
Case Courtesy Dr. Eytan Raz
The traditional surgical approach to disconnection of ethmoidal fistulas, though typically safe and effective, is giving way to a variety of endovascular solutions, at least where we come from. There are several ways to accomplish this, depending on anatomical factors — see companion cases of transvenous and trans-ophthalmic embolizations. The trans-ophthalmic route is the least favored, for obvious reasons, but can be used quite safely when surgery is not a good idea (coagulopathies, major co-morbidities, etc) and when other routes are not available.
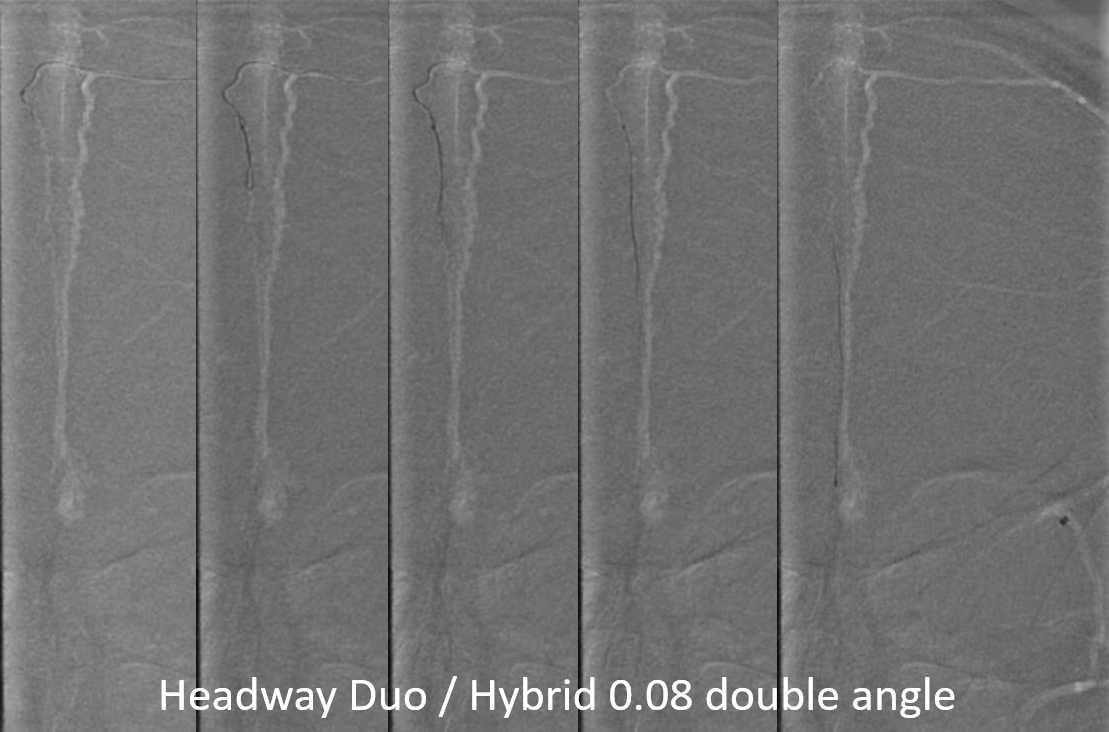
Below is an example of embolization via middle meningeal to anterior meningeal connection, facilitated by advances in access technologies — in this case the amazing Hybrid wire — Headway Duo combination
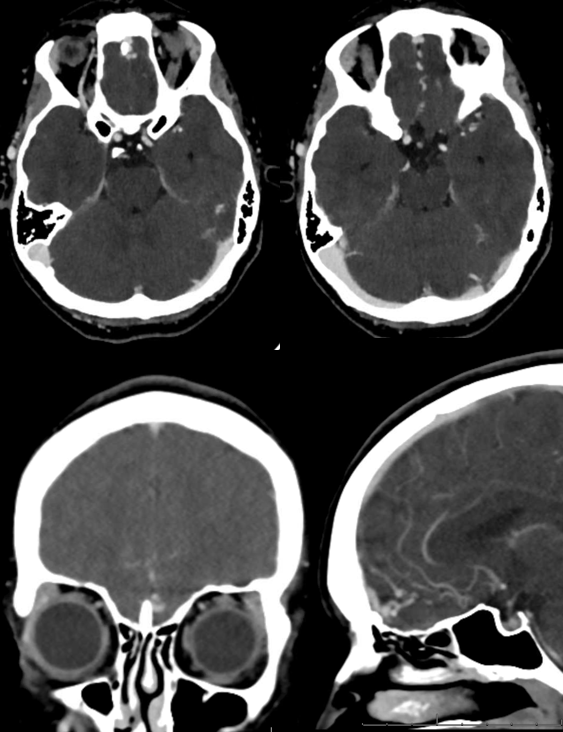
CTA
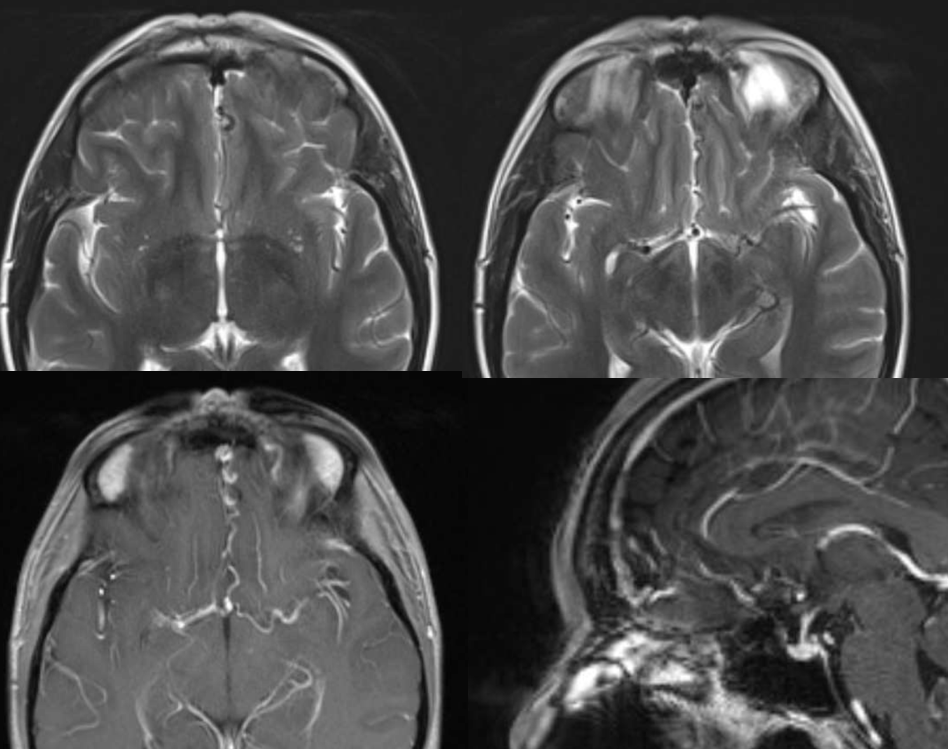
