


The best way to understand internal cerebral vein anatomy (and, actually, any venous anatomy) is to:
1 — study how the same veins appear on cross-sectional imaging and angiography. In particular it is important to understand the ventricles
2 — understand the concept of concentric rings (see below) and balance between deep and superficial venous systems
Most existing diagrams of internal cerebral vein anatomy are based on angiographic material. However, at this point cross-sectional imaging is, in author’s opinion, a better way to study this system. So, just take some good quality angiograms and corresponding venously contaminated CTAs or susceptibility-weighted MRIs and look at them together. You’ll make very quick progress.
No basal vein here
There is debate as to whether the Basal Vein is really a deep vein or not. Embryologically, functionally, etc. It is certainly deep as far as surgery is concerned. But in every other respect it is not. It lies on the undersurface of the brain, not deep inside, like the internal cerebral vein. Embryologically, is one of the last veins to form while the internal cerebral system system is the first. Functionally, as a conduit between the Galen and cavernous sinus, it has rich anastomoses. The internal cerebral vein is by far the least interconnected system — it has practically no collateral option. When occluded by thrombosis the consequences are usually devastating. Bottom line is that the internal cerebral venous system is truly the deep venous one.
How to understand the internal cerebral vein and its tributaries? Understand the anatomy/shape of the lateral and third ventricles. The rest is easy. Why? Because it is a subependymal system. Embryologically, the internal cerebral venous system forms very early. This makes sense, as the ventricular system and associated deep structures are developed well before the cortex. There is detailed information on this in the Venous Embryology page. Bottom line is that tributaries of internal cerebral vein drain structures adjacent to the ventricles, and so understanding ventricle anatomy is more than half the battle. To do that, use cross-sectional imaging
Medial/lateral groups
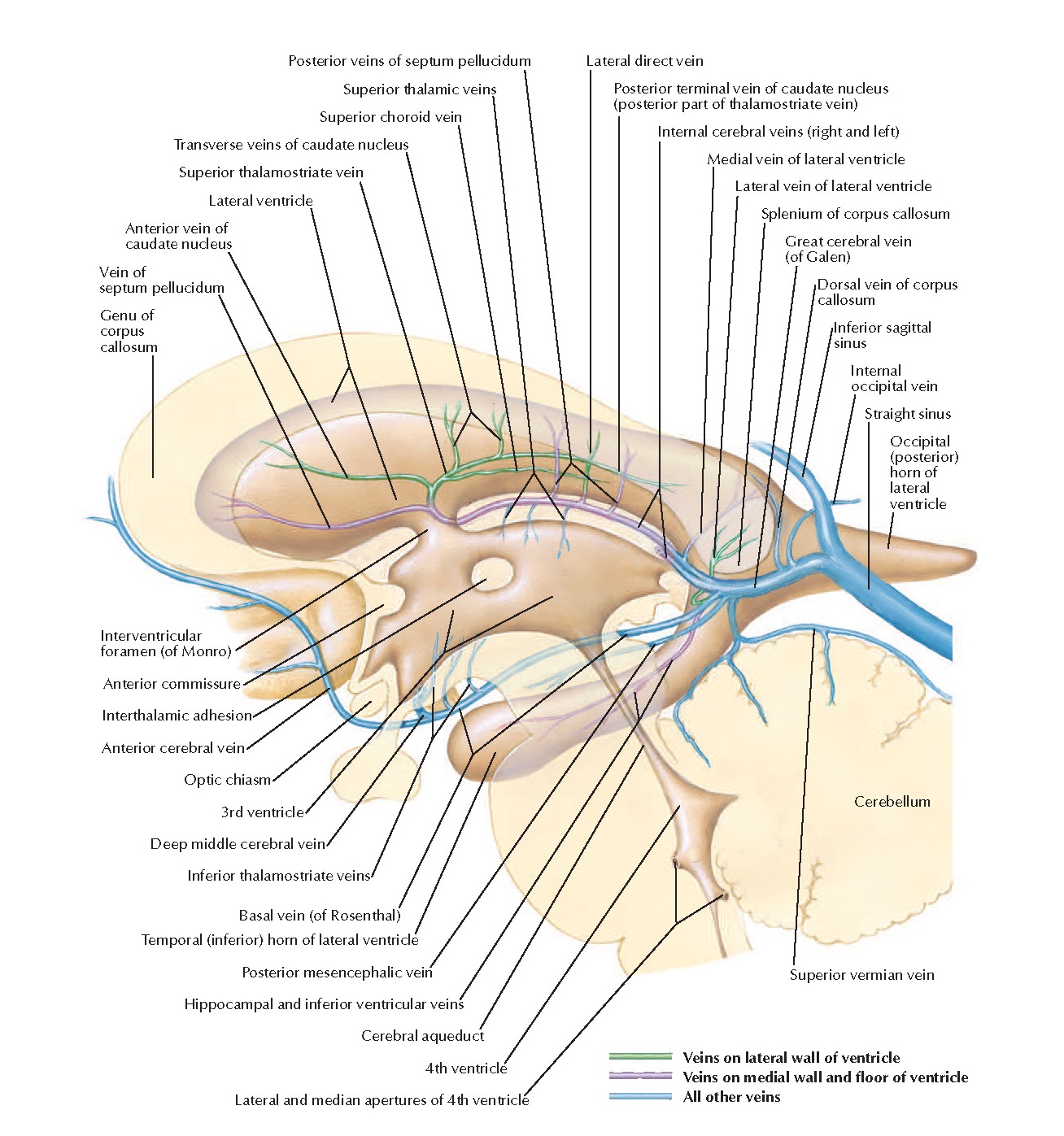
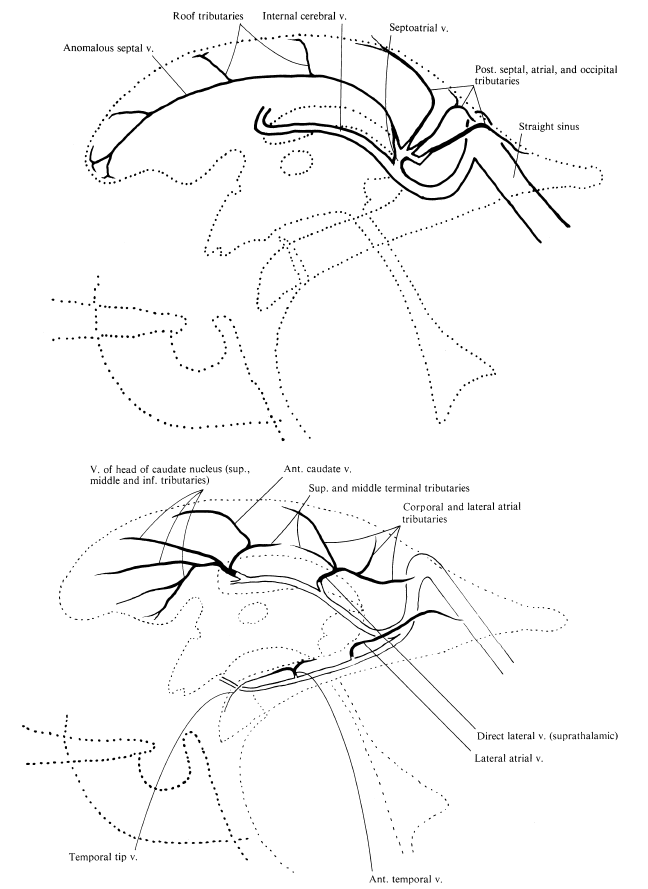
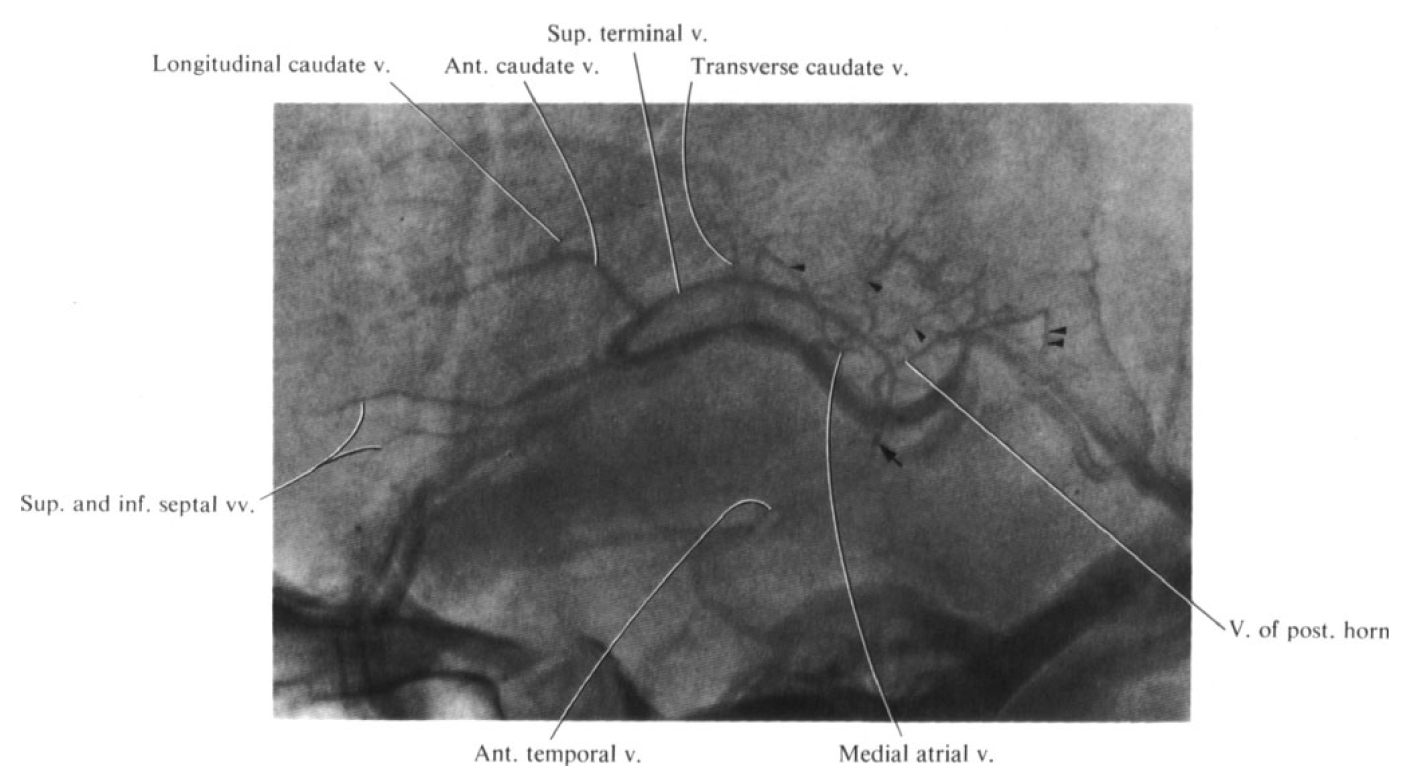
That’s the classic view, and it follows the ventricles. Everything medial to the lateral ventricles is medial group, lateral is lateral group. Easy. There is everything else, and then there is Frank Netter. This is one of Netters pictures that are worth thousands of words — still amazing.
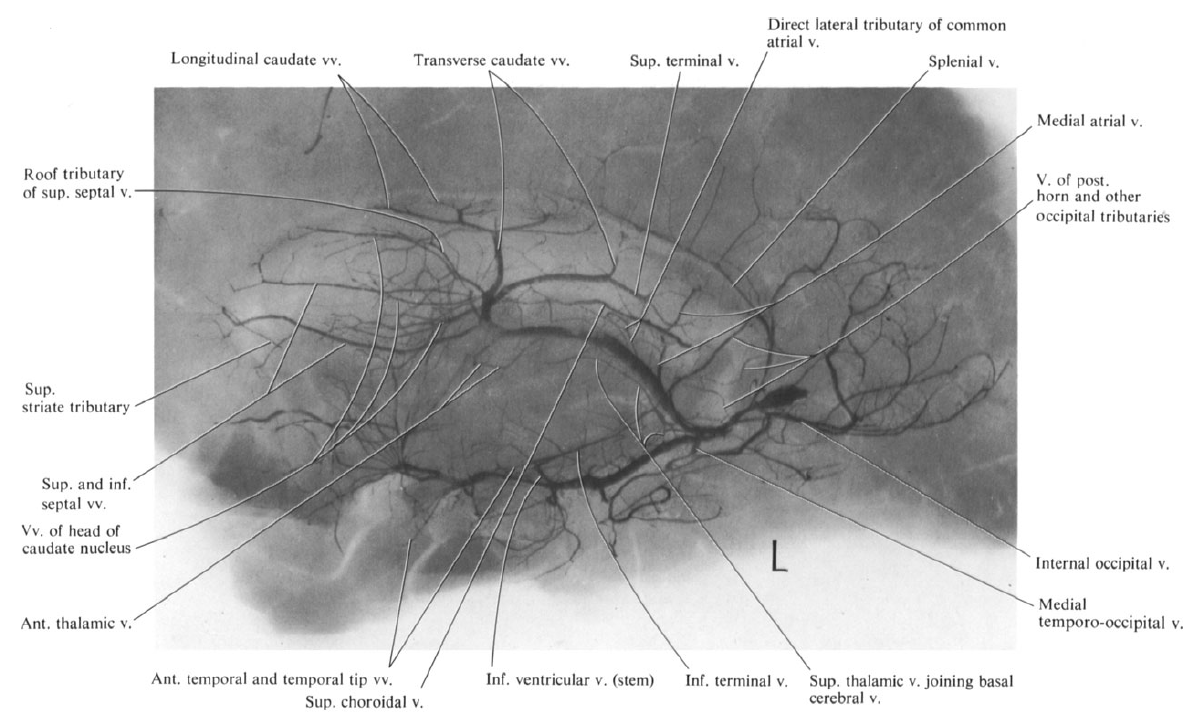
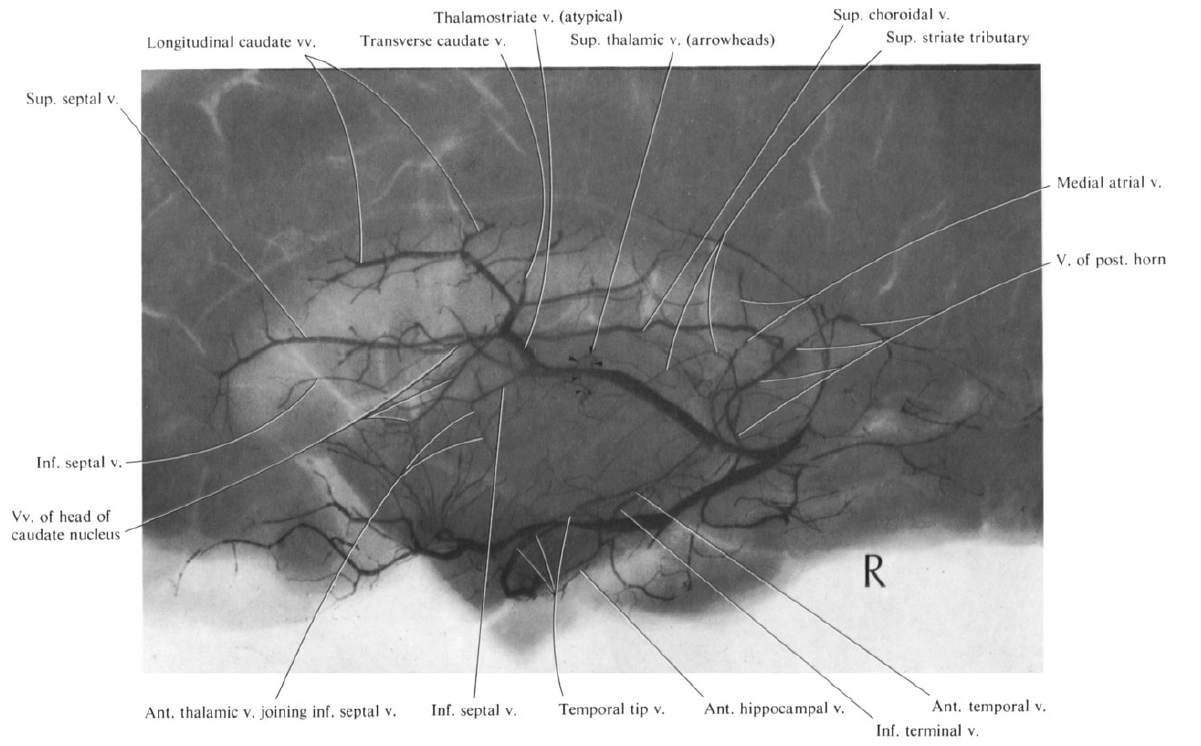
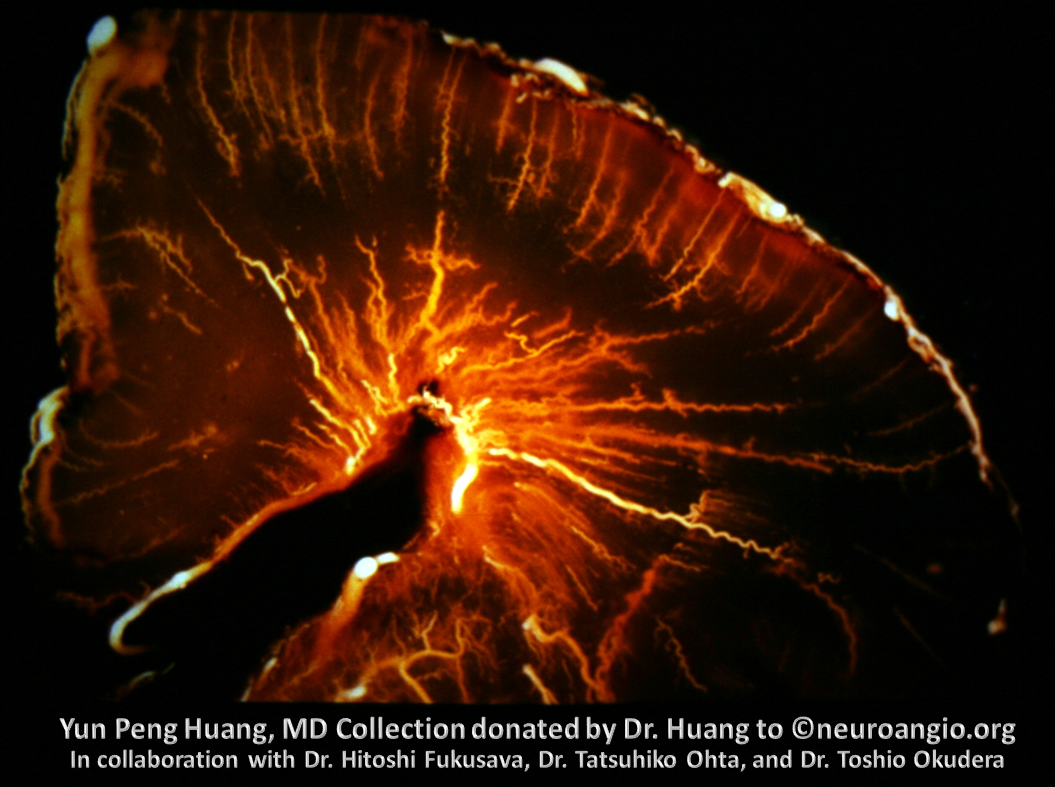
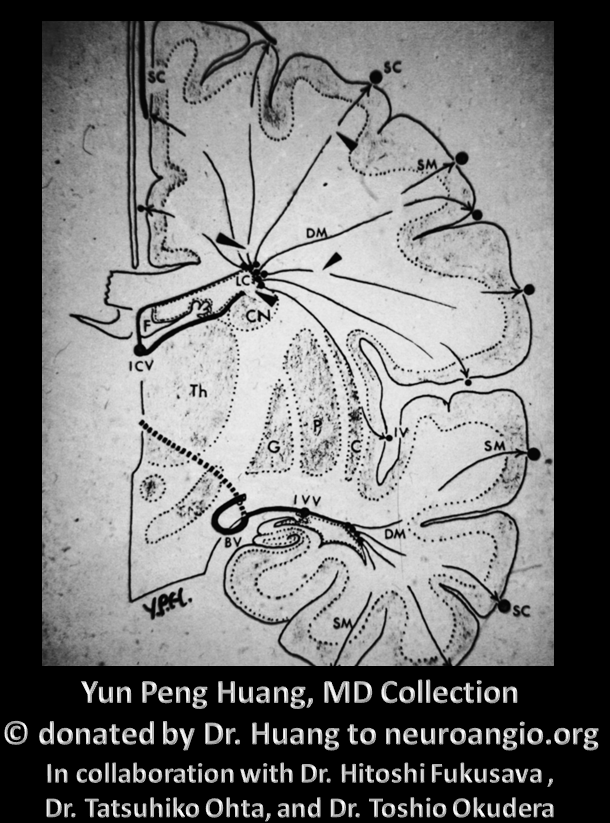
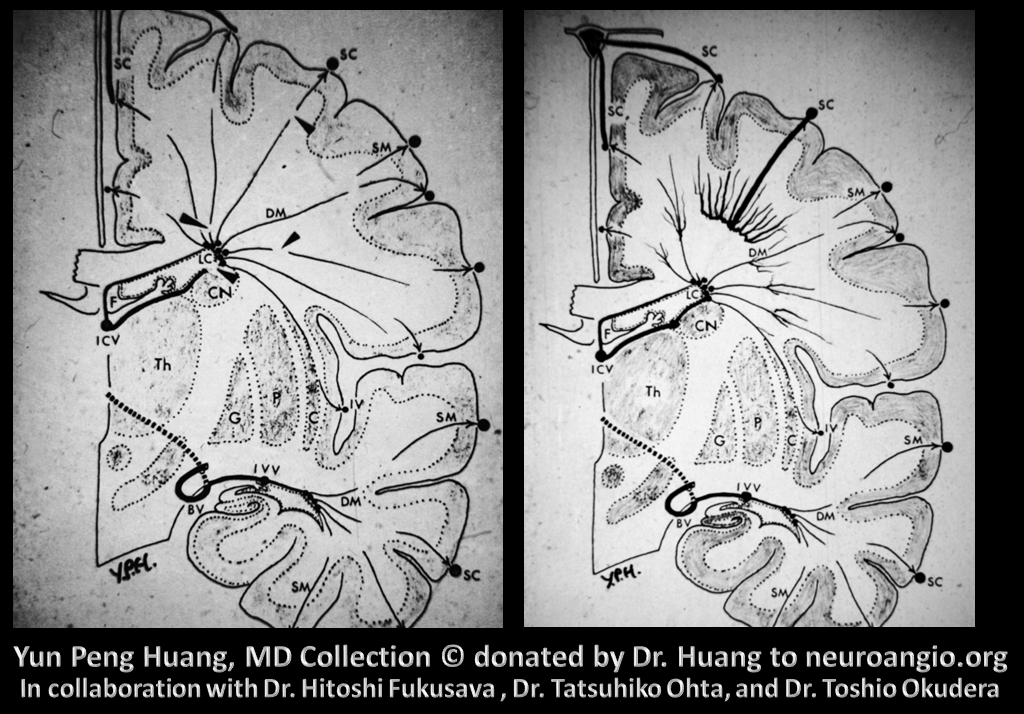
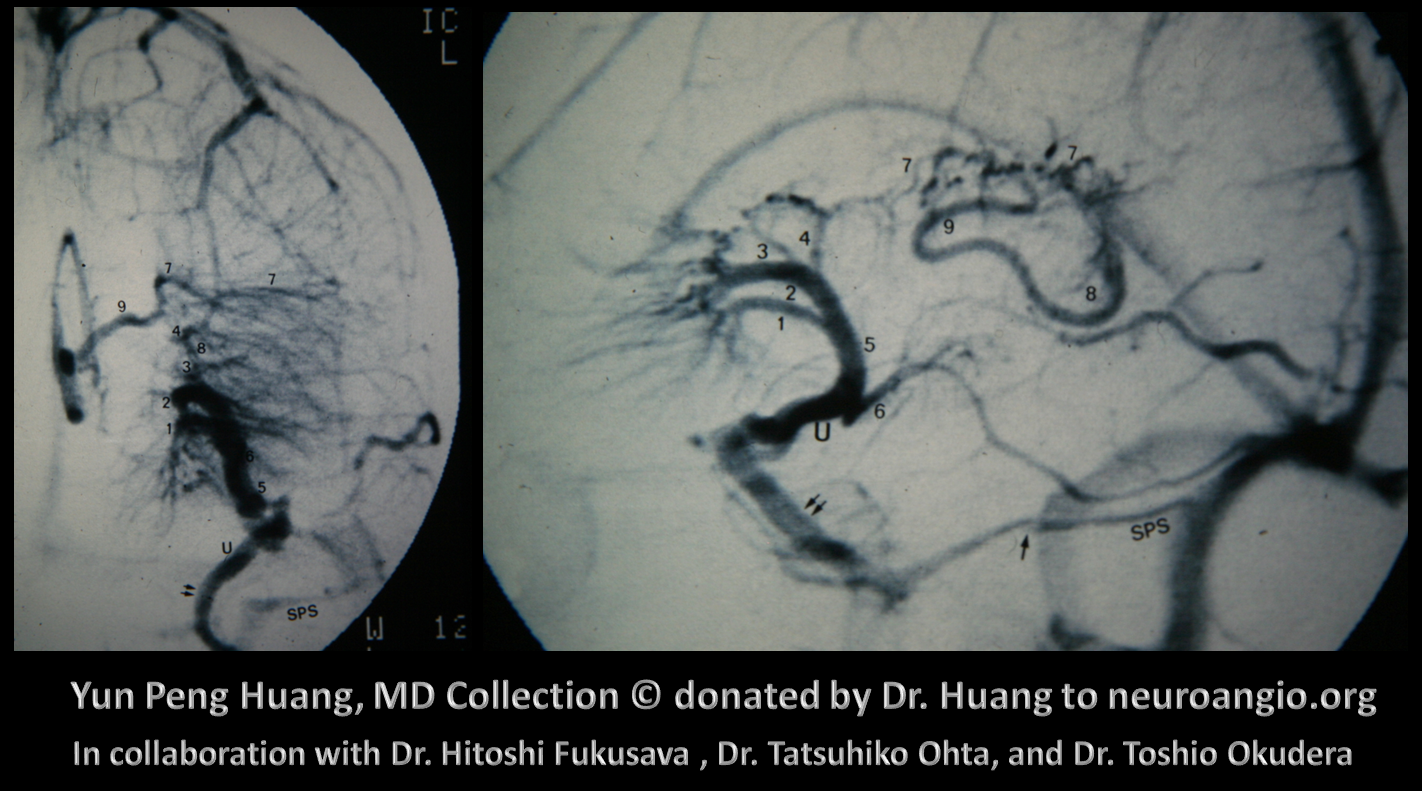
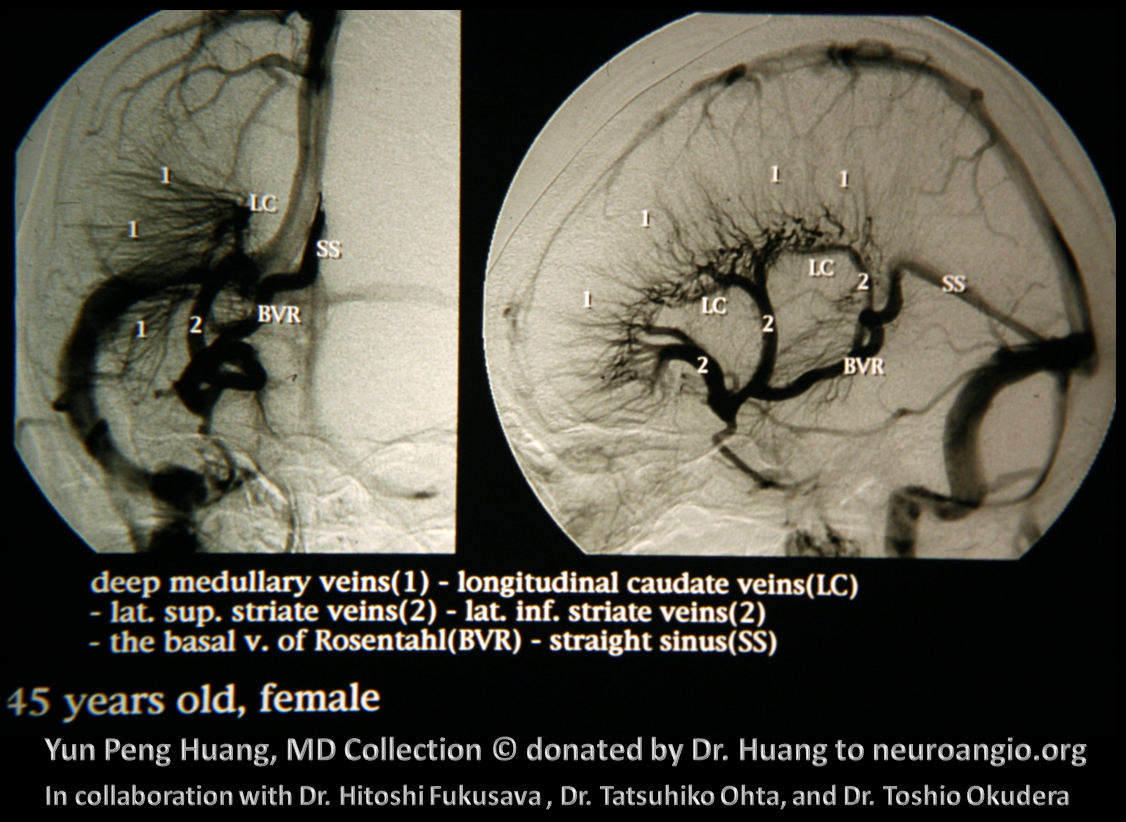
No venous talk can go without recognizing contributions of Yun Peng Huang and Okudera, whose lifetime of 35 mm Kodachromes were generously donated to neuroangio.org Before cross-sectional images, vascular angiographic anatomy and encephalography was pretty much all we had for noninvasive options. Veins more closely follow brain topography than arteries do. The best of Huang’s generation had knowledge of venous anatomy that is orders of magnitude above what is necessary now. They also generated amazing angiographic images, neither digital nor subtracted. If anyone is interested in learning this kind of stuff in-depth, Salamon and Y.P. Huang’s Radiologic Anatomy of the Brain is the way to go.
