
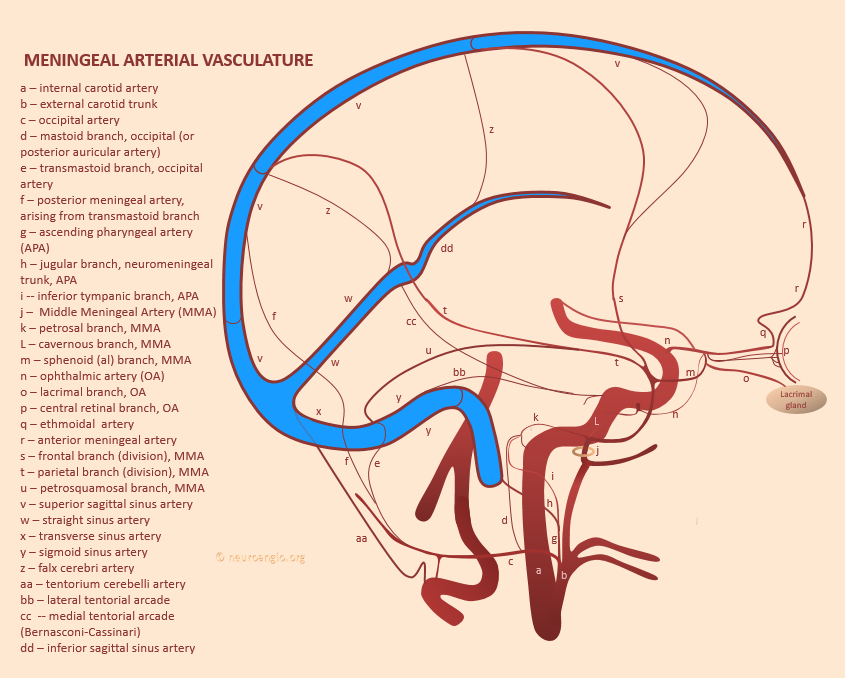
This is an “umbrella page” for meningeal arterial and venous vascular networks. The point is that there is more to the meninges than the Middle Meningeal Artery. The meninges are a highly collateralized vascular network, a critical factor in successful treatment of diseases that involve meninges, such as dural fistulas or subdural hematomas. For specific information on individual vessels contributing to the network, see Ophthalmic, Middle Meningeal, and Posterior Meningeal Pages.
As you see in figure above, it is best to think of meningeal arteries as a network. There is tremendous collateral potential between anterior, middle, posterior meningeal arteries, as well as MHT and PCA for example that often contribute to dural vascularization. Particuarly important are arteries in the walls of dural sinuses, which are the principal connecting anastomotic routes between meningeal arteries and which play key roles in anatomy of dural fistulas for example. Despite their importance they have no consistent names. Here and elsewhere on neuroangio.org we name them according to location such as “superior sagittal sinus artery” or “sigmoid sinus artery”.
Anterior Meningeal Artery (r)– branch of the ethmoid arteries (q), which are in turm branches of the ophthalmic (n). Like any branch, variably well- or under-developed. Runs in the wall of the distal superior sagittal sinus — in fact it is the only named artery that travels in the sinus wall. Usually does not extend beyond anterior frontal convexity, except when middle meningeal arteries are compromised (surgically most often). Contiguous with the “Superior Sagittal Sinus” artery (v) — the anastomotic channel running along the entire SSS.
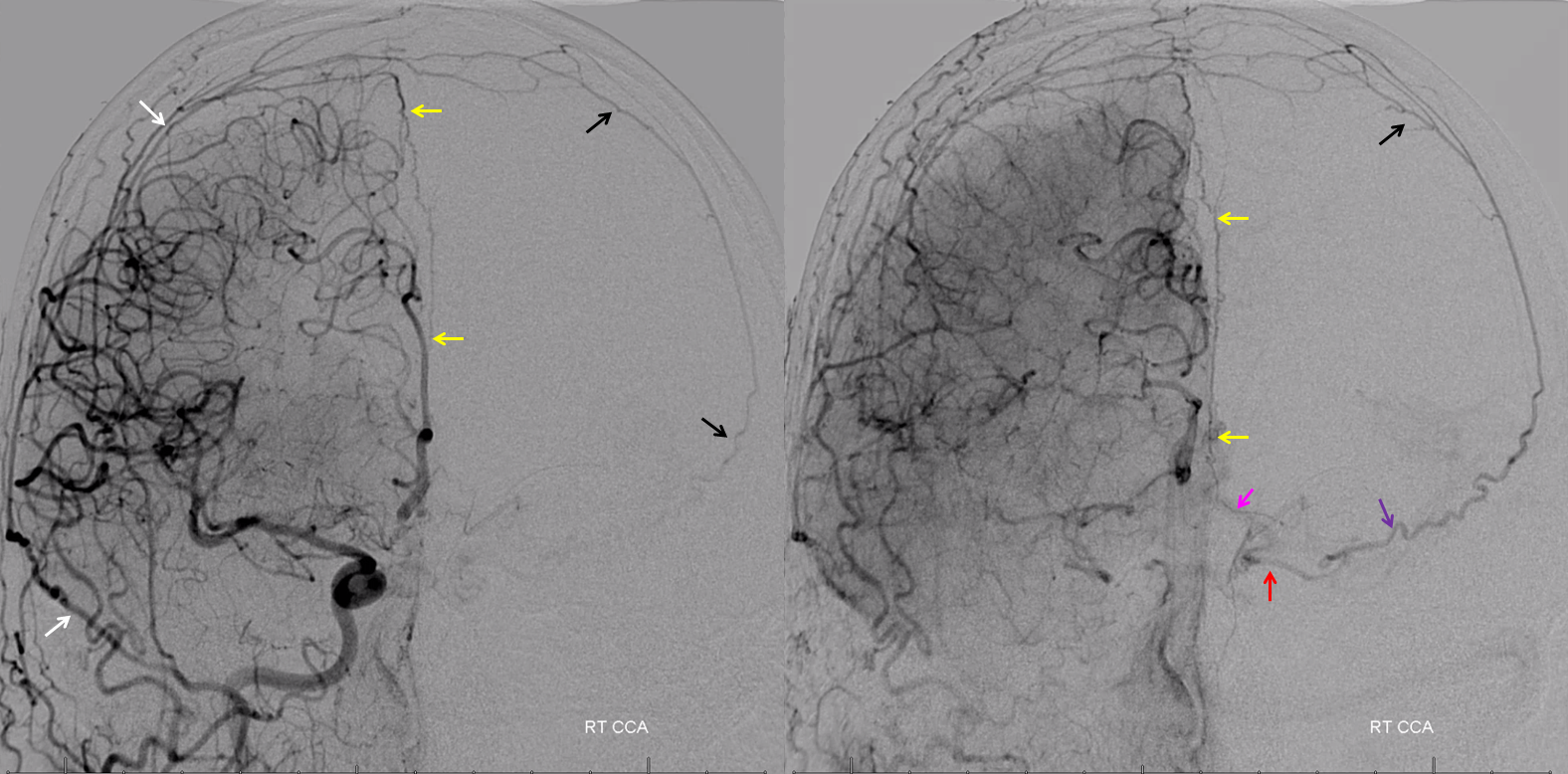
