
Case Courtesy Dr. Chandra Sen
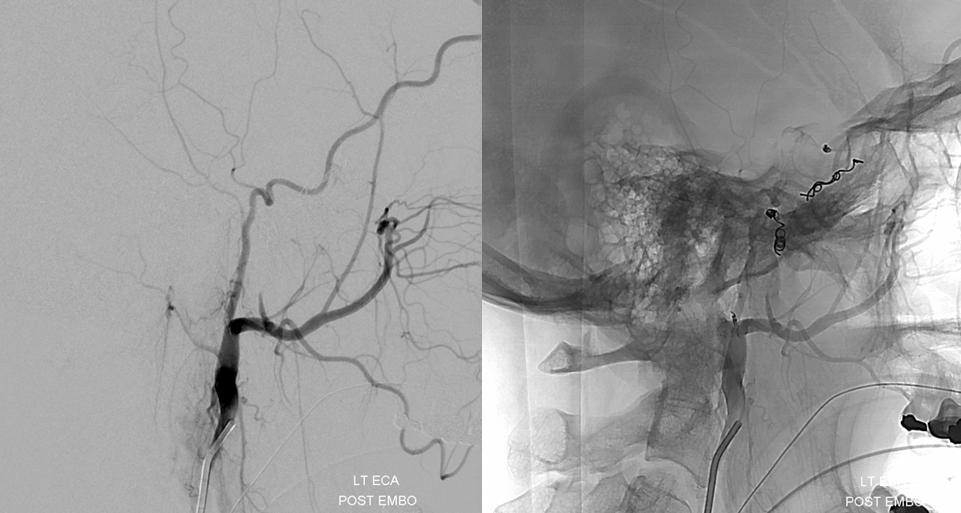
Another example of internal carotid branch embolization (ILT). The reluctance to embolize from MHT or ILT is many times unjustified. It is as easy to get into a dangerous anastomosis problem from any number of external branches which supply the same tumor. If anything, MHT and ILT make it easier because in the vast majority of times the only issue is reflux of particles into the ICA, whereas