
By Eytan Raz and Maksim Shapiro
Consistent visualization of normal Central Retinal Artery (CRA) is now possible 100% of the time with Cone Beam CT (CBCT). In our case, its DYNA CT. This was pioneered by Eytan Raz. The main page for overall topic is Ophthalmic Artery. In this page we focus on Central Retinal Artery AND on another pioneering topic — vascular supply of the optic nerve. The CRA is mainly responsible for distal optic nerve and retina. What about proximal optic nerve? Its a very small volume structure and supplying vessels will be tiny. However, as you will see, visualization is possible under some conditions.
Central Retinal Artery

About 200-250 microns in diameter (relevant for particle embo). DOES have some collaterals with ciliary arteries, but generally insufficient in cases of acute occlusion as far as we know — especially for central vision. Usually arises where ophthalmic artery swings either below or above the nerve — see above. Very difficult to see on angio — especially to distinguish from cililary arteries — and 100% consistently seen on DYNA — as pioneered by Dr. Eytan Raz. For practical purposes, staying well distal to the ophthalmic artery bend is best if embolization in ophthalmic territory is contemplated — see examples of cases here.
Orbital Metastasis Pre-Operative Embolization
Ethmoid Fistula Ophthalmic Artery Route Embolization
Orbital AVM Preoperative Embolization — particularly important case to highlight anatomy, various ophthalmic-ECA anastomoses, nBCA technique, etc.
