
In Collaboration with Dr. Eytan Raz
The concept of pure arterial malformation is relatively new (as of 2019). It may or may not hold up as a distinct entity — however morphologically it really seems like one. It is a descriptive term. Refers to tortuous, often mildly fusiformly dilated, often calcified segmental arterial abnormality, without arteriovenous shunt or frank aneurysm. When aneurysms are present, they are less impressive than the underlying parent vessel abnormality. Presentation frequently incidental. On follow up these are stable. Most often seen in the ACA territorry (see ACA dolichoectasia page). In a curious way, CTA is probably the best modality to see these. Usually I prefer modern 3T MRA for noninvasive brain arterial imaging. However, for these, calcifications can be easy to miss without gradient echo, and MRI sometimes is misinterpreted as an AVM.
Here are some examples
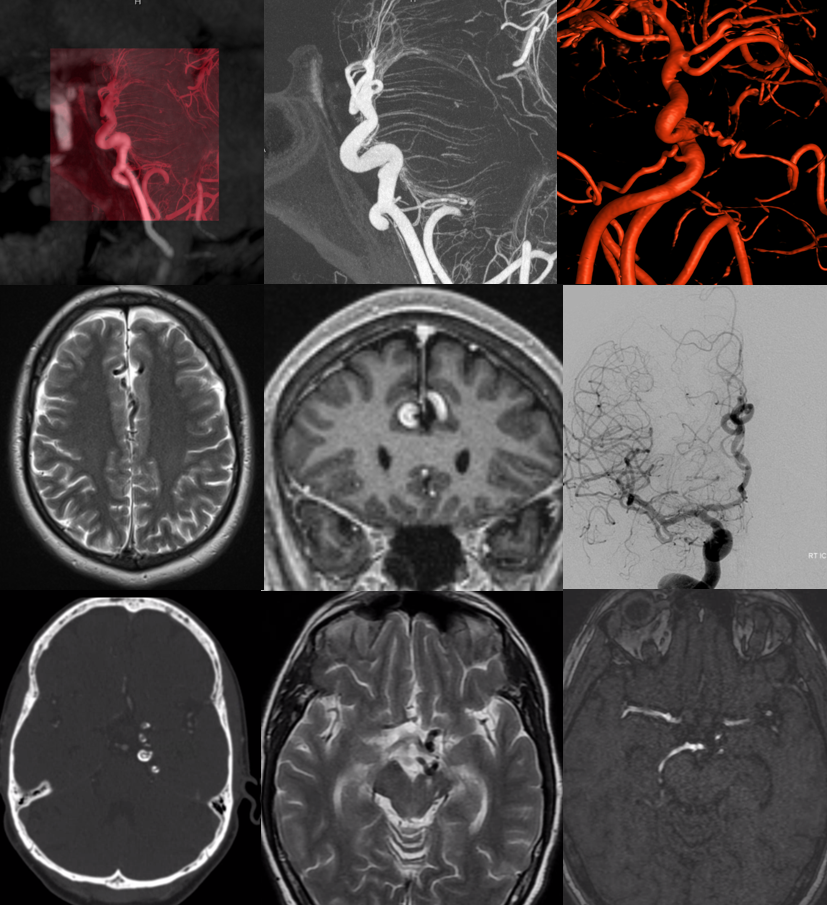
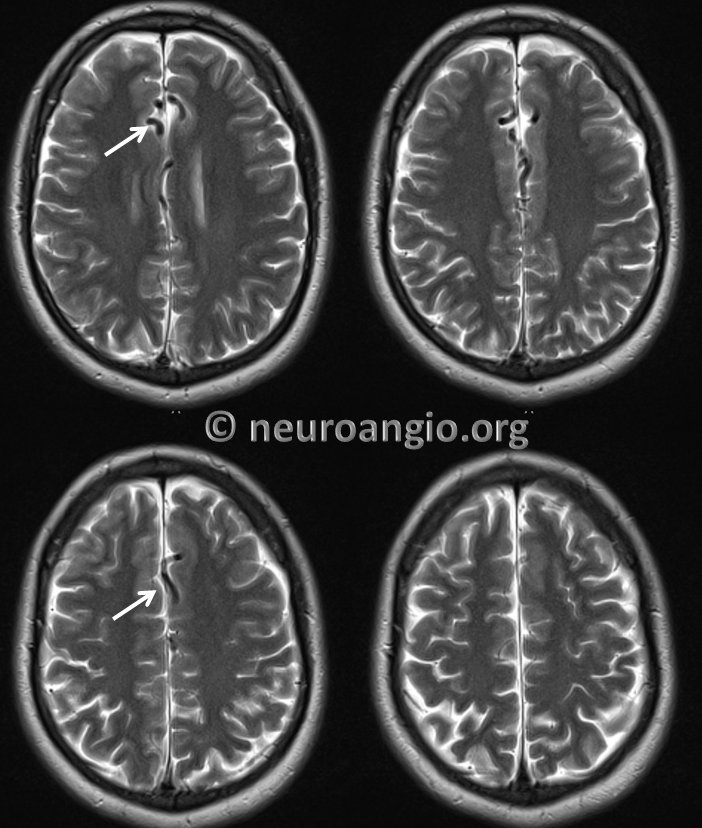
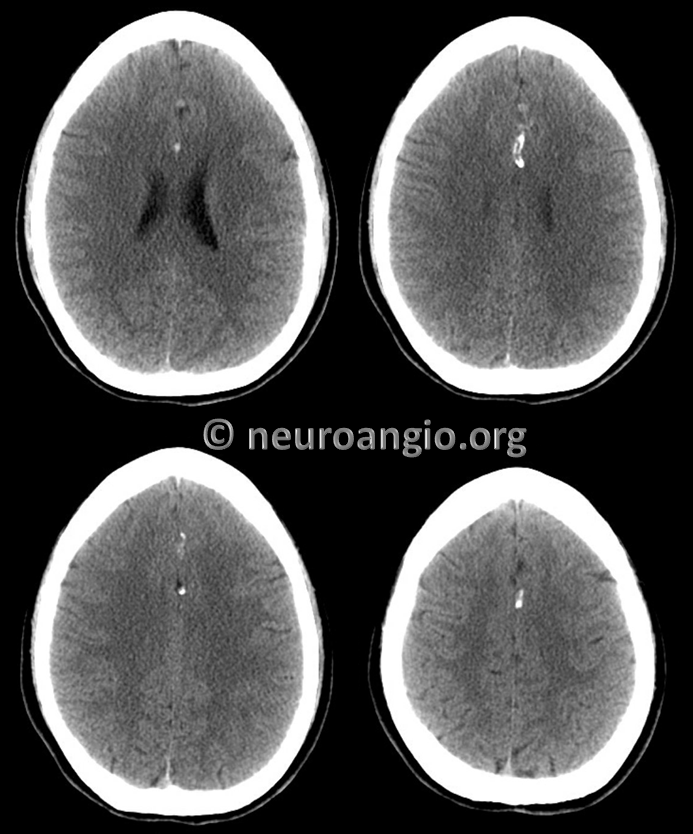
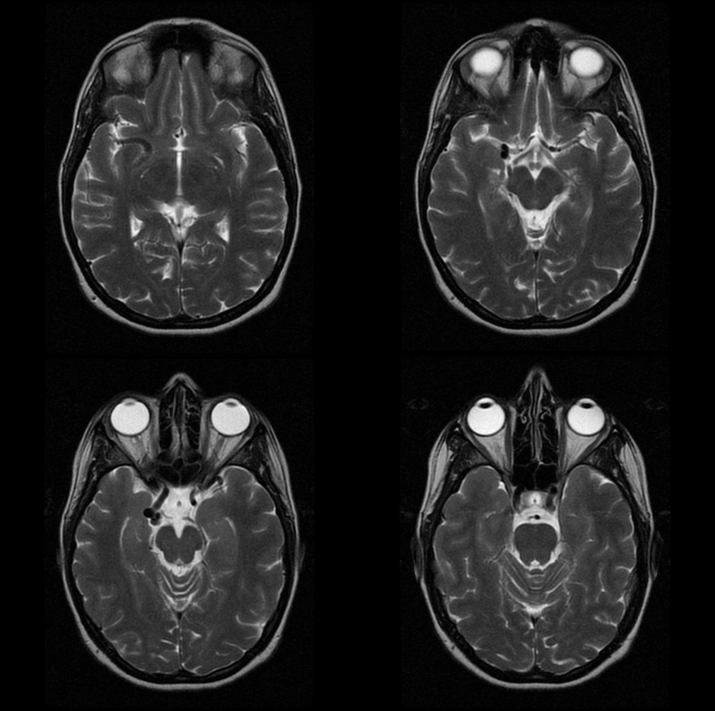
Case 1 — chronic headaches, normal exam. MRI reading was suspected AVM — except there are no dilated veins
