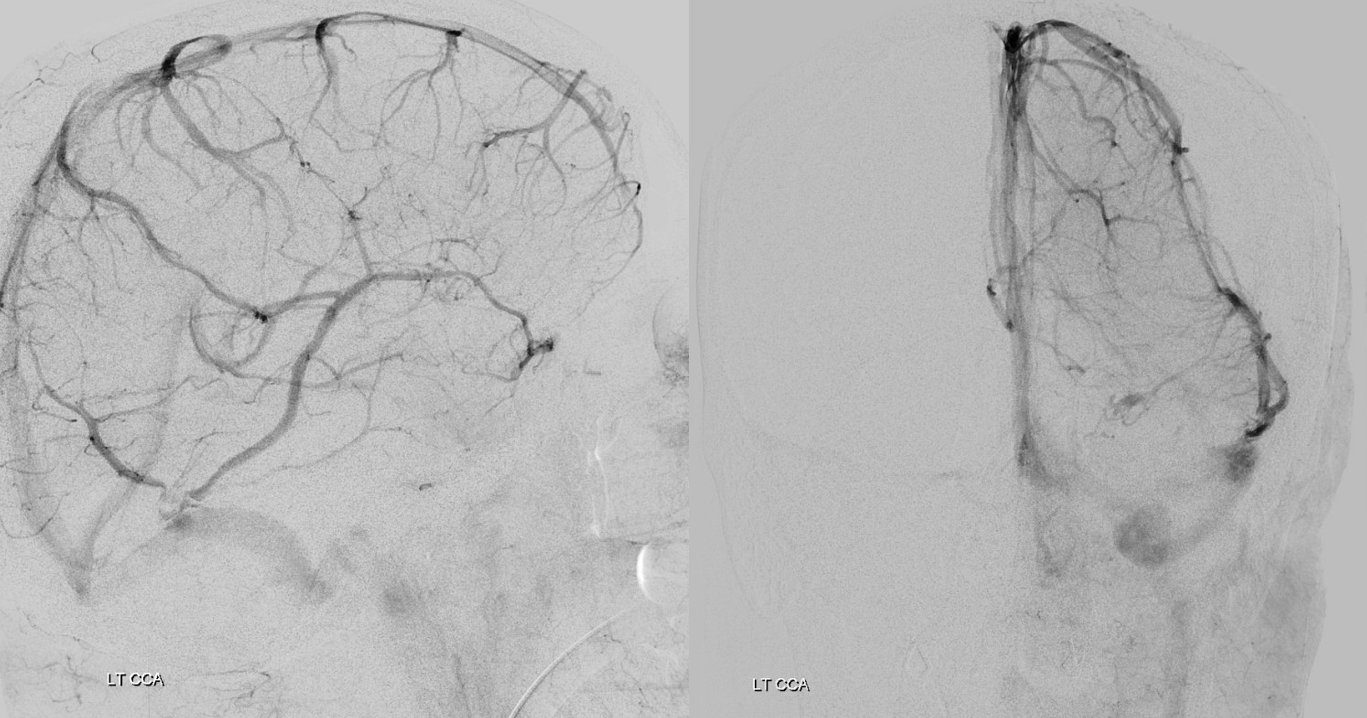
Another example of the importance of high quality embolization and understanding of collateral circulation. Classic acute on chronic subdural
Venous phase
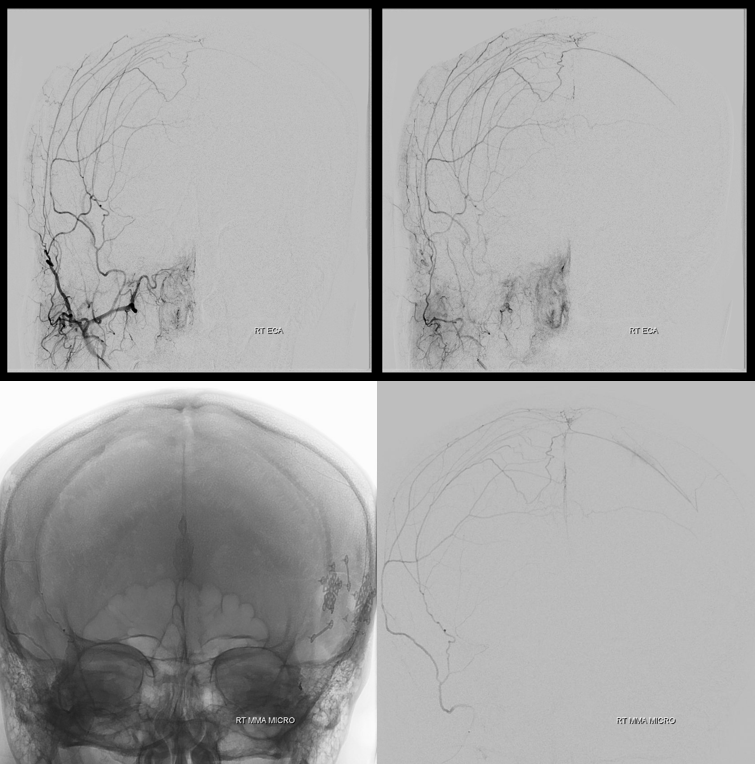
History of remote left pterional craniotomy. Both frontal and parietal (anterior and posterior) divisions