
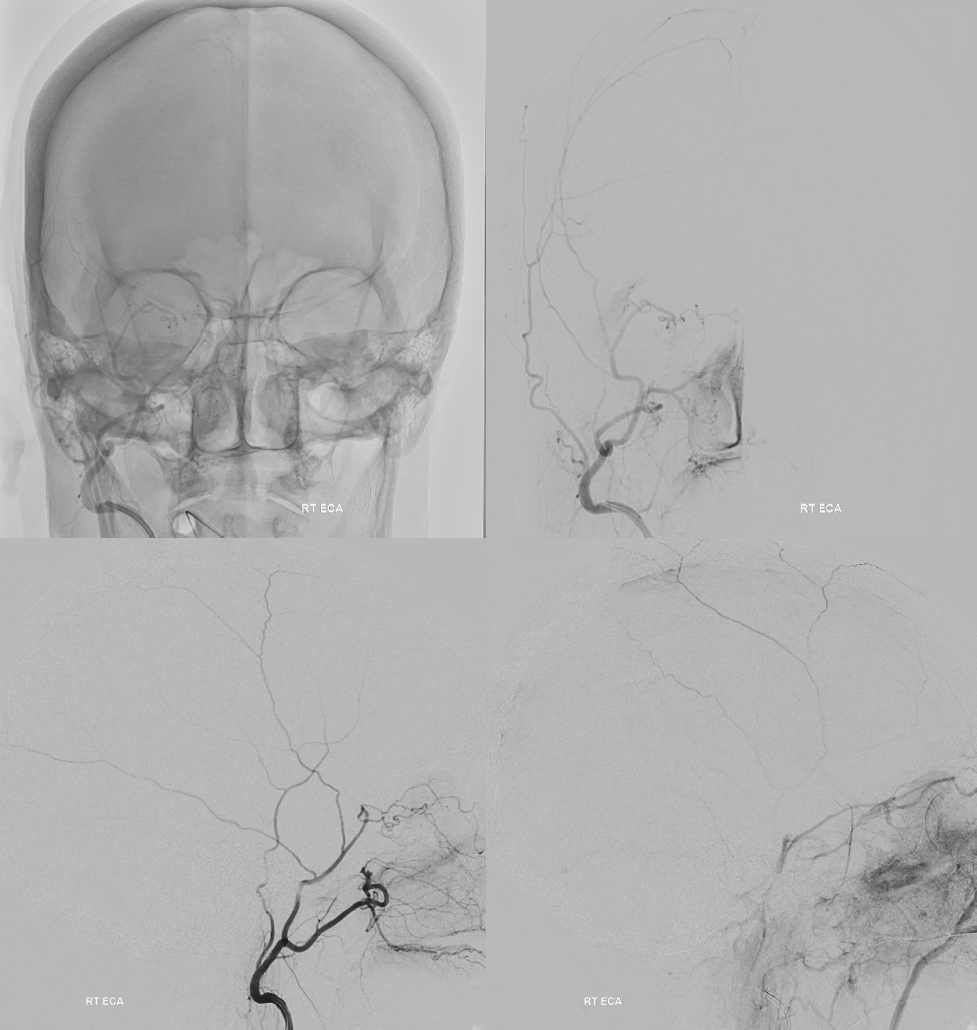
Case of Eytan Raz. Example of strategy for MMA embo with significant orbital supply — go distal in the MMA, ensure lack of reflux (pressure cooker in this case), and go ahead.
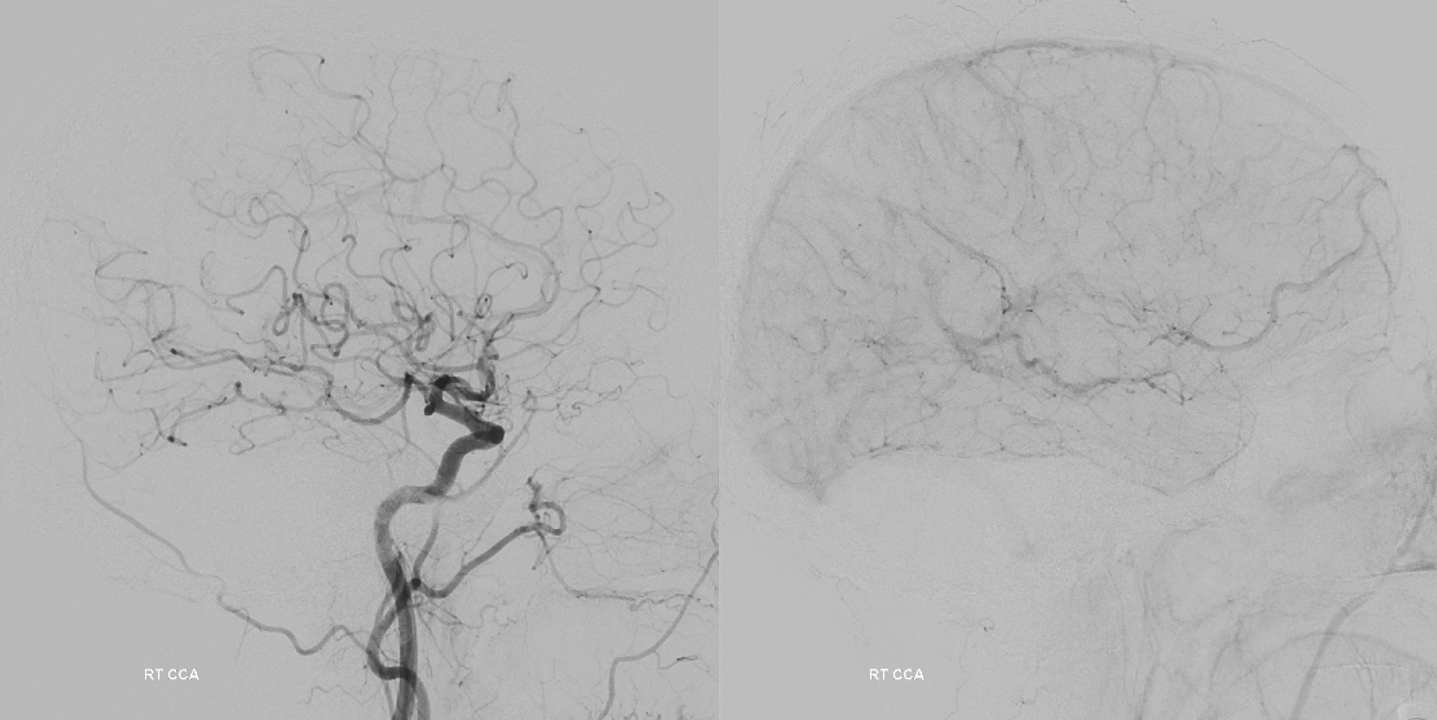
No need to catheterize internal most of the time. External points — anything over the orbit in frontal view is either in the orbit or in back of head (occipital). With this injection distal to occipital origin, what’s projecting over orbit is in orbit. See choroid blush on venous phase lateral view
Pressure cooker is the most secure way to avoid reflux. Balloon microcatheter is fine also. Here we use pressure cooker.