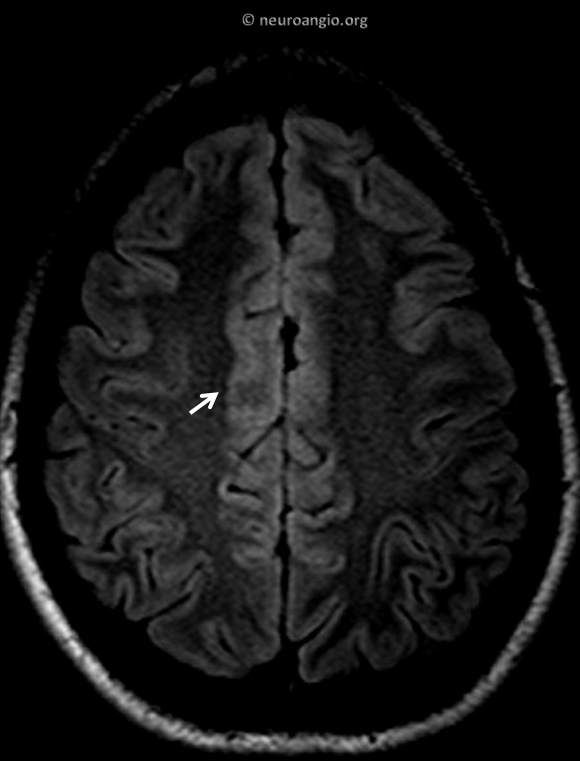
Calcification on susceptibility imaging

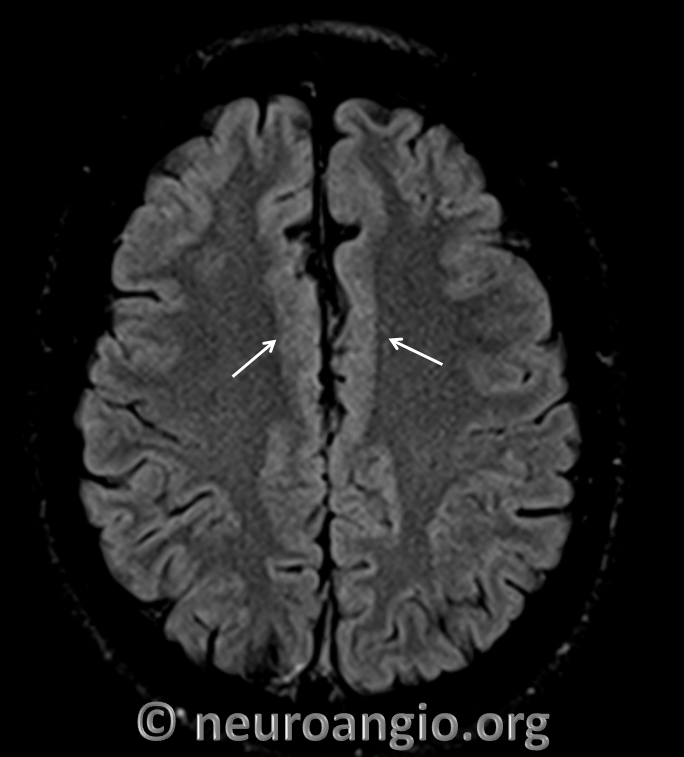
Subtle adjacent cortical dysplasia
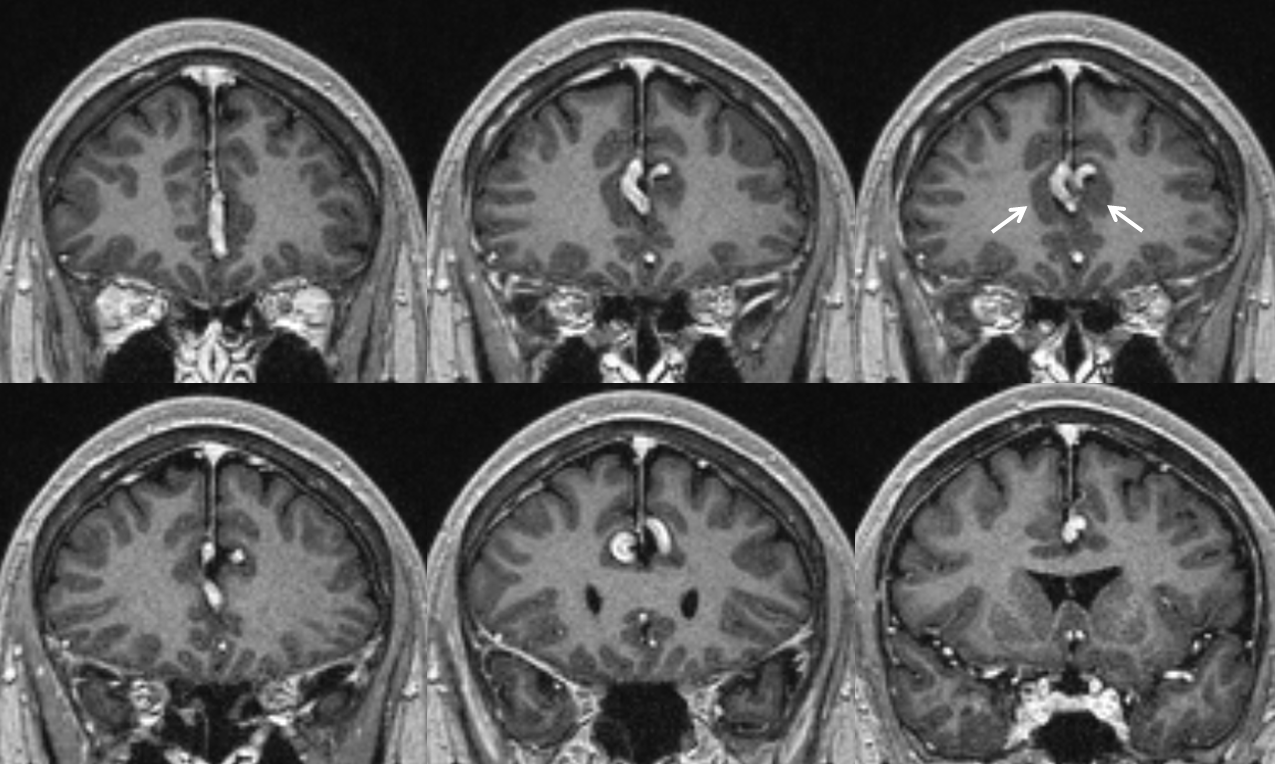
Same on coronal T1 post
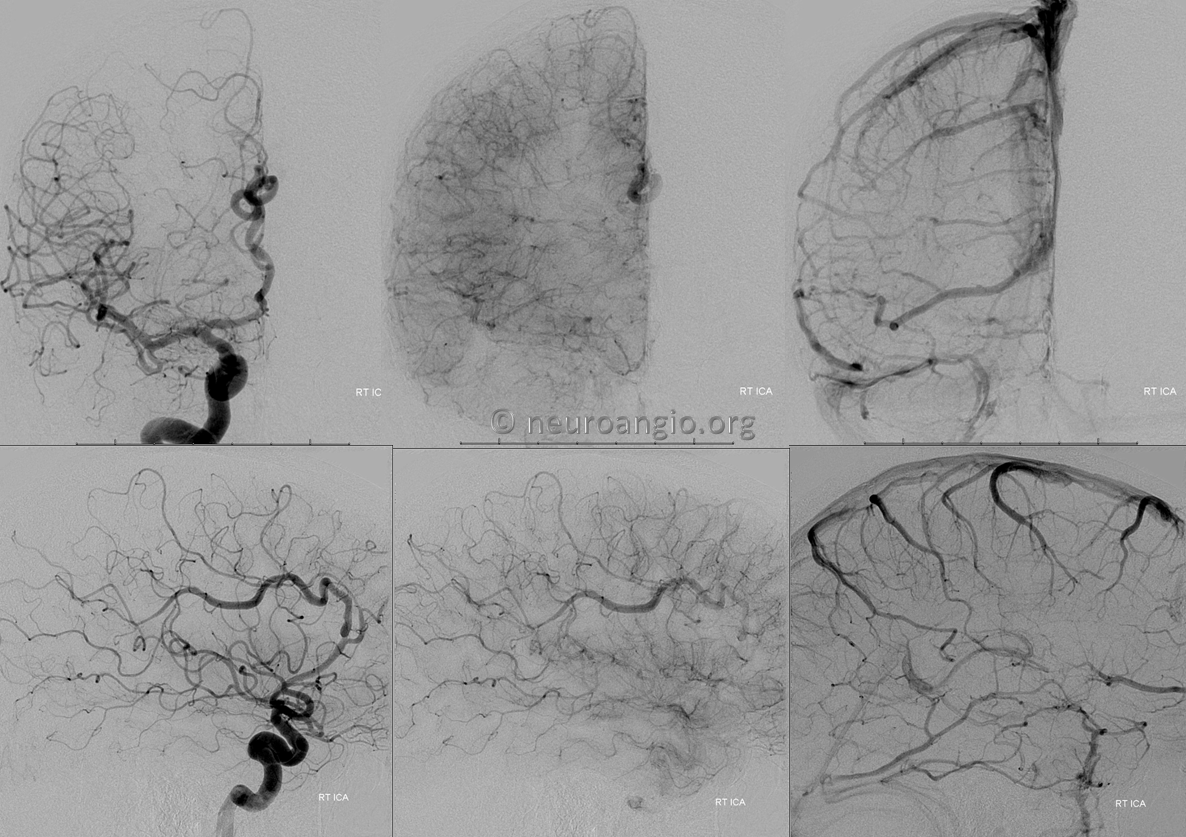
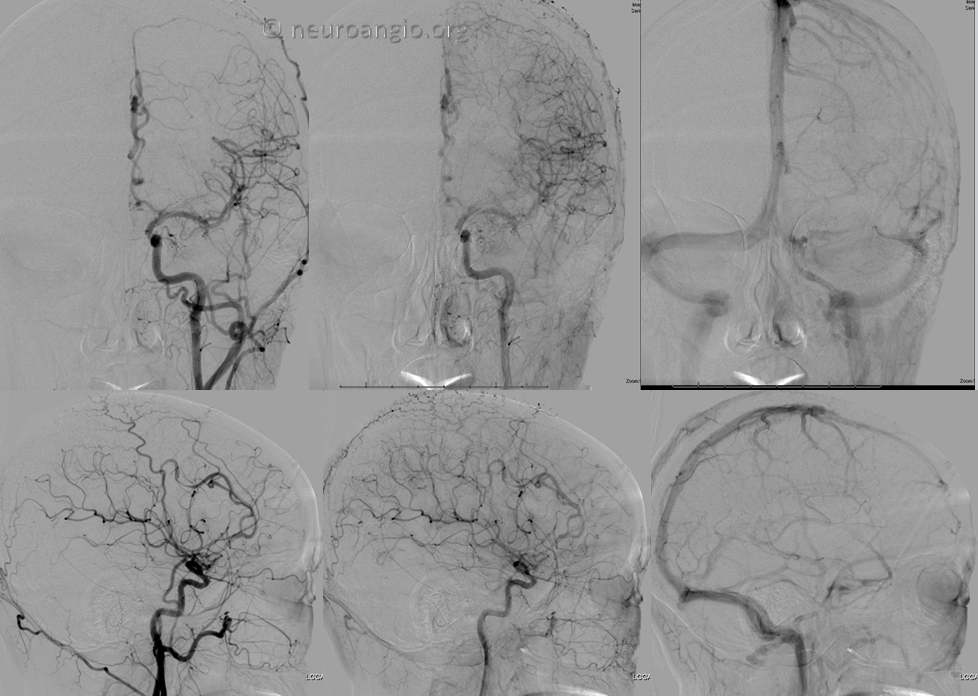
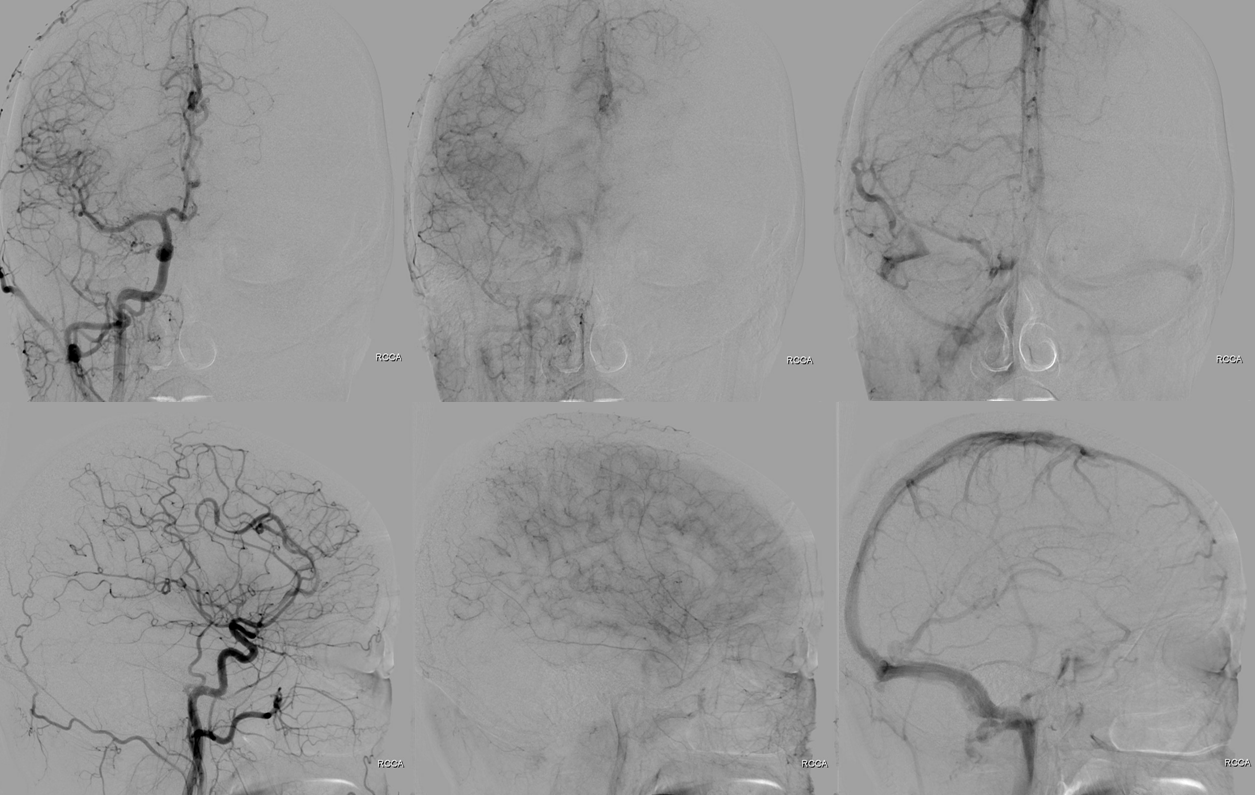
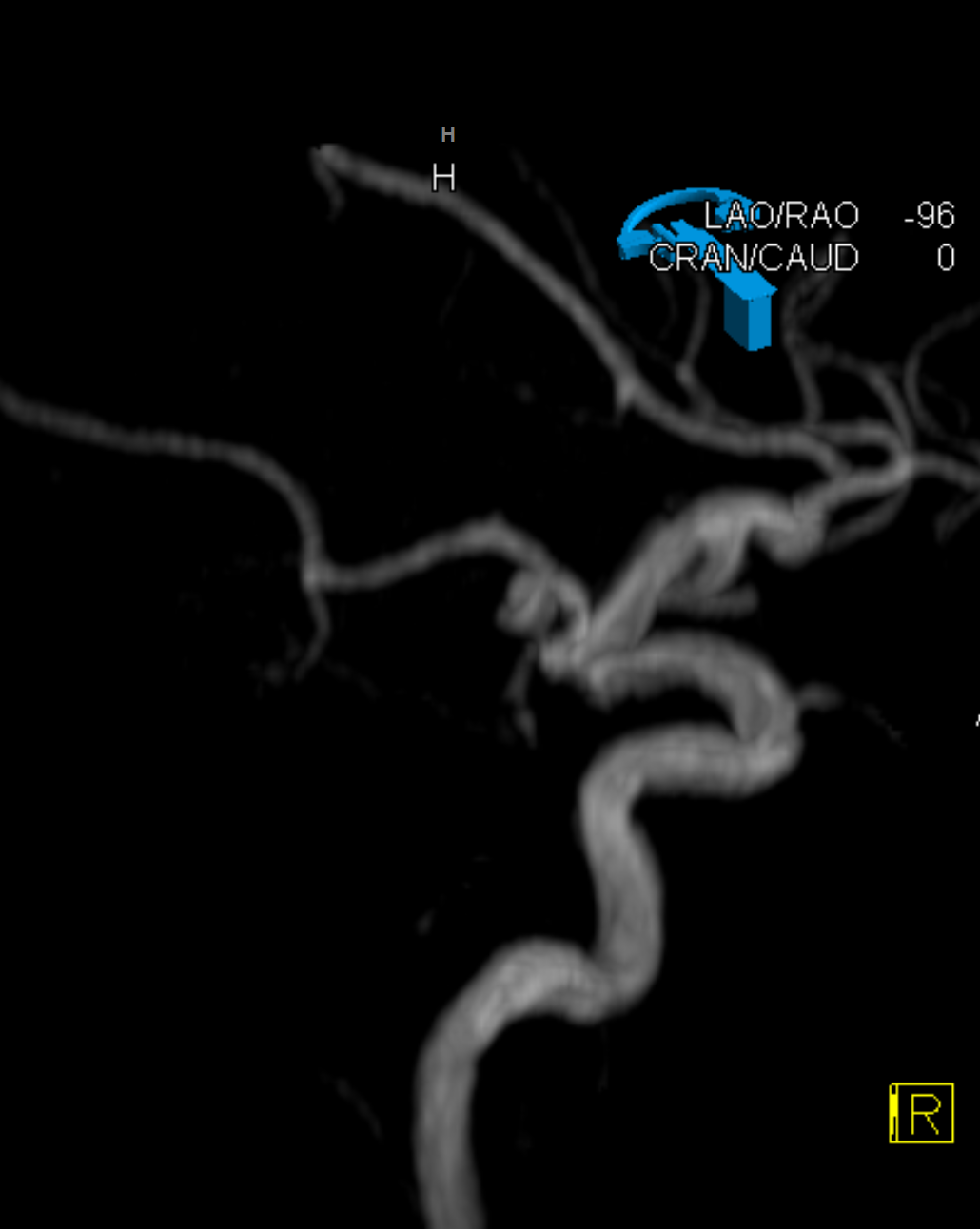
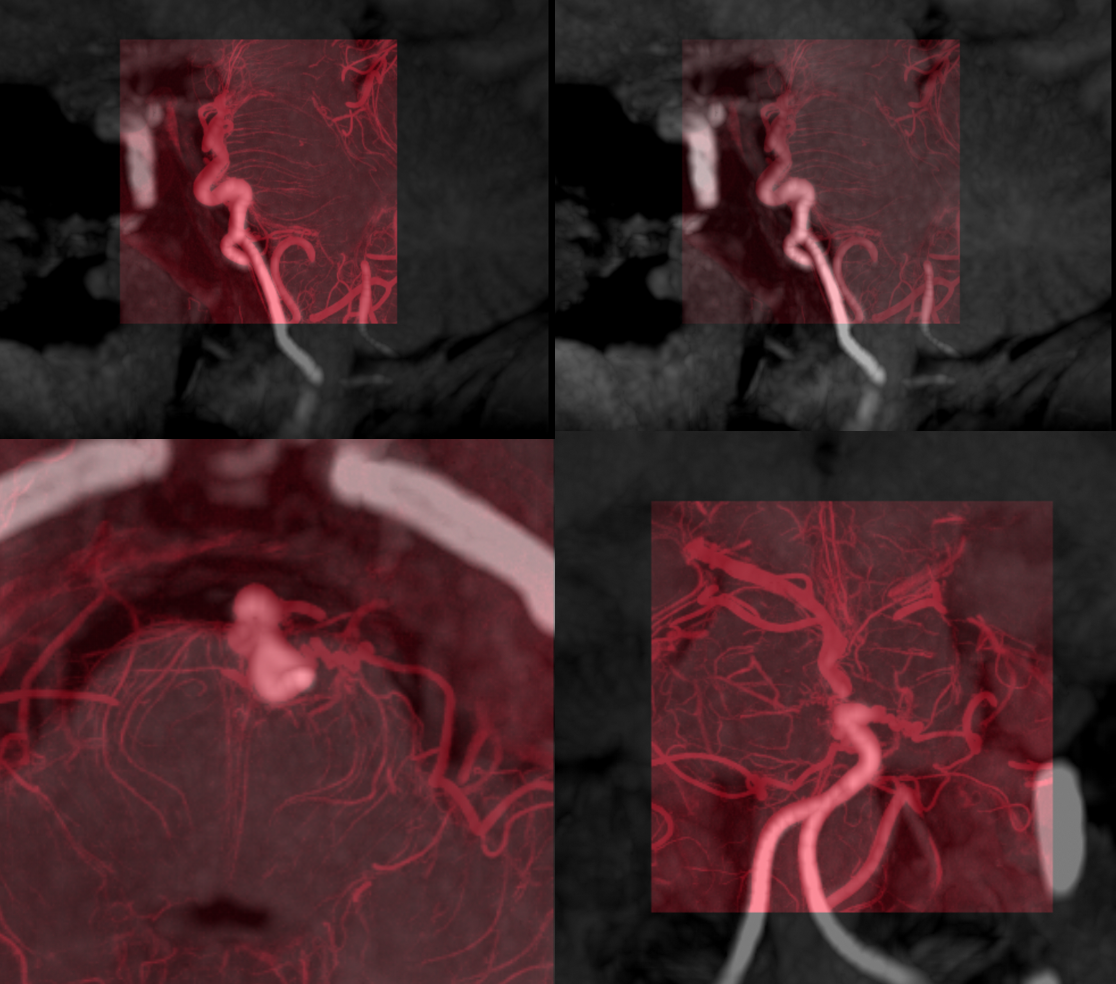
Typical angio appearance — tortuous, fusiform A2/Pericalossal, without arteriovenous shunting
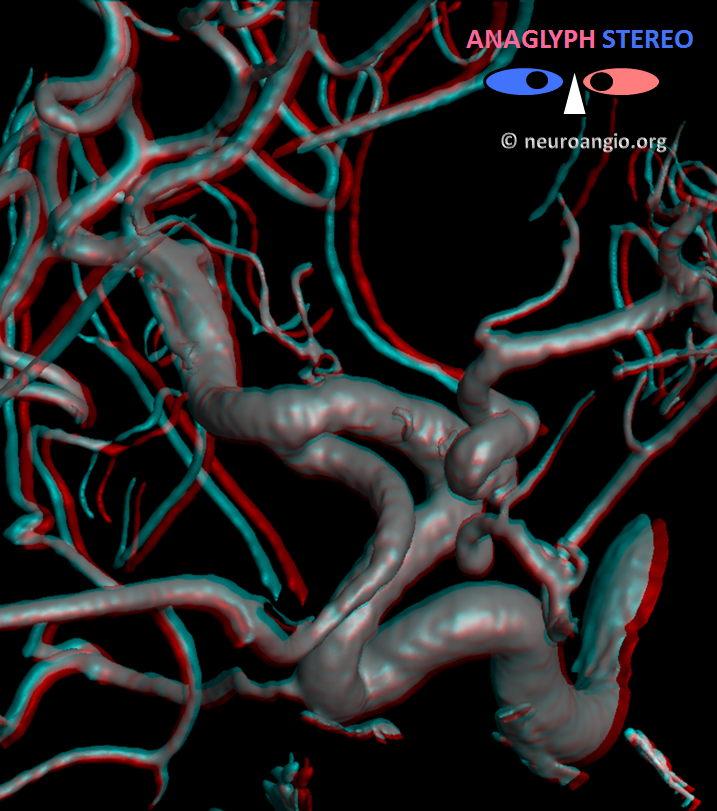
