
Excellent example of trans-ophthalmic ethmoid fistula cure
Incidental operculum AVM also…
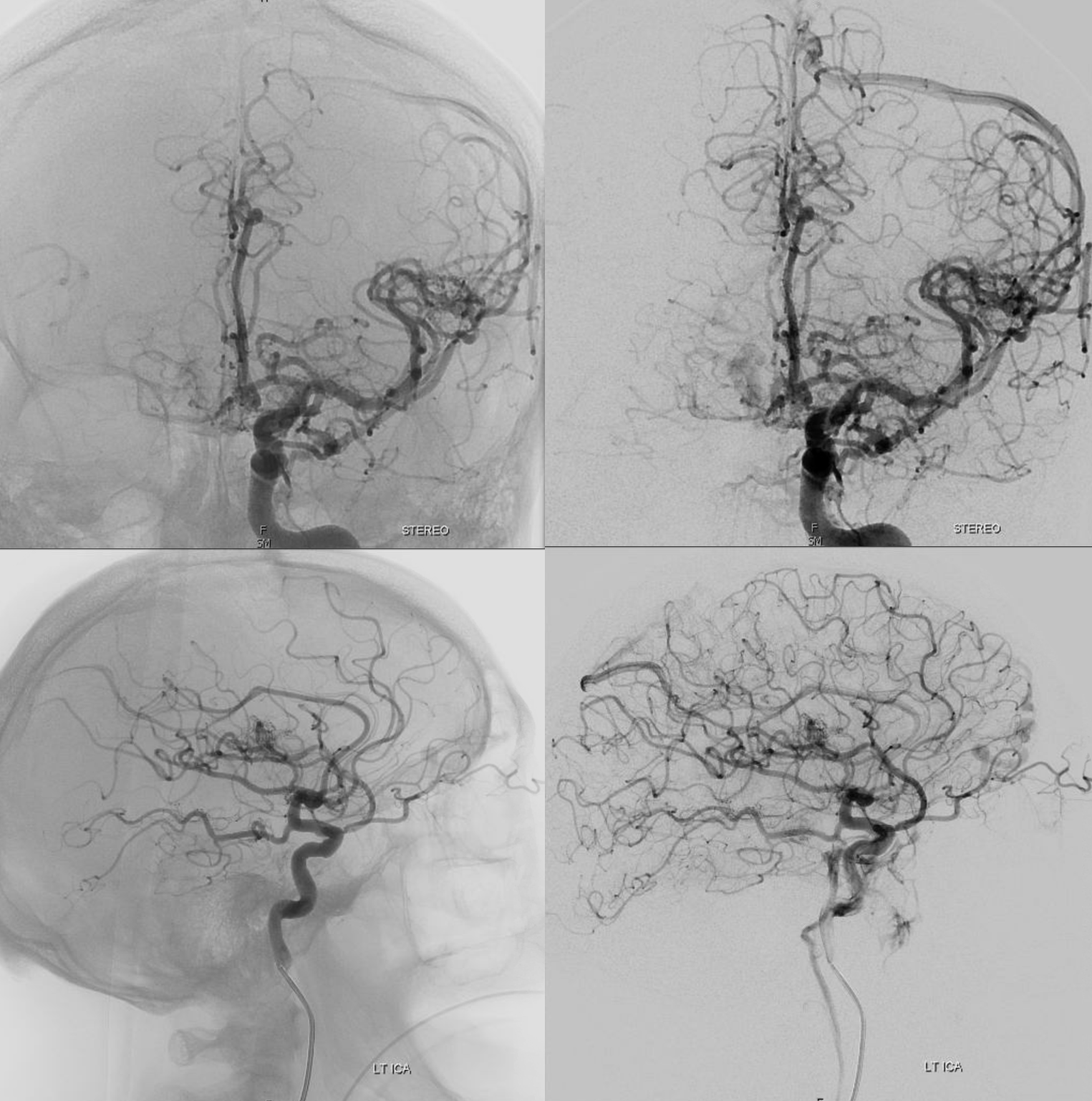
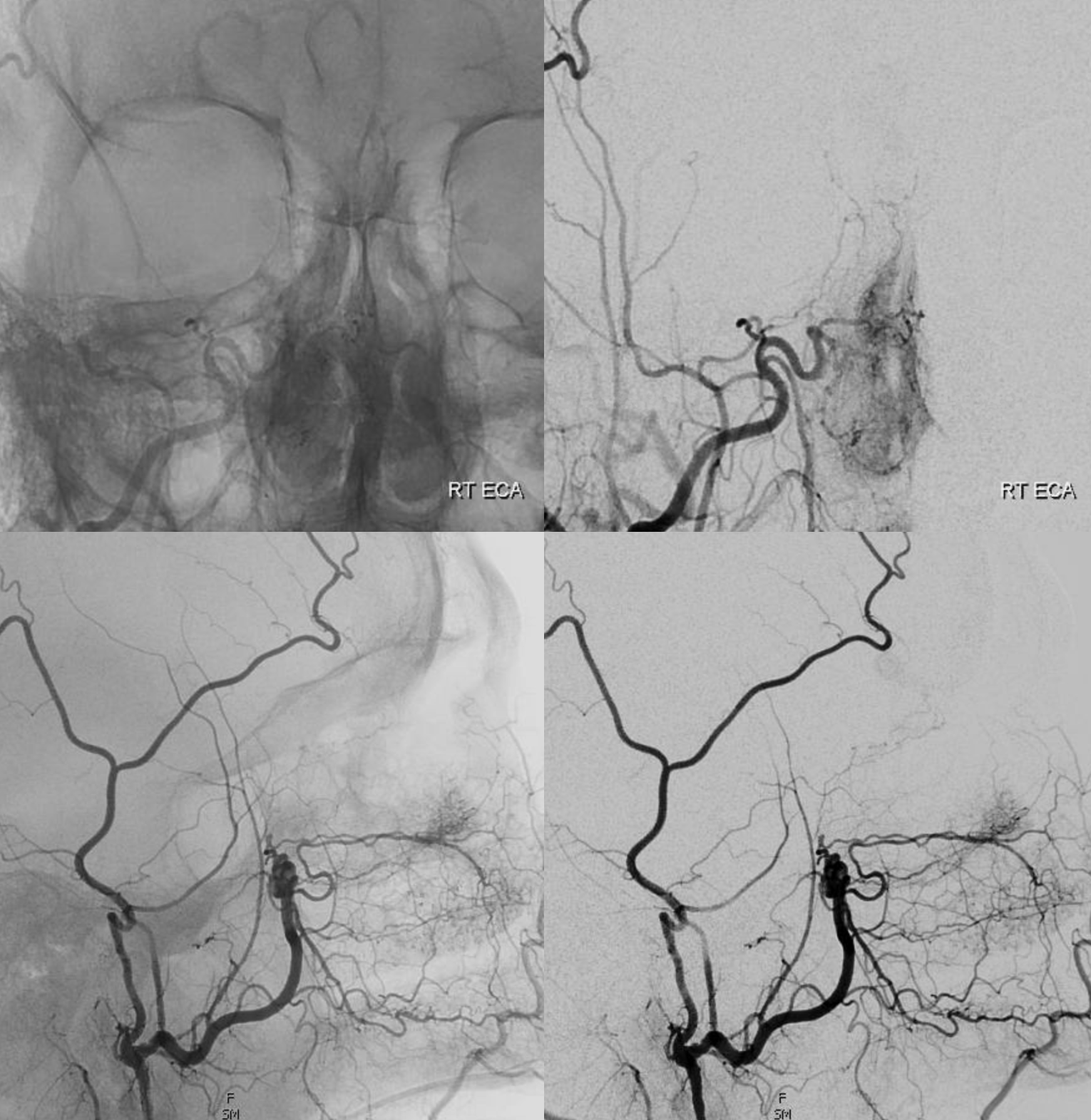
Most of supply to ethmoid fistula is from right anterior ethmoid branch
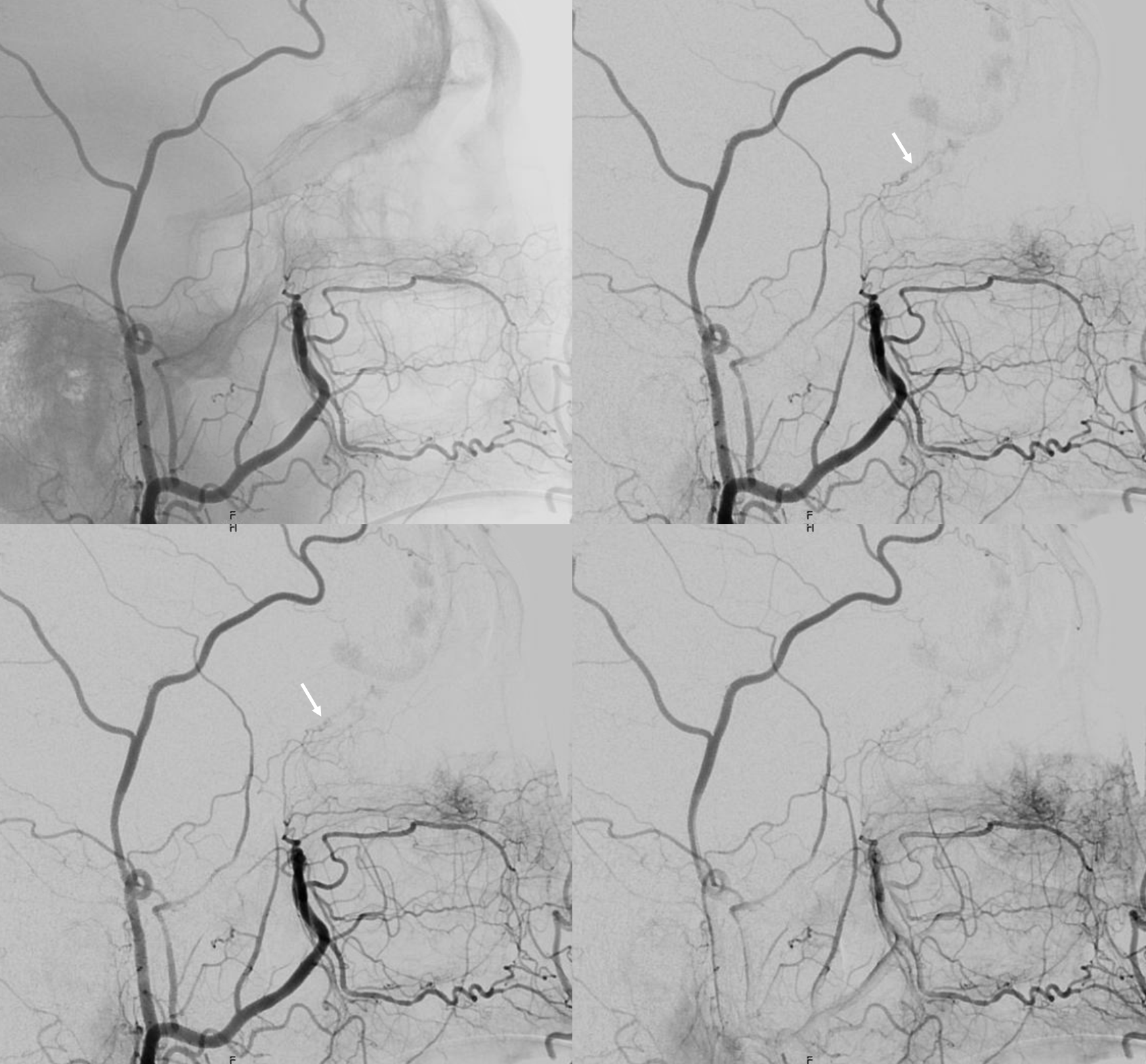
