
The following presentation of venous anatomy draws on an extensive database of stereoscopic projections obtained for purposes of stereotactic surgical planning. The credit for this goes to now retired NYU neurosurgery chairman Dr. Patrick Kelly, a pioneer in the field of stereotactic neurosurgery. Additional cases are drawn from a large NYU database, the credit for which goes primarily to Dr. Peter Kim Nelson and Dr. Tibor Becske.
Our understanding of venous embryology is based primarily on the lifetime works of Dorcas Padget (see dedicated venous embryology section).

Credit for pioneering the study of in vivo venous anatomy primarily belongs to Dr. Yun Peng Huang, many of whose images form part of this collection. Finally, a uniquely neurosurgical perspective, including dedication to stereo imaging, is provided by Dr. Alfred Rhoton

Veins are pretty sizable project. It’s a little disrespectful to lump it all together into “brain veins”. But to separate them into compartments is even worse, as everything is interconnected and subdivision is more disruptive than helpful. So we’ll start with the classic “deep” and “superficial model” and deviate from there.
Important notes on angiographic study of the veins:
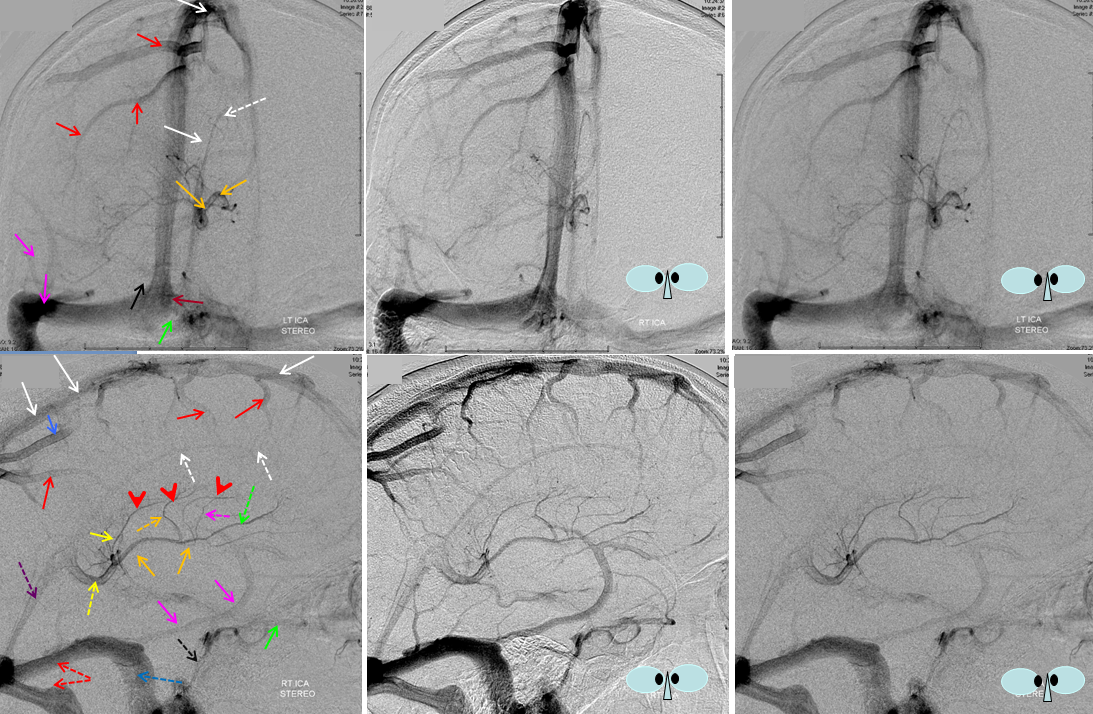
First, you only see the vein whose drainage territory is injected. Obvious but often ignored fact — if the A1 segment is hypoplastic, then an ipsilateral ICA injection will not demonstrate venous territory subserved by the ACA. Conversely, contralateral ICA injection may show bilateral venous homologs. An occluded ICA — you may see both hemispheres from a contralateral injection. You get the idea — always look at the arterial phase when analyzing veins. Here is an illustration of this concept.
