Number 70… In case you are confused where the tongue is…
The basic idea is simple — there are two of them. You can lose one, but not both… So, be careful embolizing bleeding tongues from the remaining lingual artery…
Can “arise” either from the proximal ECA (proximal to the facial), or as a common faciolingual trunk. In either case can participate variably in supply of the mouth floor (submental arteries, submandibular arteries).

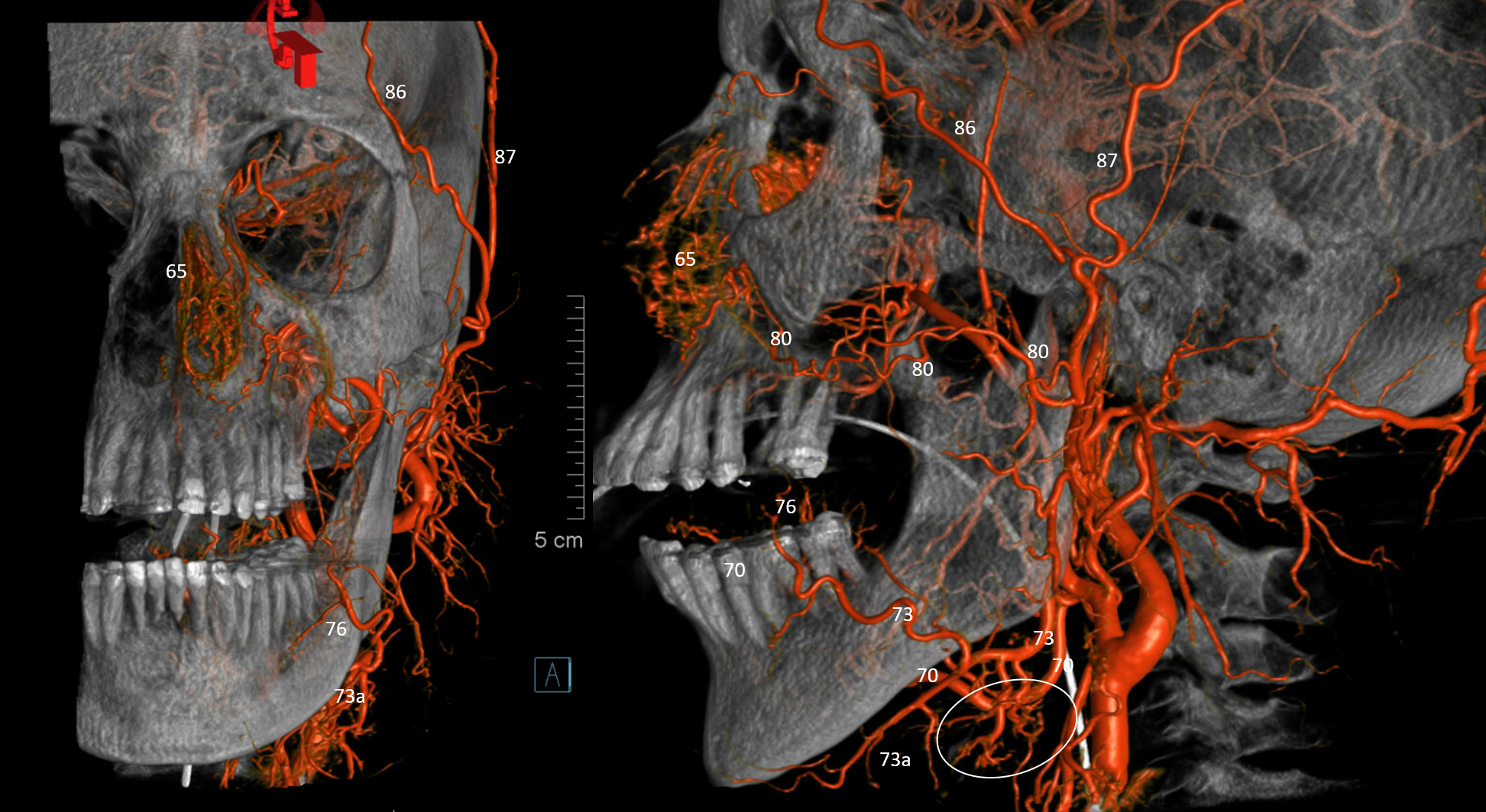