Here is a big one in a patient post pterional craniotomy. See the anterior meningeal bifurcate into two branches (white arrows), one on each side of the SSS. There is even a meningeal blush in parenchymal phase (black arrows). Often the anterior meningeal is obscured by the ACA in frontal views
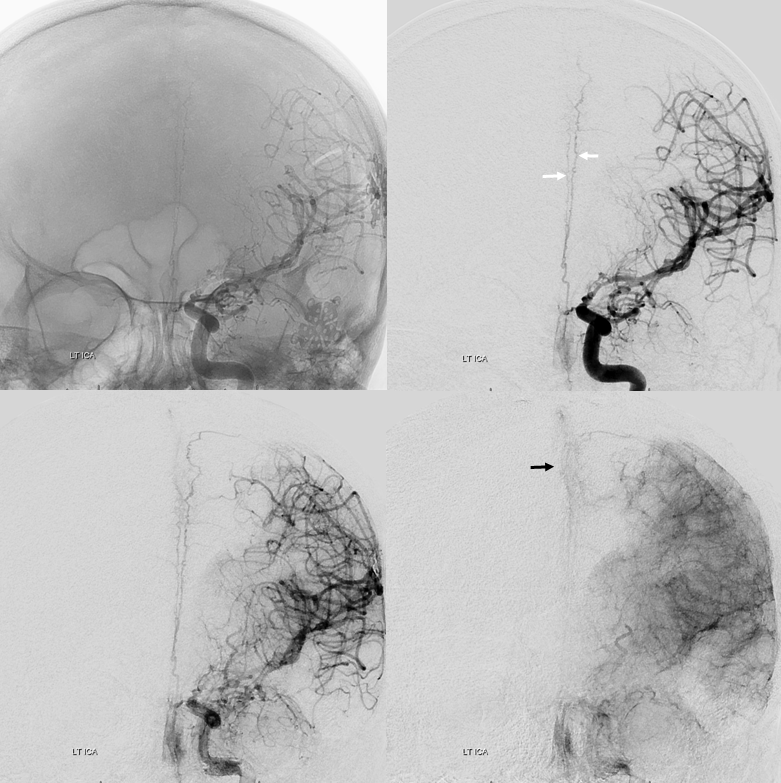
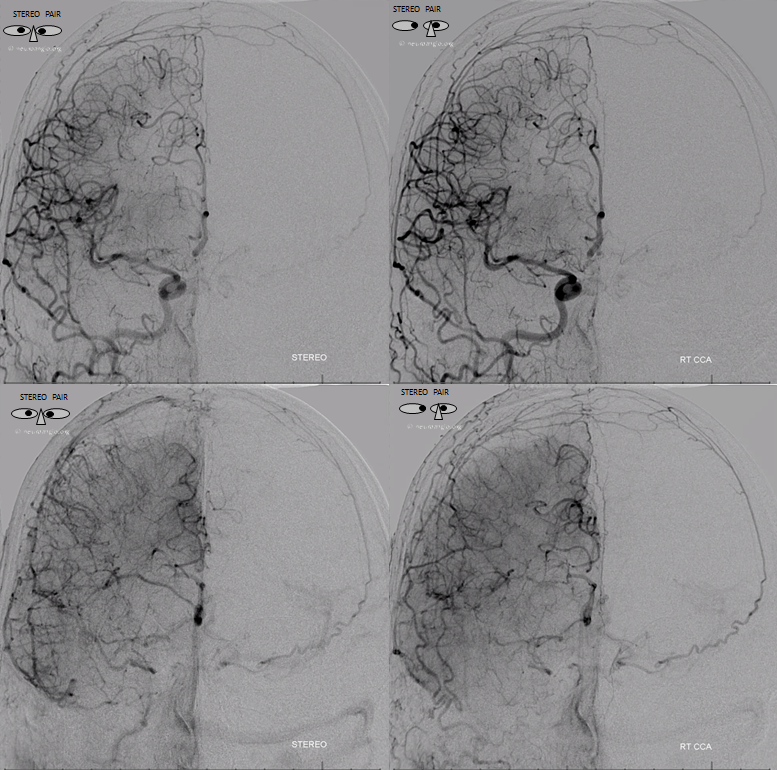
Lateral views
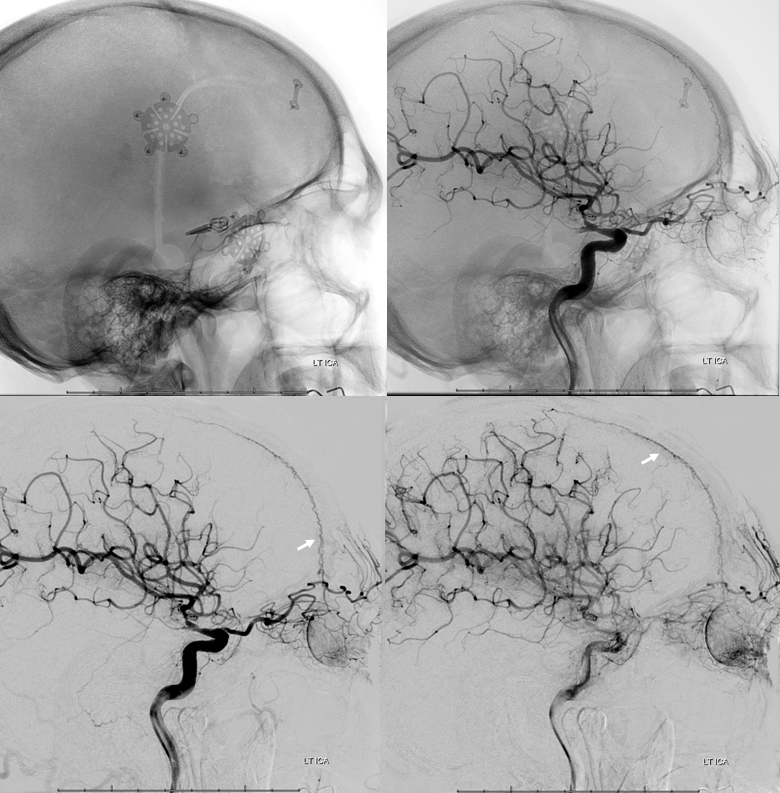
Does not have to be in setting of craniotomy either. Again, there is a balance here — sometimes anterior meningeal is large, while convexity MMA supply is smaller. Here is an example — note how the anterior meningeal splits into two as the SSS becomes larger
On the back end, look at meningeal vessels in wall of the proximal superior sagittal sinus in patient with a torcular fistula. Notice two vessels in parallel on each side of sinus — and a wider separation between them compared with the above image, since the sinus is larger posteriorly
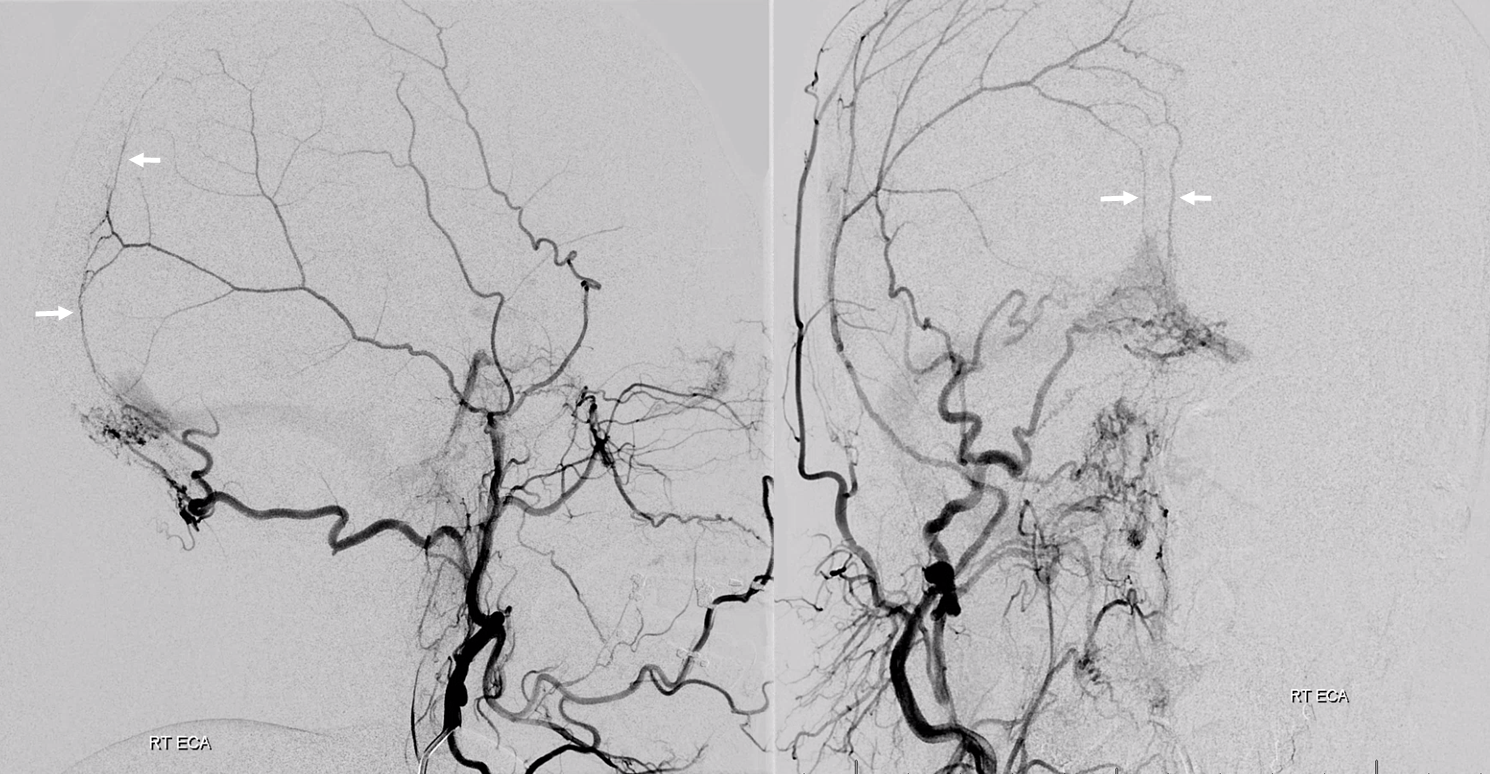
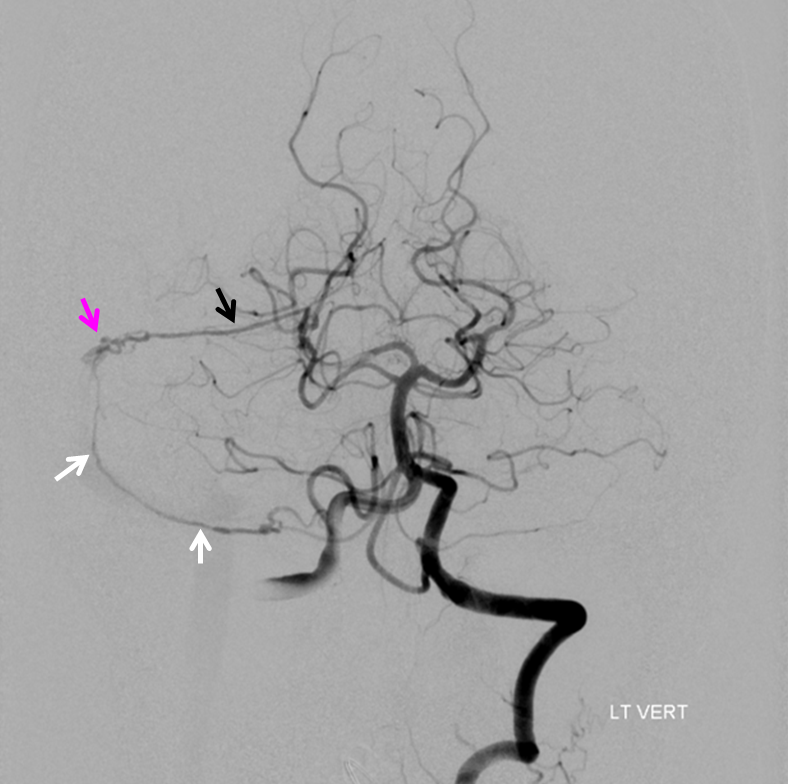
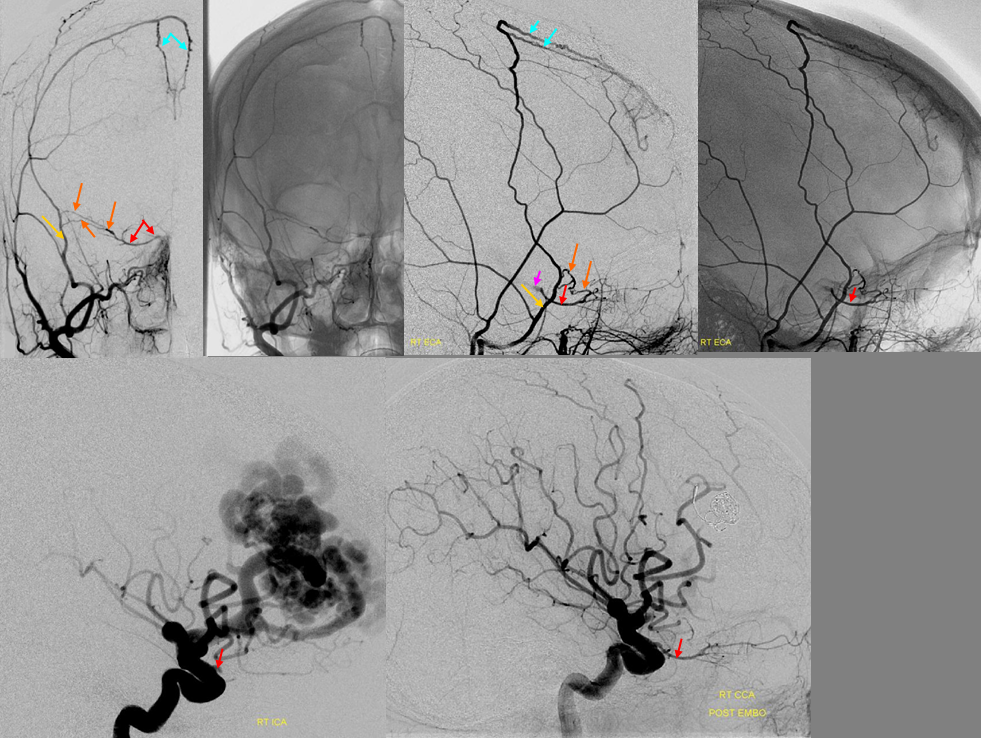
Clinical Significance — patient with left cervical ICA dissection
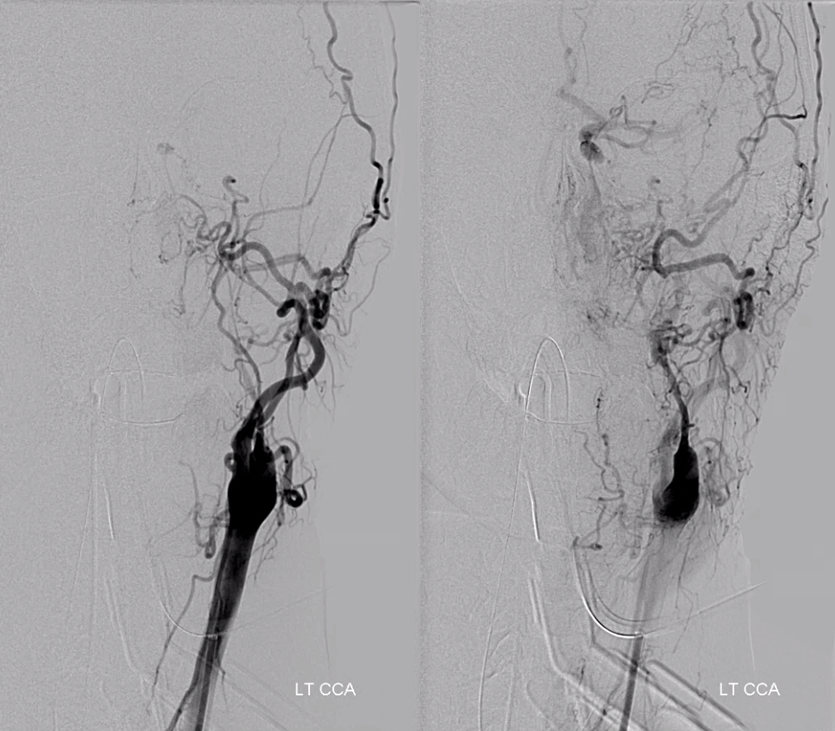
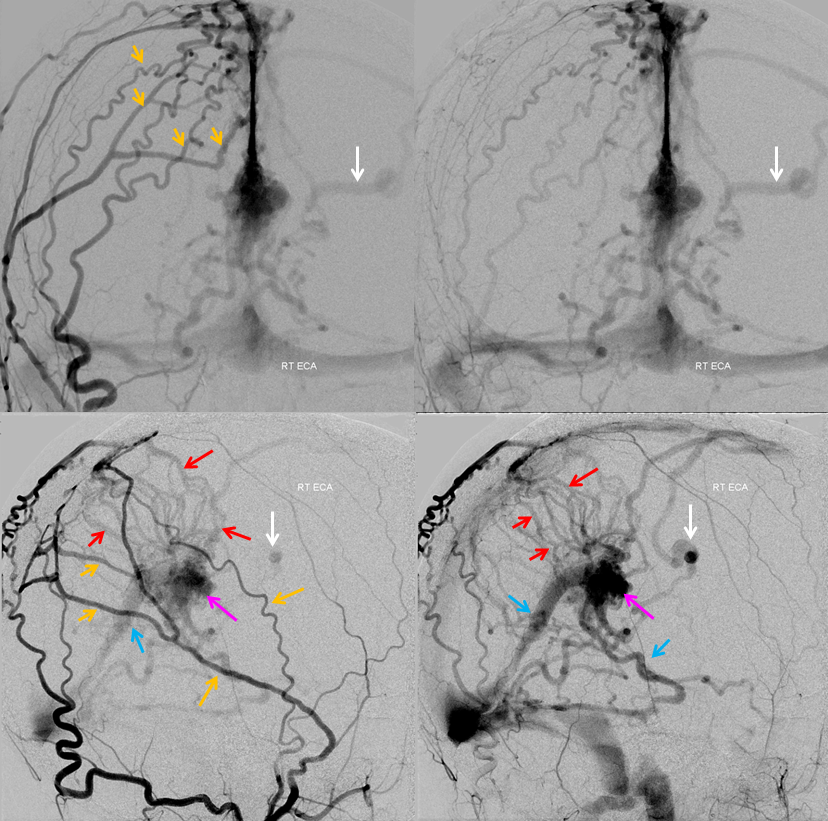
Collateral reconstitution of the left ICA is provided by right MMA (white arrows) to left MMA (meningo-ophthalmic, black arrows; sphenoidal branch -purple arrow) to ophthalmic artery (red arrow)! Notice anterior meningeal branch (yellow) reconstituting ophthalmic via the ethmoid artery (pink arrow). Case courtesy Dr. Eytan Raz
Stereos


Prominent anterior meningeal artery (white arrows) retrogradely supplying ethmoid fistula
Ethmoid Fistula supplied by Superior Sagittal Sinus Artery (white), opacified via frontal branch of MMA (black). Full case is here