Here are a few of their images
Medial (top) and Lateral (bottom) groups
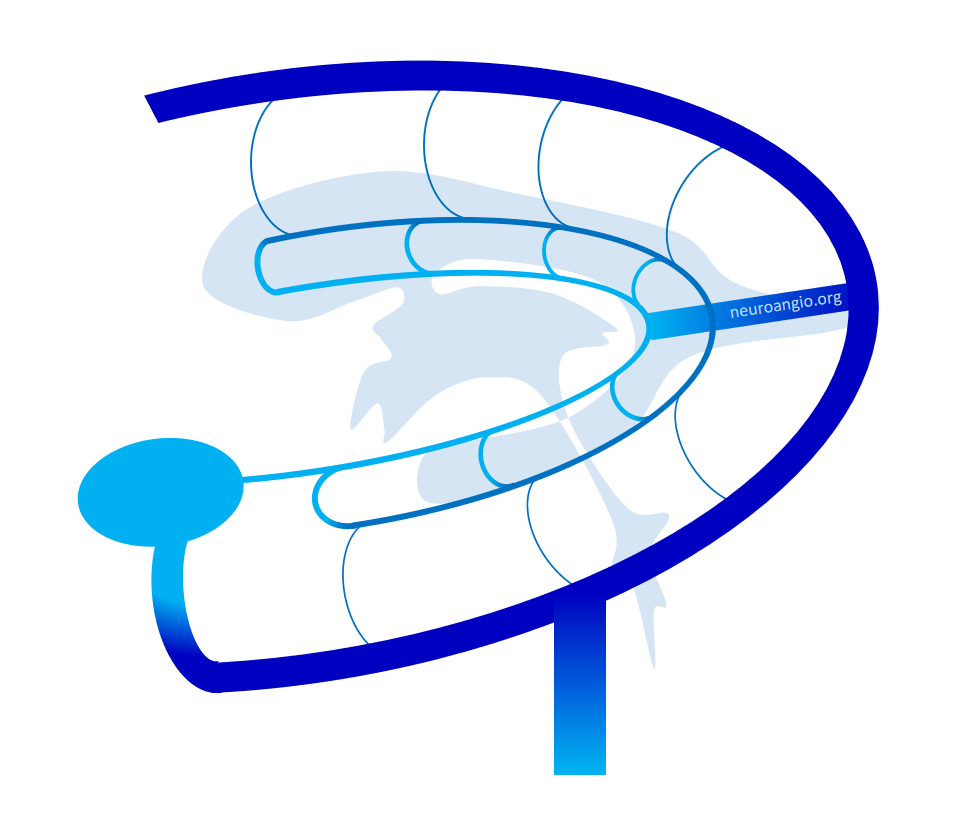
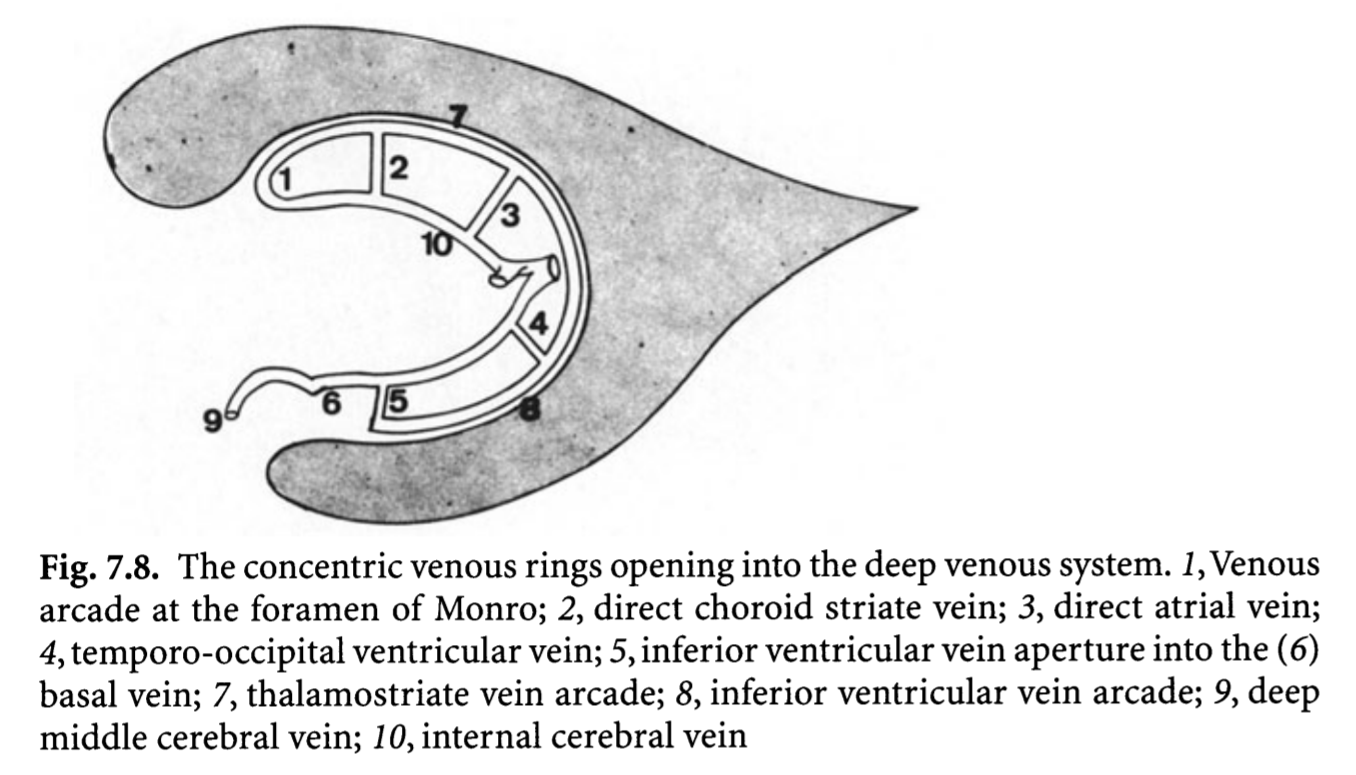
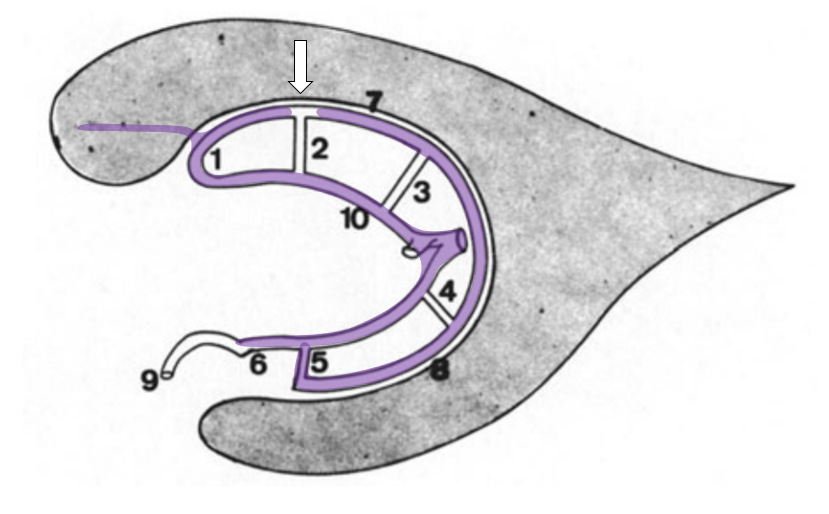
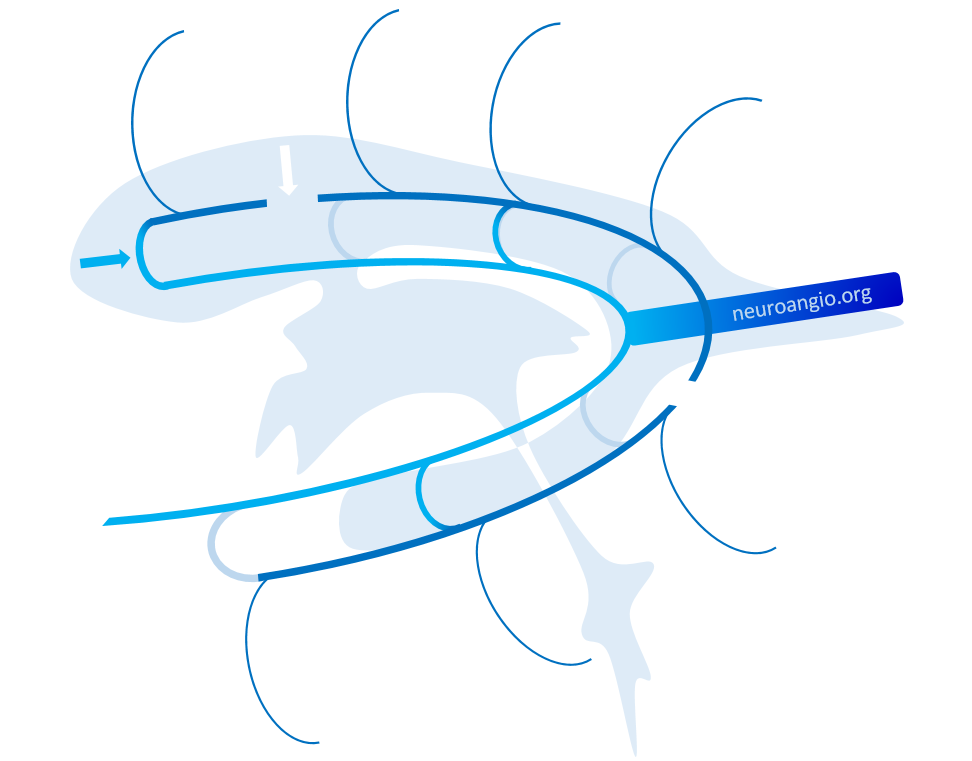
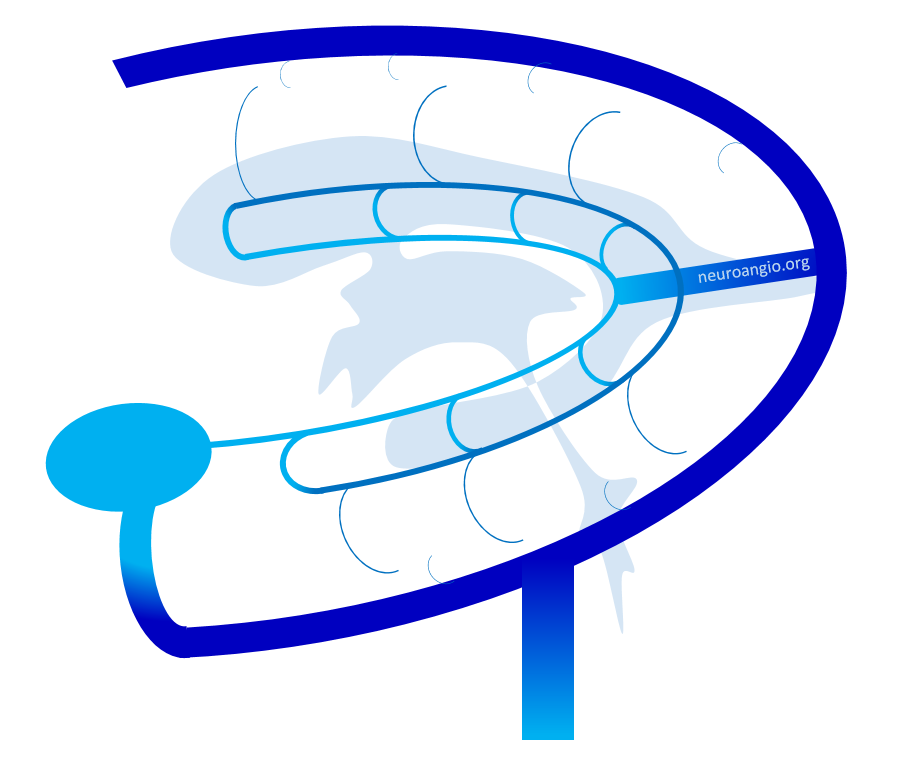
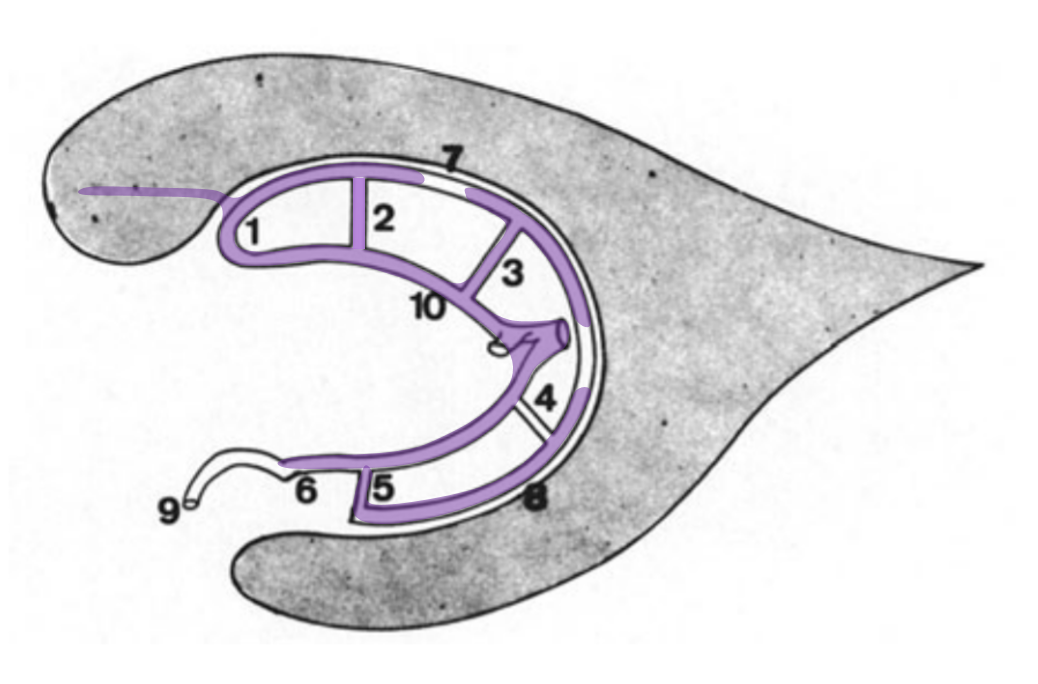
Another way — a GREAT way — to look at the internal cerebral system is Lasjaunias way. The concept is of inner and outer rings, shown below. You should know both. The idea is simple and powerful — the inner ring consists of internal cerebral and basal veins — the outer ring is made of longitudinal veins of the caudate and lateral ventricle. There are multiple connections between the rings. The rings are very useful in explaining variations, which are essentially interruptions of one of the rings, with venous flow rerouted via one of the connections someplace else. The image below is from page 639 of Surgical Neuroangiography 2nd edition. We will be using this concept a lot down below
The diagram above — and all neuroangio rings diagrams — are inspired by the above idea of Lasjaunias and Co.
Well, enough of words. Lets go to some real pictures now…
General Angiographic Concepts
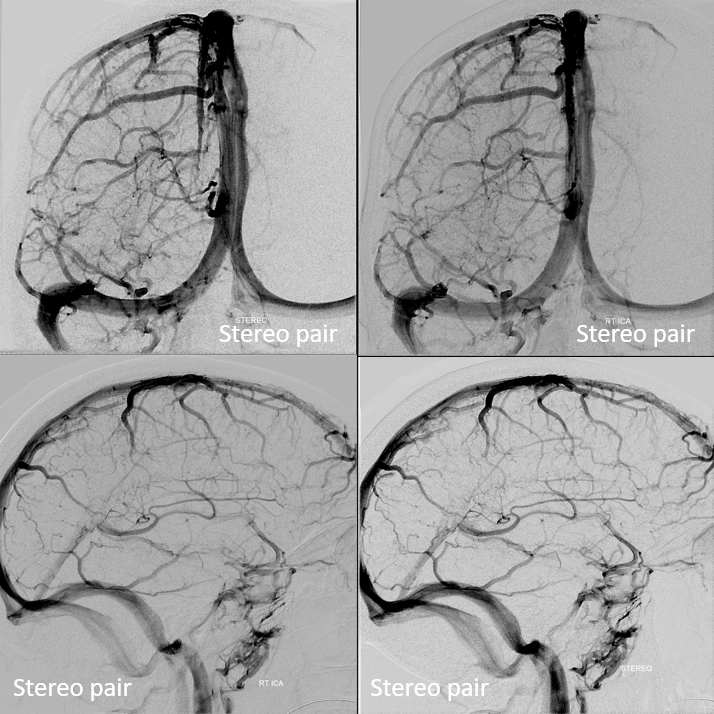
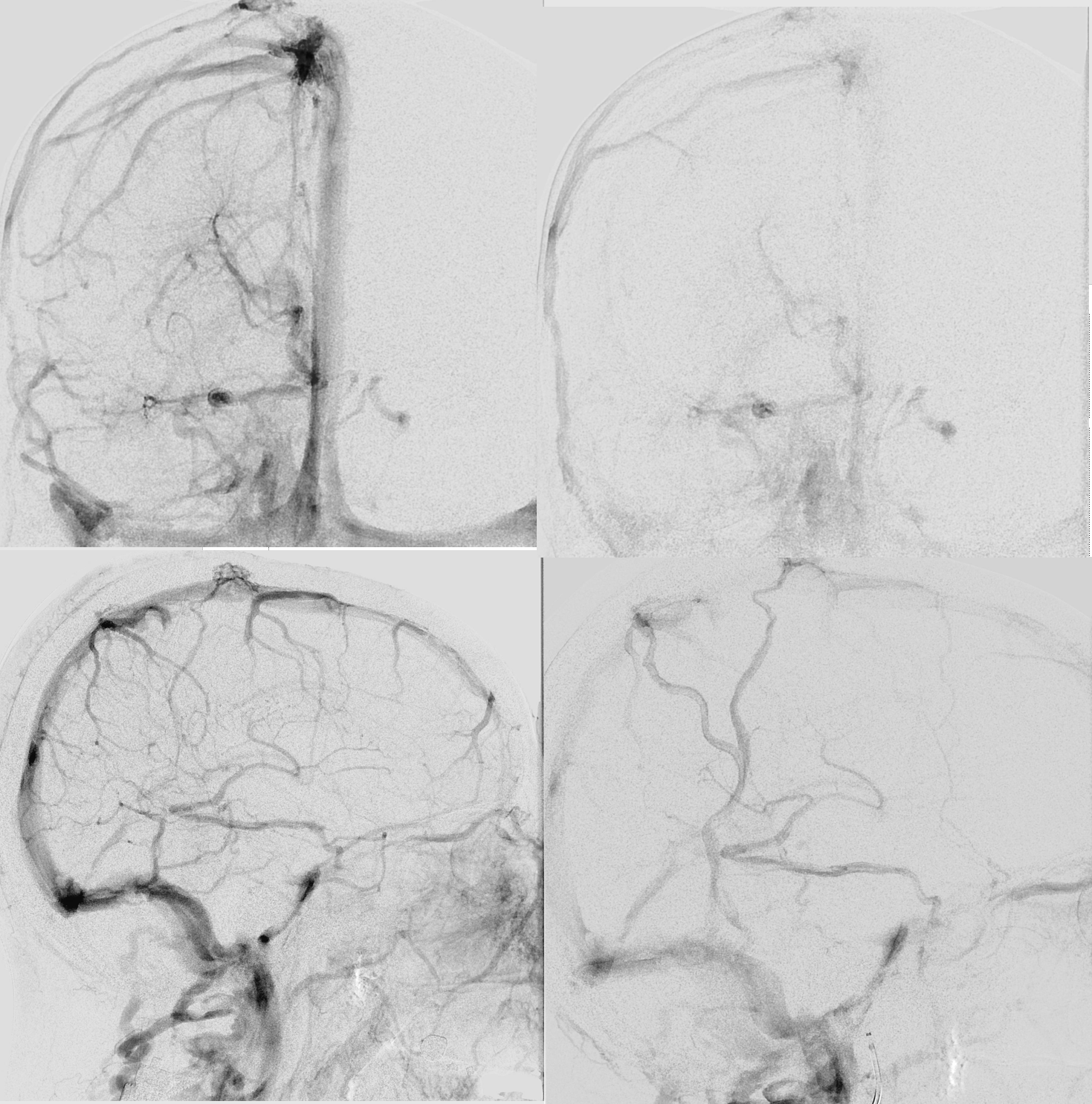
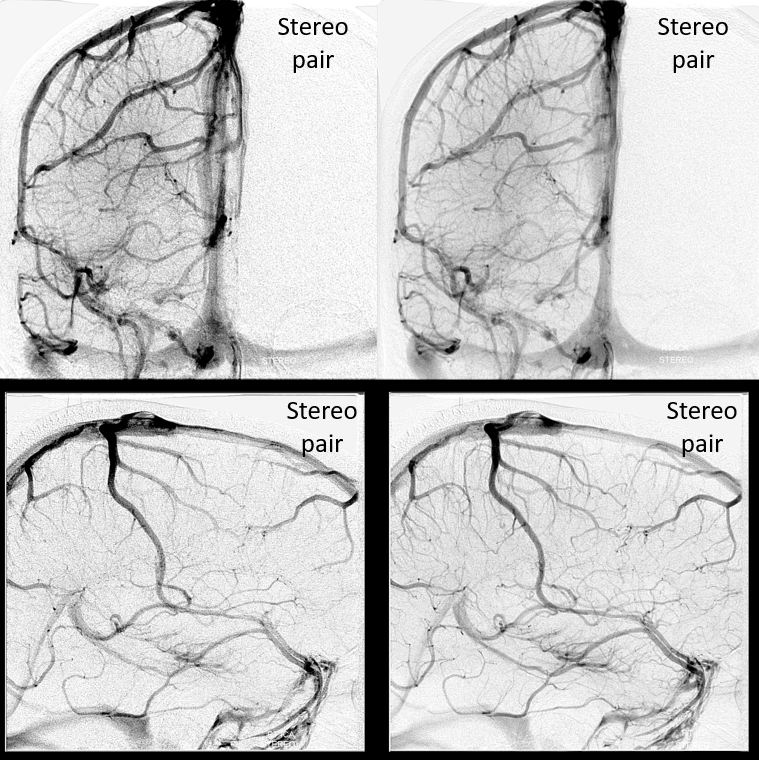
Late venous phase is best to see the internal cerebral vein in particular and periventricular/subependymal veins in general. They persist while other veins have washed out. Why? Answer is buried in the subsequent discussion — to encourage reading 🙂
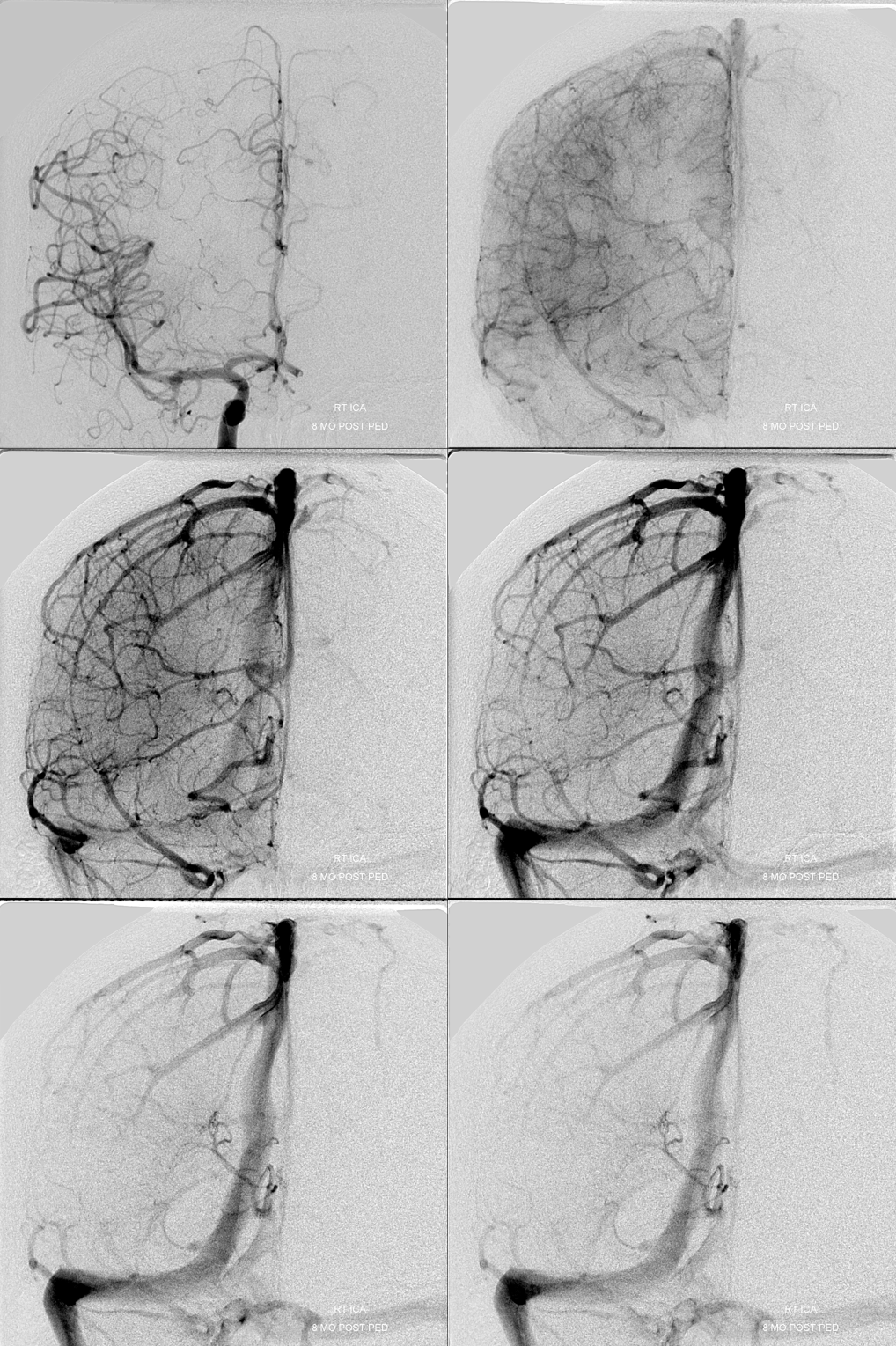
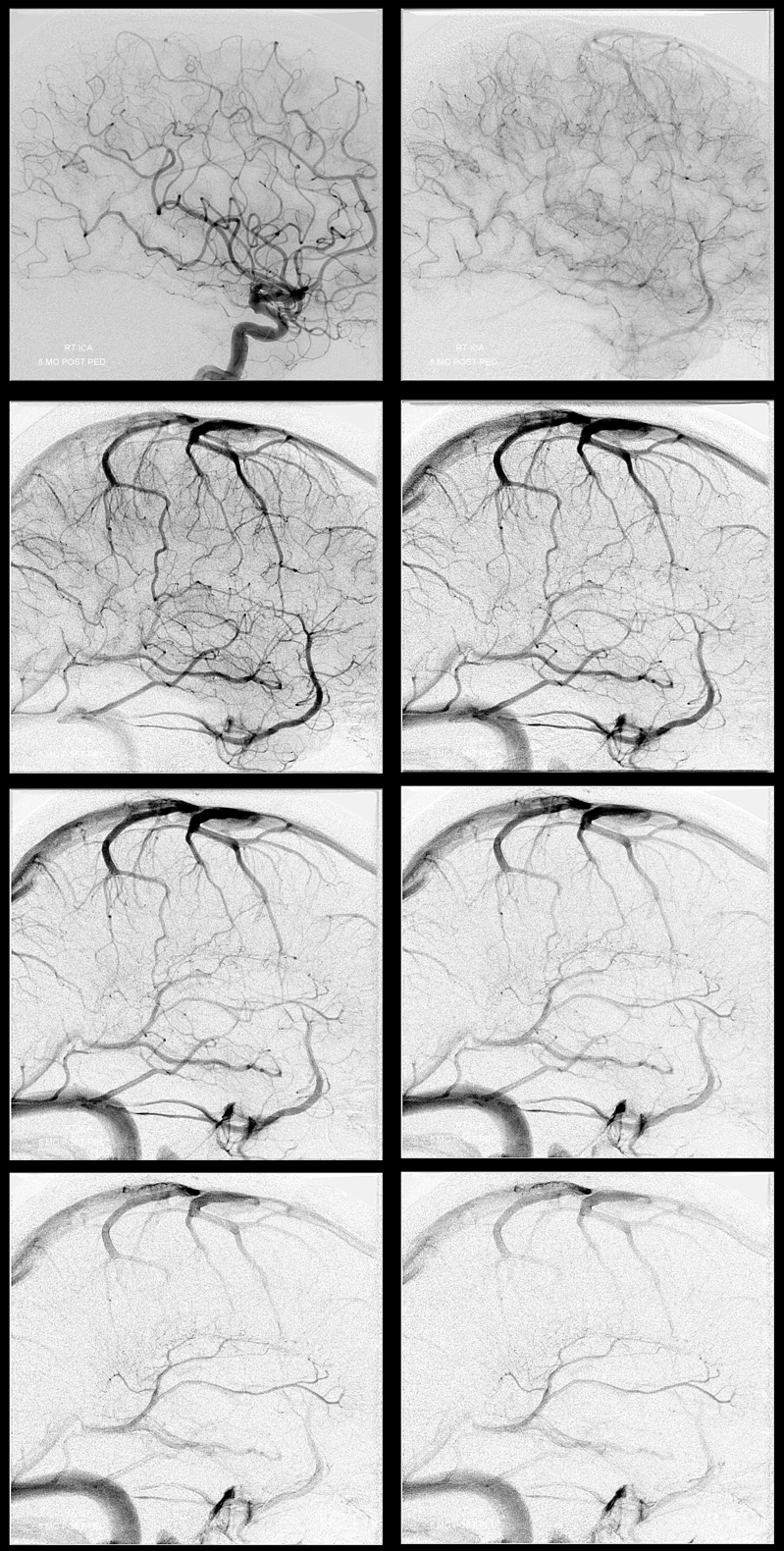
Late venous phase — notice how much better the deep veins are seen here.