The choroid blush can be present on angio with CRA occlusion, since the bulk of this blush is made by ciliary arteries, and not the CRA. In other words, having a choroid blush does not mean much — one can be blind with it and see without it — but it is psychologically relevant to the operator.
In the case below, there is extensive nBCA cast (right image) in the meningo-ophthalmic artery (pre-nBCA image on left — arrowheads on both) after a disastrous glue injection
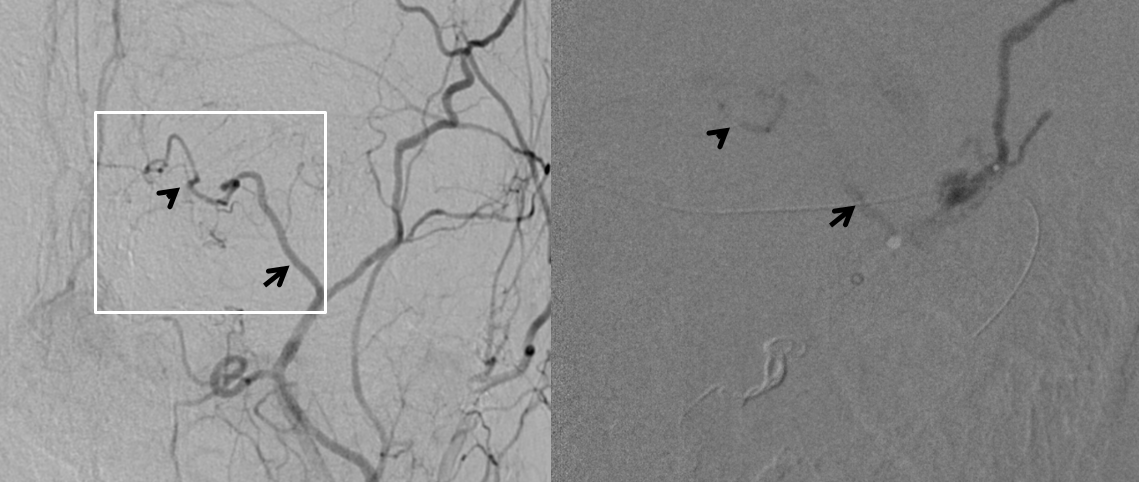
Post ICA and ECA injections show neither choroid blush not any evidence of ophthalmic artery at all — granted the phase is early, maybe something would show up in venous phase

The patient woke up with perfect vision — and stayed that way. This is certainly due to overwhelming good fortune — and a major cautionary tale — but it shows that one can have vision without at least 2-D angiographic evidence of choroid blush
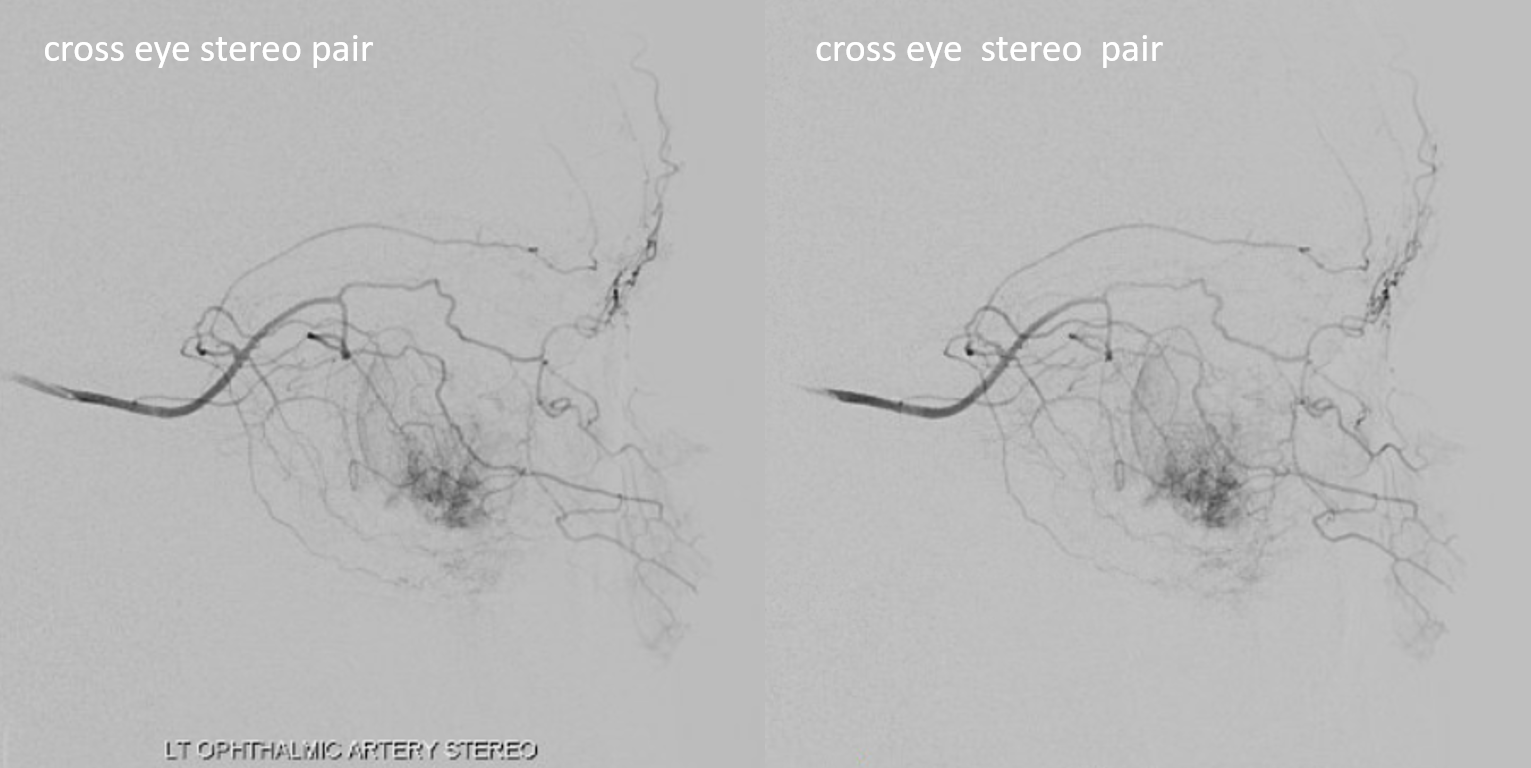
Below is a typical lateral stereo of ophthalmic artery injection. The choroid blush is well-seen. It is impossible to say however which is the CRA
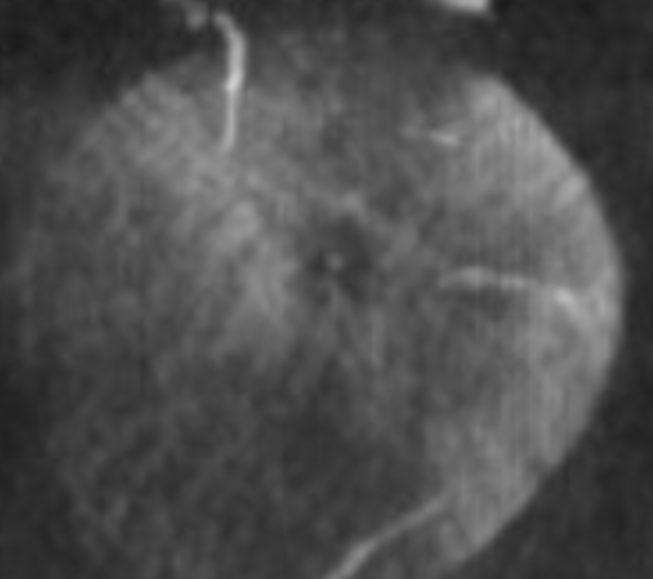
DYNA thin MIP view of the same injection with excellent view of CRA — note typical over the optic nerve angle of the artery
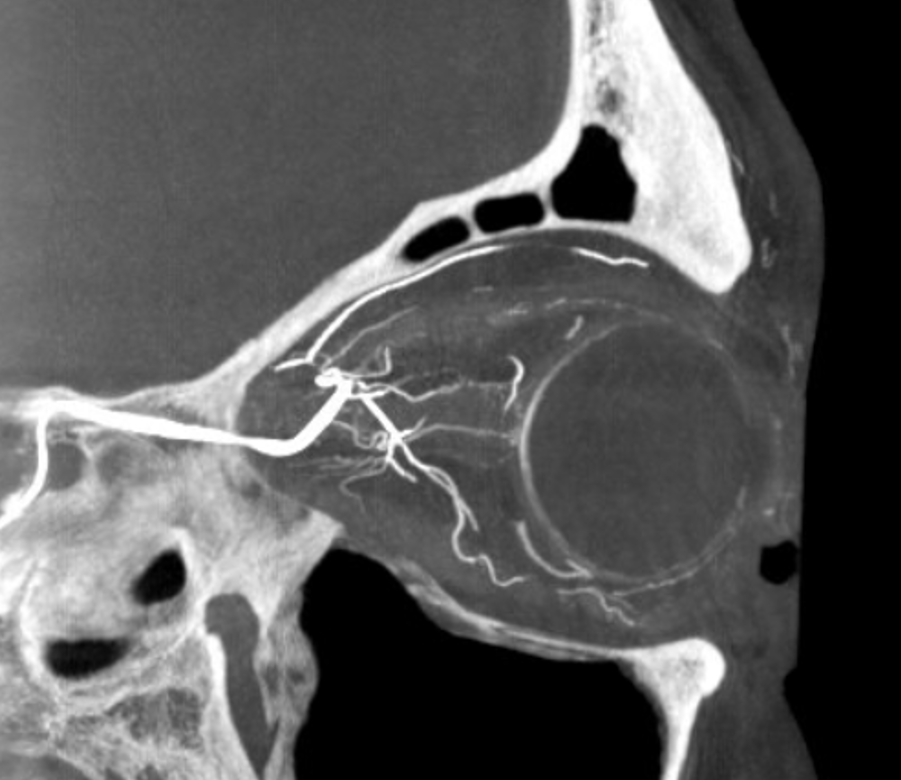
a thinner MIP shows the optic cup