from other routes there may be several potential dangerous connections. We pretty much always use only small PVA particles for tumor embo, and usually close the branch afterward with pushable or detachable coils.
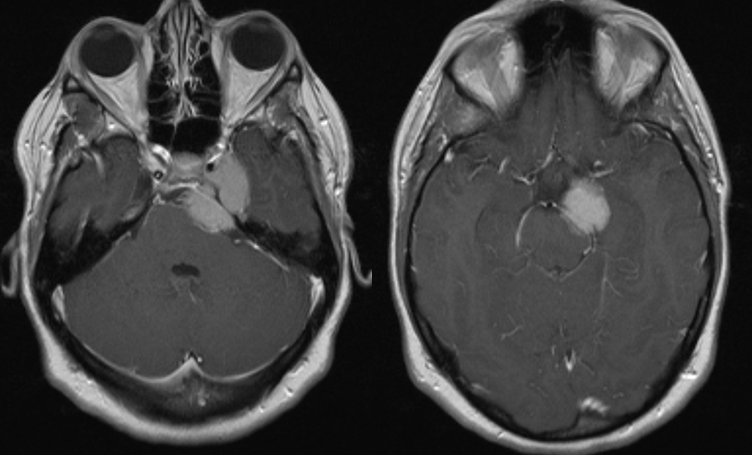
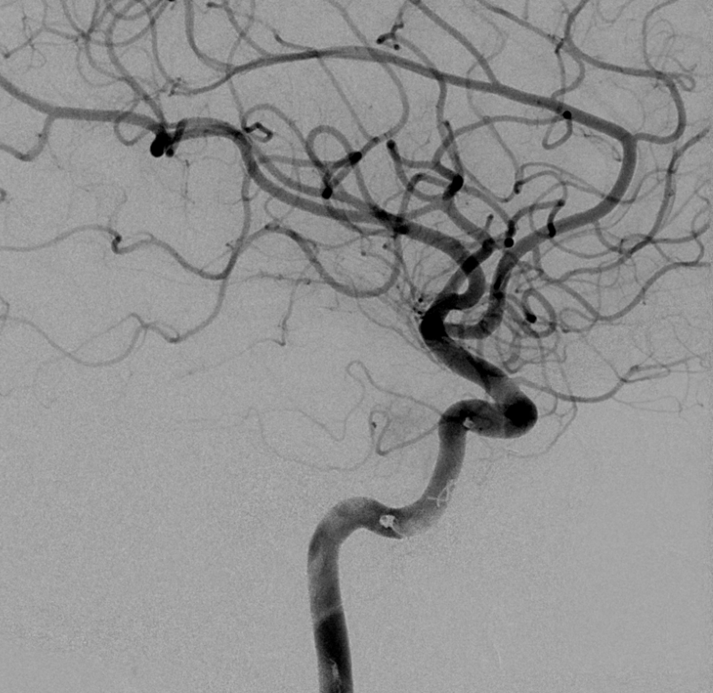
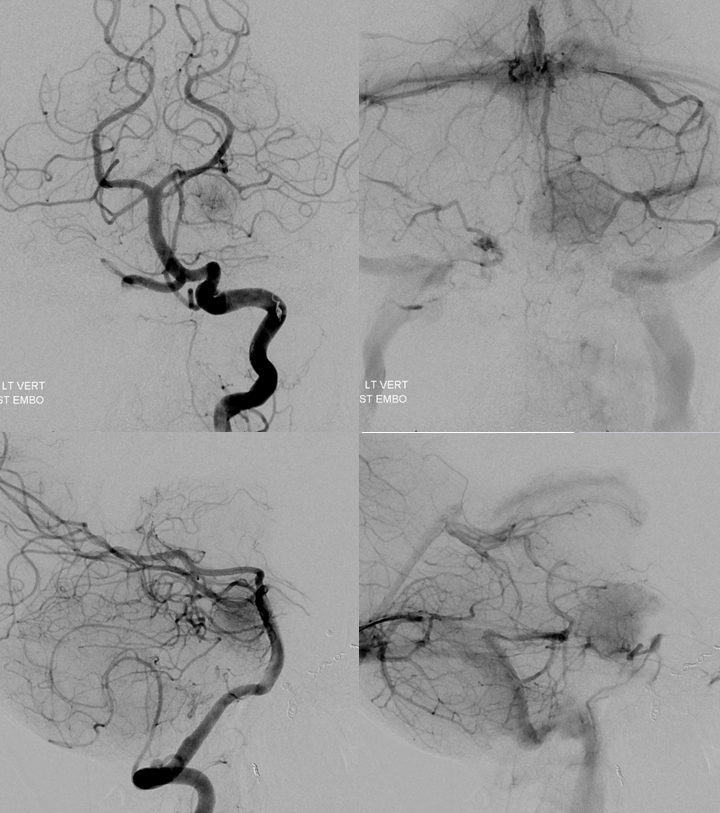
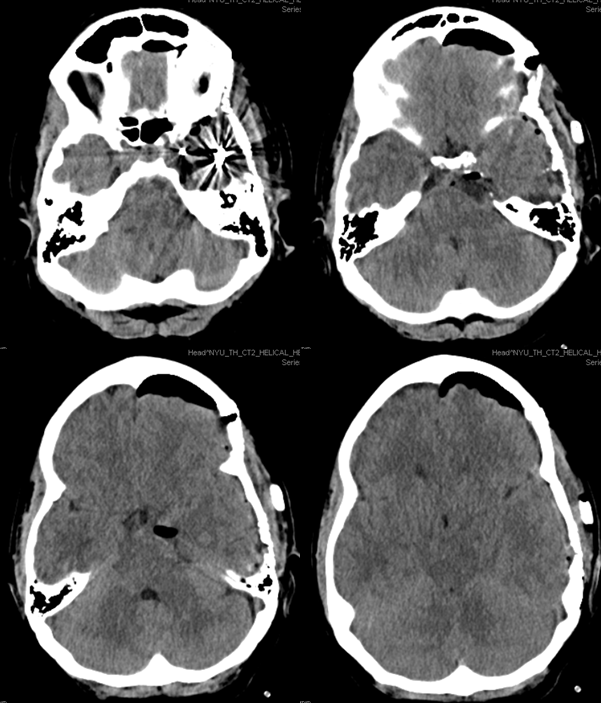
Vert shows significant pial supply from the left SCA region. Notice all kinds of mass effect.