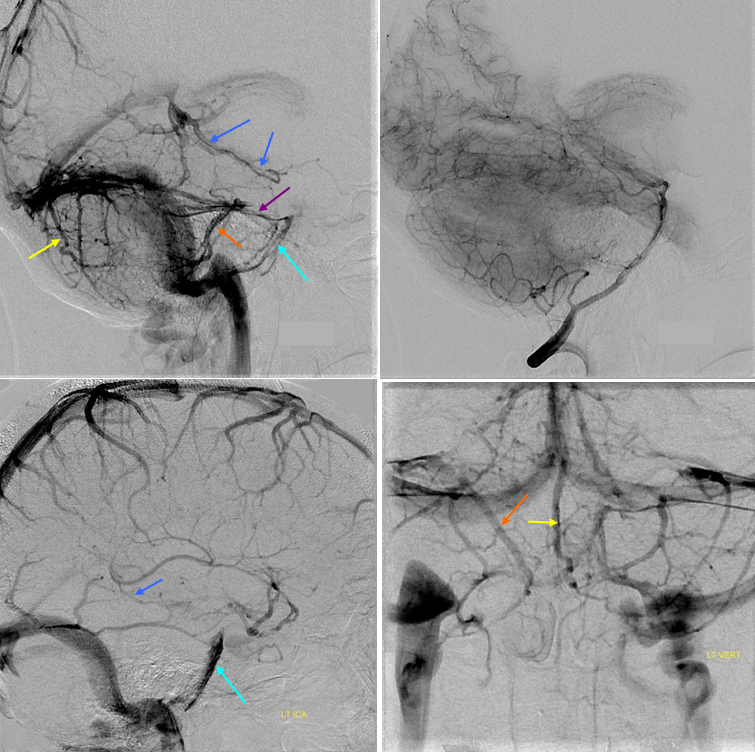
Top two images of left vertebral artery injection demonstrate a large basal vein of Rosenthal (dark blue). The same vein appears much smaller in caliber on the ICA (bottom left) injection, since the anterior segment of the basal vein drains primarily into the sylvian network. Notice also presence of the superior petrosal sinus (purple) on the vertebral injection. It is not opacified on the ICA injection and therefore may erroneously be presumed absent. The inferior petrosal sinus (blue) is well seen on both injections. Superior vermian vein (yellow). Ignore orange..
Here is another example: the right vertebral injection transiently fills the left PICA, yet insufficiently to see the left vermian vein (V, top row). Rather than concluding that the vermian vein is unpaired, one should either inject the left vert or allow for sufficient reflux into it from the VB junction to adequately fill the PICA territory. In the follow-up angiogram (bottom row) the left vertebral was injected with sufficient reflux to see both well-developed inferior vermian veins:

Second, veins are opacified in sequence. Look at the whole study before you decide that a given vein does not exist. The “superficial” — meaning surface — veins are generally seen first. This includes the basal vein, which is in effect a superficial (surface) vein that happens to be on the bottom of the brain. From here, contrast progresses into the venous sinuses, which are usually opacified well about 1-1.5 seconds after the superficial cortical veins. Anterior frontal, mid-frontal, and temporal convexity surface veins may be seen just a touch earlier than posterior frontal and parietal ones, just as the “shorter” arteries to the frontal lobe are vialized before those of the far parietal convexity. So, from a technical standpoint, contrast material reaches the posterior frontal and parietal ARTERIES just a touch later than frontal and temporal ones, because of the longer length of MCA branches to those regions, and so the veins may in turn opacified a little later (less than 0.5 seconds later, to be exact). The sequence of deep vein opacification is more complex — the earliest tributaries of the internal cerebral vein (such as septal veins) are seen as early as the cortical surface veins. The caudate veins (lateral group of internal cerebral tributaries) come in late and stay EXTREMELY late into the venous phase, even after contrast has washed out of the dural sinuses. DVAs are generally LATE as well, which is very convenient if you are looking for one angiographically next to that huge hematoma (be careful, however, as normal veins compressed by hematomas are going to be seen later than usual as well). All of this is as much as to say that you should study the venous sequence carefully in totally NORMAL patients, over and over again, as the only way to acquire the kind of visual memory you will need to decide on pathology.