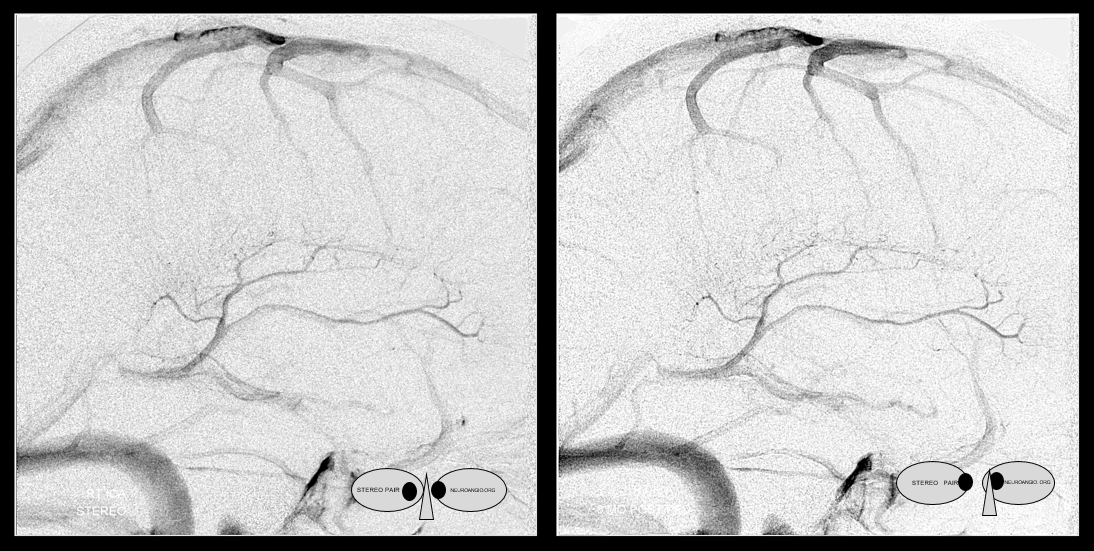
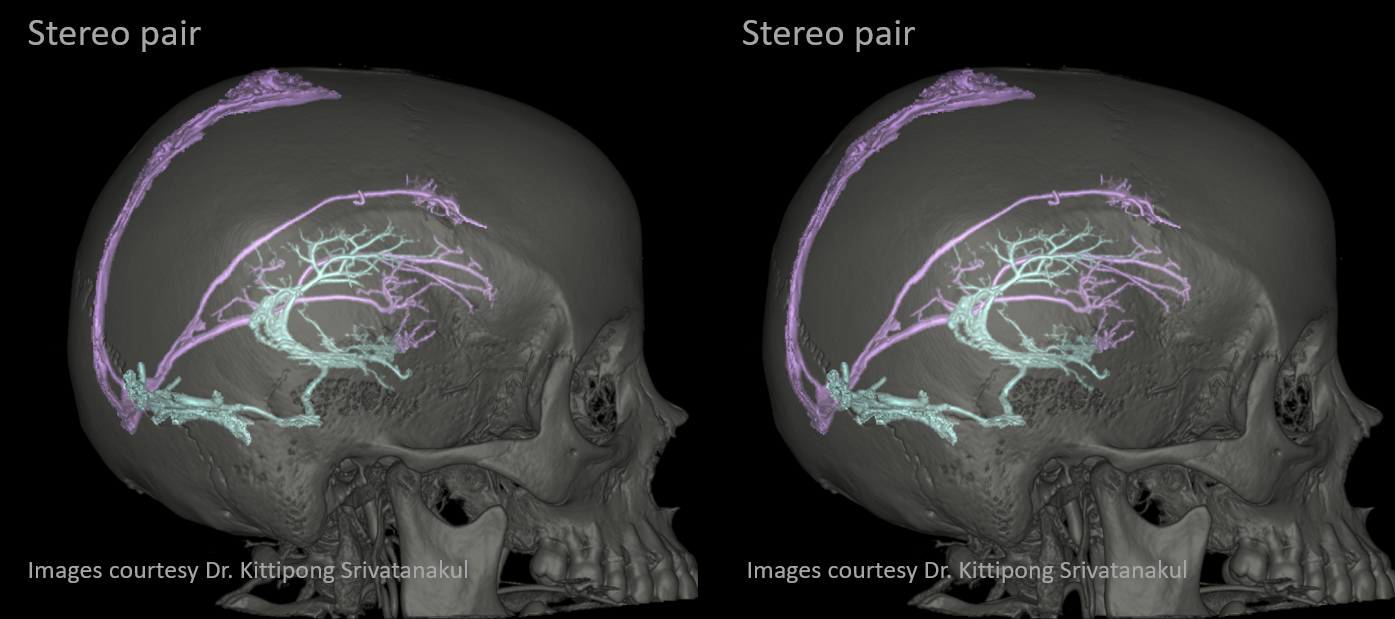
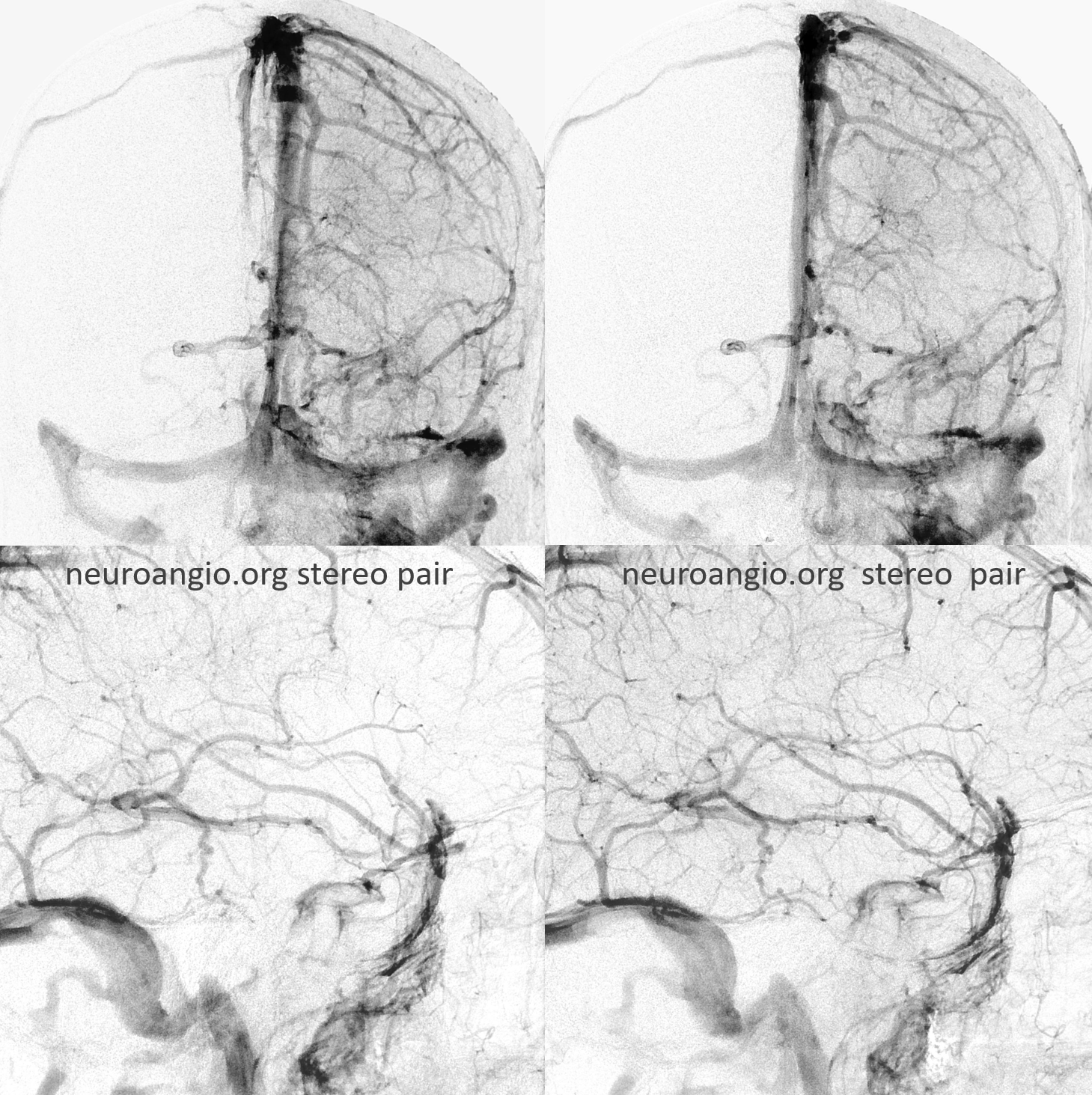
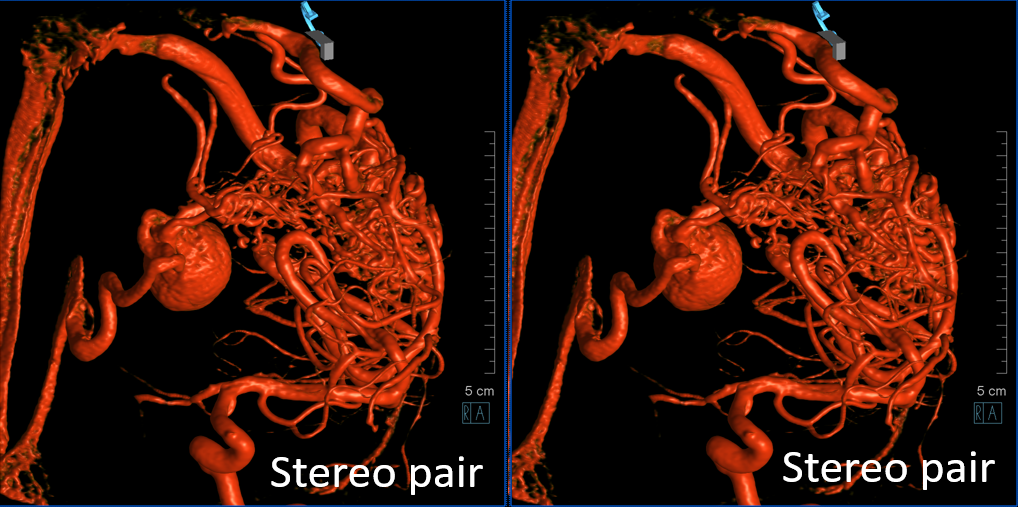
Stereos
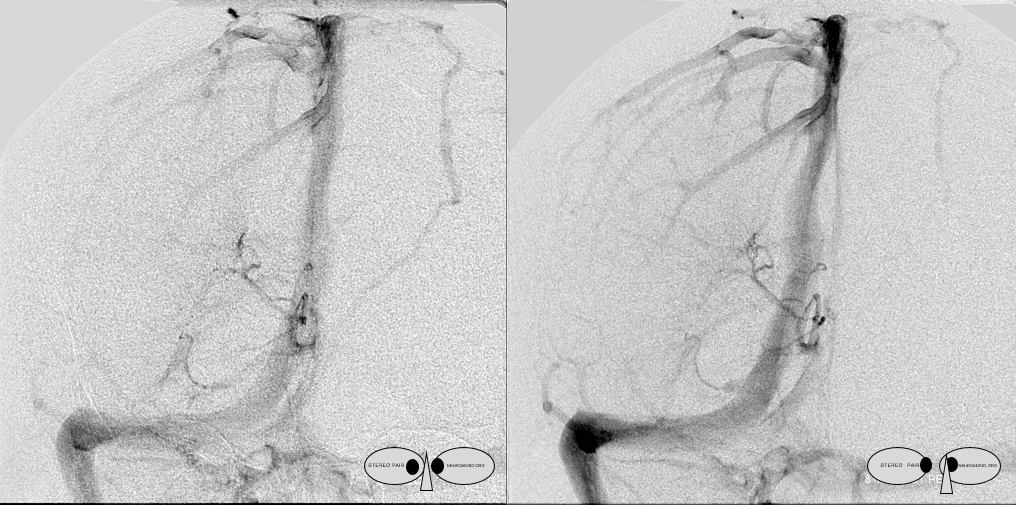
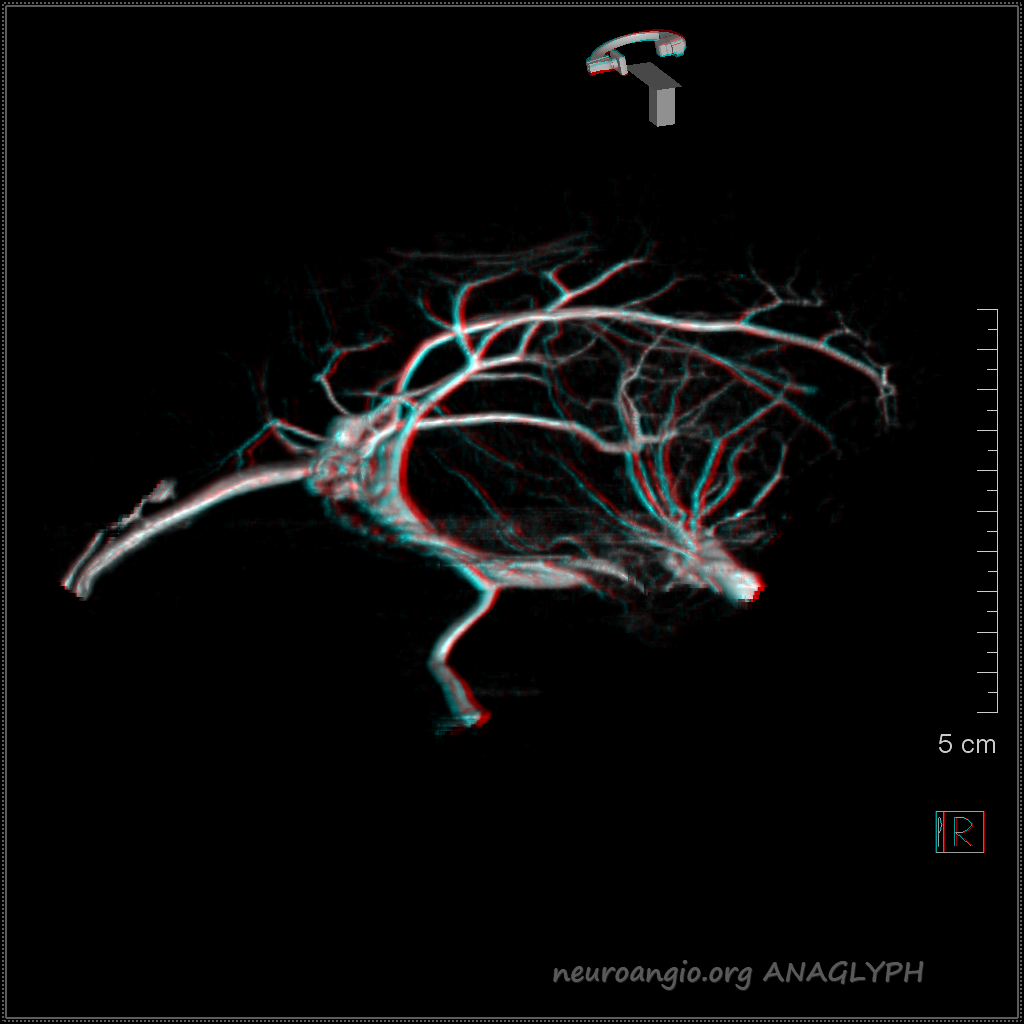
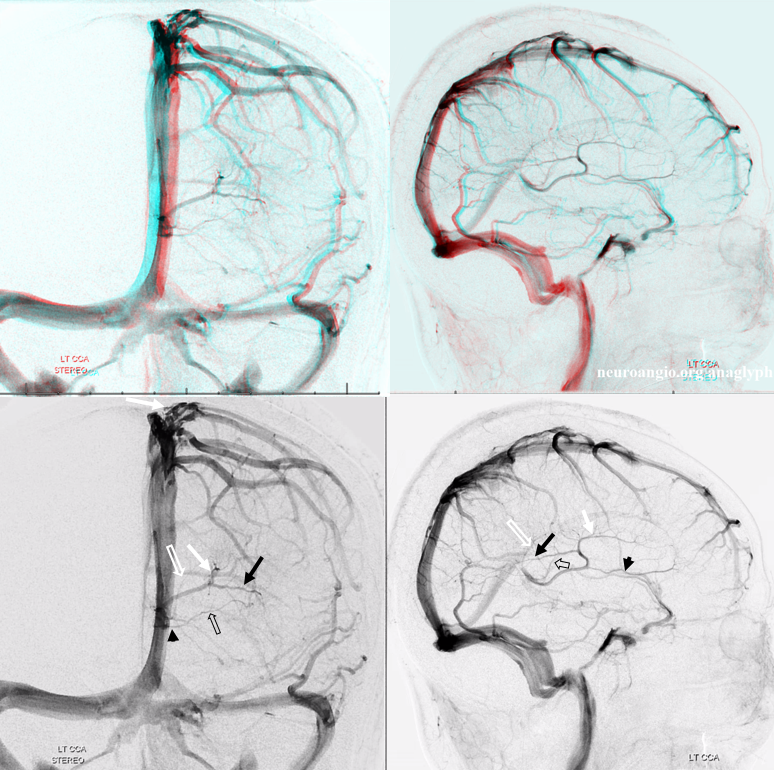
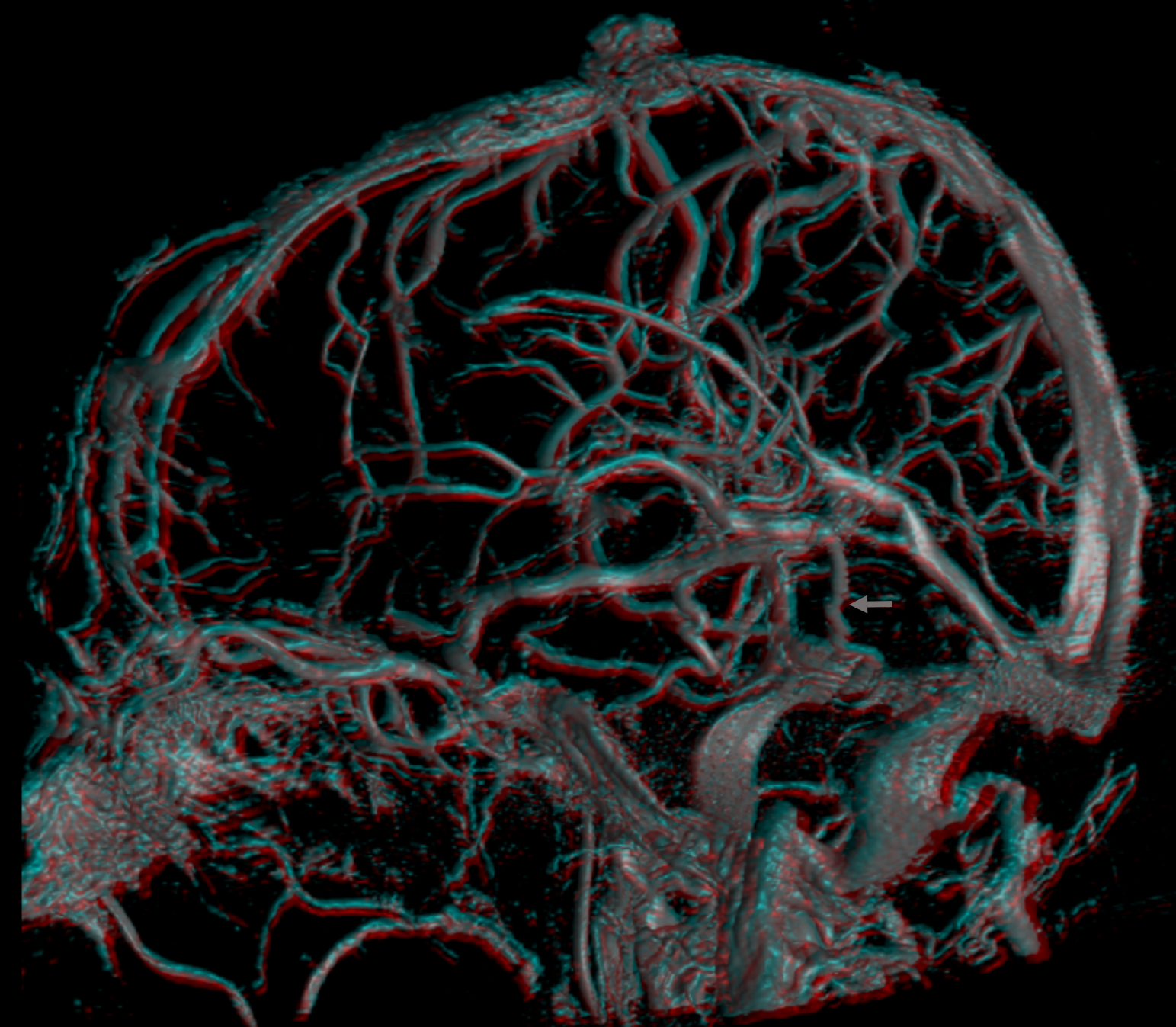
Frontal Anaglyph
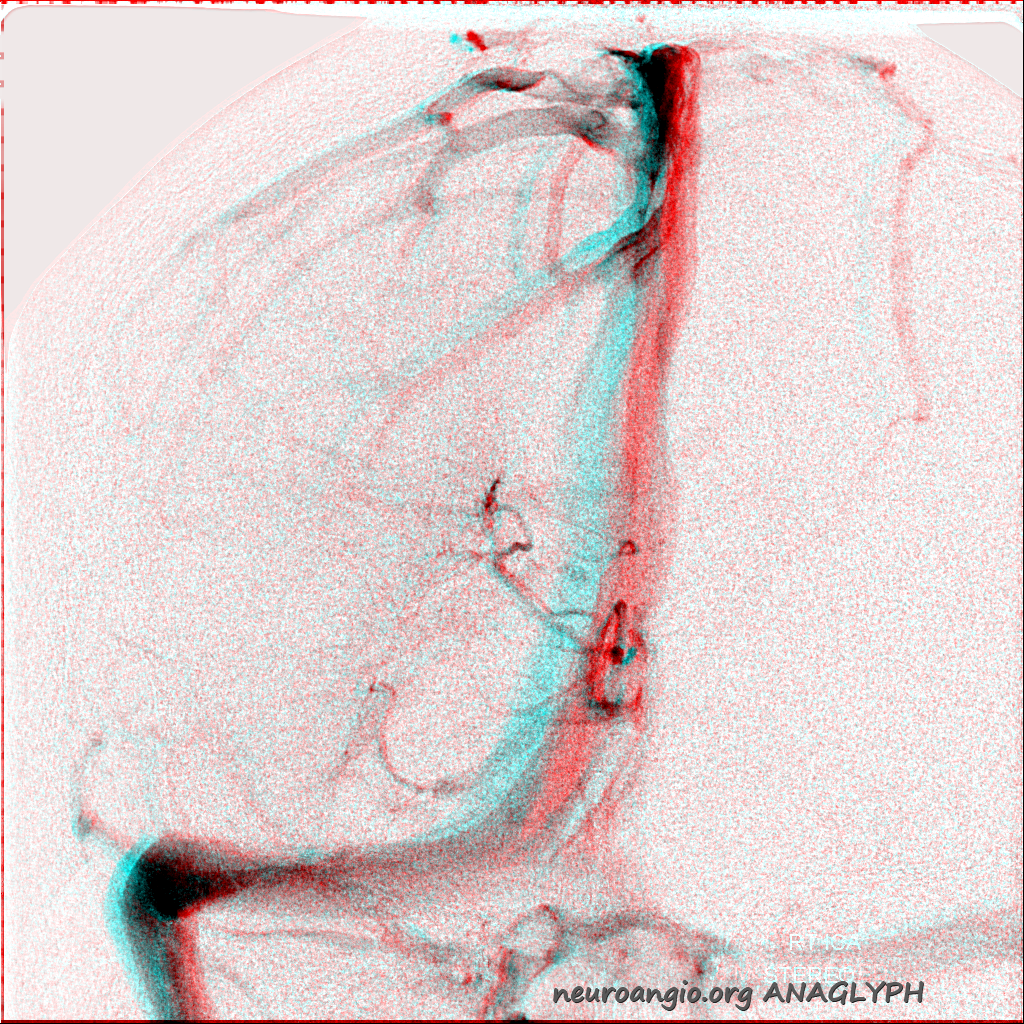
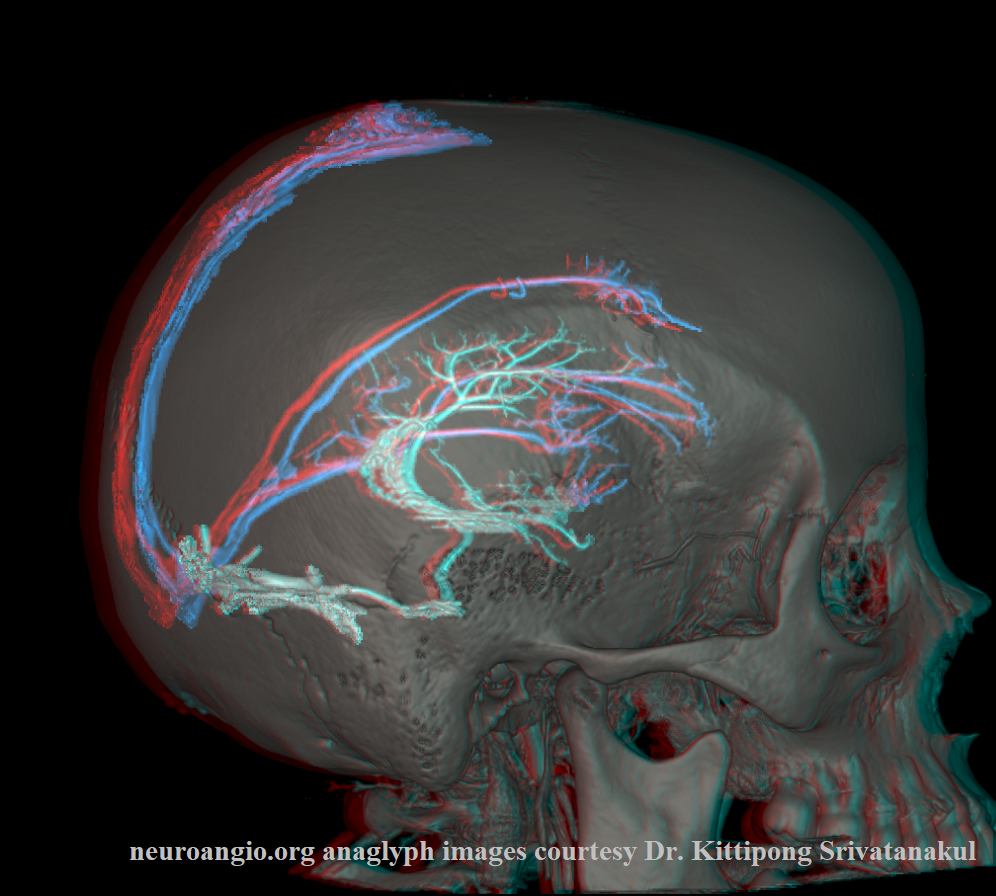
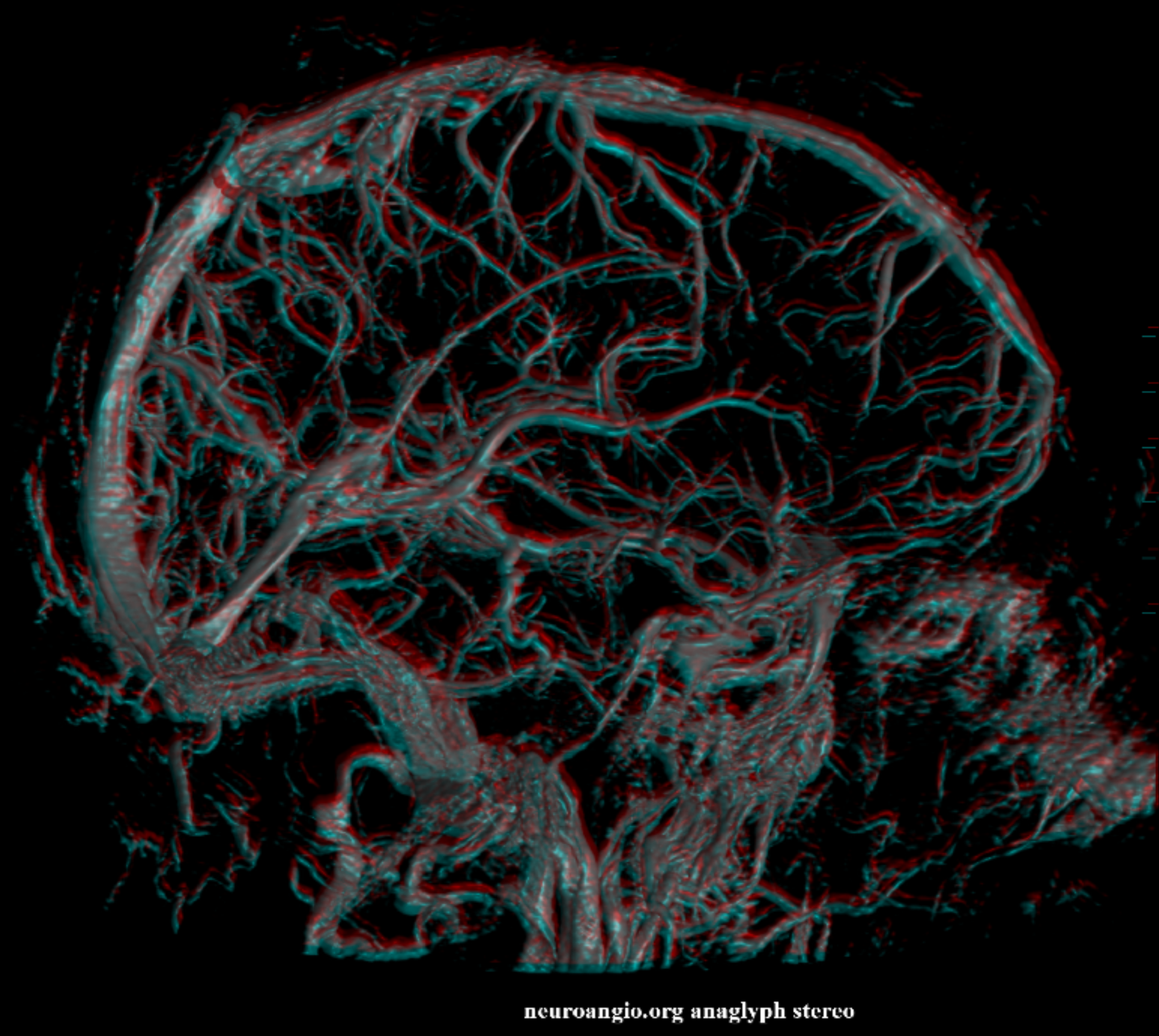
Lateral Anaglyph

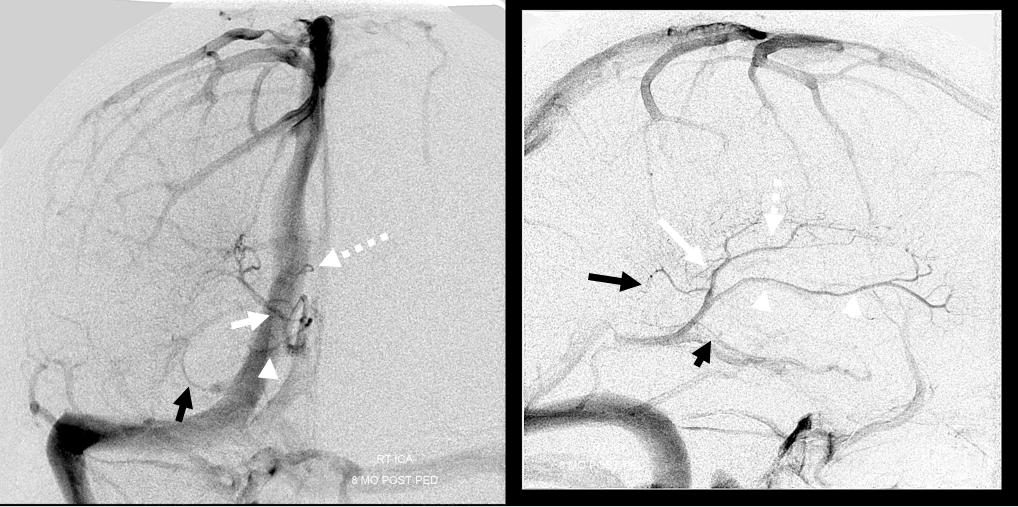
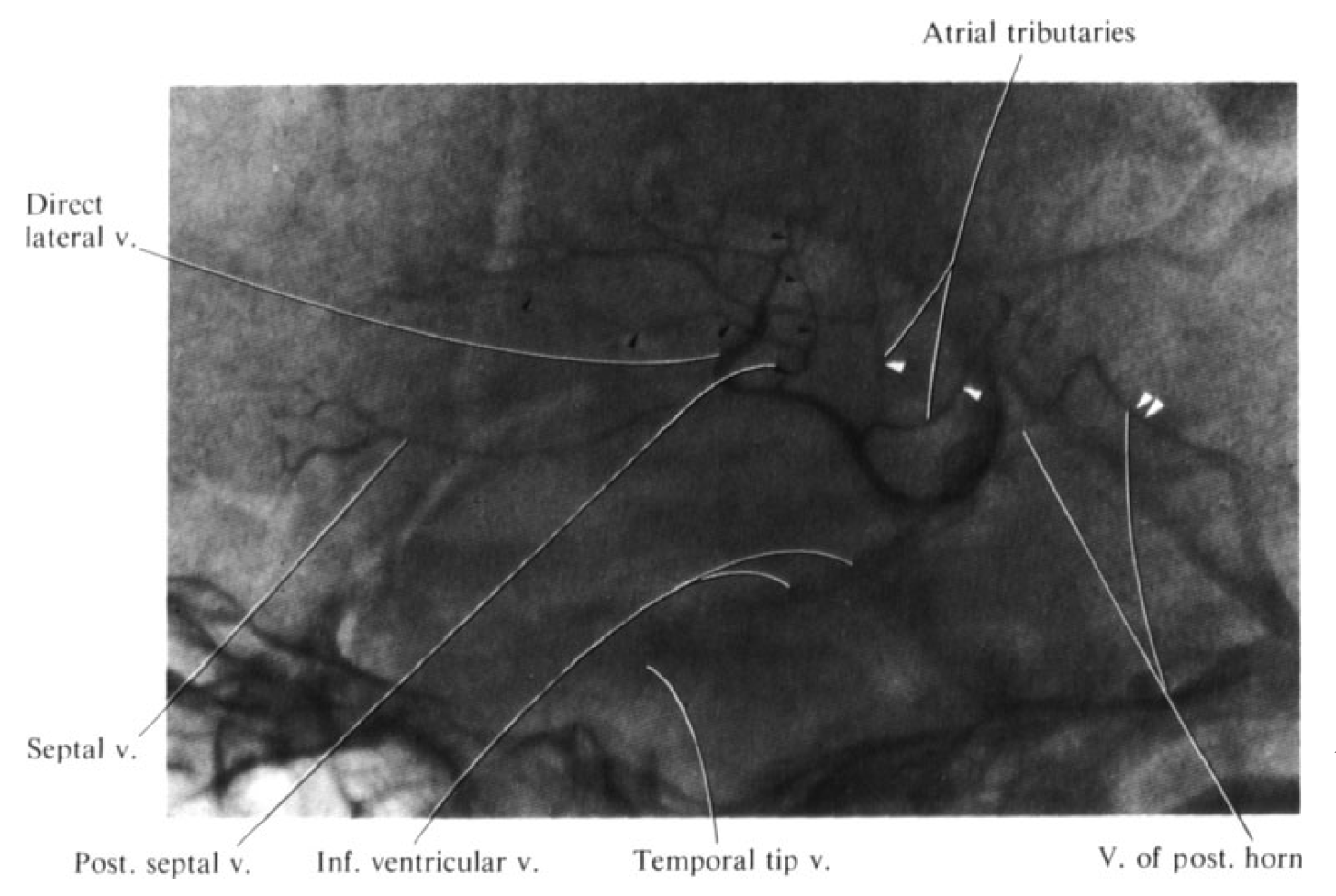
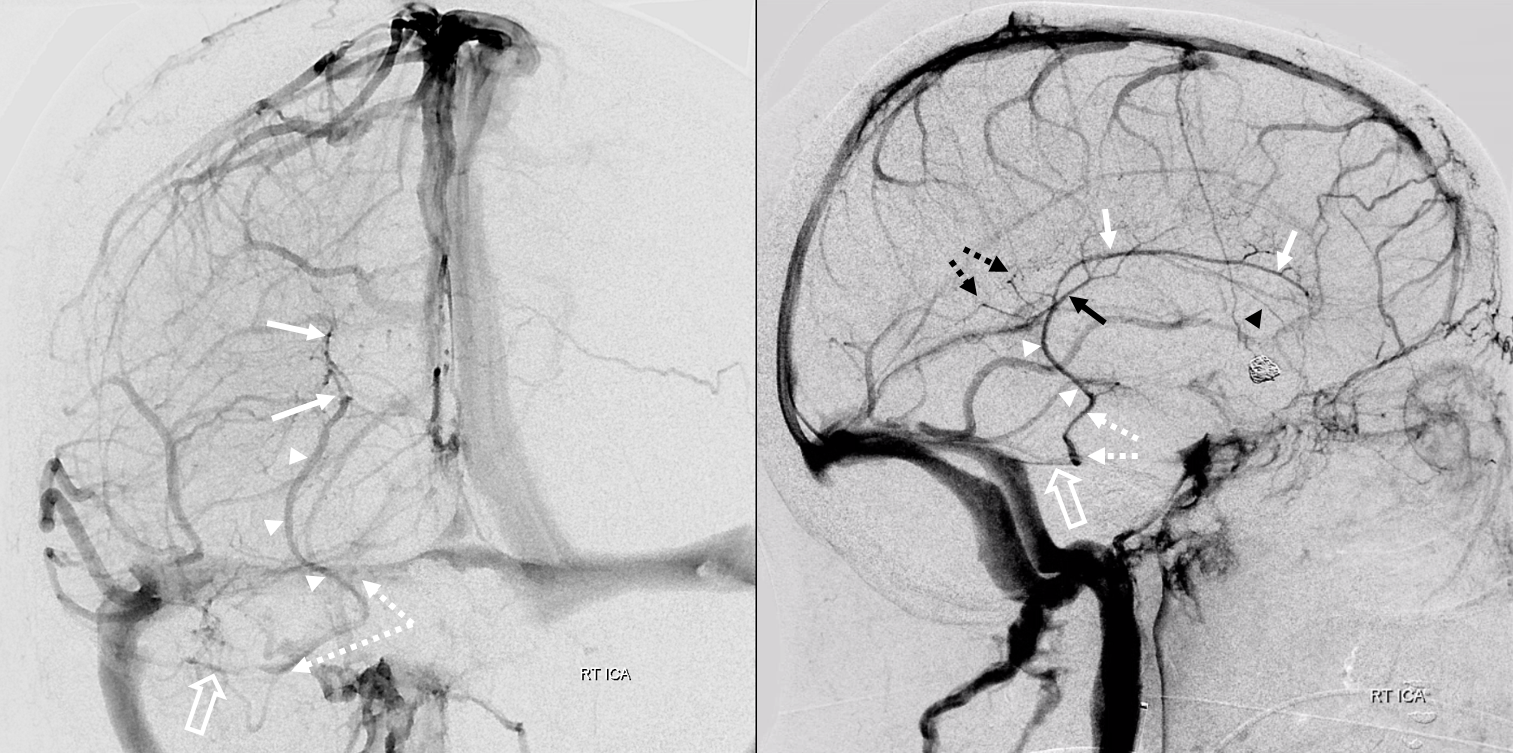
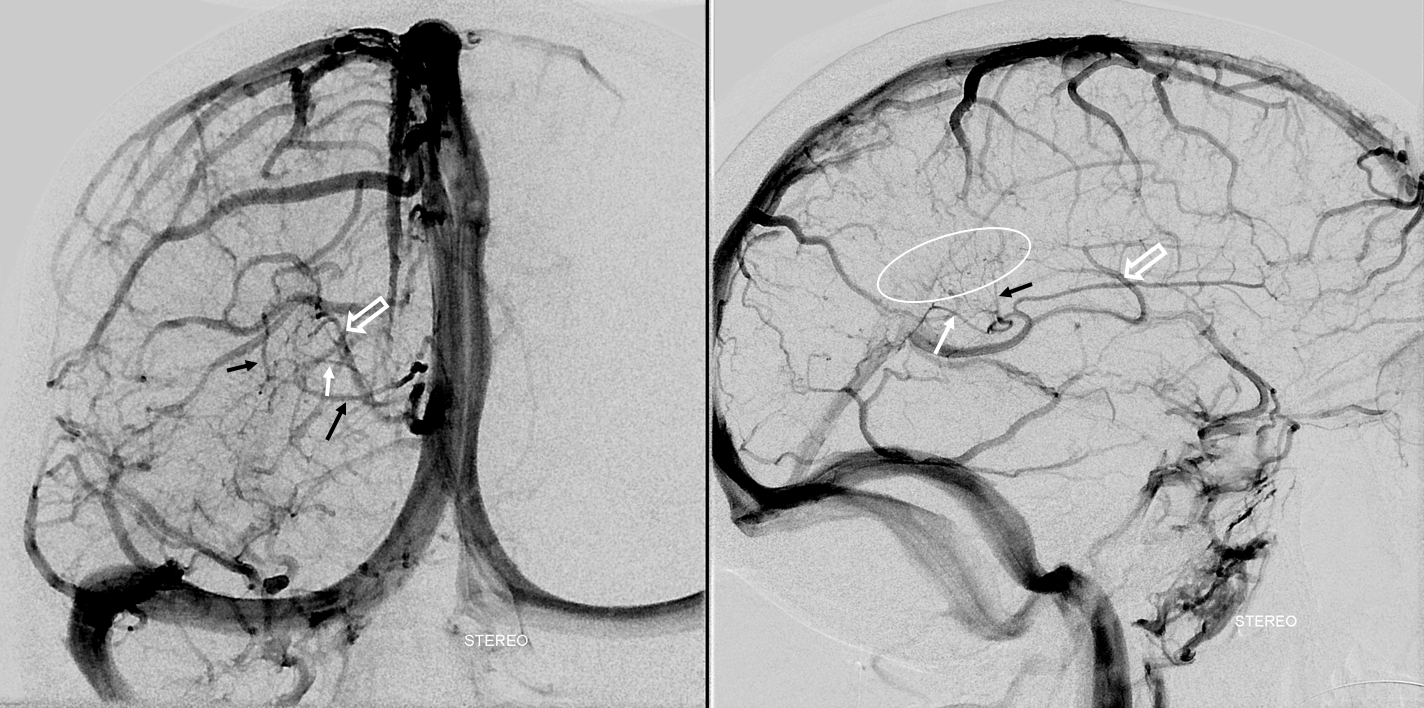
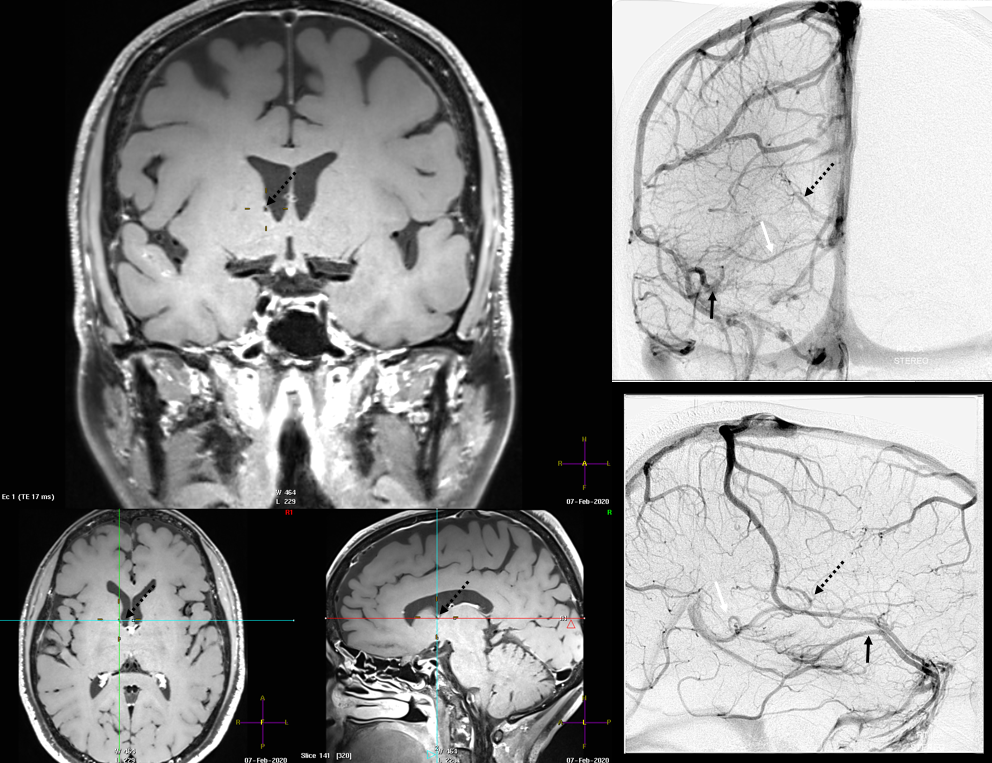
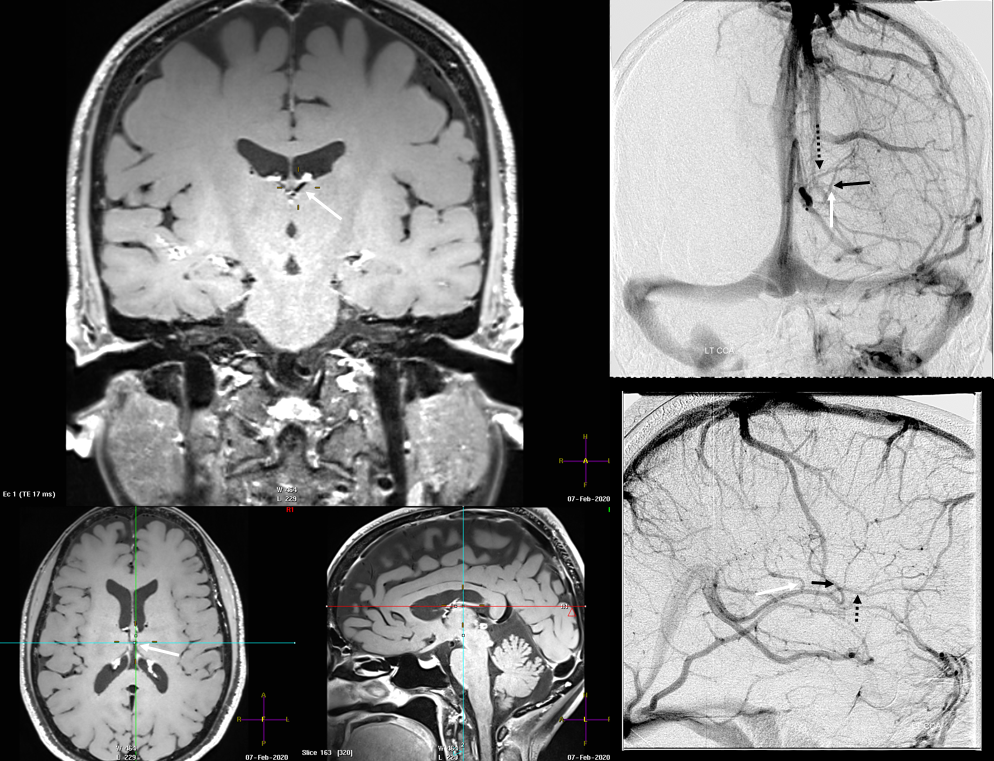
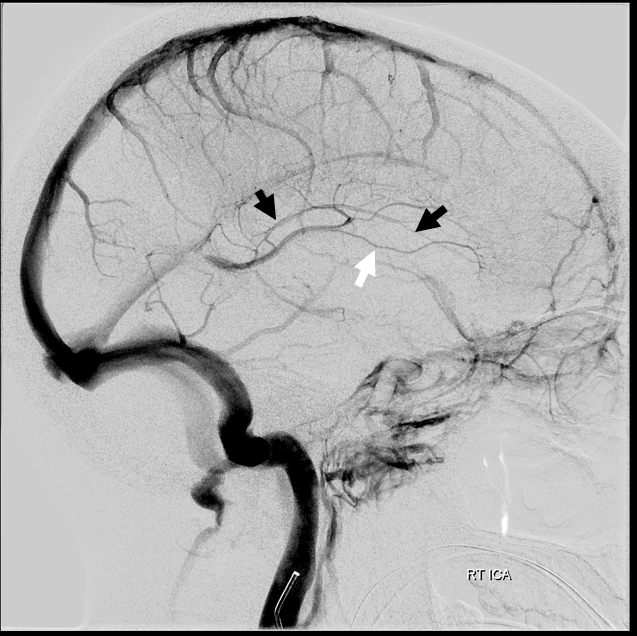
What do we have here? The thalamostriate arcade is marked by dashed white arrows. The “thalamostriate vein” (white arrow) appears to join the septal vein (white arrowheads) quite posteriorly. Just before the junction, it is also joined by the medial atrial vein (black arrow). Also present faintly is the inferior ventricular vein (black arrowhead).
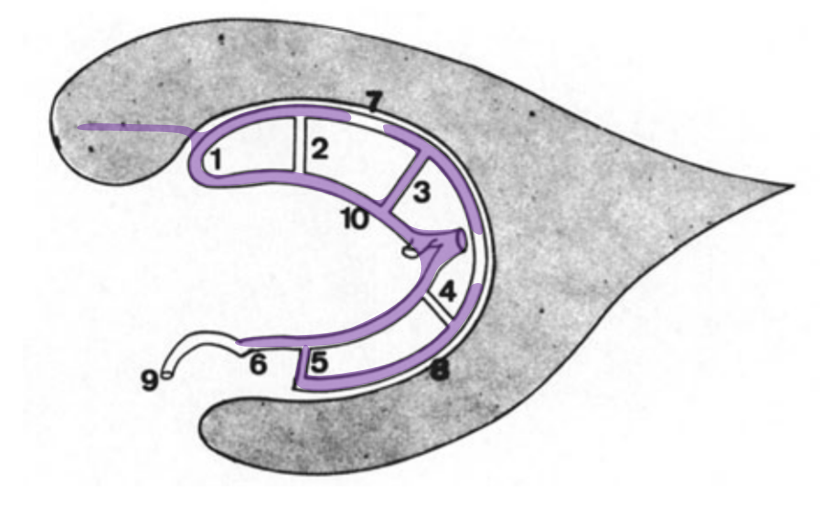
How do we explain this? Rings. There is developmental hypoplasia of the thalamostriate vein at its usual segment of the foramen of Monro (arrow on the schematic below). The direct lateral vein (3) serves as connection between the thalamostriate vein arcade (dashed white arrow) and internal cerebral vein instead — see schematic below. So, it is not that thalamostriate vein is too posterior. It is hypoplastic. What we have a is a different connection between the thalamostrate venous arcade and the internal cerebral vein — via the direct lateral vein in this case. The schematic is facing backwards — to keep your mind flexible…
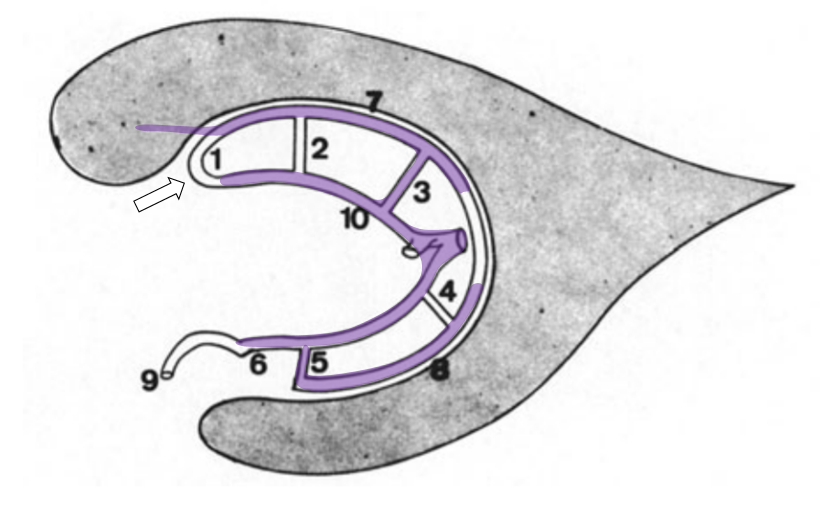
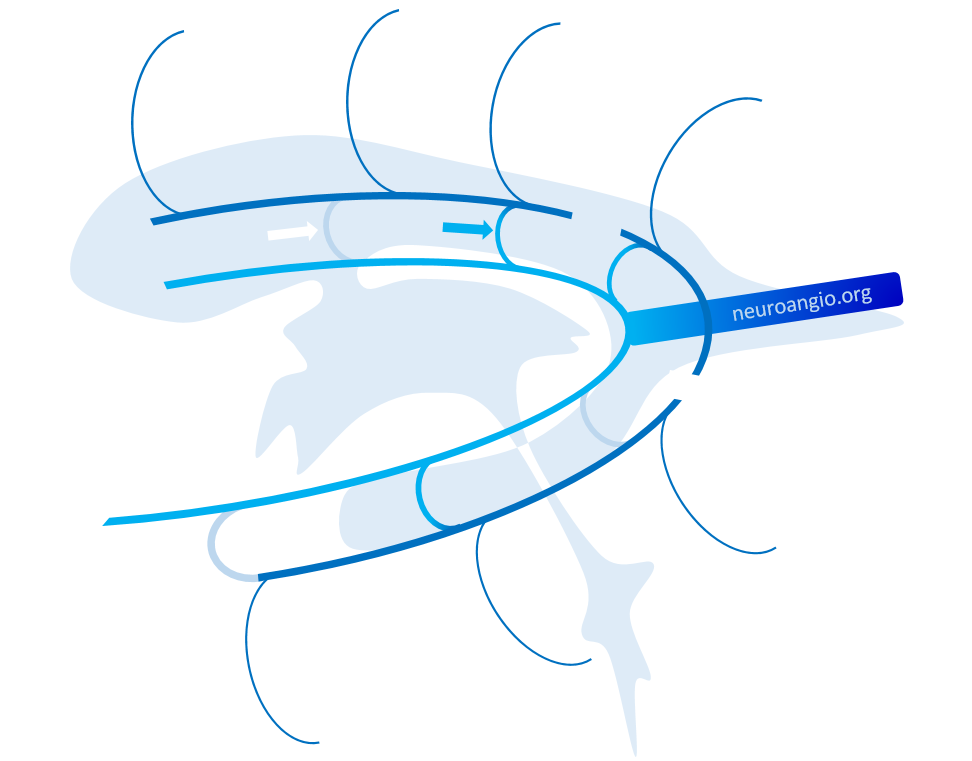
The same idea with neuroangio diagram — hypoplasia of the typical Monro opening of thalamostriate vein (white arrow) is associated with prominence of the direct lateral vein (blue arrow)