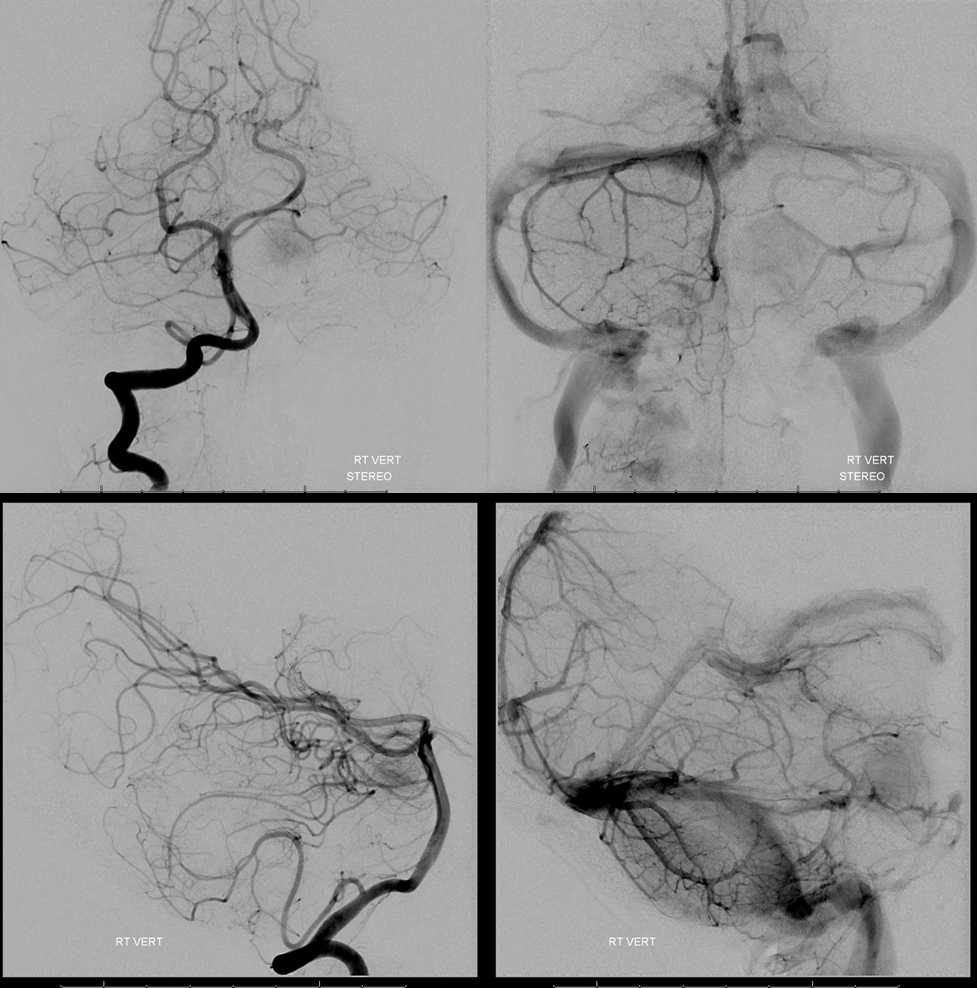
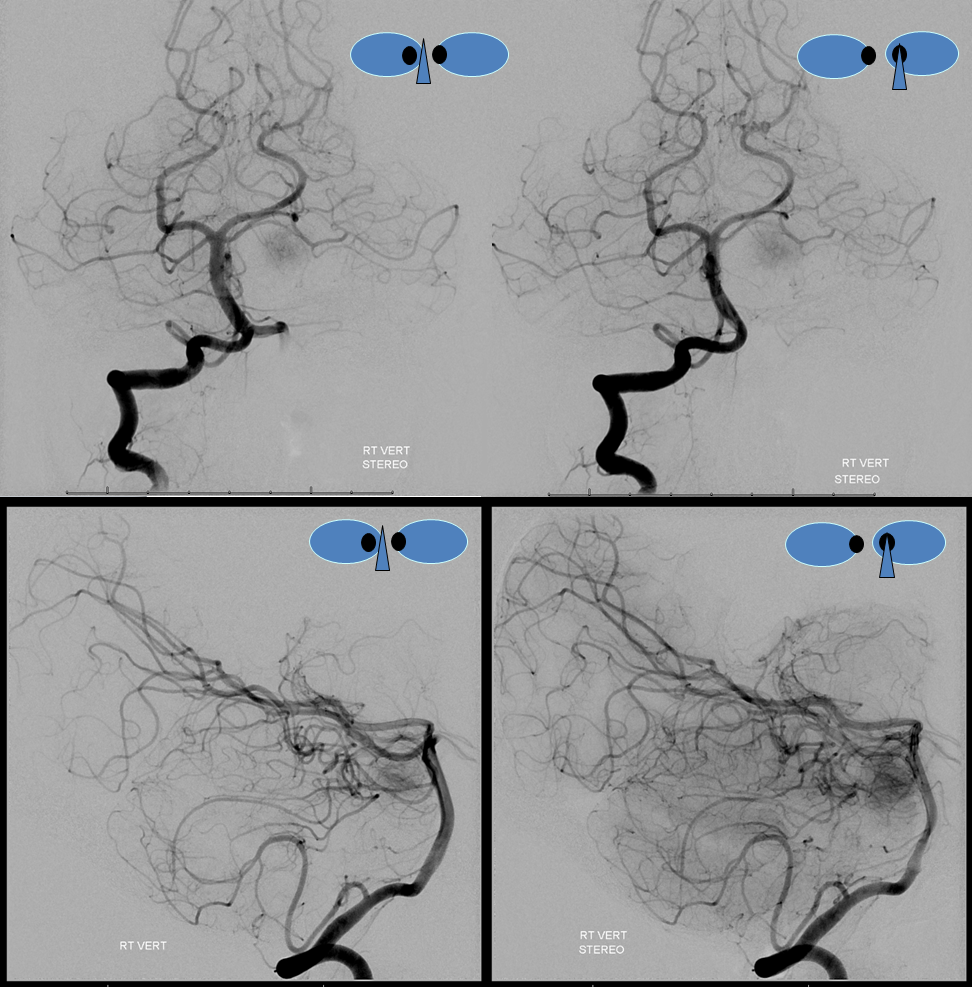
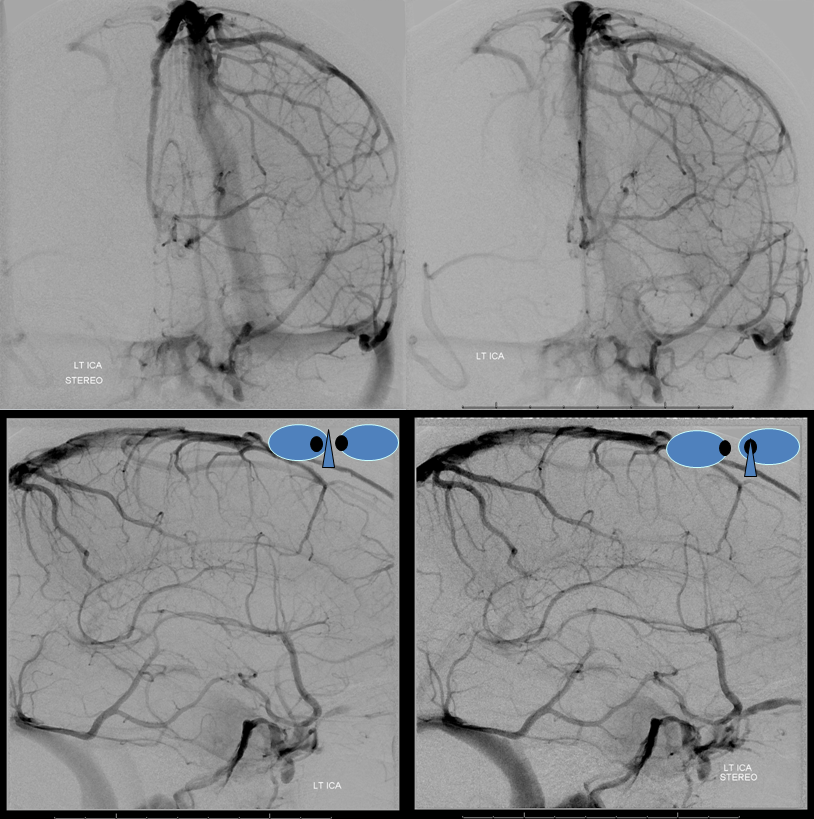
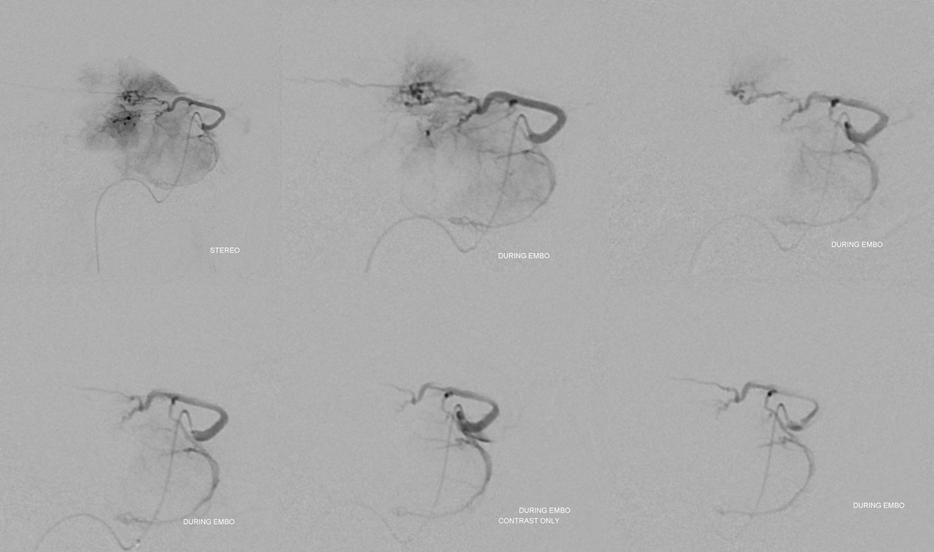
Obligatory stereos. Great for looking at mass effect
Left ICA shows dominant ILT supply. Notice an unusual thing here — the left cavernous sinus is open. In fact, both deep and superficial Sylvian veins drain