The external contribution is via septal branches collateralizing with the anterior ethmoid (arrow) partially opacified via this connection
Frontal and lateral
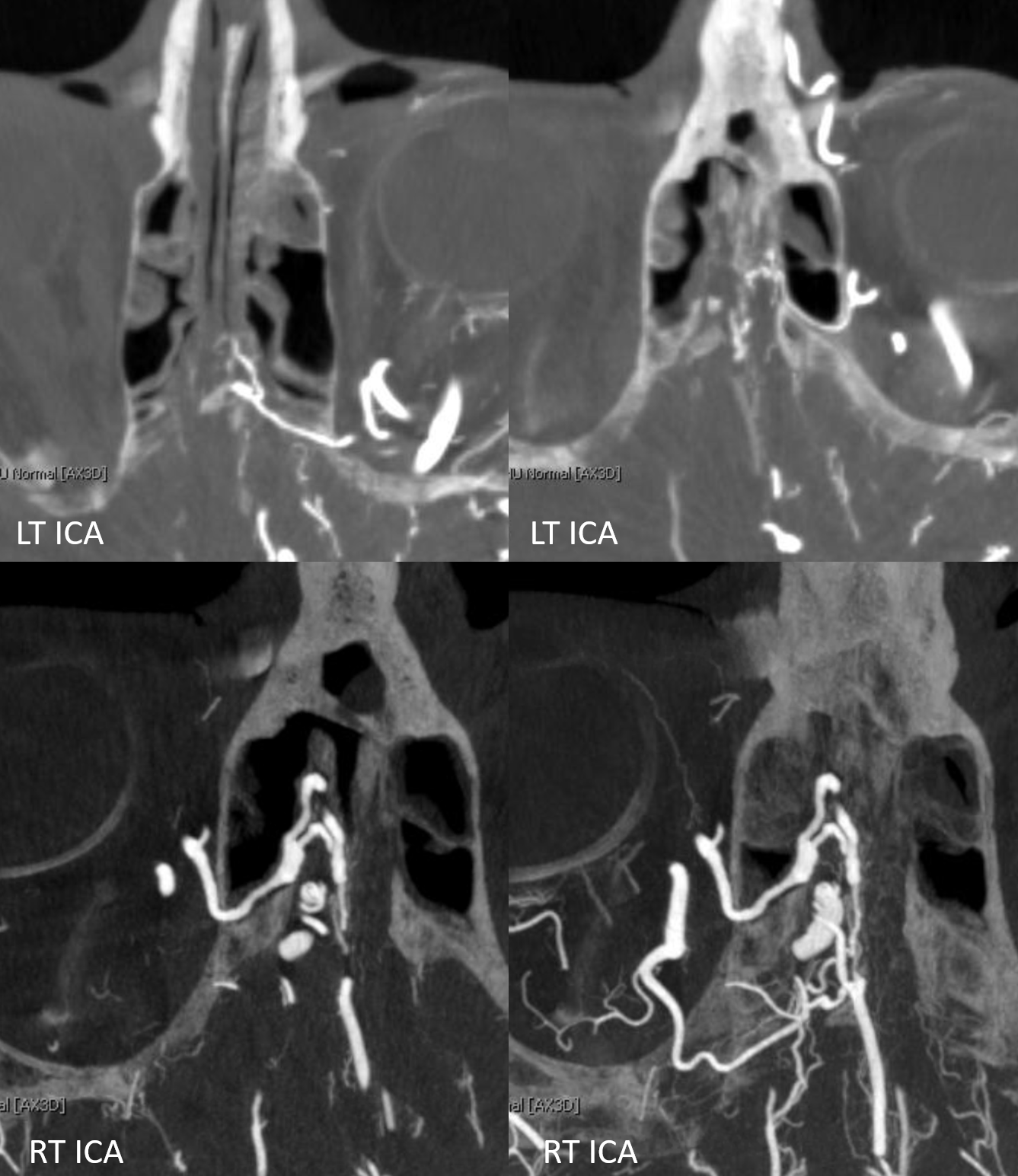
DYNA is always nice. See bilateral anterior and posterior ethmoidal arteries
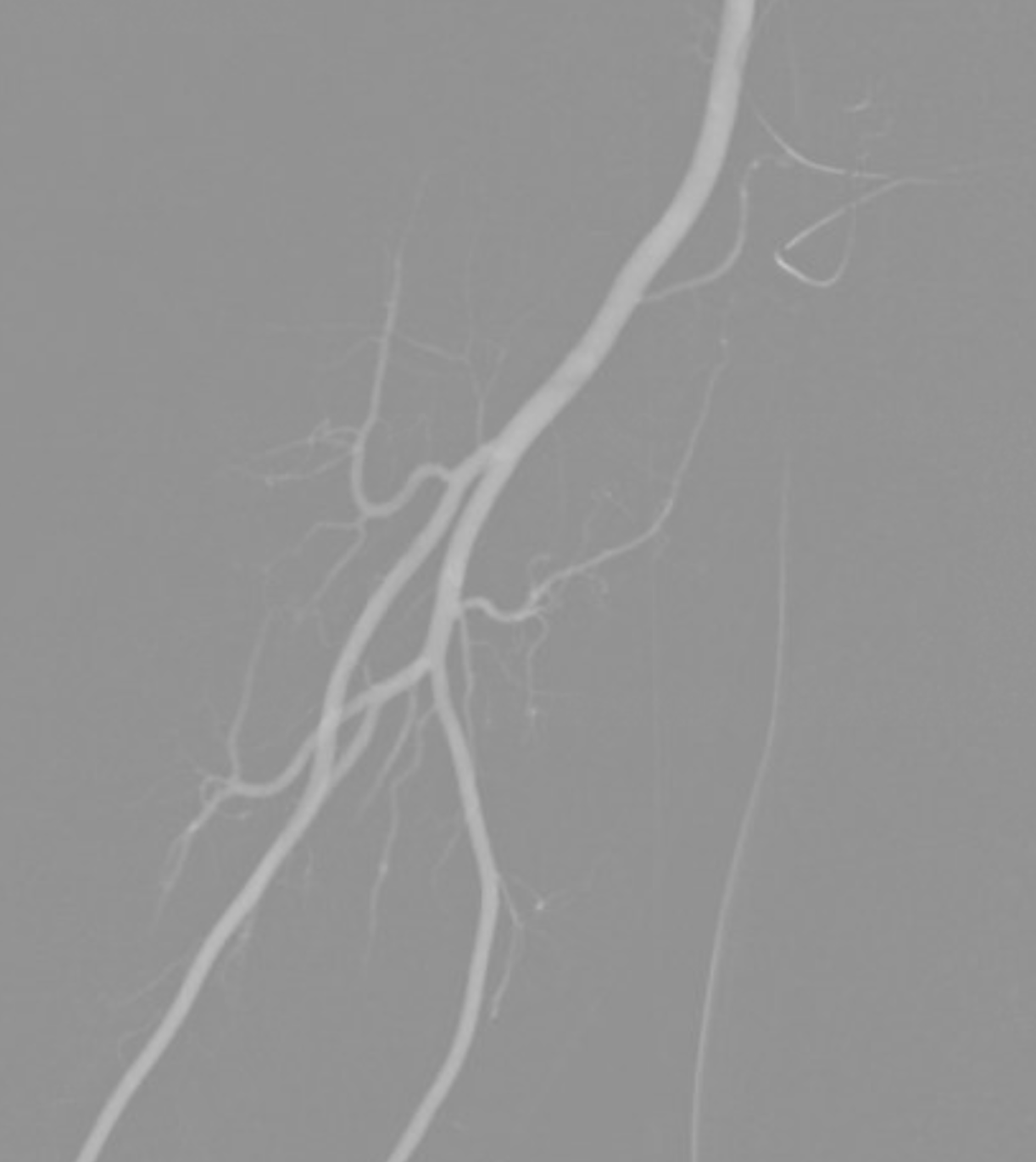
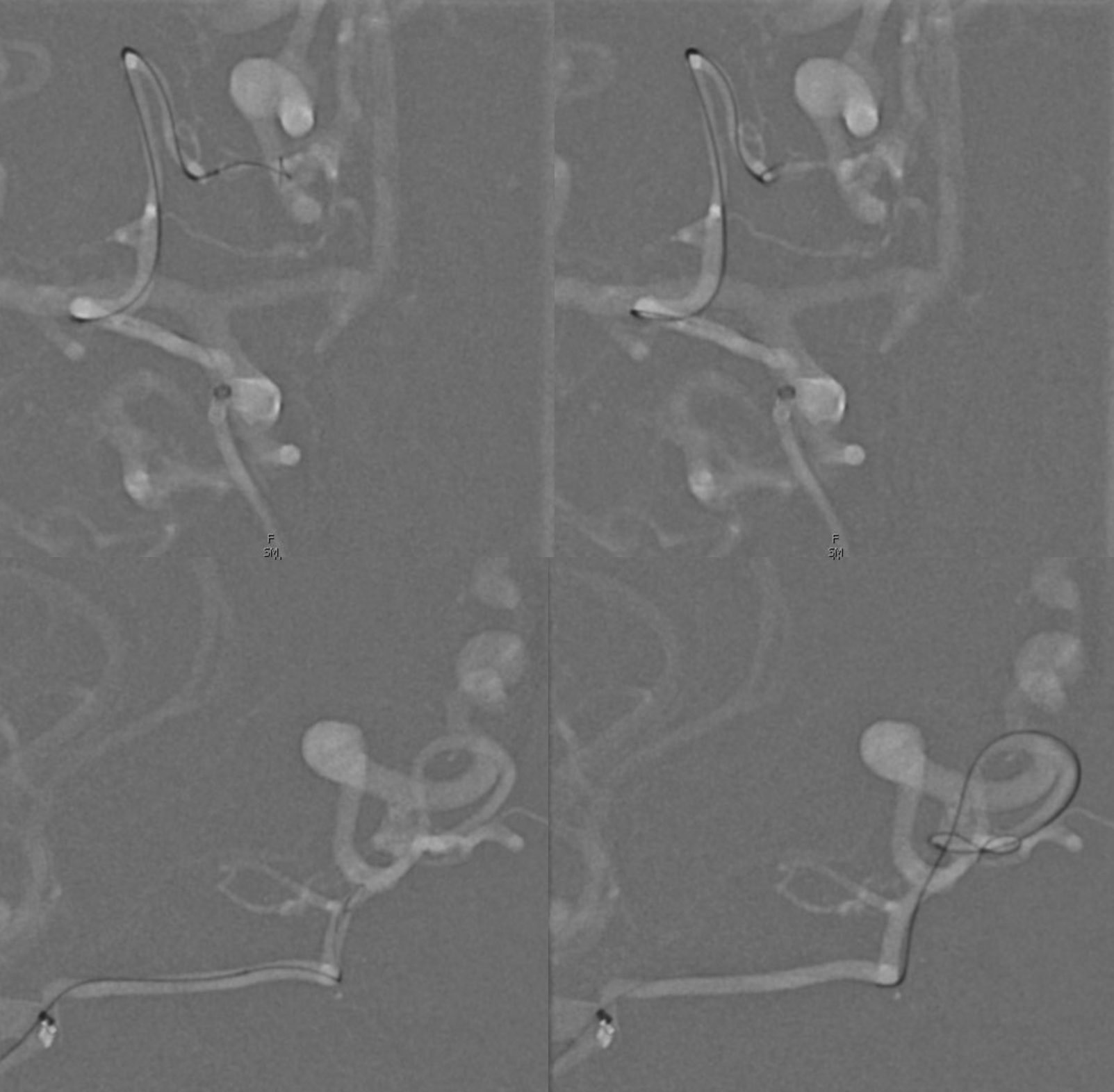