And, of course, for all these reasons using the classic “venous angle” as a landmark for the foramen of Monro is not an idea inspired by wisdom. The posteromedial-posterolateral choroidal artery junction is much better.
Here is an example of same thing from YP Huang’s collection — this is still neither digital nor subtraction angiography — just angiography, with ionic contrast. But just as clear
Below is another modern example of the same thing…
Thalamostriate Vein
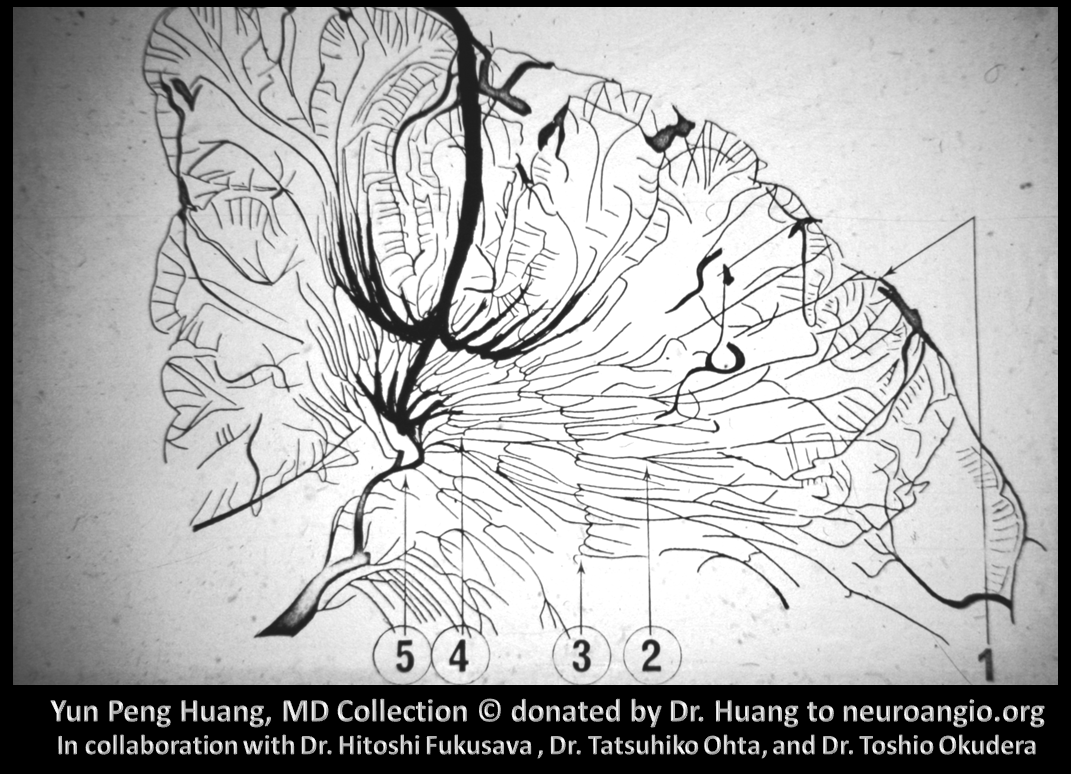
The “outer ring” is primarily made of the tributaries of the thalamostiate vein. Everyone knows that thalamostriate vein does not drain the thalamus. Better to think of the territory it typically drains — the caudate and adjacent white matter — we will call it the caudate veins.
Caudate Veins
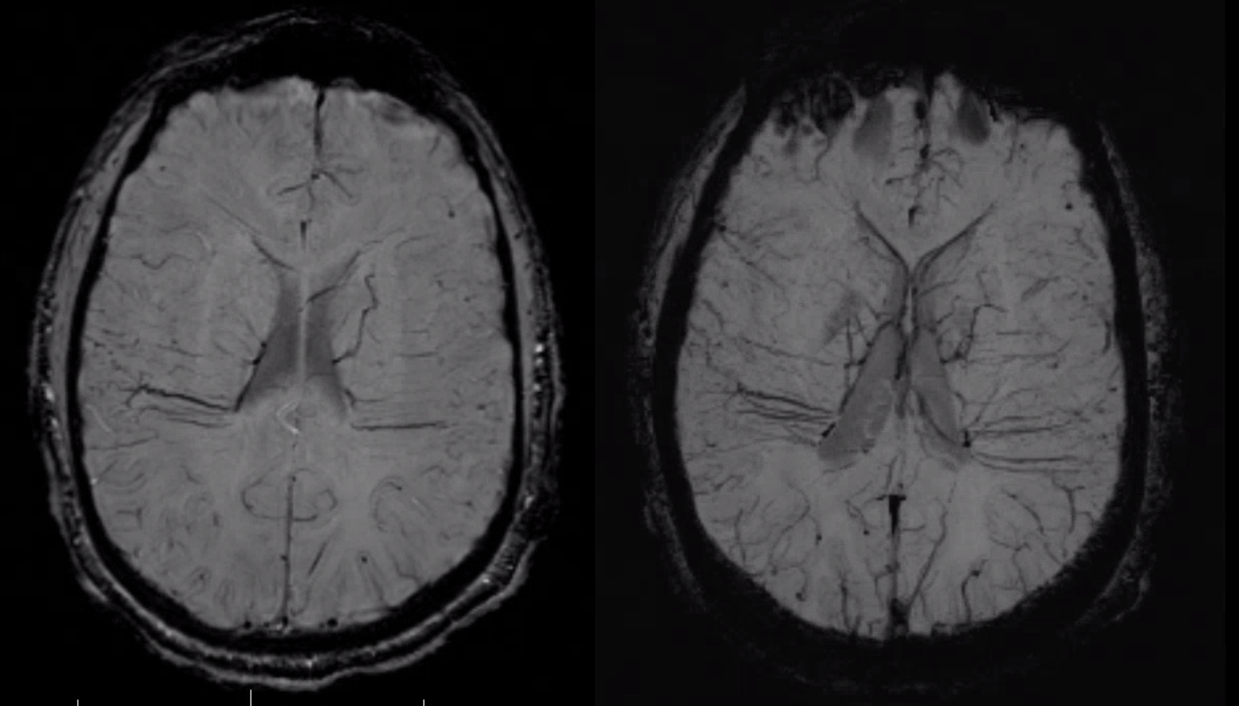
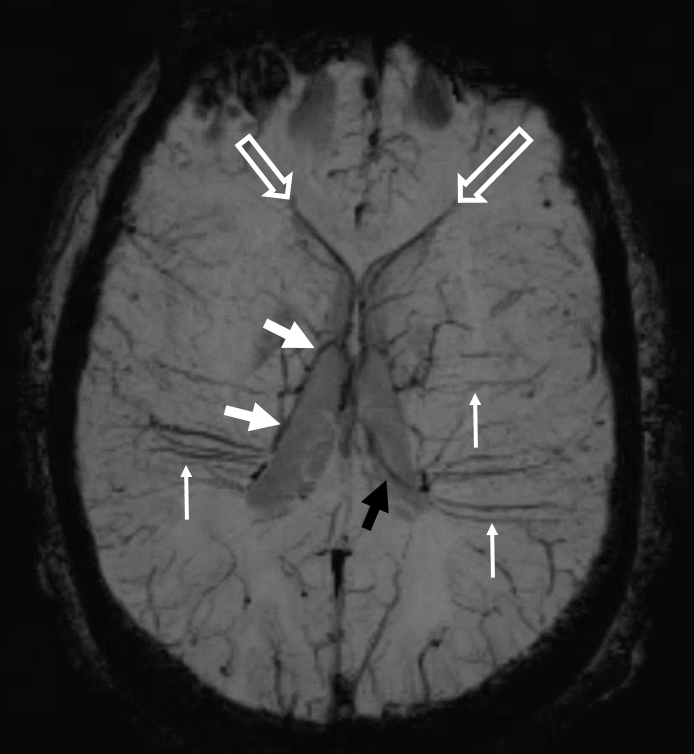
These are organized into — guess what — longitudinal and transverse veins. The transverse veins are part of the medullary / deep white matter system. The longitudinal caudate venous arcade forms the “outer ring” that is named “thalamostriate arcade” in Lasjaunias figure. In the figure below, the longitudinal caudate veins are marked by thick white arrows, the (longitudinal) anterior caudate vein by thick black arrows, the transverse caudate veins by thin black arrows, and transverse medullary (deep white matter) veins by thin white arrows.

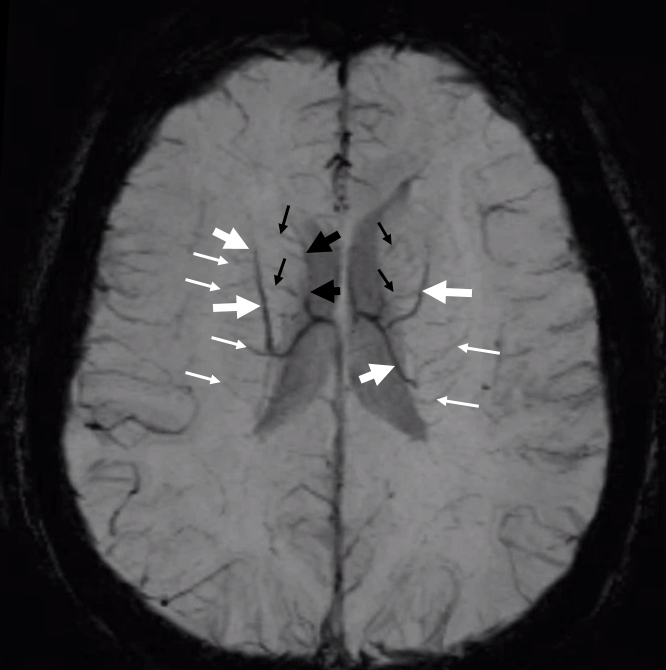
How to look at this SWI? Again, its all about balance. On the right, the longitudinal caudate venous channel is dominant anteriorly (white arrows). The posterior portion (white arrowheads) collects into what ultimately becomes the inferior ventricular vein (open white arrow). On the left, the posterior longitudinal caudate vein is better formed (black arrowhead). The anterior part is somewhat hypoplastic (black arrow) and is compensated by greater size of the anterior caudate vein (black open arrow)
Back to the rings — how do the longitudinal caudate veins drain?
