sand means to see a world of neurovascular anatomy in a single case. This is one of these… to be showcased in a BANANA BITES video — this will be more like a multi-course dinner…
This page is dedicated to my mentor Peter Kim Nelson, who has championed this approach since my earliest training, to Eytan Raz, my closest colleague and friend and, last but not least, to William Blake, whose vision is reflected here.


Just some points for preview here — excellent MRI/angio correlations, loads of arteriovenous normal and pathologic anatomy, applications of flat pannel CT, stereo imaging, venous balance, and a particularly excellent and underused method to access the cavernous sinus.
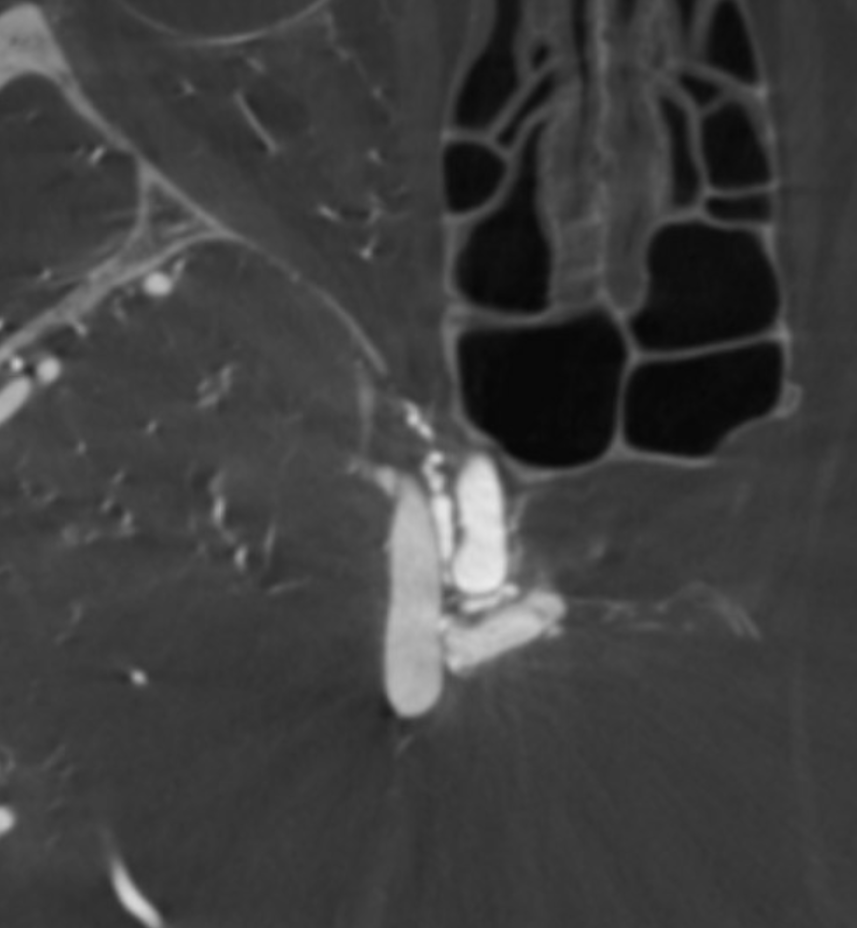
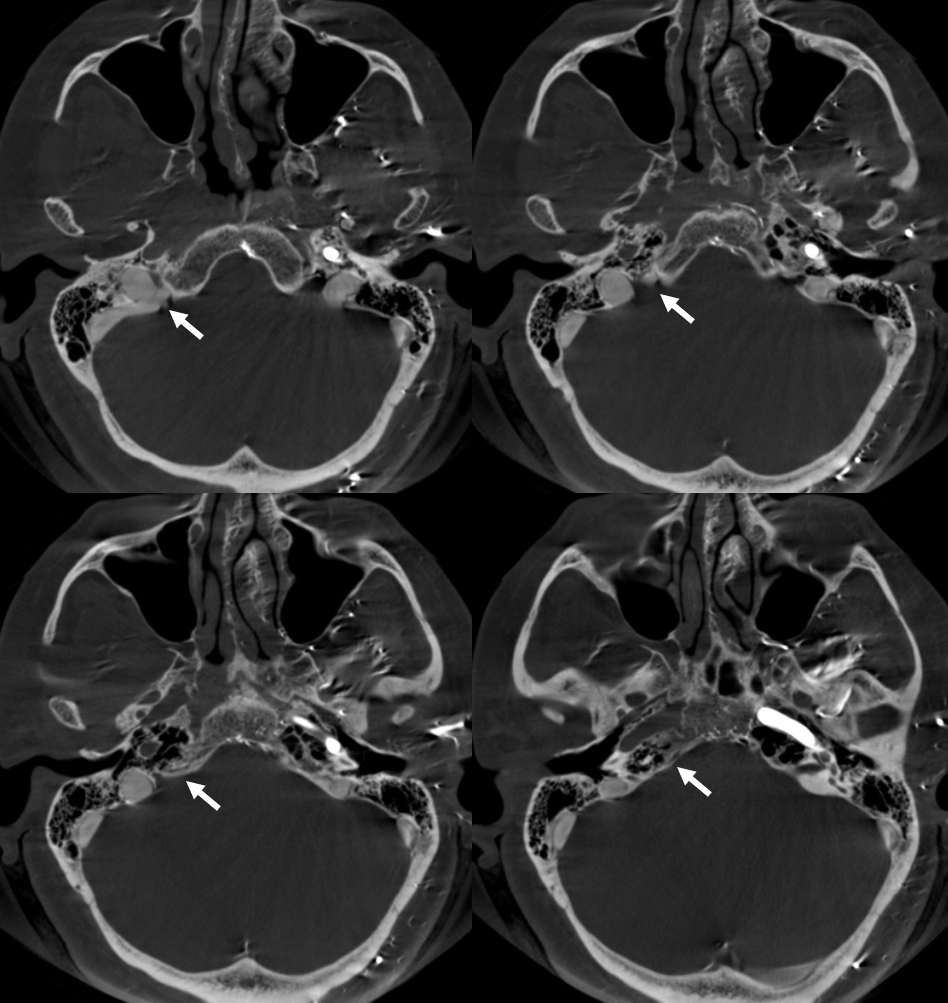
The inferior petrosal sinus (IPS), even if not visualized, might be present but occluded due to fistula-related venopathy. Looking for it on bone windows of CT or flat panel imaging helps to know if one was there. If yes, it is sometimes possible to go through this occluded channel and reach the posterior cavernous sinus, where most fistula common collectors / venous pouches / shunted pouches are. The myriad arterial “feeders” usually drain into one spot somewhere in the back, and closing this in a superselective way — the Achilles heel — will usually produce a cure. Here is an excellent example.