In this case, separate origins
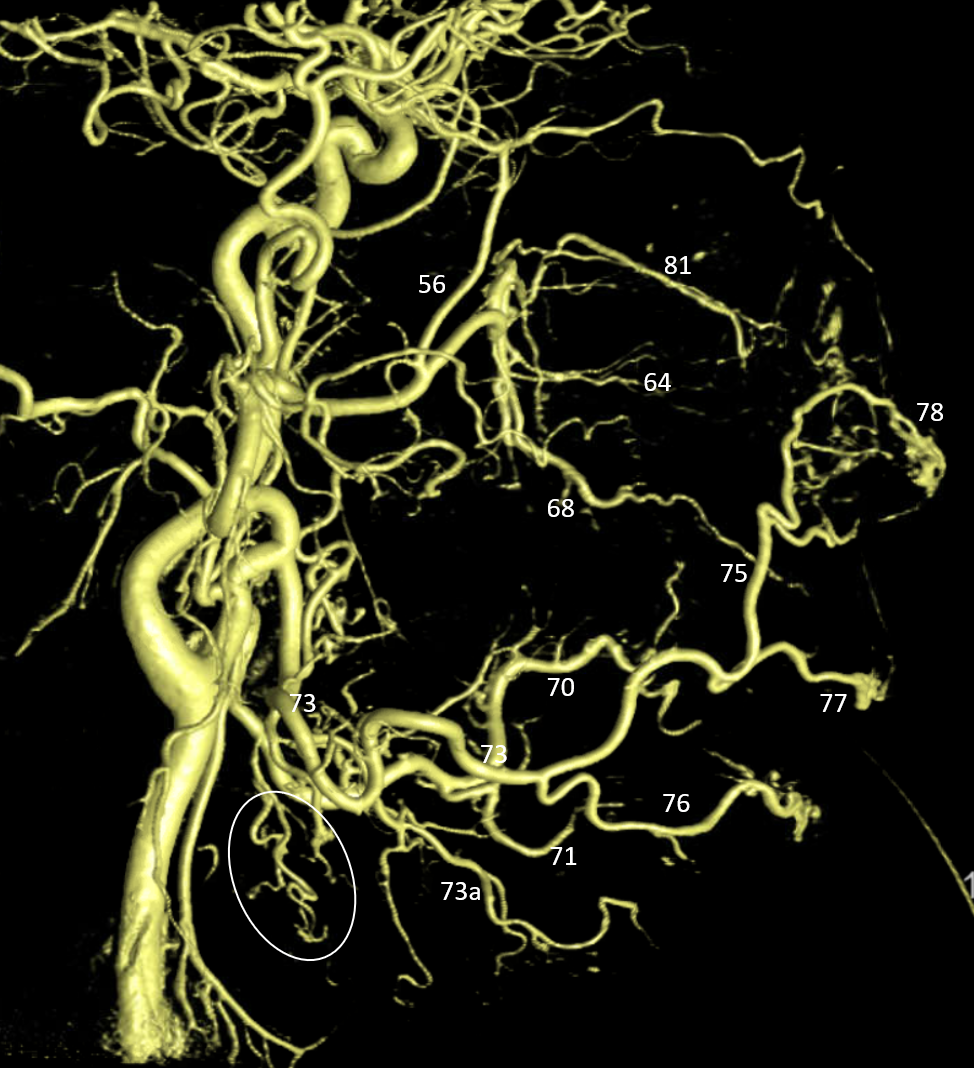
Lingual supplies the submandibular gland (oval). Facial takes are of the submental 73a
Common origin here
Tongue AVM — Reconnecting Ligated ECA
In the bad old days, ECA ligation was sometimes done in a desperate and usually unsuccessful attempt to stop oral/tongue bleeding. Of course, if it did not work, endovascular access to bleeding source became a problem. This is what happened — full case here — check it out!
