
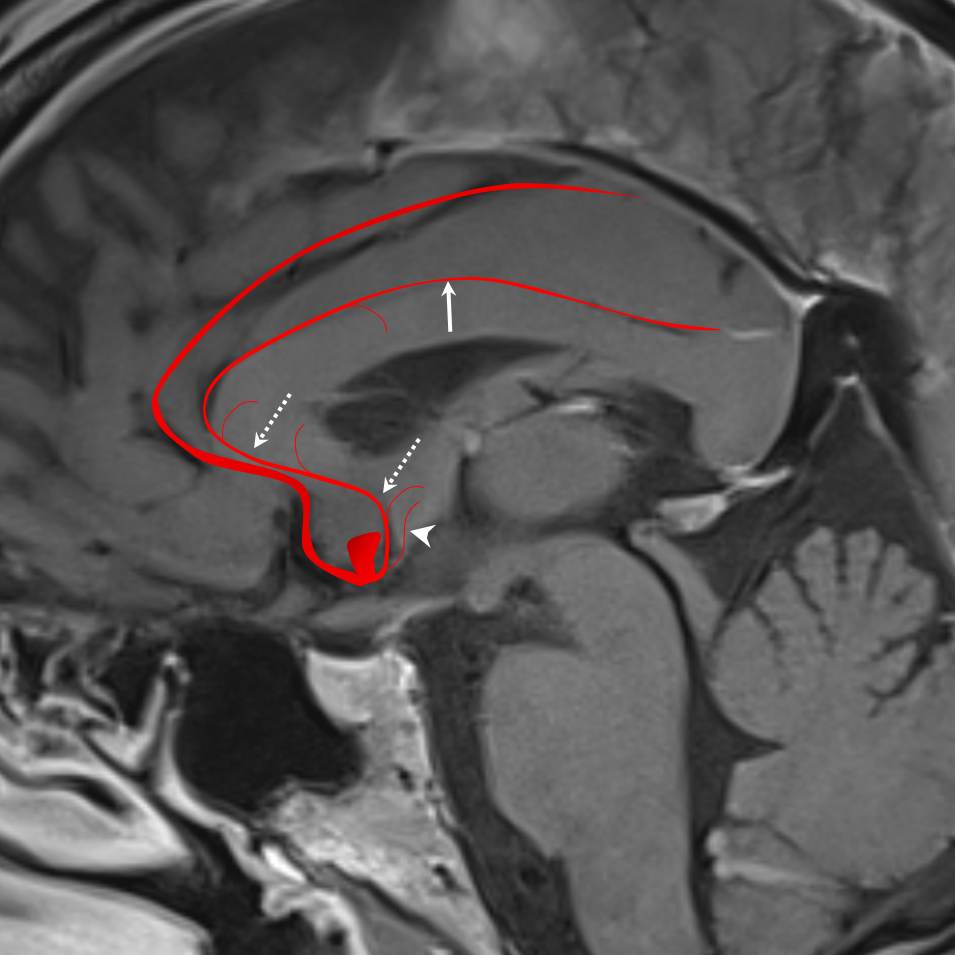

What its really about is when someone wakes up after anterior communicating artery aneurysm clipping (or less often coiling) and can’t form new memories (anterograde amnesia), plus/minus visual and behavioral issues. The problem is iatrogenic occlusion of the subcallosal artery with subsequent infarct of the fornix (part of Papez memory circuit) plus/minus hypothalamus and optic chiasm region.
The subcallosal artery is part of the pericallosal / callosomarginal family on one hand and of a perforator / lenticulostriate