Optic Disk can usually be appreciated in coronal views. This is the limit of current resolution — of course vastly inferior to fundoscopy. But, for anything posterior to the globe — DYNA is by far the best we have
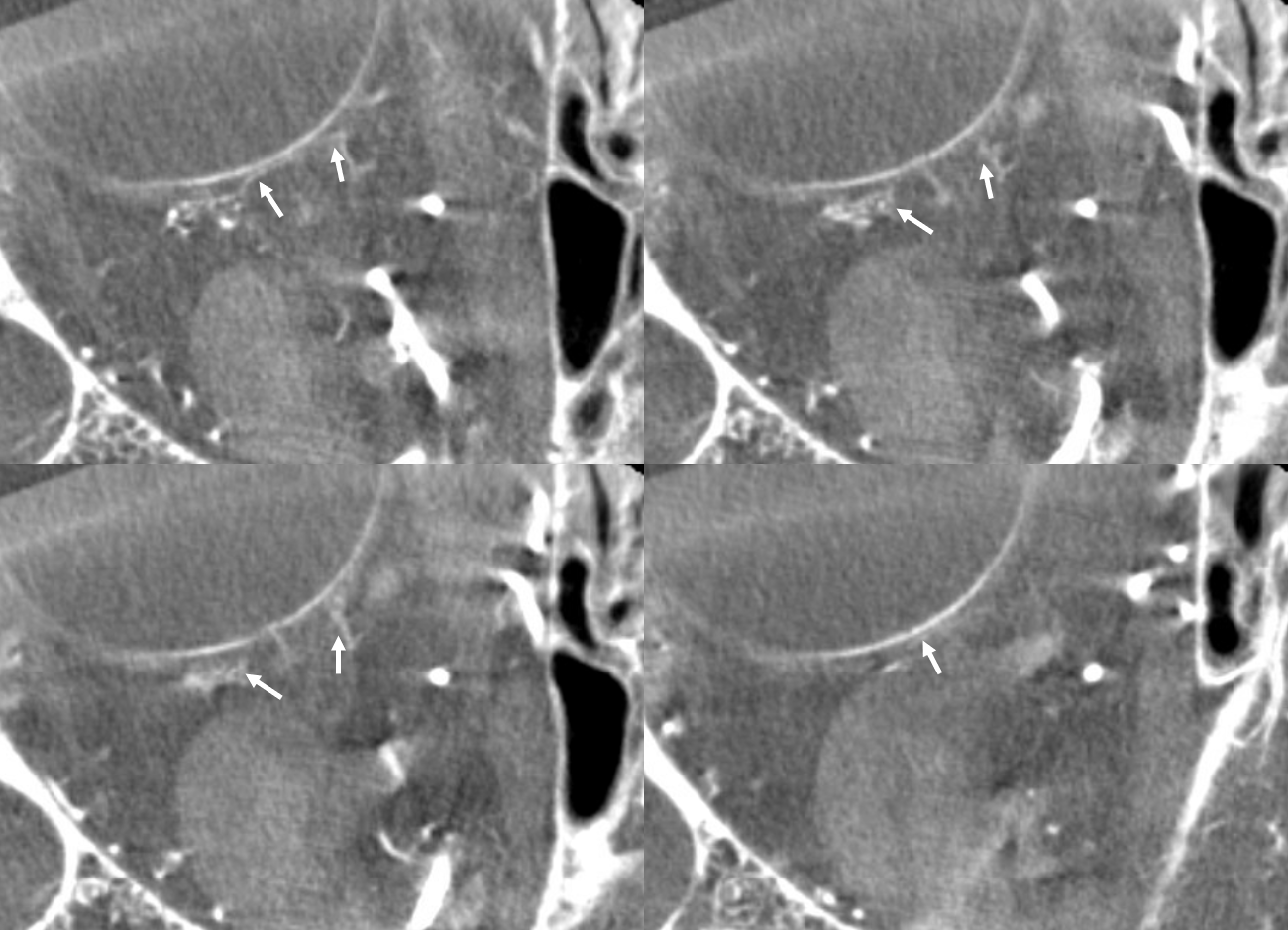
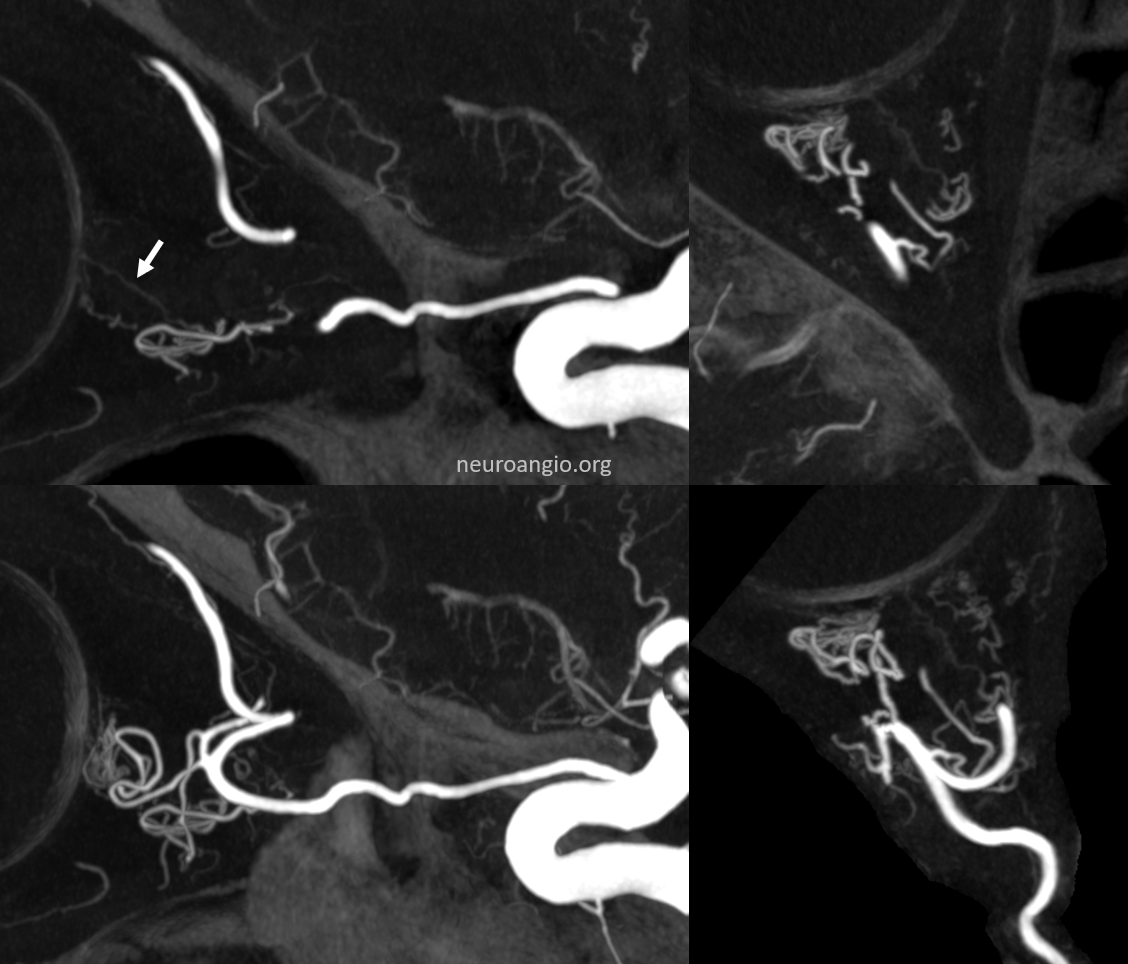
A duplicated central retinal artery (arrows below) converging on single vessel in this case is not so rare — again the more you look the more you see.
A large ciliary artery is present in this patient also — in this case arising more proximally than the CRA — also see DSA images of the same case above

Below is a movie of axial, coronal, and sagittal DYNA images of this patient — pause it and scroll thru individual frames.
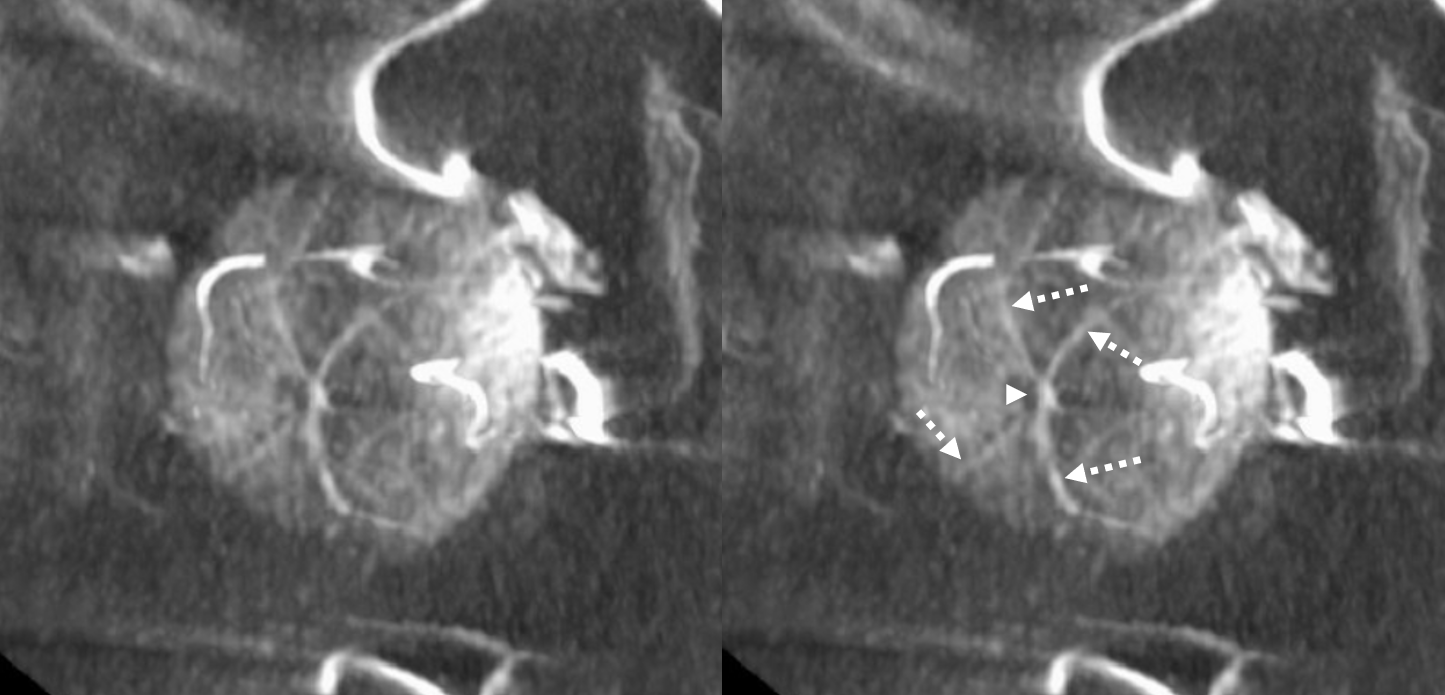
Circle of Zinn-Haller — yes, we can see that also…
Axials
Movie — axial
Movie — coronal oblique perpendicular to optic nerve — notice faint vessels supplying the more proximal portion of the optic nerve — canalicular and orbital apex segments, as well as the Zinn-Haller…
Central Retinal Origin from Ciliary Trunks
Extremely import is to know the classic origin of the central retinal from the more proximal ophthalmic artery (at the “bayonet” segment in the more typical configuration). This makes it possible to embolize more distal ophthalmic targets such as ethmoidal branches in cases of dural fistula with more confidence. The ciliary arteries contribute to supply of the retina also in up to 30% of cases classically — which means one can have a proximal CRA occlusion and tolerate it.