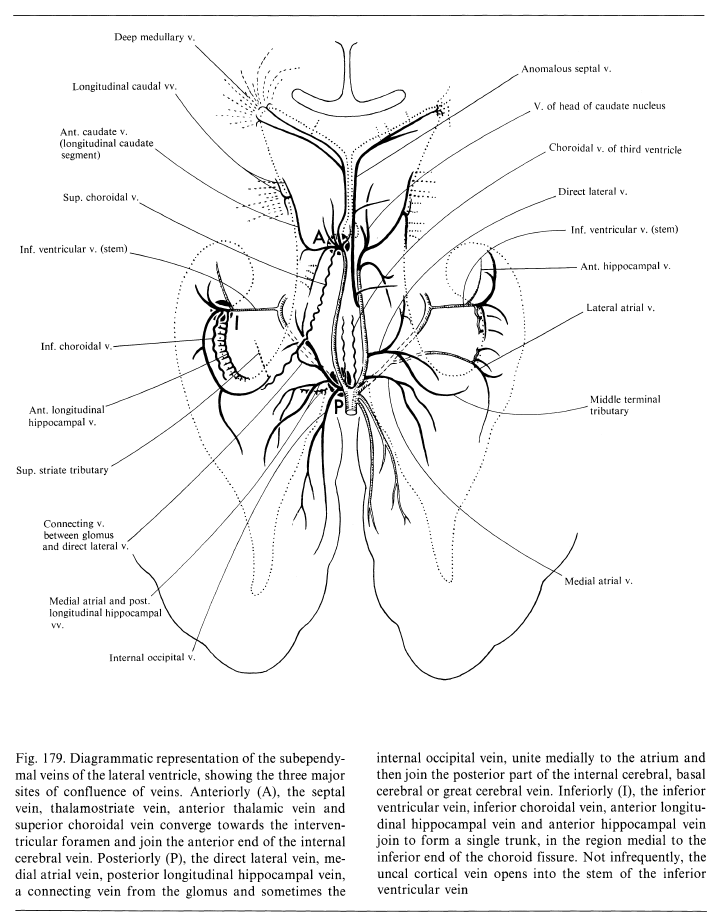
The key to understanding internal cerebral vein is not the vein itself — it is the structures that drain into it. Prinicipally the caudate veins. They can reach the internal cerebral system — or the basal vein via the inferior ventricular vein — by a number of pathways that are shown by the rings approach.
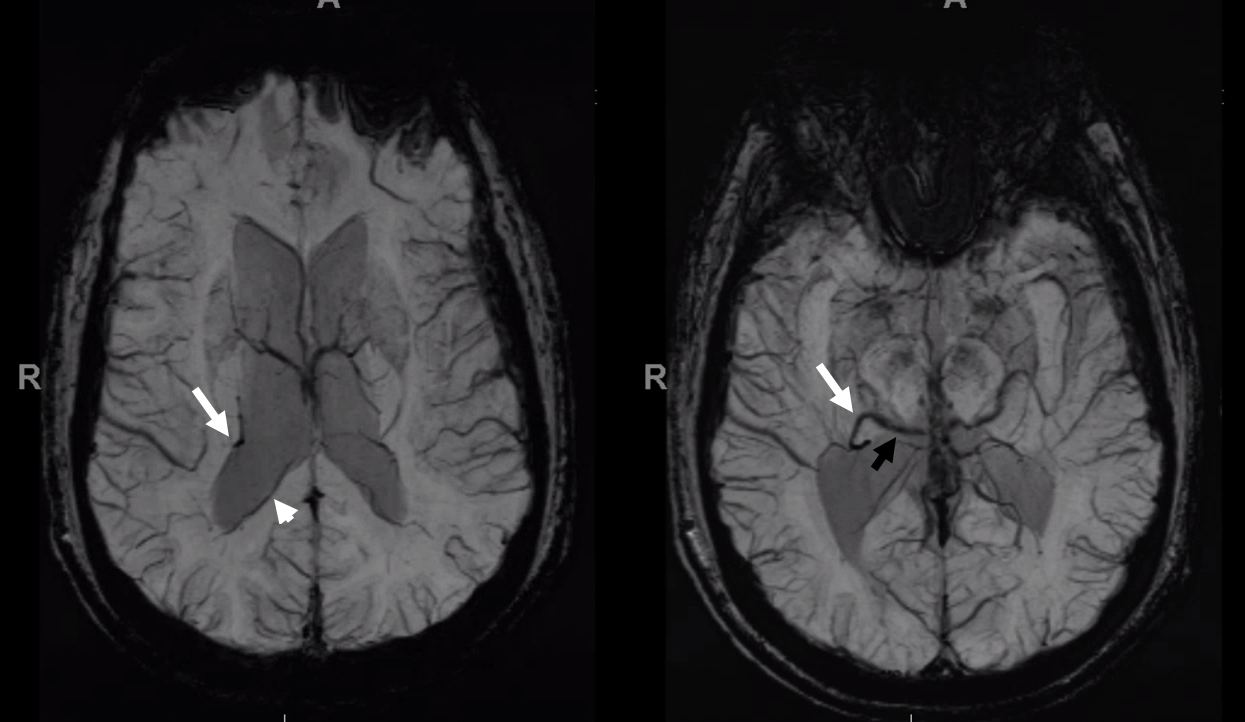
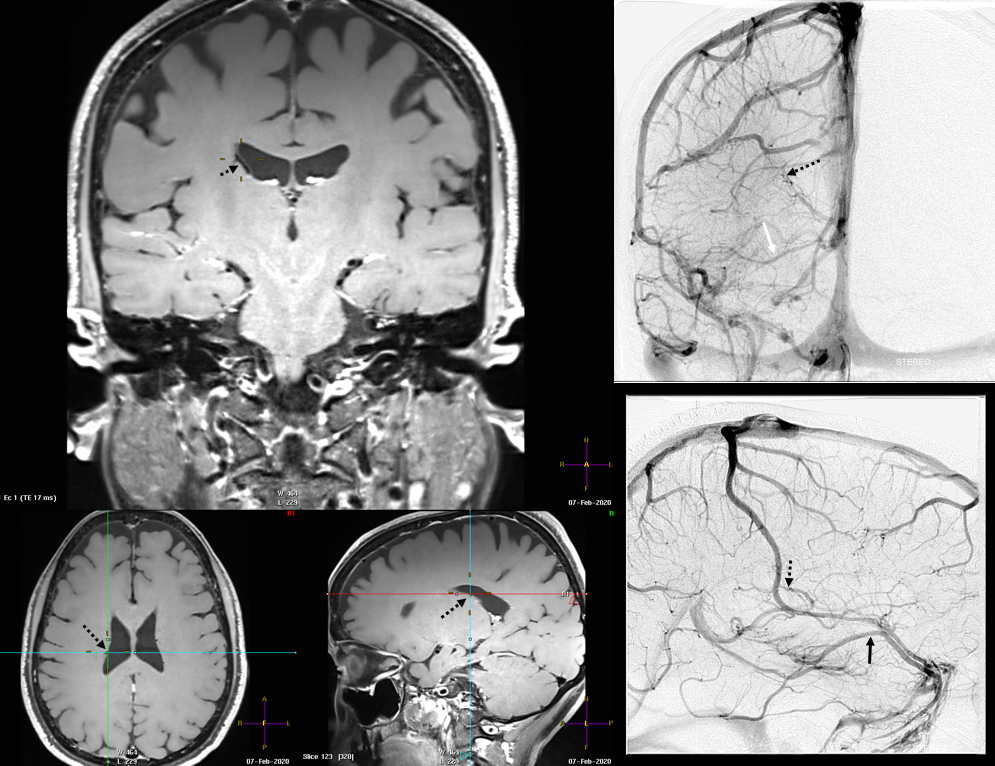
The structures adjacent to the venticles (outer ring) will drain into either the internal cerebral vein or basal vein, using any of the connections shown in the rings picture. Here is an example of the inferior ventricular vein (5,6) draining territory of the caudate tail / posterior lateral ventricular zones. Why, because of a “break” in the outer ring (white arrow) and hypoplasia of the direct lateral vein (3)
Hypoplasia of lateral direct vein and lack of posterior longitudinal caudal vein access to the thalamostriate vein (white arrows) result in inferior ventricular vein picking up the slack

Angio. Inferior ventricular vein collects territory of posterior caudate/lateral ventricular area (white arrows)
Same can be seen extremely well on what is state of art in 2020. Here is vessel wall imaging
SWI. Inferior ventricular vein is white arrow. Medial atrial vein is white arrowhead. The basal vein is black arrow
More CWI
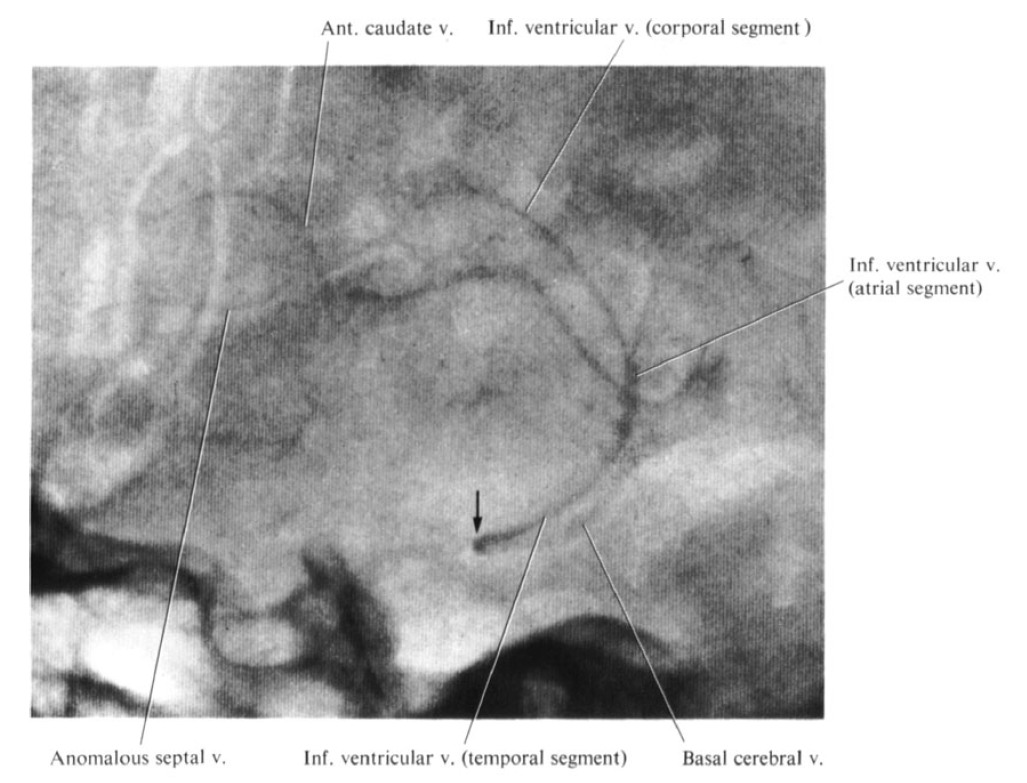
YP Huang image of same variant, frontal
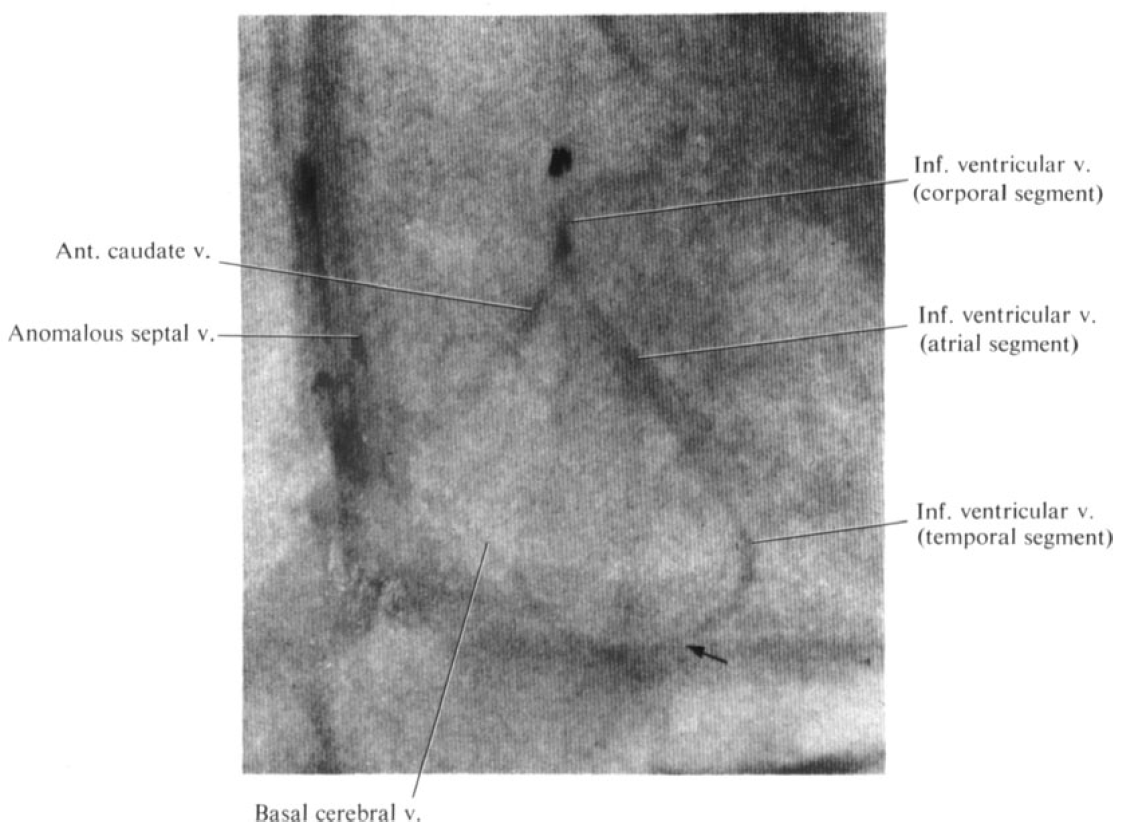
Lateral
Caudate Drainage into the Lateral Mesencephalic Vein
This is an example of rare variant where the internal cerebral vein or some of its components do not drain into the Galenic system. Here, the lateral group / caudate veins (white arrows) drain via the inferior ventricular vein (white arrowheads) into the lateral mesencephalic vein (dashed white arrows) and then into the superior petrosal sinus (open white arrow). This variant is an extreme of what was shown above — when the caudate was drained into the basal vein of Rosenthal via the inferior ventricular vein. However, there is also a variant where the basal vein mesencephalic segment drains into the lateral mesencephalic vein — that is common. So, combine the two, and you have internal cerebral vein going into the lateral mesencephalic vein. This is the famous “epsilon” sign that is seen in “Vein of Galen” anomalies. See basal vein of Rosenthal and lateral mesencephalic vein pages for more info on understanding this variant.
Without arrows
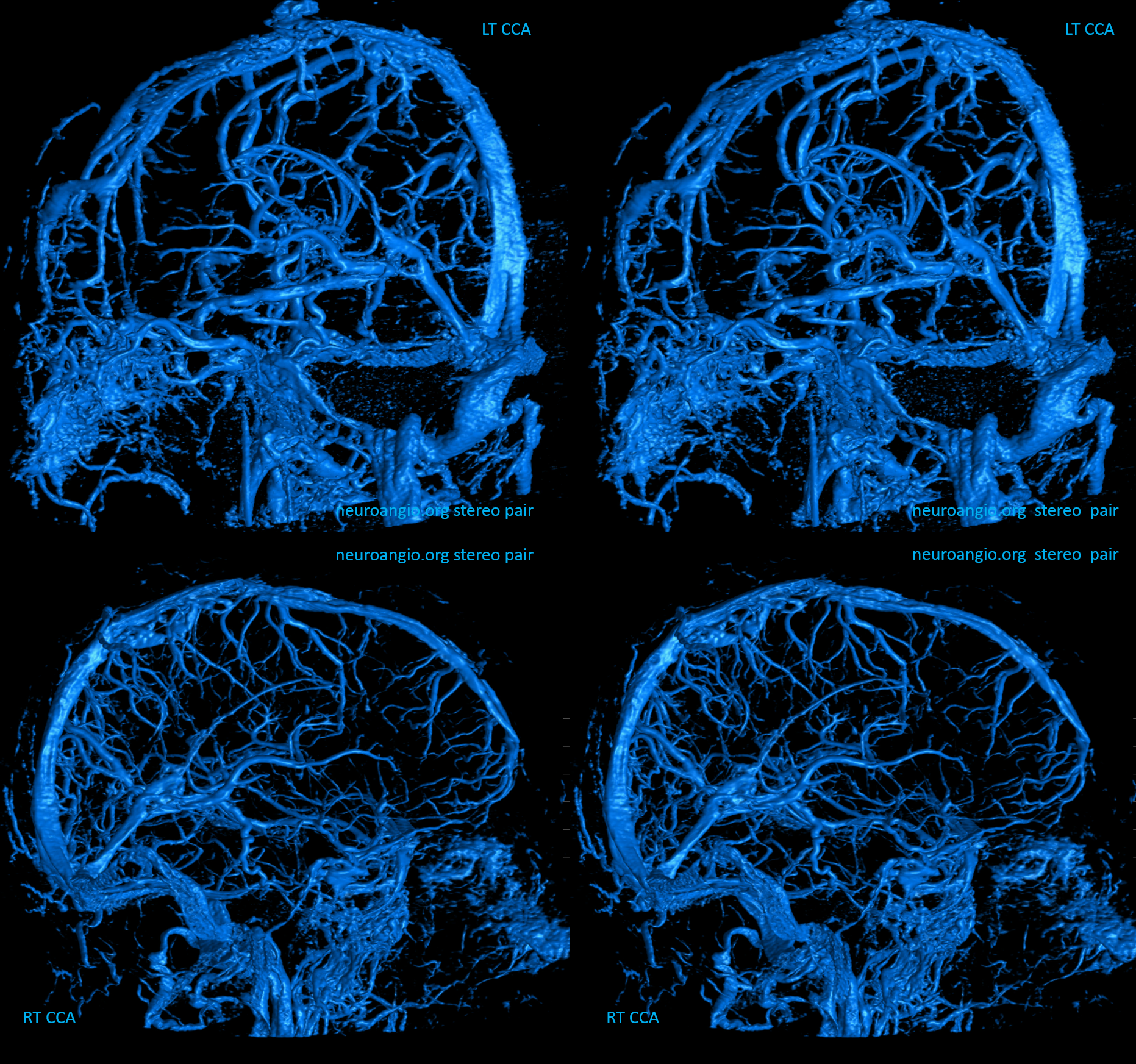
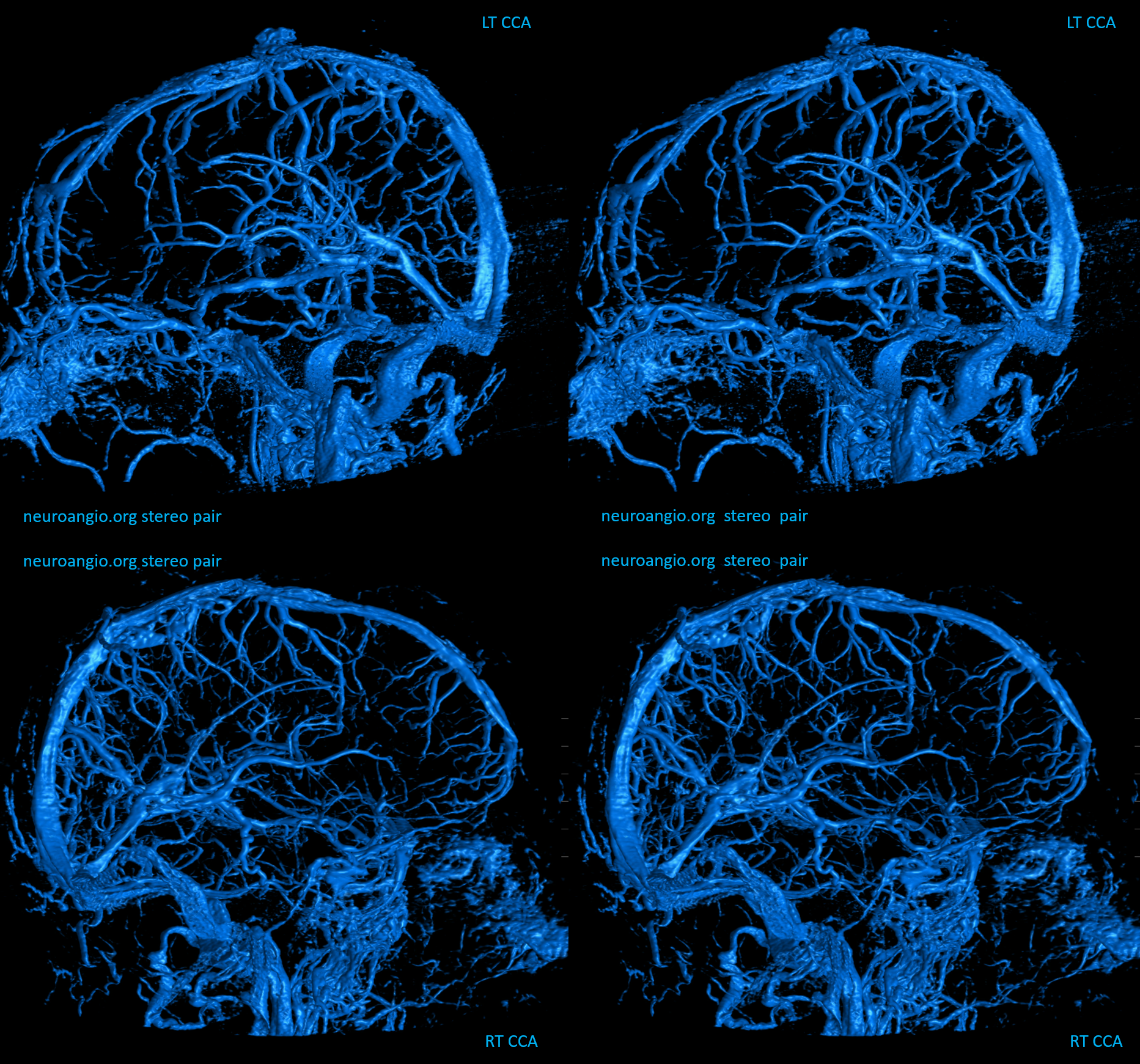
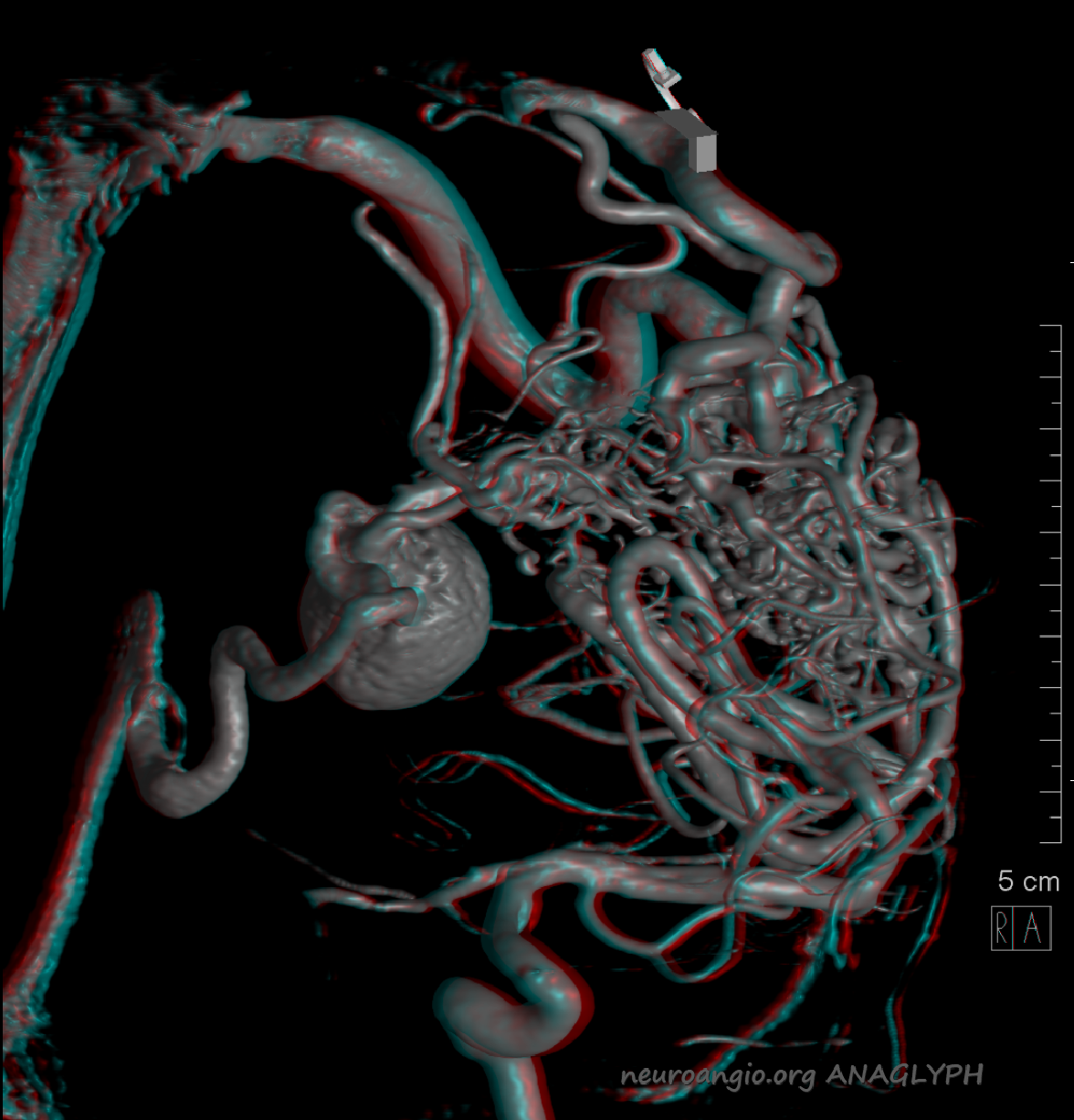
Stereo ANAGLYPH

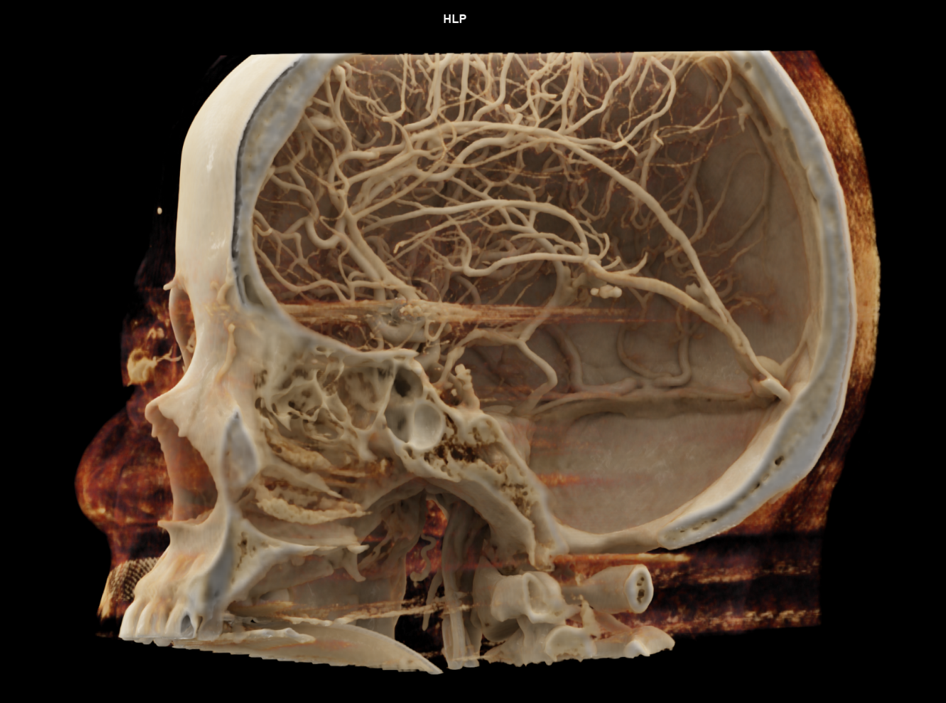
ANAGLYPH Volume Rendered DYNA CT Image
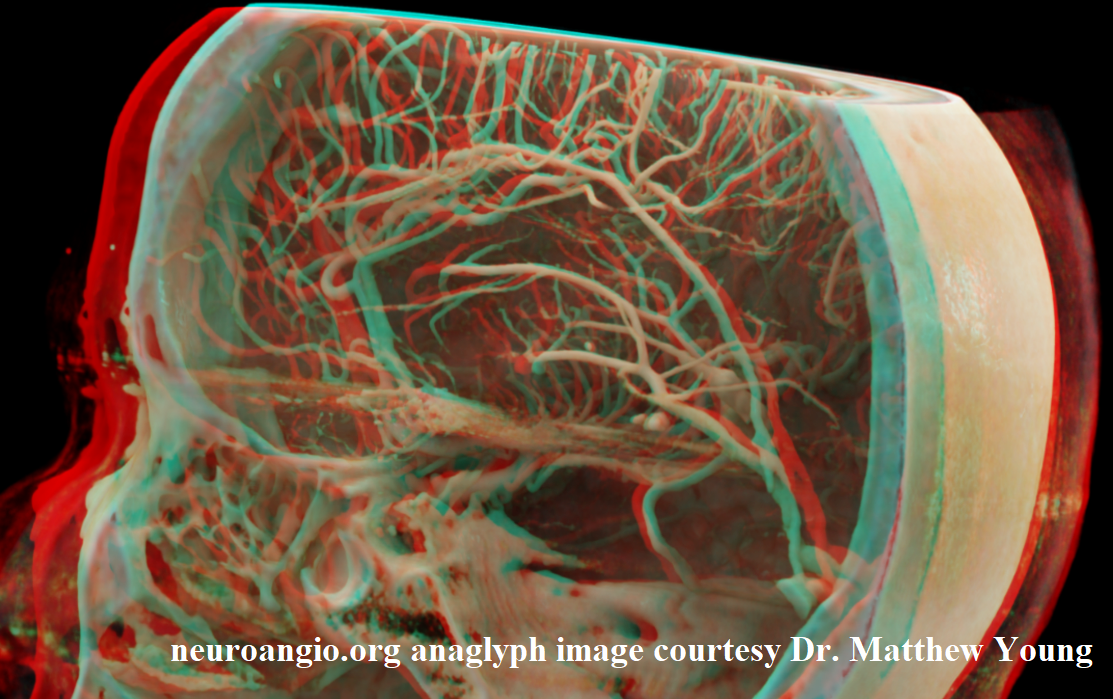
More ANAGLYPH

Cinematic rendering of DYNA CT by Dr. Matthew Young
Amazing ANAGLYPH cinematic renderings

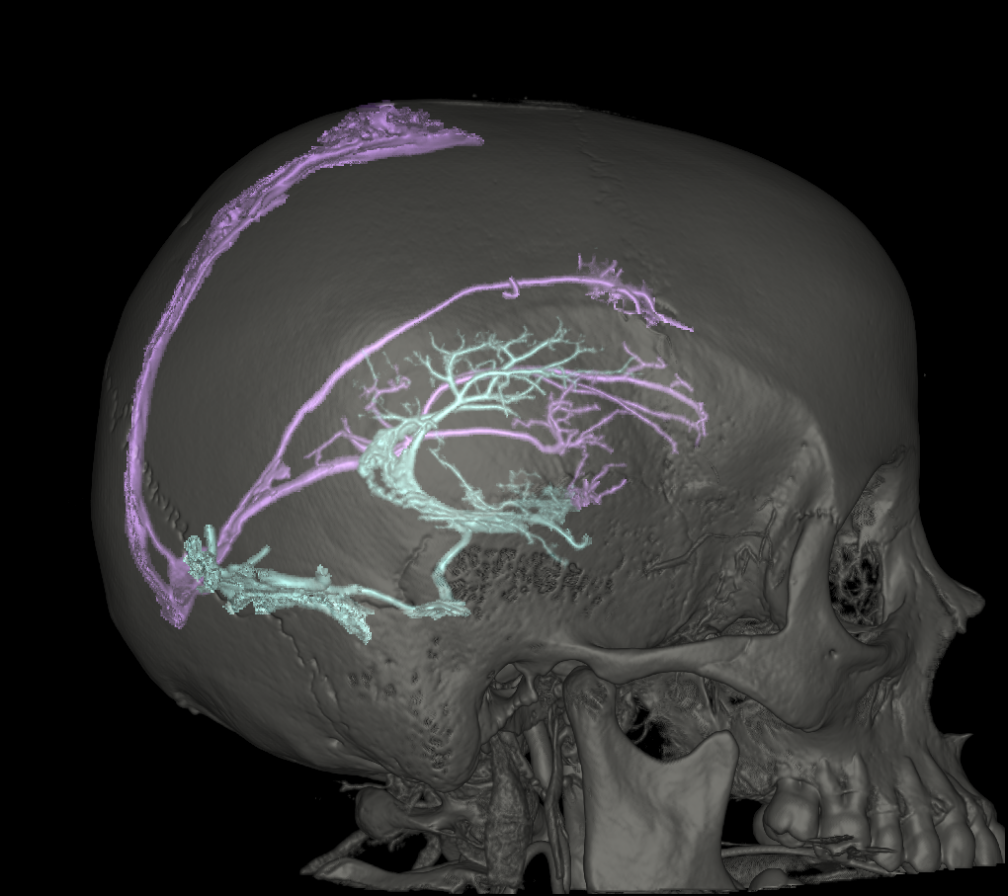
Even more — segmentation VRs courtesy Dr. Kittipong Srivatanakul
Cross-eye stereo
Anaglyph stereo
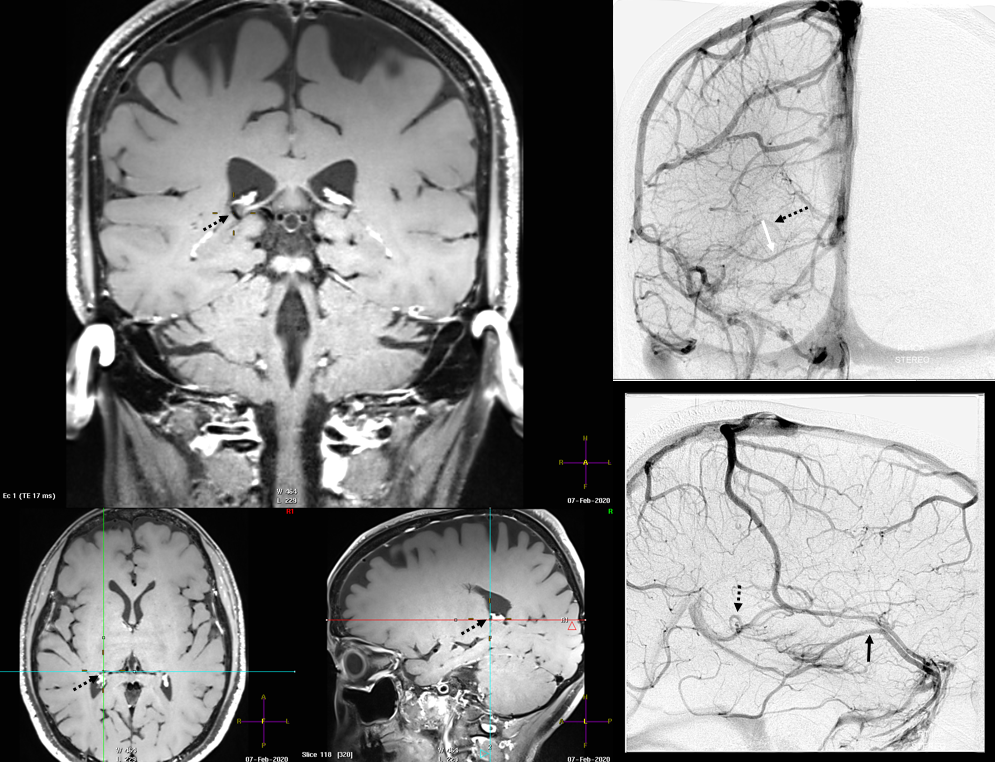
Lateral Atrial Vein / Lateral Direct Vein / Direct Lateral Vein
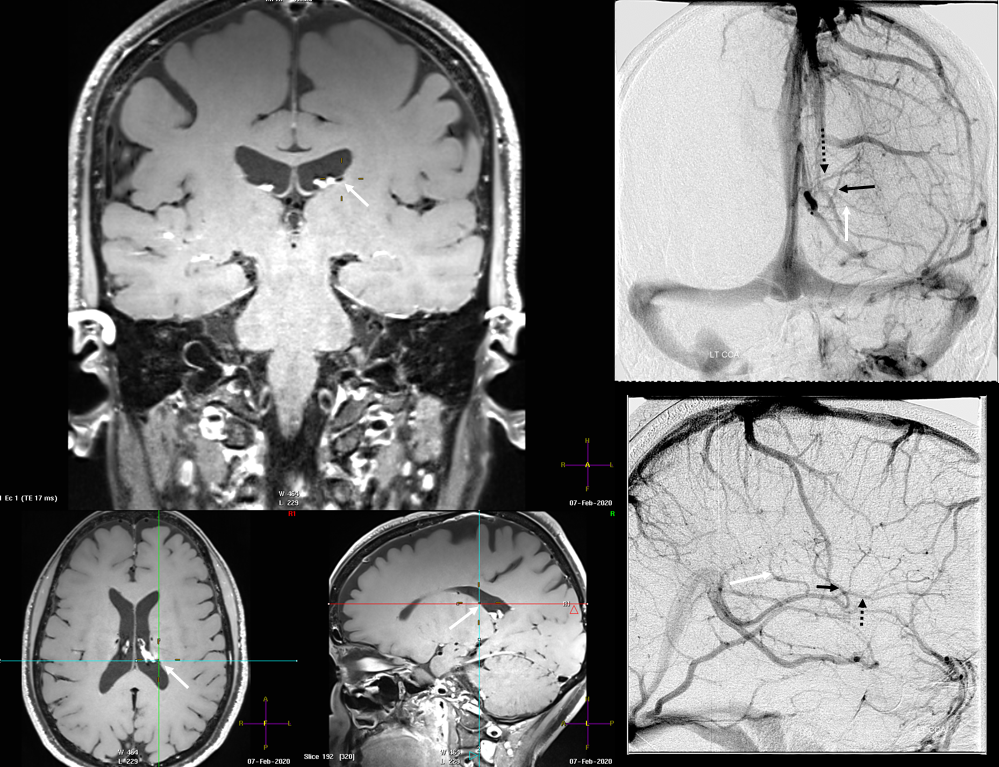
The lateral atrial vein (black arrows) is a very commonly seen vein, collecting usually the territory of the posterior caudate and other tissue tissue near the lateral ventricular surface. More posteriorly, the same is done by the medial atrial vein (white arrow). In this example, these two veins form a common stem known as the “common atrial vein” (not labeled). It is prominent because the thalamostriate vein (open white arrow) territory is restricted to the anterior caudate veins.