of MMA are interrupted. There is desent collateral supply of the parietal / posterior division via the petrosquamosal branch. Inferior images are wedge position micro injections into the petrosquamosal
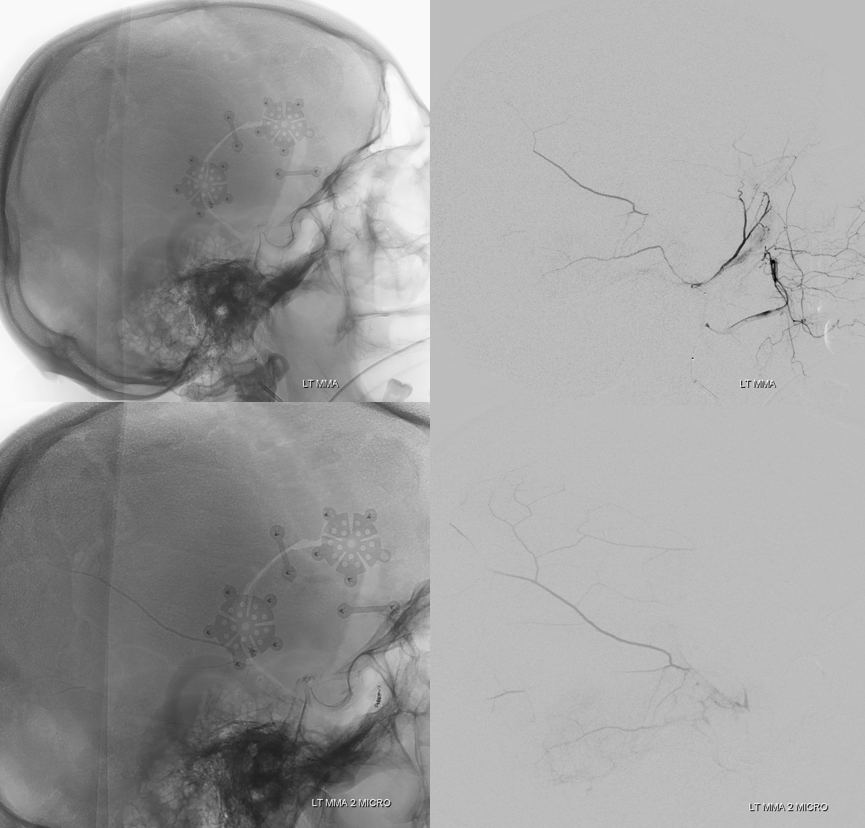
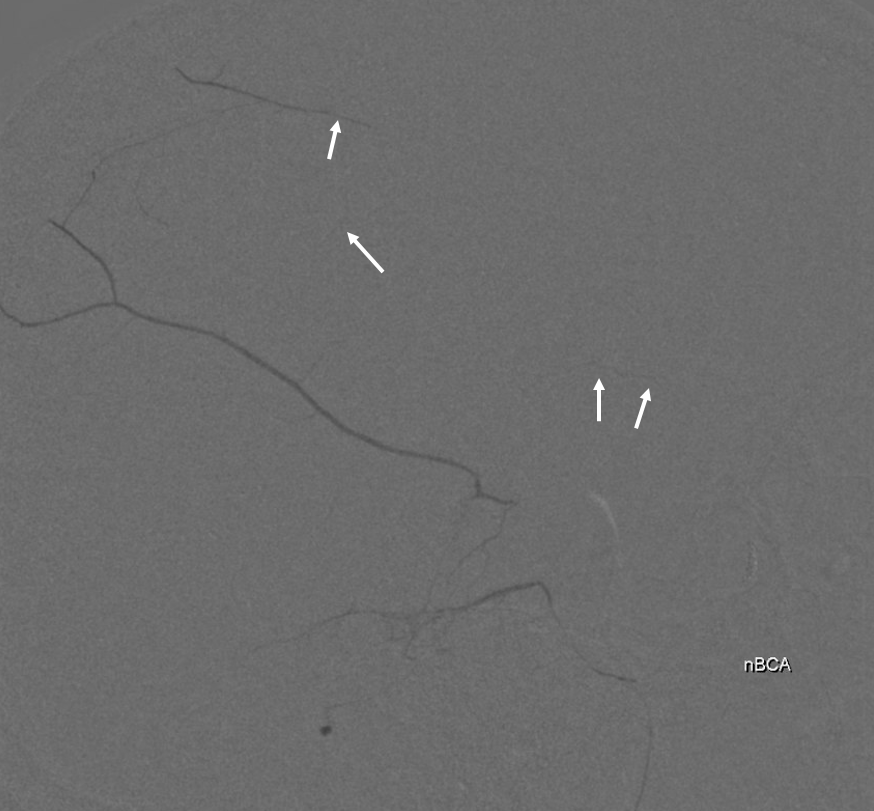