![]()
MIDDLE MENINGEAL ARTERY — see dedicated page here
POSTERIOR MENINGEAL ARTERY — see dedicated page here
INTRINSIC MENINGEAL ARTERIES / ARTERIES OF DURAL SINUS WALLS
The intrinsic vascularity of the dura has been under-appreciated, despite frequent visualization of consistently present arterial channels other than named anterior, middle, and posterior meningeal arteries. There is more awareness of intrinsic vascular arrangement and its importance because of subdural hematomas. However of chief interest, to neuroangio.org at least, are arterial channels in walls of dural venous sinuses, specifically at points of dural confluence. Examples of named ones are anterior meningeal artery (in wall of distal/anterior portion of the superior sagittal sinus), the medial tentorial arcade (aka Bernasconi-Cassinari, located in the edge of tentorial leaf), lateral tentorial arcade (extending from MHT to sigmoid sinus along the confluence of dural convexity and tentorium cerebelli). However, other vessels, which as just as prevalent, located in walls of transvers, sigmoid, straight, and proximal/posterior sagittal sinus, are under-recognized and un-named. These are frequently seen in any condition that result in more flow, either globally (dural fistulas, meningiomas, etc) or when rearrangements such as pterional craniotomy require collateral reconstitution. According to figure below, these vessels are here named based on where they are found, such as “superior sagittal sinus artery” or “sigmoid sinus artery”. There is bound to be overlap, just as transverse sinus transitions to sigmoid sinus. Likewise, the distal or anterior-most portion of the “superior sagittal sinus artery” is the same vessel as Anterior Meningeal Artery.
