
Another variant — rare but instructive…
Accessory meningeal artery — can “arise” from either common stem with MMA or separately from IMAX — a famous (among some cult embryology followers) distinction based on course of IMAX relative to the medial pterygoid muscle.
Anyway, the accessory meningeal classically has 2 divisions — intra and extra-cranial. The extra-cranial one supplies regional soft tissues, and principally anastomoses with pharyngeal division of ascending pharyngeal and ascending palatine arteries.
The intracranial division enters the cranial cavity thru foramen Ovale — an important point as proximal embo would endanger V3. Once inside, anastomoses with MMA, ILT and ophthalmic branches are possible — the “usual” territory is variable and mostly confined to medial cranial fossa floor. Basically, the accessory meningeal is an MMAwanna be — either one can do the job of the other — but usually MMAcarries the day. Here accessory meningeal supplies “typical” MMA territory — the frontal MMA division — similar to how a recurrent meningeal is usually confined to frontal branch (see MMA page for more). It also supplies the PETROSAL / FACIAL arcade territories — very important, and has ophthalmic anastomoses
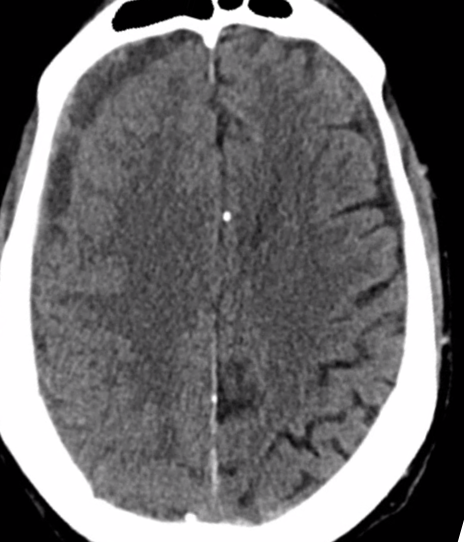
Right bigger than left subdurals
Right MMA embo
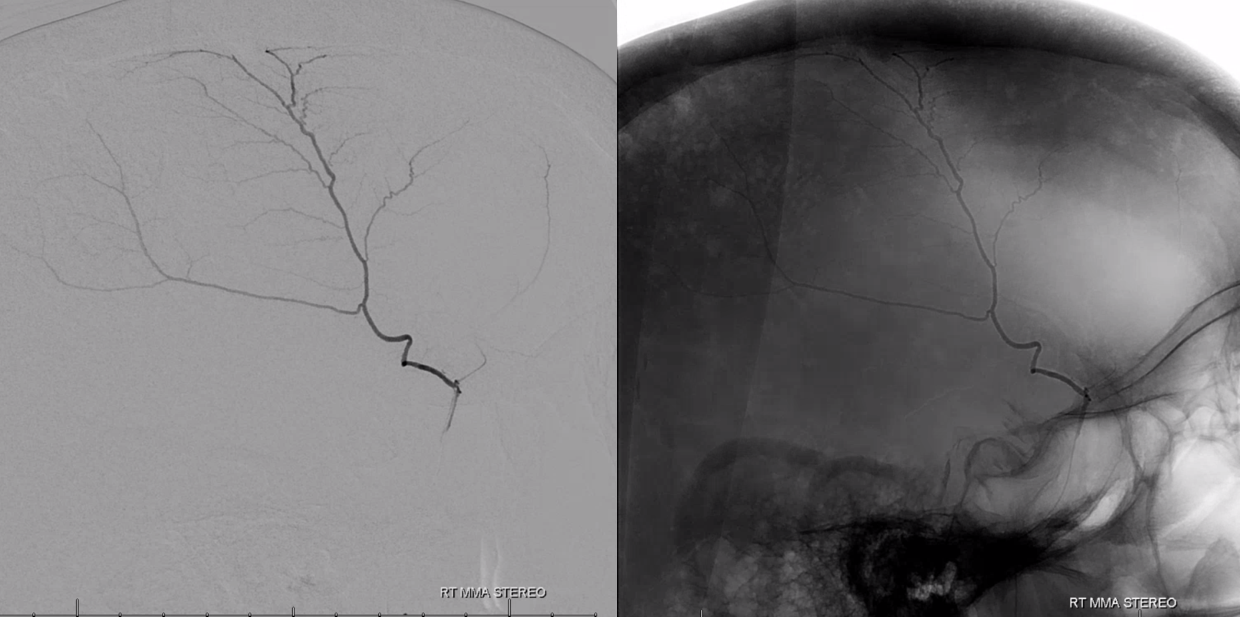
Note contrast washout from embolized territory into MMA venous system
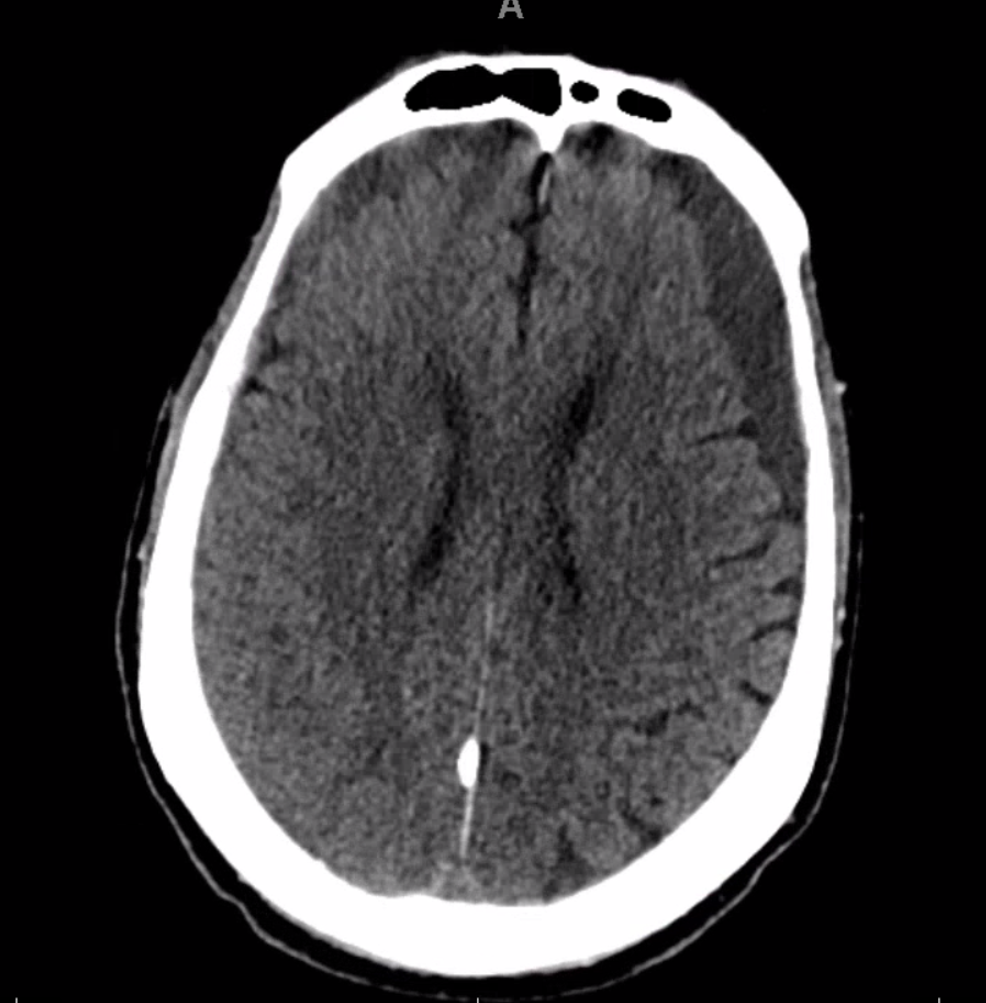
Tree weeks later, right is smaller, left is bigger…
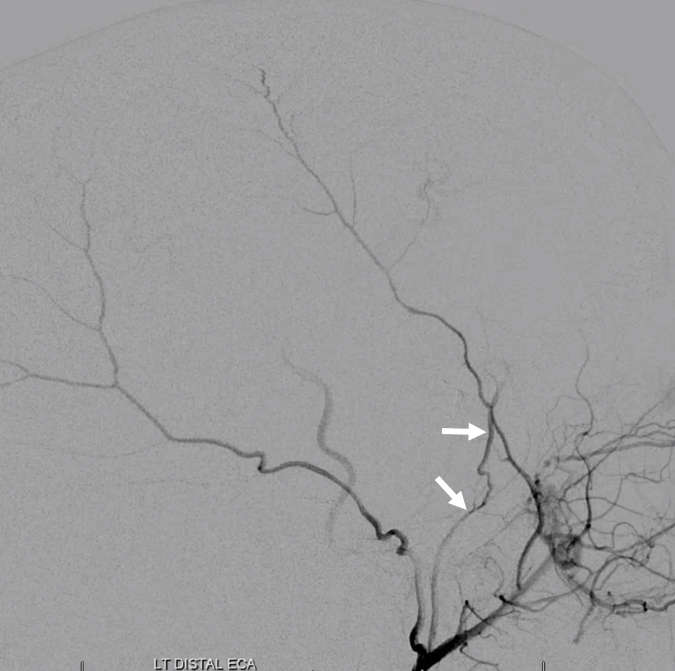