The same variant shown with concentric rings concept. Number 3 corresponds to the lateral direct vein.
Cross-eye stereos
Frontal Anaglyph

Lateral Anaglyph — looking from medial to lateral

YP Huang image of same
Finally, classic lenticulostriate anatomy. A well-developed lenticulostriate vein collects both anterior (white arrow) and posterior (black arrow) longitudinal caudate veins. There is appropriate corresponding hypoplasia of the lateral direct vein. A small medial atrial vein (black open arrow) is present, as well as a posterior calossal vein (white open arrow). Septal vein is marked by black arrowhead
Venously contaminated CTA of same case
Another example — classic thalamostriate vein anatomy. Longitudinal caudate venous arcade is shown with purple arrows and within the white bordered regions below. Classic Monro opening with arrowhead. Inferior ventricular vein collects posterior portion of the arcade and is shown in black arrows
So, for the time being — you get the idea — its about balance within the deep venous system — there are many possible connections between the deep venous territories and the internal cerebral vein. Any connection can be used, and variations thus explained.
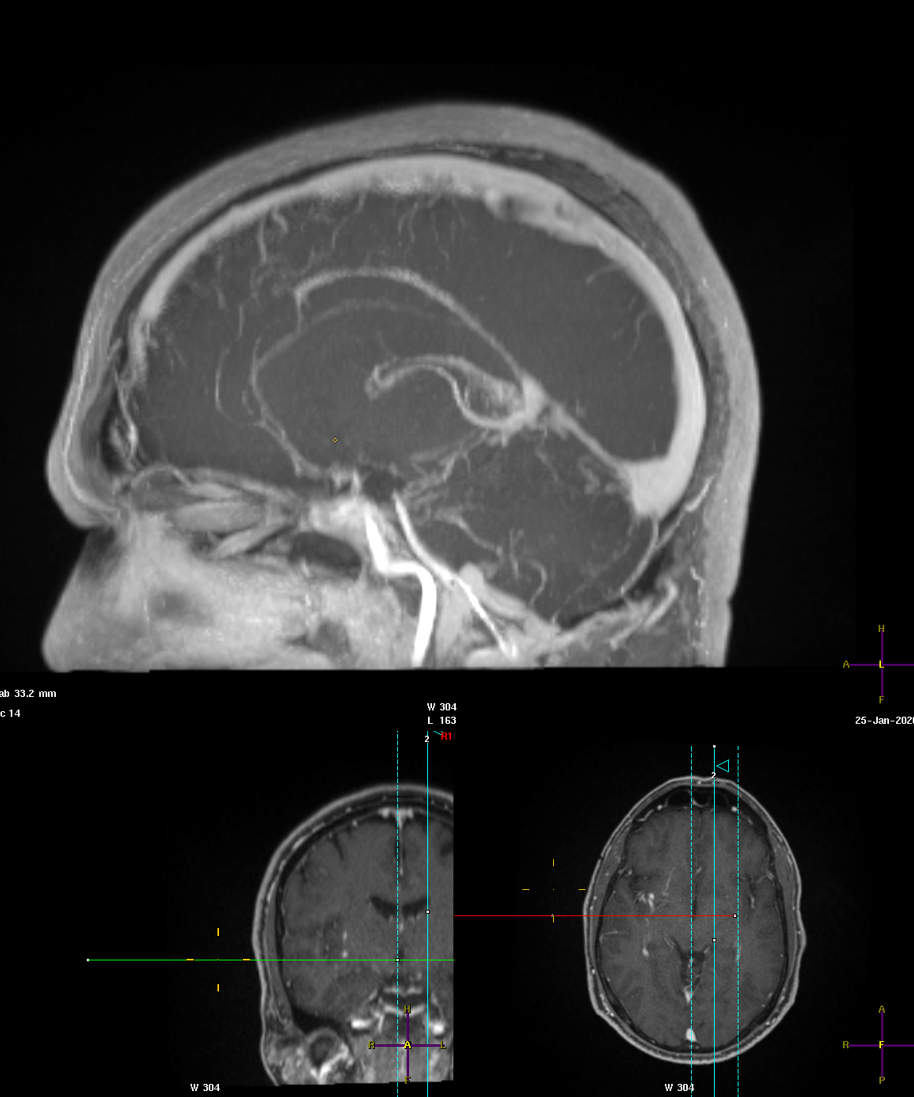
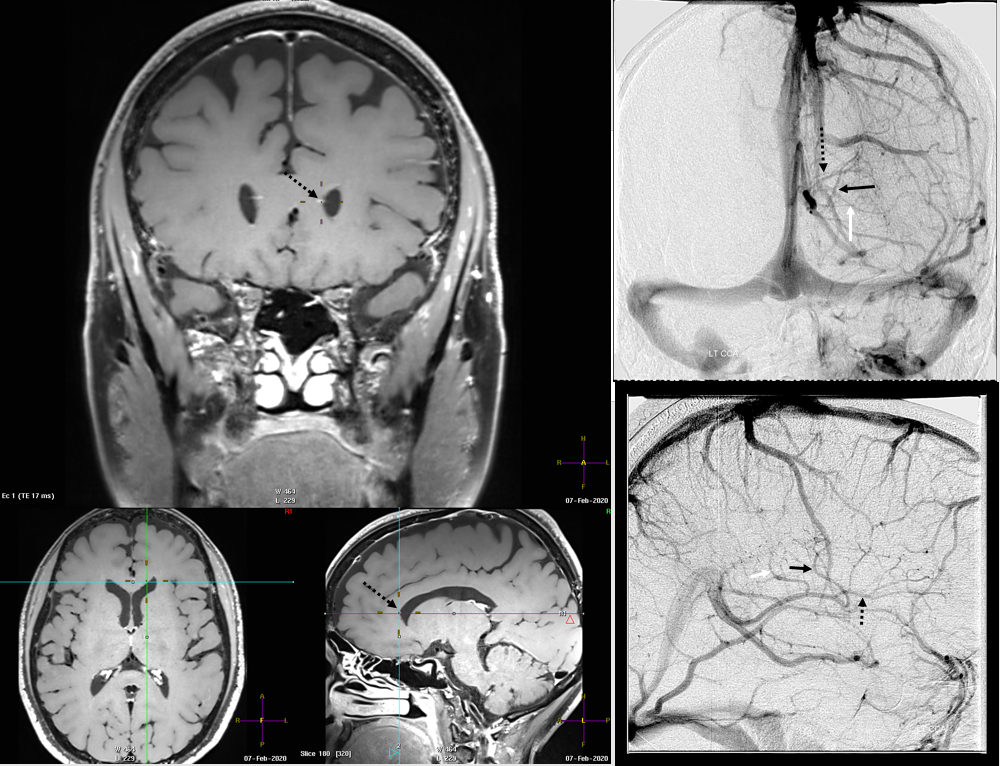
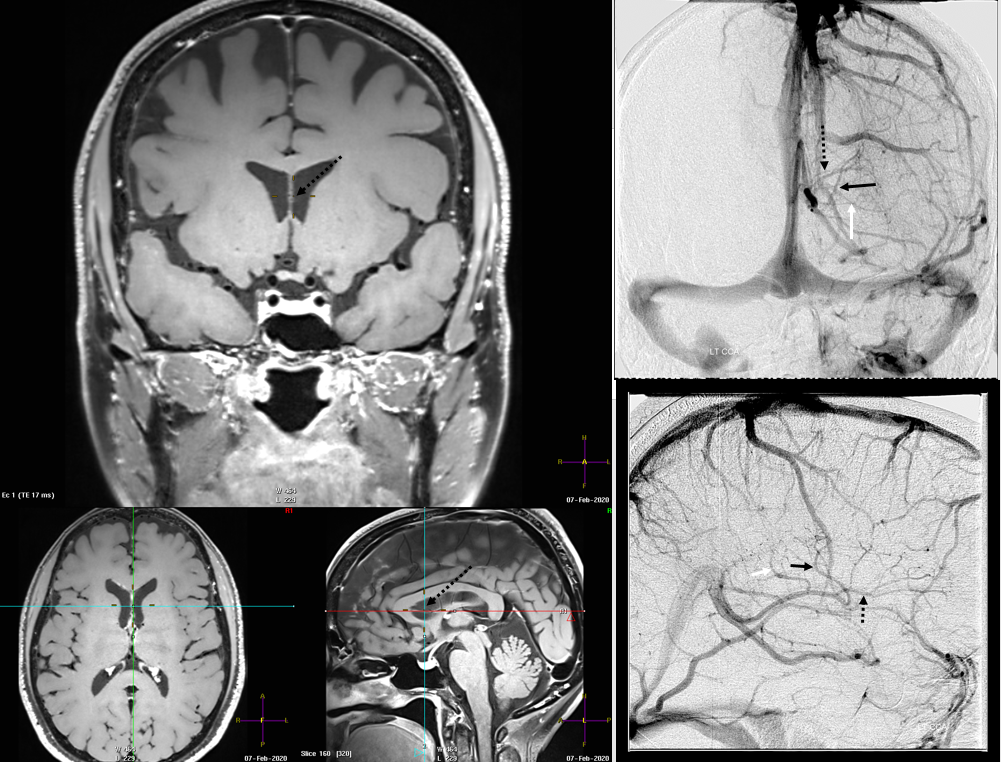
Straight Sinus Outflow Obstruction and Internal-Cerebral-Basal Vein Anastomoses
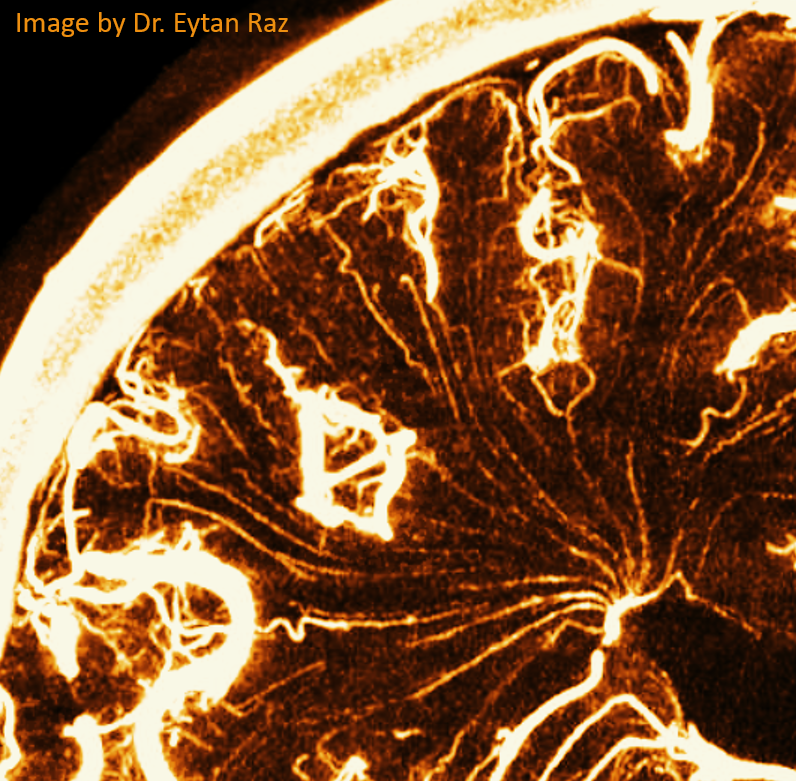
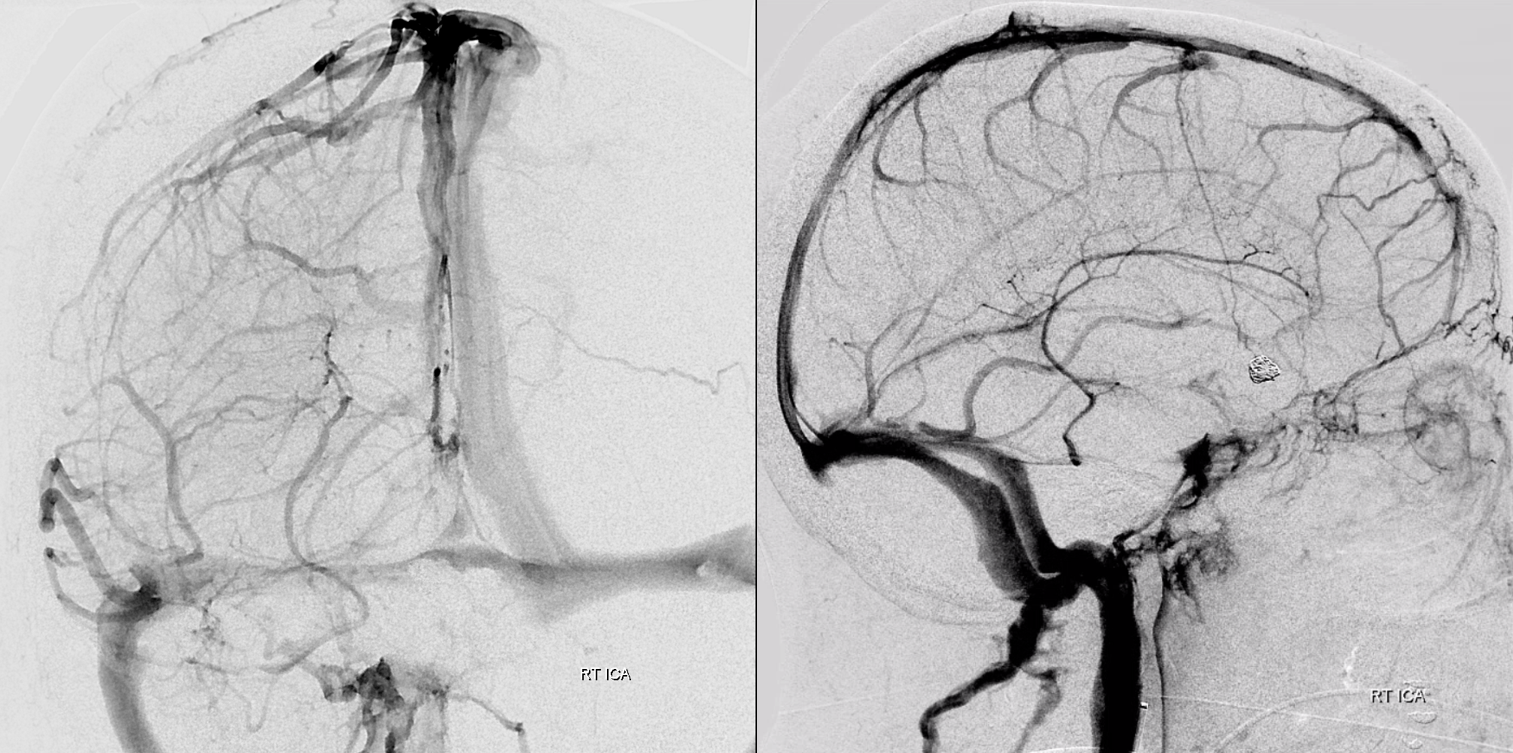
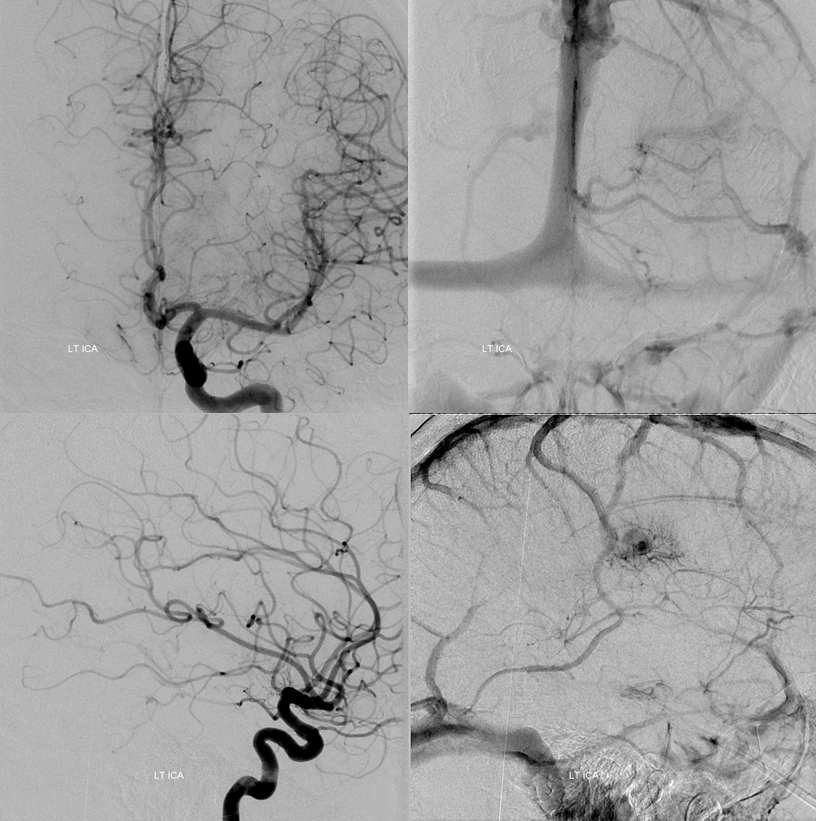
Obstruction of the Galen, especially acute (venous thrombosis) is often catastrophic, because of paucity of internal cerebral venous collaterals (see case here. Also see below for discussion of transmedullary veins). However, obstructions of straight sinus can be very well tolerated, because of the ICV-Galen-Basal Vein connection. The basal vein has more outflow potential (into cavernous sinus or lateral mesencephalic veins for example). Below is an example of this disposition, case of Drs. Eytan Raz and Maria Borja Angulo.
