
In Collaboration with Dr. Eytan Raz
A tortuous, usually moderately fusiformly dilated, frequently calcified anterior cerebral artery, particularly at pericalossal and distal A2 segments, is a rare but characteristic finding. Sometimes mistaken for an AVM on cross-sectional imaging, the lesion shows no arteriovenous shunting, but is almost always associated with adjacent cortical dysplasia. The latter can be subtle and frequently there are no seizures or other clinical issues. The finding is typically asymptomatic. Literature is understandably limited but relatively consistent in portraying it as an incidental finding.
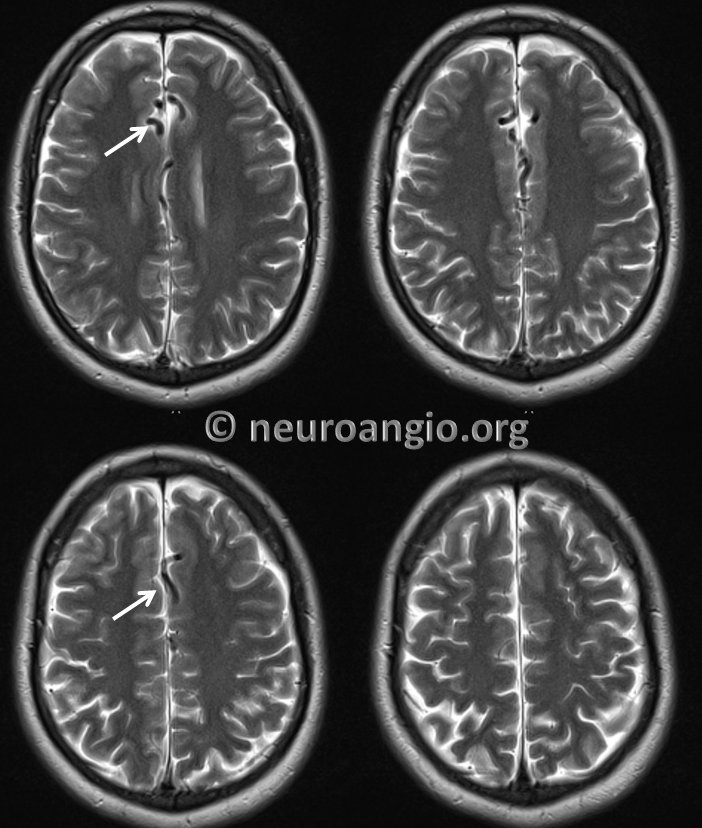