MR
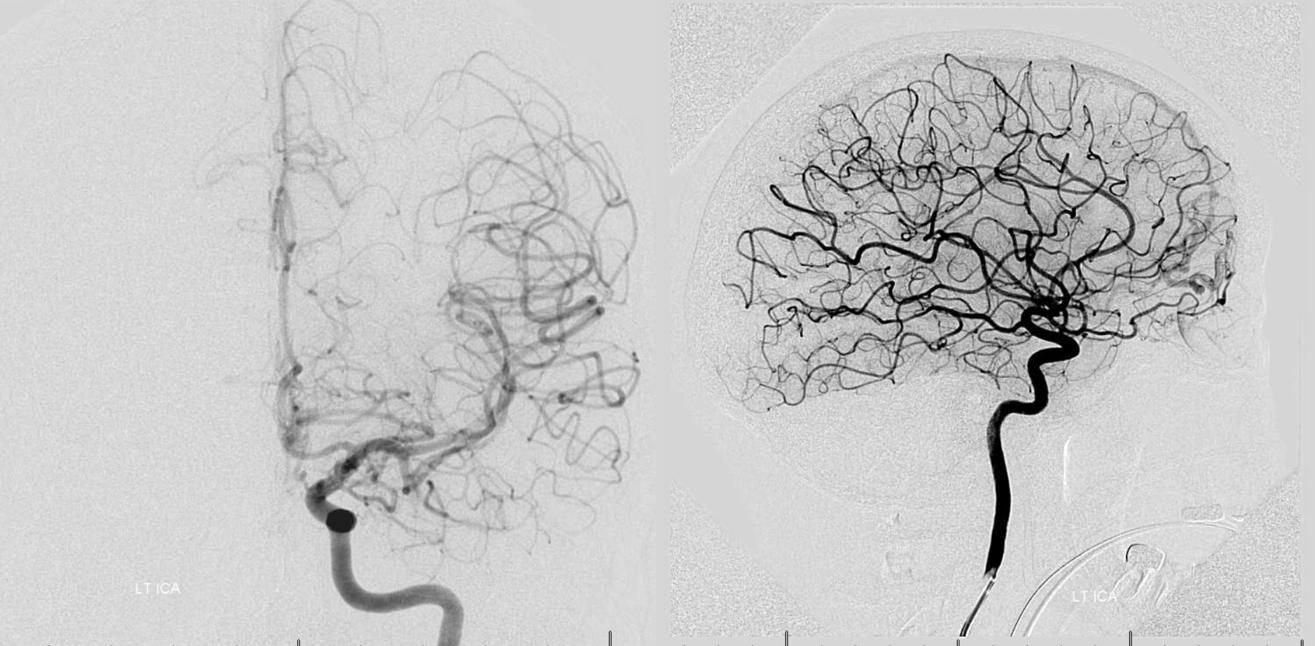
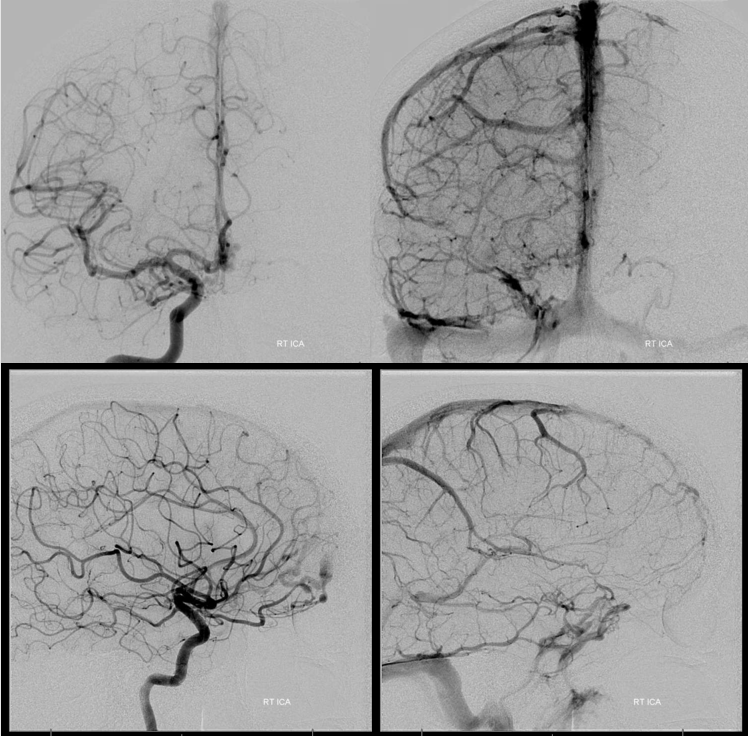
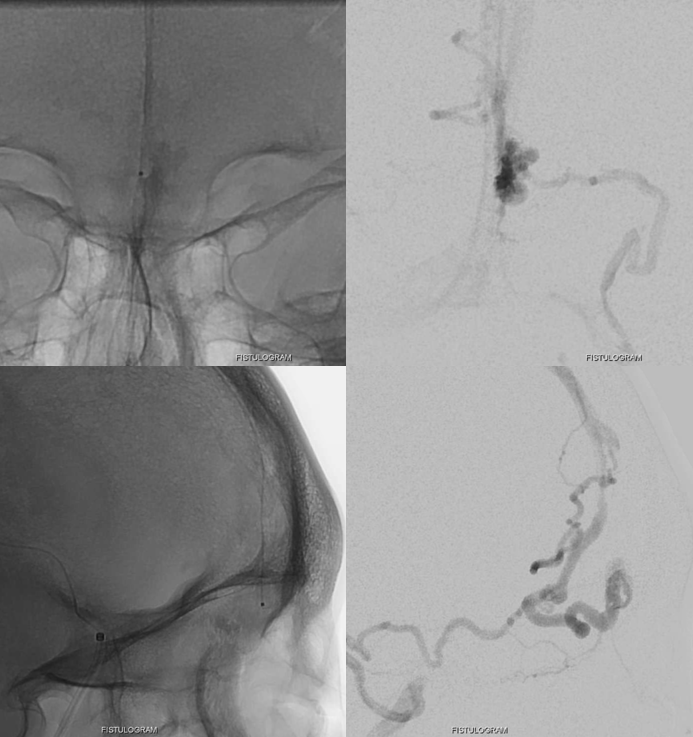
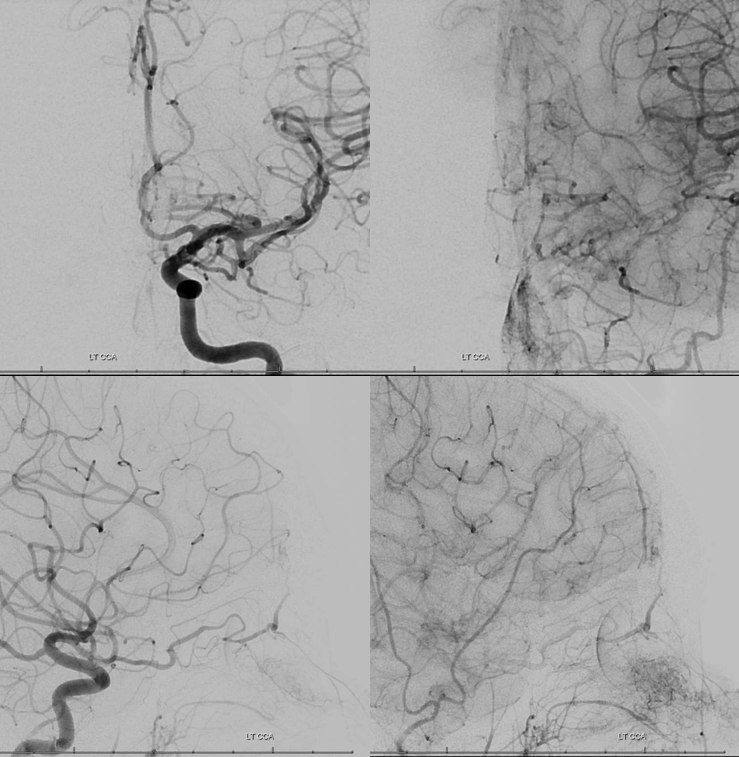
left ICA
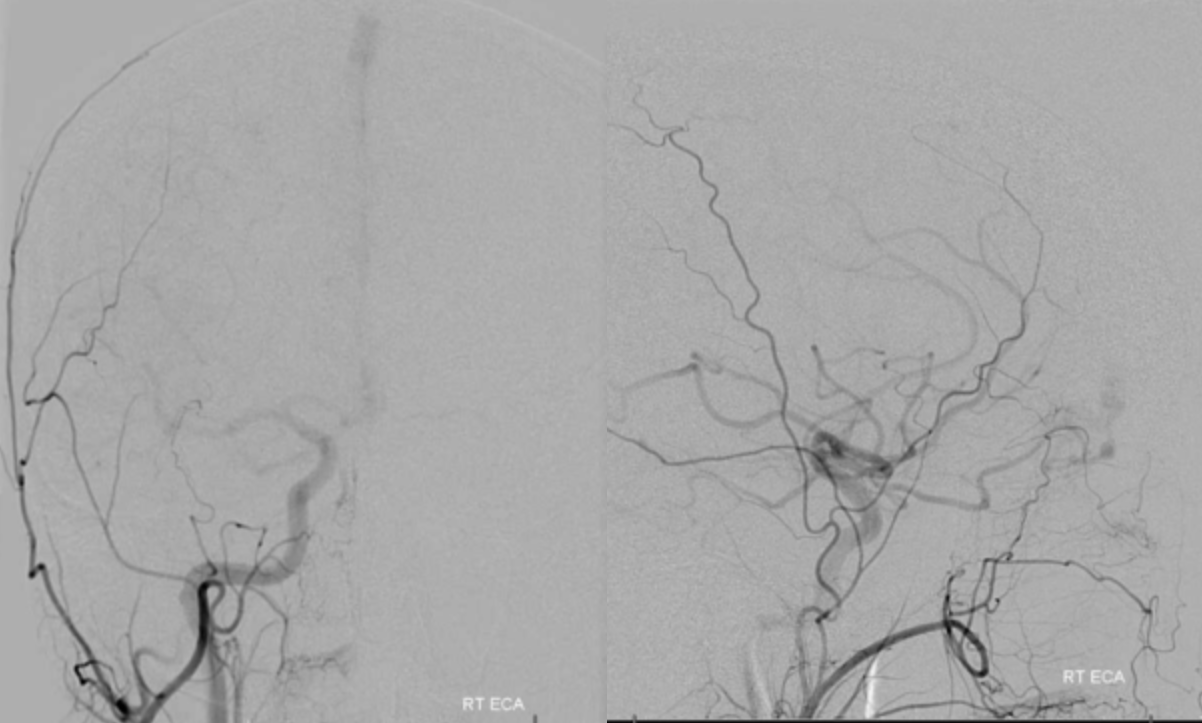
left ECA — major supplier. Classic morphology of anterior meningeal arterial arcade in the wall of superior sagittal sinus. Both channels are quite tortuous.
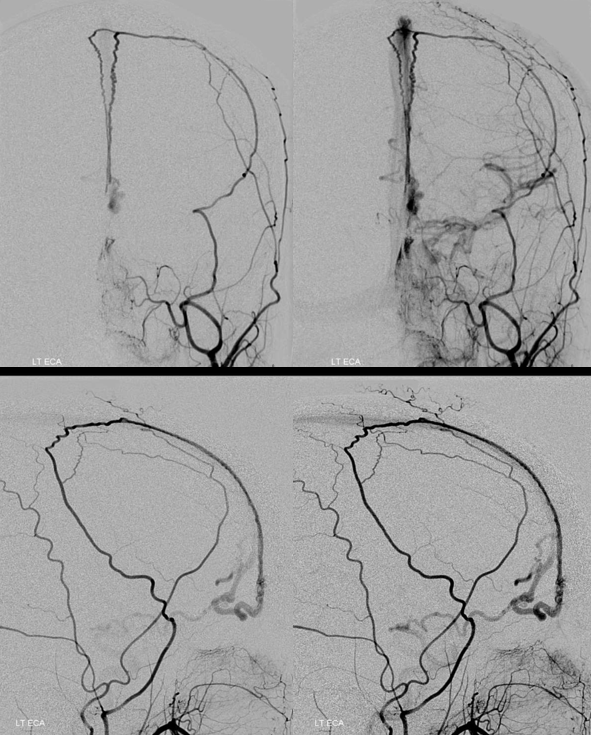