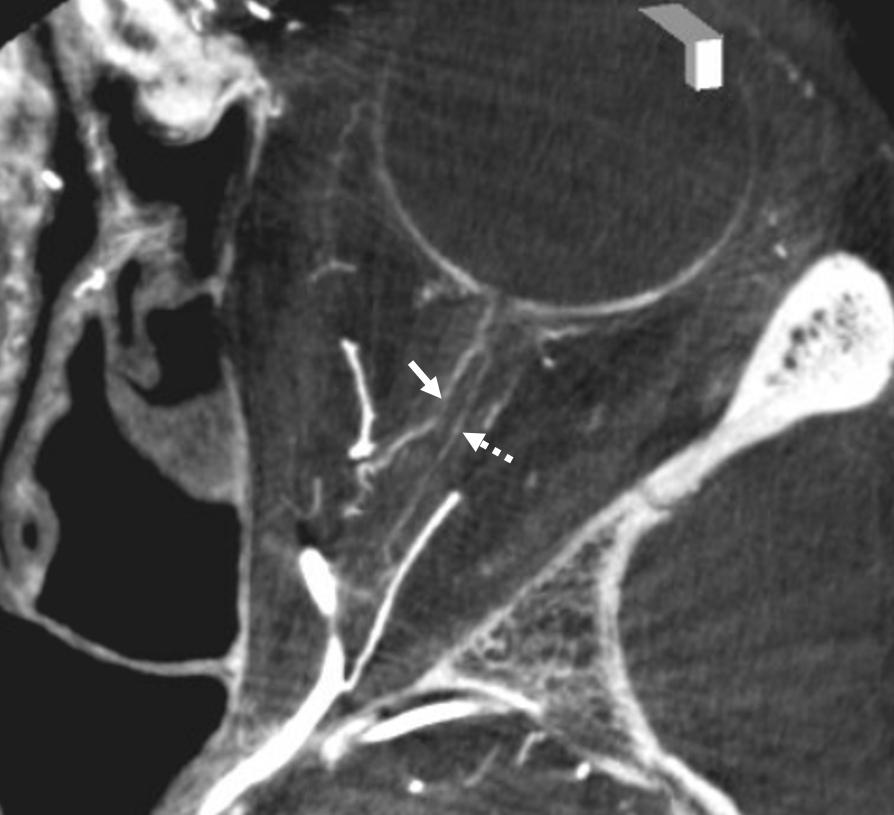
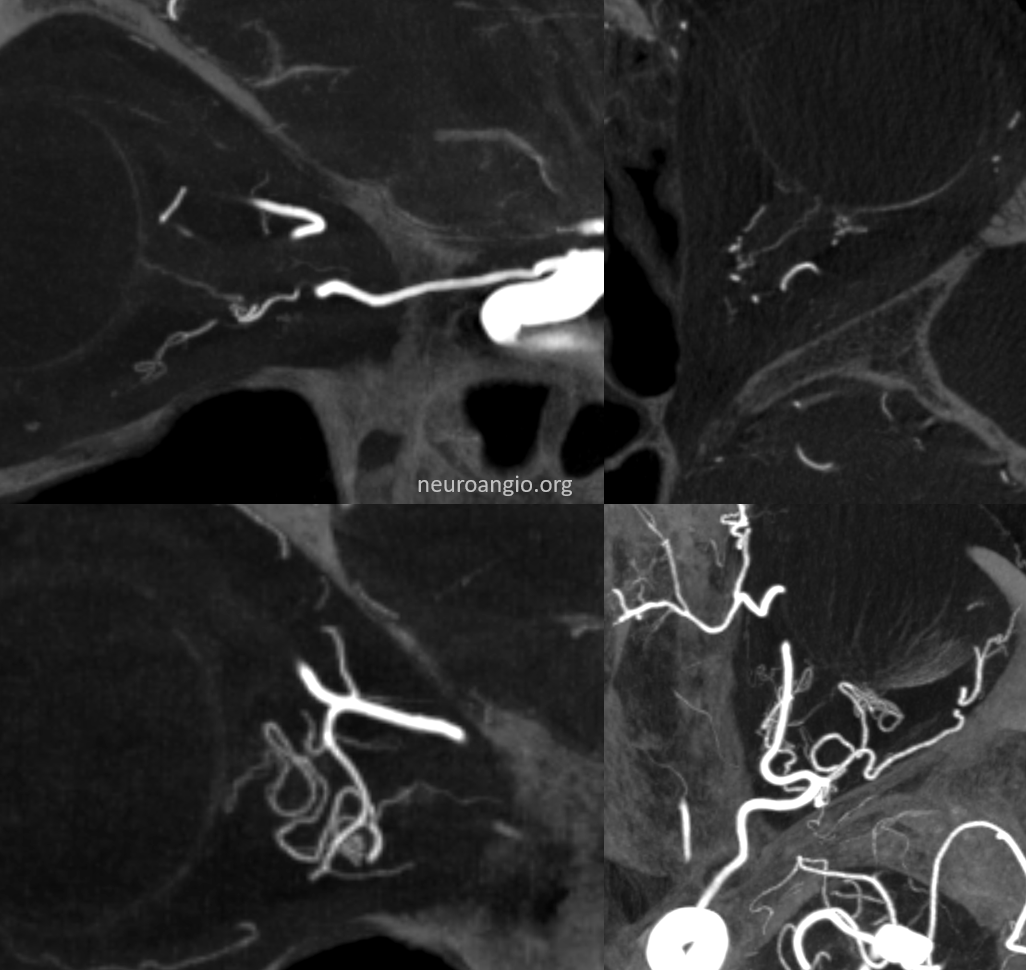
In some very rare cases, the CRA can “arise” from a variant location — such as ciliary artery trunk – much more distal along the ophthalmic. Here is an example — bilateral in this patient, so cant blame athero for it either.
Left side. CRA is labeled with arrow, while ciliary contributions to choroid/retina with dashed arrows.