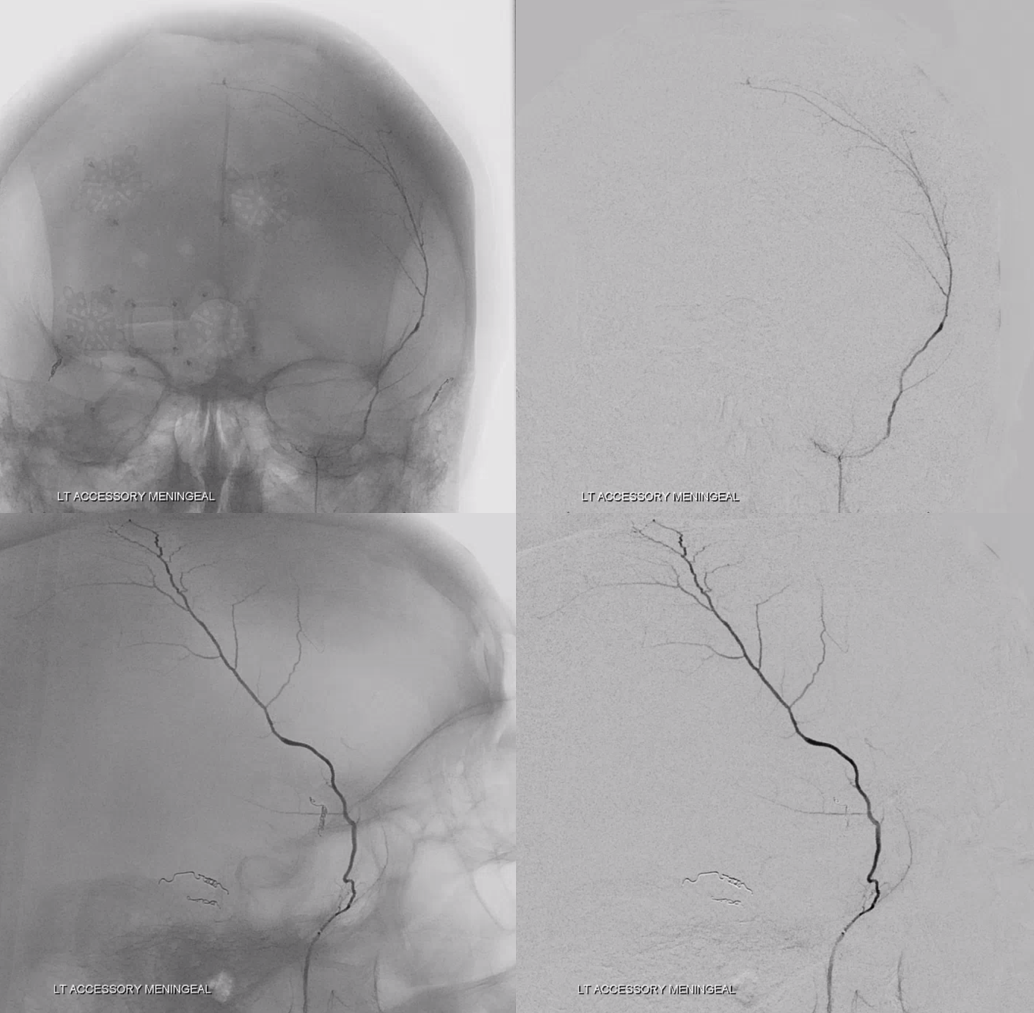
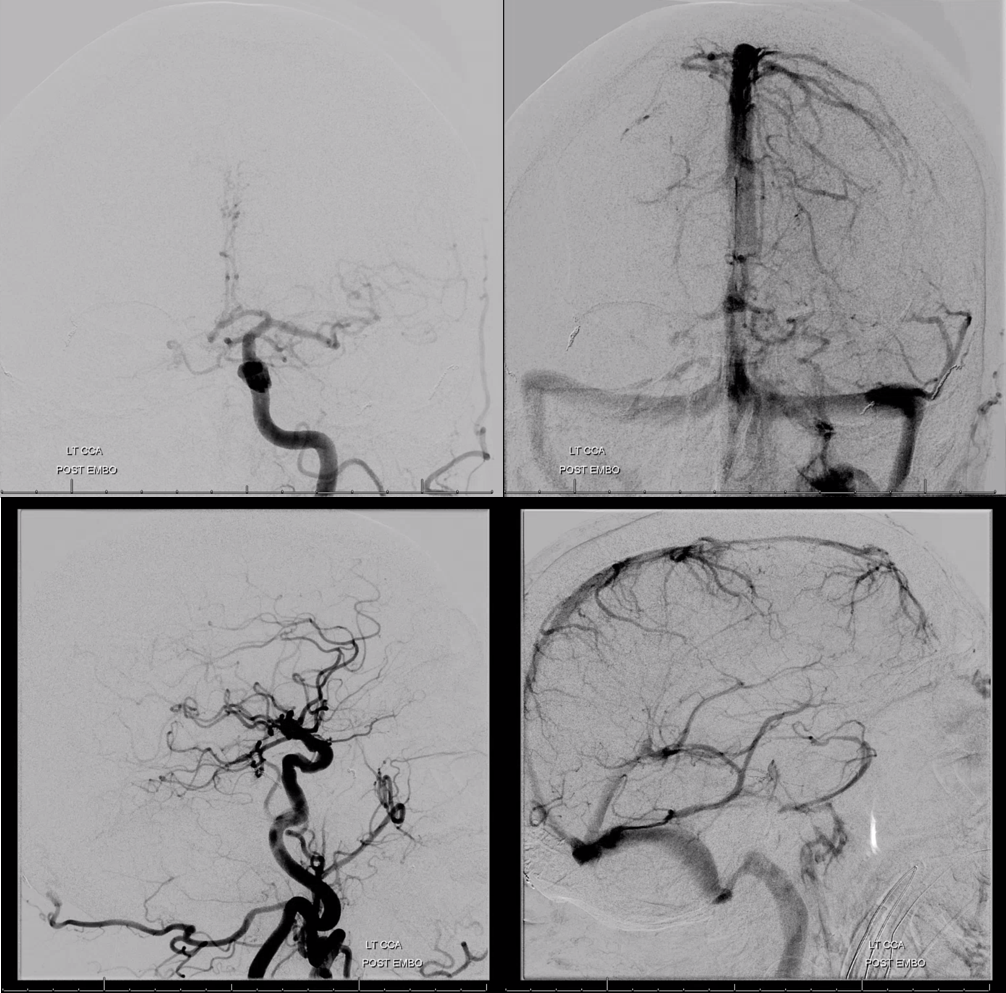
Distal left ECA injection. Accessory meningeal supply of frontal meningeal branch (arrows)
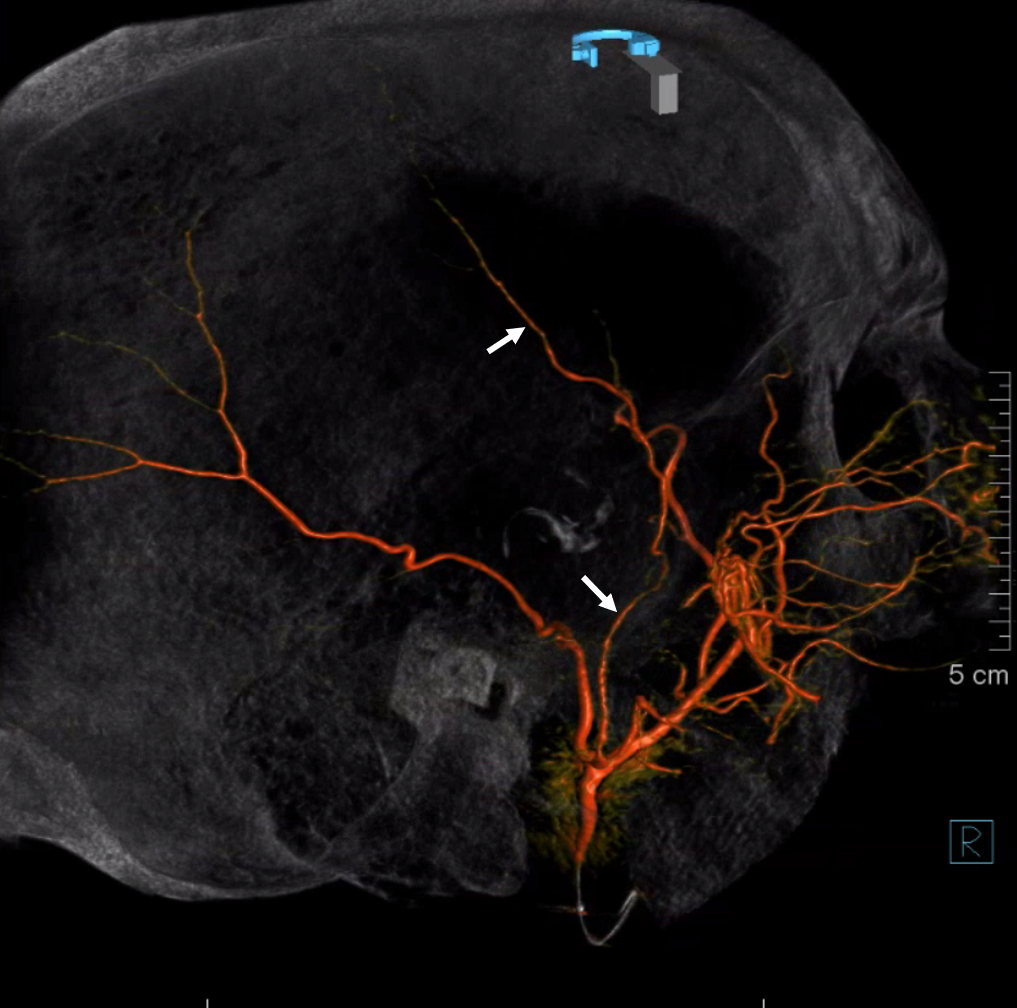
VR
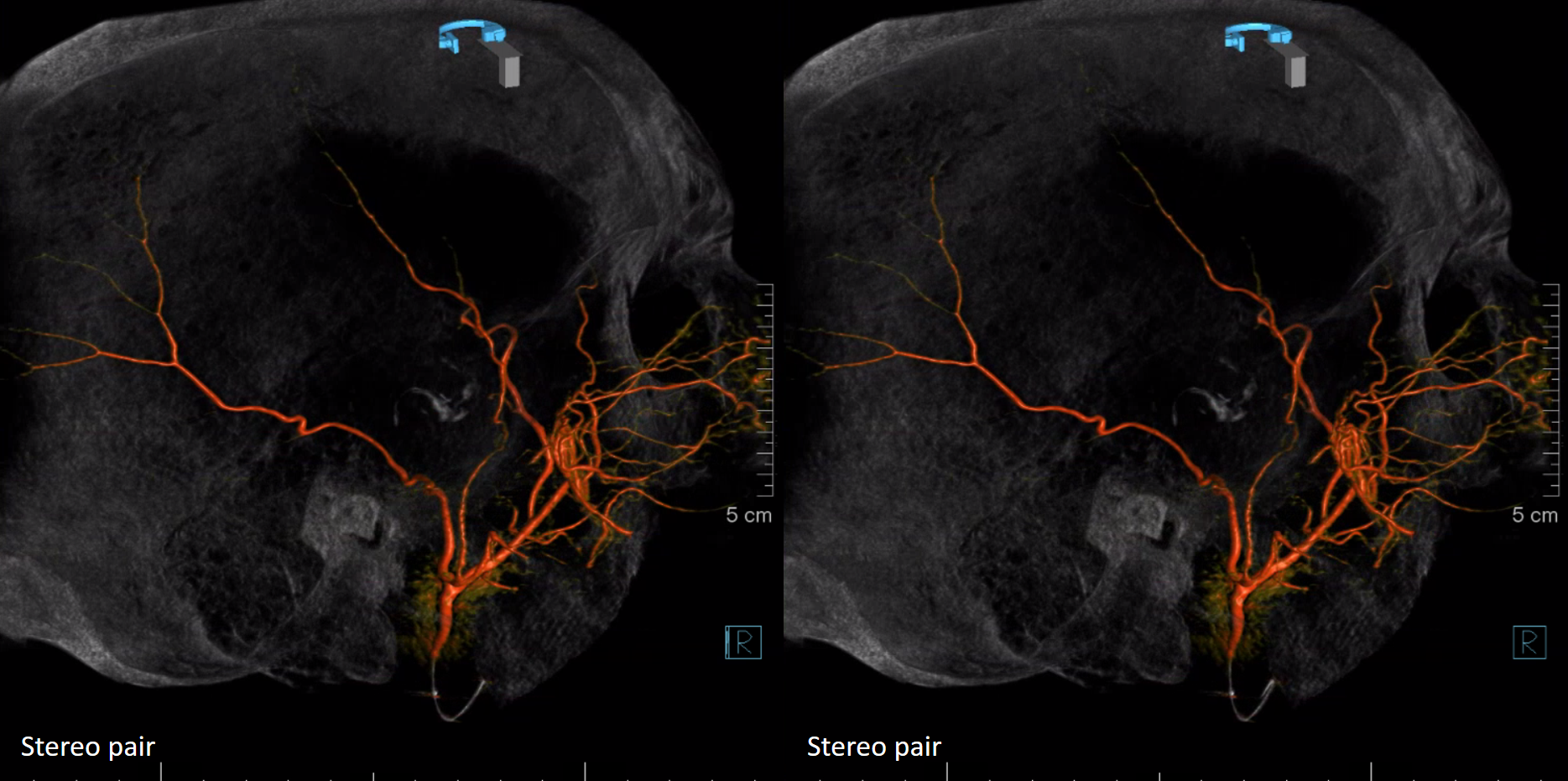
Stereo
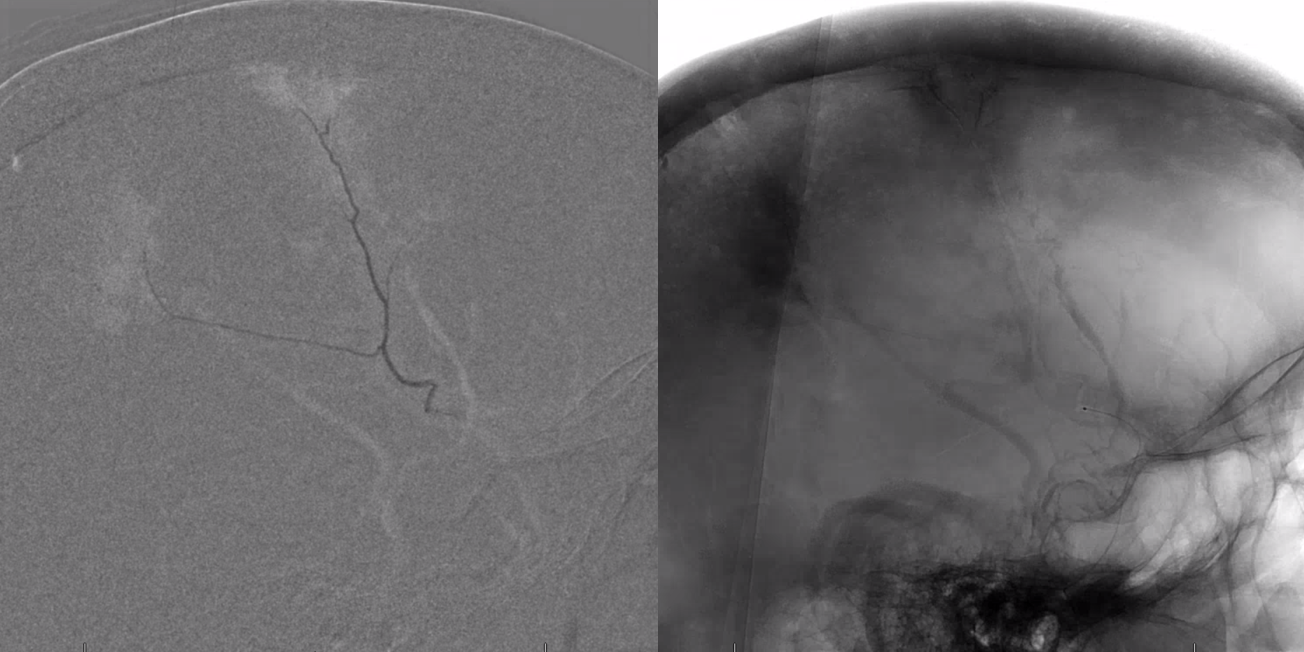
Petrosquamosal branch supplying parieto-occipital dura — no contribution to the facial arcade is visible here
