Flow diversion for ACOM aneurysms is a fantastic and still underused as of 2024 treatment. But one has to be aware of details. Of course, high-end imaging helps. Below is a rare variation of the ACOM complex — which helps.
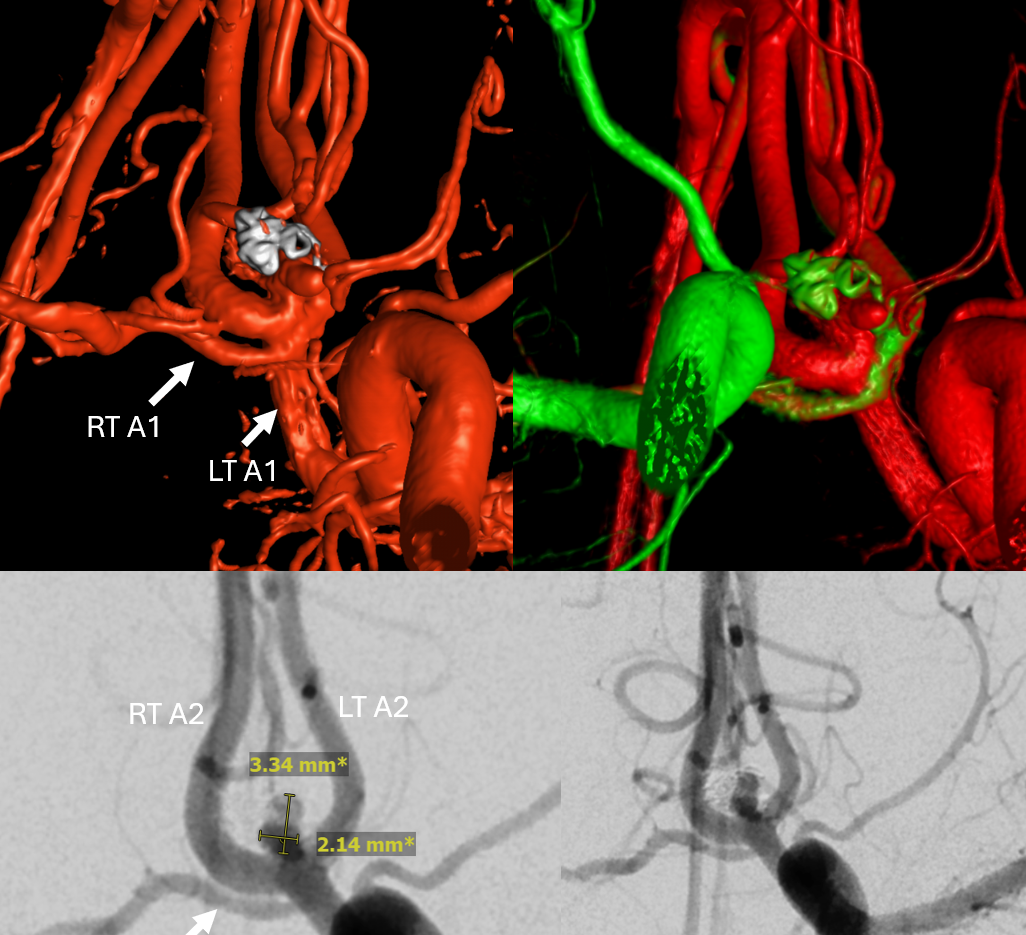
This is a standard “plug and pipe” aneurysm — with expected recurrence. Patient is coming in for a Pipe — except there is a variation here. And, as it happens, also resistance to BOTH Clopidogrel and Brilinta… It happens. P2Y12 on in-house given Brilinta was 299 and 354.
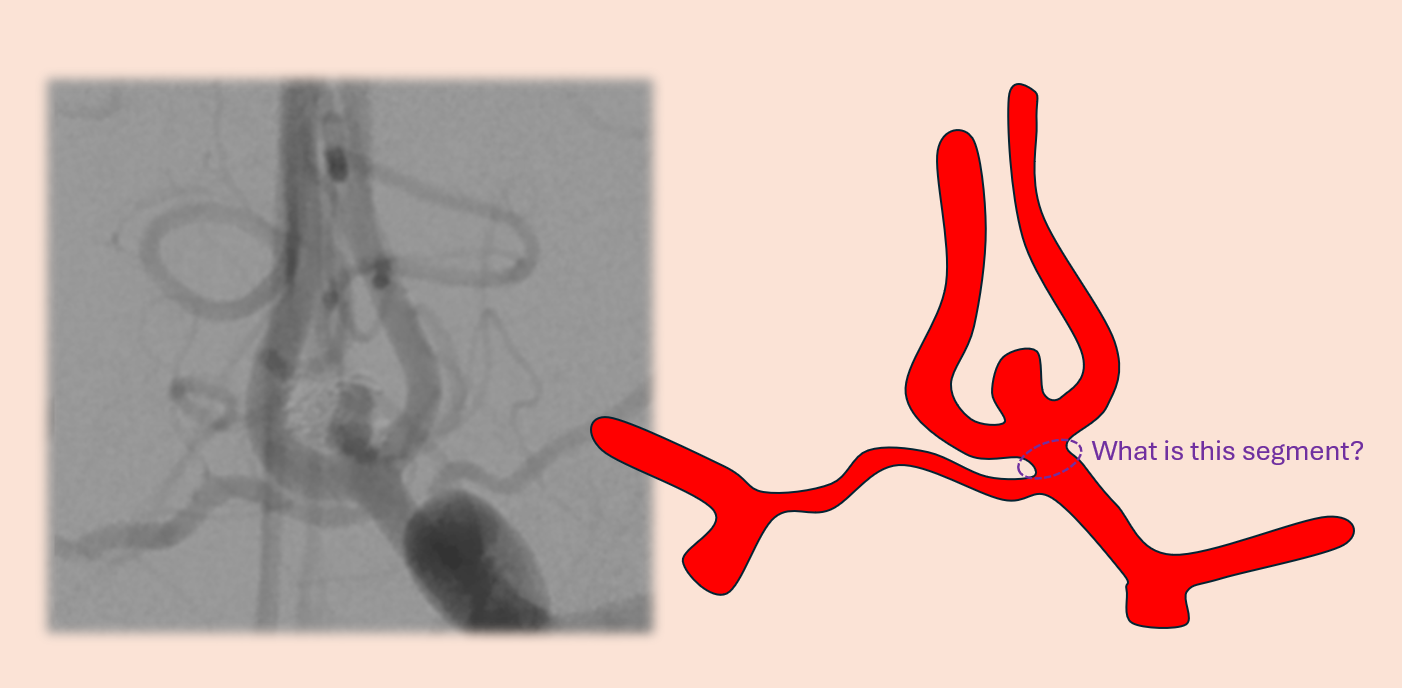
DSA — see slipstreaming of unopacified contrast in BOTH A2s — thats the angiographic sign that the contralateral A1 participates in supply of both A2s — thus a question of what is the exact relationship. Question to consider — how to conceptualize this kind of ACOM arrangement?
The aneurysm was re-coiled…

So, how to think of this?