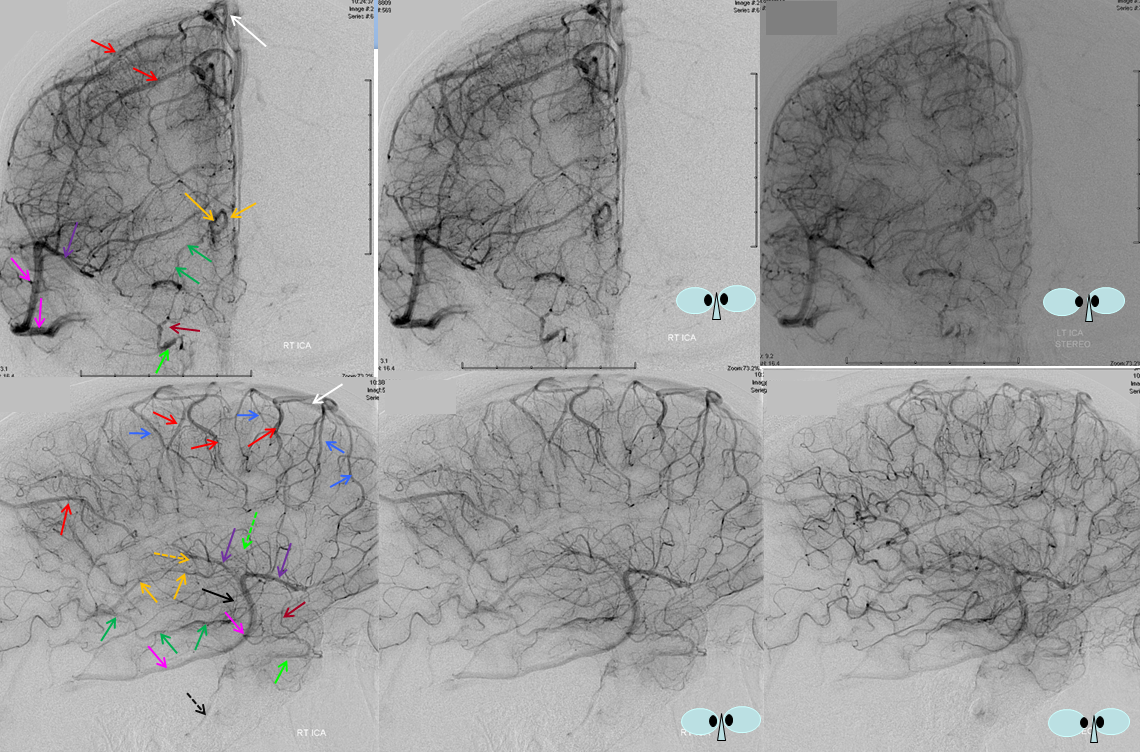
Early Venous Phase: Surface cortical veins are opacified early in the venous phase. The lateral (red) and medial (blue) superior hemisphere surface vessels are well seen, as is the superficial sylvian venous system (purple) draining into the inferior temporal vein (pink), which is the dominant venous drainage in this hemisphere. Part of the sagittal sinus is filled also (white). Inferior striate veins (brown) are, in this case, draining towards the sphenoparietal sinus (green) and subsequently into the inferior petrosal sinus (dashed black). The basal vein (a surface vein, practially, but a deep vein surgically) is also visible (green), with relatively small contribution from deep sylvian (insular) veins (black). Although dominated by cortical surface vessels, the internal cerebral vein (light orange) is already visible on early venous phases, with its anterior septal (dashed green) and thalamostriate veins (dashed light orange).
This phase is useful for evaluation of “shunting”, or premature opacification of the venous system. High flow shunts, such as AVMs, will appear in the arterial or capillary phases. Low flow shunts, however, may be best seen in late capillary or early venous phases as a region of especially good venous filling in comparison with the rest of the territory. This is a more subtle type of shunting, caused by tumors, inflammatory lesions, etc.
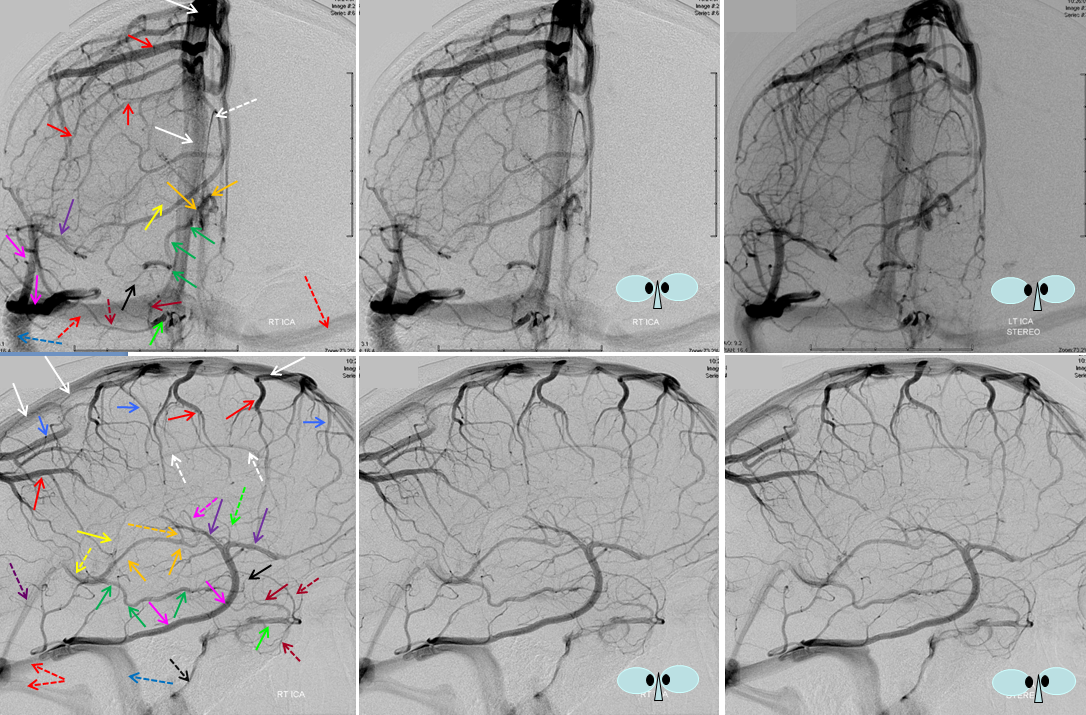
Mid-venous phase: Best phase of overall picture, where you can see veins and dural sinuses well (only lateral ventricular veins and dural sinuses are better seen in late phase). Medial (blue) and lateral (red) cortical surface vessels are well seen, as well as the dominaint superficial sylivan system (purple) draining into the inferior temporal vein (pink). The temporal pole veins (dashed brown) and striate veins (brown) are draining into the sphenoparietal sinus (green) — somewhat unusual pattern, but everyone has variations, and I purposefully did not want to put in a “classic” case. Basal vein (dark green) is well seen, in its classical aspect, with deep sylvian tributaries (black). The internal cerebral vein (light orange) is also visualized well, with anterior septal (dashed green) and thalamostriate tributaries (dashed pink and dashed orange), as well as direct lateral tributary (yellow).
