
Great spinal case, even if there is no angio…
Case courtesy Dr. Kaitlyn Lillemoe, Dr. Zhang, and Dr. Rostanski, among our larger group of super vascular neurologists at Bellevue HHC/NYULMC
Multiple vascular risk factors, chronic right carotid occlusion, CAHD — presenting with acute bilateral lower extremity weakness. Near-complete recovery after IV t-PA.
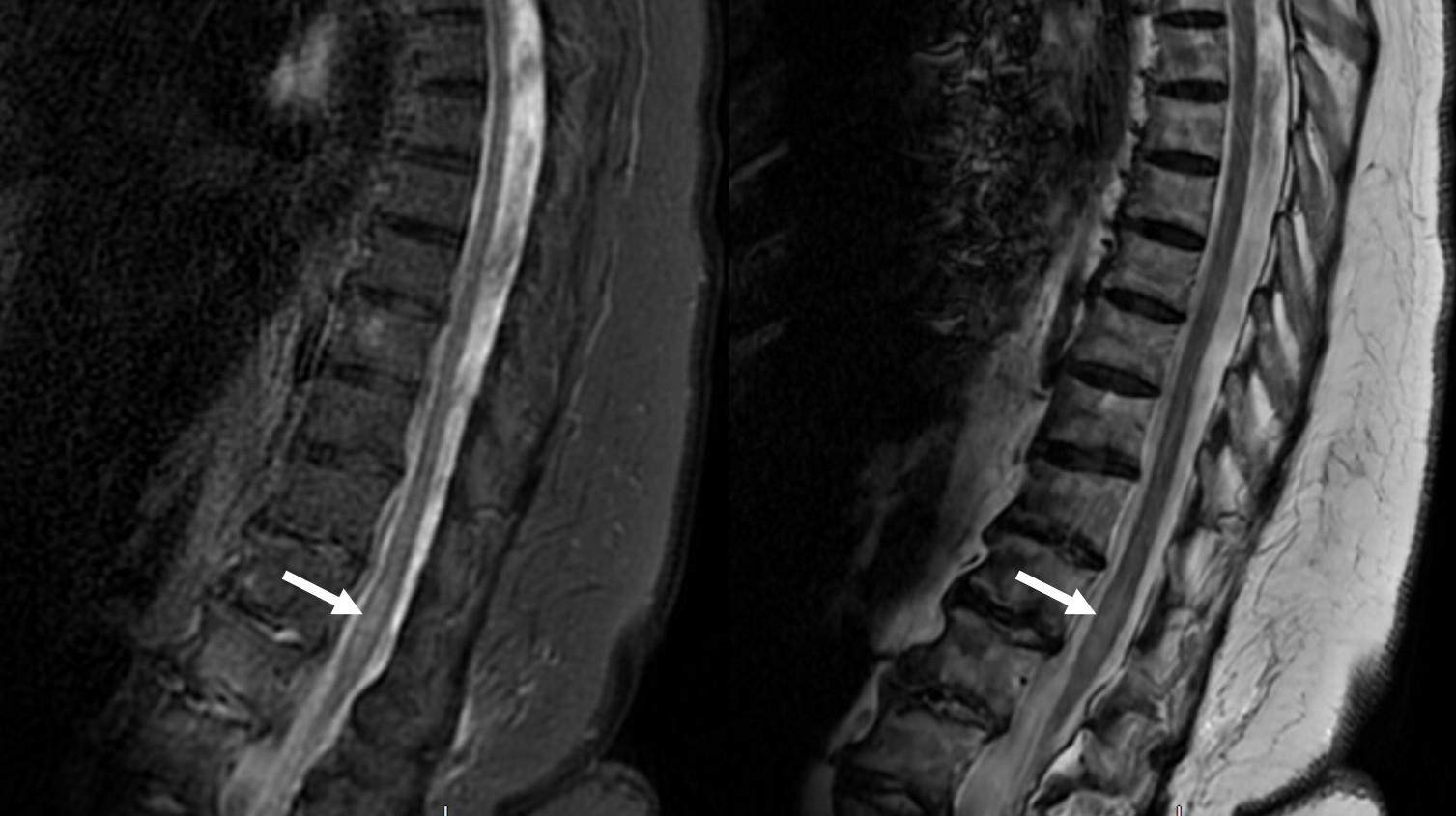
Day 1 MRI is normal
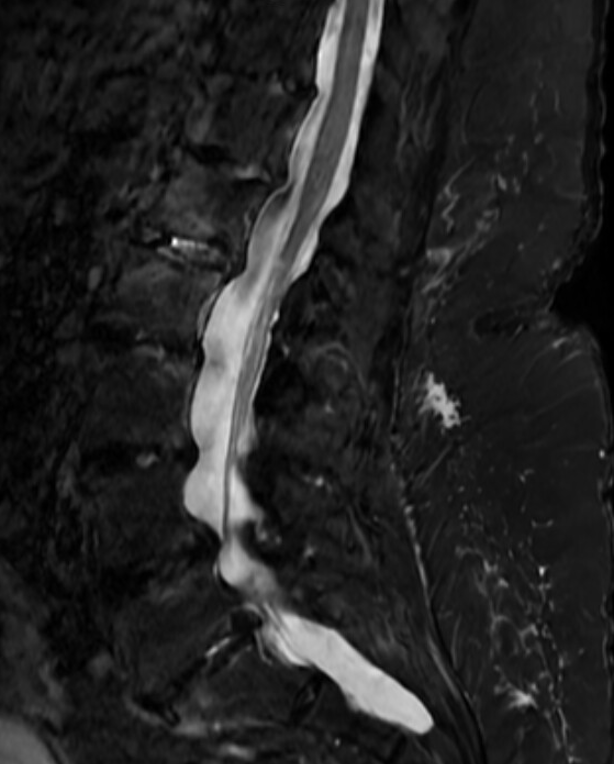
Day 3 MRI shows evolving limited conus T2 signal, consistent with infarct