into its lateral compartment (some call it paracavernous sinus). From there, drainage is usually via foramen ovale into the pterygopalatine venous plexus. Here, it does not happen. There is an occlusion apparently at the ovale area. Instead, the left lateral cavernous sinus drains into the posterior cavernous sinus and from there into both inferior petrosal sinuses (via the intercavernous sinus). See cavernous sinus page for more info. These patent sylvian veins are going to be an issue during surgery. On the good side, the Labbe is somewhat small and the superior petrosal sinus which is often sacrificed in these operations is also hypoplastic.
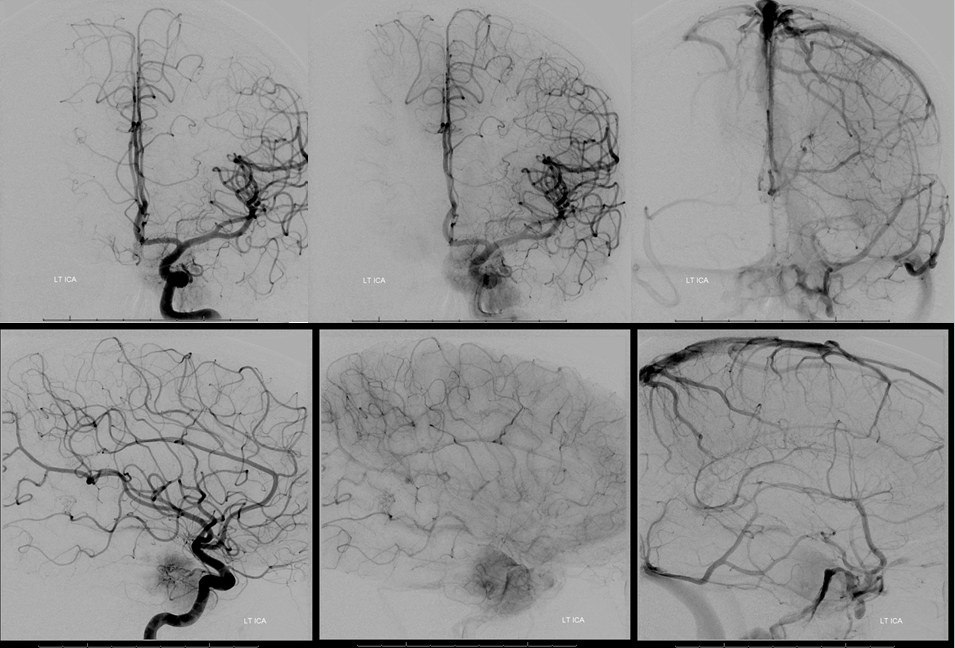
Venous phase stereos to look at how the sinus is draining.