Glue is the best option from this location. Particles will not work well without flow. Onyx is likely to rupture the artery before penetrating distal enough. Long coils are not what we prefer.
Note opacification of the anterior meningeal artery. Very frequent. Good to glue it to prevent reconstitution of subdural membranes without getting too close to the ethmoid area
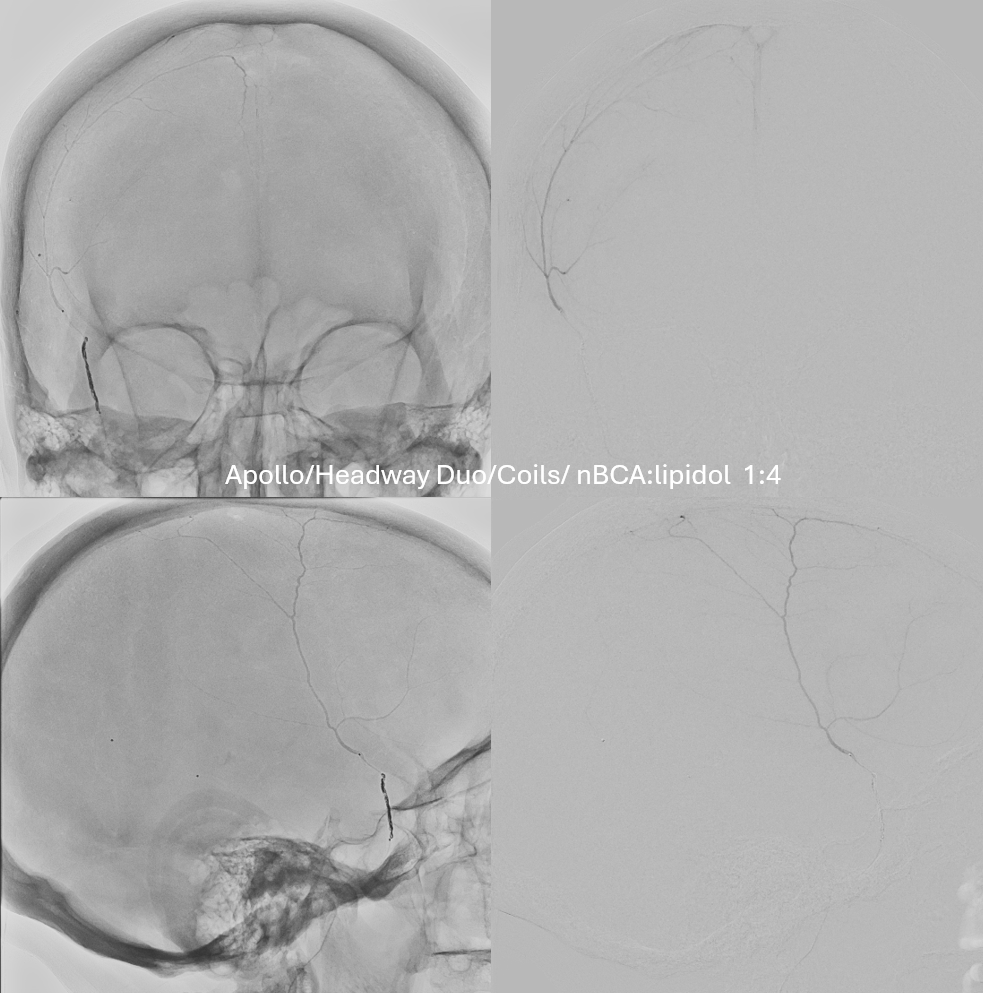
Post. Supply to orbit is preserved. In fact its ok to close the MMA proximally too — the orbit will reconstitute from somewhere else. Problem happens when embolic material gets into the central retinal artery or short ciliary arteries.