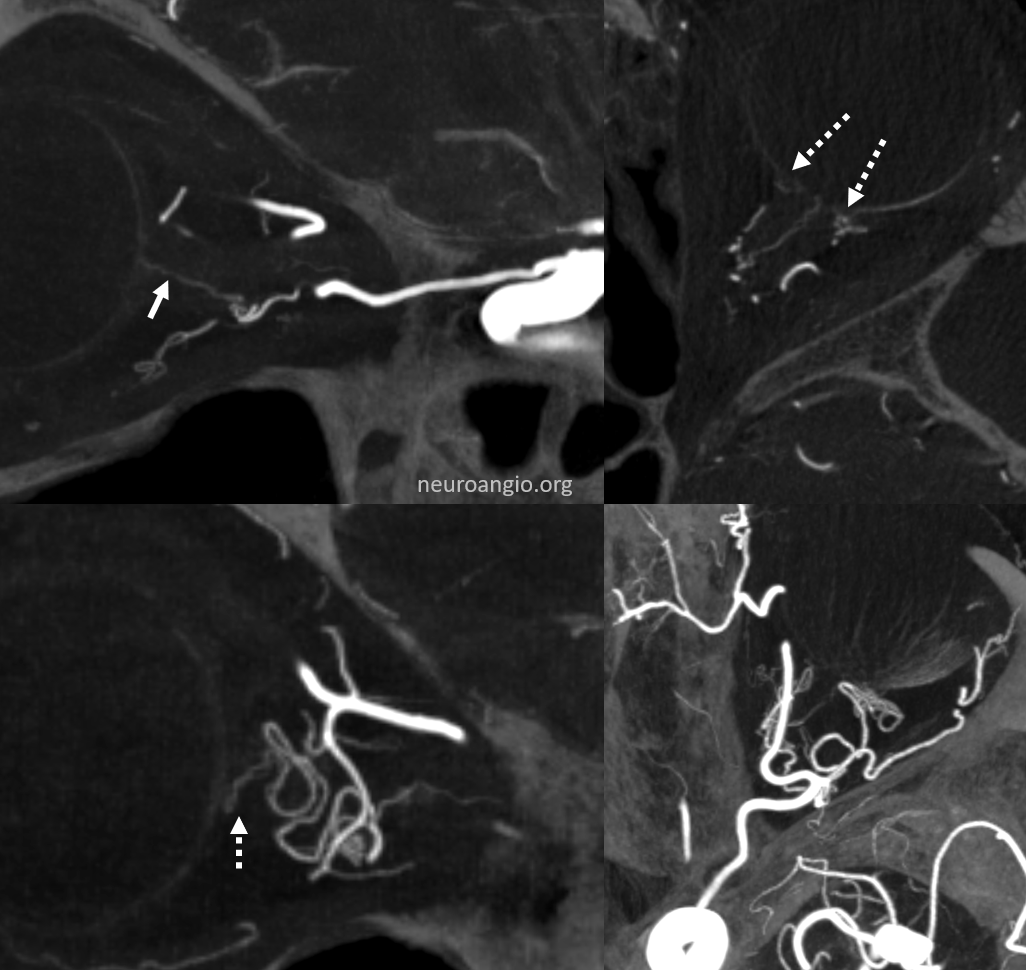
without labels
MIP movie in full resolution
Right side
MIP movie
Proximal Optic Nerve / Chiasm/Tract
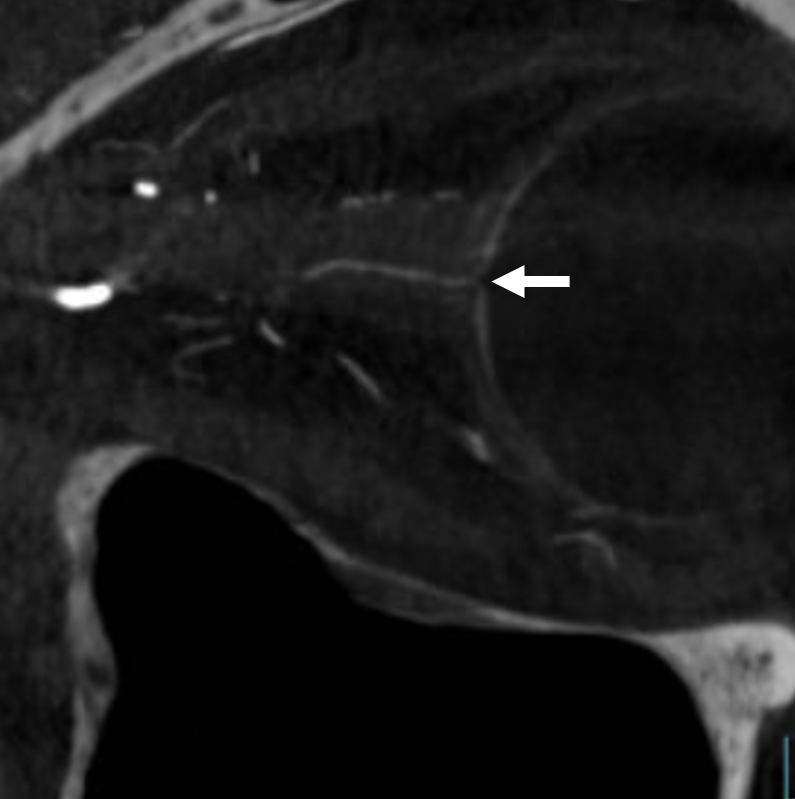
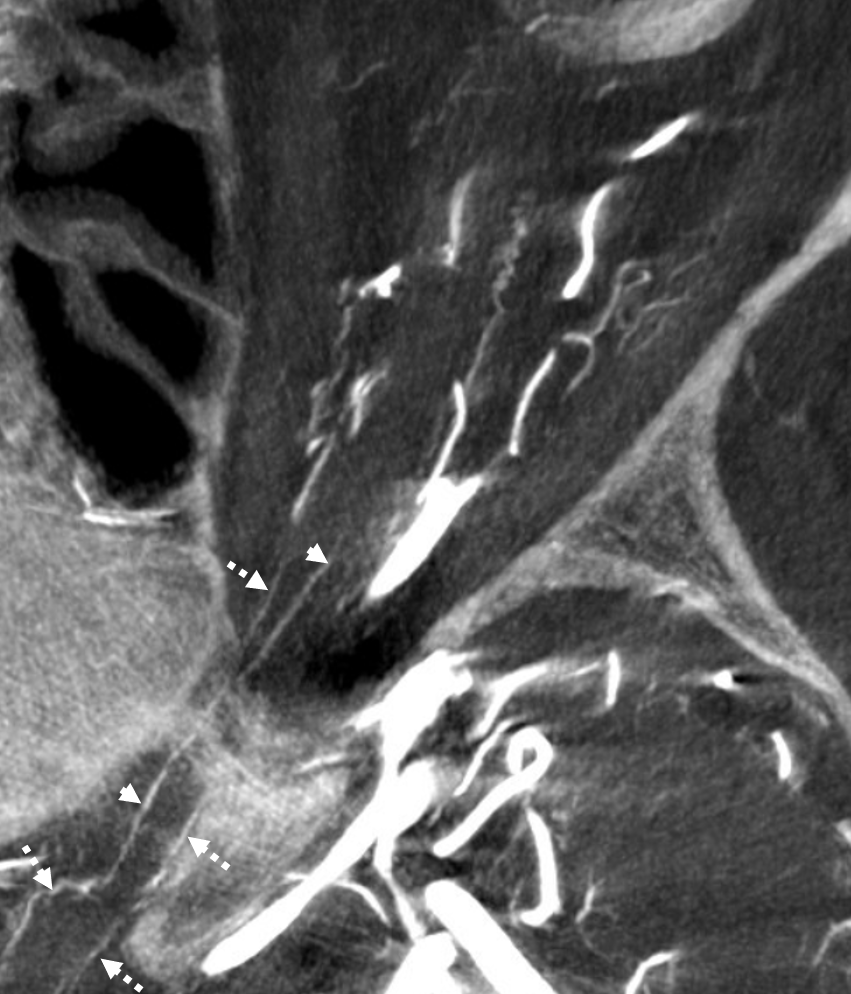
The central retinal artery is relatively small, by macroscopic standards. Yet, most of its volume goes to the retina. The nerve itself has truly microscopic requirements. Which is why, proximal to the CRA, there is usually no “central” vessel or angiographically obvious supply without a microscope. But, with flat panel imaging, we are getting there. The vessels there will supply both the optic nerve sheath and nerve itself. Visualization is inconsistent at present time. However, as in everything, it is clear that there are variations. In some cases, like the one below, visualization is particularly stunning. In addition to CRA (arrow), there are vessels surrounding the canalicular (arrowhead) and intracranial (dashed arrows) portions of the optic nerve and, amazingly, the optic tract (ball arrows). Its a 20 second DYNA, so some of them are are veins for sure.