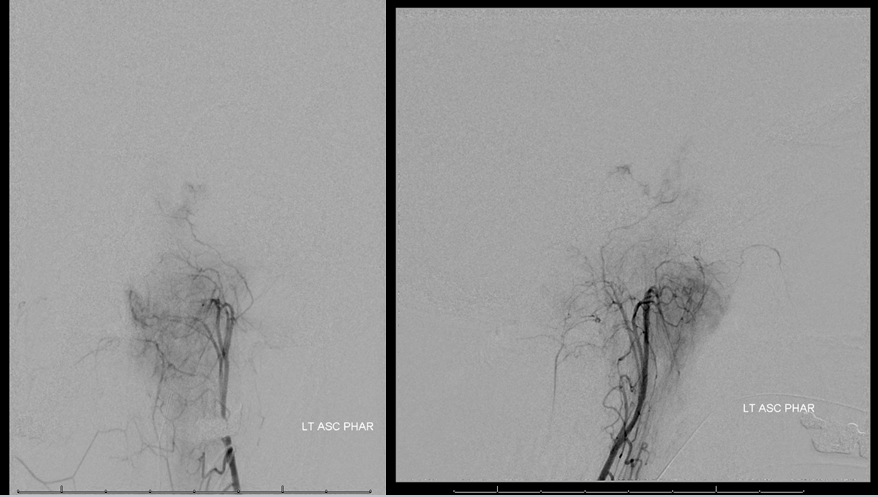
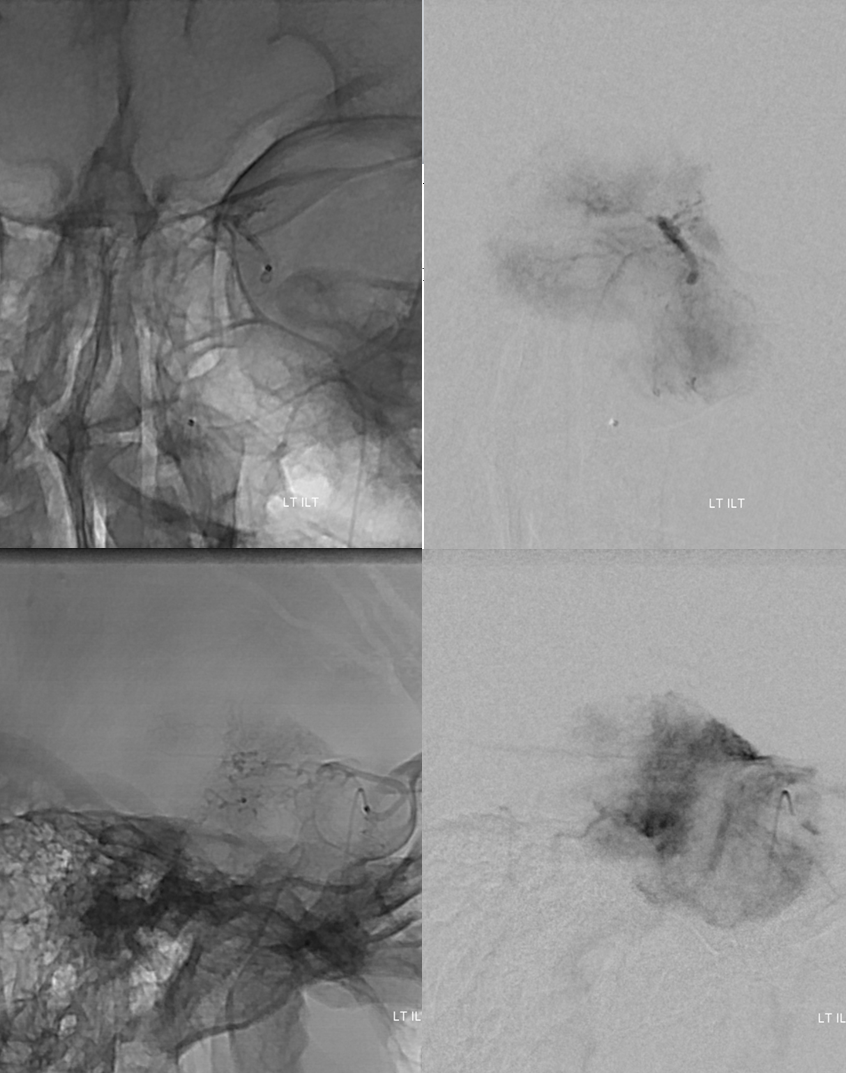
There is a very little bit of neuromeningeal trunk supply. Also present was a bit of proximal MMA supply via the petrosal branch.
Here is a magnified vie of the ILT . It is usually more difficult to get into the ILT compared to MHT, which as a rule is just straight back from the posterior genu, whereas the ILT is on the lateral wall and particularly difficult to get into when the siphon is tortuous
My preferred tools today are a combination Synchro 14 soft and Headway Duo. The duo is the smallest profile catheter on US market that will take a US market coil, and it follows the Synchro nearly perfectly so that even with a small amount of purchase into a trunk such as ILT catheterization is likely