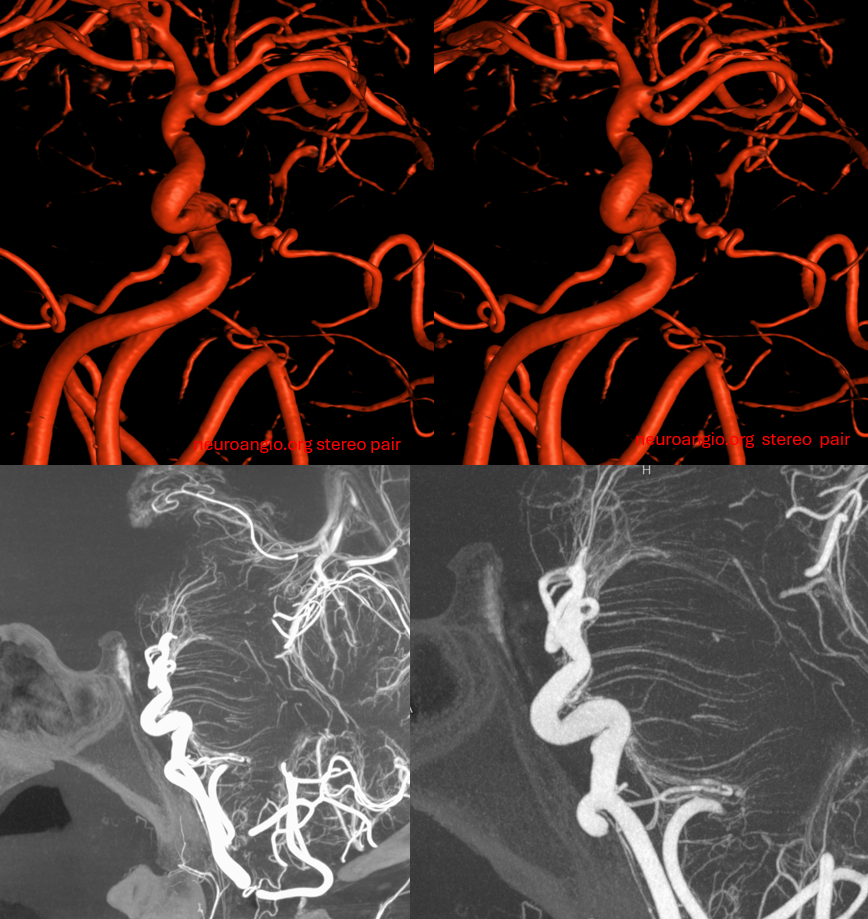
Stereos
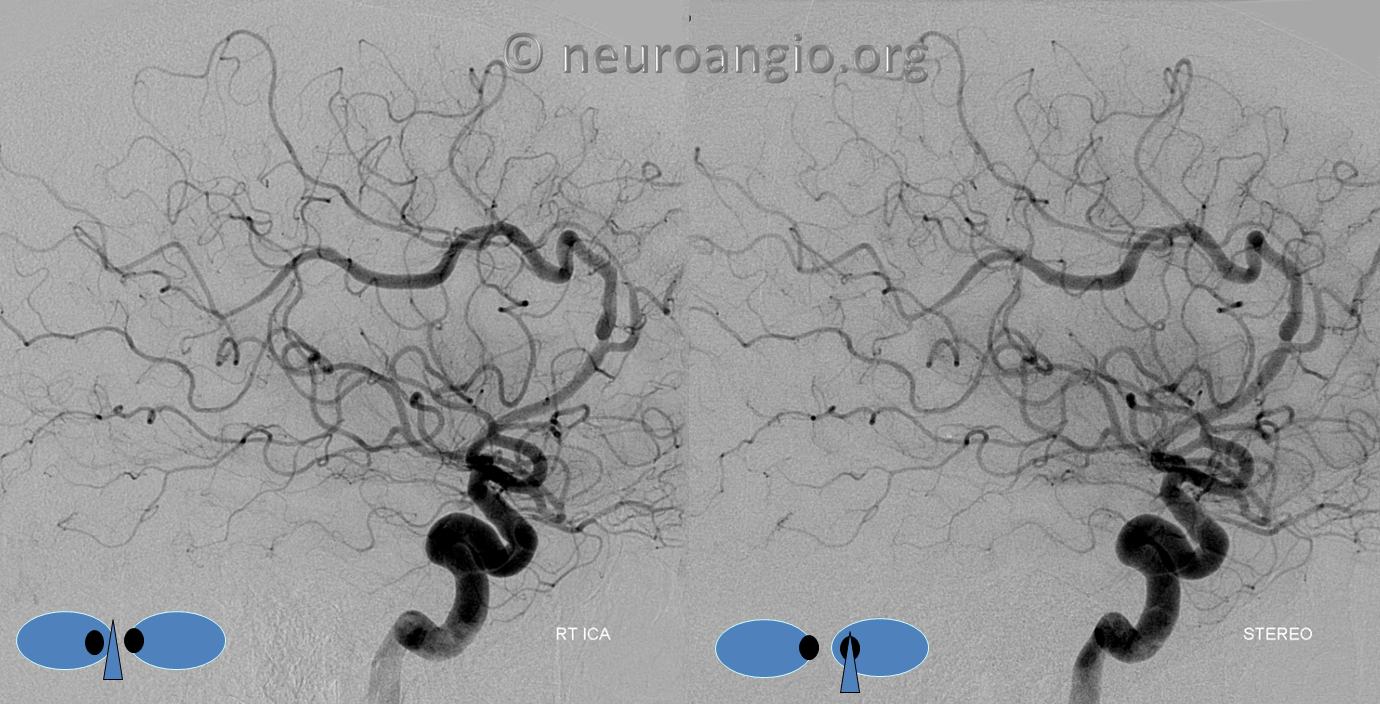
Red/cyan anaglyph stereo

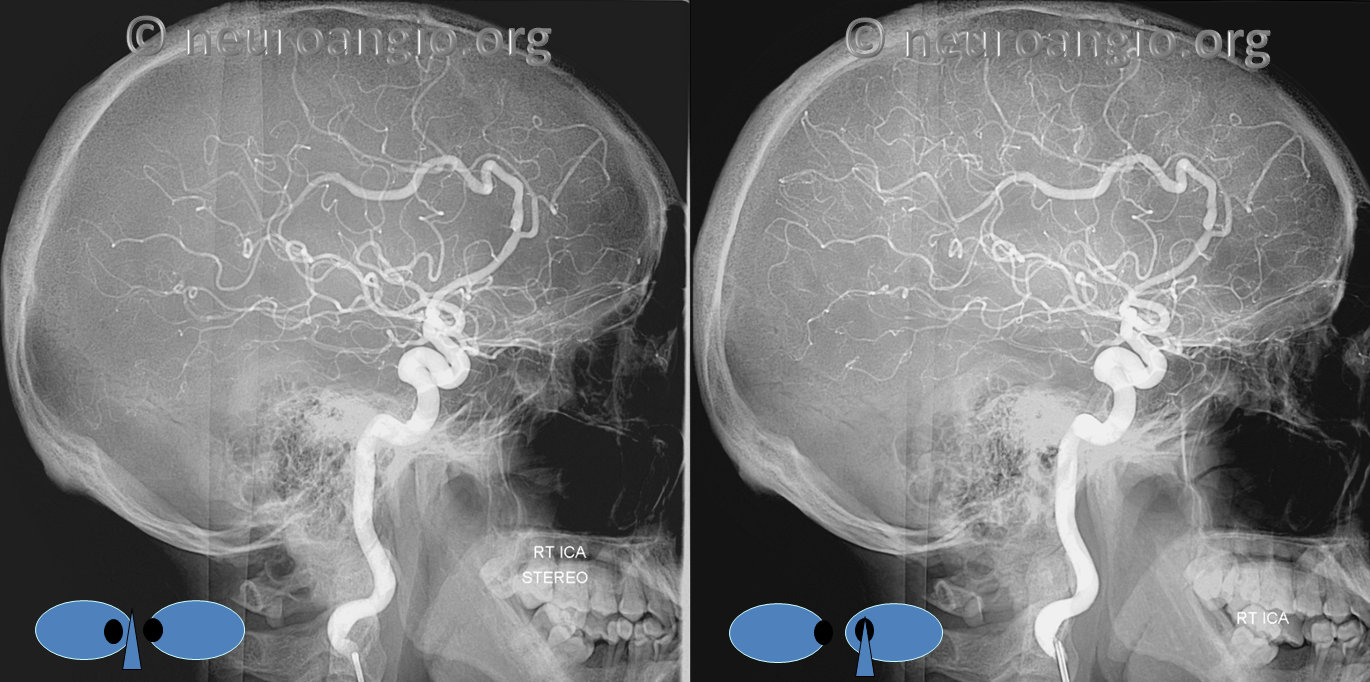
Native stereos, retro style

Usually the finding is bilateral, as it is here (see unilateral Case 4 below)
Case 2 — young woman with syncope. Normal exam. Typical calcification
Less subtle cortical dysplasia
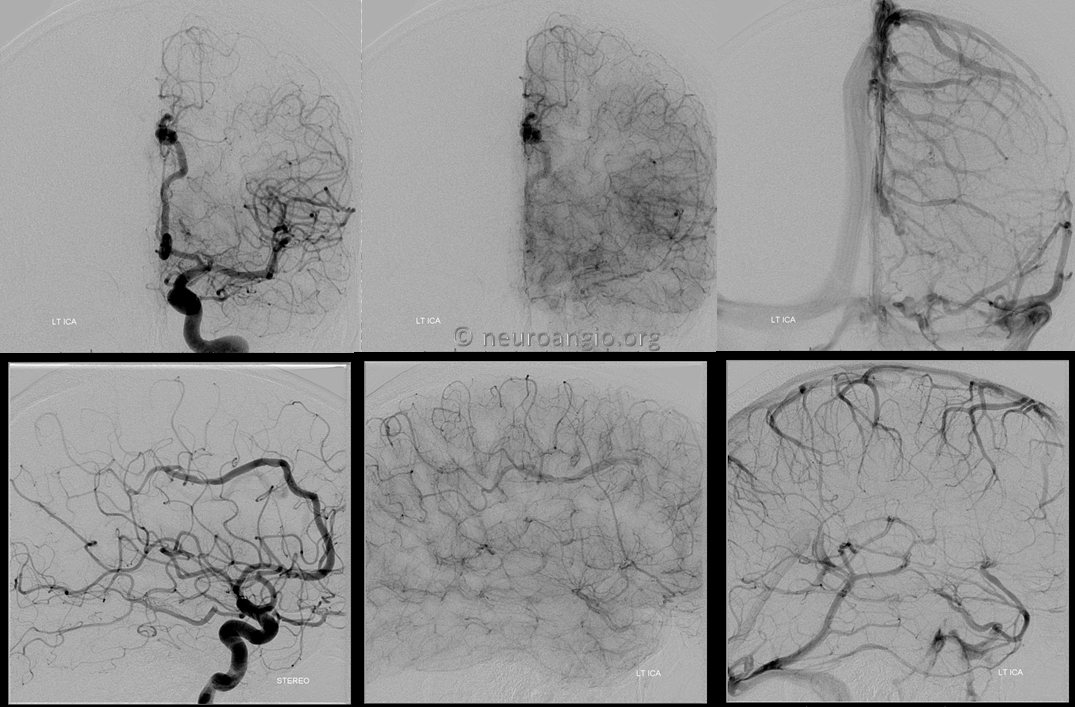
Angio. Less obvious but real ACA findings
Right side
Case 3
Here is an ICA/PCOM/PCA example. Very rare. May attest to embryoic origin of the PCA as an anterior circulation vessel aka “Caudal Ramus” (see embryology section)