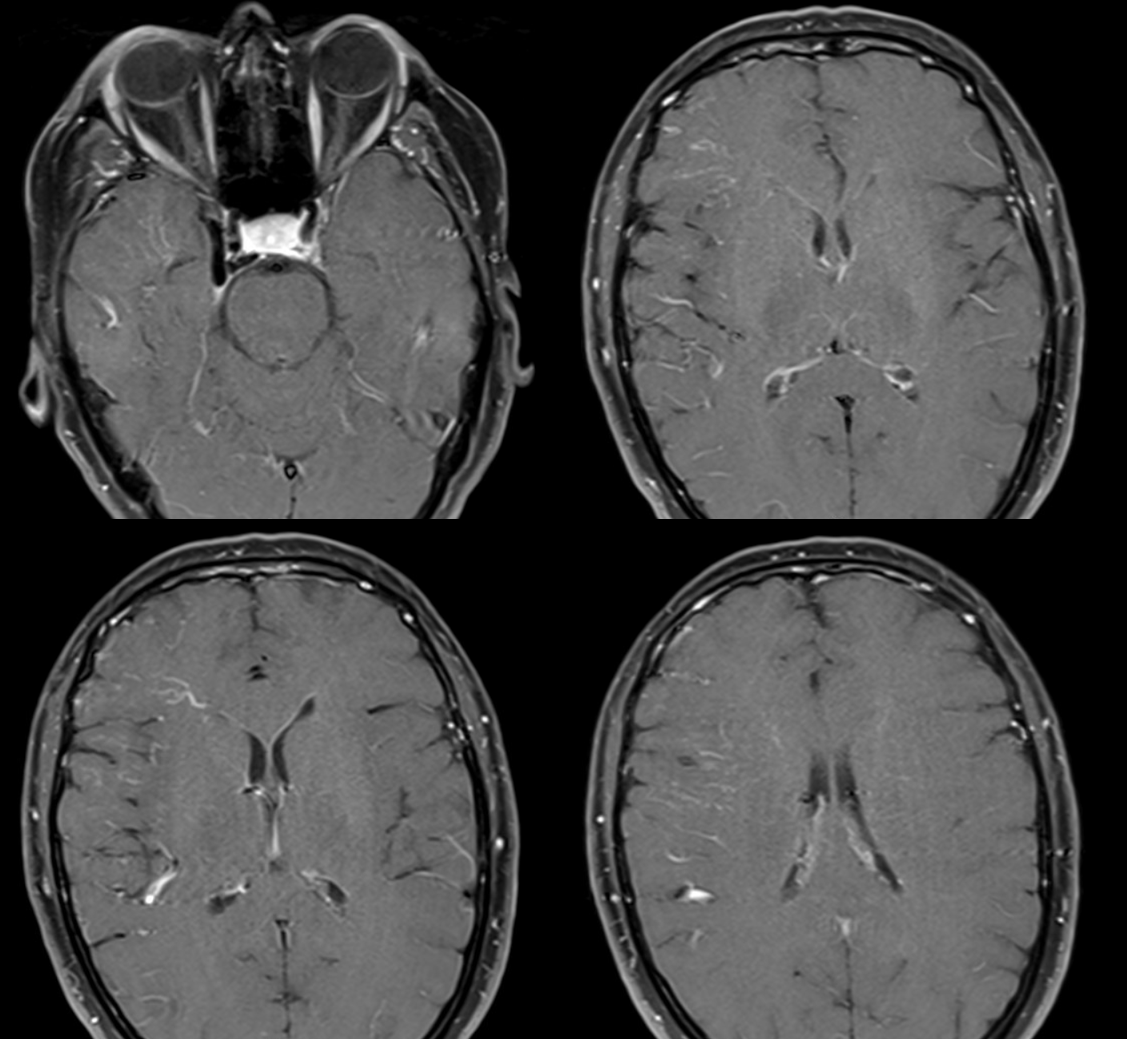
Brain looks fine. There is a flow void in right cavernous sinus
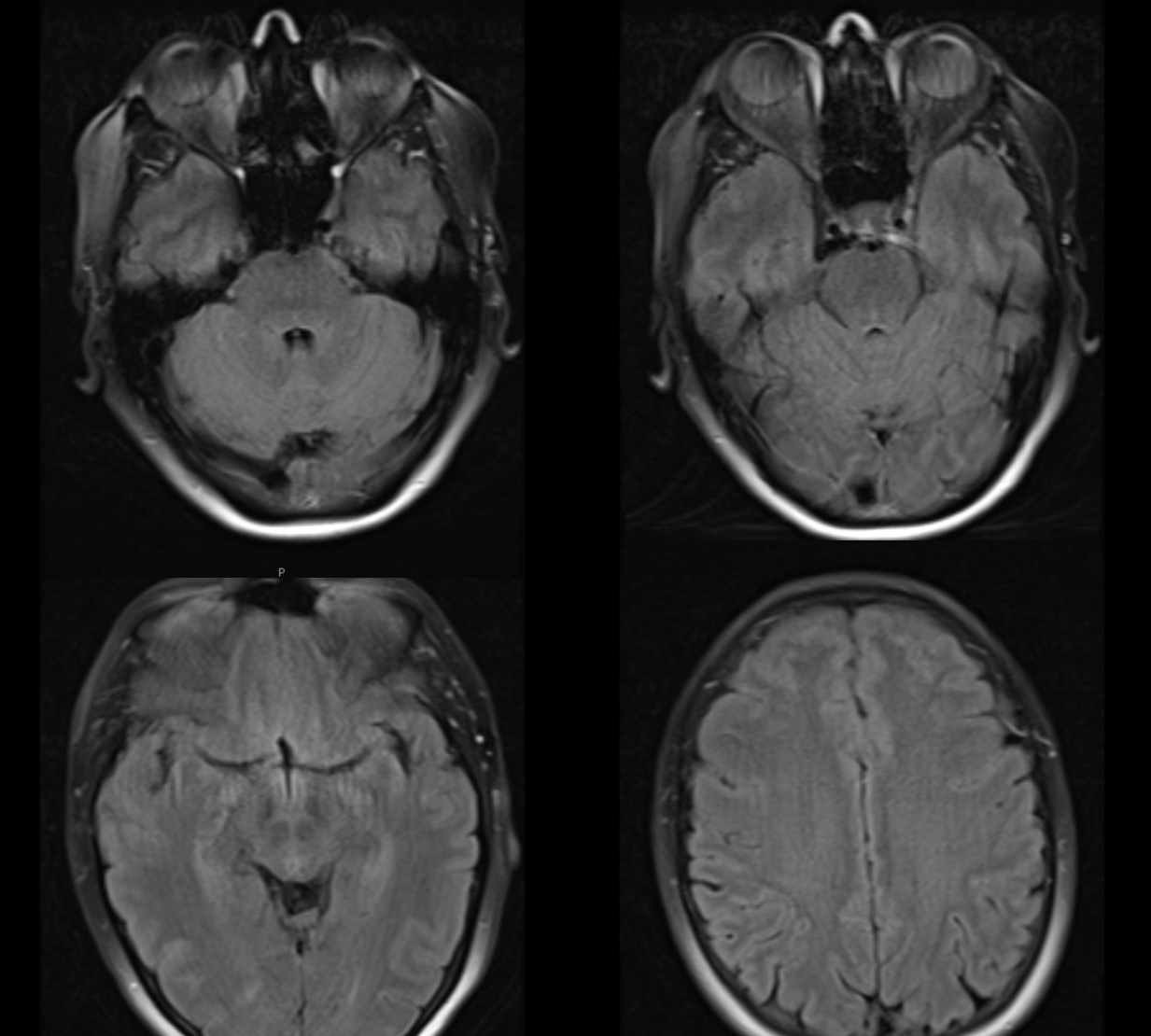
Notice subtle prominence of transmedullary veins in the right anterior temporal lobe extending towards the frontal horn and in the right centrum semiovale on volumetric post T1 images
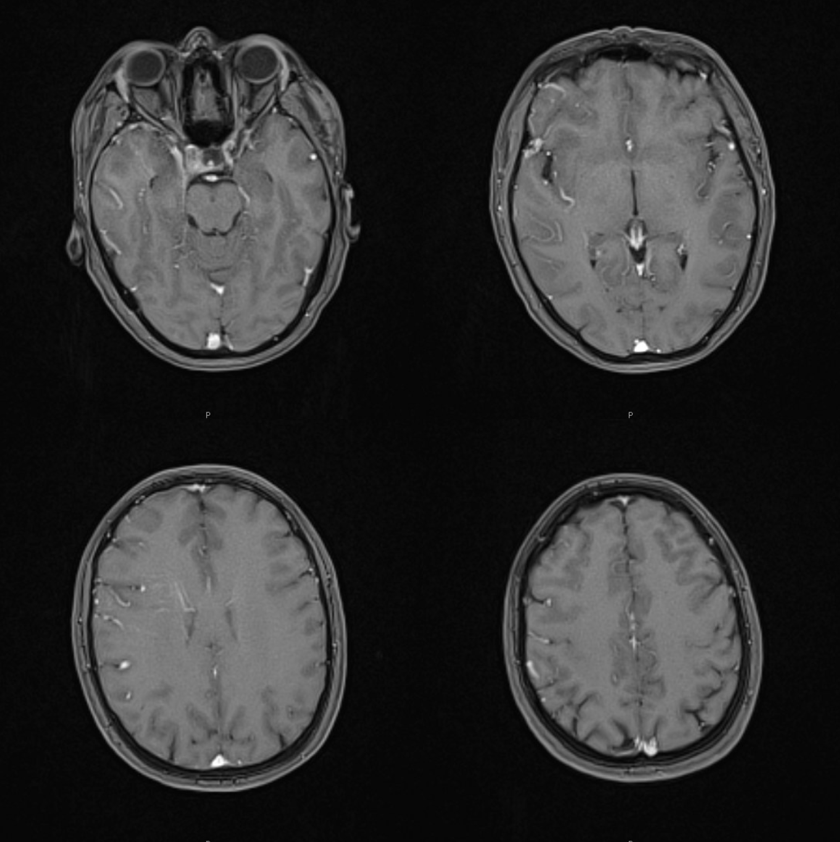
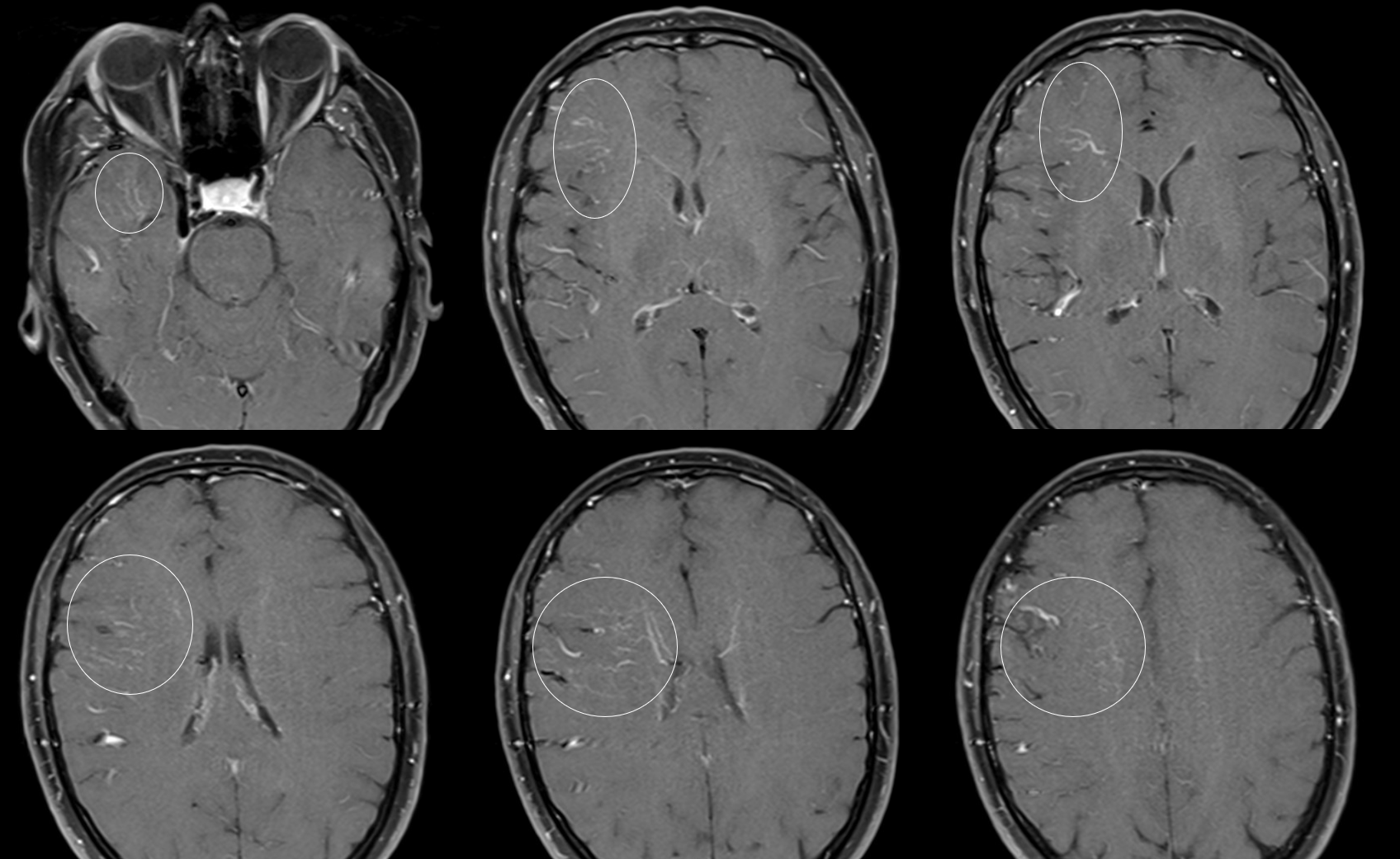
The same veins are better seen in a 2D post-T1
Same — circled below
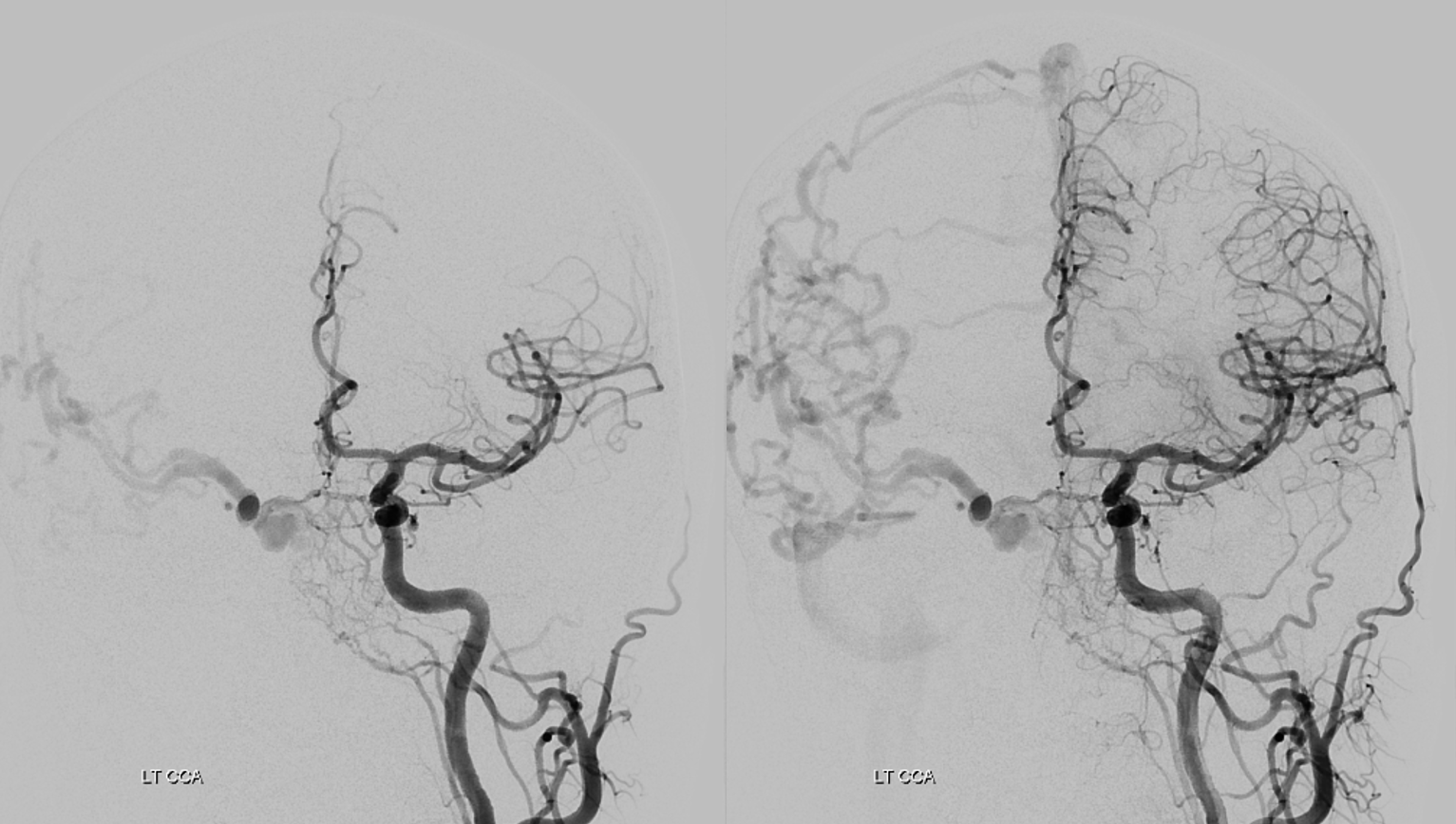
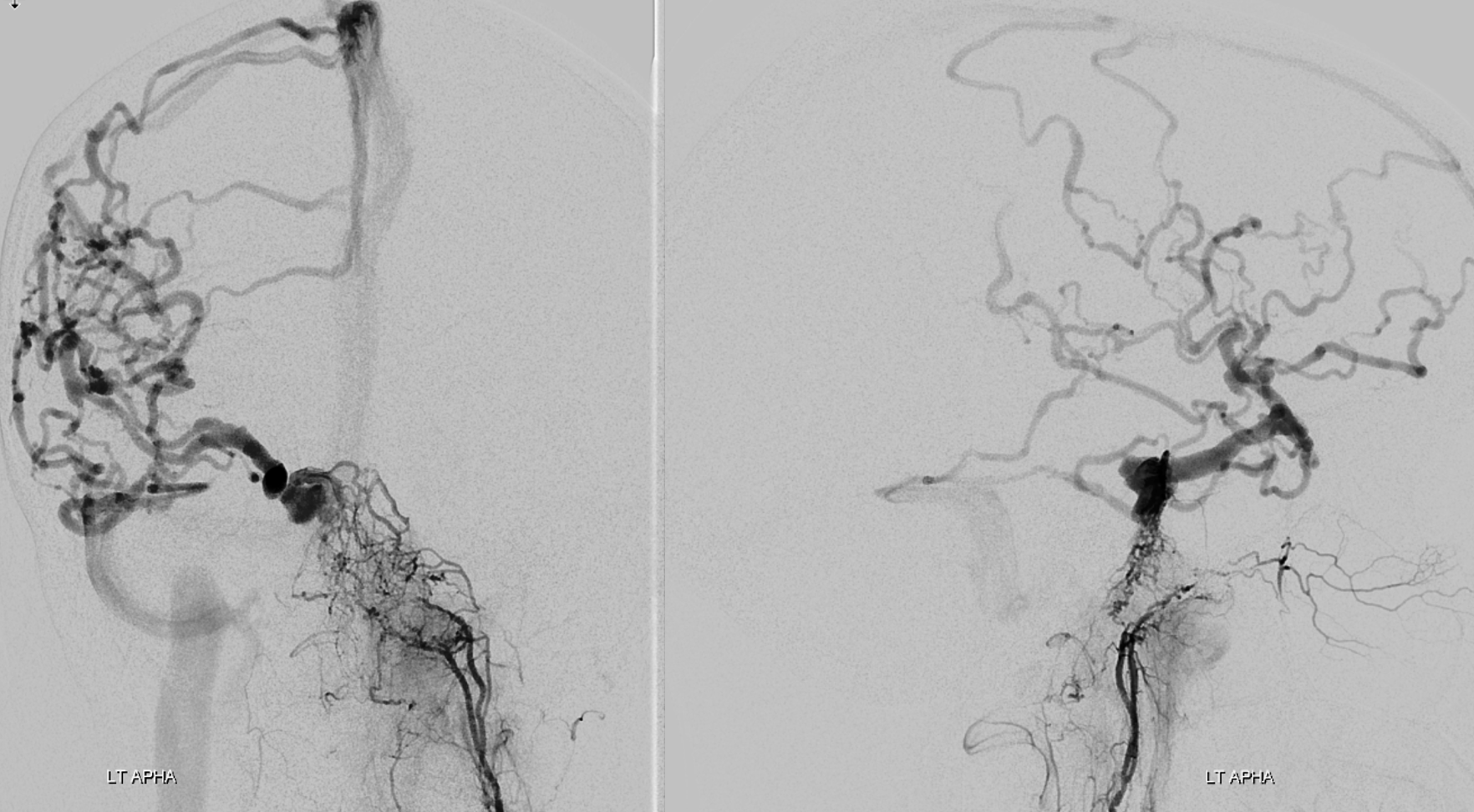
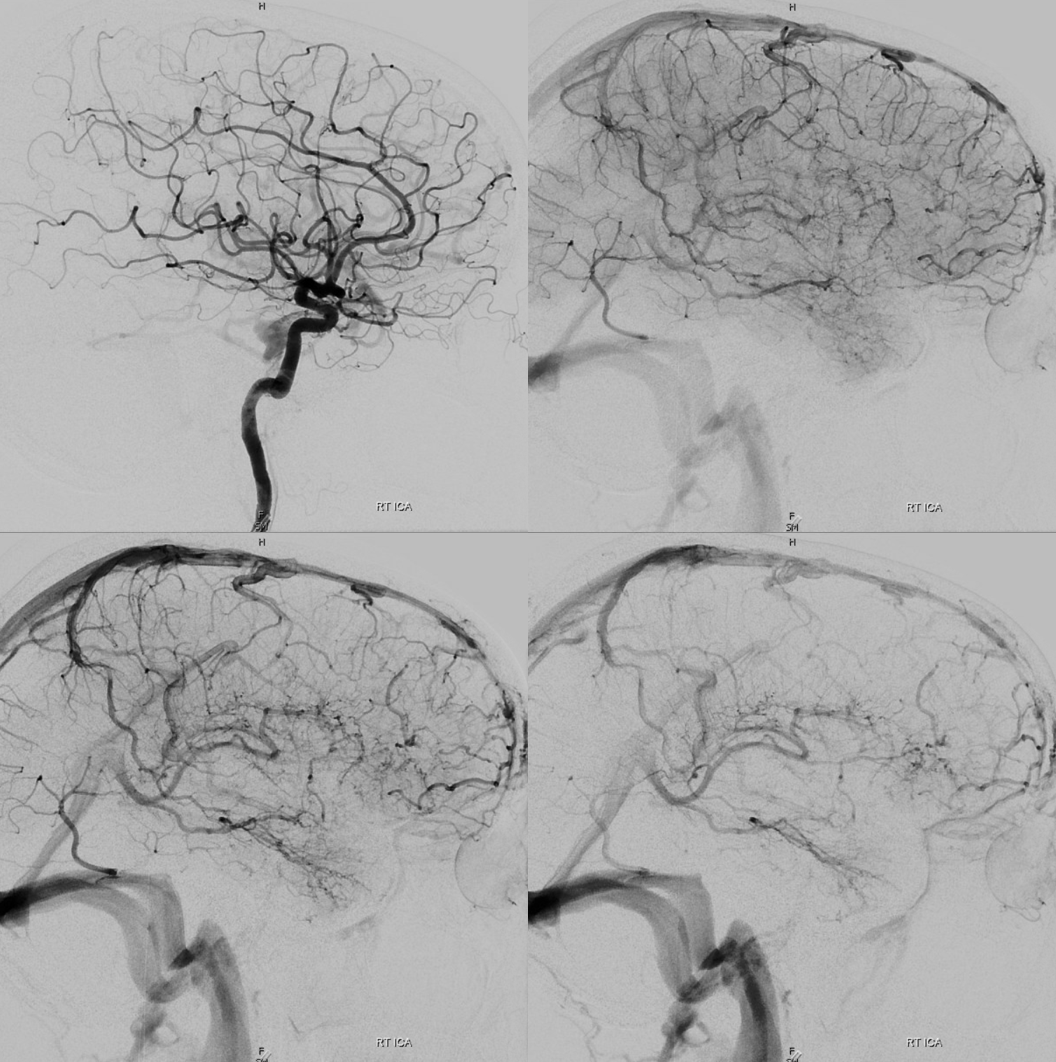
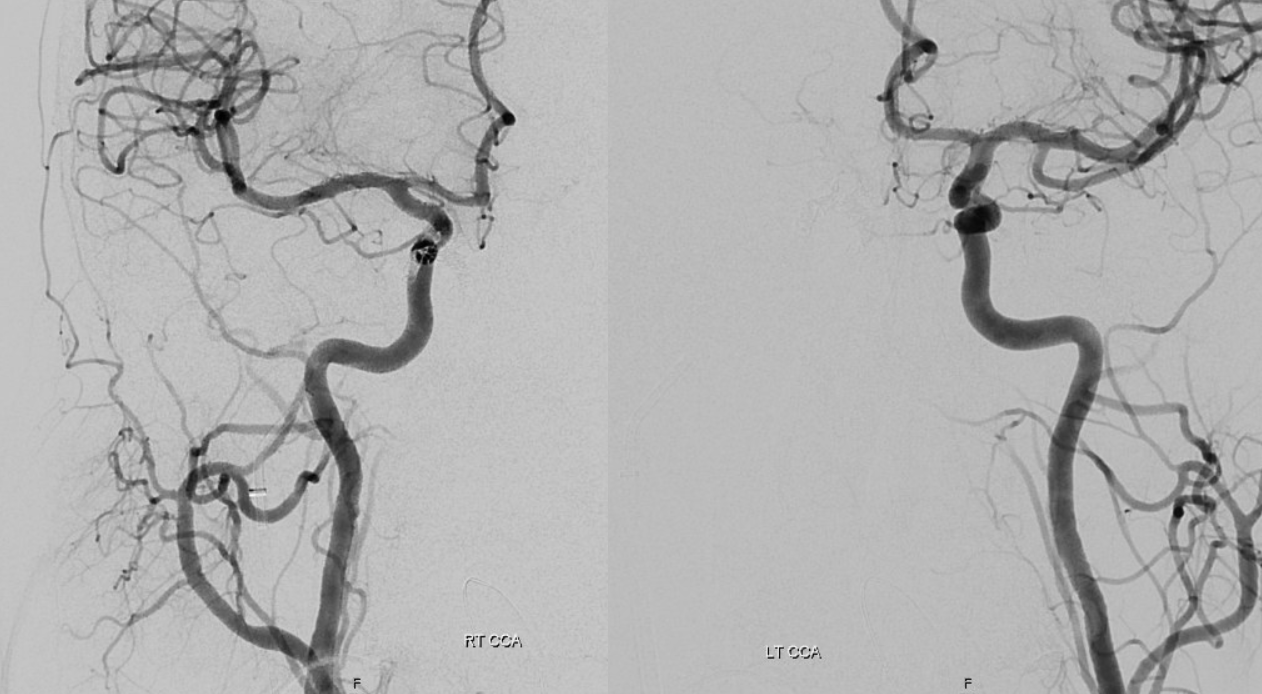
