
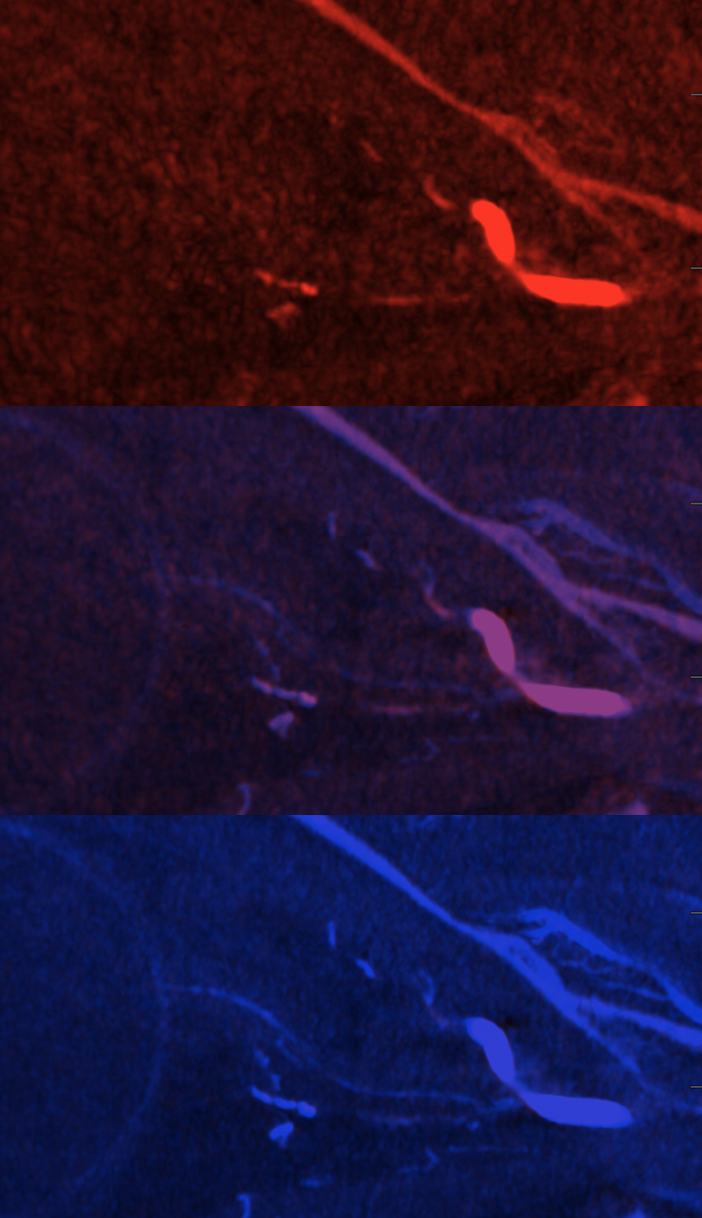
CRAO can be very hard to diagnose. Clinical history and ophthalmologic exam are current standards. However exam can be difficult especially when occlusion is retrobulbar — looking for secondary signs etc. High resolution cone beam CT can reliably identify the central retinal artery — see our publication here. However, cone beam CT images can take a while to acquire, mixing arterial and venous phases. There is a central retinal vein — adjacent to the artery — that can make distinction difficult.