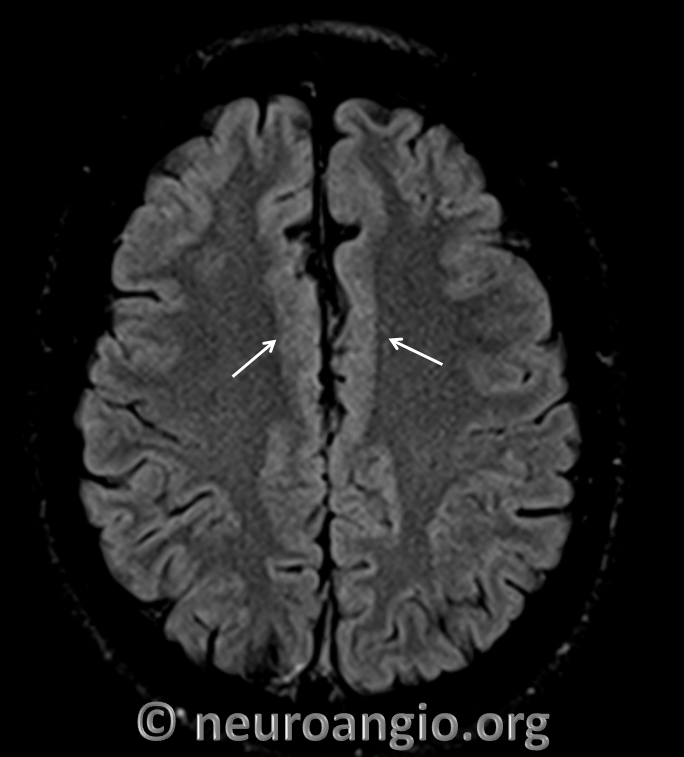
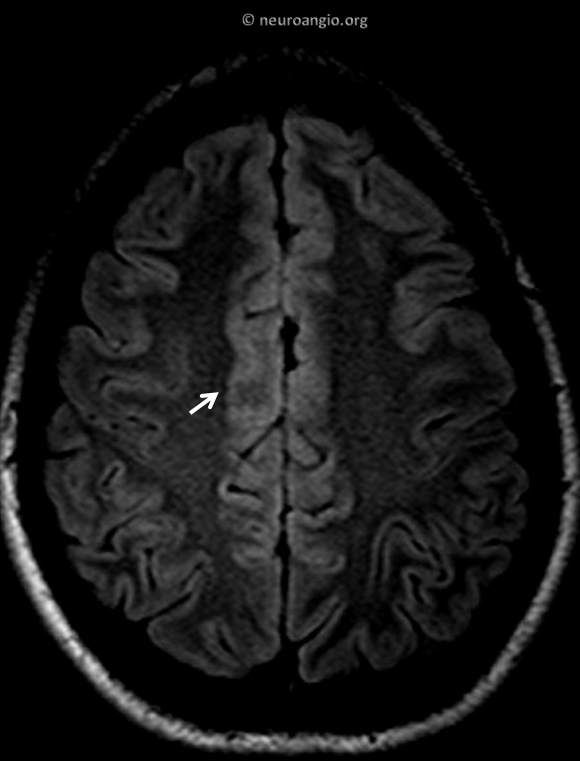
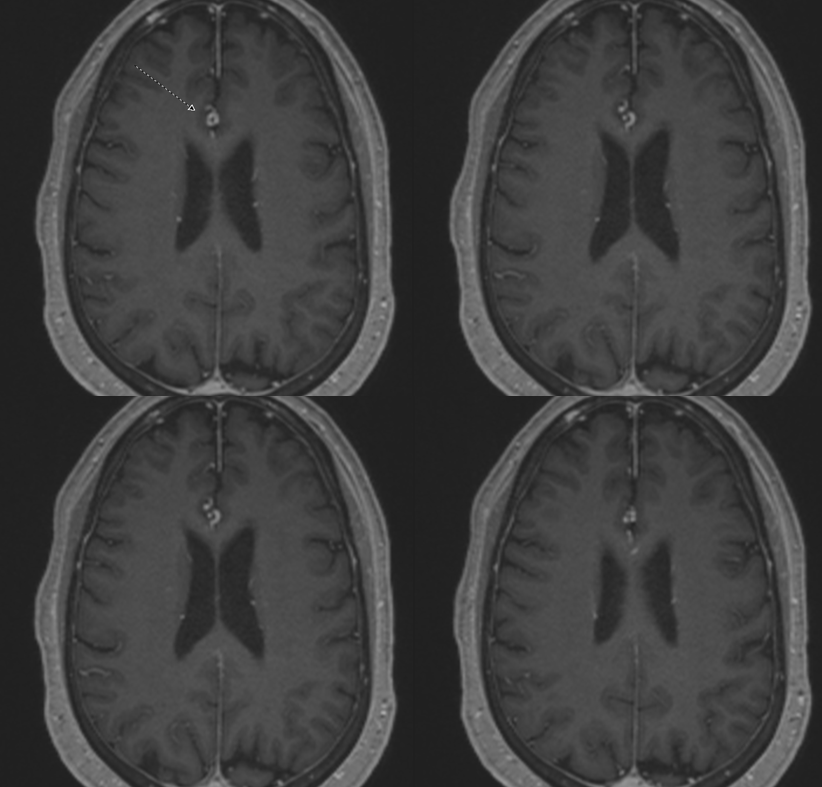
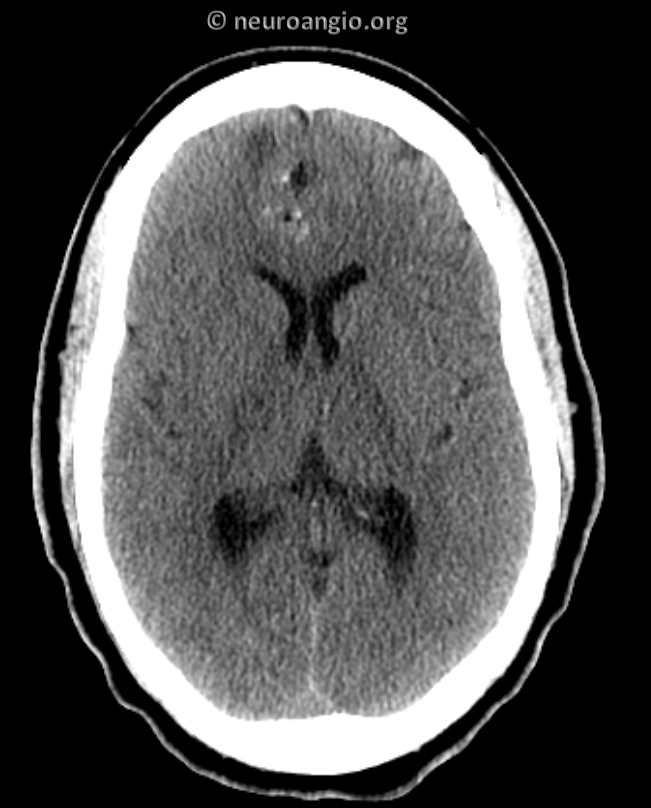
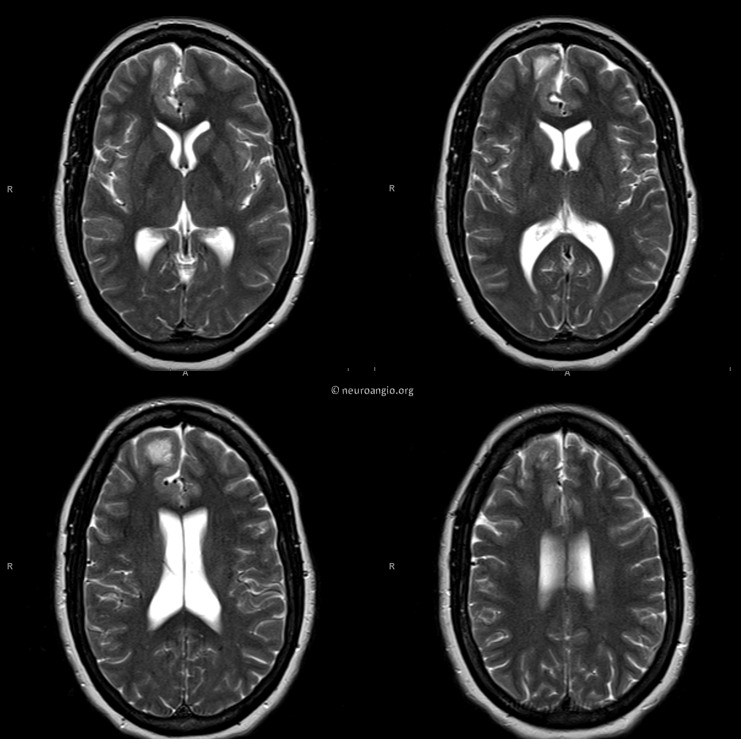
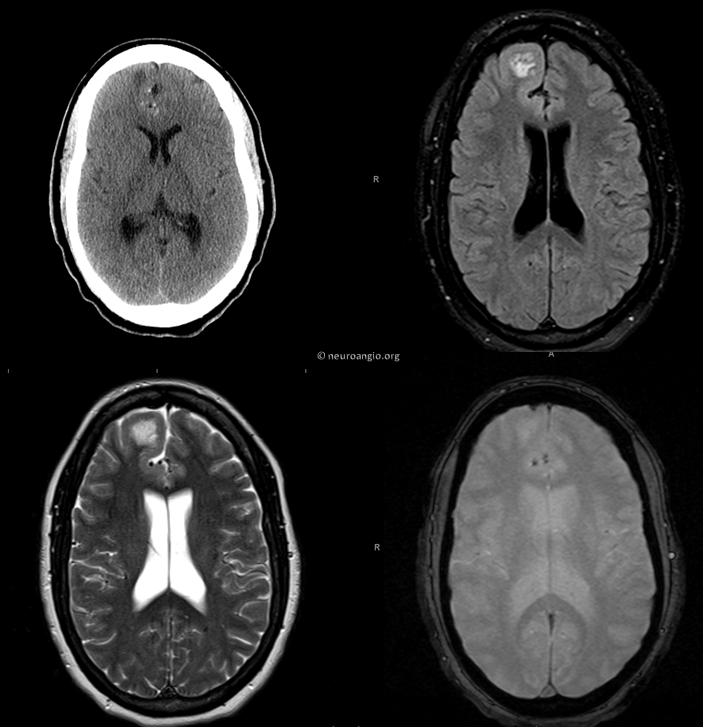
Case 1 — chronic headaches, normal exam
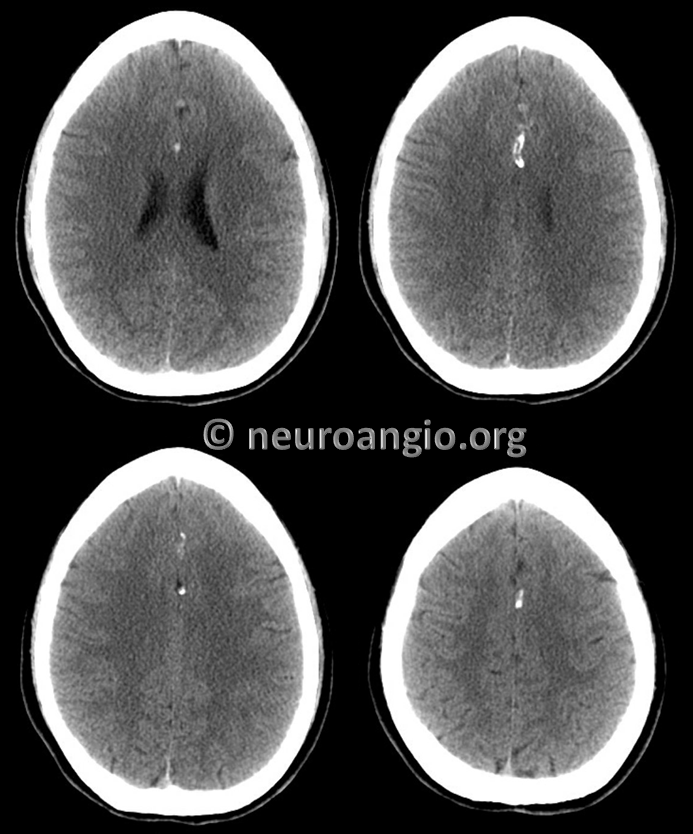
Calcification on susceptibility imaging