Examples of dural arteries in walls of sinuses
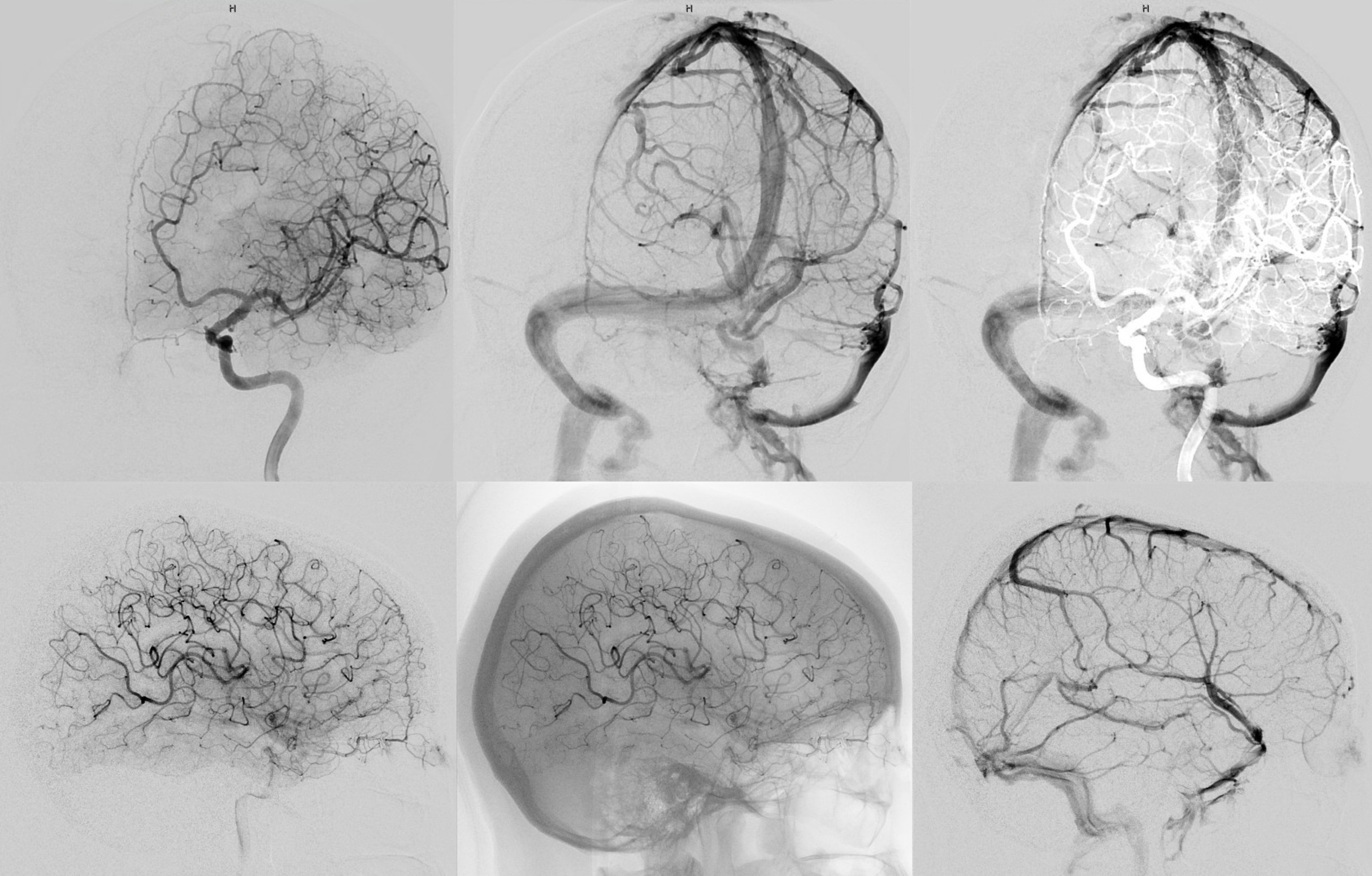
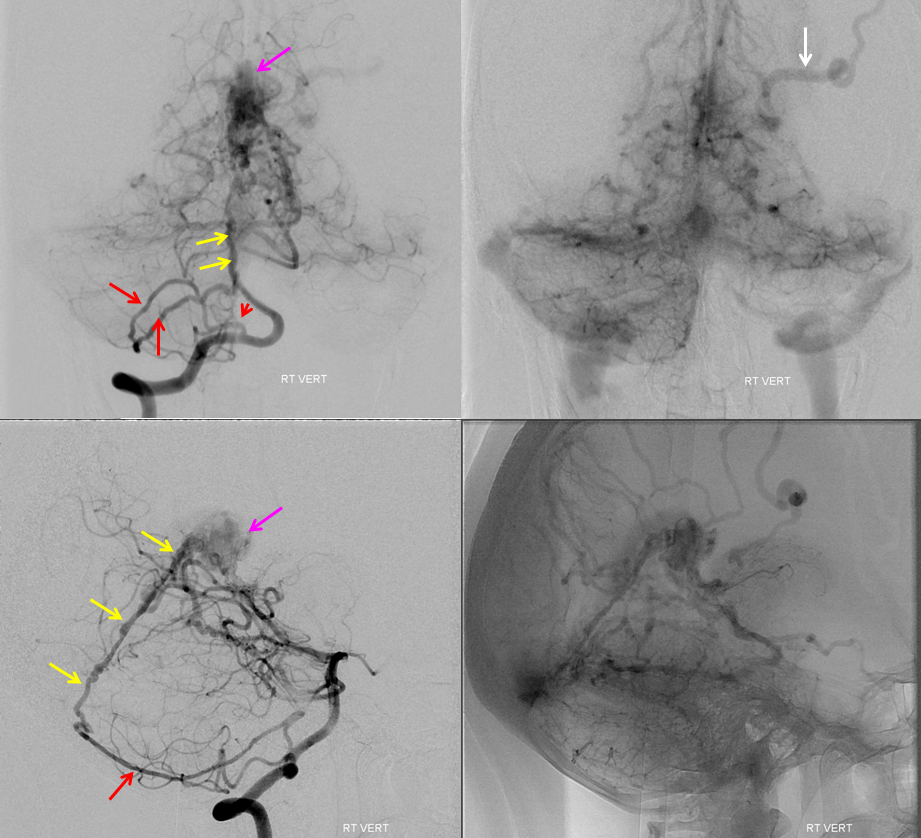
In this patient post bilateral pterional craniotomies with secondary MMA sacrifice, the whole territory fills from posterior meningeal arteries. The artery of the tentorium cerebelli (red) gives rise to the posterior meningeal artery, whose territory has considerably extended due to bilateral MMA sacrifice, demonstrating an impressive meningeal network (yellow arrows)

Same, in beautiful stereo

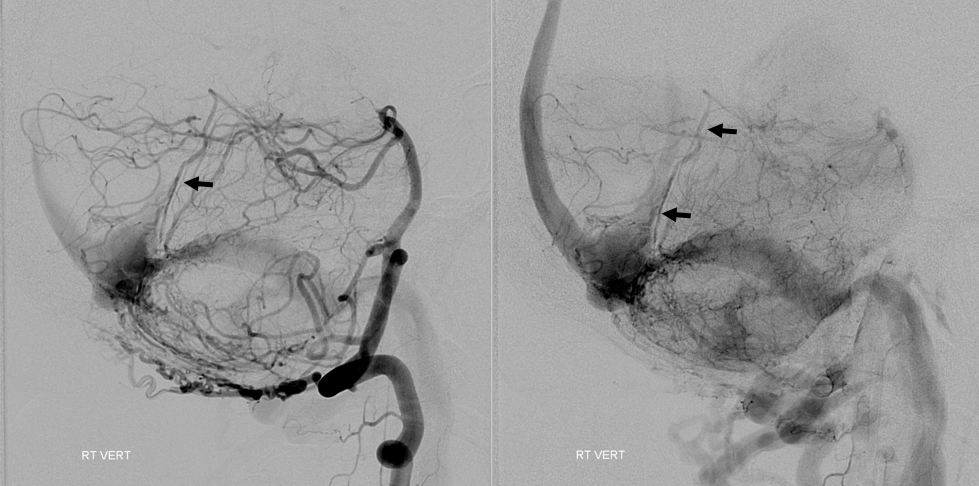
Below is a normal angiogram with well-developed arteries of tentorium cerebelli (white arrows, aa) and artery of the inferior sagittal sinus (black arrows, dd). The letters correspond to ones of the diagram above. The tentorium cerebelli artery extends beyond the torcular region where it is labeled as the artery of the superior sagittal sinus (pink arrows, v). This is analogous to the anterior meningeal artery in the wall of the distal superior sagittal sinus.