system on the other. Probably the best way to think about it is as a medial-most /midline perforator, (more medial than Heubner for example). It typically arises from the ACOM area. It is not always present — the same hypothalamic / fornix perforators can arise singly or separately from the proximal A2. When the subcallosal artery is particularly large, it assumes control of the body of corpus callosum — the so-called median callosal artery.
The main problem again is when this vessel is occluded, usually iatrogenically (see cases where this is recognized and avoided below)
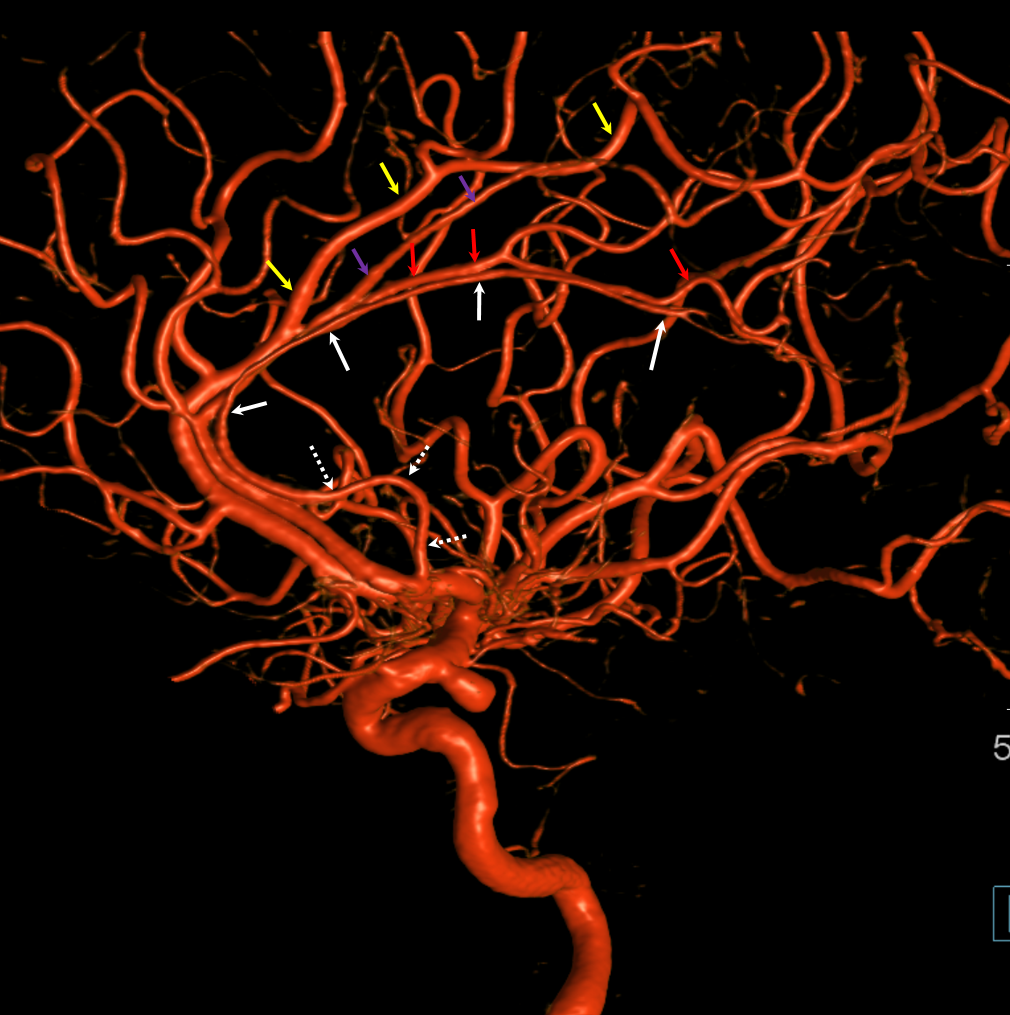
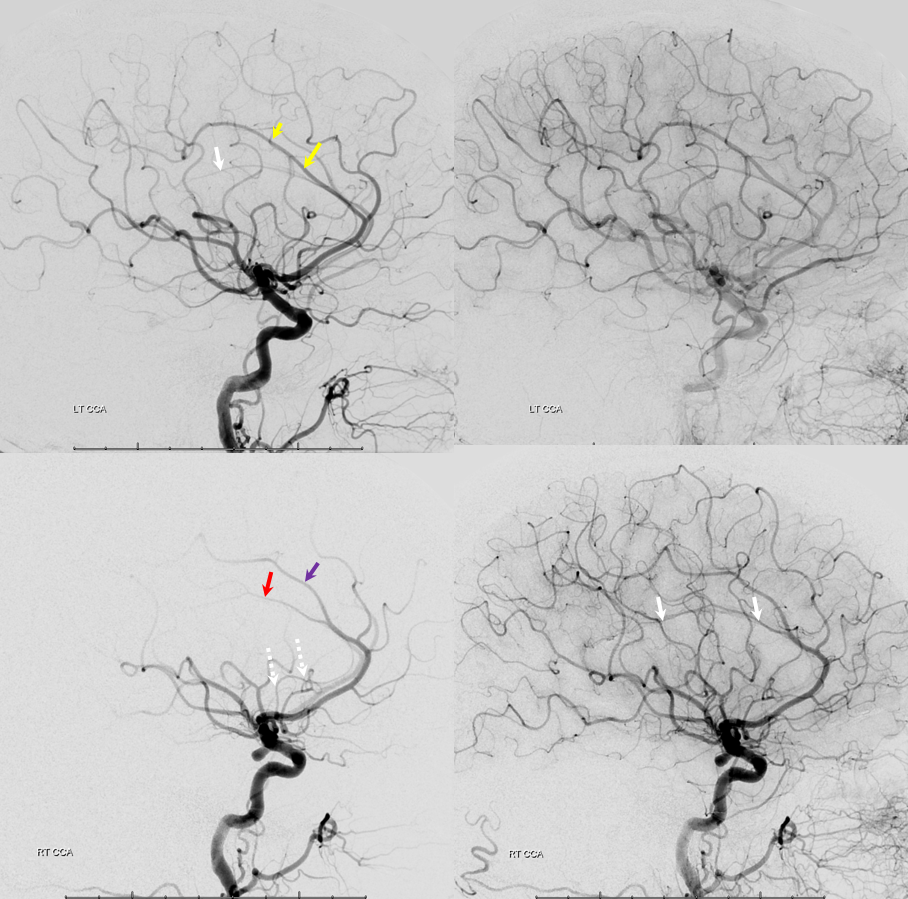
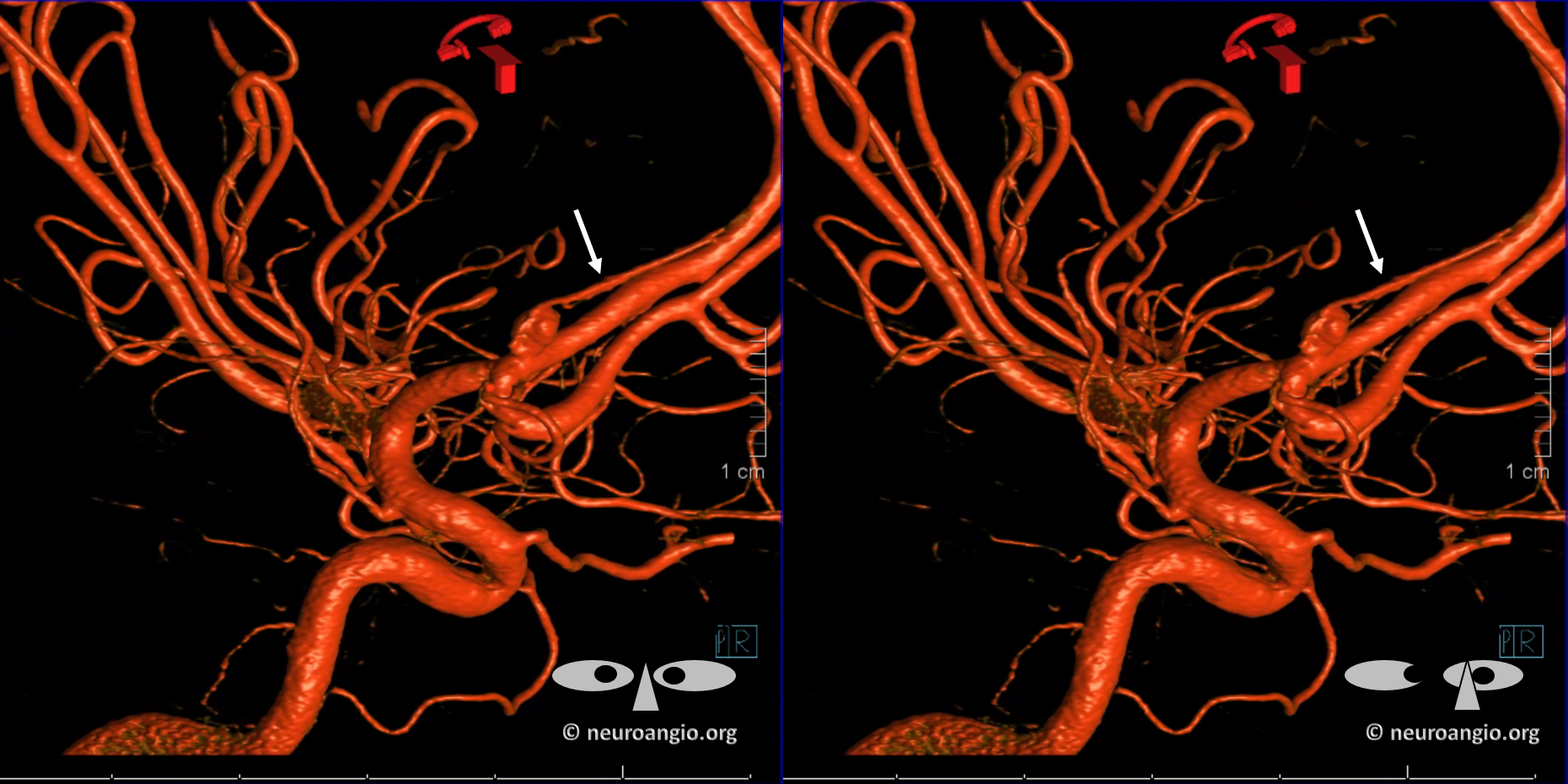
Picture below shows this “subcallosal-median callosal artery. The more proximal subcallosal is dashed white arrows, distal “median callosal” is solid white. On the left, there is a more dominant callosomarginal system (yellow arrows) whereas on right there is a more balanced pericallosal (red) and callosomarginal (purple) trunks.

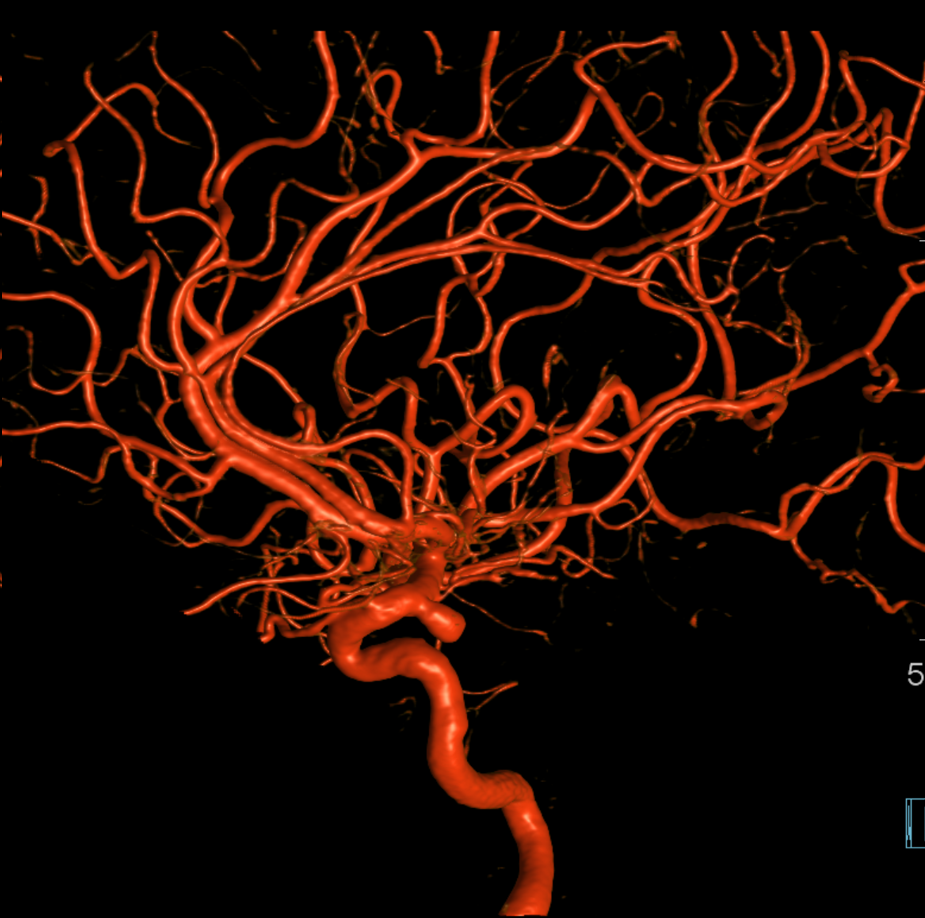
without labels
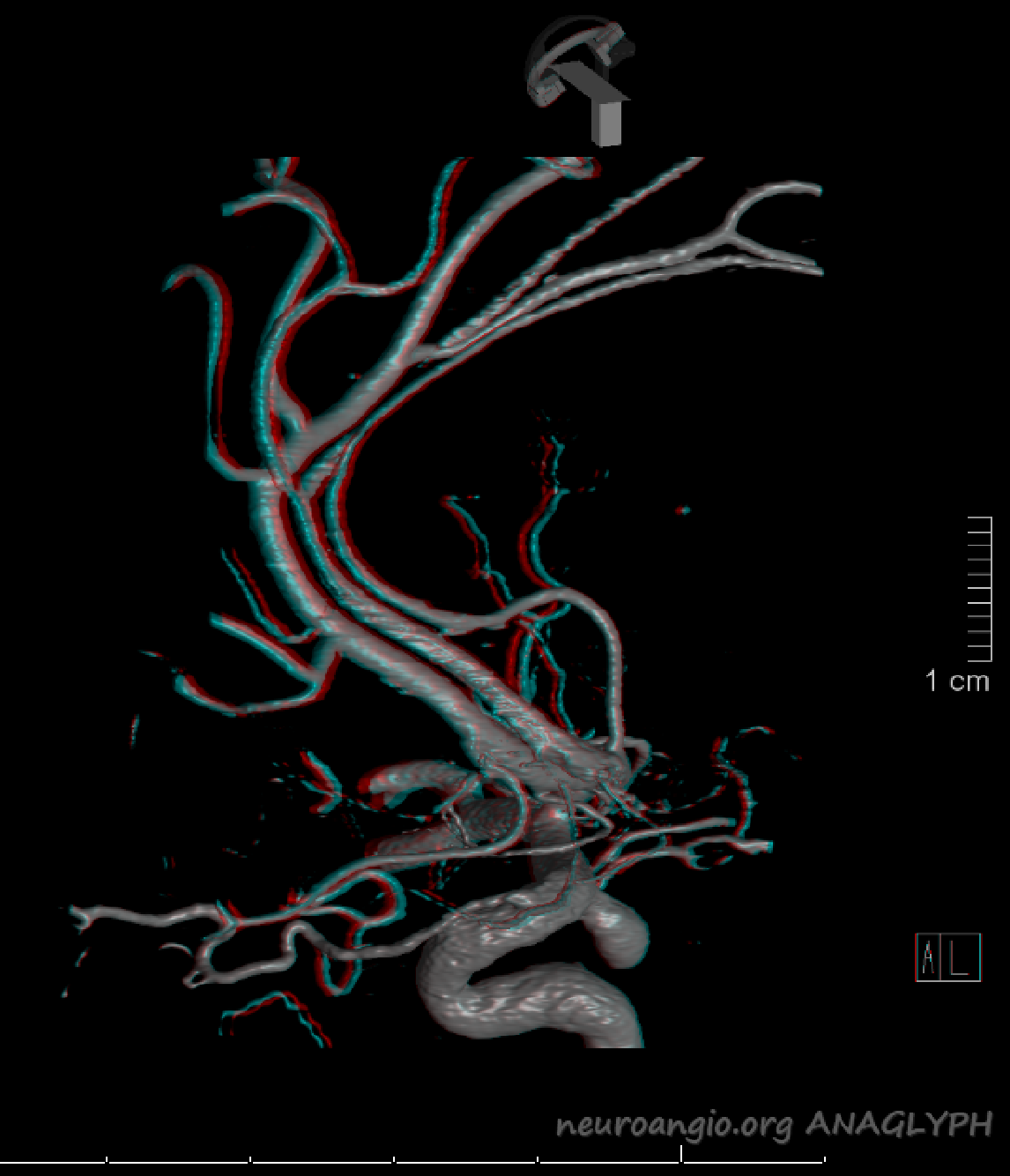