Subtle adjacent cortical dysplasia
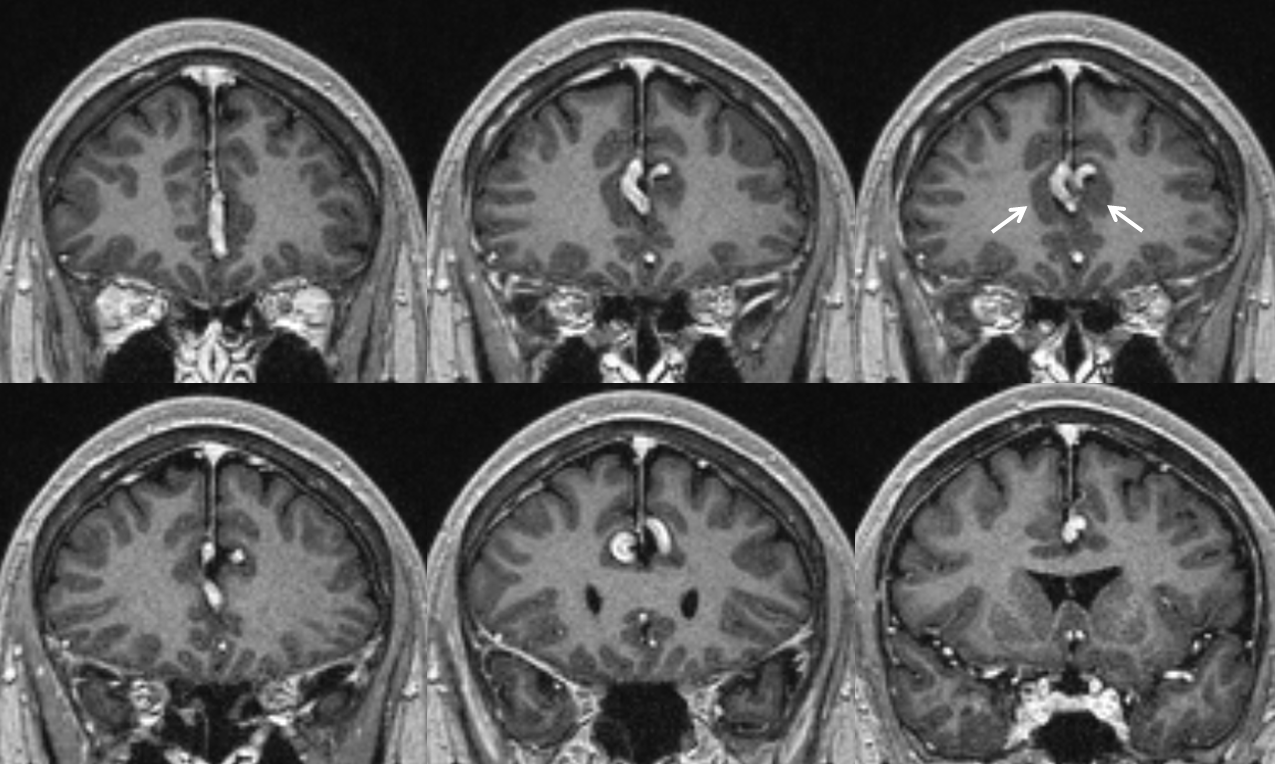
Same on coronal T1 post
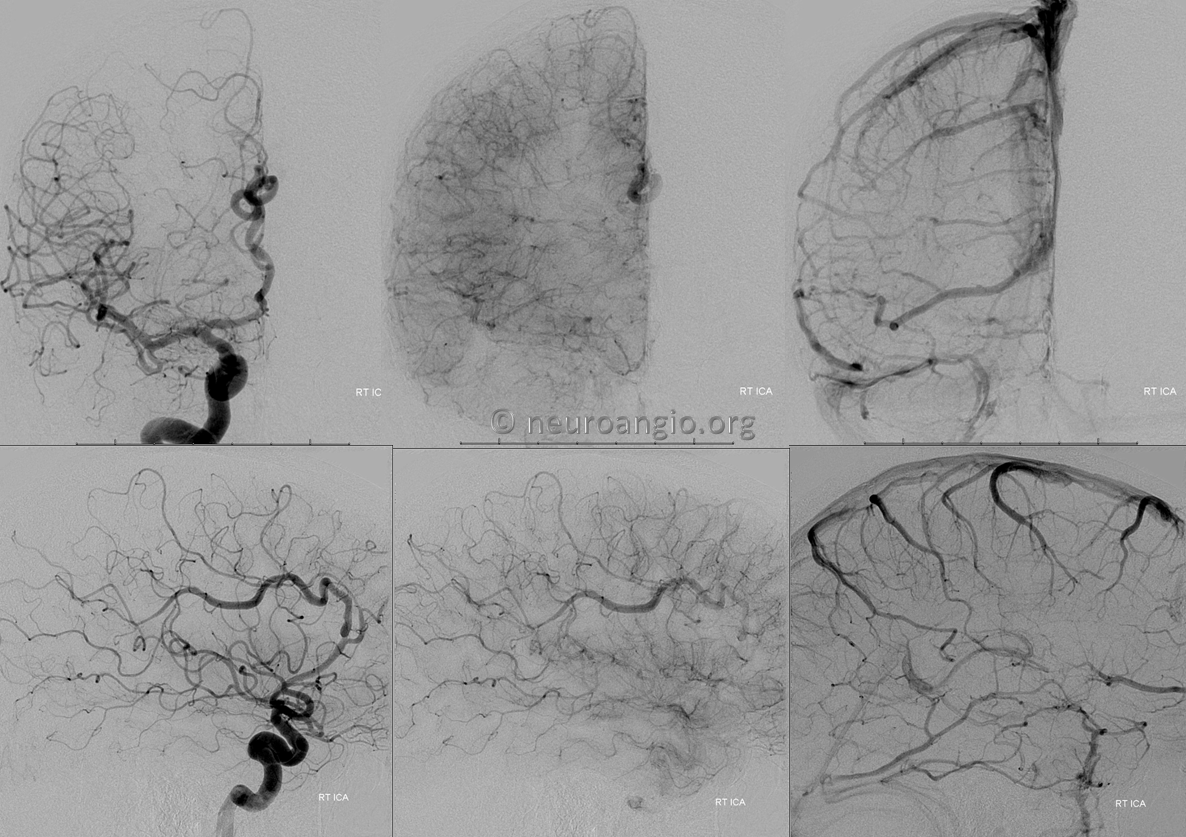
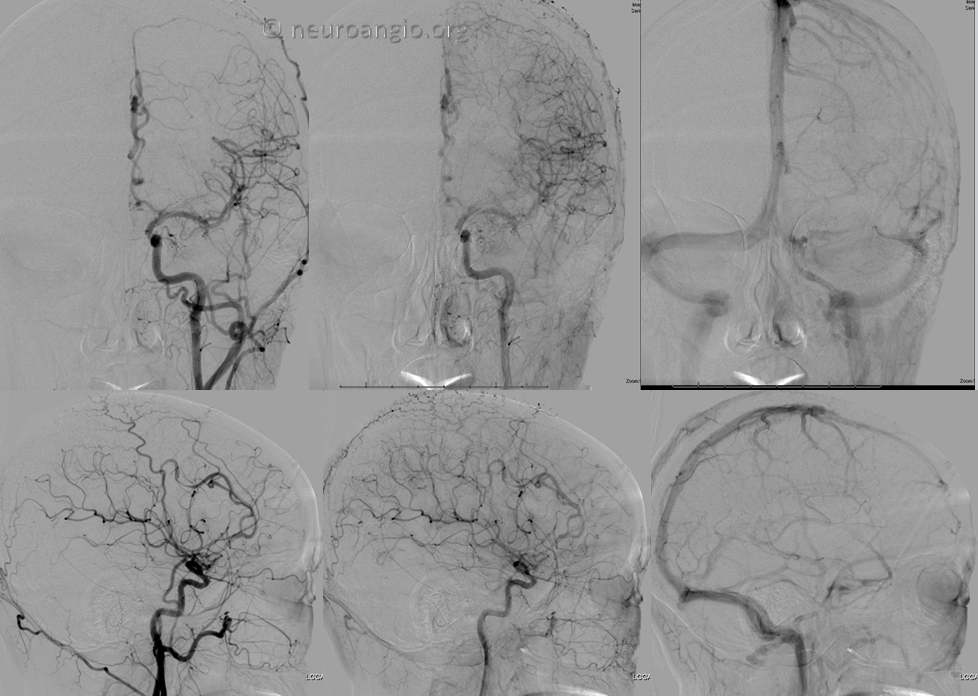
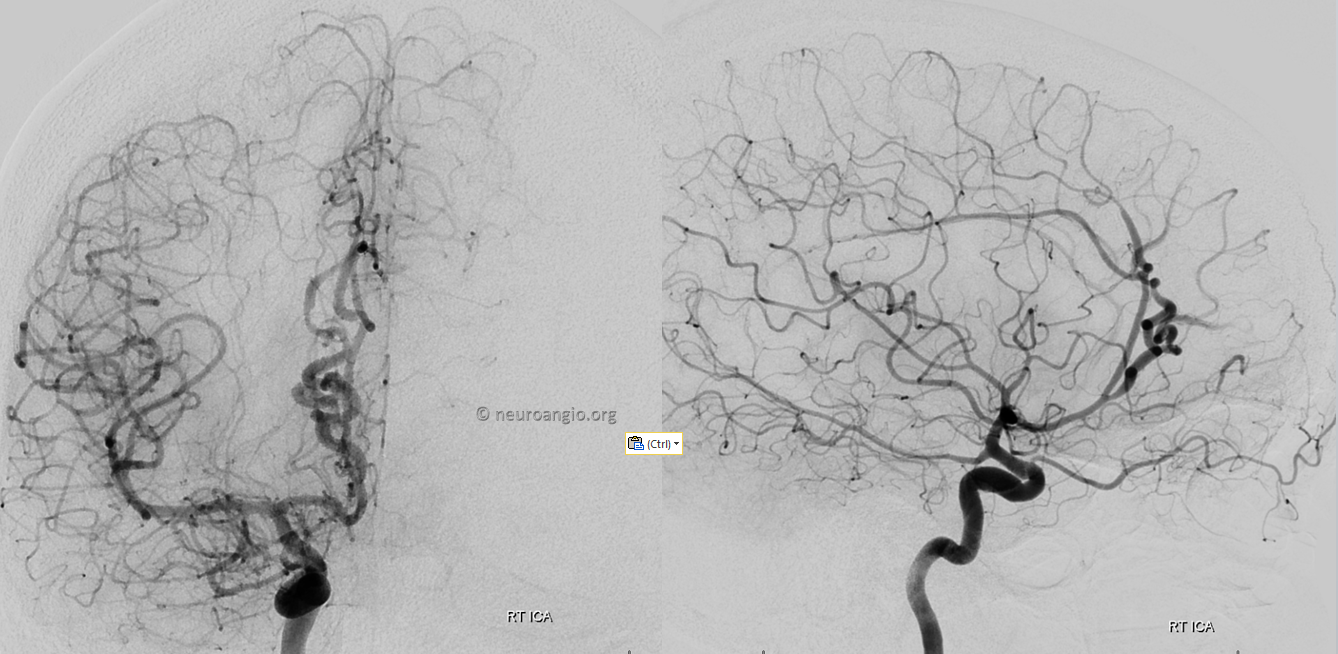
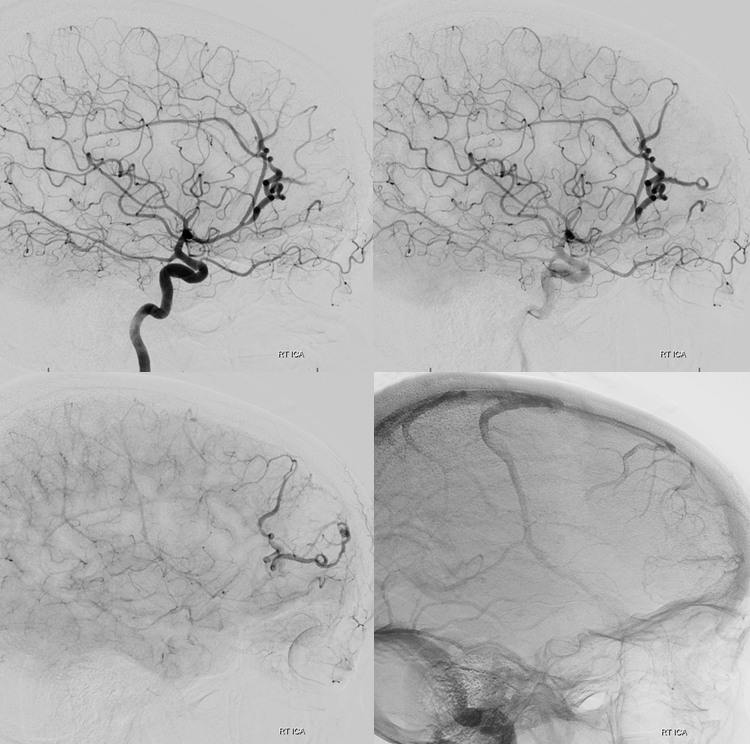
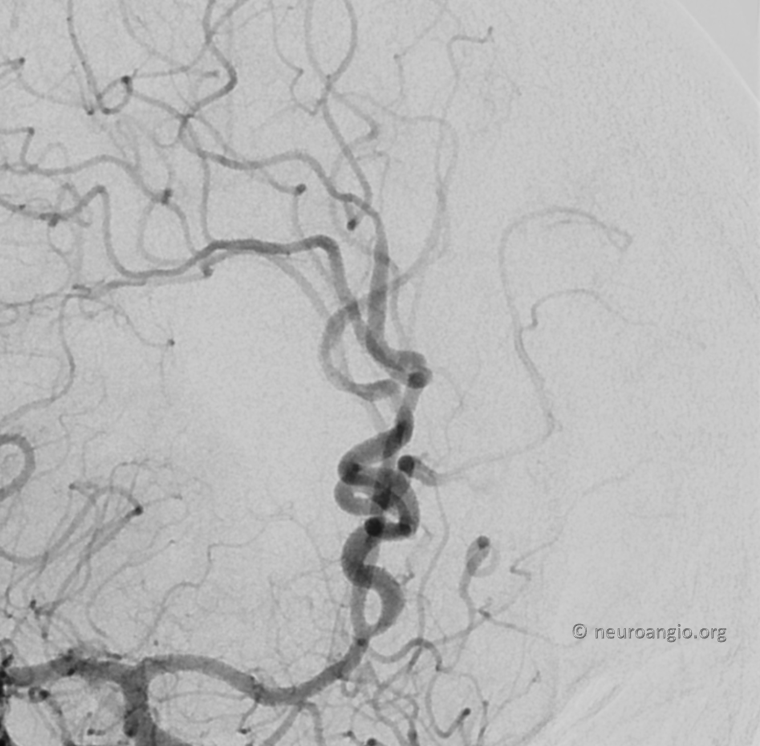