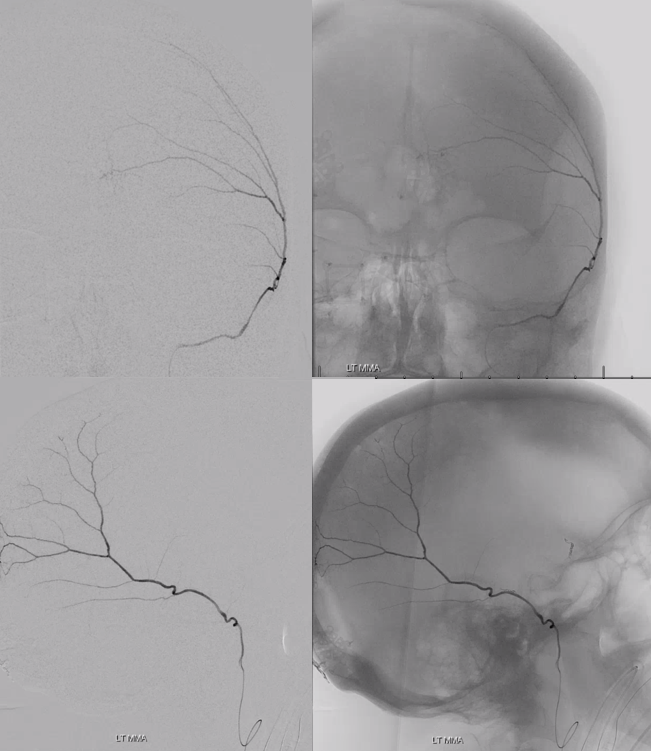
Accessory meningeal injection — frontal meningeal branch supply. Notice the characteristic proximal medially projecting branch — towards the cavernous sinus region and the ILT / carotid anastomosis. watch it…
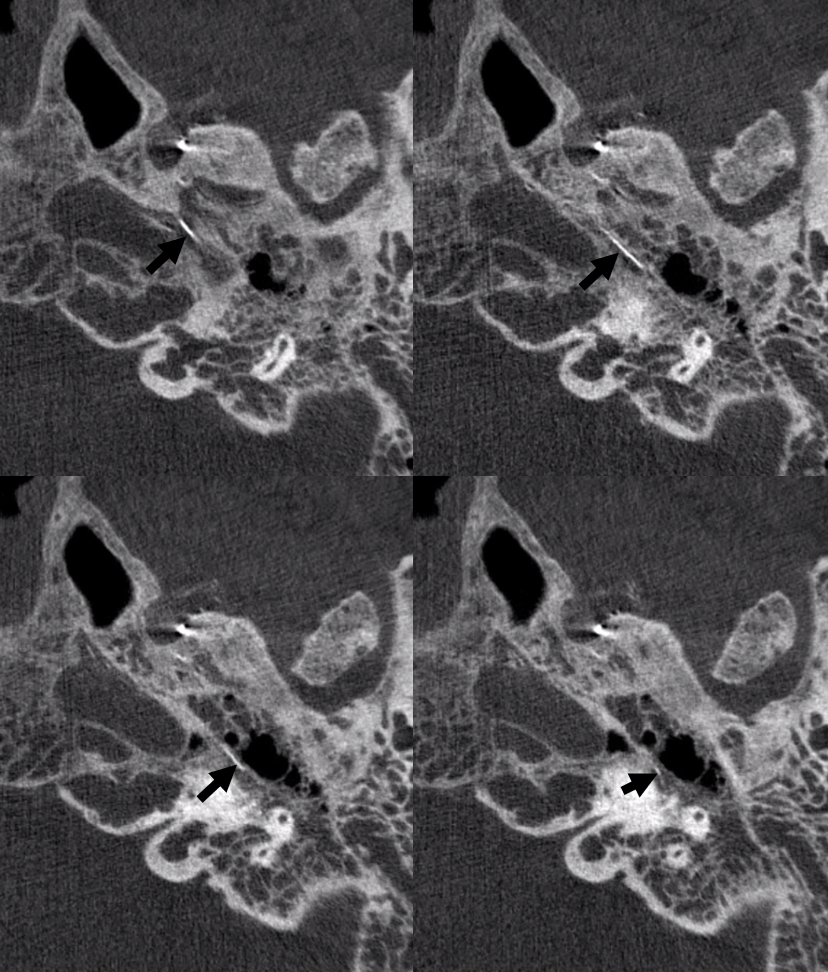
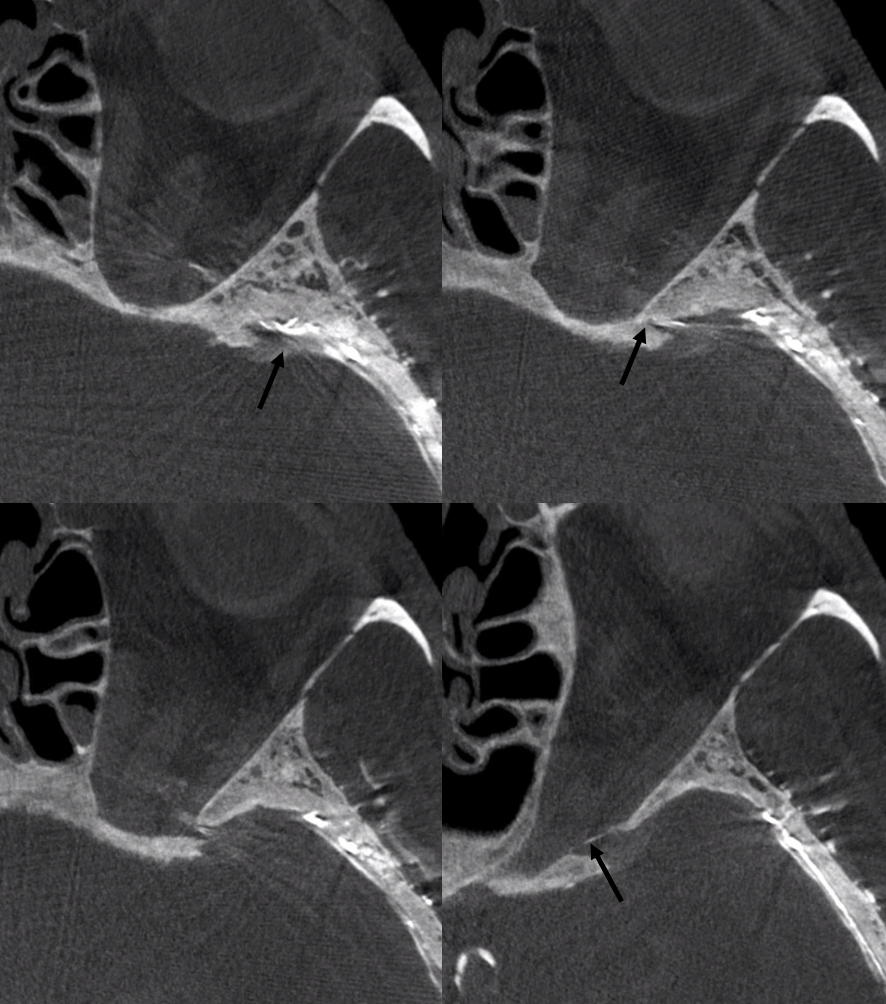