Anaglyph stereo below
Ethmoid Fistula supplied by Superior Sagittal Sinus Artery (white), opacified via frontal branch of MMA (black). Full case is here
![]()
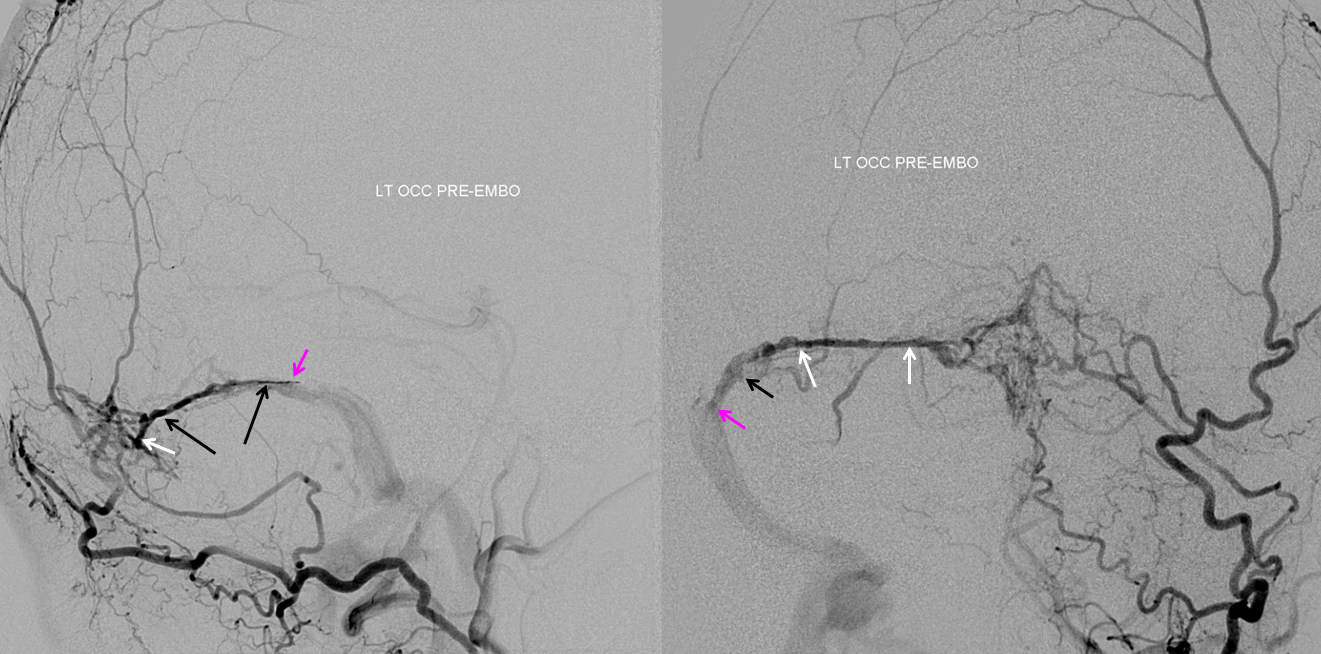
Sigmoid Sinus Fistula
Pial and posterior meningeal supply to sigmoid sinus fistula (pink) opacifying arteries in wall of the sigmoid sinus (white) and transverse sinus (black). Full case here
Sigmoid Sinus Fistula 2
Another patient with a sigmoid sinus fistula — multiple contralateral posterior meningeal and cutaneous occipital branches converging on Artery of Transverse Sinus (white) leading into Artery of Sigmoid Sinus (black) that forms a common arterial collector opening into the fistula (pink)
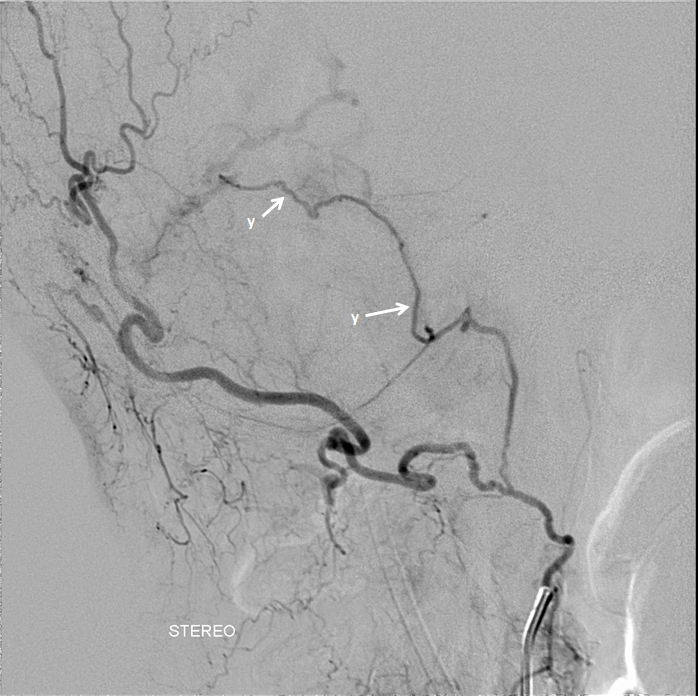
Sigmoid Sinus Fistula 3
Beautiful demonstration of “sigmoid sinus branch”. A fistula in “trapped” segment of sigmoid sinus, supplied by MMA and ascending pharyngeal artery. The latter is a pharyngo-occipital variant, with the jugular division of the neuromeningeal trunk supplying the fistula via the “sigmoid sinus branch” (white arrows, v)
 \
\
Anaglyph stereo views
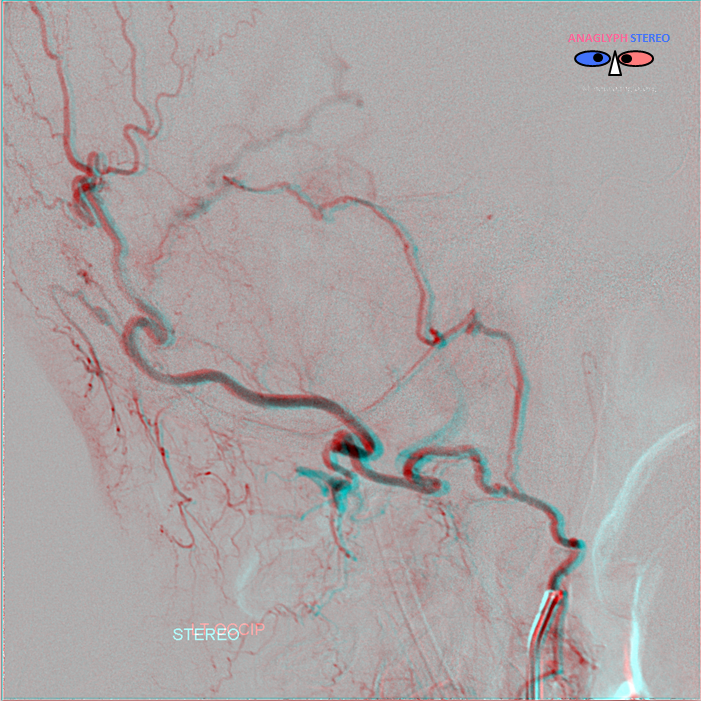
Below is the middle meningeal artery petrosquamosal branch (white, purple) supply to the fistula. The fistula point (red) is located in a trapped segment of the sigmoid sinus, draining via an ectatic inferior temporal vein (pink) into the Galen (Cognard IV, Borden III)