Lots of info here. Fistula is in the back of right cavernous sinus. Supply is from left ascending pharyngeal and left MHT. Drainage is key — there are neither ophthalmic veins nor petrosal sinuses seen — all drainage is intracranial via the sylvian veins. The back part of the right superior petrosal sinus is open but it does not connect to the cavernous sinus
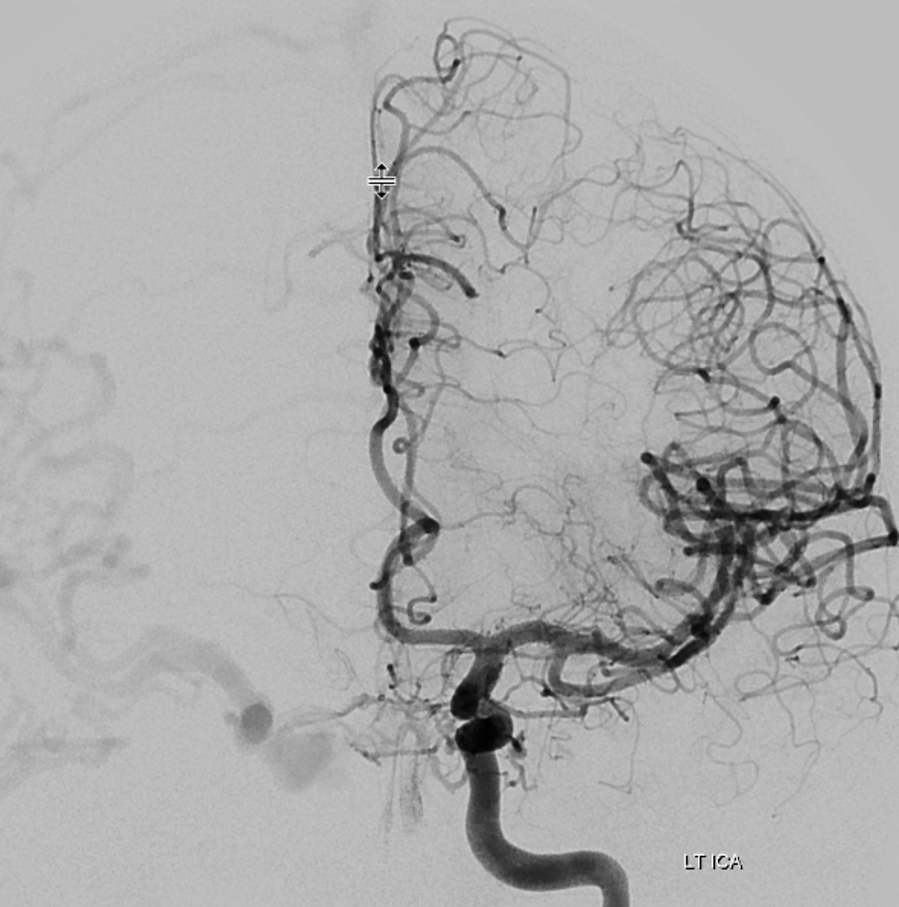
Left ICA — just to show those MHT posterior cavernous branches
Beautiful left ECA images — the transosseous network of the ascending pharyngeal artery can be a decent route for embolization
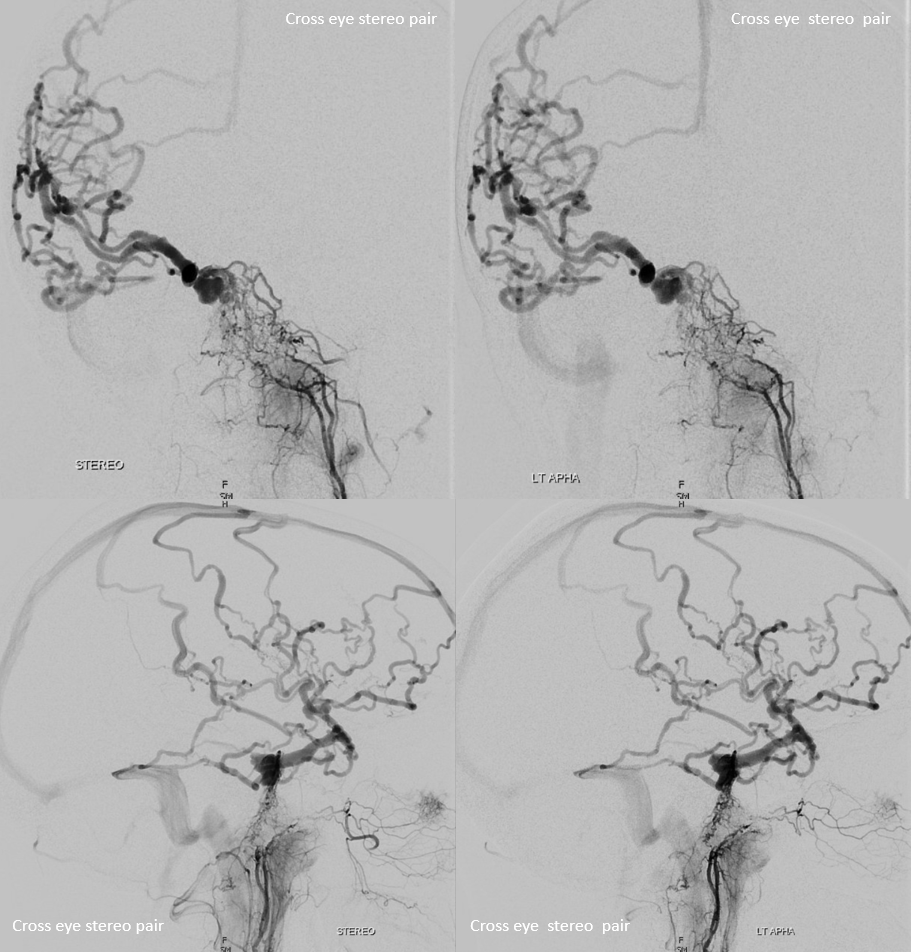
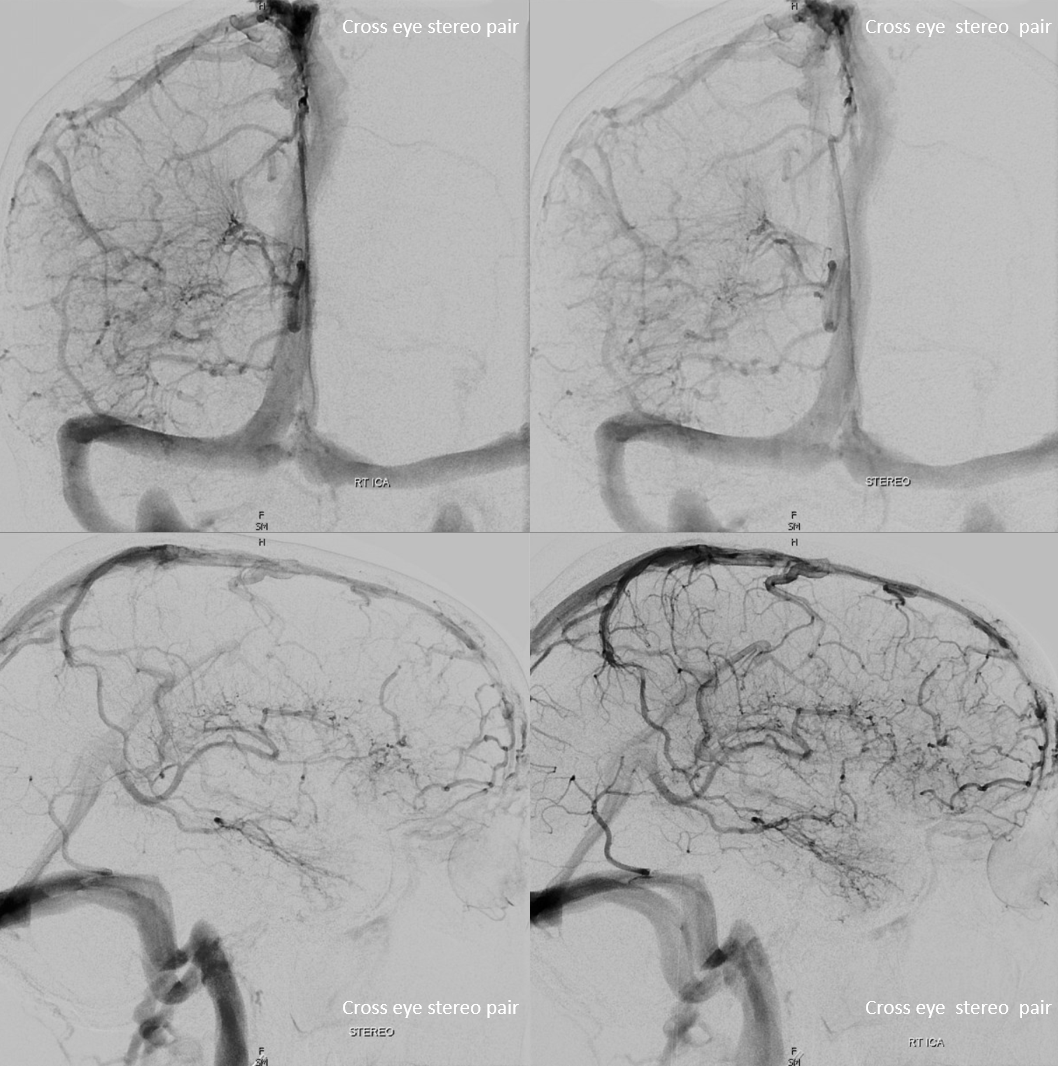
Beautiful cross-eye stereos
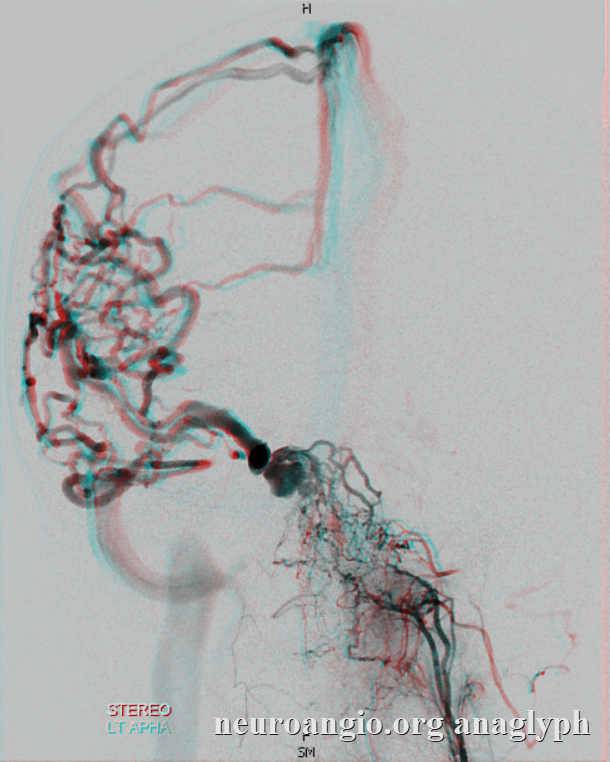