Dilute nBCA injection penetrates very well into the posterior/parietal division and even a little bit into the frontal / anterior division (arrows)
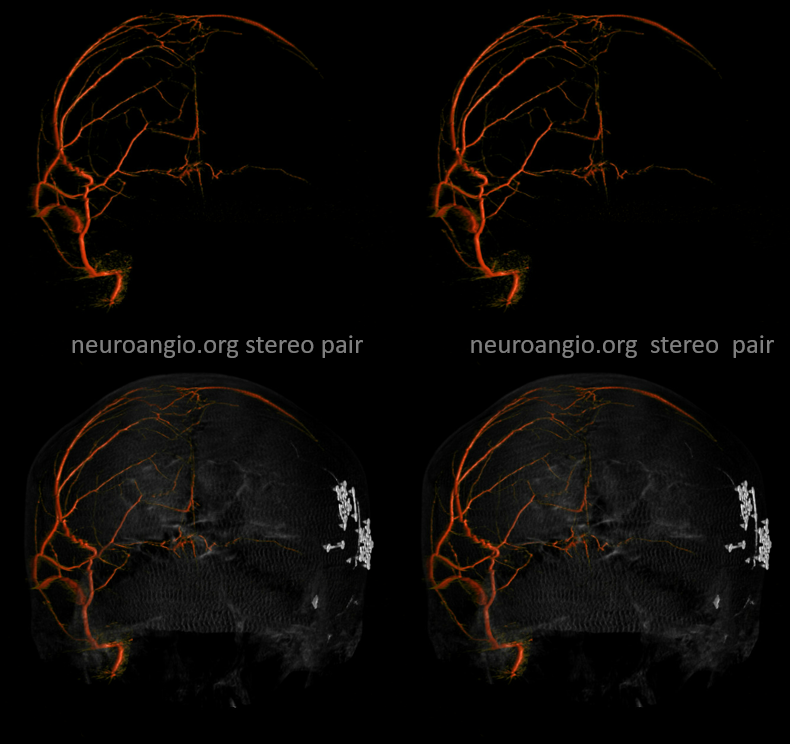
What more to do? Go to the other side. Good cross-midline right to left MMA anastomoses are present
Micro injection wedge position frontal division
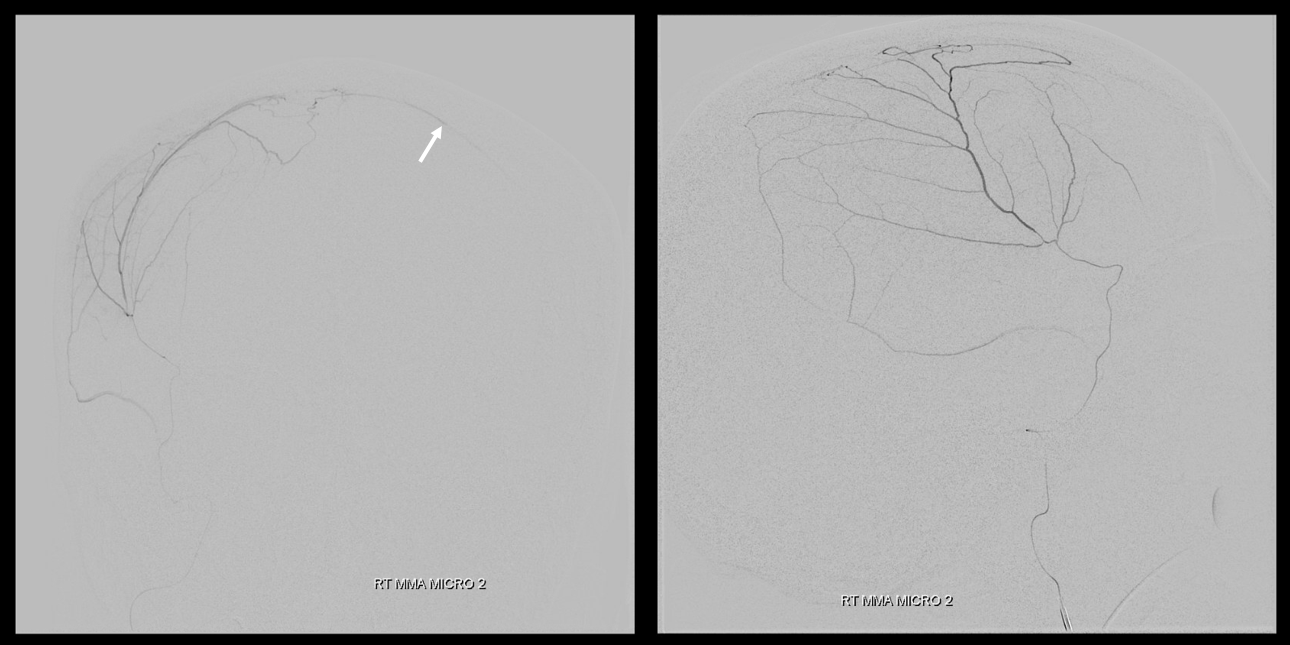