cross-eye stereos
Anaglyph stereos
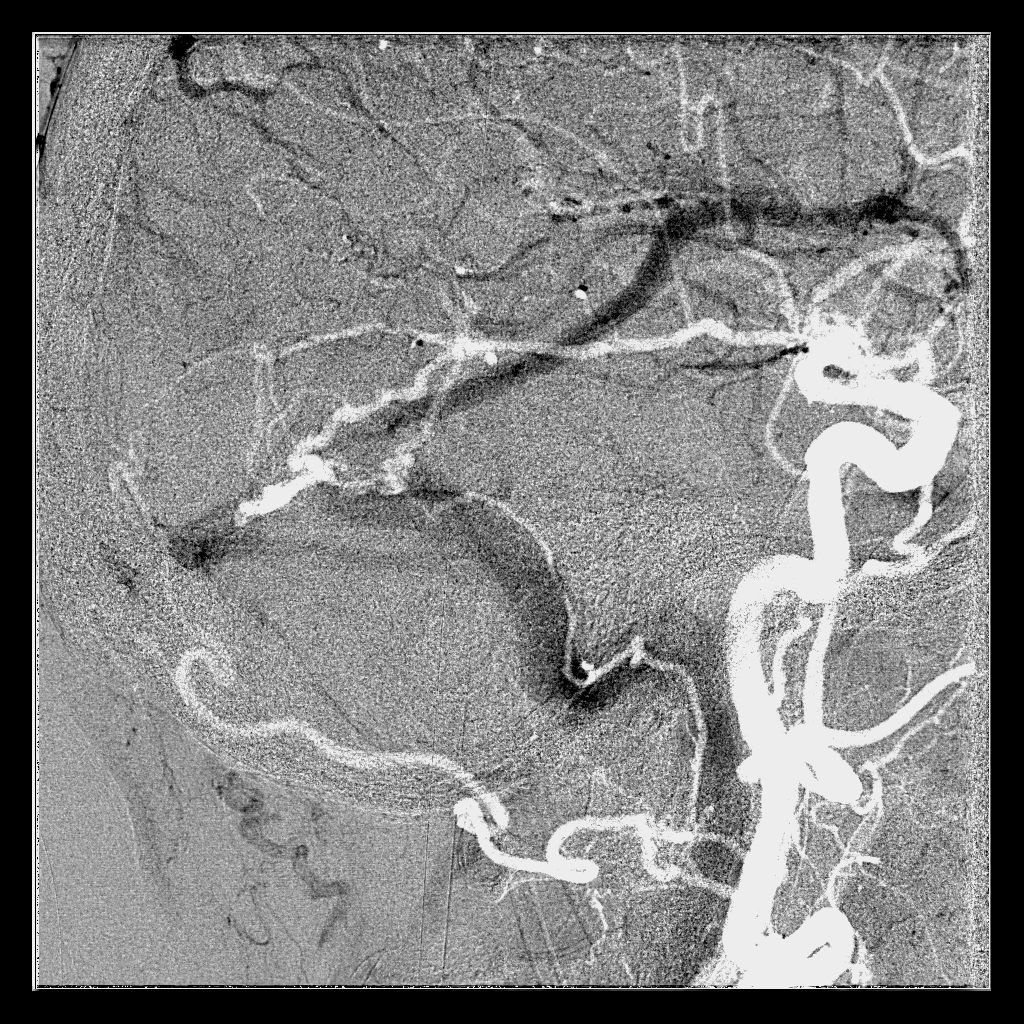
Finally, common carotid injection with arterial phase mask shows artery of the sigmoid sinus paralleling the course of the sinus
Torcular Fistula
Complex Sigmoid / Torcular fistula (top row) with supply to the torcular fistula (pink) via paired Superior Sagittal Sinus Arteries (white arrows) opacified by parietal branches of the MMA (black arrows)
Same case, image below — supply via artery of the straight sinus (black arrows)
Multiple arteries in wall of the falx cerebri — “falx cerebri arteries” (red arrows) supplying a falcotentorial junction fistula (pink). Full case is here
Same case, with posterior meningeal artery (red) opacifying the artery in wall of the straight sinus — “straight sinus artery” (yellow). Fistula point is pink again.
AVM
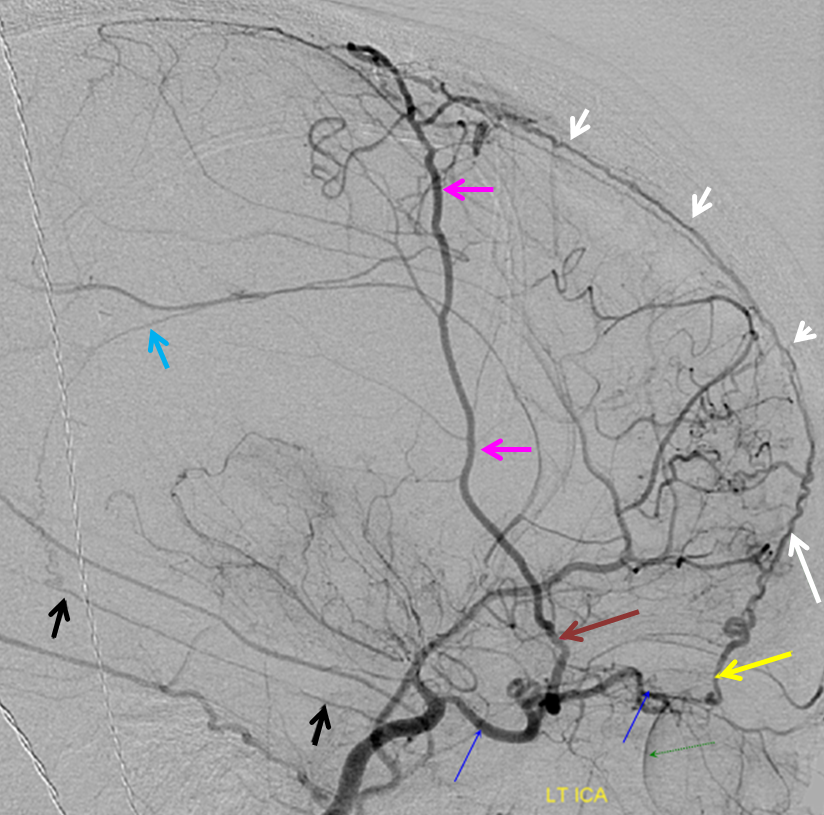
Sump from AVM reverses flow in the ophthalmic artery (red) with primary retrograde supply via the sphenoidal artery (orange) branch of the MMA (yellow). As a consequence of AVM reorganization, an autosynangiosis of the mid-sagittal anterior frontal convexity developed, supplied by two Superior Sagittal Sinus Arteries (blue arrows).