Bleeding from Tongue Squamous Carcinoma
Happens also. Bottom line is as above — usually one of the linguals is already closed or diseased — from the cancer, or the subsequent surgery/radiation. If bleeding is from the cancer side, whatever remains from the ipsilateral lingual can be closed as long as the other one still exists. Frequently, no pseudoaneurysm or other source is seen — so closure can be done anyway if risks/benefits are felt to be worth it.
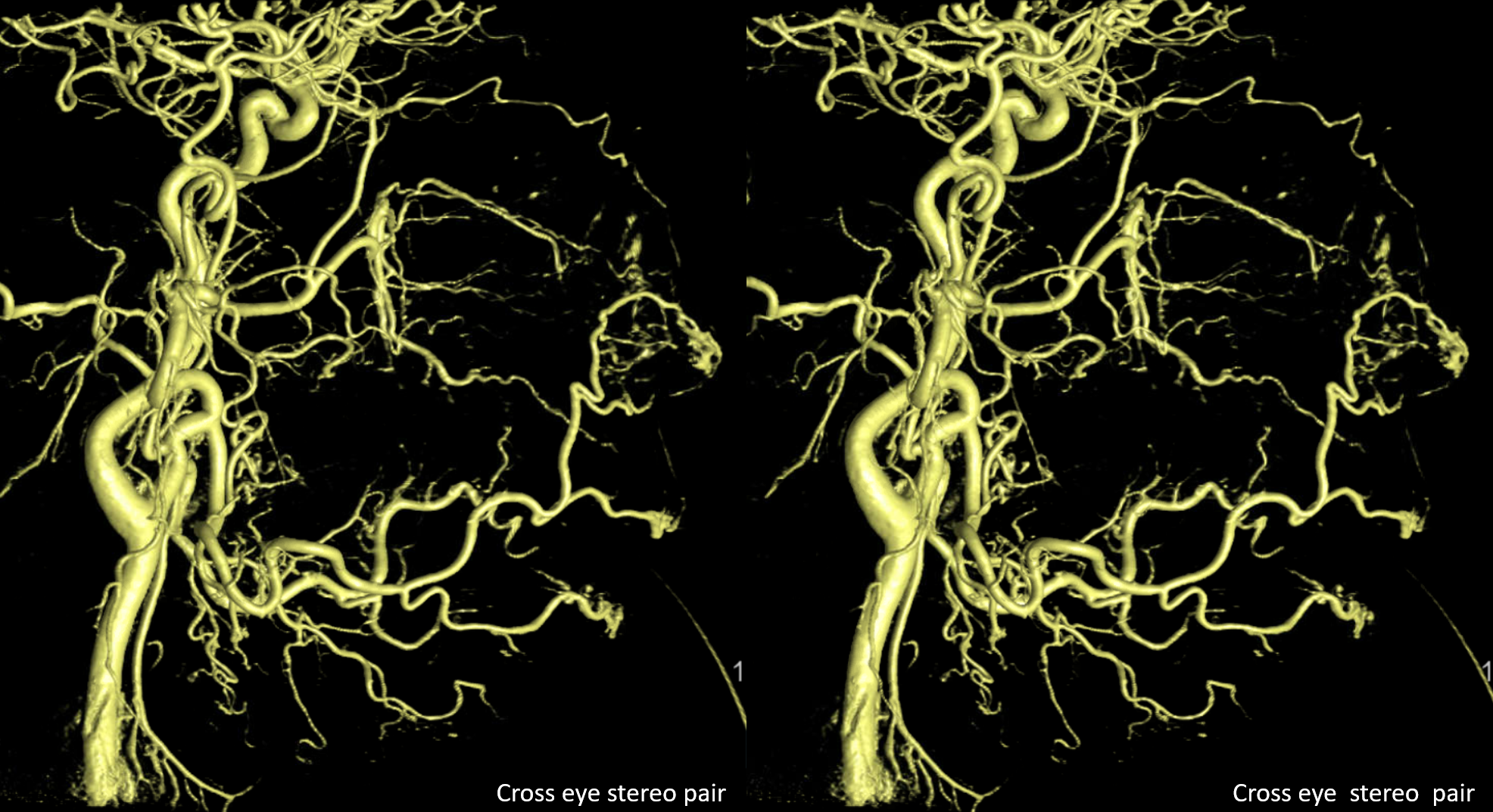
Here the cancer is on the right. Frontal views show crossover of contrast from left to right lingual / tongue territory. This tells you that the right lingual must be diseased
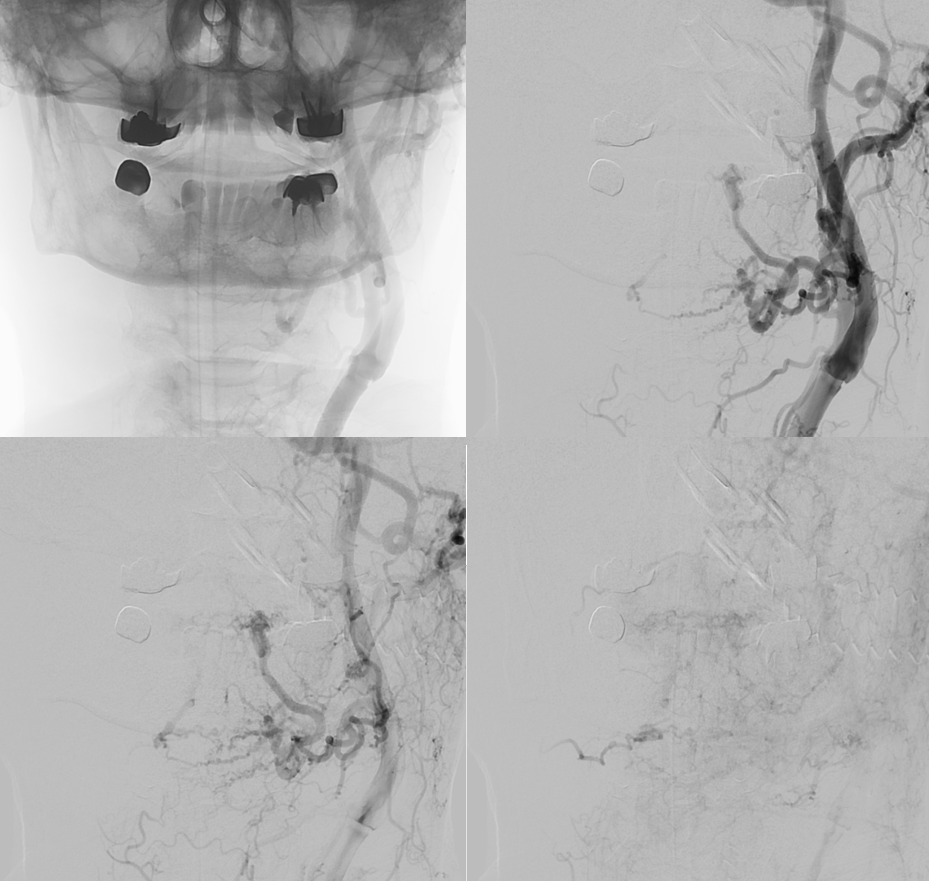
Here, right lingual is diseased — what remains of it. The facial is gone also.