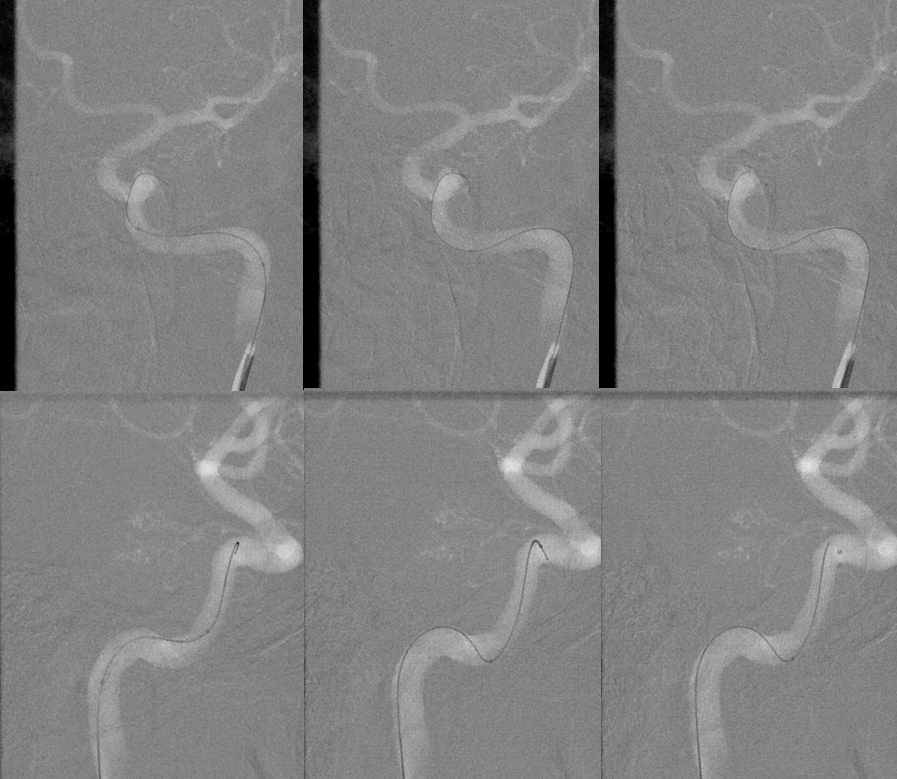
Micro DSA of ILT. Pretty juicy
A few millimeters of safety is plenty if you are careful. The more dilute the particles the longer the embo but less penalty for reflux and the particles dont clump as much. It is important to have runoff in the vessel and not be wedged. Wedge position is good for glue but bad for particles as they do not naturally flow into the tumor vascular bed with the current. Here we had awesome flow. Successive images show progressive devascularization of the tumor parenchyma with 45-150 micrometer PVA Contour particles. By the end, only the big trunks are visible but the actual tumor parenchyma is embolized.