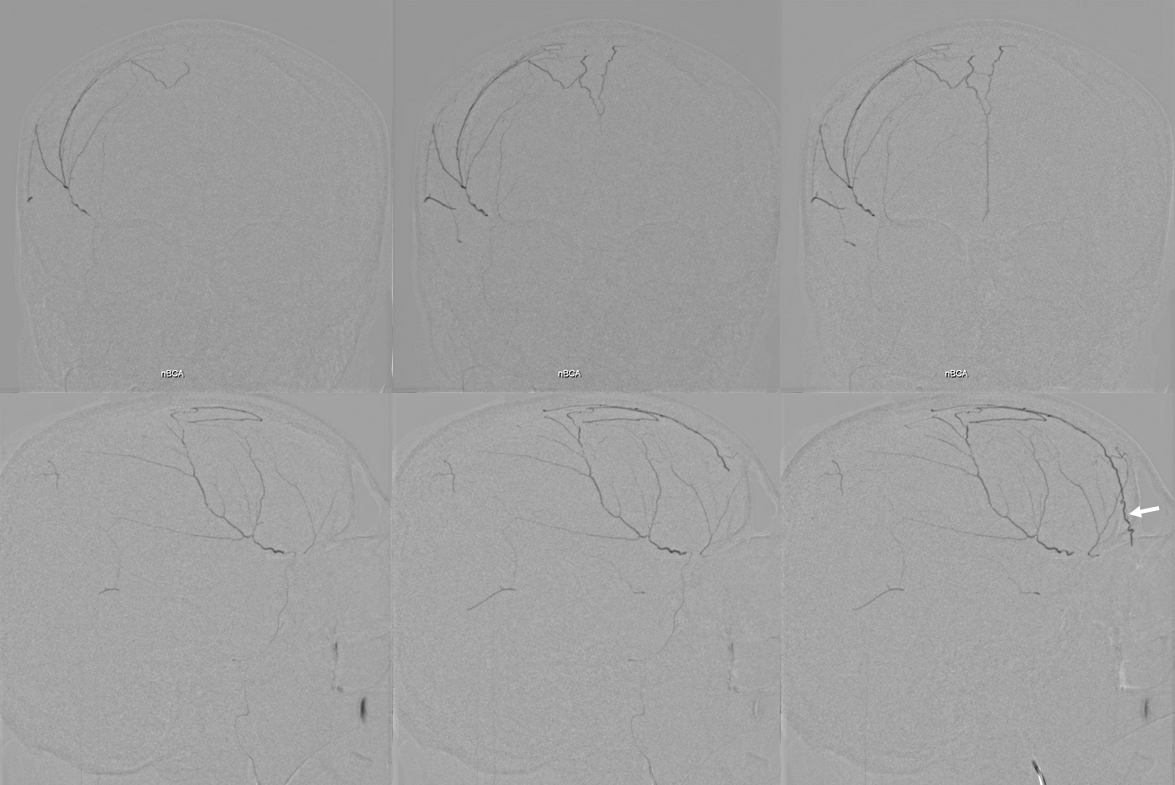
Dilute nBCA:lipidol (1:4) injection — notice, in addition to desired filling of the SSS collateral network and penetration to the left, a frequenly seen major glue filling of the anterior meningeal artery (arrow). This of course is connected, via ethmoidal arteries, to the ophthalmic artery