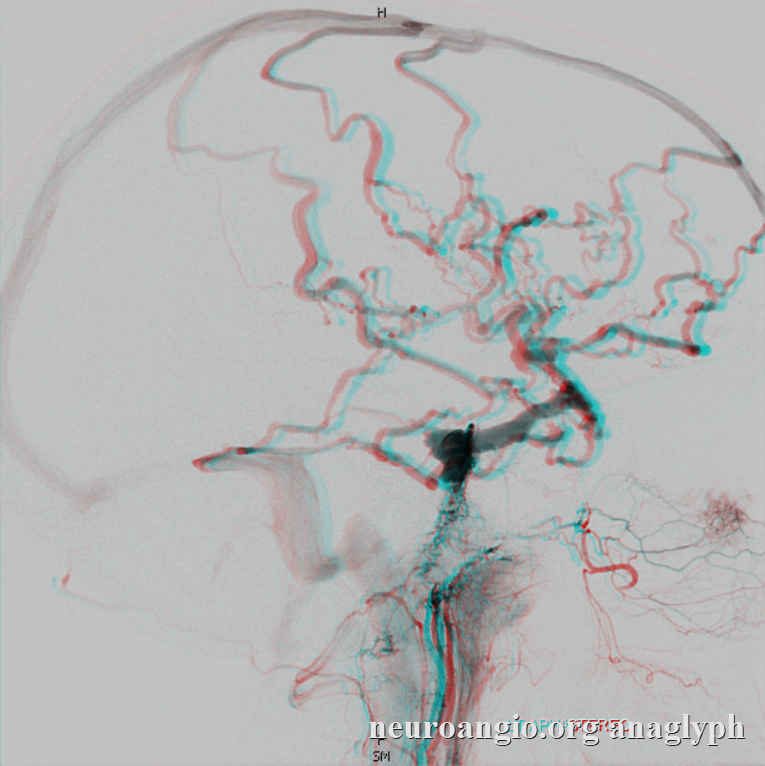
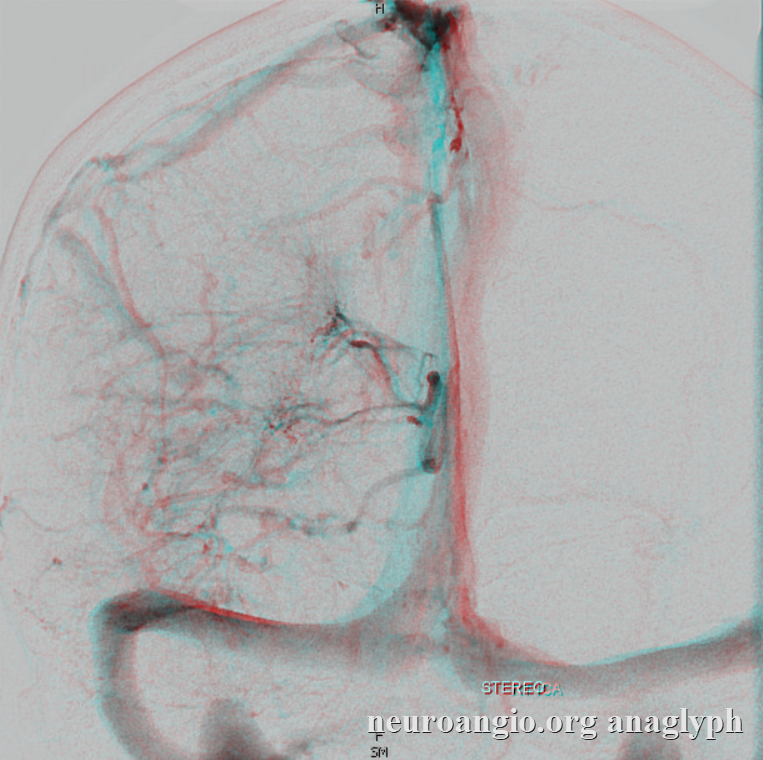
Anaglyph Stereos — get those old red-blue glasses to see them — nothing beats anaglyph (except cross-eye) for versatility
Below is a movie of left common carotid Dyna — it is an anatomy atlas in itself. Pause it to scroll thru individual frames. See those myriad branches of the AP in the clivus. Its a good route for transarterial shot — the least bad transarterial option
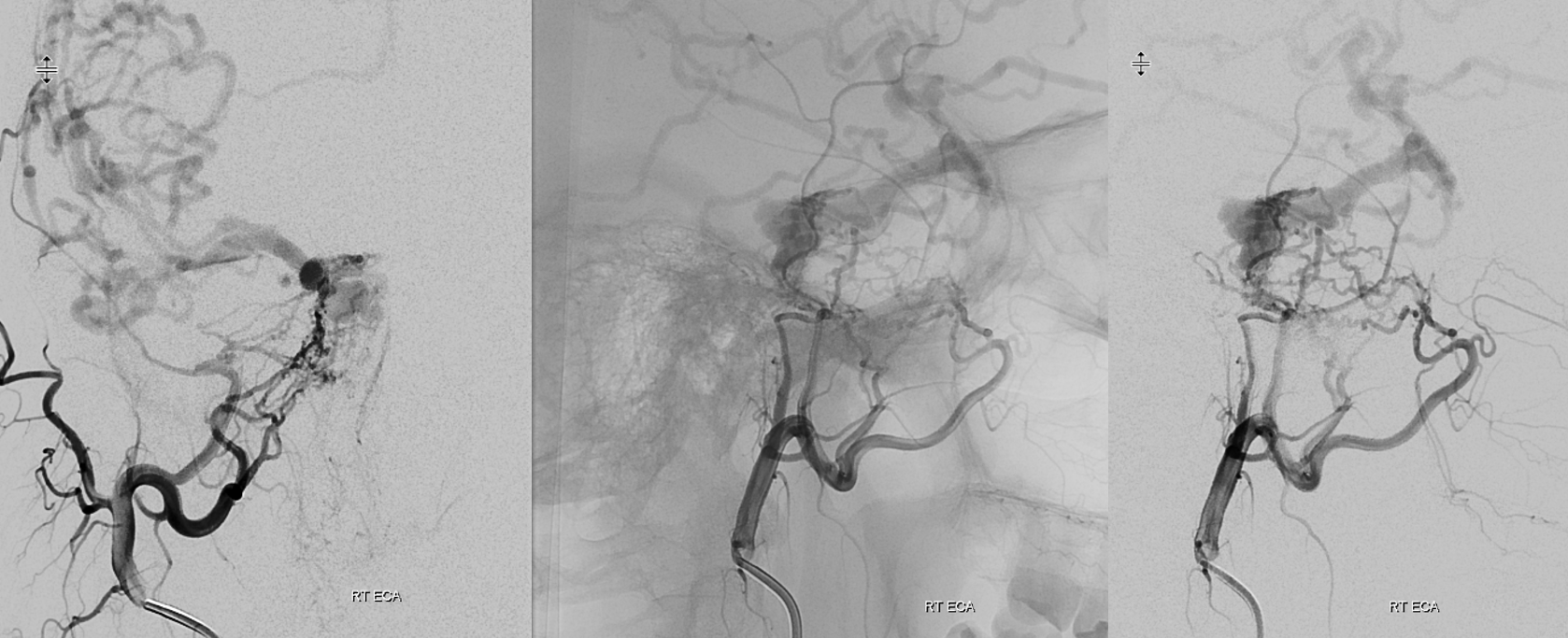
Right ECA — beautiful network from MMA and accessory meningeal arteries using the “cavernous branch” route — except there is not a single cavernous branch — tons of them — as well as rotundum, etc.
