
CASE 2 – advanced sigmoid sinus fistula.
This patient presented with headaches and pulsatile tinnitus, having no other symptoms.
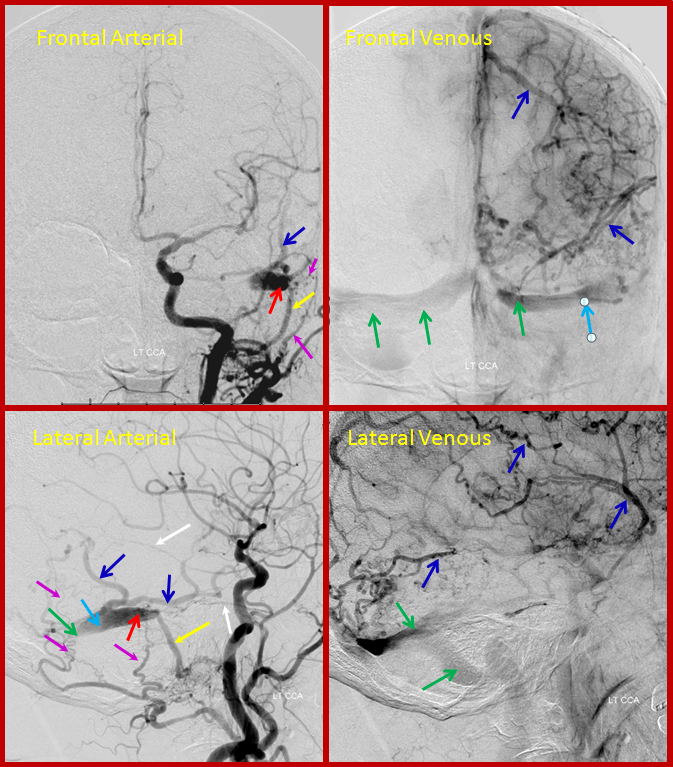
Arterial and venous images of left common carotid injection during diagnostic angiography show sigmoid sinus (light blue) single hole fistula (red) supplied by occipital (pink), middle meningeal (white), and ascending pharyngeal jugular division (yellow) arteries, draining retrogradely into the transverse sinus (green). The ipsilateral jugular outflow is occluded. Extensive retrograde drainage into cortical veins is present (dark blue).
The patient returned for treatment 2 weeks later, and reported that her tinnitus has disappeared. The pre-treatment angiogram, below, showed interval left transverse sinus occlusion proximal to the fistula (bright green arrow points to new occlusion), such that the fistula (red) empties into a short segment of the transverse sinus, and having now nowhere else to go, drains exclusively into cerebral cortical veins (blue arrows), which then in retrograde fashion opacify the torcula and right transverse sinus (dark green). We typically caution our pre-embo dural fistula patients to contact us should their tinnitus improve, for this very reason.
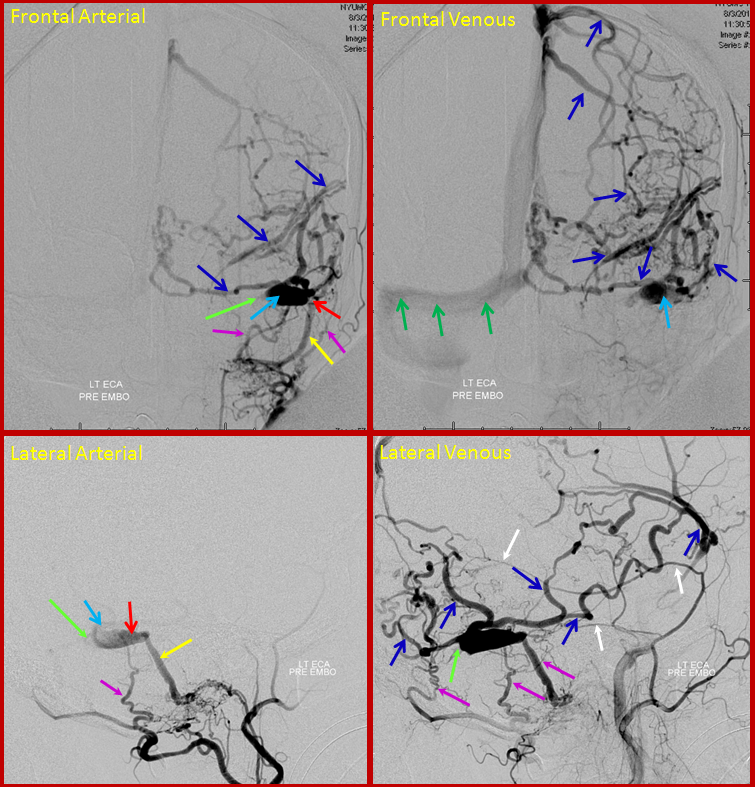
AP and Lateral Pre-embolization videos show exclusive intracranial drainage of the fistula
In deciding whether to adopt transarterial or transvenous approach, we were apprehensive of potentially depositing embolic agents into the cerebral venous system. Knowing that the transverse sinus was open several weeks ago, we felt that attempting to go through the occlusion and access the sigmoid sinus was reasonable.
In the above video, a wire has been passed through the occlusion, and subsequently through the fistula, into the ascending pharyngeal artery jugular divison pedicle supplying it. The objective was to start “coiling back” from the arterial side and accross the fistulous region into the sigmoid sinus. The movie below of the ECA injection shows coils in the jugular division, with reduced shunting.
Continuing to drop back and coil into the sigmoid sinus…
Finally, the fistula is closed, as can be seen below.
As you can see from the following left transverse sinus injection, the coil mass has been extended just to the ostium of the Labbe, which were careful to preserve. The left transverse sinus remains closed, however, and therefore the left lateral convexity still cannot drain in a physiologic fashion, relying exclusively on the superficial sylvian system.
The transverse sinus was opened with balloon angioplasty and t-PA, as is seen in this final post-embolization venogram.