Post-radiation vasculopathy — a sad case of total brain irradiation in a child, treated abroad for a presumed malignancy. Years later there is extensive Moya-Moya like change. There are multiple meningeal autosynangioses, with a prominent anterior meningeal artery (the anterior part of Superior Sagittal Sinus artery — white arrows) forming a network with frontal branch (pink) of MMA (recurrent meningeal variant, sphenoid branch = brown arrow). Also notice medial tentorial (Bernasconi-Cassinari) branch (black arrows) of MHT supplying dural branch in the wall of inferior sagittal sinus (light blue arrow). The separate pericalossal arteries are faintly seen slightly higher
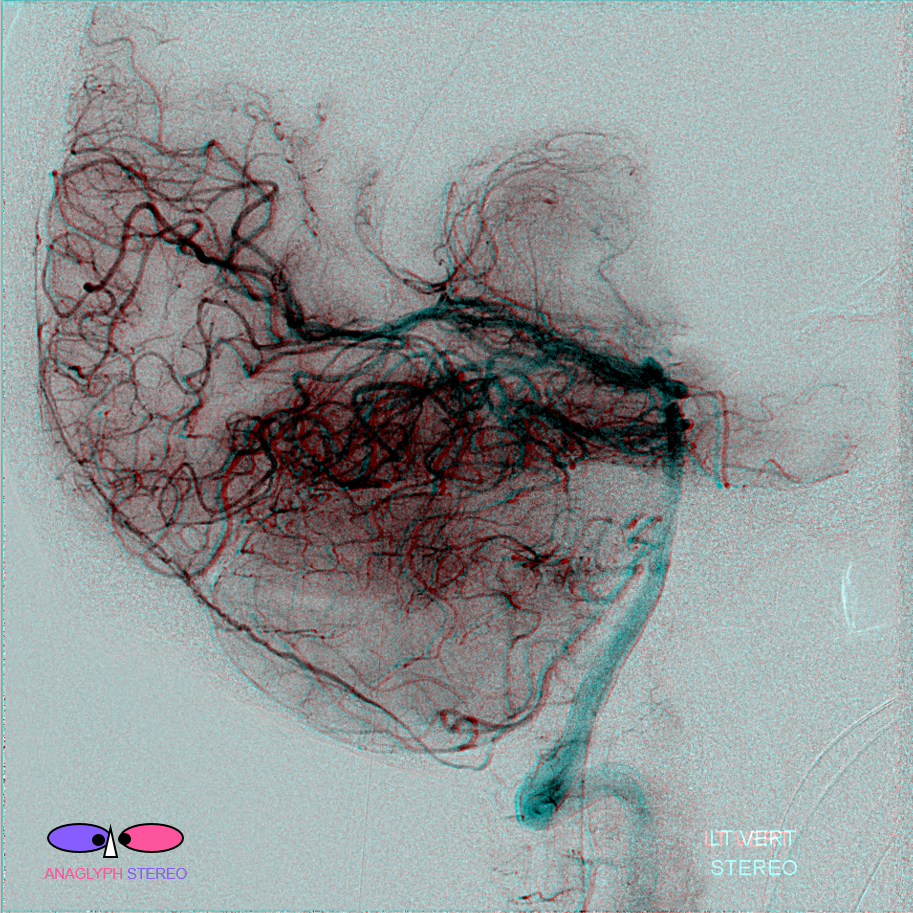
Surgical Dural Synangiosis
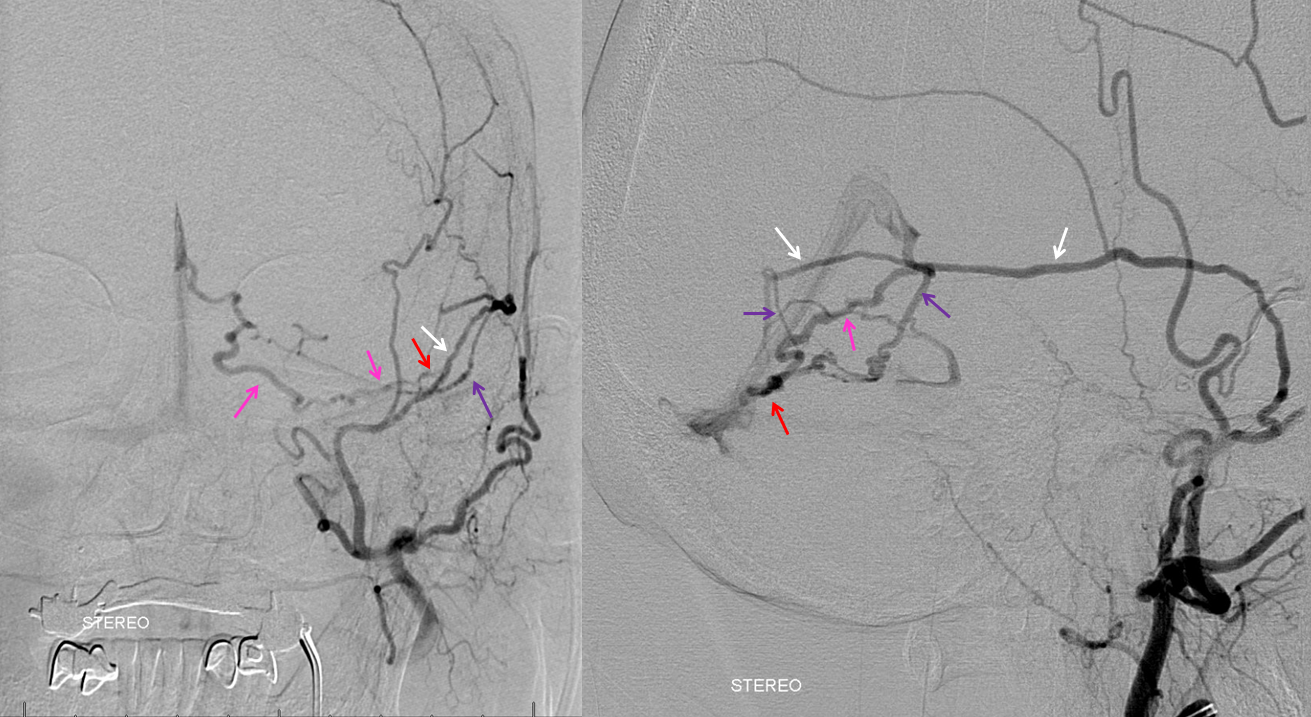
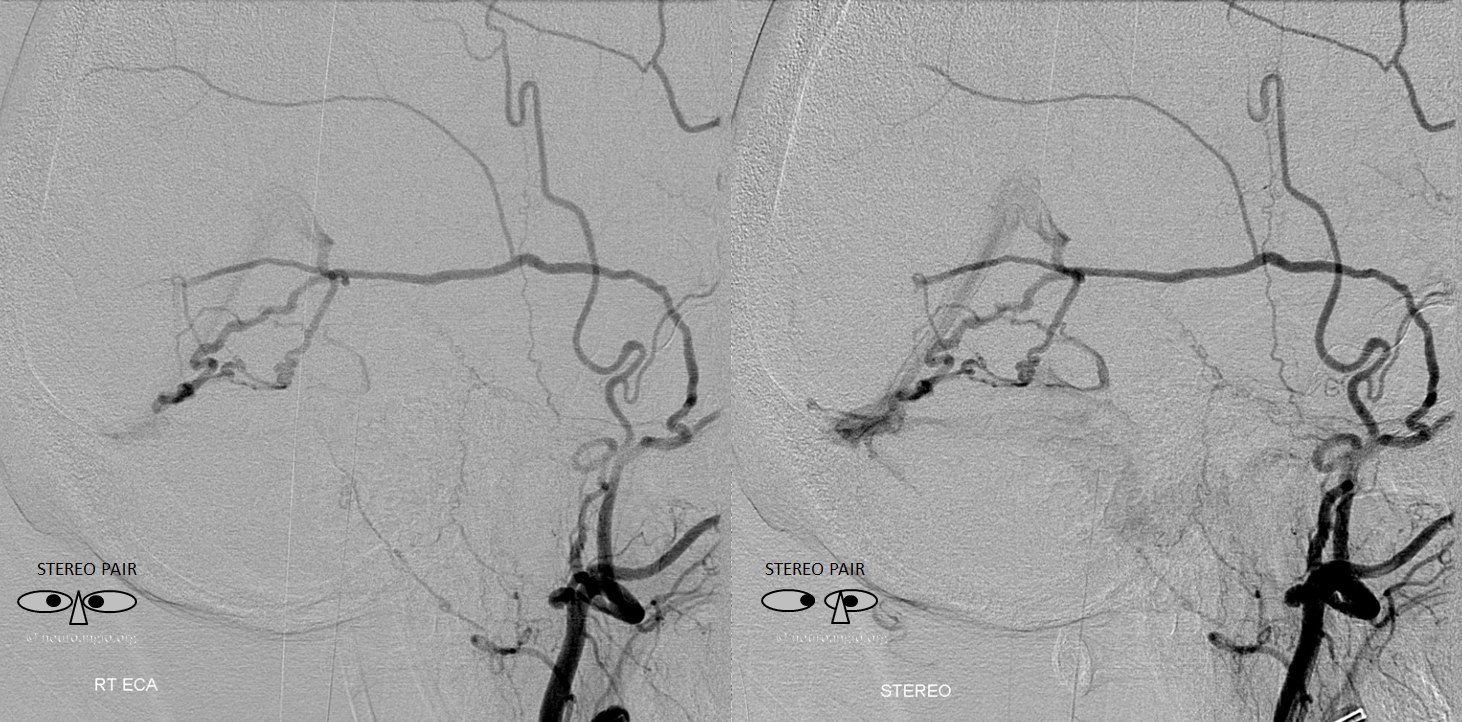
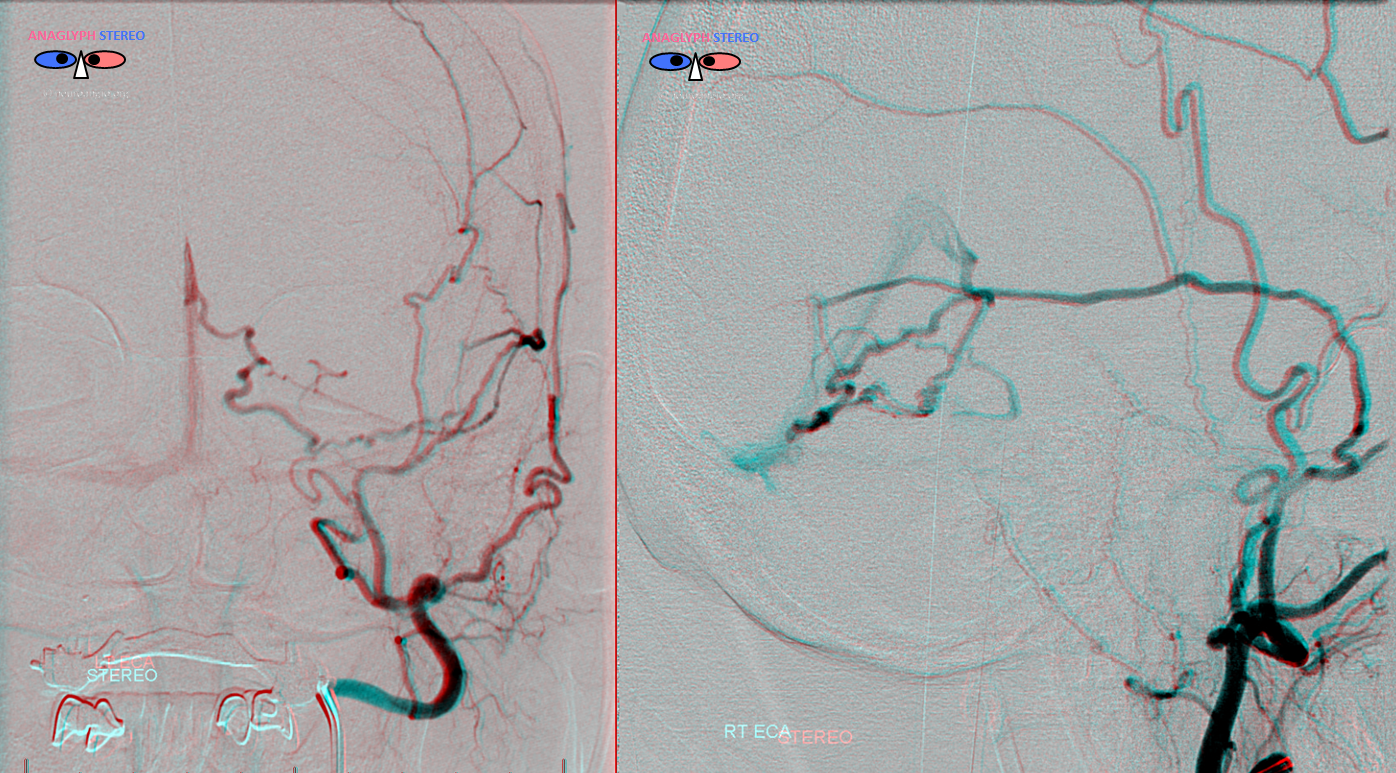
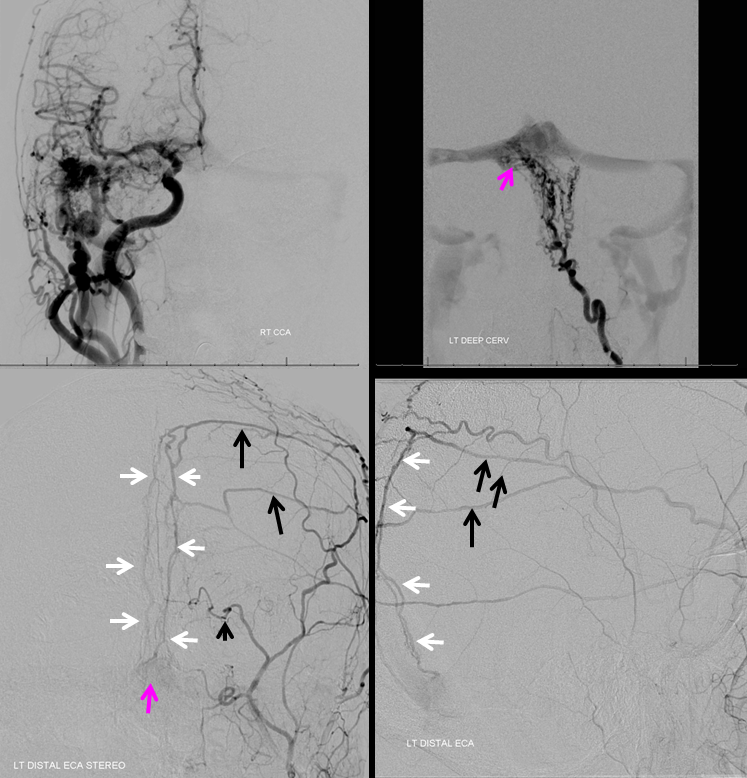