Stereo cross-eye
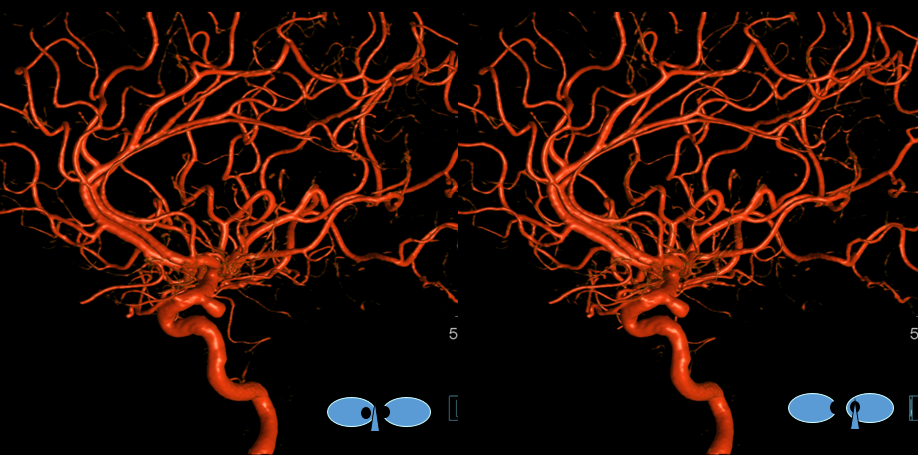
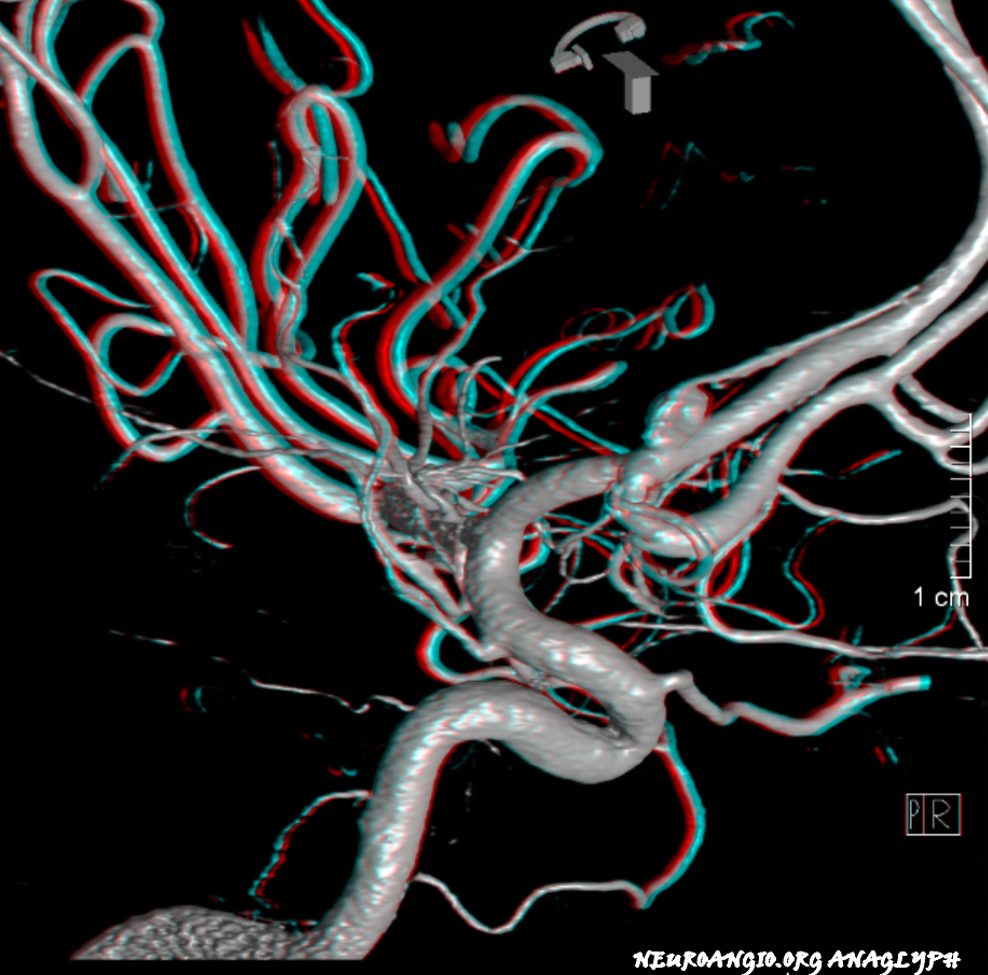
Anaglyph stereo
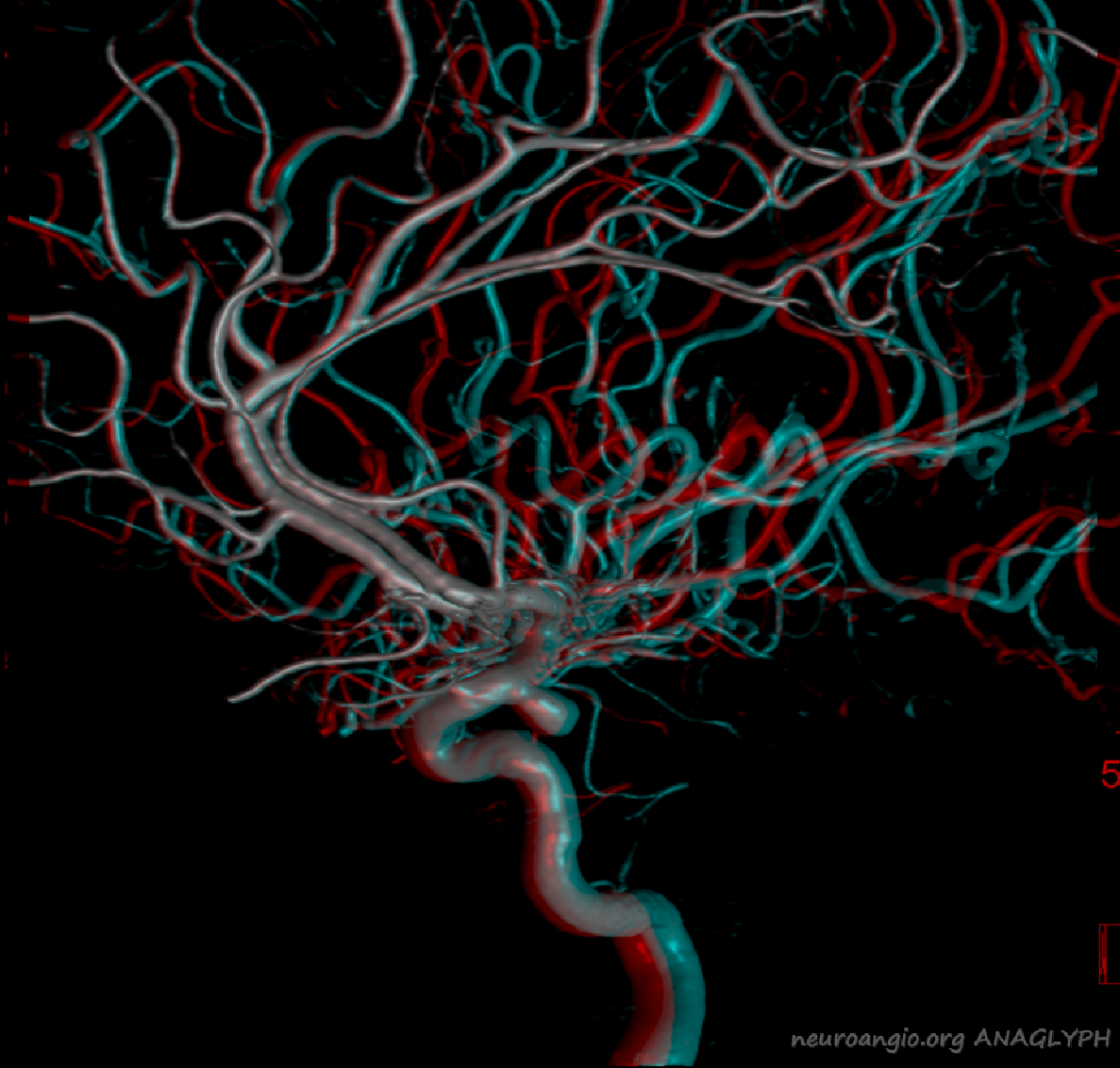
A less deep anaglyph
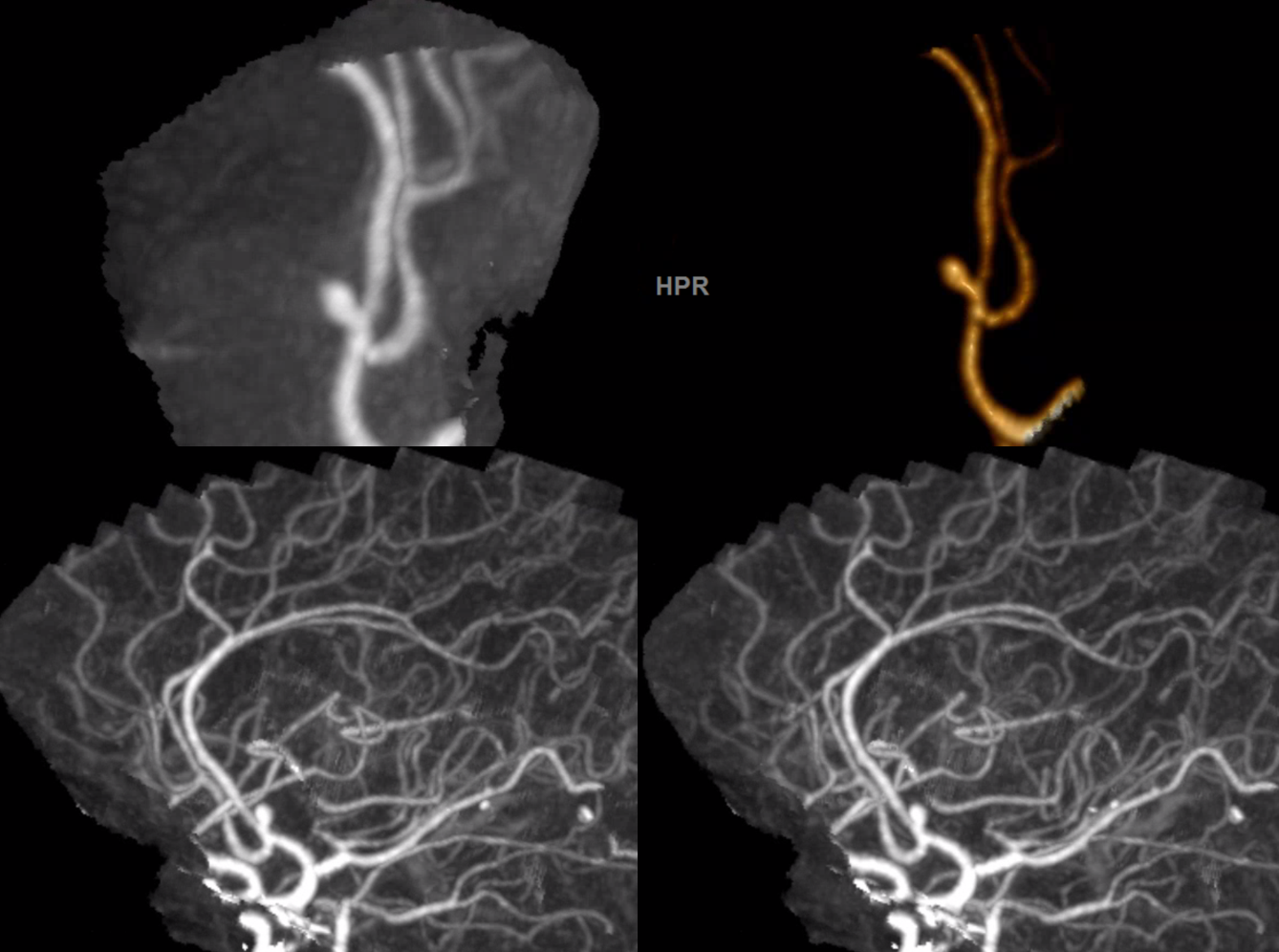
Angios — much harder to figure out than VRs
Almost always the subcallosal artery arises from the ACOM itself. Below its coming off one of the two ACOM fenestrations
Case 1: Courtesy Dr. Erez Nossek
Ruptured ACOM aneurysm — CTA. Notice how this aneurysm does arise directly from the A1/A2 bifurcation, nor point in the direction of A1.