The more downstream venous channels (dural sinus veins) are now visualized — the superior (white) and inferior (dashed white) sagittal sinuses, the Vein of Galen (dashed yellow) and straight sinus (dashed purple), and transverse (dashed red) and sigmoid (dashed blue) sinuses, as well as the inferior petrosal sinus (dashed black). The superior petrosal and cavernous sinus are not seen — which is not to say absent. They may be visualized from vertebral or external carotid injections (which visualizes the cavernous sinus through the ophthalmic veins) and the superior petrosal sinus through cerebellar and brainstem (lateral medullary, for example)veins.
Late Venous Phase: Very useful for visualization of the internal cerebral vein and distal parts of the dural sinuses. As you can see, tributaries of internal cerebral vein (orange) continue to drain contrast when most other brain veins are not longer visualized. The late veins consist of basal ganglia structures, such as the thalamostriate vein (in this case there are two closely spaced veins [dashed orange and dashed pink] which drain the region normally assumed by a single thalamostriate vein, another anatomical variant),as well as the direct lateral vein (yellow) and anterior caudate vein (dashed green). The superior aspect of these veins (red arrowheads) outlines the body of the caudate, which is classically collected by the longitudinal caudate vein — in this case the region is drained by several discontiguous veins. The venous sinuses are also well seen, as well as the Vein of Galen (dashed yellow). Even later phase can be imaged with still persisting internal cerebral vein. Of note, DVAs often stay late in venous phase as well, and their presence can be looked for on the late phase images.