Patient with bilateral Moya-Moya, post bilateral dural synangiosis and burr hole (see Intracranial Collateral Pathways for the remainder of this case). Stereo image pair on top, with dural/ arterial vasculature in white, and venous outflow in black, outlining an arterial arcade which runs within the dural sheath of the transverse/sigmoid sinuses, partly made up by the jugular branch of the neuromeningeal trunk of the ascending pharyngeal artery. Anastomoses with middle meningeal and occiptal branches are clearly demonstrated. These arteries frequently participate in supply of sigmoid sinus dural fistulas.
. 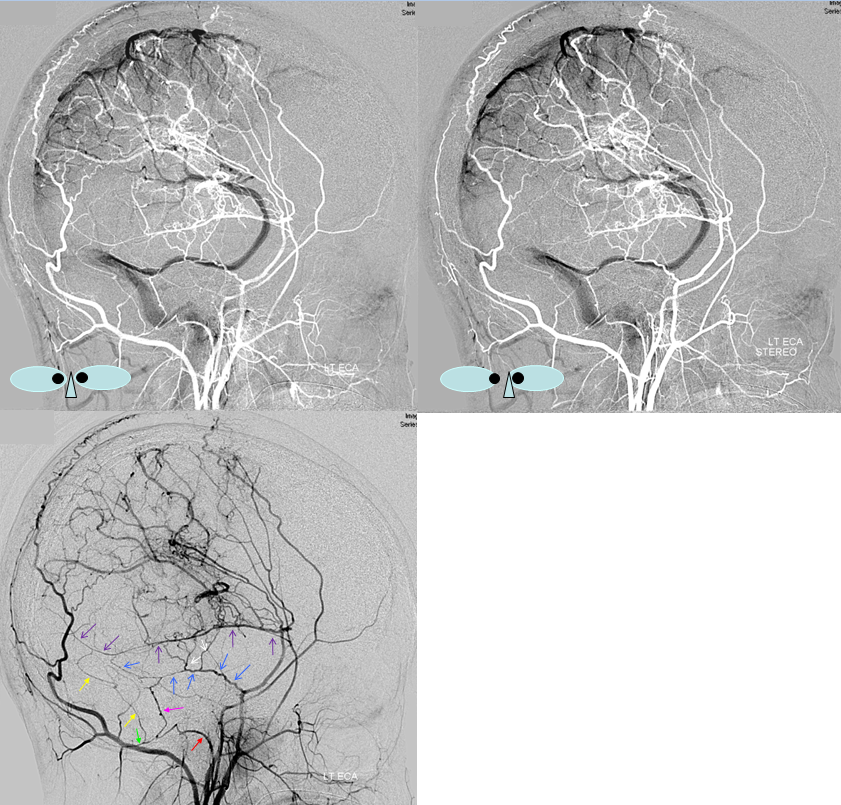
•Red – ascending pharyngeal artery, neuromeningeal trunk
•Pink – superior sigmoid sinus branch, supplied by jugular division of the neuromeningeal trunk
•Blue – middle meningeal artery, basal tentorial branch
•Purple – middle meningeal artery, petrosquamosal branch
•White – anastomotic connections between basal tentorial and petrosquamosal branches
•Green – transmastoid branch, occipital artery
•Yellow – inferior sigmoid sinus branch