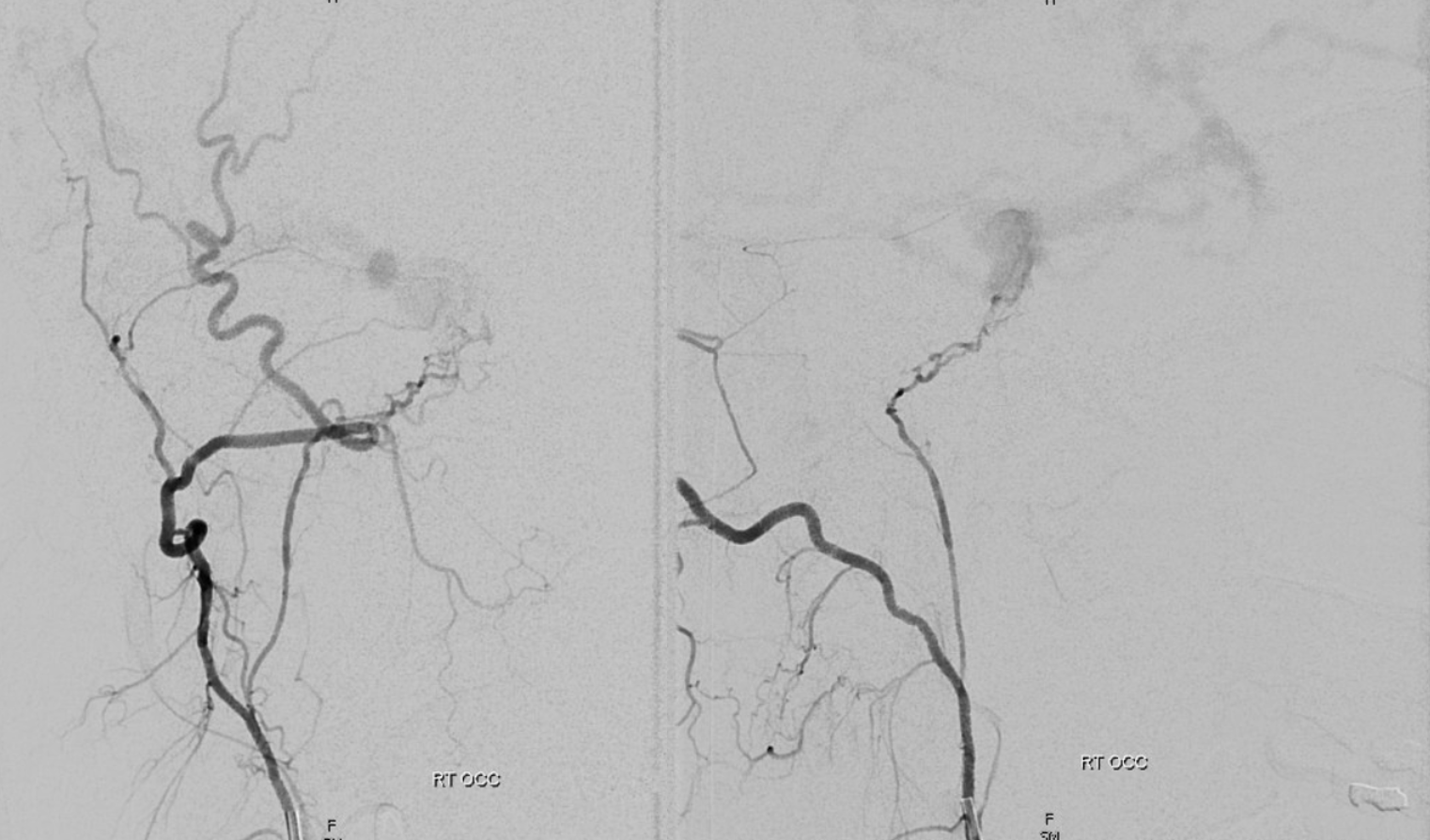
Right occipital artery injection shows isolated jugular division origin (normally from ascending pharyngeal artery) contributing to fistula. Opens a whole discussion of occipital/ascending pharyngeal supply to lower cranial nerves…
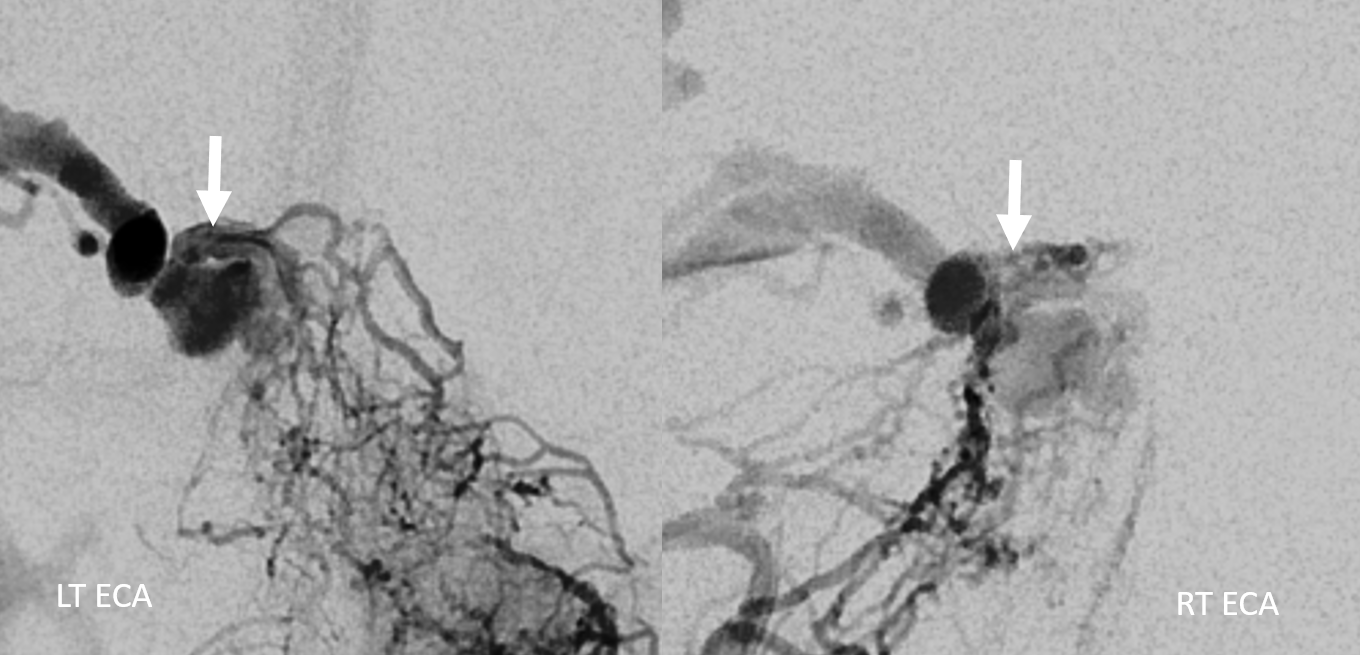
All roads lead to Rome — or Achilles heel — as you might feel — converging on the arc-like structure marked by arrows. Is it a “common collector artery” or a “shunted pouch” vein? Probably the latter.