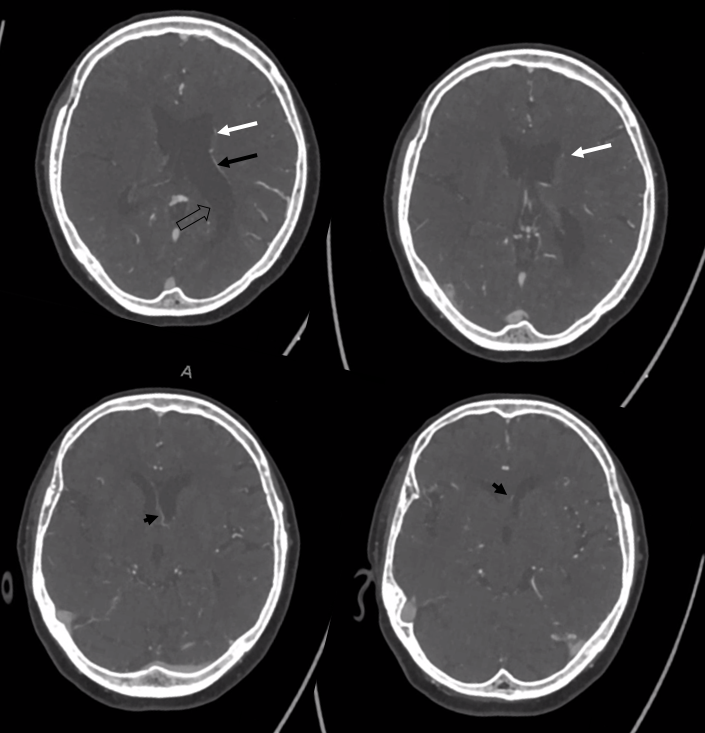
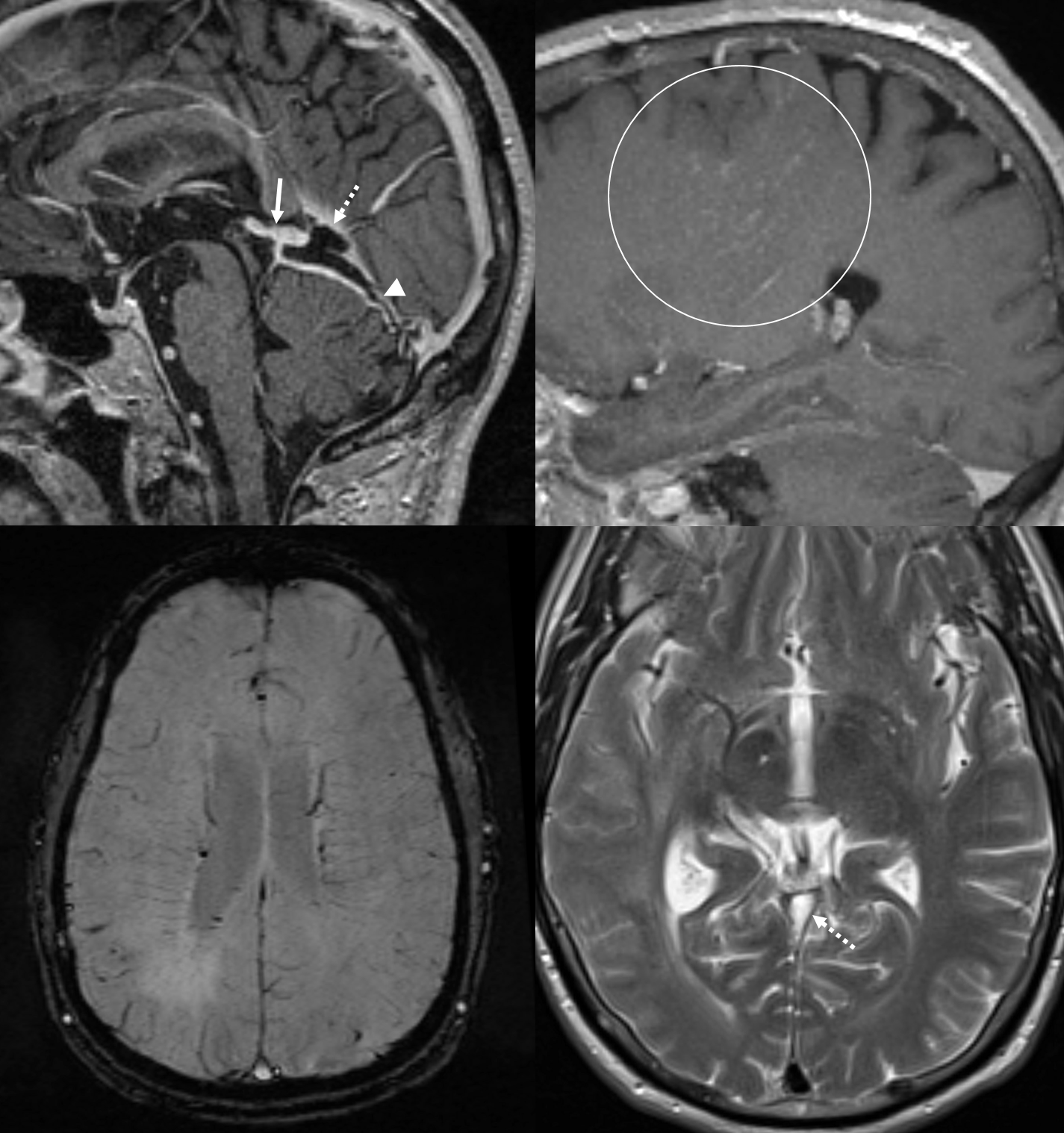
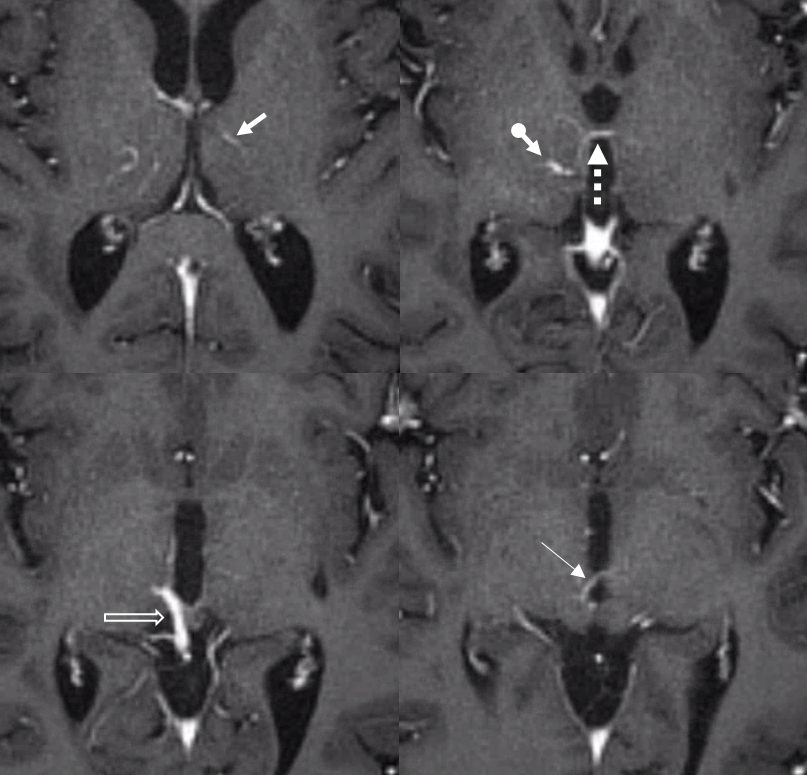
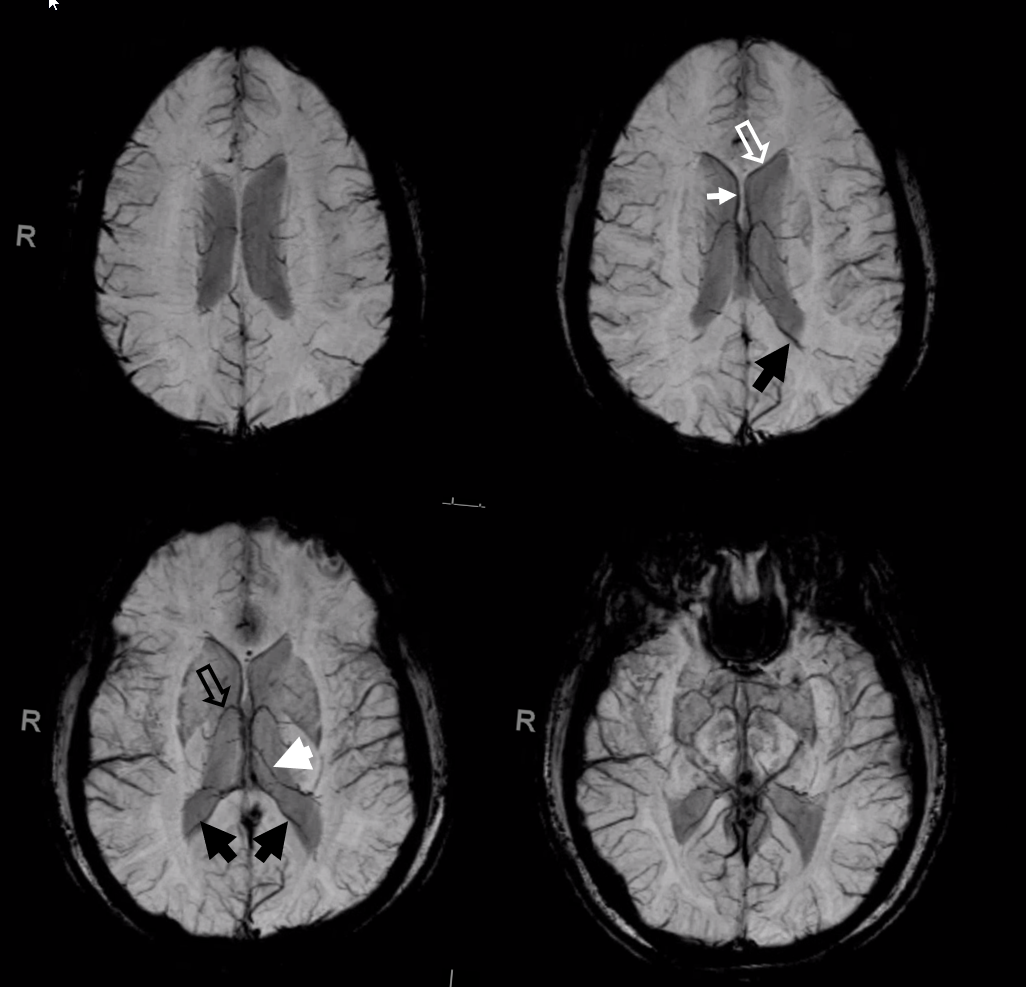
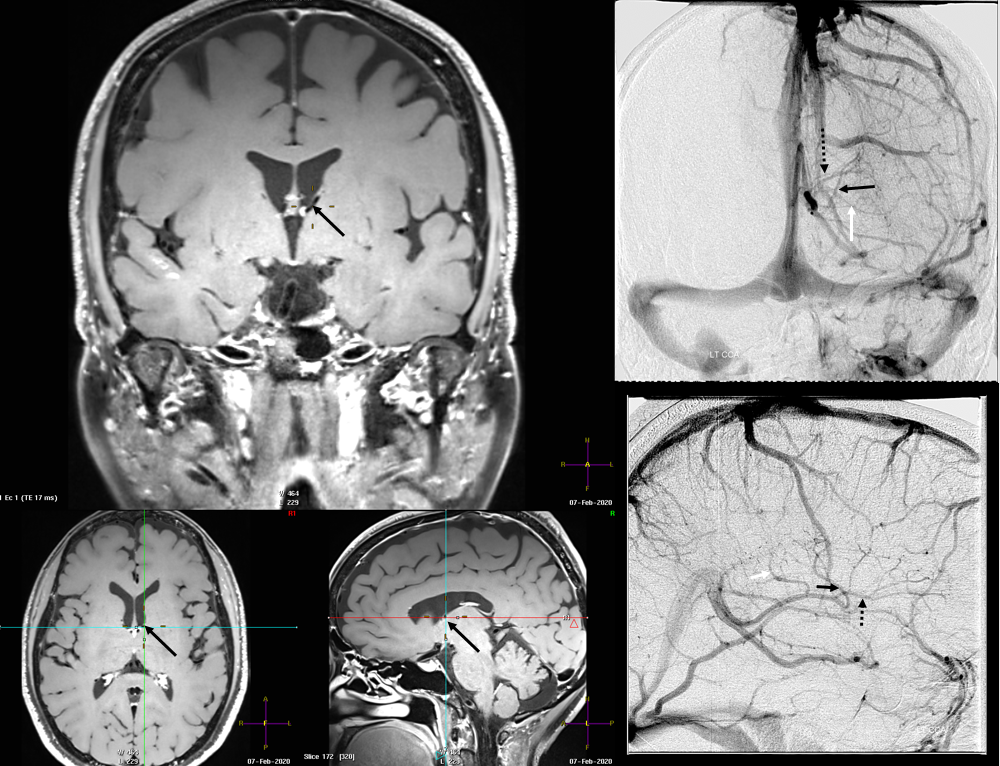
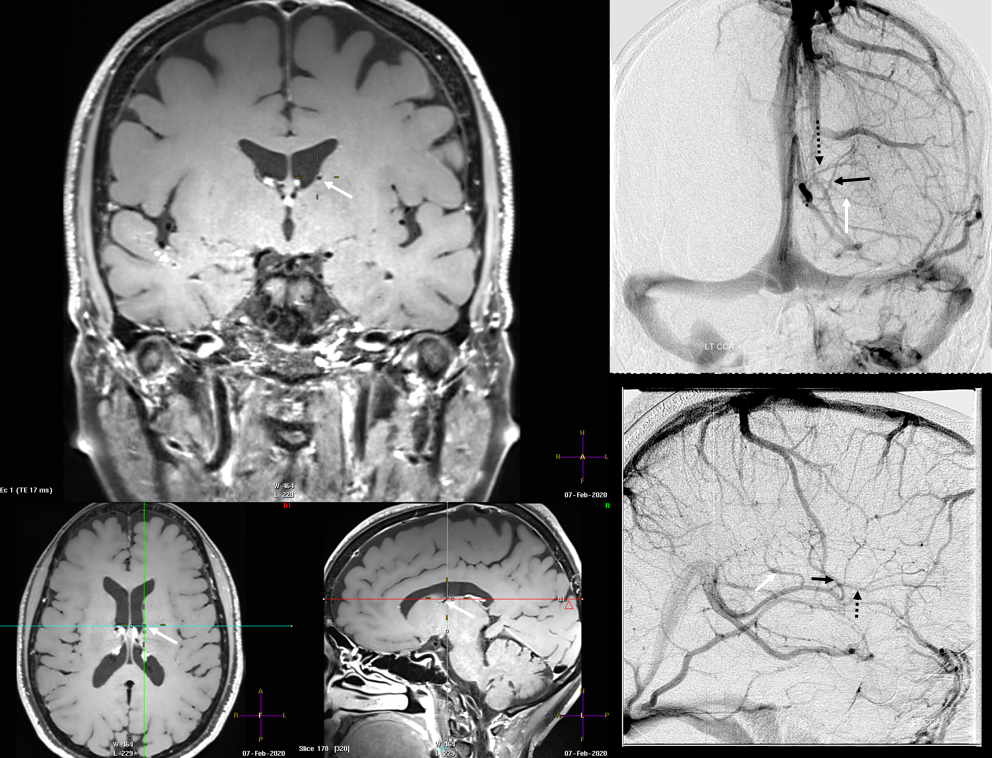
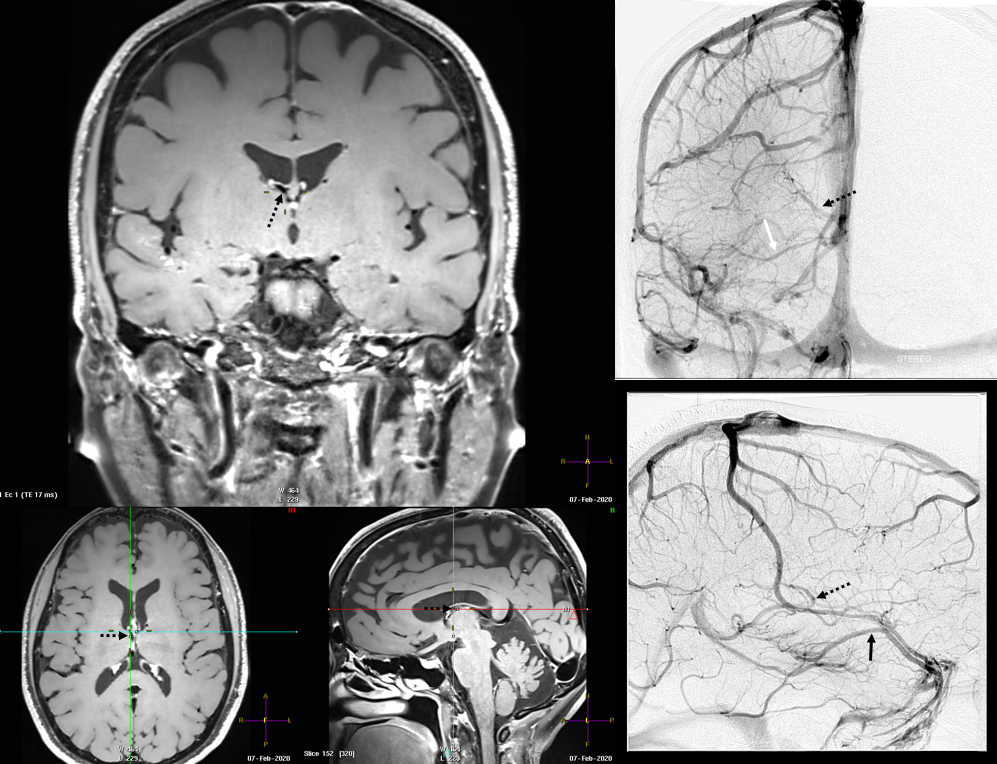
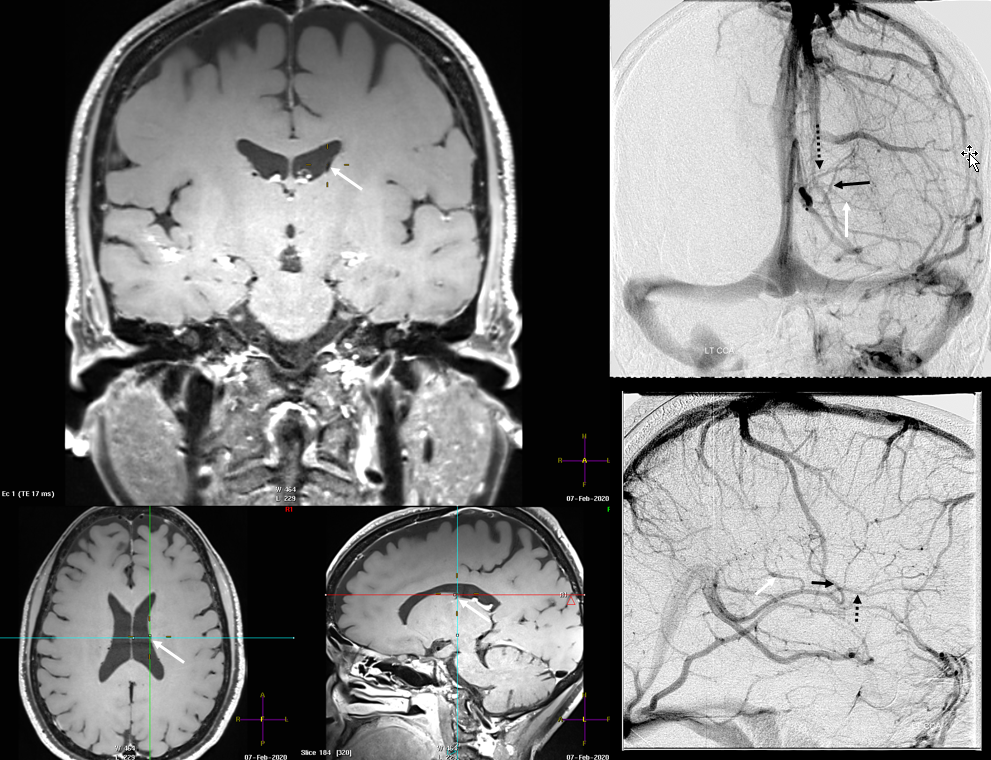
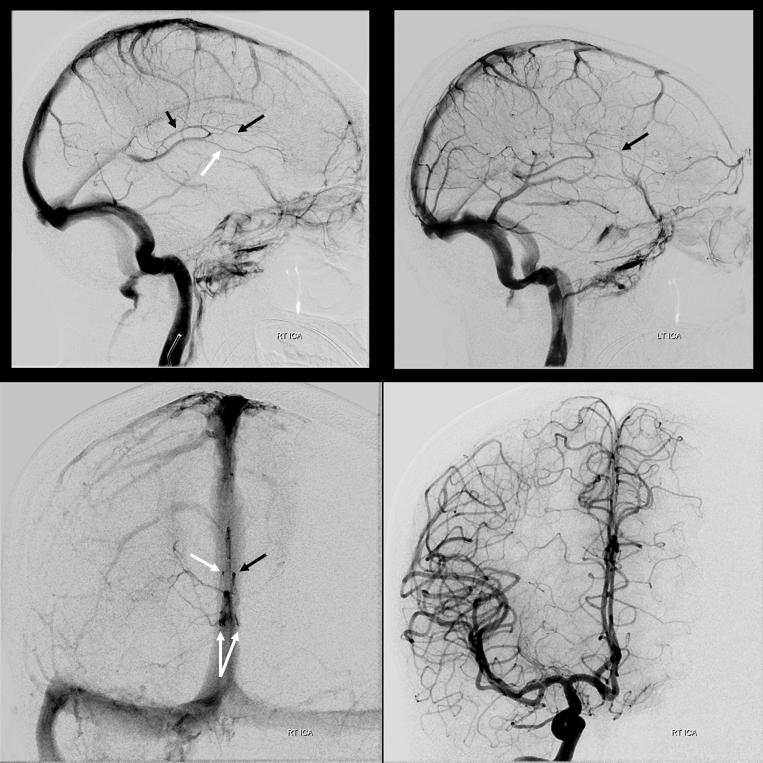
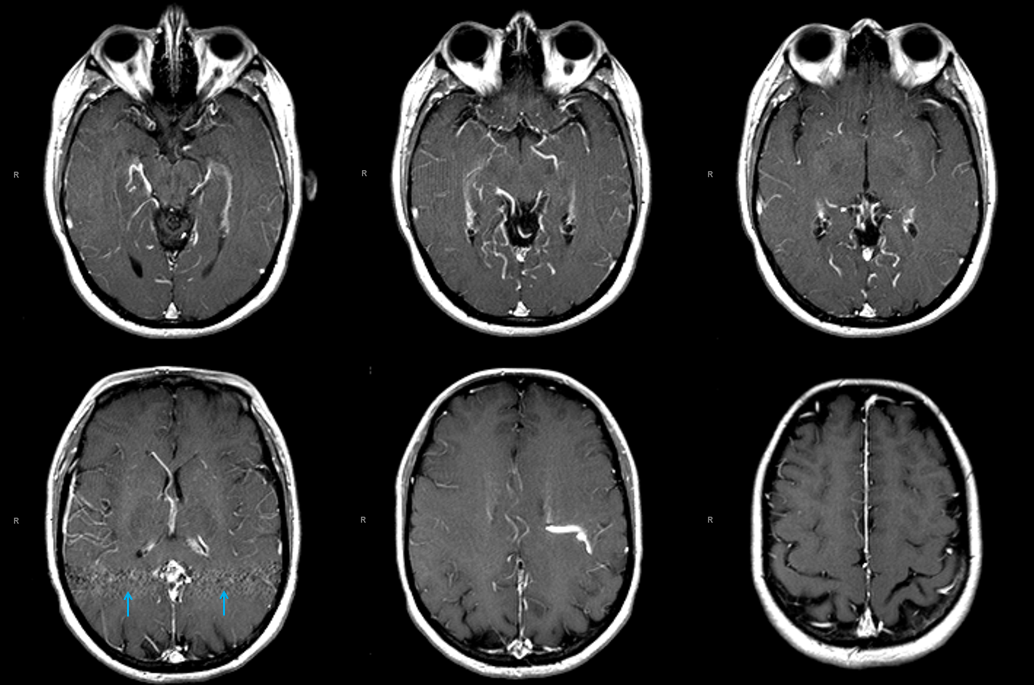
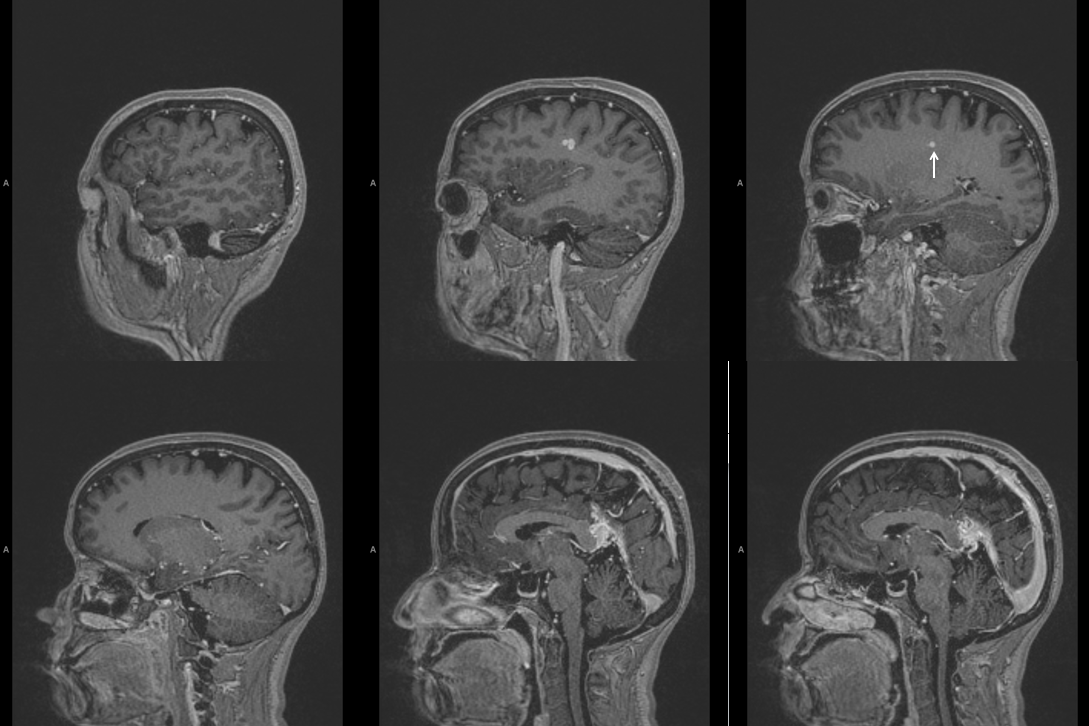
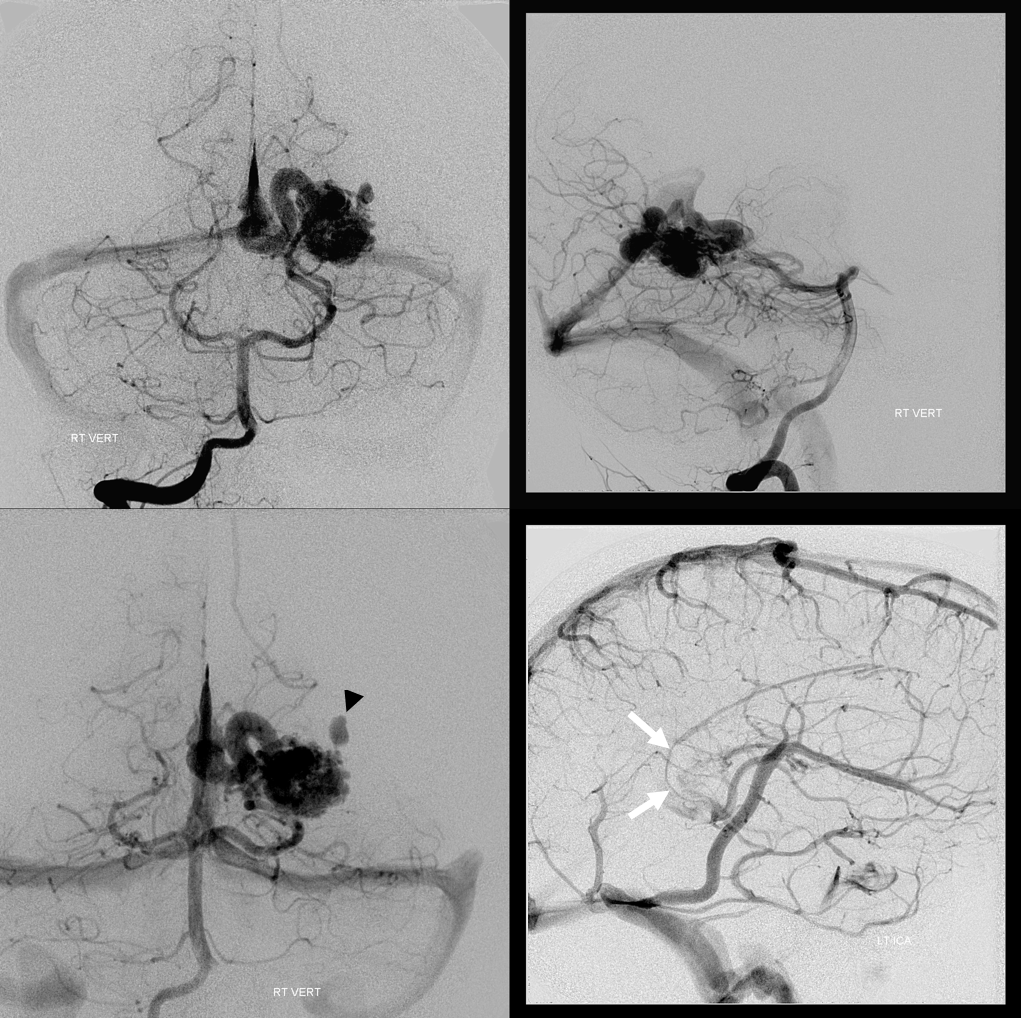
MRI: prominence of medullary veins (circle), normal size Galen (arrow), hypoplastic straight sinus (arrowhead), and a granulation/nodule structure in the distal straight sinus (dashed arrow).
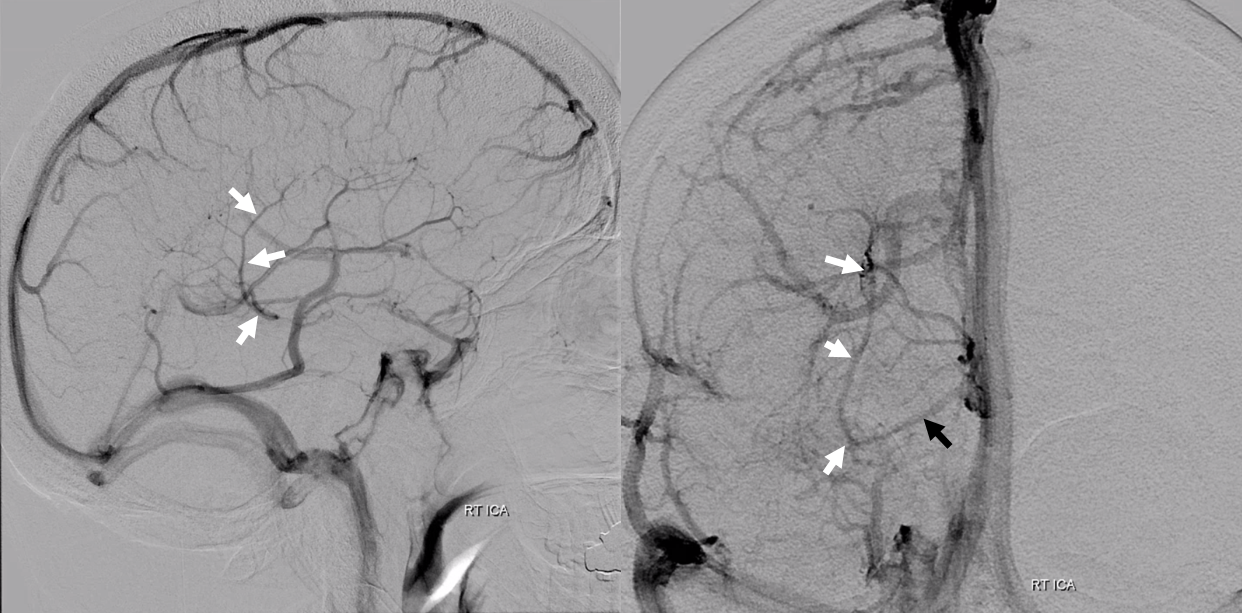
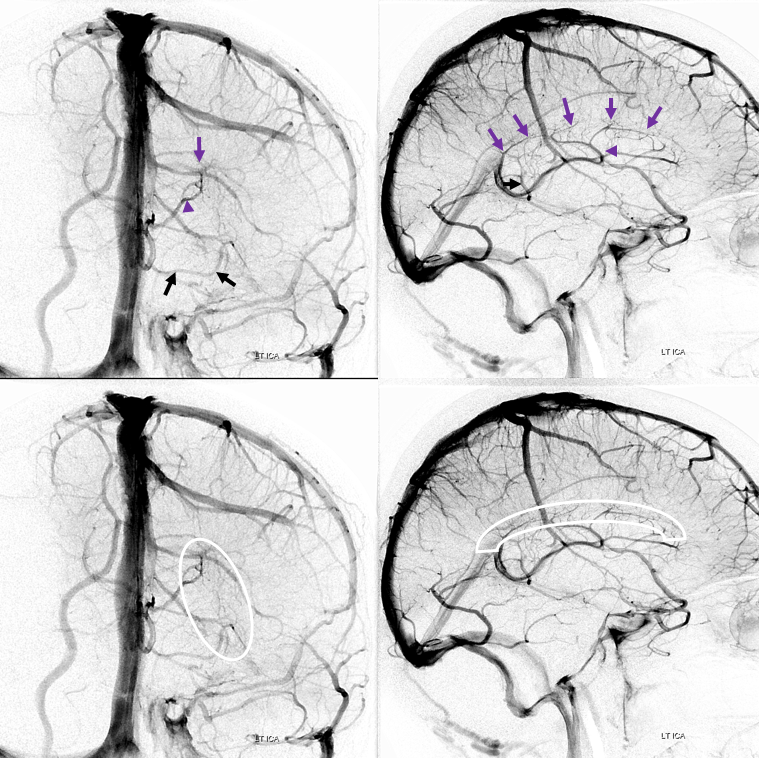
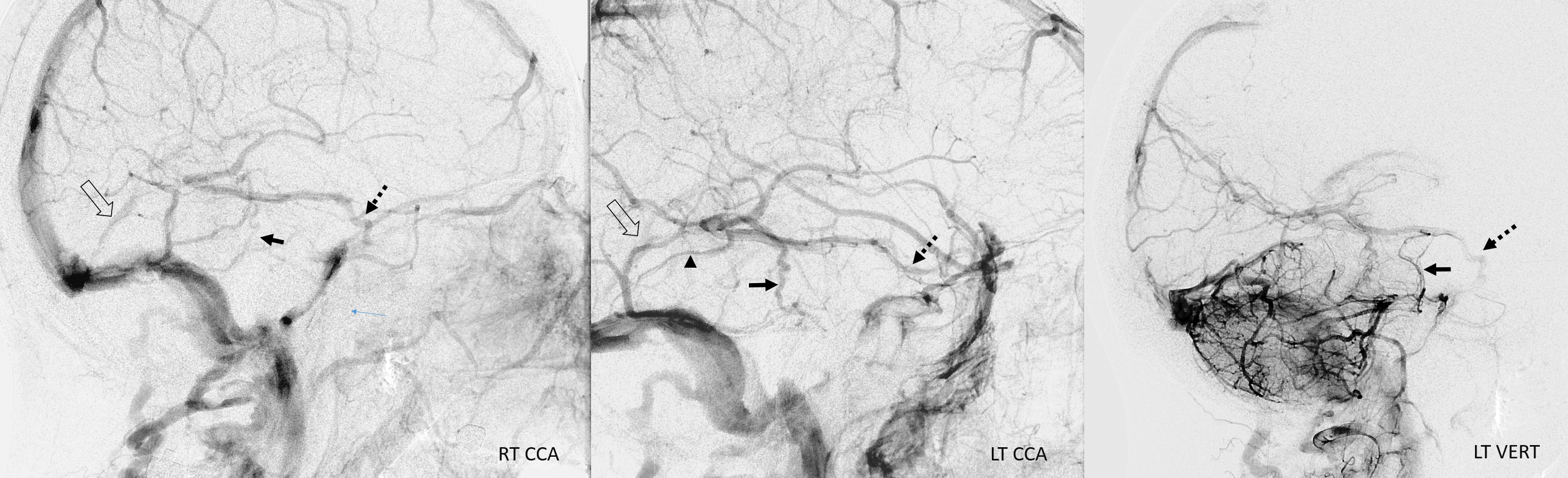
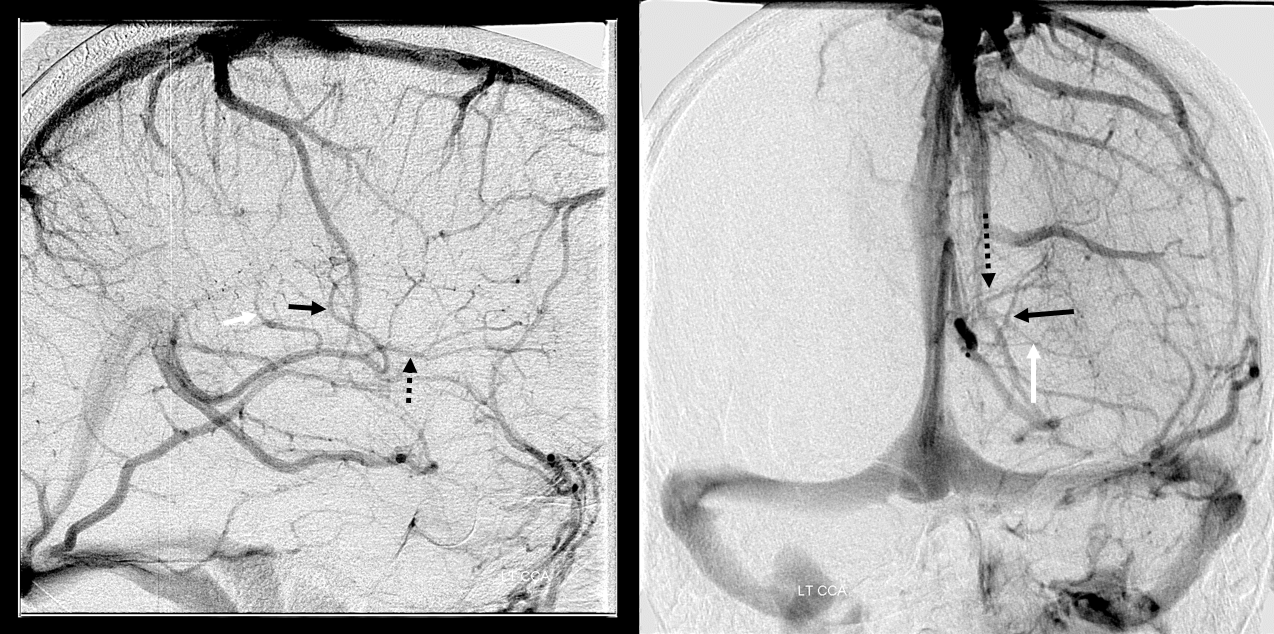
Angio — bilateral CCA and left vert injections. The straight sinus (open arrows) is hypoplastic. Bilateral ICVs drain via bilateral basal veins, into the lateral mesencephalic veins (arrows), into the cavernous sinus via the telencephalic / anterior segment of basal vein (dashed arrows), and on the left via a tentorial sinus (arrowhead) into the sigmoid.