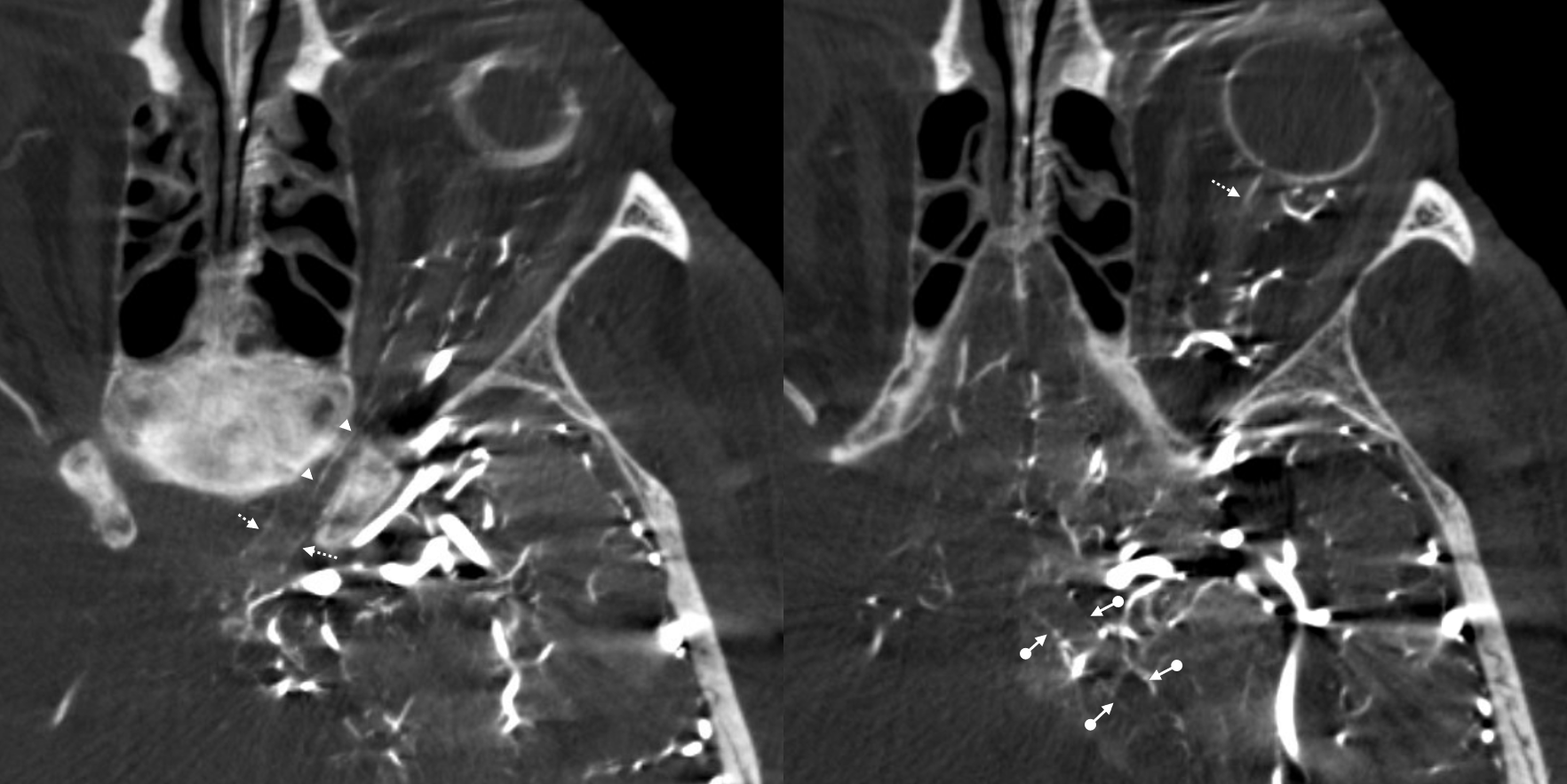
Magnified view
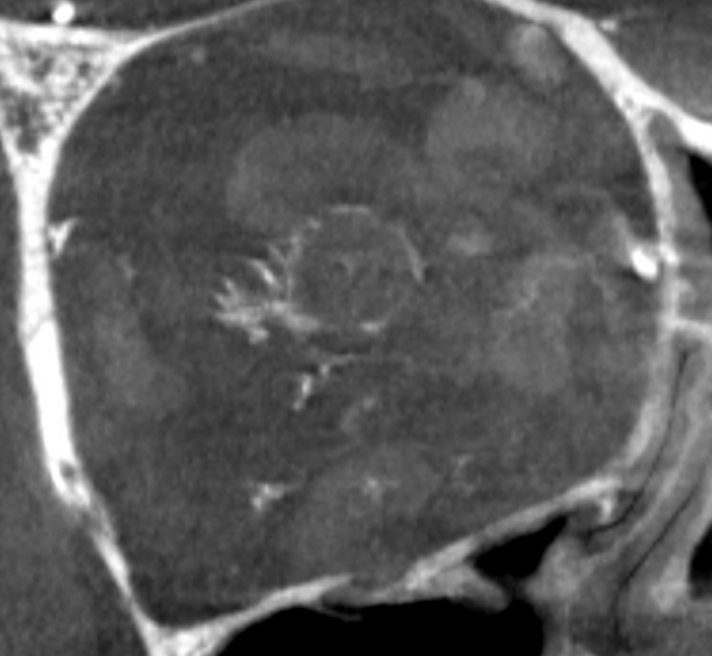
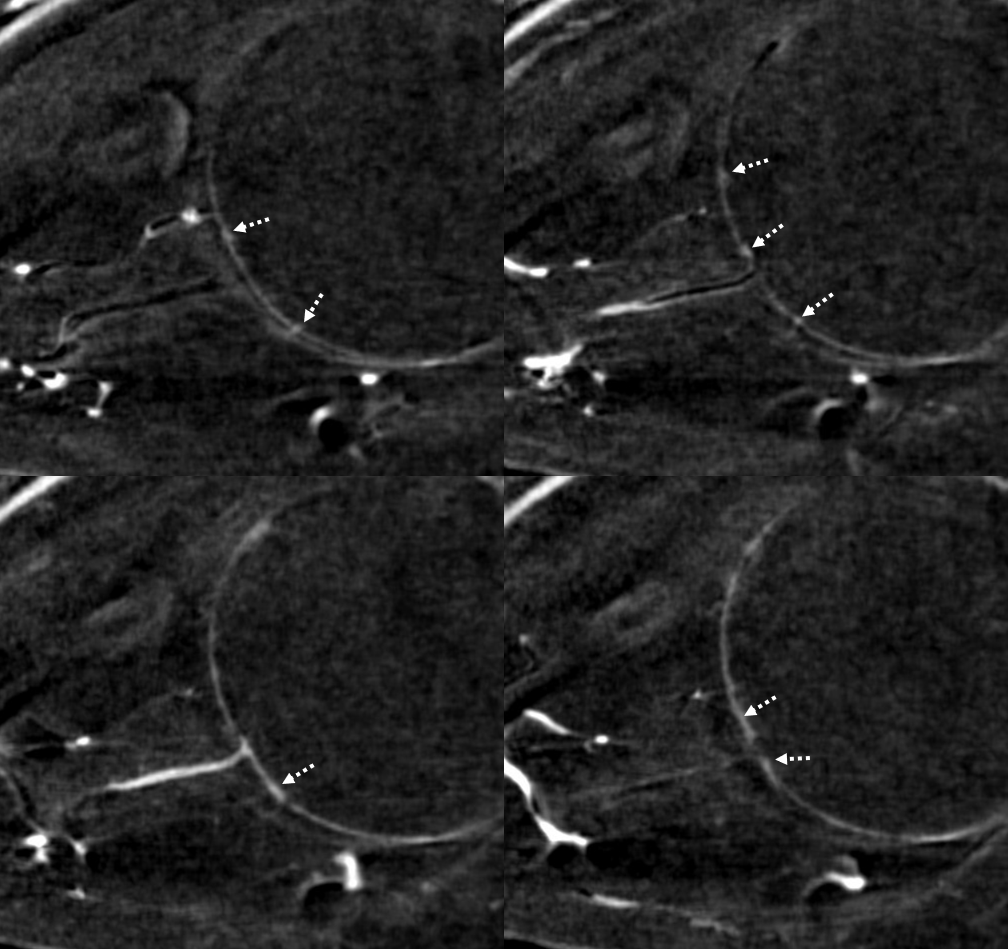
Coronal views are excellent to show that those proximal nerve vessels are not in the nerve, like CRA, but supply the nerve from the surface — makes sense, like all other nerves
Coronal movie of the same
Look at those retinal branches!
Movie
Coronal MIP — super visualization for flat panel 2021
Optic Nerve / Pituitary Supply! — ischemic disease