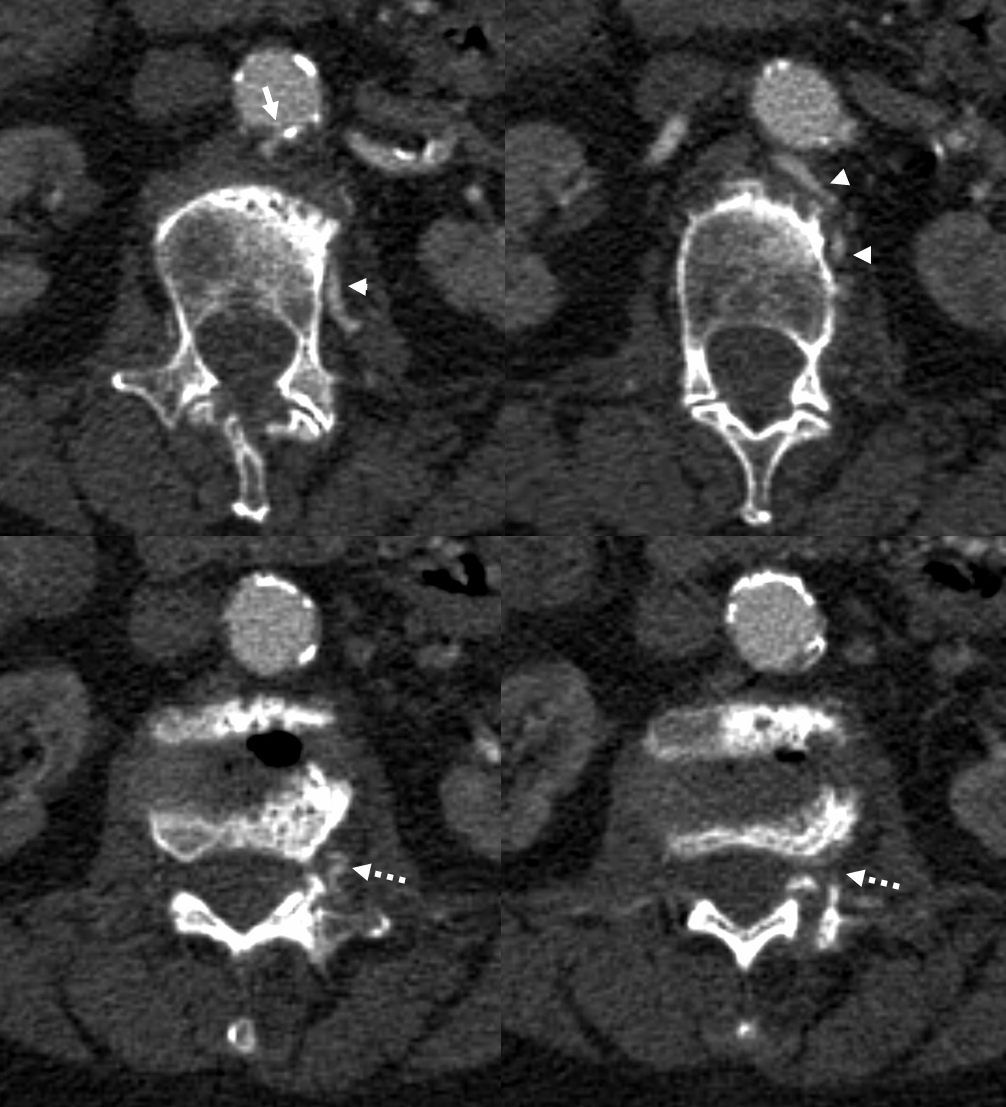
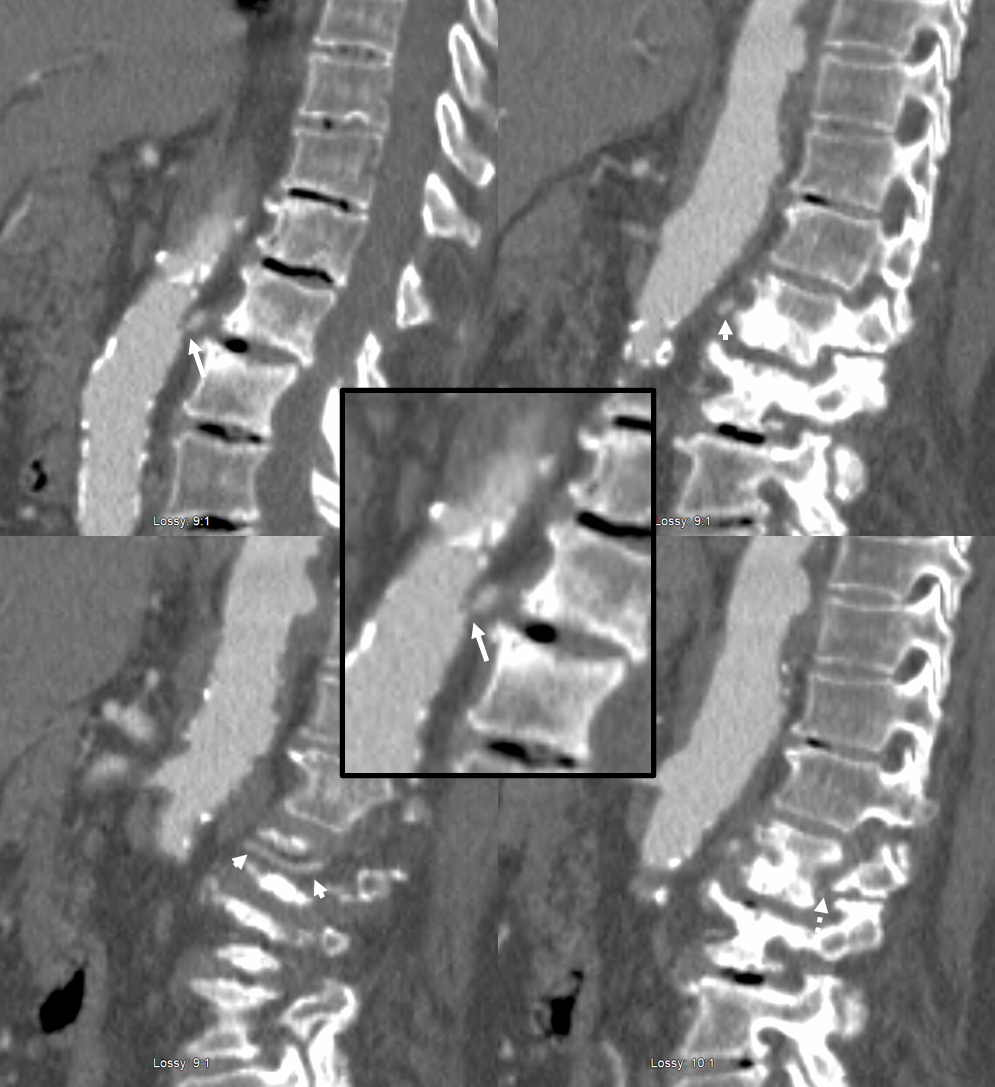
CTA — this is the great part of this case — how often can one make a diagnosis of spinal stroke etiology on CTA? Usually the size of segmental artery has nothing to do with where the Adamkiewicz comes from. Here, though, things are different. There is extensive athero. Many segmentals are occluded. The patent ones tend to be larger, as they also serve the territory of occluded ones. There is a big left L2 one here (arrowheads), with stenosis at the ostium (arrow), and faintly seen radiculomedullary (Adamkiewicz) segment (dashed arrows)
Best seen on sagittal images
The treatment by Dr. Lillemoe is similar to extensive athero anywhere — maximal medical management — dual antiplatelets in acute phase, aggressive cholesterol targets, etc.
This is super detective work. One might even argue that an angiogram would be less likely to catch this ostium stenosis, since whatever catheter is used to do the angio would sit in the ostium of the vessel and obscure stenosis visualization — and any catheter can be occlusive for a few reasons.