system, and should be watched carefully. However, it is also important to fill this branch so as to shut down this major collateral reconstitution route to the target left dural convexity
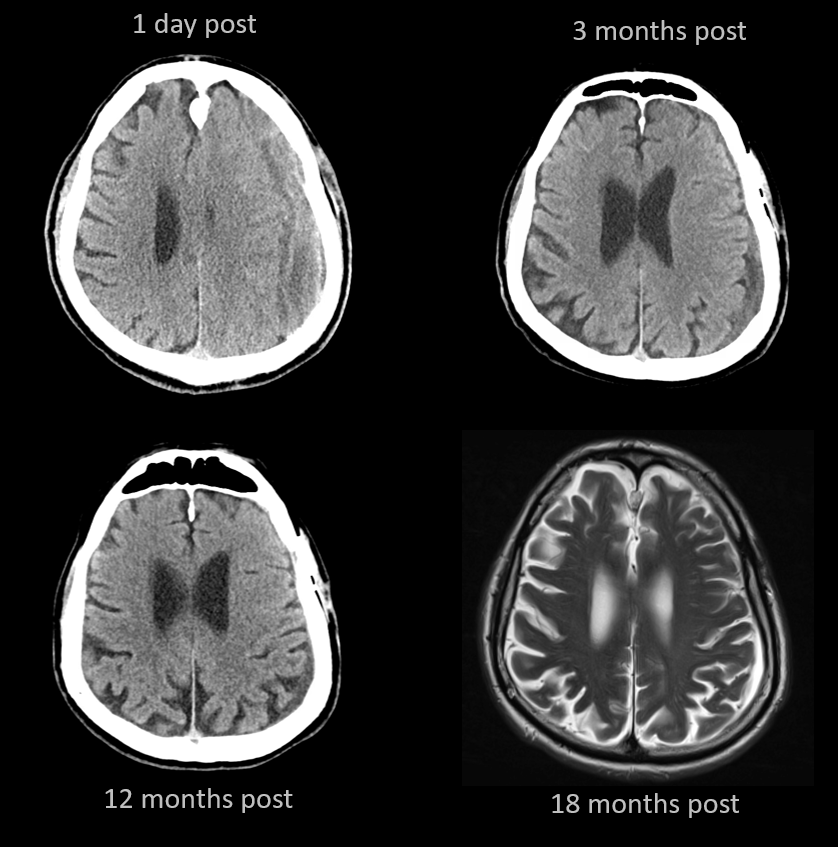
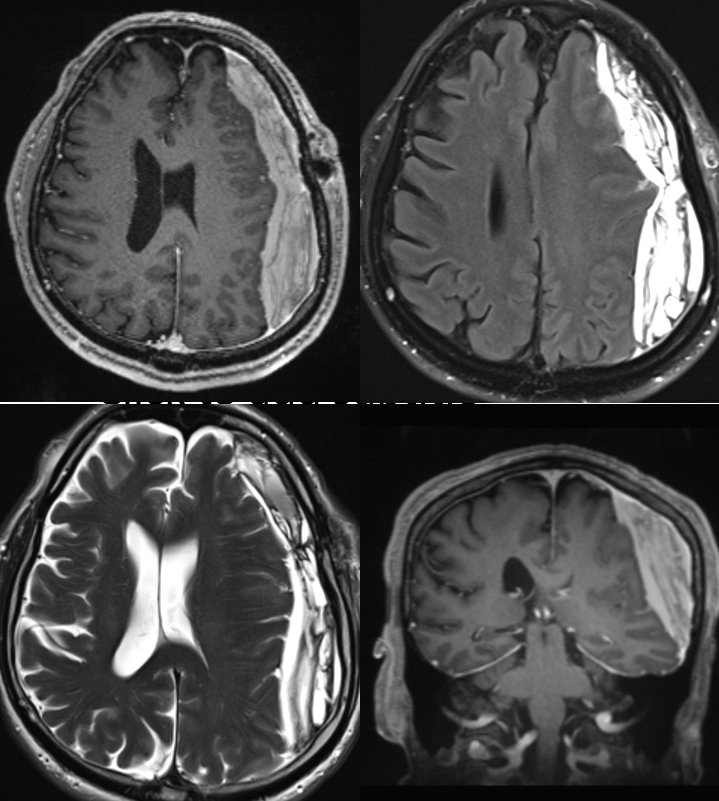
Sequential post-embo images show successful resolution of the hematoma