Right side is not contributing mainly via the ethmoid branch of ophthalmic artery
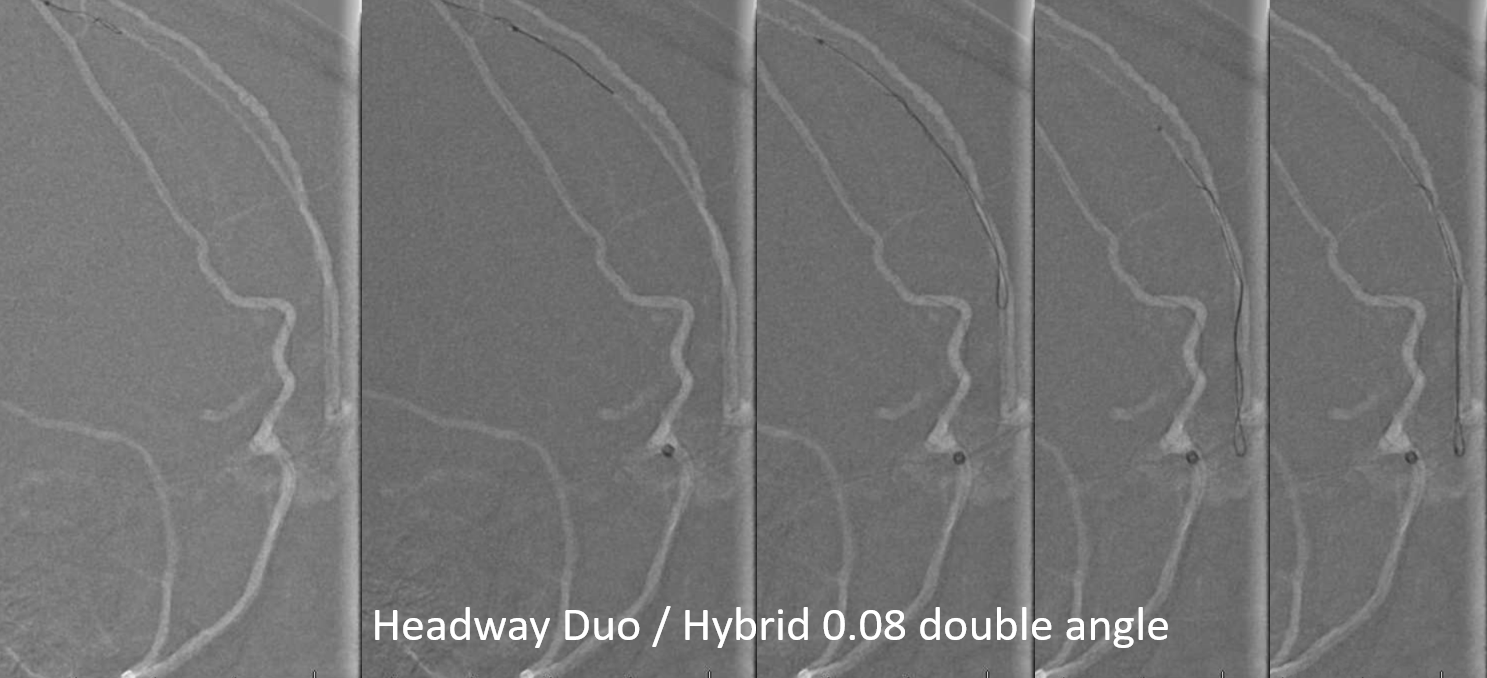
The J-shaped double angle Hybrid wire does its magic, advancing down the entire anterior meningeal artery on its own, with headway duo at the convexity, until the j-shaped wire reaches nearly to the fistula point. The headway follows easily. Noone was certain at all if this was going to work, given multiple tortuosities of the anterior meningeal artery. Mainly, this case is about how improvements in access technology make this kind of treatment possible. Support to duo/hybrid was provided by Phenom Plus 115 cm (seen on far right image)
Lateral views
Micro injection
What embolic agent to use? Onyx is the clear choice here. Why? In the trans-ophthalmic companion case the clear winner was n-BCA. It is important to know properties of both. Here, there is plenty of competing inflow present from bilateral ophthalmic arteries and from other channels of the anterior meningeal artery. These will work against n-BCA, possibly polymerising it before sufficient quantity reaches the venous system (this was not true for the trans-ophthalmic companion case, where the ophthalmic artery was the sole supplier). Second, the Onyx “pull” is not a problem here — we can pull with good confidence in the MMA/AMA (for the trans-ophthalmic case, a zealous pull is obviously not desirable).