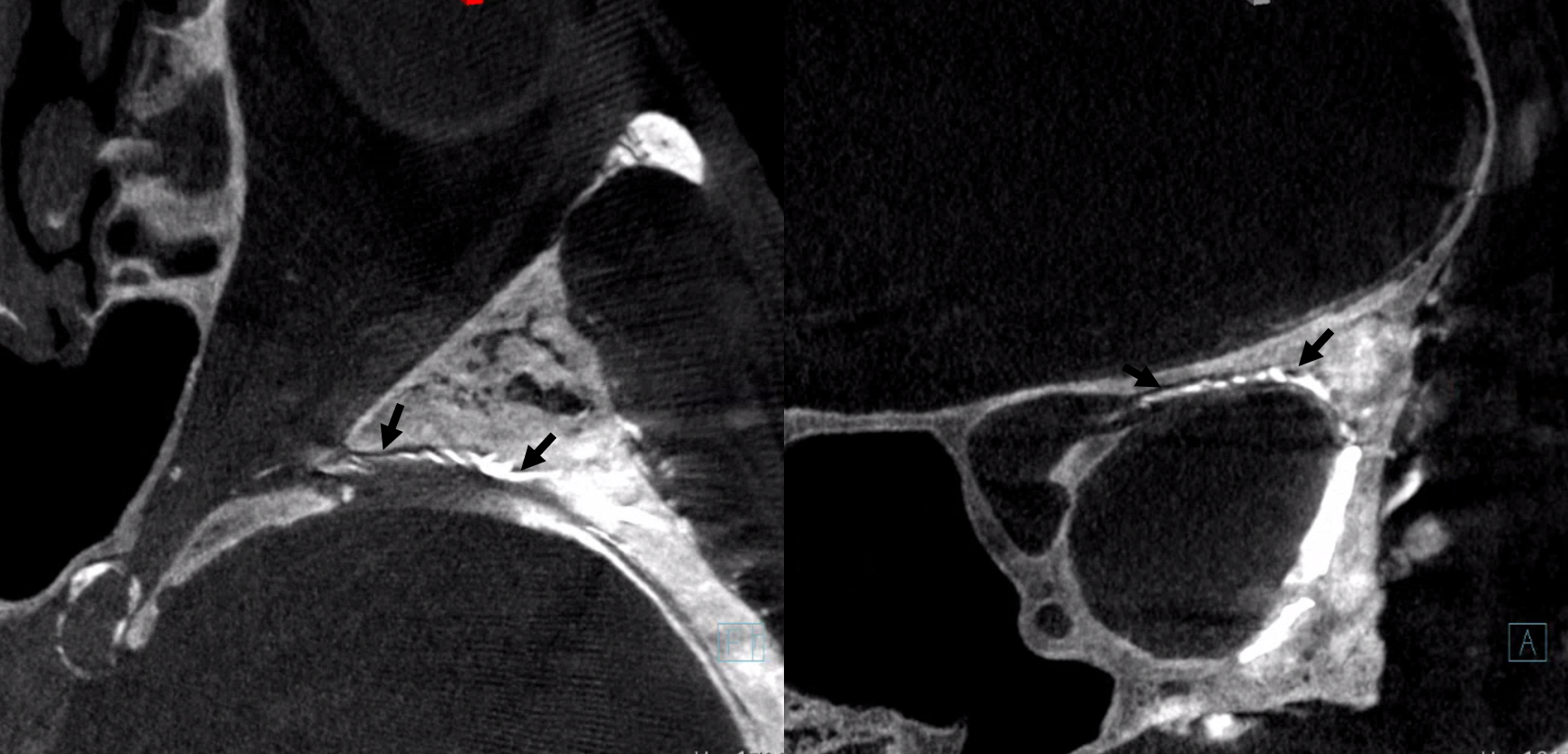
DYNA nicely shows supply to a juicy big facial / gasserian ganglion branch (arrows). The catheter is in the ovale — not labeled. Funny how ovale is further to the facial canal than spinosum but still takes care of it
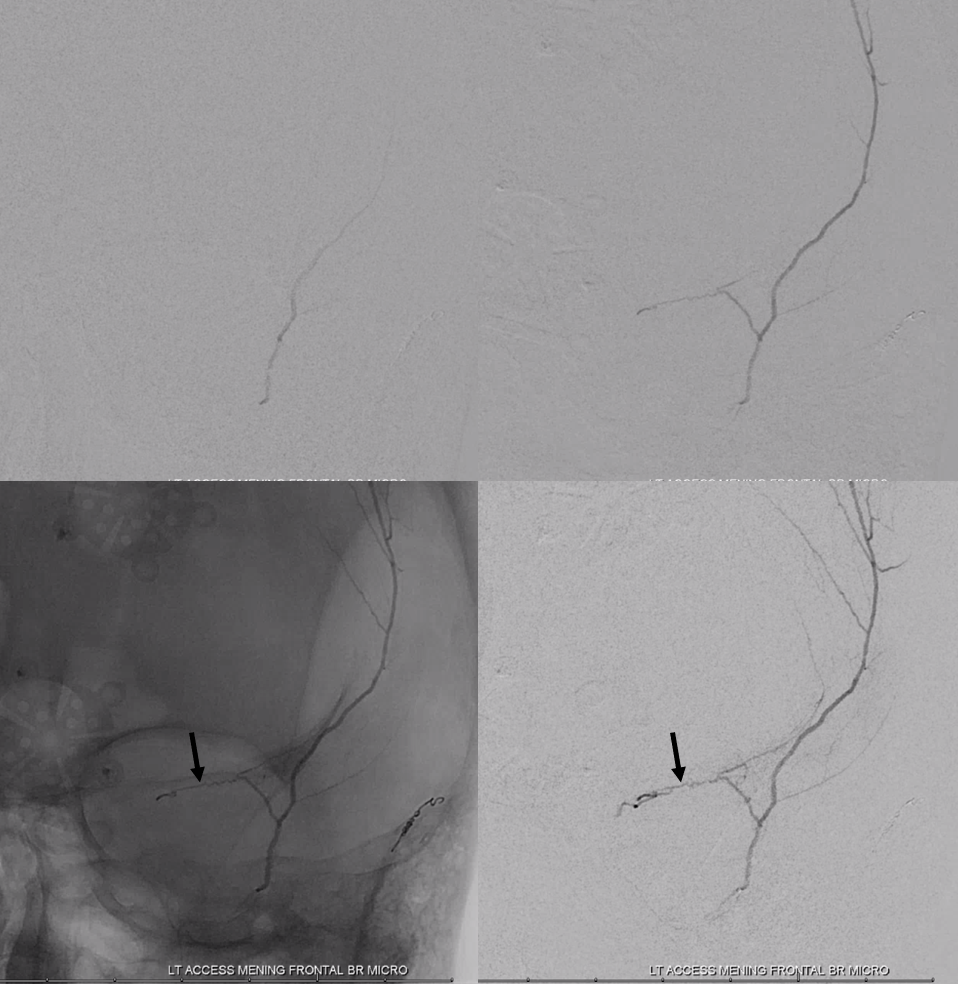
A more distal frontal branch injection (to protect the facial) now shows the typical anastomoses