CTA is probably the best modality for these – not how i usually feel, with modern MRA being first choice for most anything. However it is very easy to miss the bulk of finding on MRA, whereas CT shows calcifications and dolichoectasia very nicely.
Here is a CTA of an asymptomatic patient. Notice tram-track calcifications and tortuosity in distal ICA/PCOM/PCA
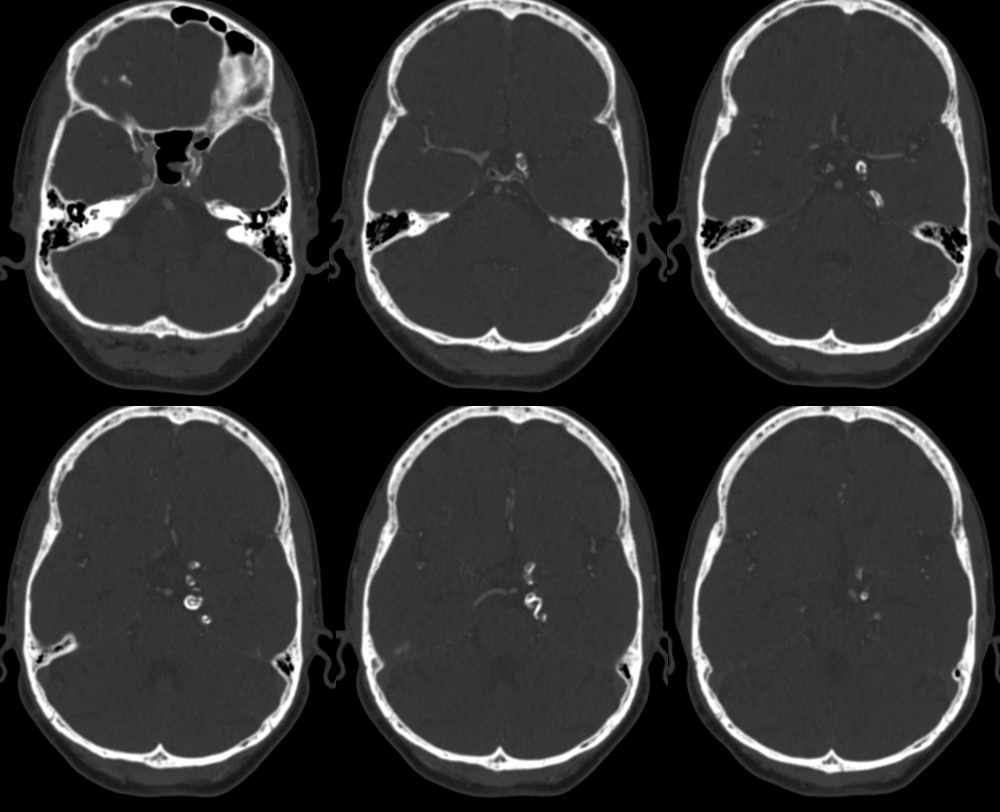
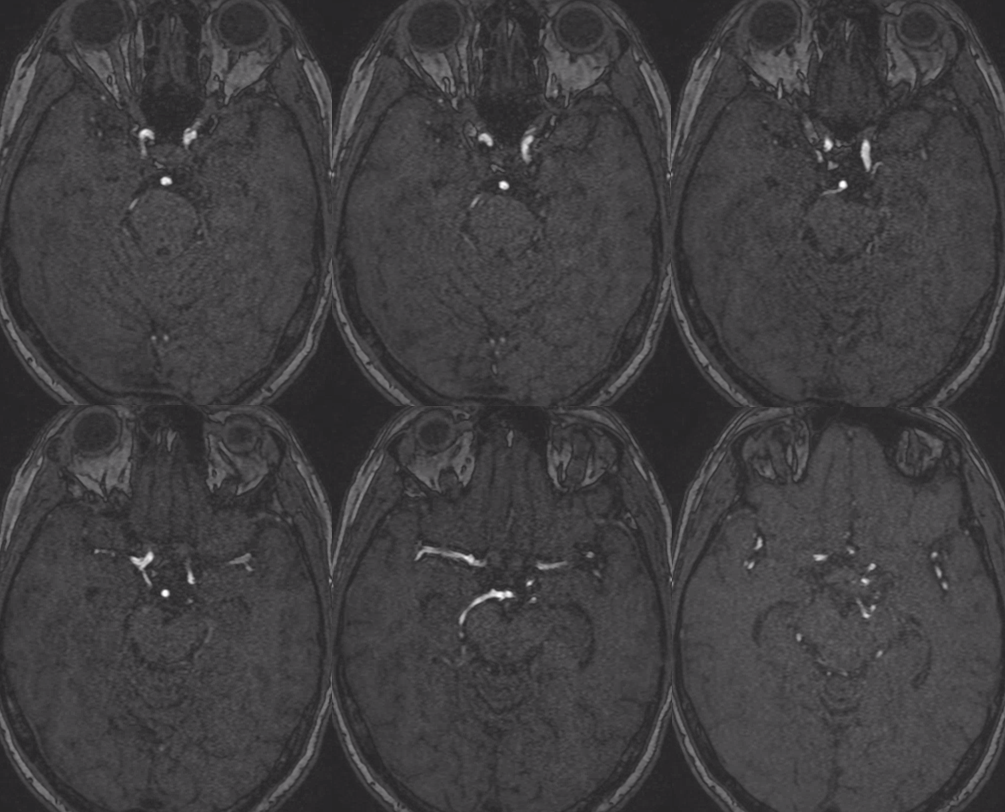
MRA is rather bland. If anything would suspect occlusive /stenotic disease here