Global angio STEREO views
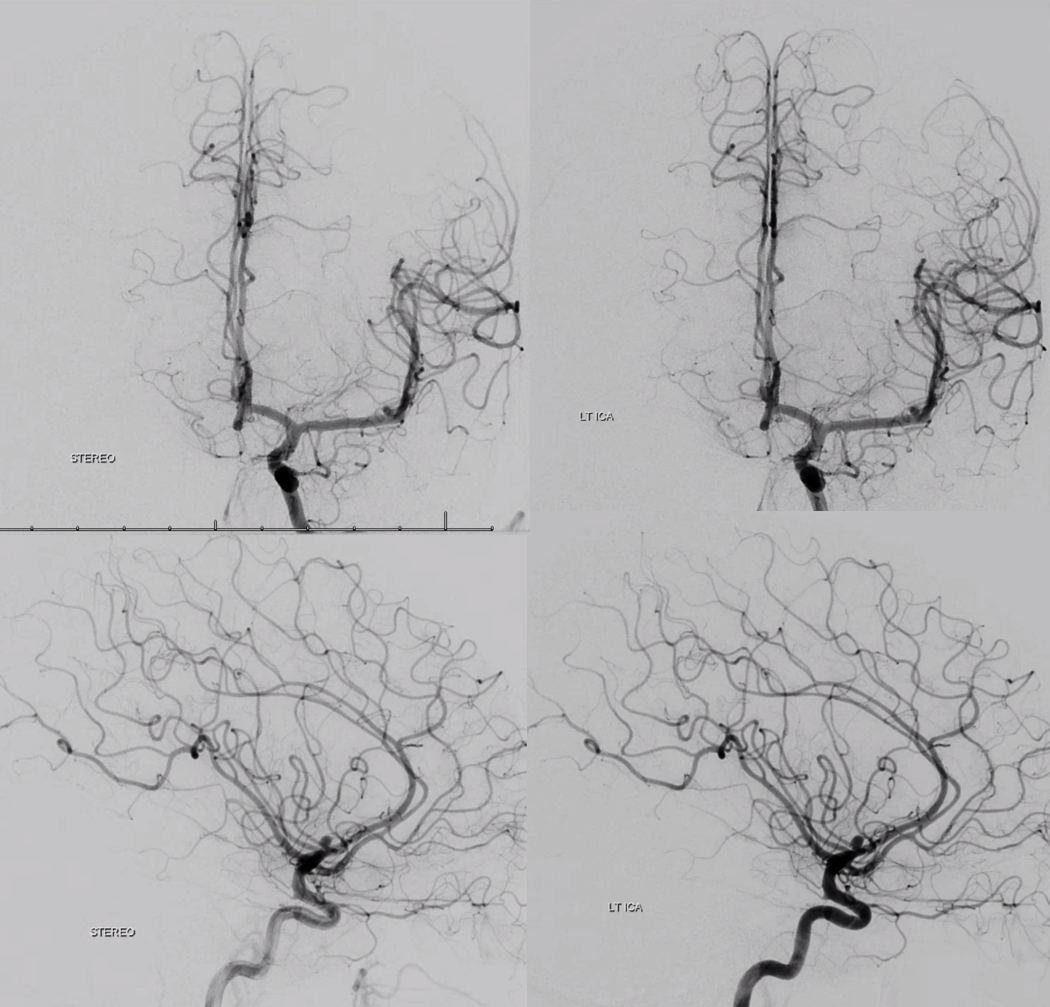
Dyna CT clearly shows a very sizable subcallosal artery that is totally invisible on CTA and barely appreciated on global angio
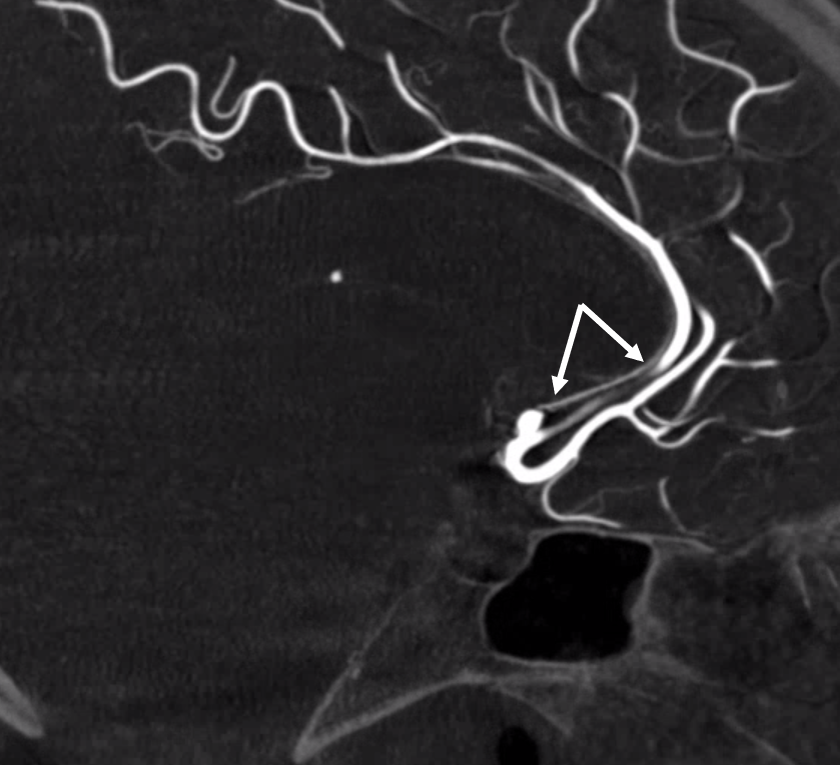
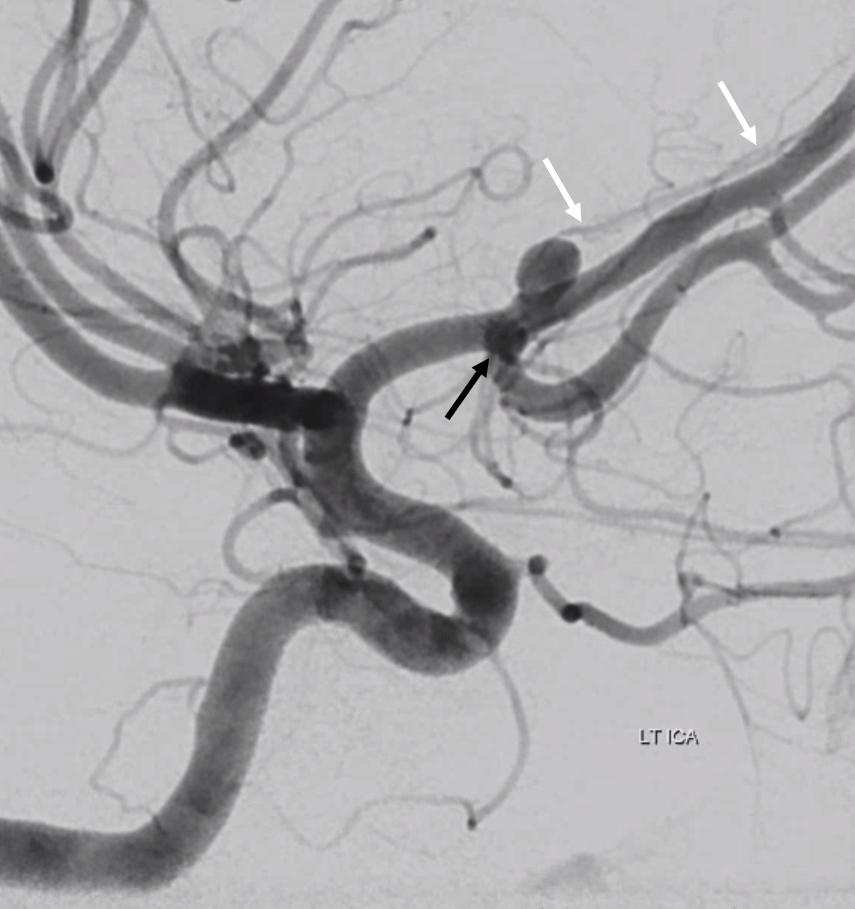
Magnified oblique view with vessel arising from aneurysm base. You see how important it is to identify this vessel and preserve it.