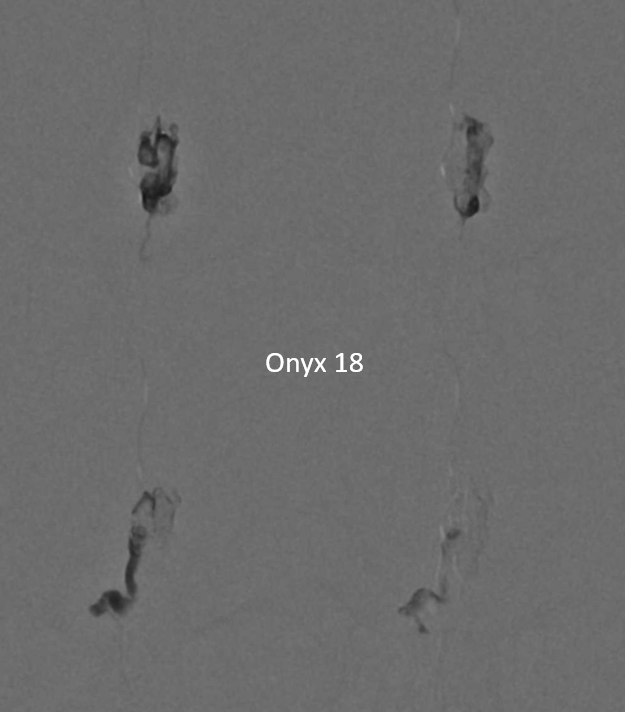
Below are sequential frontal images of Onyx-18 injection
Lateral views
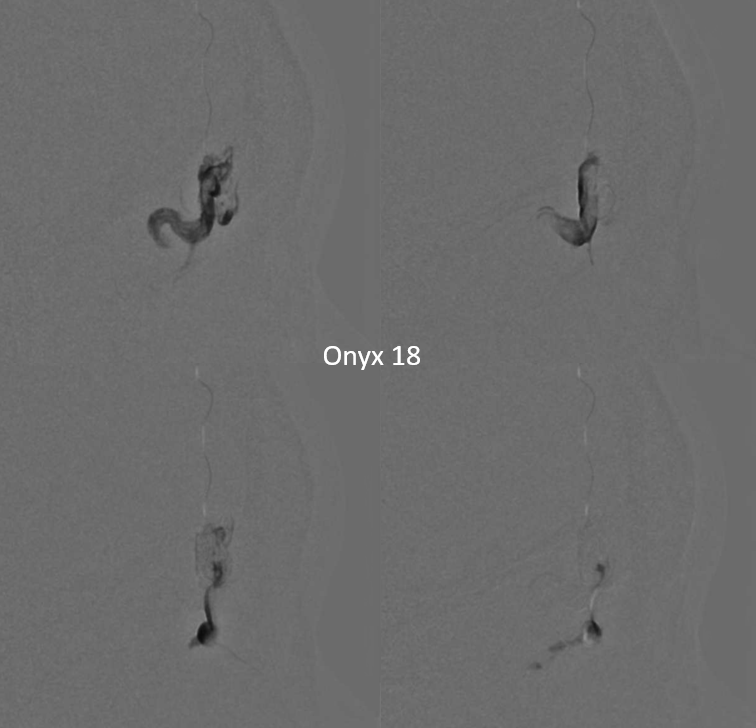
When you are this close to the fistula, and reflux is not an issue, success is as sure as one can ever be
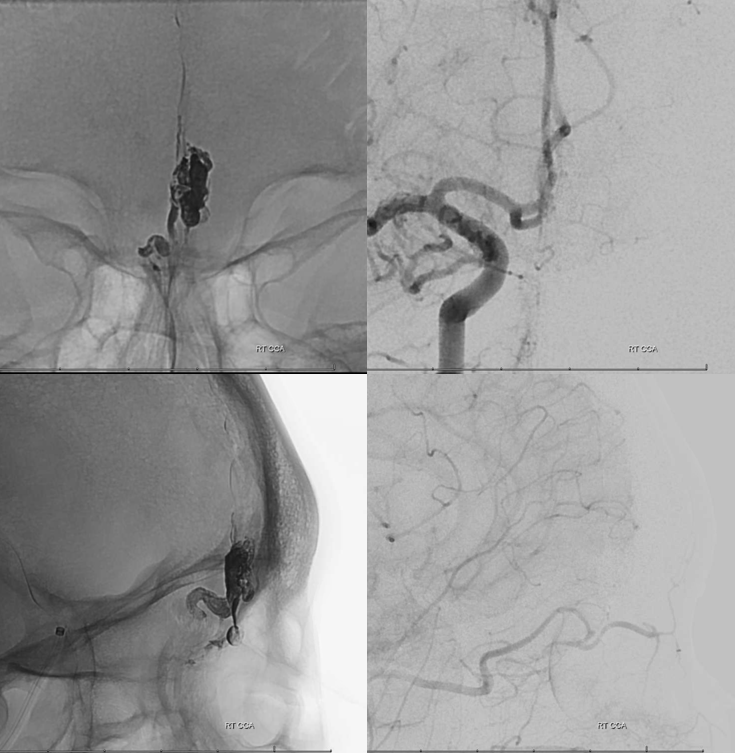
The conclusion is that improving access tools and anatomical understanding are converting another standard surgical target into an endovascular one