Typical enlarged vessel caliber on T2. Sometimes the bulk of enlargement is a thick, calcified wall, as in this case. Sometimes the lumen is also dilated. Gradient echo sequences are very useful here for picking up calcs
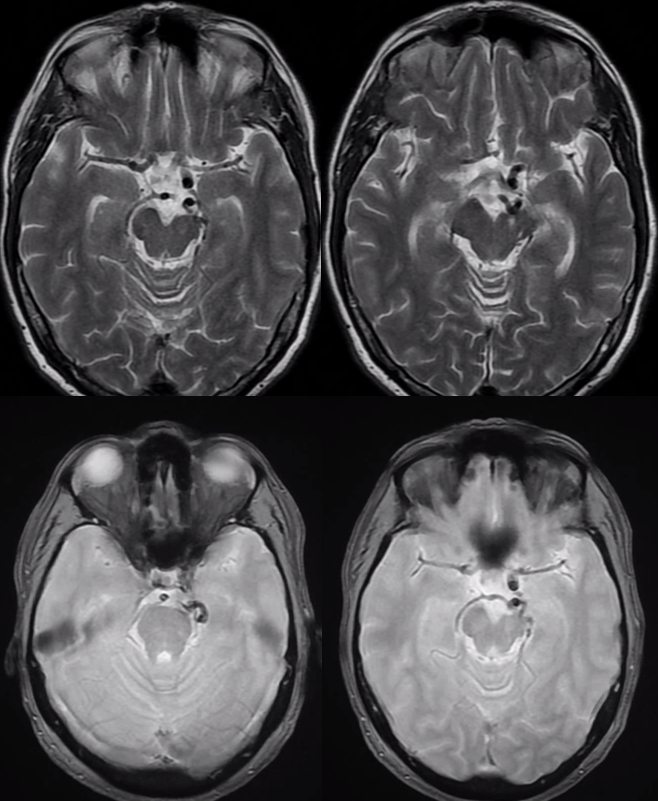
You can see how CTA is probably the single best modality here. MRA could miss this. MRI gives rise to suspicion of AVM or fistula, especially when quality of imaging is inferior
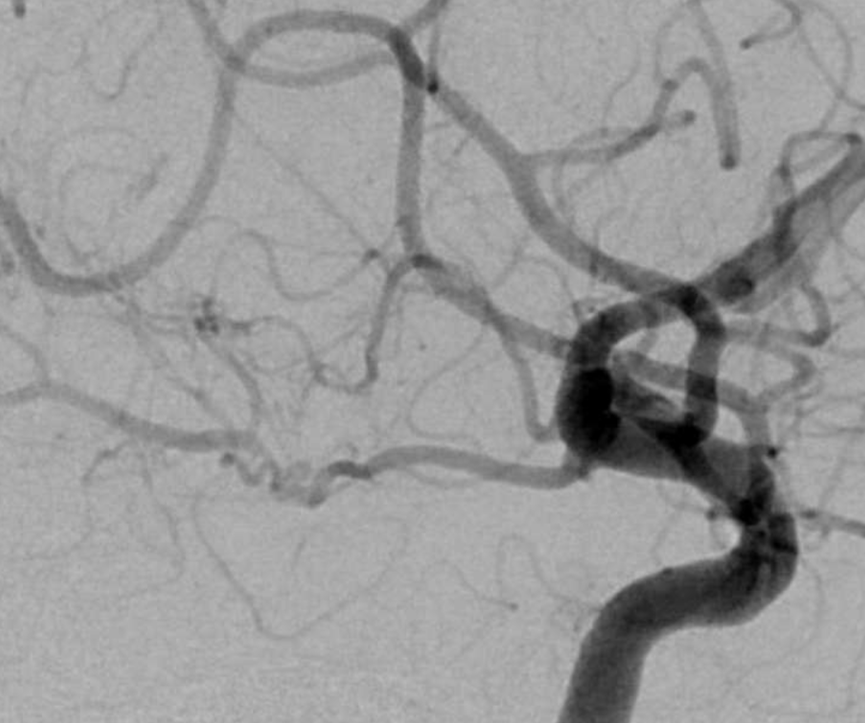
Here is an angio of a different patient with what looks like a PCA malformation
Here is one of the Middle Cerebral Artery

BASILAR ARTERY — PURE MALFORMATION? CORKSCREW ANGIOPATHY OF THE BASILAR ARTERY.
Although this is reportedly extremely rare, I have seen 3 in a 15 year period — which is not exactly vanishingly so. The appearance is extremely typical — midbasilar tortuosity with focal indentation upon typically the pons and generally brainstem. Among the small number there has never to my knowledge been an instance of rupture or enlargement in caliber that would merit the diagnosis of “aneurysm” with which this entity may be easily confused. In my opinion this is not an aneurysm. We follow them with MRA and so far so good. It is hard to imagine an acquired /postnatal etiology given normal appearance of brainstem in my cases and the asymptomatic nature. The theory of mid-basilar agenesis / meeting of caudal ramus and longitudinal neural systems is nice but unprovable. Bottom line is that the natural history has so far been benign in known cases. So there.
Below is a typical example:

Involving AICAs
MRI-Angio fusion
Movies
Literature:
http://www.ajnr.org/content/16/7/1548
https://www.ncbi.nlm.nih.gov/pubmed/28960150