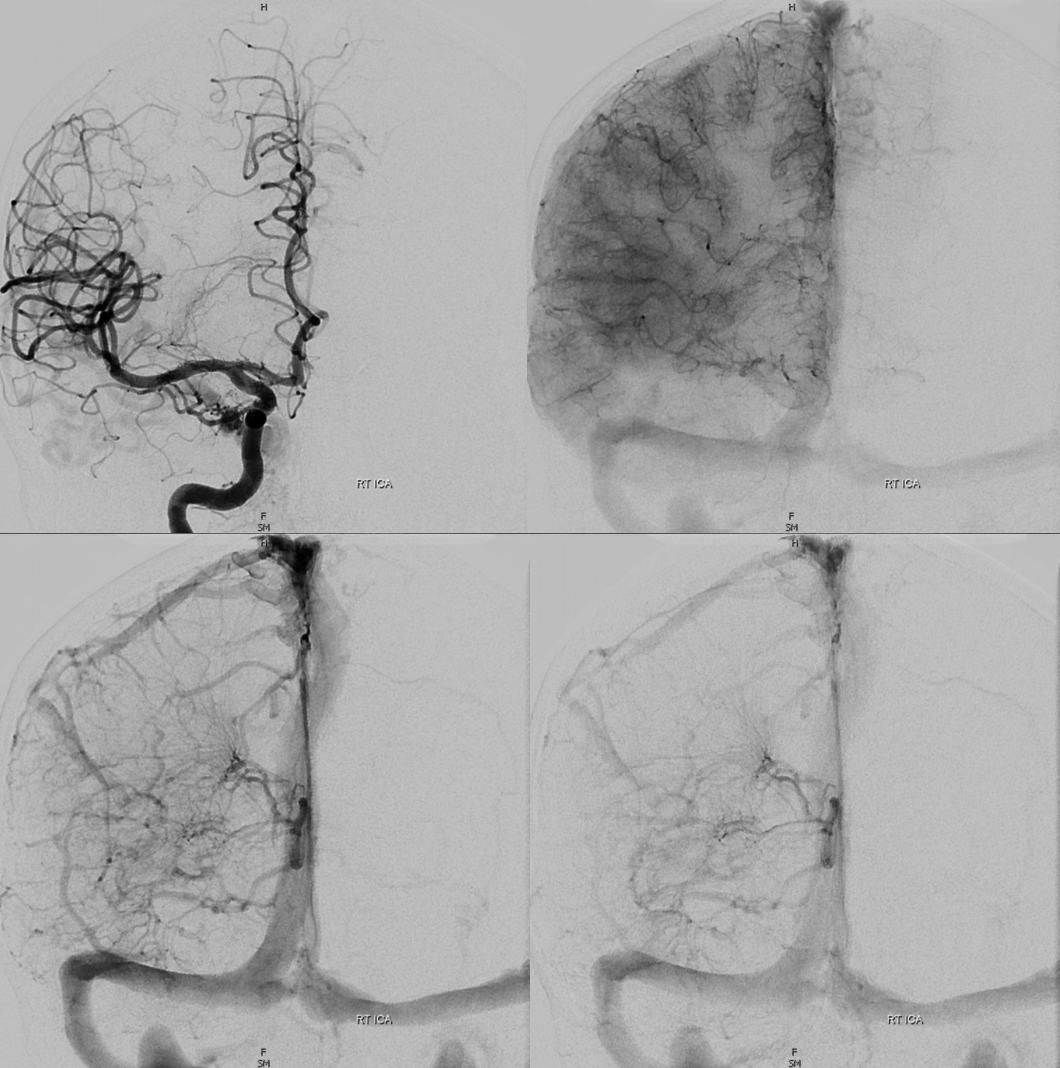
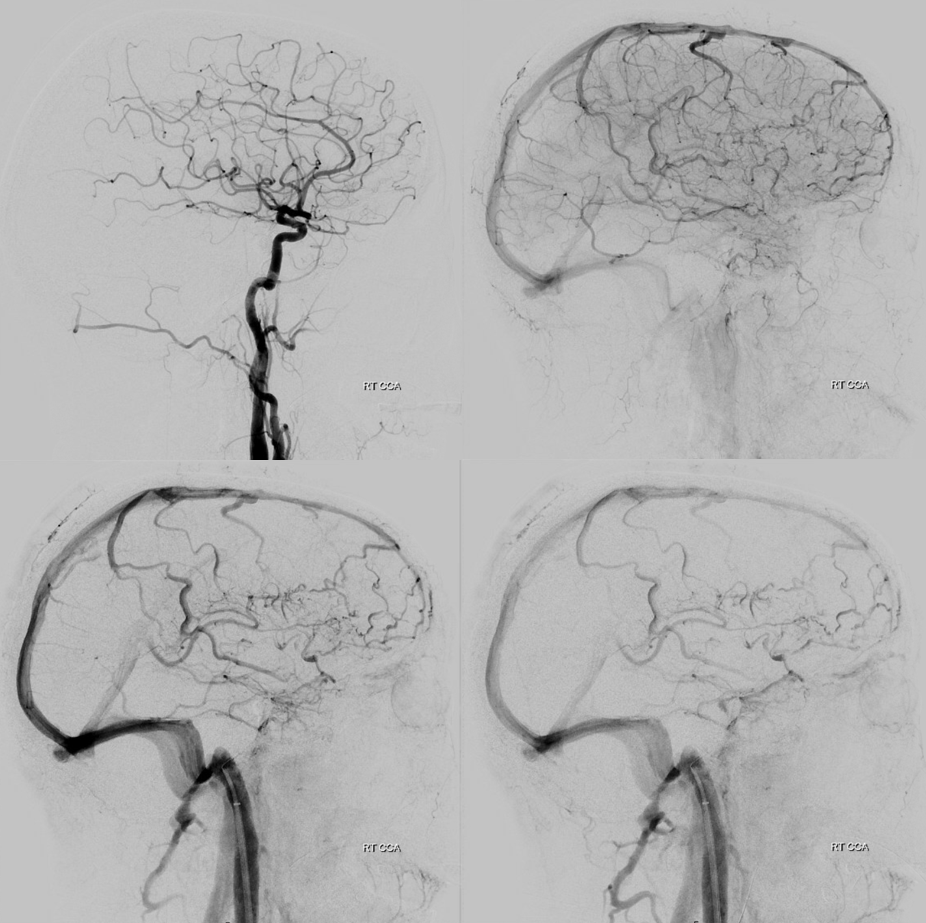
Now lets see how the brain is draining in spite of this high-grade hardship. Pretty well, given absence of flair signal problems. The images below show where cortical drainage has shifted. Can you tell?

DYNA of right CCA injection — another atlas of anatomy here…
What to do now? Transarterial options are not so great — aside from the transosseous ascending pharyngeal branches there is not much that makes sense — and any transarterial shot risks retrograde penetration into a myriad potential problem areas.
Direct transorbital — see case example here and and another case of technical video here— is not a straightforward path in this case — there seems to be no open cavernous sinus adjacent to the superior orbital fissure (see below) — perhaps that would work anyway, but not the sure entry into the sinus that we like direct transorbital to be.
Intraoperative cavernous sinus exposure? Excellent option, and probably as sure a thing as can be, if craniotomy is in the cards.
Finally, inferior petrosal sinus option. Access via occluded IPS is an excellent thing to try. But, its a long shot here — its one thing when there is a big one that occluded. Here, though, it is hypoplastic at best (arrows)
We were not sure about this at all, thinking to try it before going transarterial. Between PKN, Eytan, and myself, Eytan held had the most enthusiasm for trying. It worked!
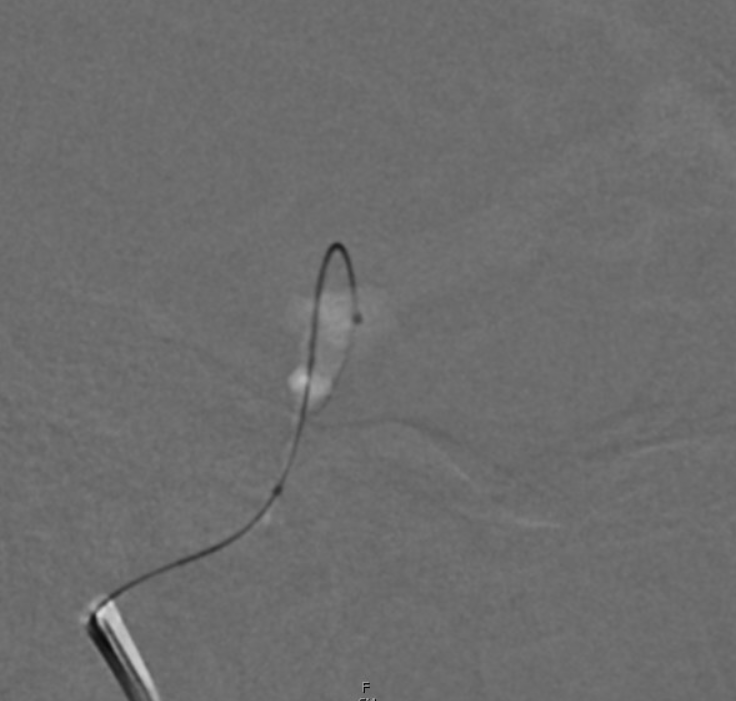
Our typical triaxial access setup is a 6F guide (BMX), 5F vert pointing into the sinus (a sturdy Cordis vert, not a flimsy Penumbra one), and a Headway Duo on an Aristotle 14. The wire choice is flexible, whereas the low profile but widely coil-compatible Headway Duo is usually king for this kind of work.