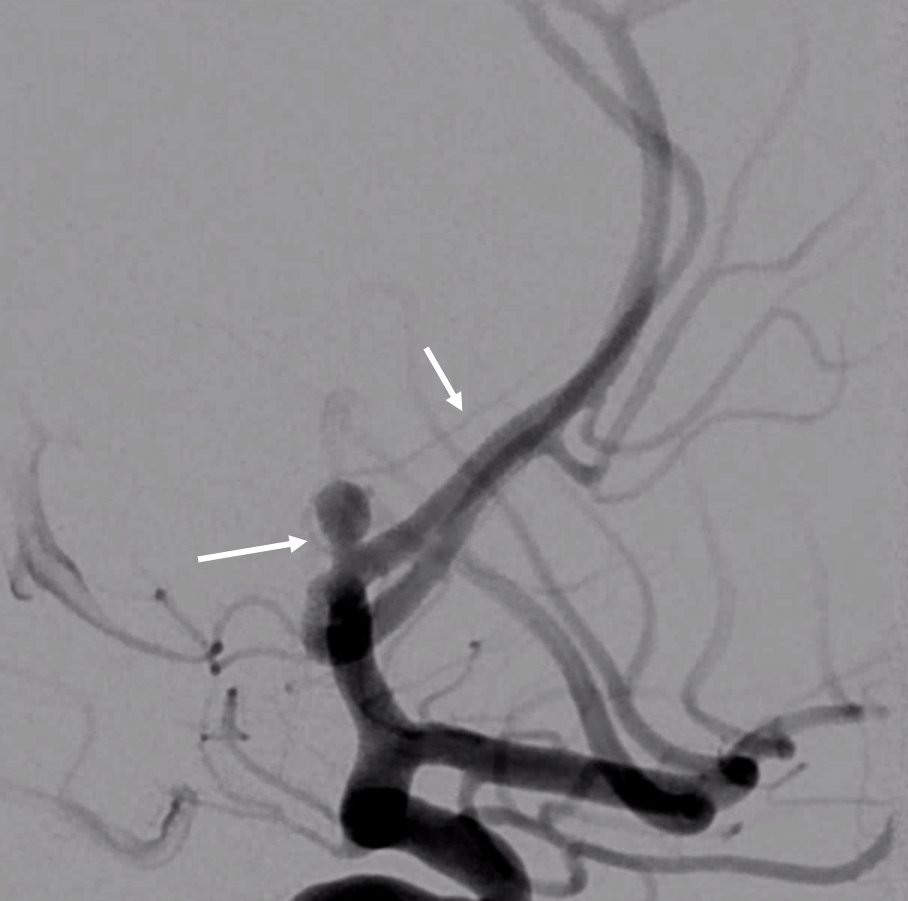
The A1/A2 bifurcation is labeled with black arrow. The aneurysm is really not arising from there, but rather from the origin of subcallosal artery. Therefore, it is in fact a “subcallosal aneurysm” — if you will
Stereo VRs
Anaglyph stereo
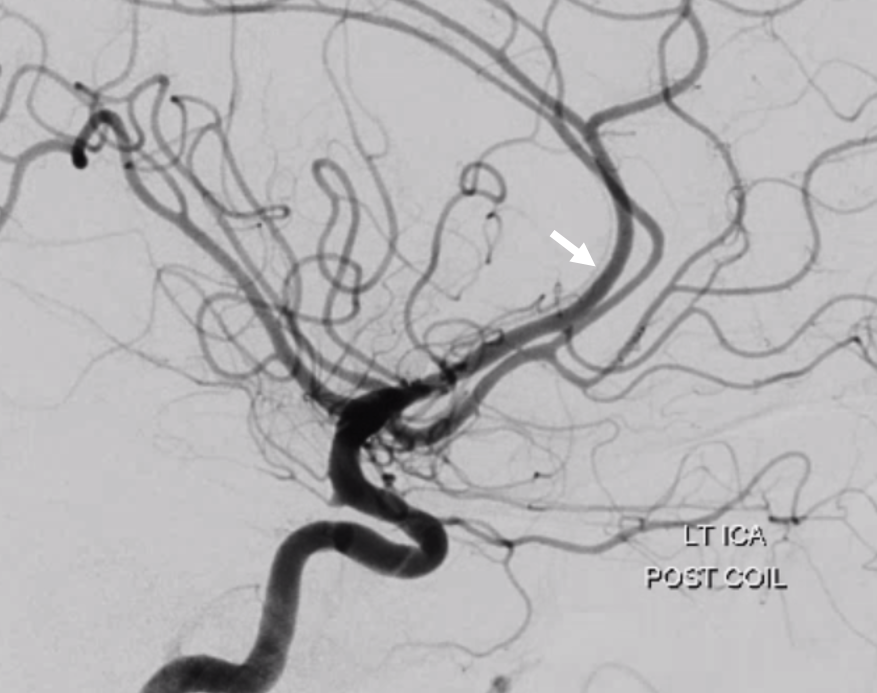
Treatment with Comanechi-assisted coiling — to keep that loop from closing the subcallosal
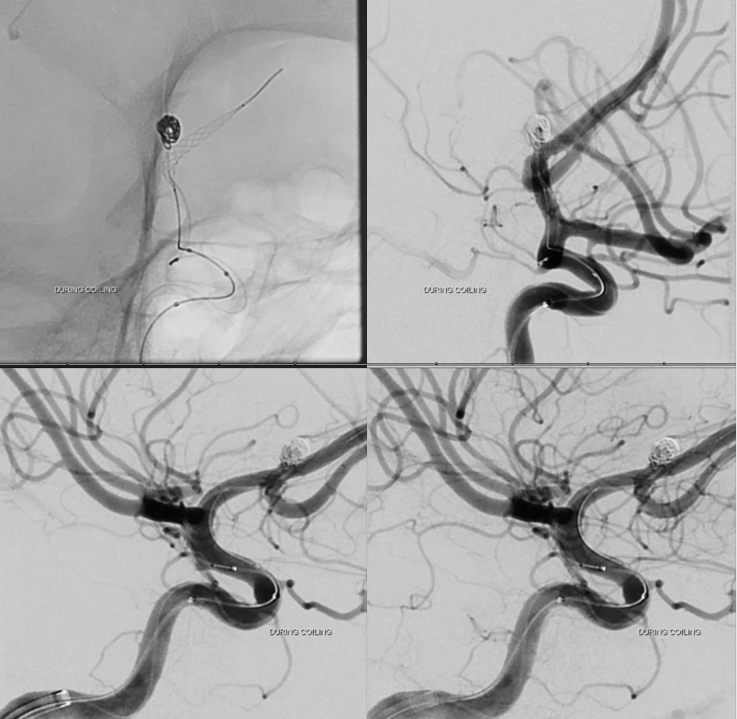
Post. Subcallosal is patent
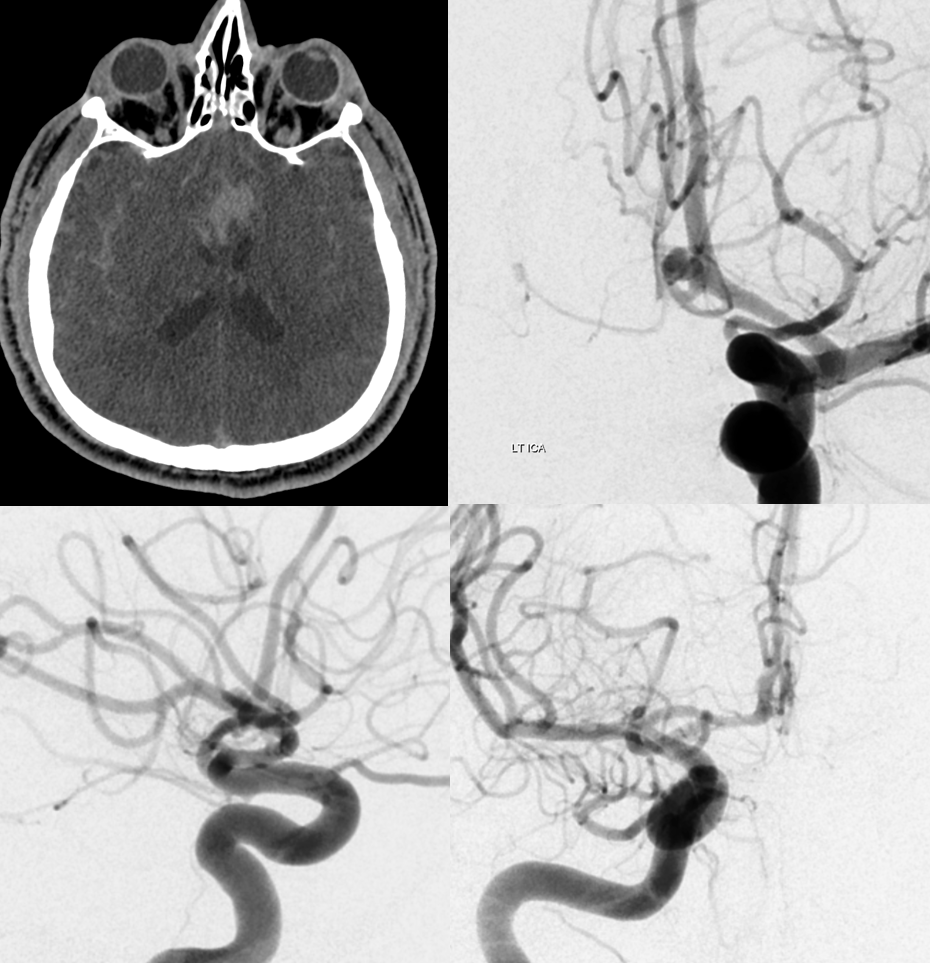