with the ophthalmic system via the sphenoid ridge branch (black)
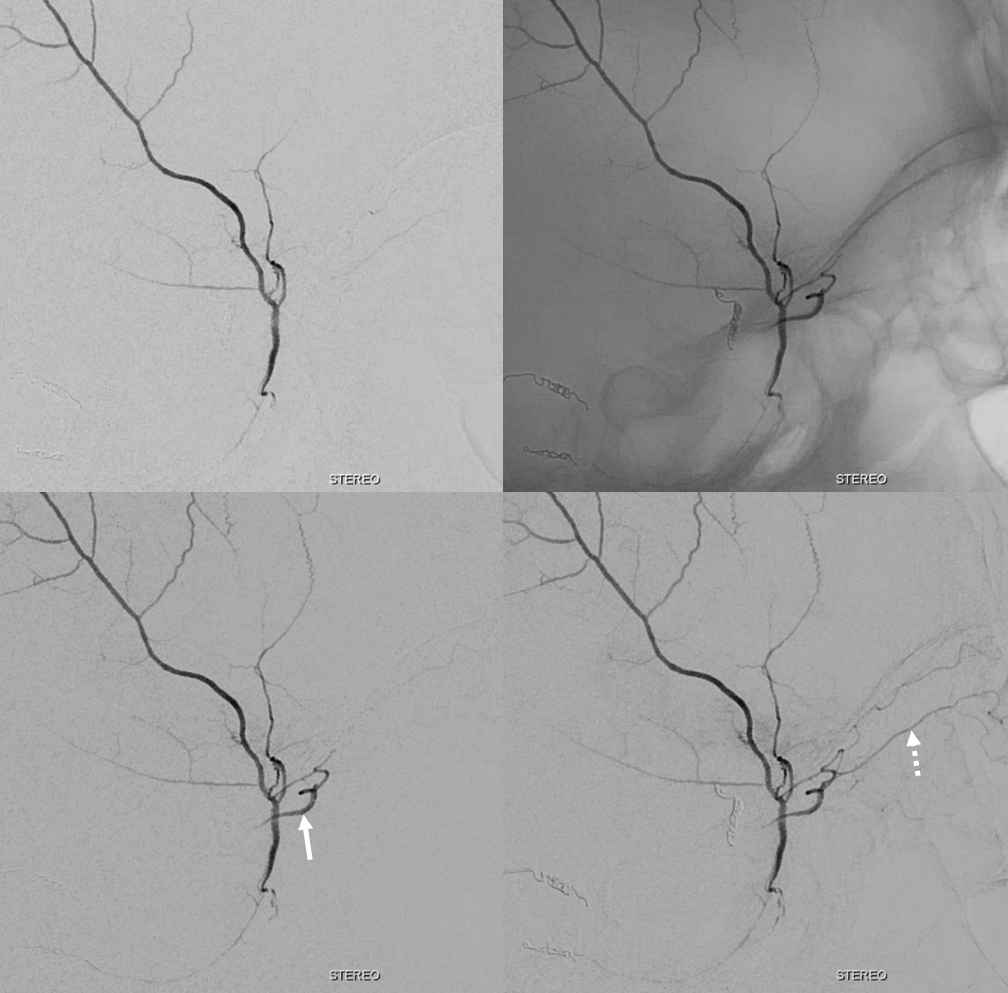
Lateral views — ophthalmic system (white arrow, principal runoff upper branches to superior rectus, forehead tissues etc (dashed arrow). So be careful here too 🙂
DYNA of same (arrows on the sphenoid ridge branch)
Oblique MIP DYNAs
Post
See more subdural embo cases in archives…