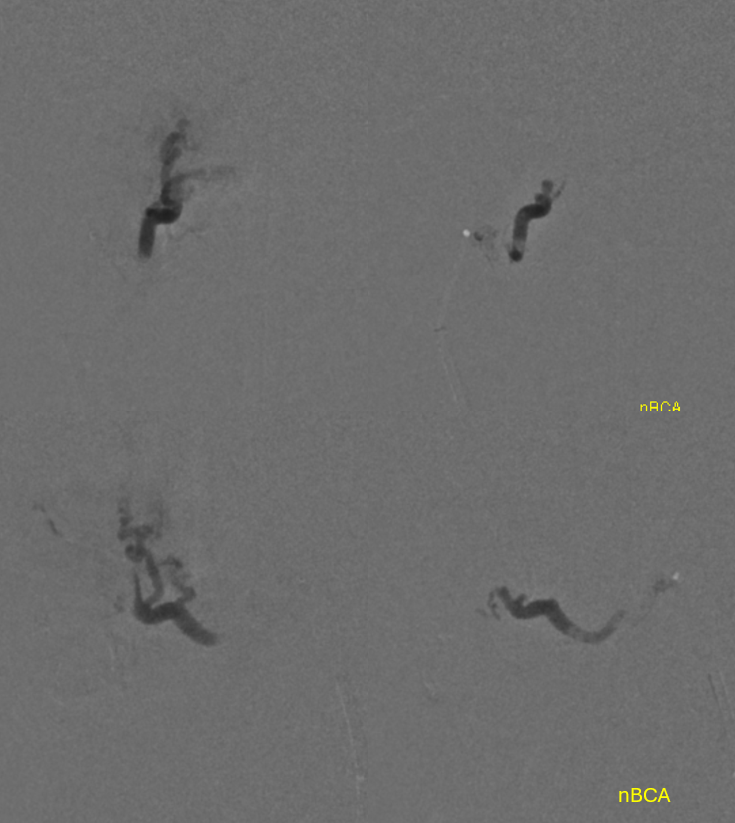
Proximal right lingual injection — friable diseased proximal segment with no clear pseudoaneurysm of the right tongue
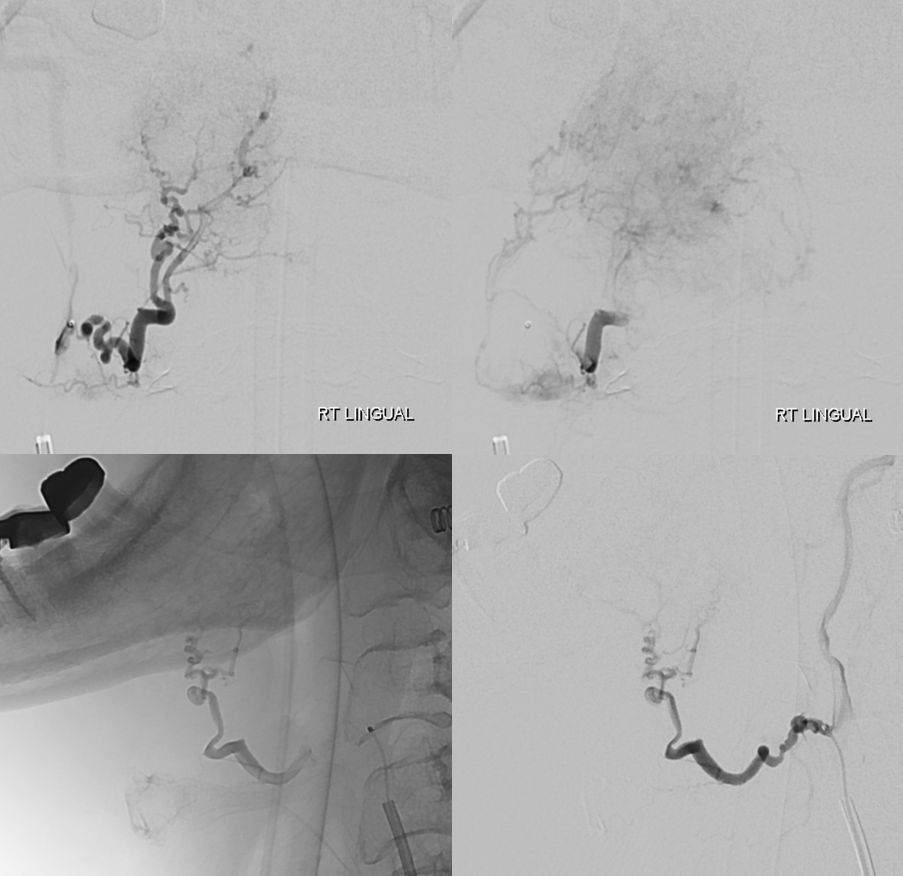
Plan — right lingual was treated with a small, judicious amount of 150-250 contour particles and closed with nBCA. Bleeding stopped. Whatever was preset of the tongue stayed the same.