Typical angio appearance — tortuous, fusiform A2/Pericalossal, without arteriovenous shunting
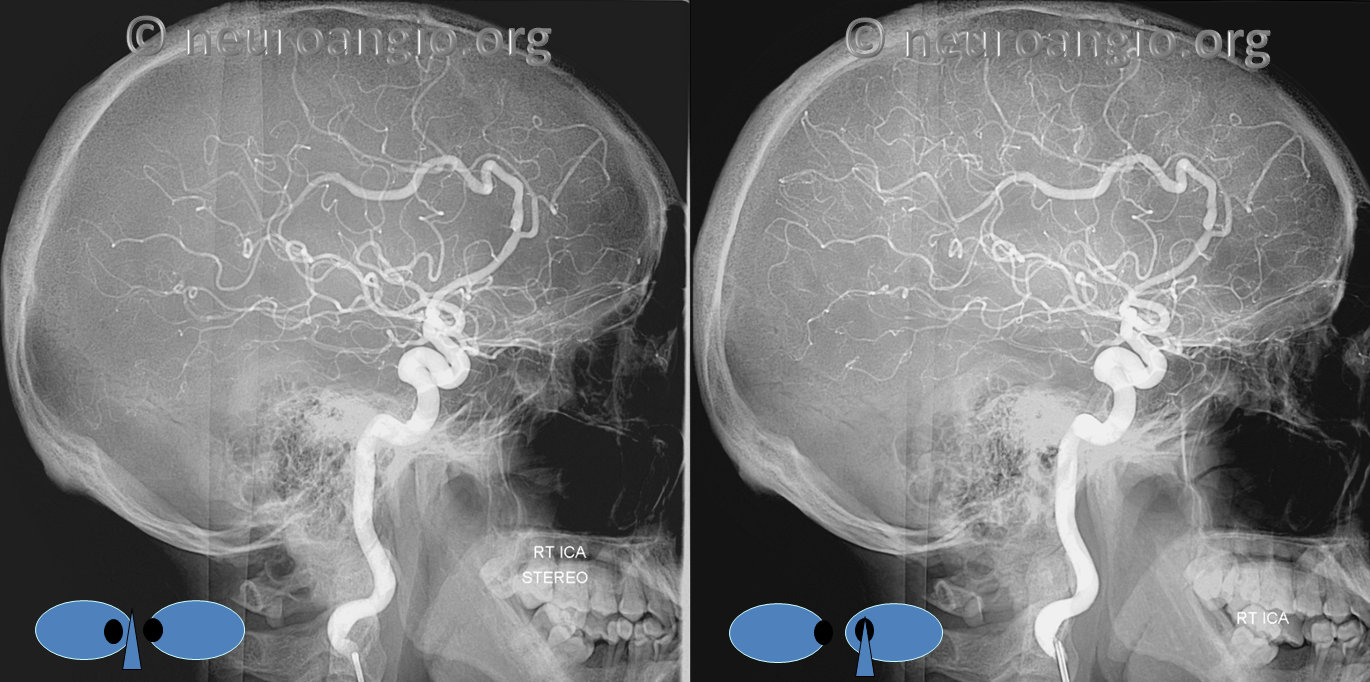
Stereos
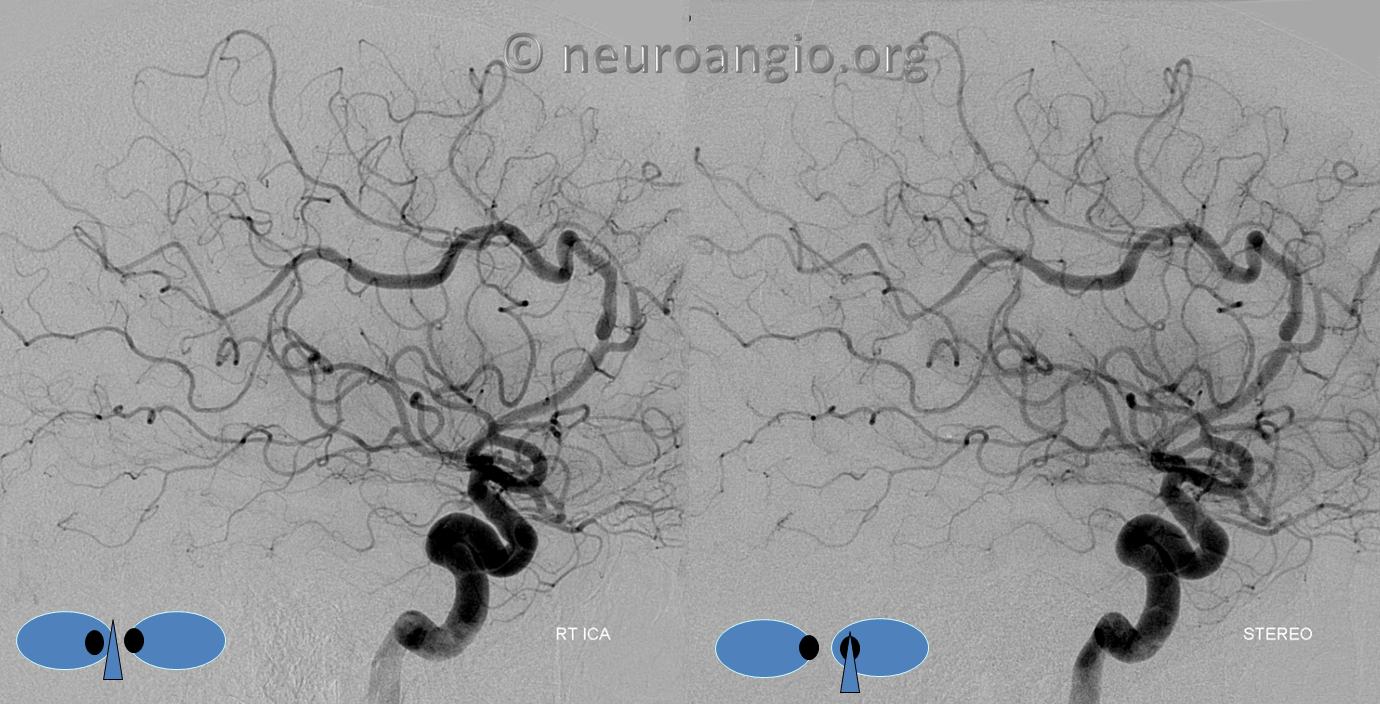
Red/cyan anaglyph stereo

Native stereos, retro style
Anaglyph stereo

Usually the finding is bilateral, as it is here (see unilateral Case 4 below)
