
A spectrum of post-traumatic fistulas can be encountered, the most famous of which is the direct carotid–cavernous fistula which is established by complete through and through tear of the cavernous segment of the internal carotid artery. However other less well-known ones are seen commonly when trauma patients are subjected to cerebral angiographic evaluation. One of these is a fistula between middle meningeal artery and adjacent middle meningeal vein or venous sinus (see case here). This patient regained consciousness after an accident where she was struck by a car, to discover new pulsatile tinnitus and right orbital congestion. CT shows multiple fractures. Notice enlarged right SOV (pink)

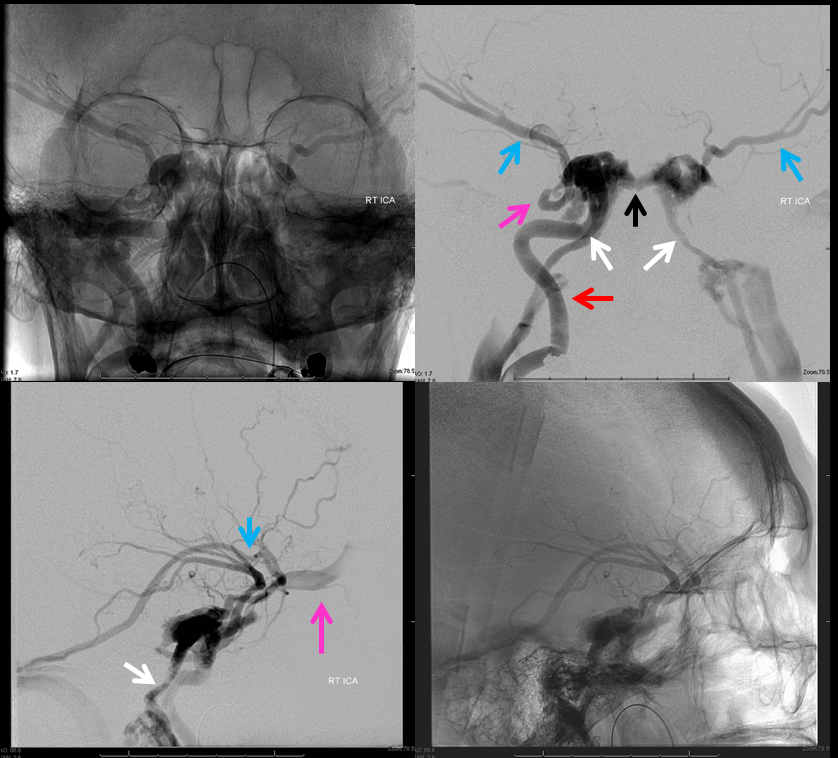
Right ICA (red) injection, visualizing bilateral superficial sylvian veins (blue), inferior petrosal sinuses (white), intercavernous sinus (black) and the right SOV (pink)
Vertebral injection opacifies the sigmoid sinus (blue) via C1 muscular branches (yellow); see CT scan above for occipital fracture in region of fistula. Notice retrograde PCOM support of the right MCA territory, and retrograde contribution to the fistula (red)

More vert injections showing the occipital, marginal, and sigmoid sinuses (blue) via C1 branches supplying the fistula

Occipital artery injection opacifies the same C1 muscular network seen already via the vert

Another consequence of trauma is a stable accessory meningeal pseudoaneurysm, without hemorrhage. The carotid cavernous fistula has since been closed with coils

Questions/ comments apply here