Our preferred ophthalmic catheterization is with a flow-guided catheter and a low profile wire. Here its Magic 1.5F Olive and Hybrid 0.08 with a Sofia 5 as intermediate. The Magic is likely to allow good flow around the microcatheter and tends to do its Magic going distal without wire sticking out. A J-wire tip helps a ton to go to the right place and will not poke the central retinal either
Glue position on top, glue cast on bottom. This was a 1:1 Lipidol:nBCA dilution. See the inflow from other pedicles in the proximal vein? The fistula is at the tangle just before that
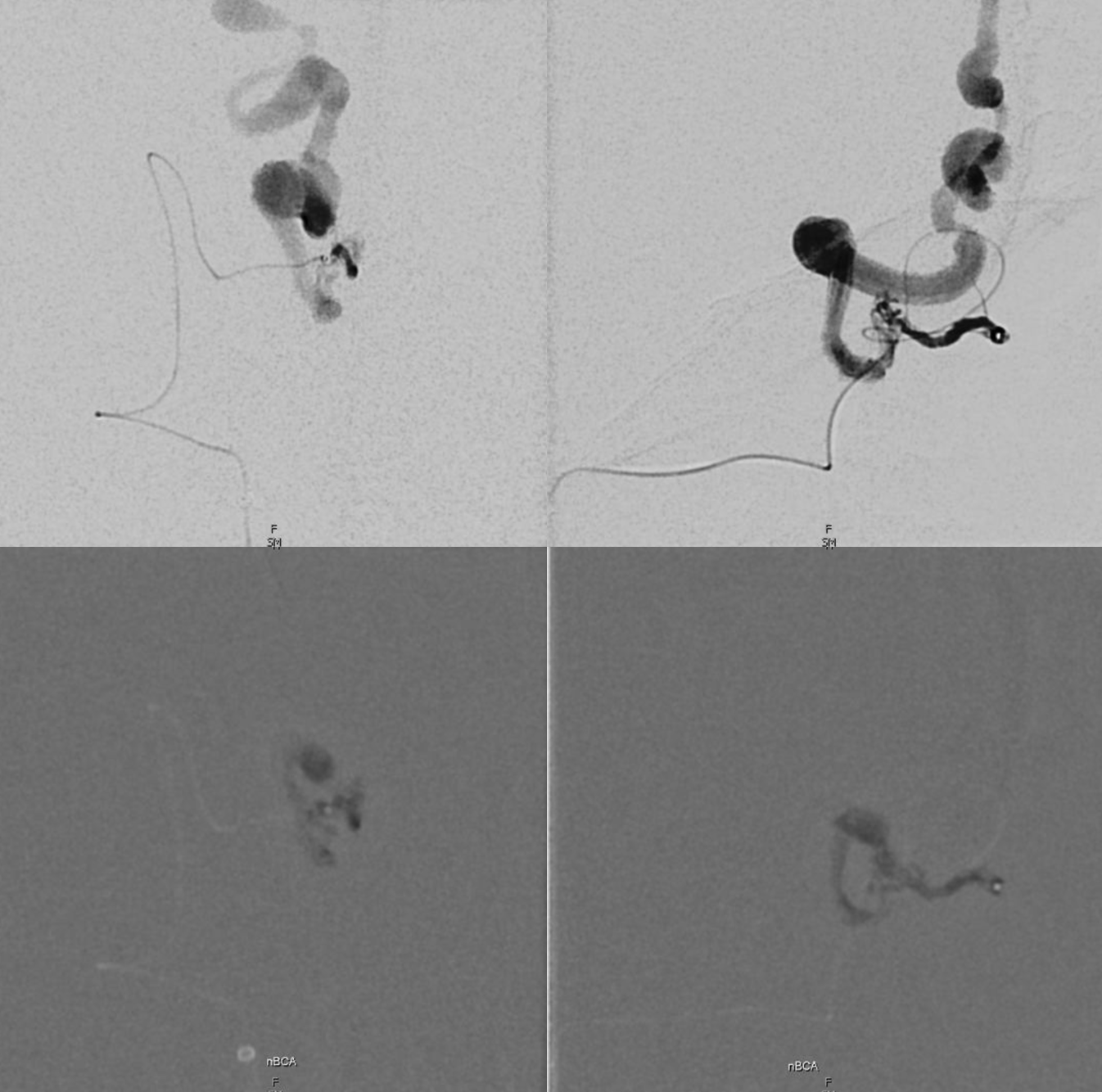
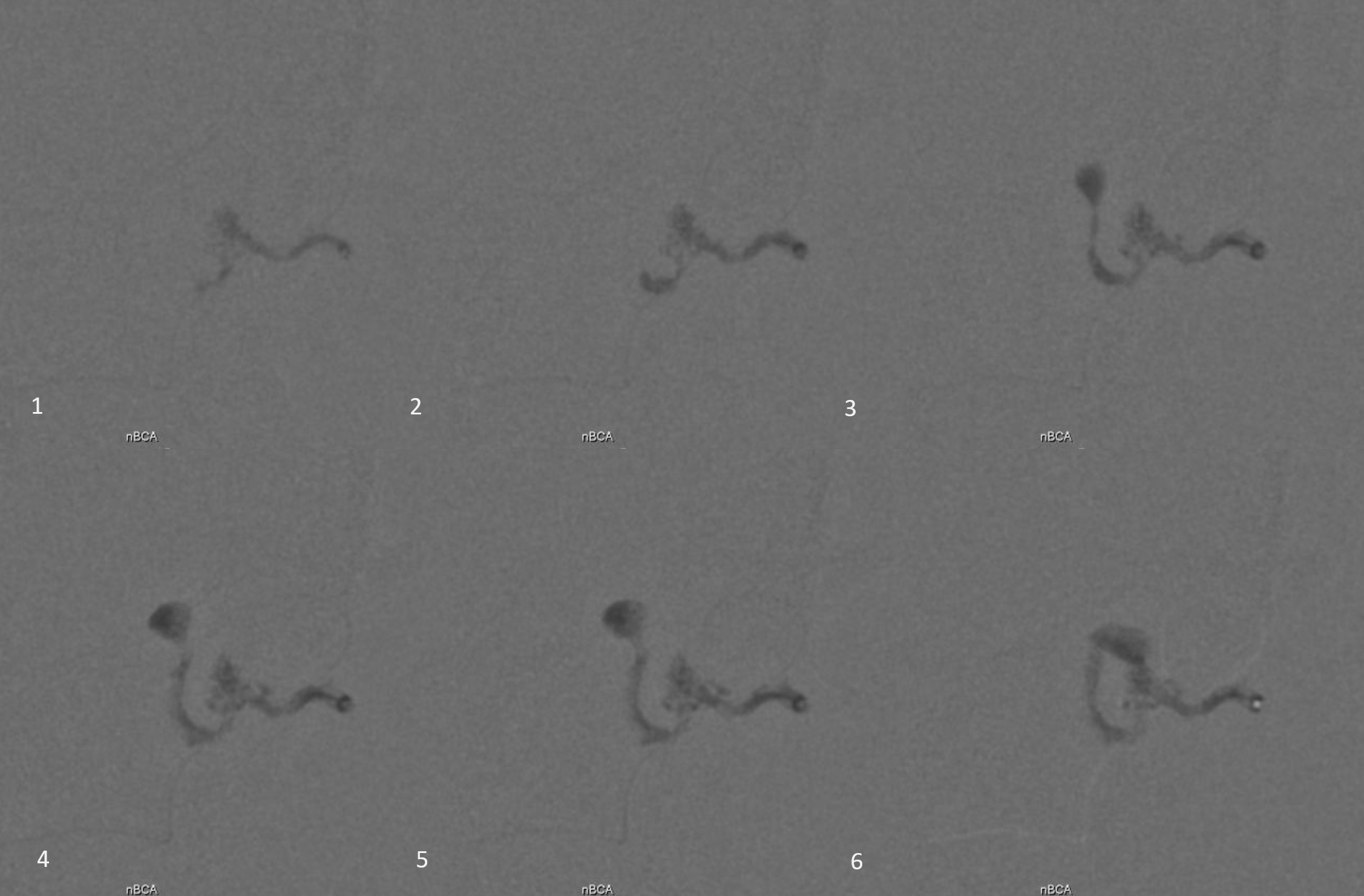
Sequential frames of glue injection. Definitely have a good amount of it in the vein. The most important thing in this kind of glue injection is not to have reflux, for 2 reasons. First, because refluxed glue often stays on the catheter tip as it is being pulled, and has a chance of breaking off somewhere during the pull — say in the proximal ophthalmic. Not good. The second reason is that when there is no reflux the pull can be gentle and easy. Its reflux that leads to forceful pulls, even if “gluing in” of the catheters is exceptionally rare now. A forceful pull in the ophthalmic is probably best avoided. How to avoid reflux — wedge or flow control position. That’s what we had here, and it worked.