Case 2 — young woman with syncope. Normal exam. Typical calcifications
Less subtle cortical dysplasia
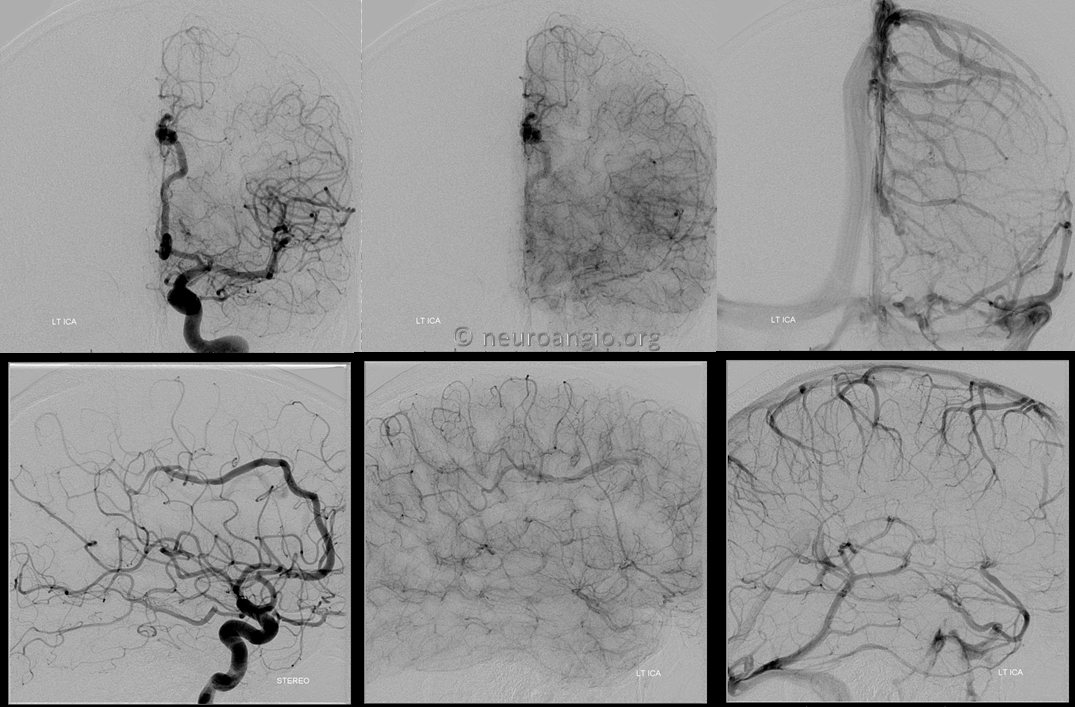
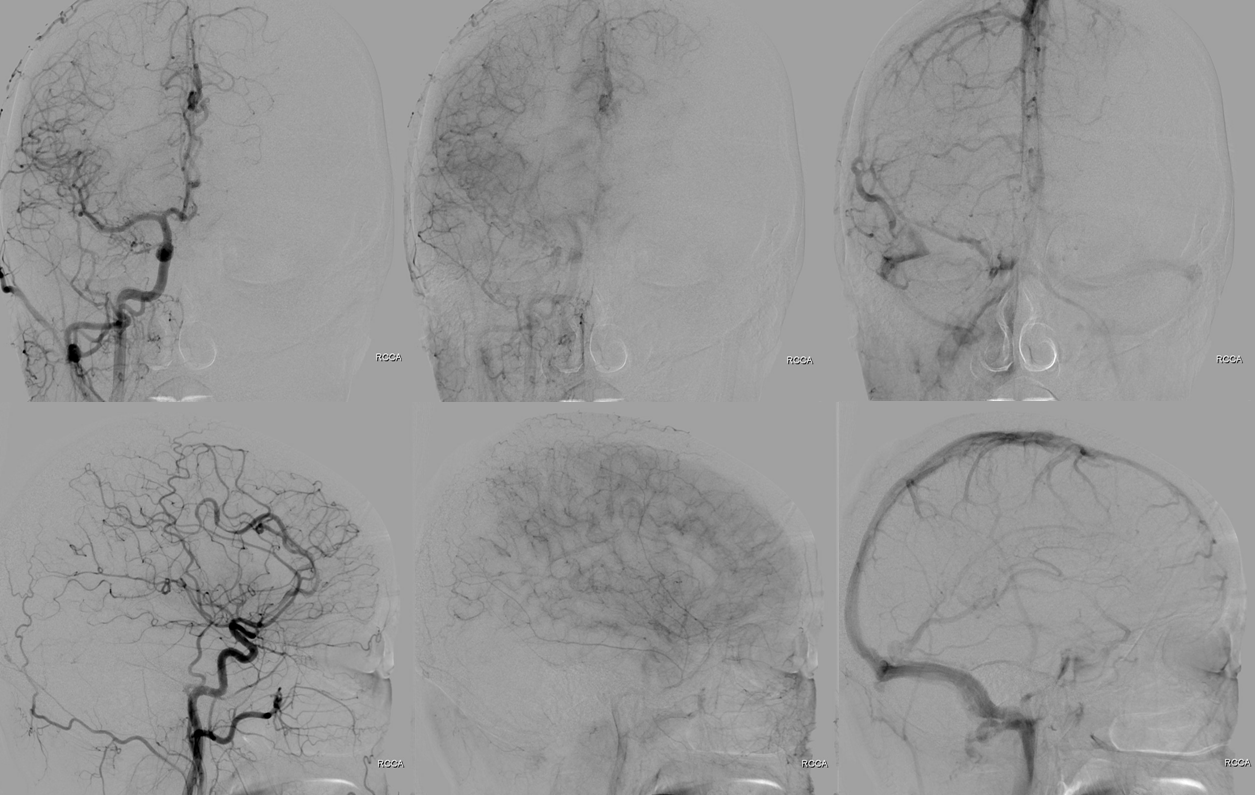
Angio. Less obvious but real ACA findings
Right side
Case 3 — incidental finding.
As in anything, there is a spectrum of findings. Case of short segment dolichoectasia.