We are very close — but not there yet. A very thin channel now connects our blind IPS pouch with the cavernous sinus. Onyx might work, but not sure…
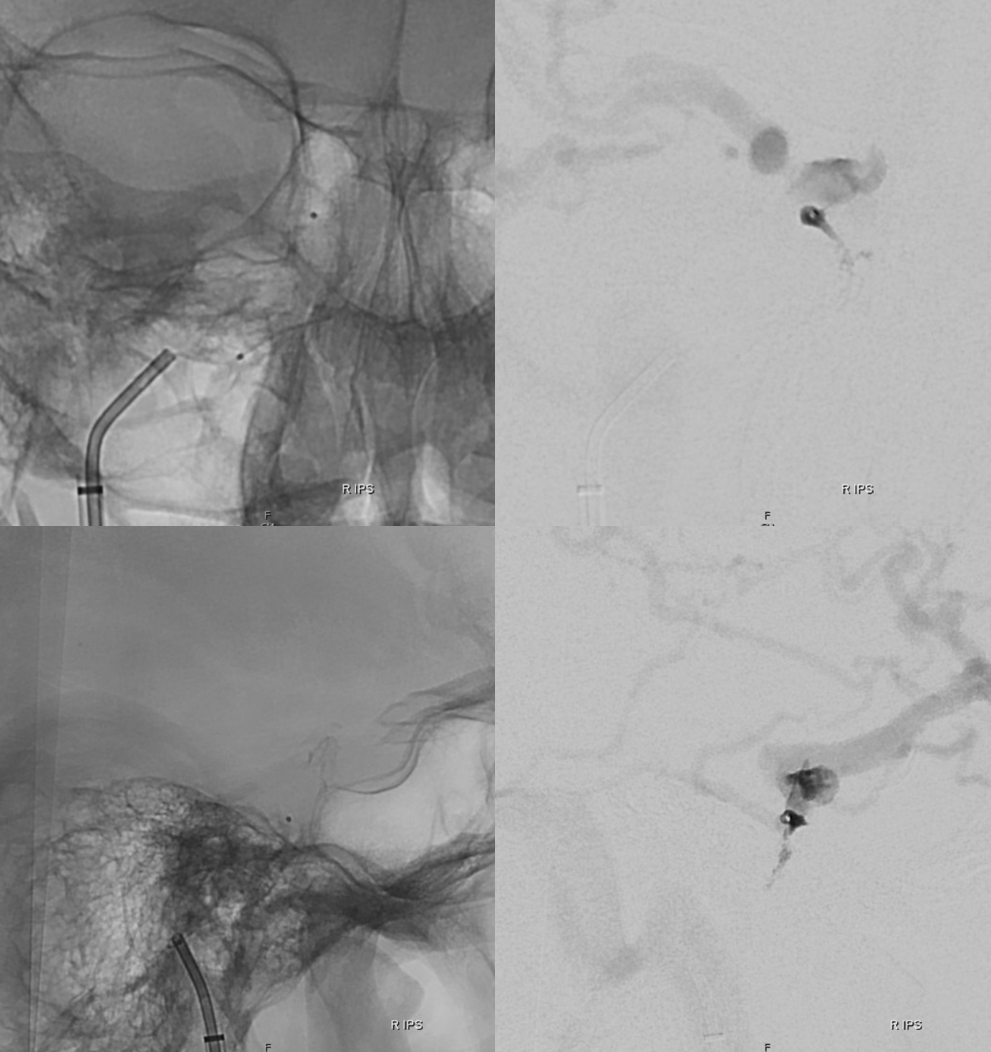
After some more trying by Dr. Raz, the wire finds another path — not the small connection above, but another one a bit more laterally, and enters the sinus. Duo follows
Lateral view below
Below is a video of access
A GIF
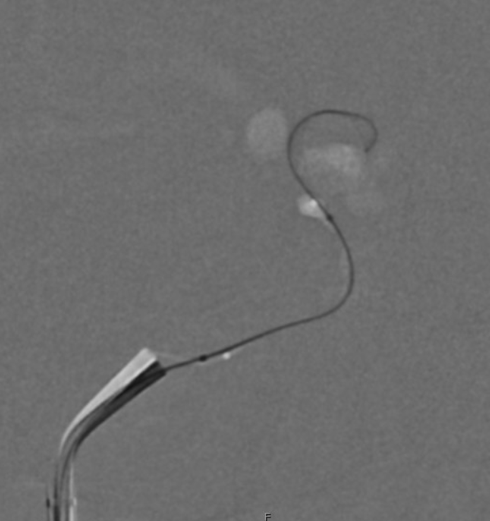
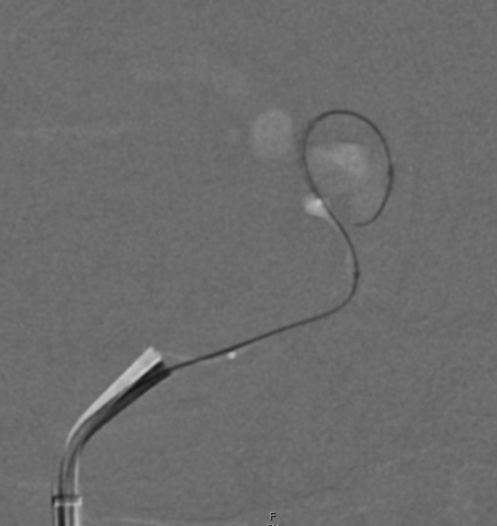
We are in the heart of the fistula — at the arc collecting its myriad arterial feeders. A Headway Duo injection — a fistulogram
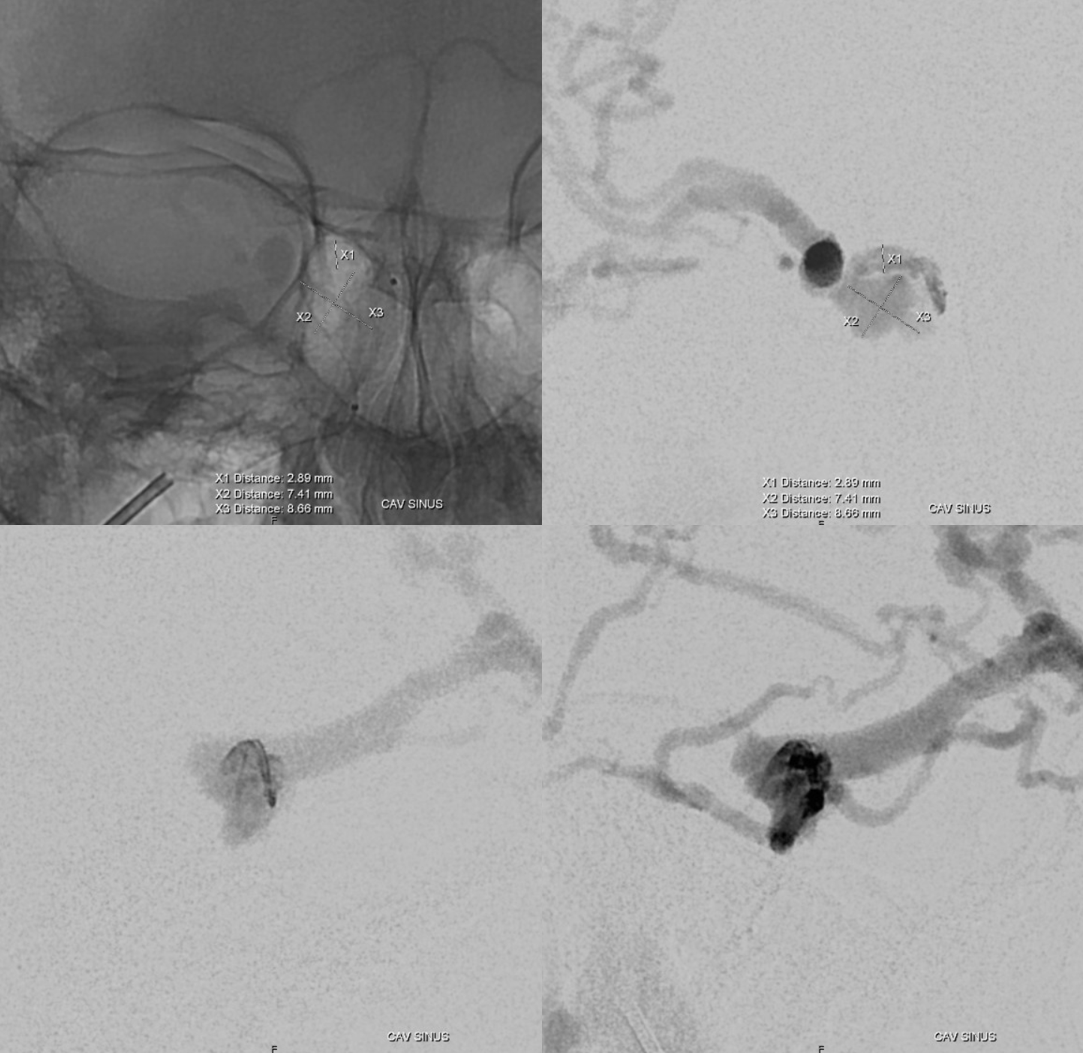
This is the beauty of superselective embolization — a few coils (or whatever embolic you want) on the venous side are more effective than tons on the arterial side. It is the location of supreme vulnerability — a true Achilles heel of this mighty fistula. It only took a few coils…
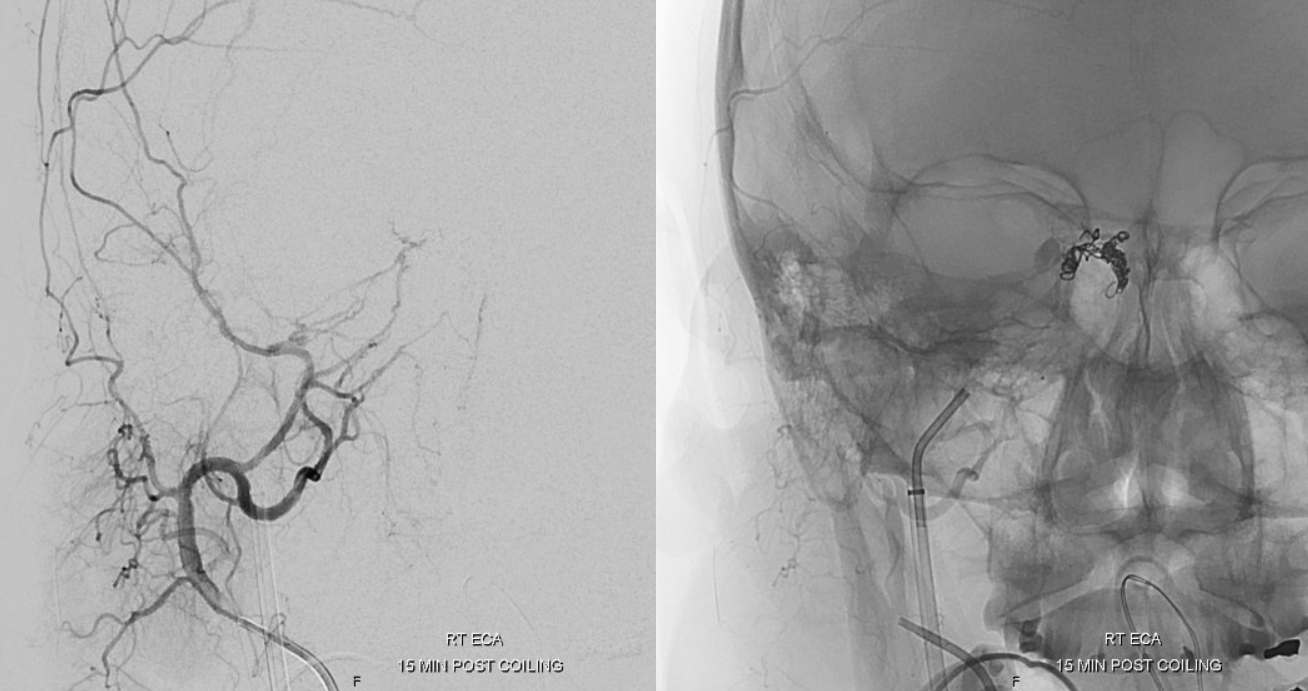
Note how the brain is now back to using all those cortical veins that were owned by the fistula until minutes ago.
Moral — try the IPS…
For an answer as to where the right cortical venous drainage shifted in setting of prominent fistula-related takeover of superficial cortical veins, you will have to wait for a www.youtube.com/neuroangio BANANA BITES video of this page…
See another Achilles heel example here
Check out other superselective / magic bullet transvenous dural fistula embolizations in the Case Library page
The “shunted pouches” approach of Hiro Kiyosue and colleagues can be read about here and here
For comprehensive discussion of cavernous sinus dural fistulas by Goetz Benndorf look here