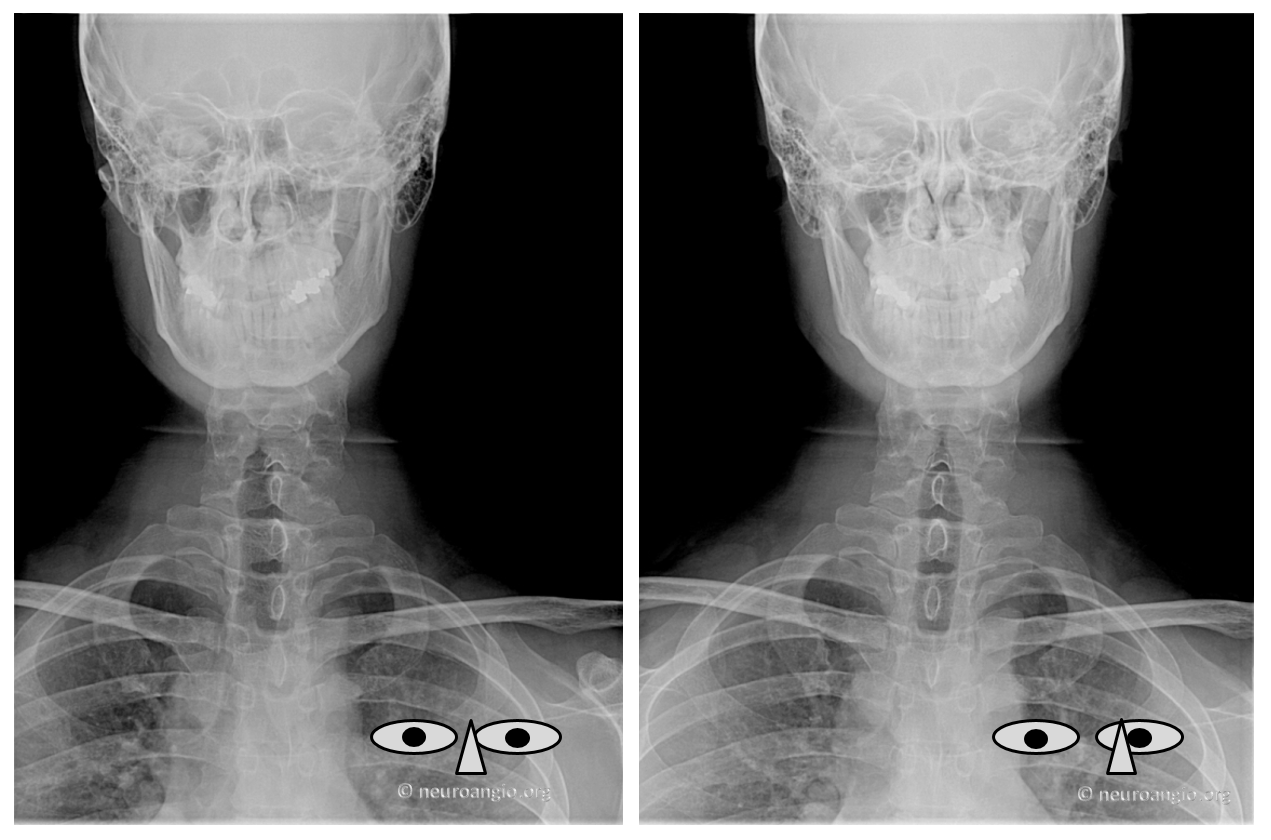
Third, I highly suggest learning to view veins in stereo, if you can. The venous apparatus, particularly deep vs. superficial components, is stunningly clear when viewed in stereo. Most of the illustrations here can be viewed in stereo (crossed viewing method), either by crossing your eyes or by wearing prism glasses made to that effect. From a technical standpoint, stereo projections are acquired by rotating the camera head along the craniocaudal axis (which would be parallel to the ground and in line with your eyes while looking at the standing patient) by 6 degrees or so, while keeping everything else constant.
Learning to view in stereo is a separate subject, which can be readily accessed by googling (or otherwise searching) the internet. Essentially, the idea is to cross your eyes so that the picture on the left ends up on the right, and vice versa. Then, slowly “relax” your eyes so that the magnitude of “crossing” is gradually diminished, allowing the pictures to drift closer together and finally to “fuse” in your mind. At point of fusion, stereo effect will be suddenly manifested, to your certain amazement. Learning to “cross” your eyes is the more difficult part. “Relaxing” will take care of itself, as the eyes will get tired and drift to their natural uncrossed stations. Headaches are guaranteed during the learning process. I suggest learning stereo viewing on pictures of familiar objects rather than veins — your brain already knows what to expect the stereo to look like. http://www.lhup.edu/~dsimanek/3d/stereo/3dgallery.htm has an incredible amount of all kinds of stereo pictures for you to practice on. http://en.wikipedia.org/wiki/Stereoscopy is more of a general overview, and will appeal to those who have the need/desire to understand the optics underlying the process. Having said all that, about 10% of people (as far as I know) can not train their eyes to view in stereo (perhaps due to an underlying amblyopia, or various forms of mild/functional diplopias). You can try purchasing prism glasses which do the eye crossing for you, but results are not guaranteed (depending on the underlying reason for the issue). Here is a representative stereo photo from ihup.edu — very nice one for practice
Stereo imaging was known long before development of angiography. It found value in early work of pioneers, such as Yung Peng Huang, M.D. A stereoscopic specimen from his collection, highlighting the medullary veins, is shown here:
The following links will take you to the next sections in the venous anatomy division — dedicated to Venous Sinuses, Superficial Venous System, Deep Venous System, and Posterior Fossa Veins, which are treated separately.

A stereo movie of lateral angiographic injection in a patient with a small frontal DVA.
Finally, there is much going on in world of 3D flat panel imaging. Here are some examples. You can pause movies and scroll through individual images

Enjoy the show
Retro view