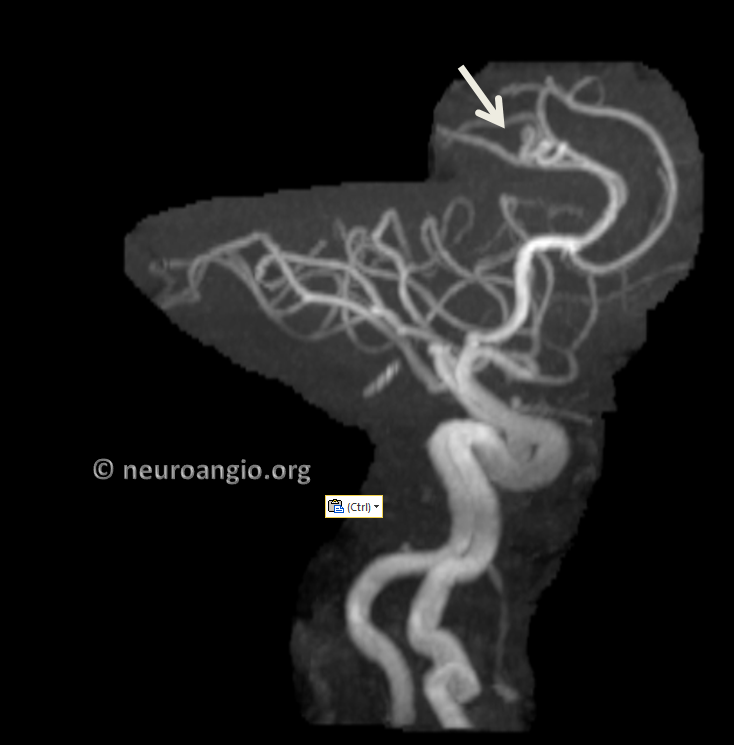
Case 4 — unilateral dolichoectasia. Why not? Could it be a dissection — theoretically yes but given overall appearance i think no.
Less calcification
Very much not subtle dysplasia, unilateral.
Different views.
Angio normal on left

Not normal on right
No shunt.
Oblique view
Conclusions — characteristic appearance. Dont mistake it for a fistula. If unsure angio will solve the dilemma. Look for adjacent cortical dysplasia.
Etiology — unknown. May be part of “Pure arterial vascular anomalies” — see https://www.ncbi.nlm.nih.gov/pubmed/28960150
Literature:
http://www.ajnr.org/content/16/7/1548
https://www.ncbi.nlm.nih.gov/pubmed/28960150