Case 2 — courtesy Dr. Erez Nossek
Another ruptured ACOM
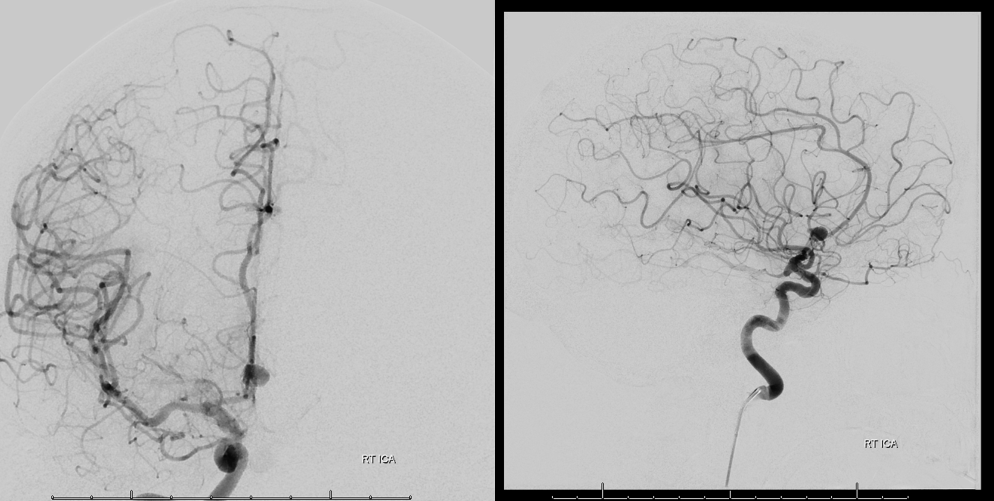
Again, Dyna CT shows it best — with hypothalamic perforators also (lower left image)
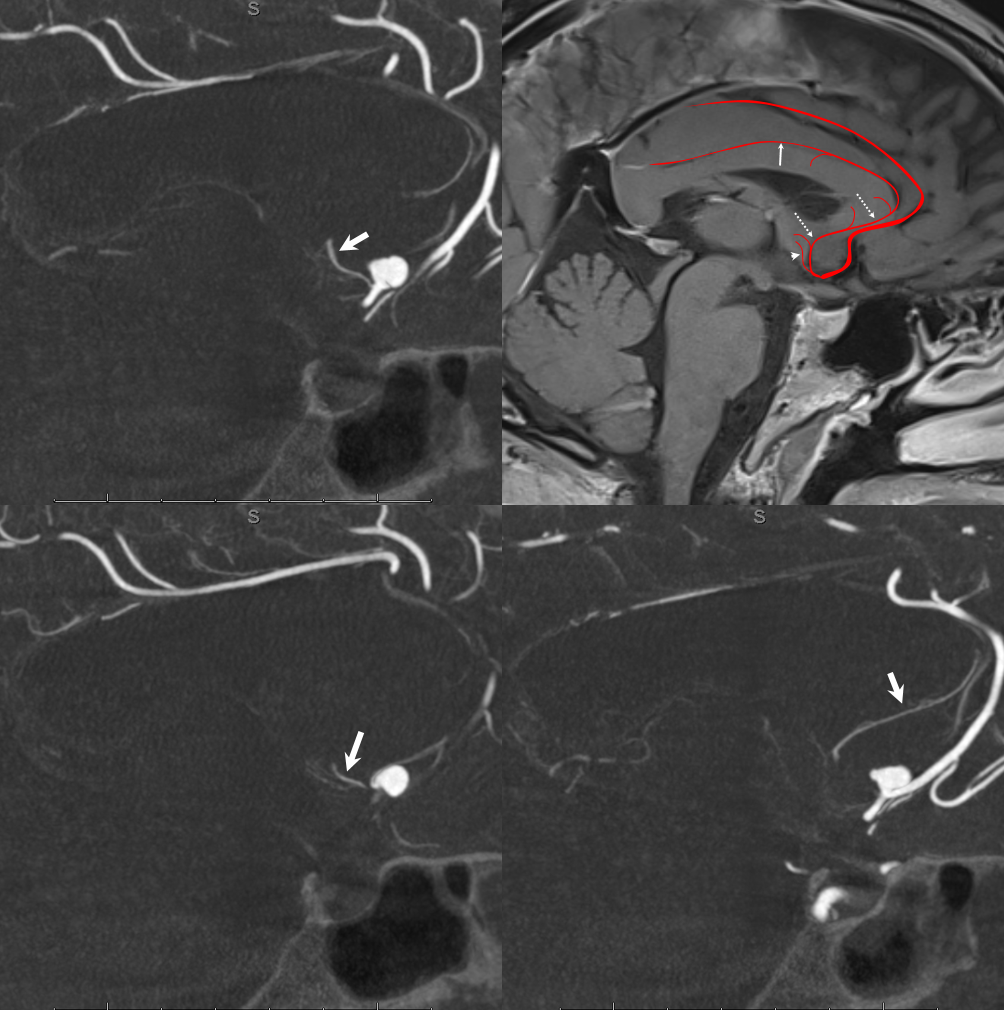
Post coil there is delayed perfusion of ACA territory
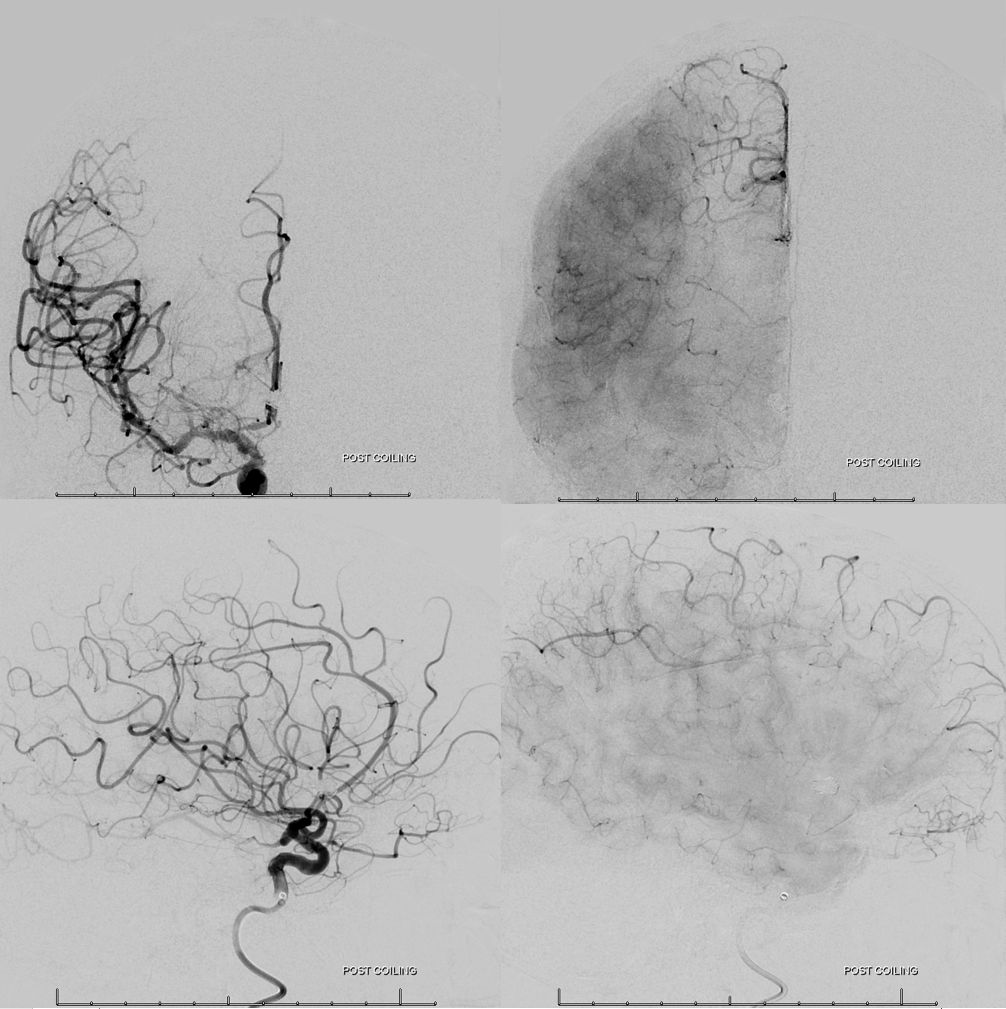
Working projection views — there is clot at coil base extending into the A2. The subcallosal artery is patent (white arrows). The Heubner is marked by dotted arrows.