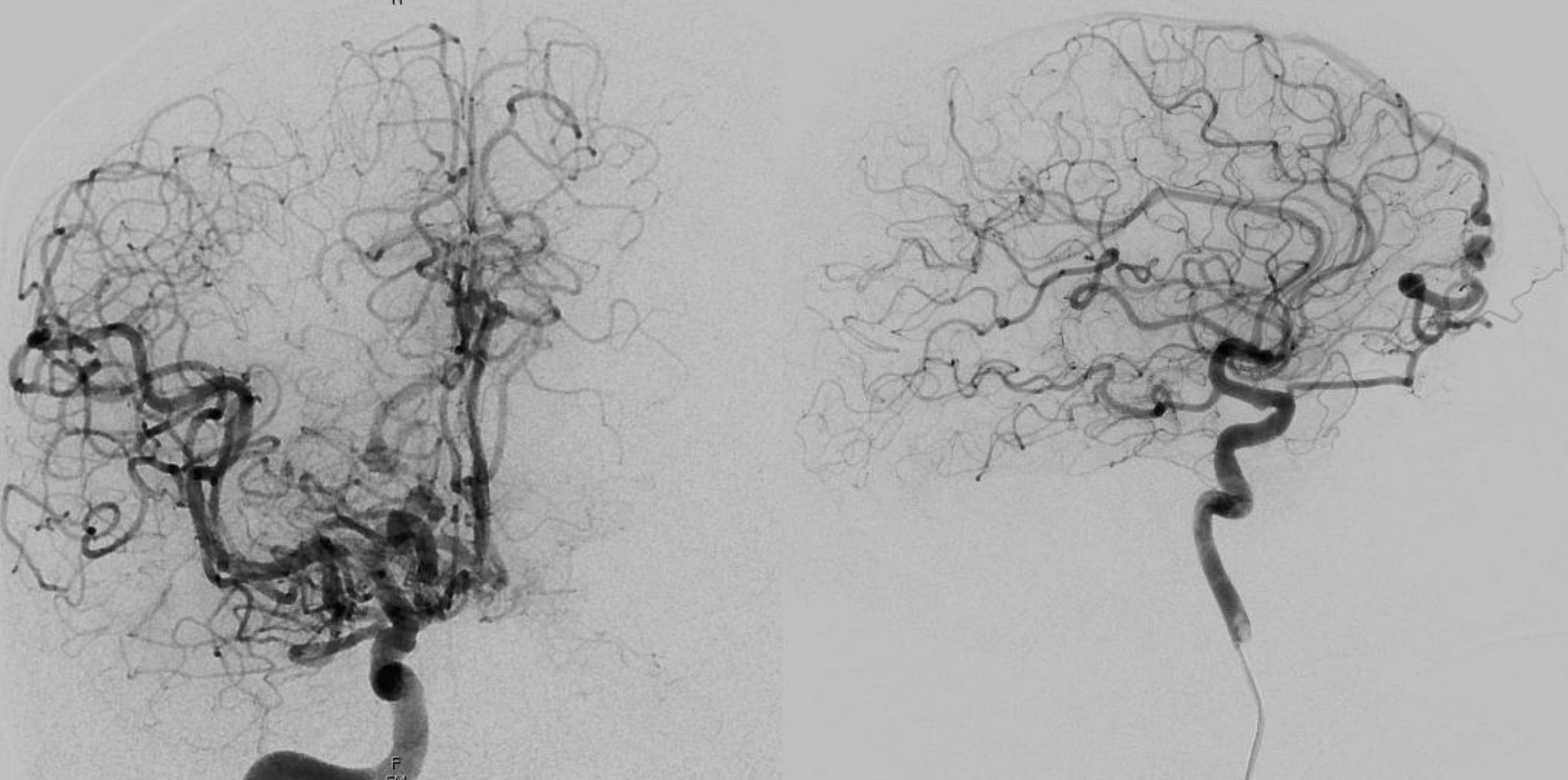
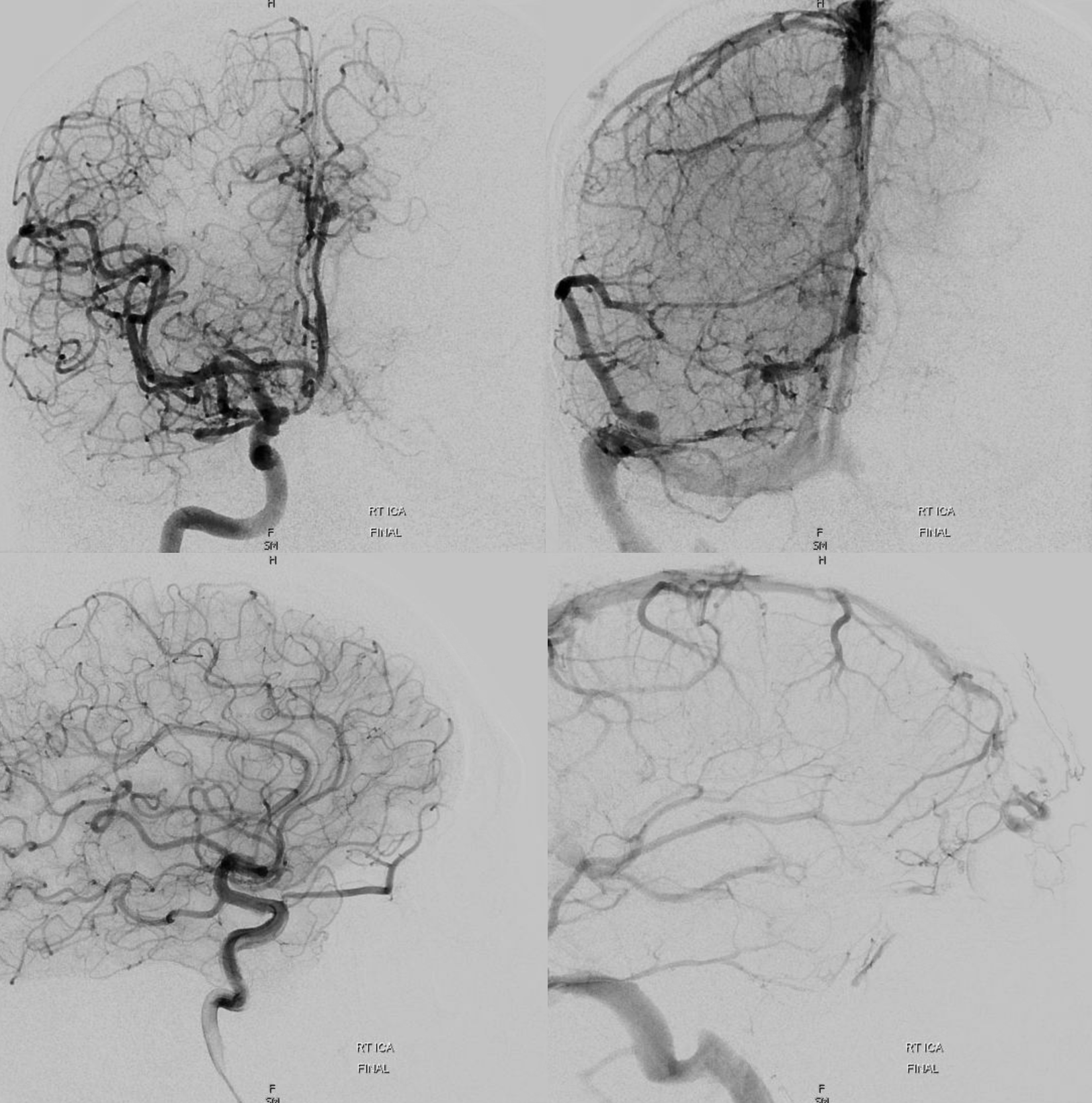
Despite that, fistula is still alive immediately after
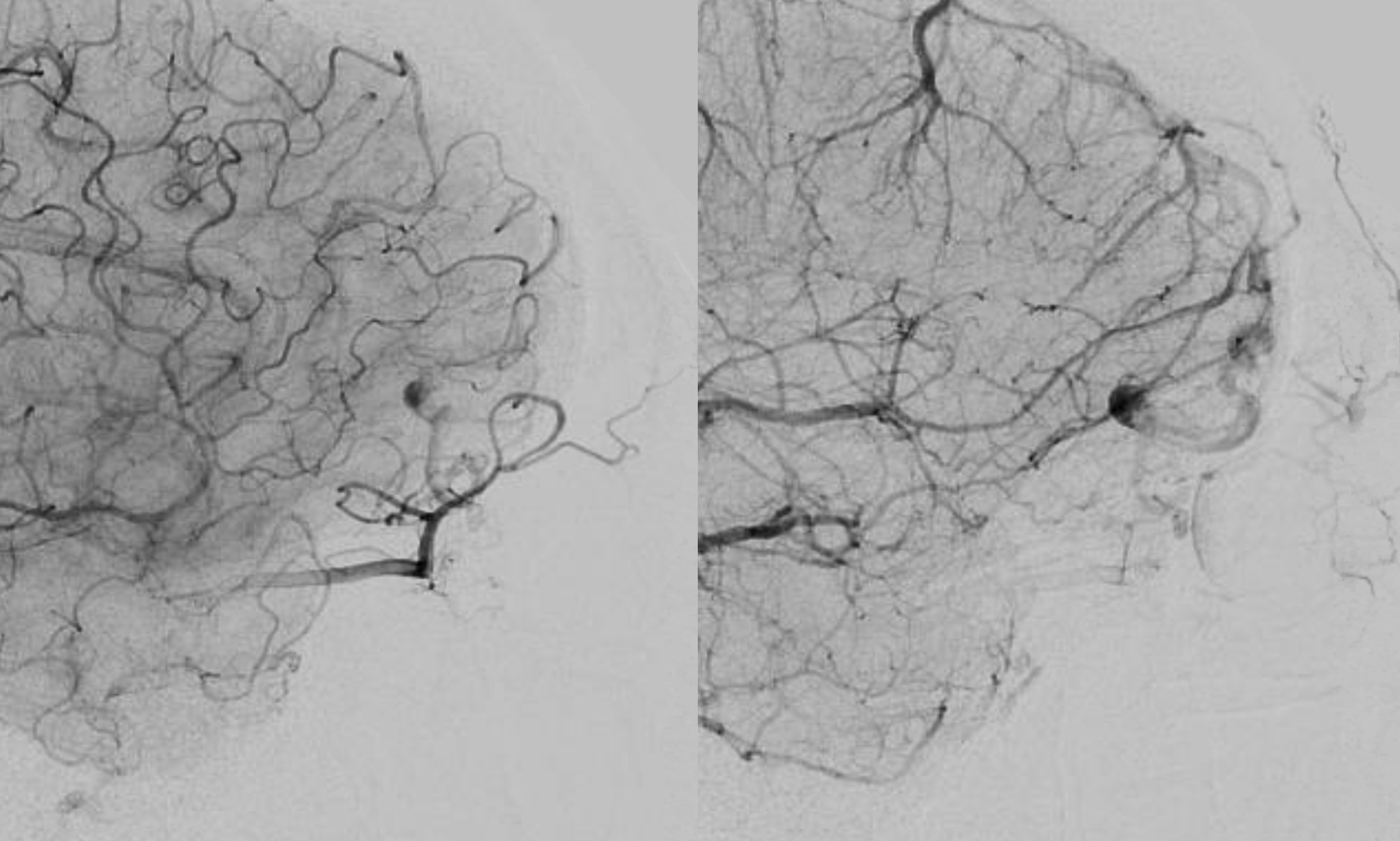
No prob. Just wait a bit — with lots of glue in the vein, thrombosis is likely, as seen below after about 20 minutes.
See another case of ophthalmic route ethmoid fistula embolization here