A few Target nano coils finish the job. The nanos work great for this kind of tenuous purchase with little safety. If the catheter falls out at this angle it is likely that getting back in will not be possible without a wire. So, choose the softest coil
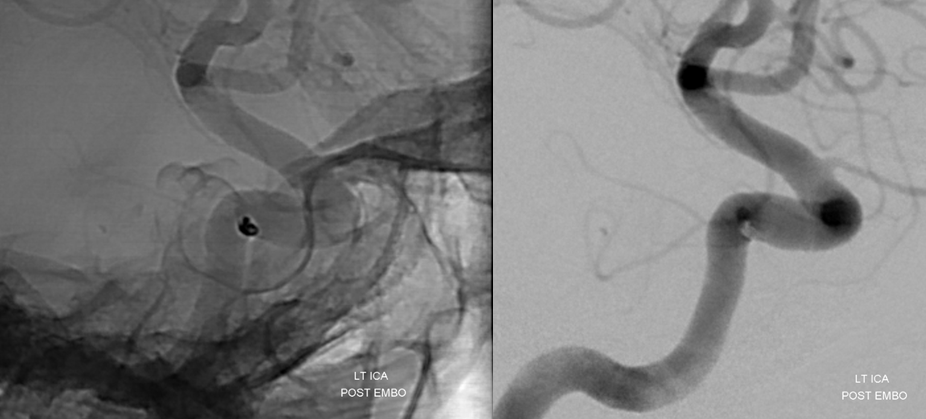
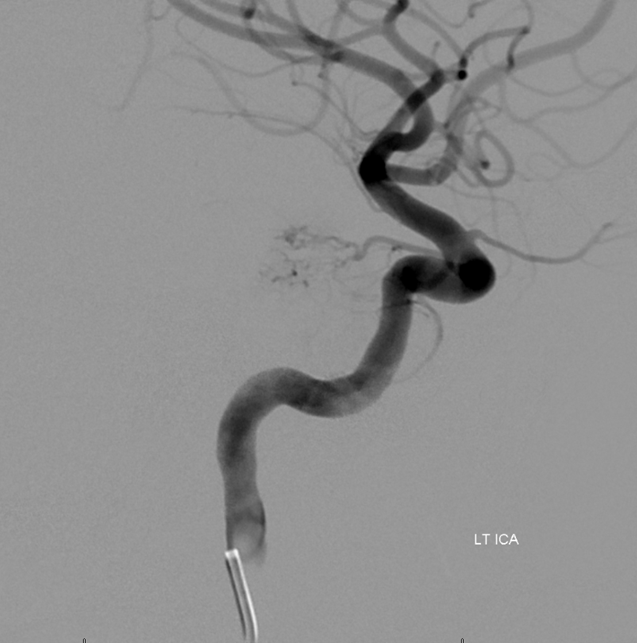
A more global ICA view
The distal MMA was closed with a few pushabl coils, followed by embolization of the petrosal contribution with small particles. In our experience the risk to facial nerve is real but quite low with particles alone. The parent MMA is then closed proximally with more coils. The neuromeningeal trunk was embolized with small particles next, followed by closure with a very small coil
Now, make no mistake. The back of the tumor is still very much alive via pial supply. Sometimes this can be embolized when the pial branch is in a non-eloquent area, as adjacent brain infarct is almost certain. In this case, we must leave the hard part to the amazing Dr. Chandra Sen
Well, the amazing Dr. Chandra Sen does it again! Pretty awesome resection, and those in the know understand how ridiculously skillful it is
See many other cases of mening embo in Cases section and on dedicated page “Preoperative Brain Tumor Embolization”