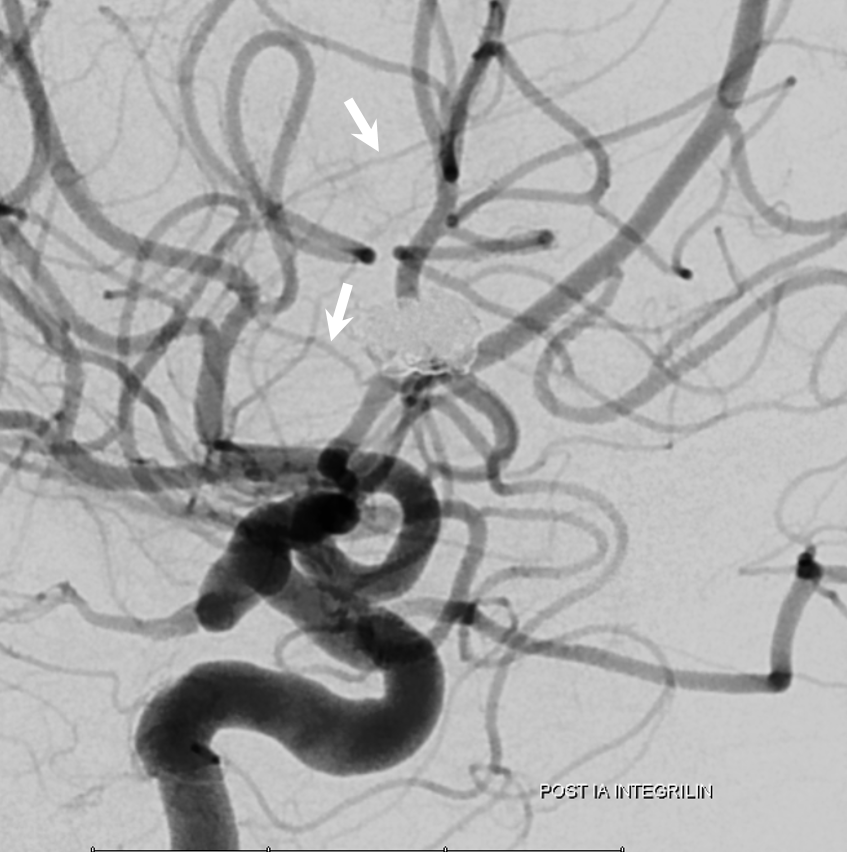
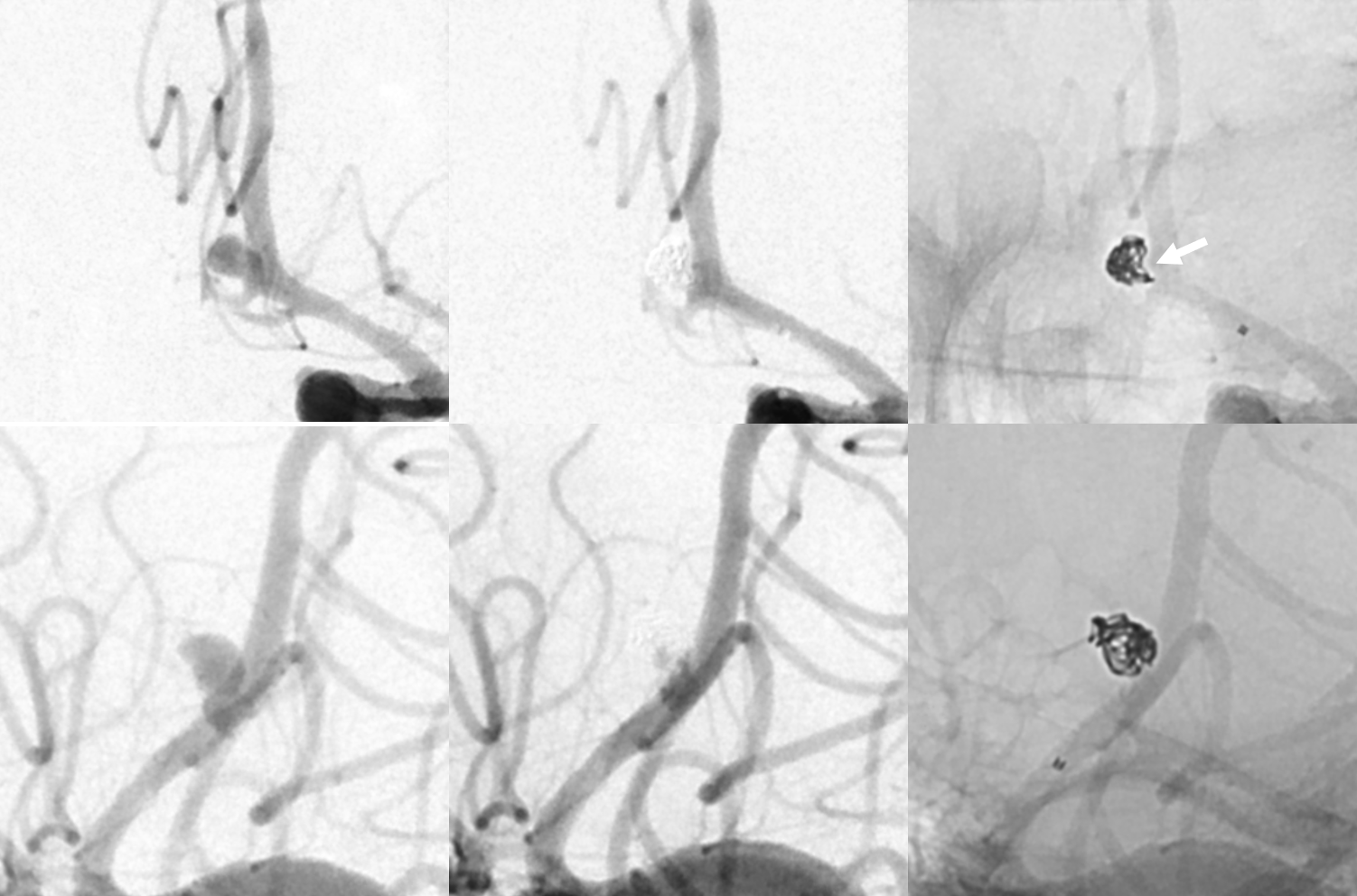
Frontal oblique

Post IA Integrilin — subcallosal artery again marked by white arrows
Subcallosal AND Duplicated Hypothalamic Perforators!
Great case by Vera Sharashidze and Sitara Koneru. Ruptured ACOM. Nothing much to see on 2D DSA — standard issue acom aneurysm, projects posterior…
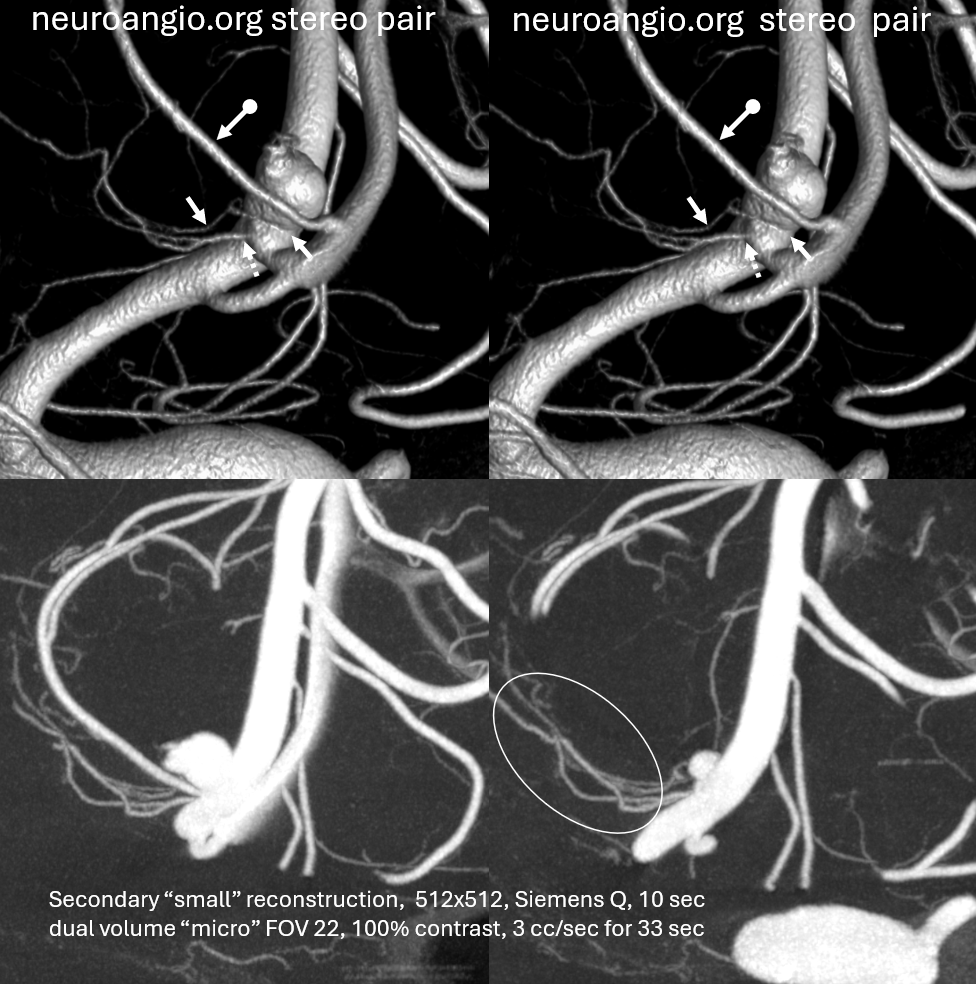
Volume rendered stereo images of 10 second “micro” FOV 22 dyna Siemens Q — natural fill reconstruction, 3 cc/sec for 33 sec injection. Already better quality than most 3D-DSAs out there
Now we see a subcallosal artery from proximal A2.

Done? of course not. Secondary “small volume” reconstruction. Look at the two hypothalamic perforators — one from acom (dashed arrows), one from aneurysm neck (arrows). Both extremely important, all must be preserved for the sake of hypothalamic function…
Movie
Now we know what we need to do. Aneurysm coiled subtotally to ensure neck and acom remain open. Plug and pipe later.
FINALLY — FANTASTIC CASE OF THREATENED COIL OCCLUSION OF SUBCALLOSAL ARTERY AND RECOVERY BY DR. RAZ IS HERE — DONT MISS IT
So, conclusion is dont let this happen to you. Watch for the subcallosal artery by doing careful angiography and keep it patent. Usually, its what we don’t see that hurts us — once u see it, avoiding problems becomes much easier.
References
https://academic.oup.com/ons/article/17/1/79/5250966
http://www.ajnr.org/content/35/12/2293.long