DYNA offers a whole world of insight — no one suspected it before. Amazing stuff. Look at this acute stroke code — critical petrous segment stenosis, perfusional exam — straightforward stenting. Note that ophthalmic is missing before and after stents
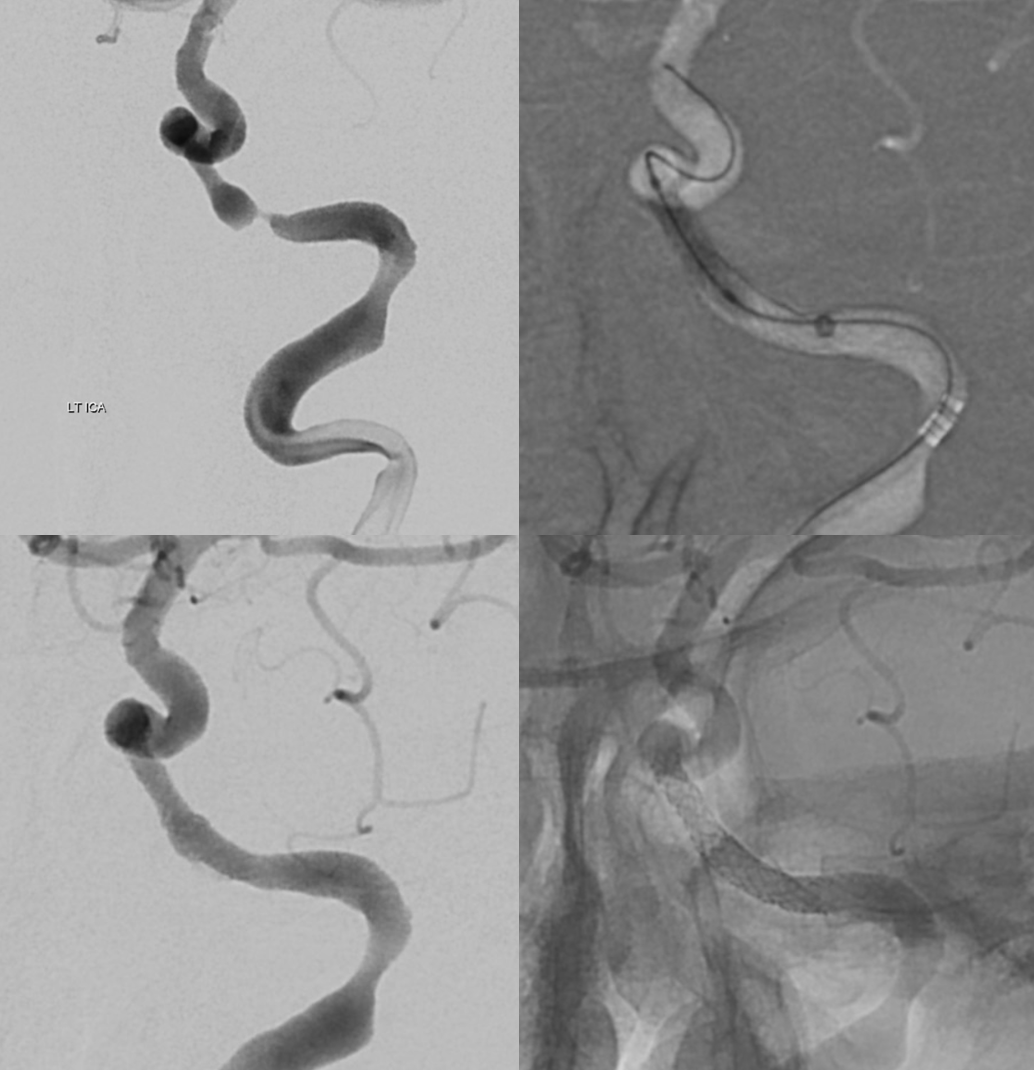
ECA run — typical meningo-ophthalmic right? Not much else to see
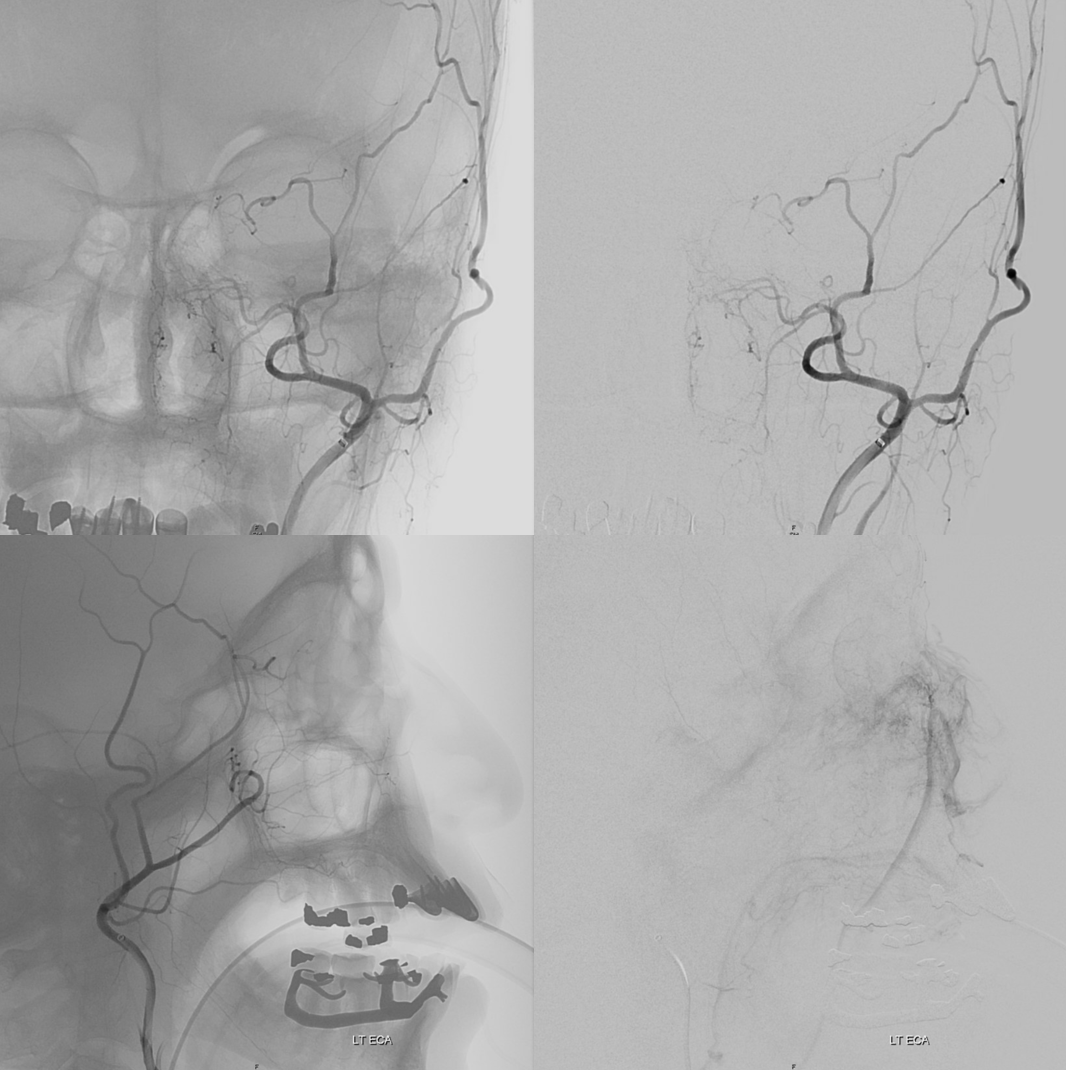
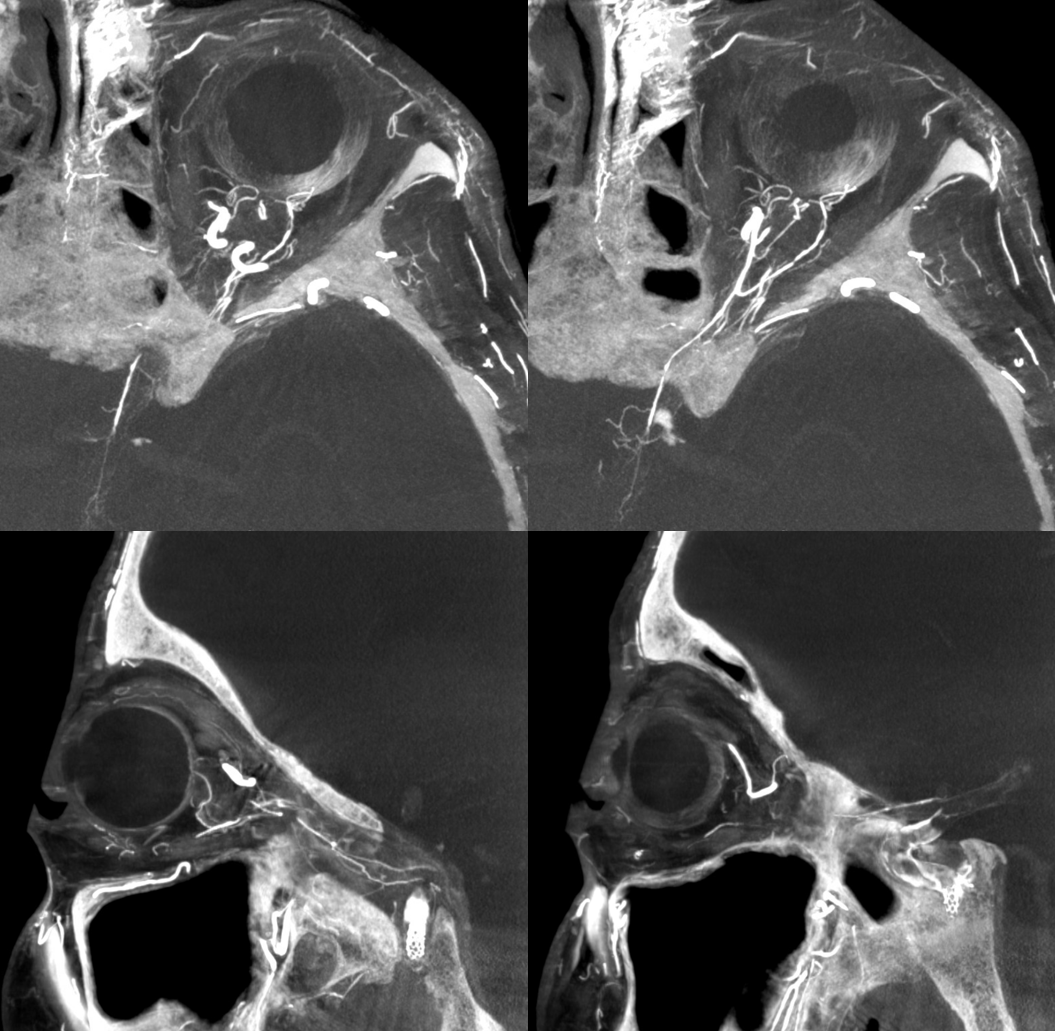
Well, check out these DYNA MIPs — look at proximal optic nerve / chiasm/ optic tract supply! and ACA / ventral ophthalmic channel also… Movie (pause and scroll) shows MMA entry into orbit via foramen of Hyrtl. The embryologic implication of this is that MMA supply to orbit in this case is acquired rather than developmental — in latter cases (complete meningophthalmic variant) the MMA entry into orbit is via the SOF. Probably, supply of optic tract/chiasm and pituitary (incredible) is an adaptation to petrous stenosis hypoperfusion also. Incredible…
See Ophthalmic Artery page for much more