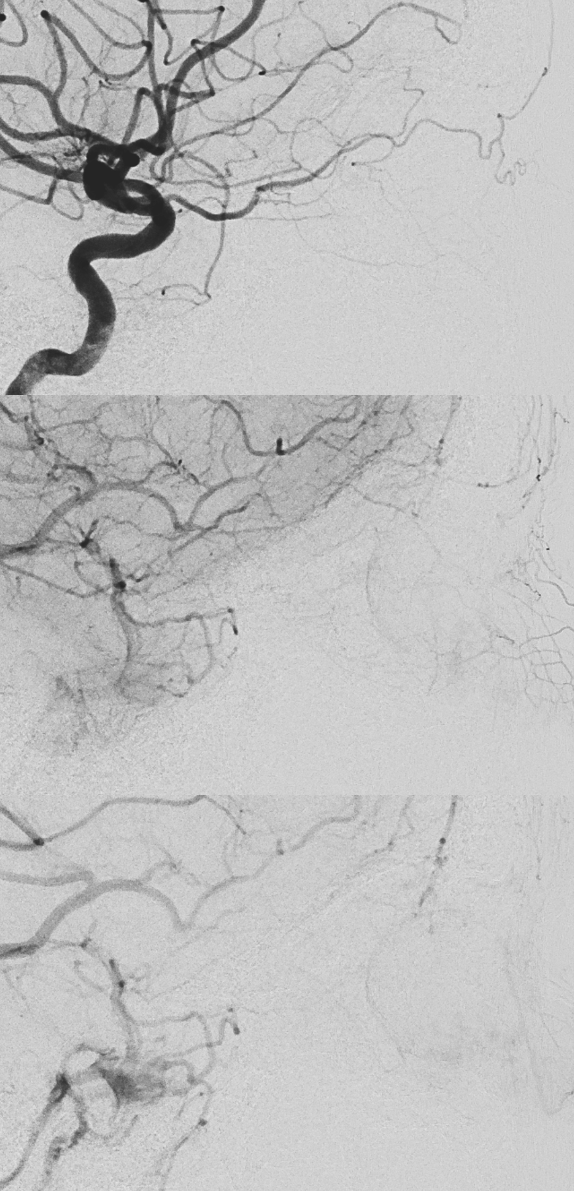
Below is an example. Patient presents with sudden onset vision loss. Angio is classic — globe still there — because of choroid blush — choroid supplied by long and short ciliary arteries. Presence of blush does not rule in our rule out blindness
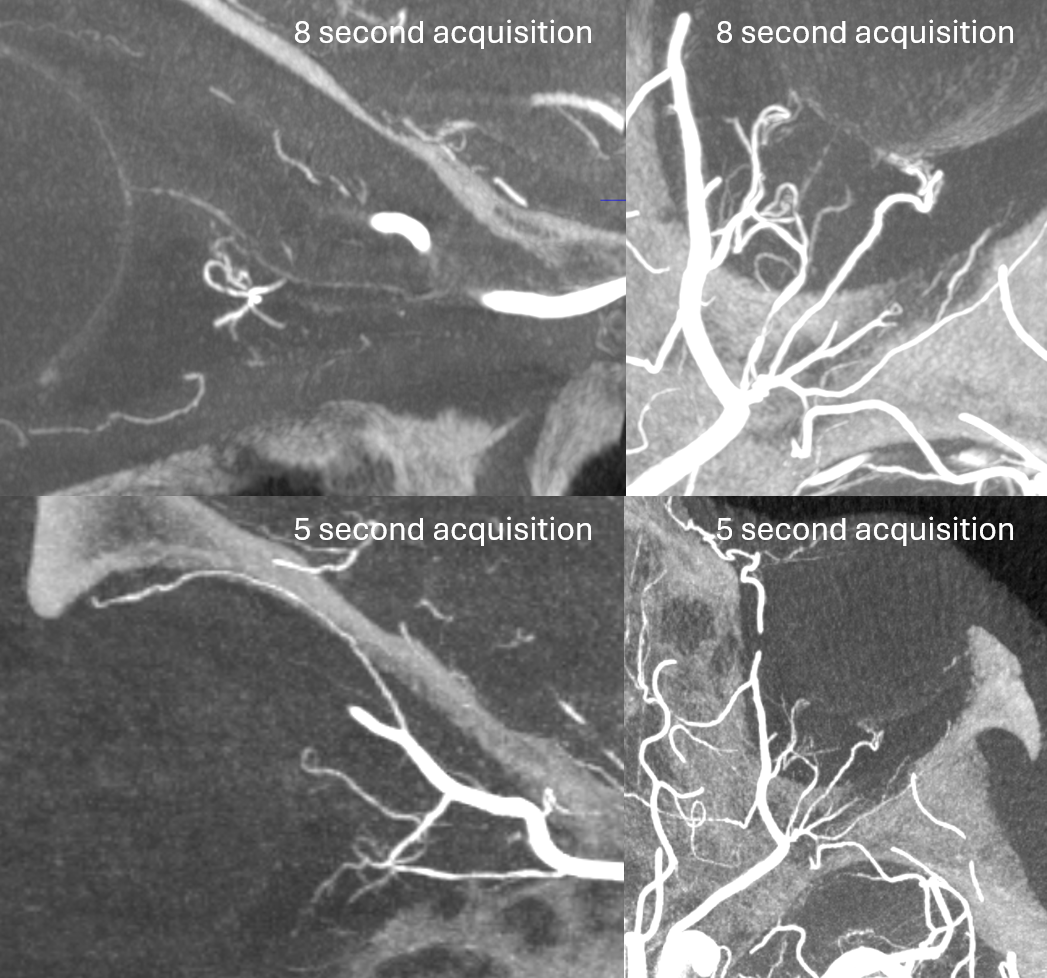
DYNA CTs — see the difference between 5 and 8 second acquisitions — there is a 1 second delay with 4 and 7 second “DYNA” options currently available on the Siemens Icono

Patient improved markedly following IA tPA infusion