Right hemisphere. Note presence of diploic veins as well
Left hemisphere
Stereo cross eye
Deeper stereos
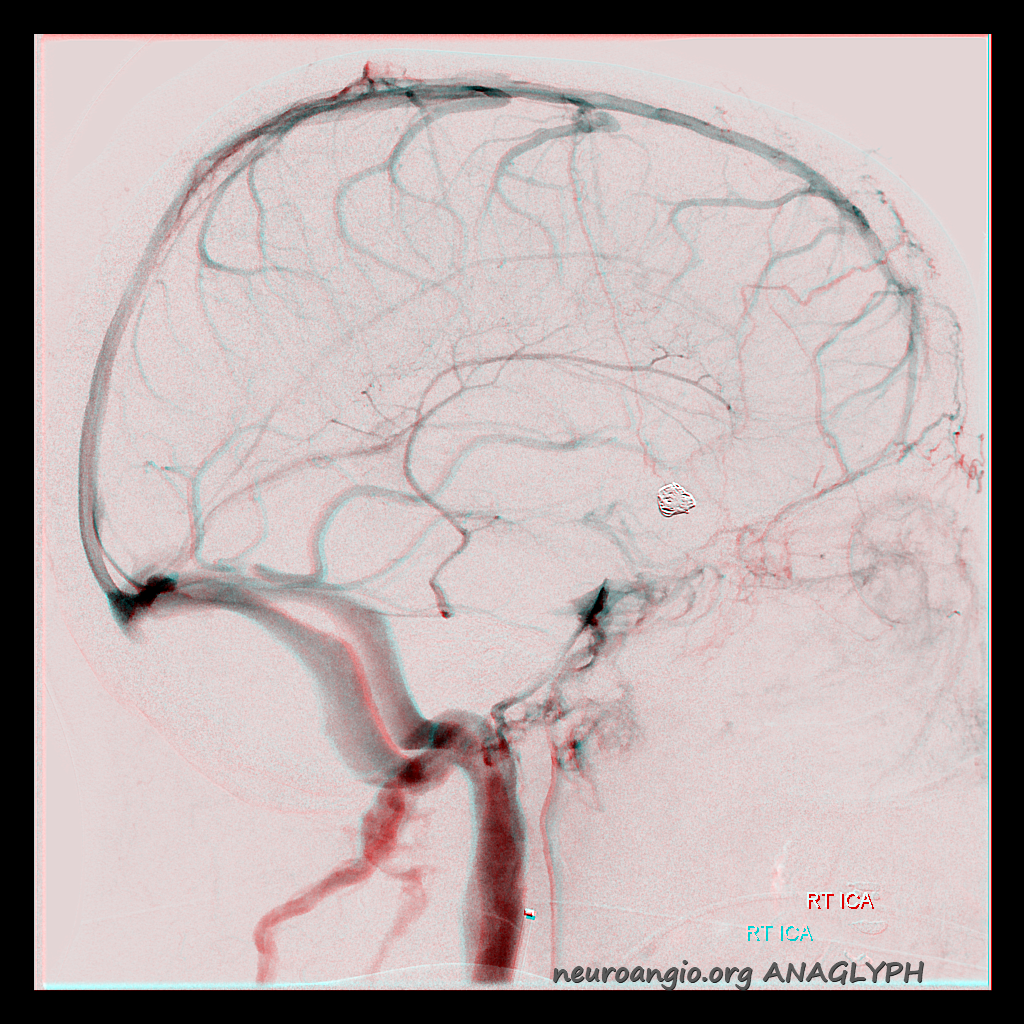
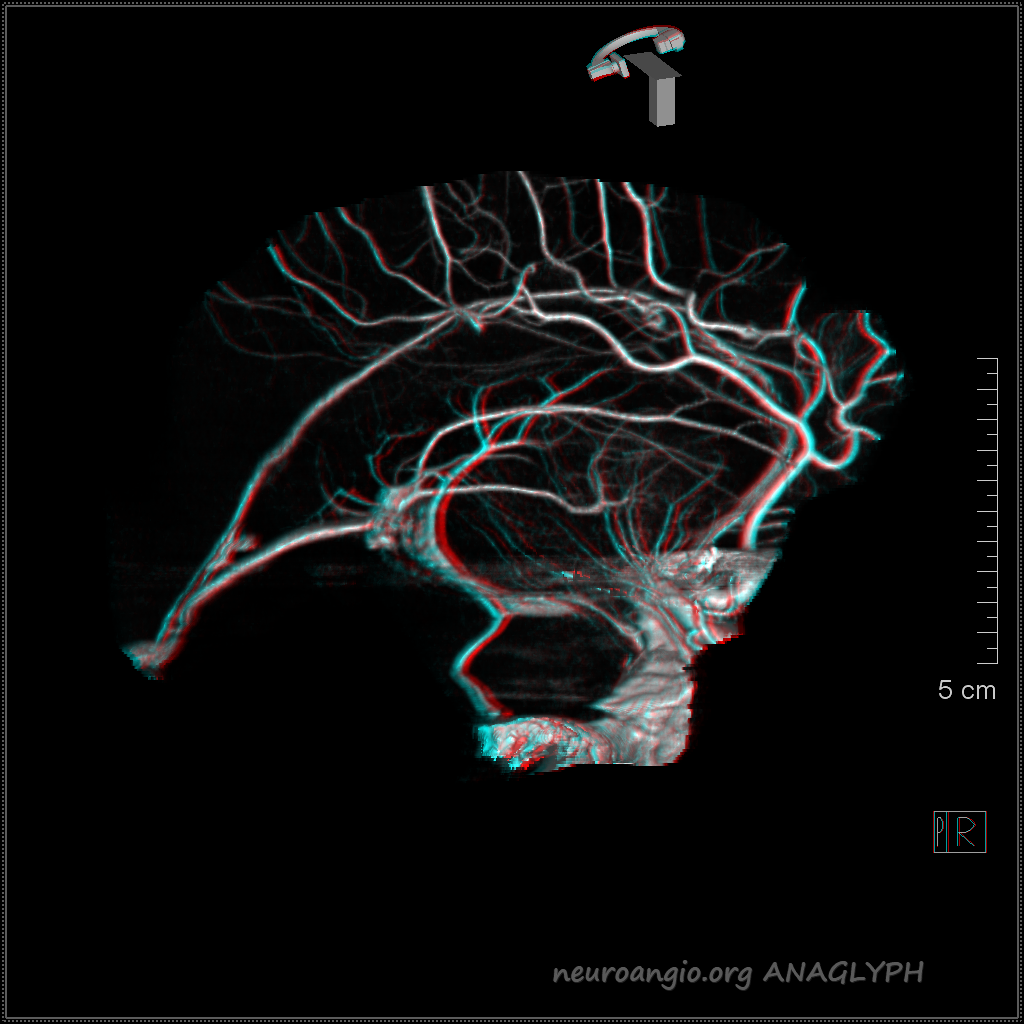
RT Anaglyph
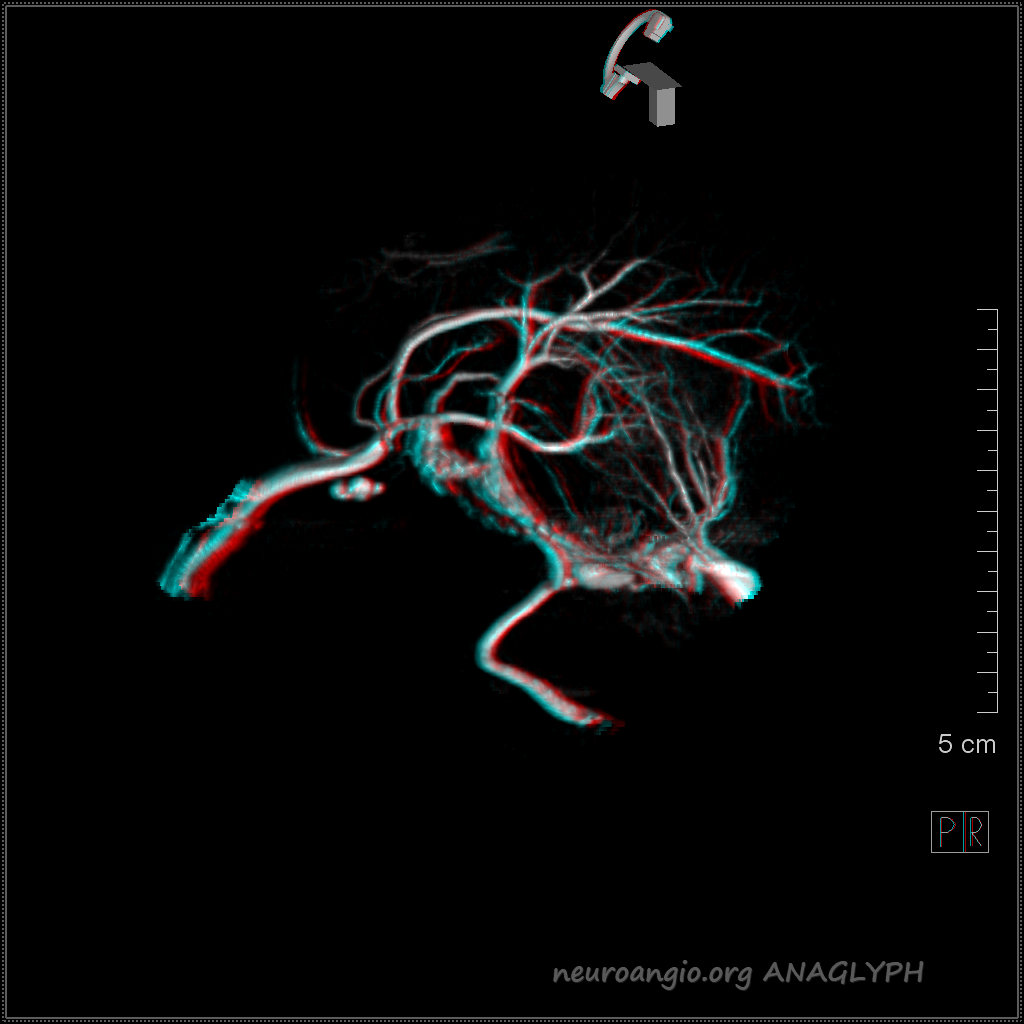
LT Anaglyph — arrow on the tentorial sinus
Superficial-Deep Venous System Balance
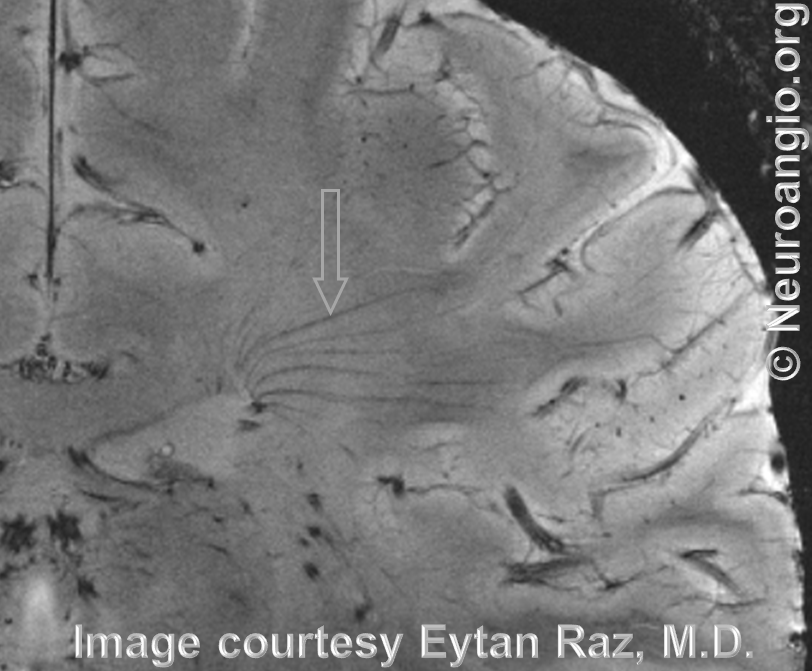
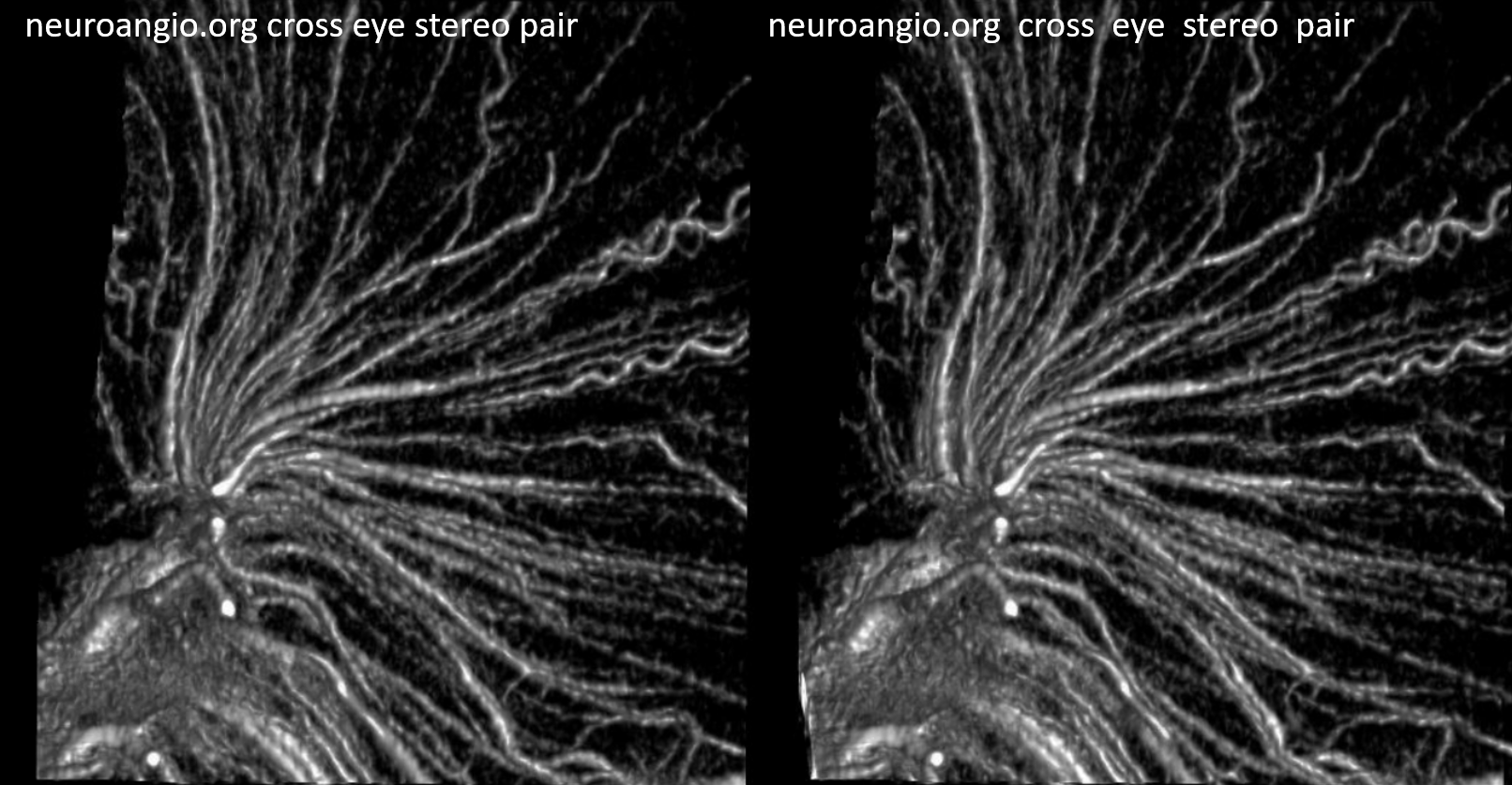
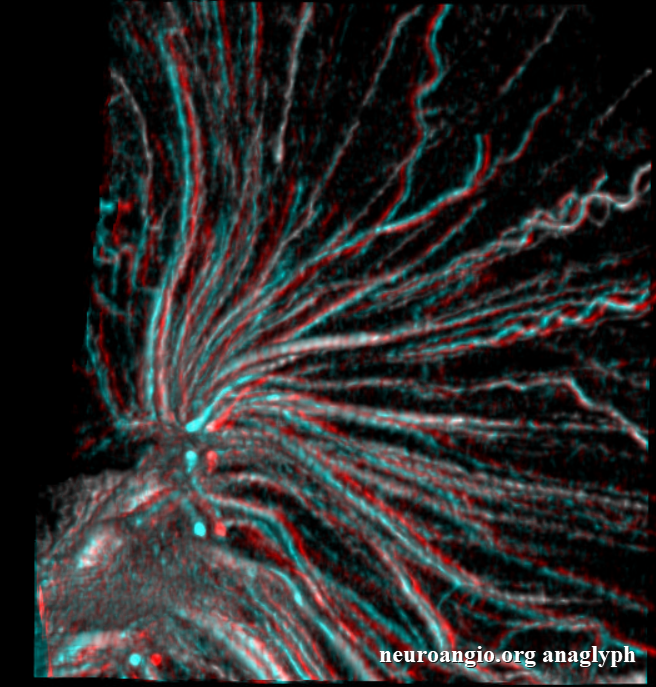
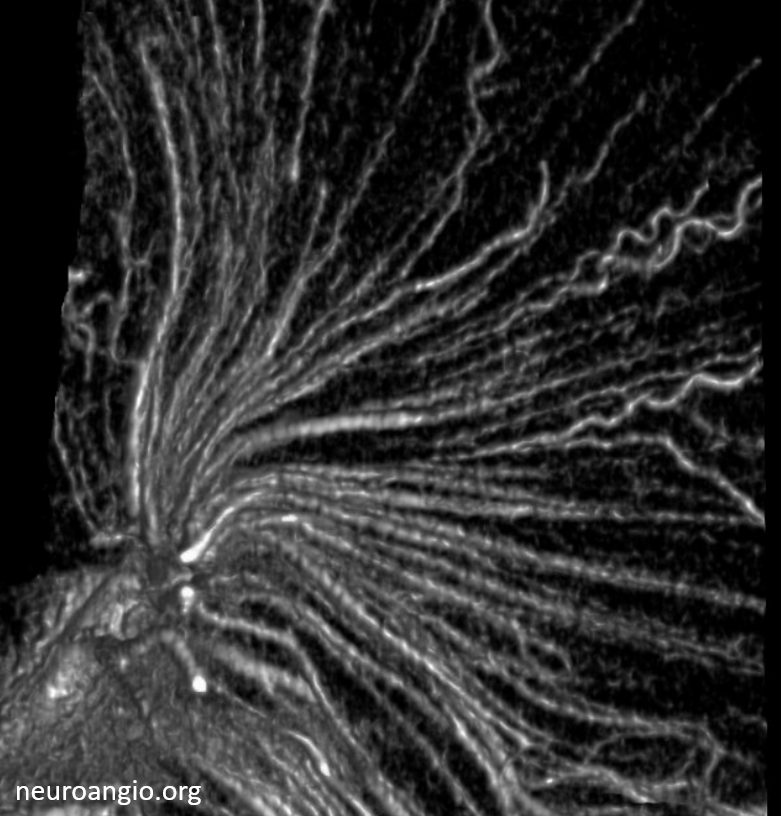
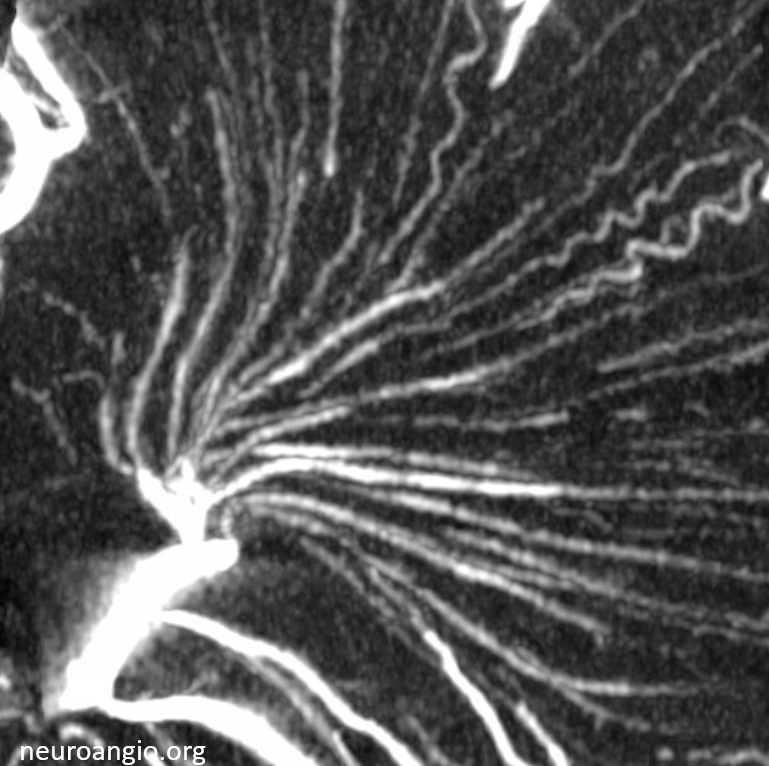
Just like there is a balance within the deep venous system, there is of course a balance between the superficial and deep systems. It is not very obvious at first. The connection are the transmedullary veins. Look at the veins traversing the white matter in stereo radiograph below
Here they are on a 7T MRI
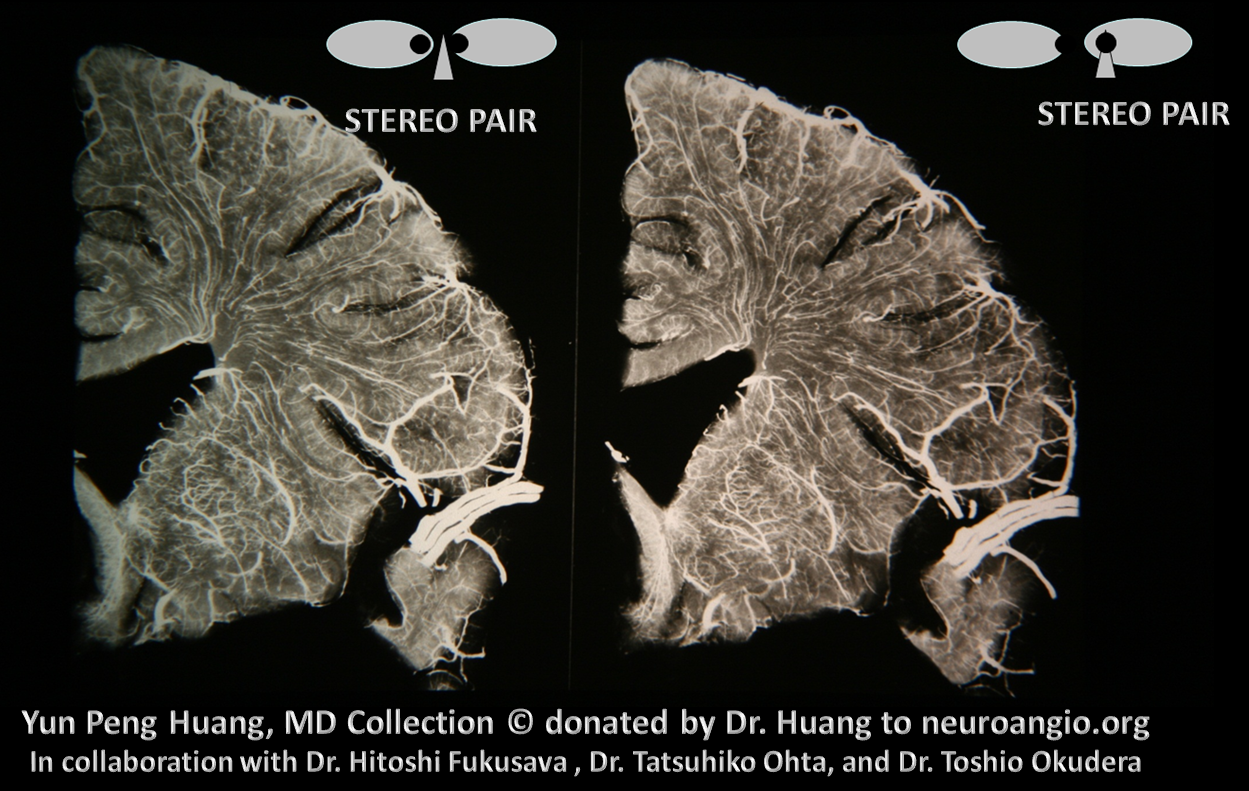
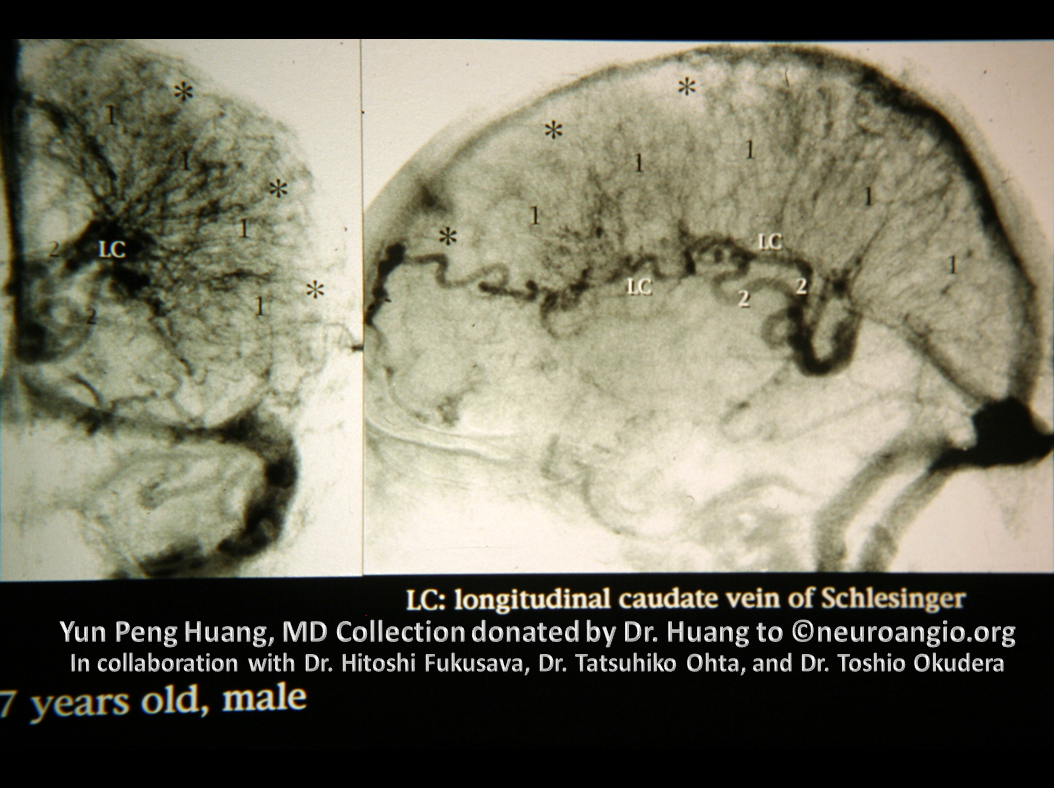
Yung Peng Huang — a masterpiece showing the balance of deep white matter drainage between superficial and deep systems
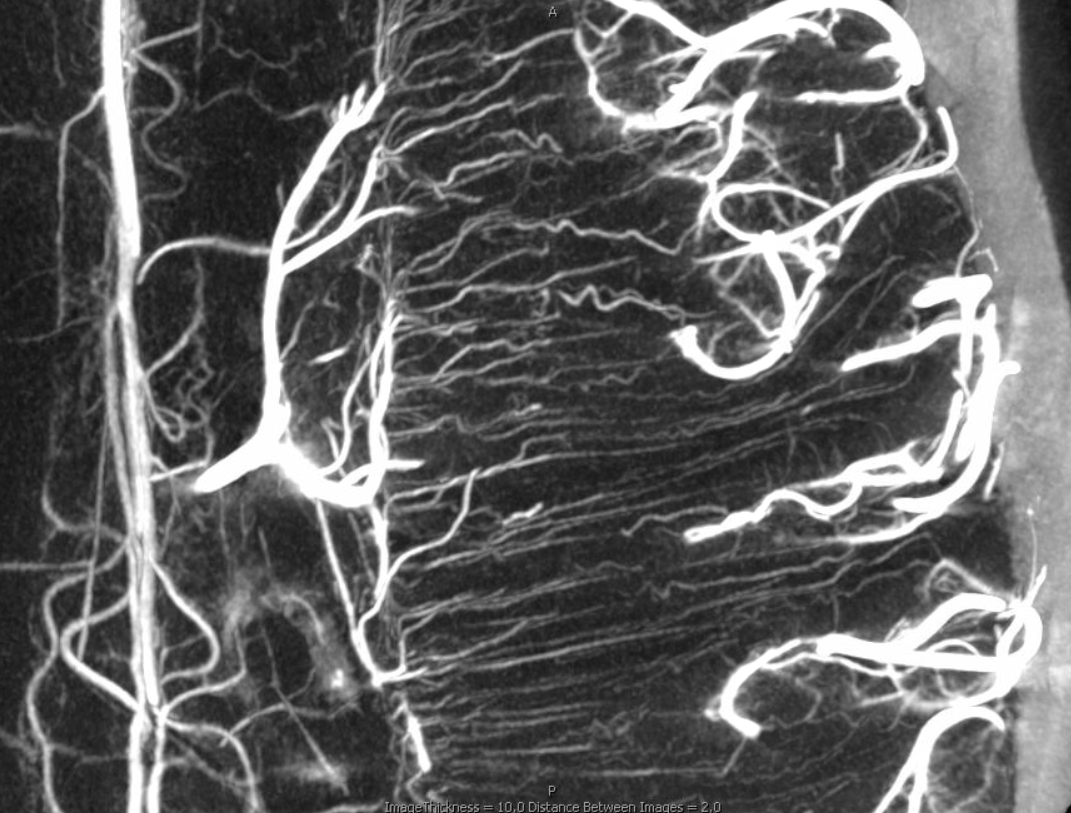
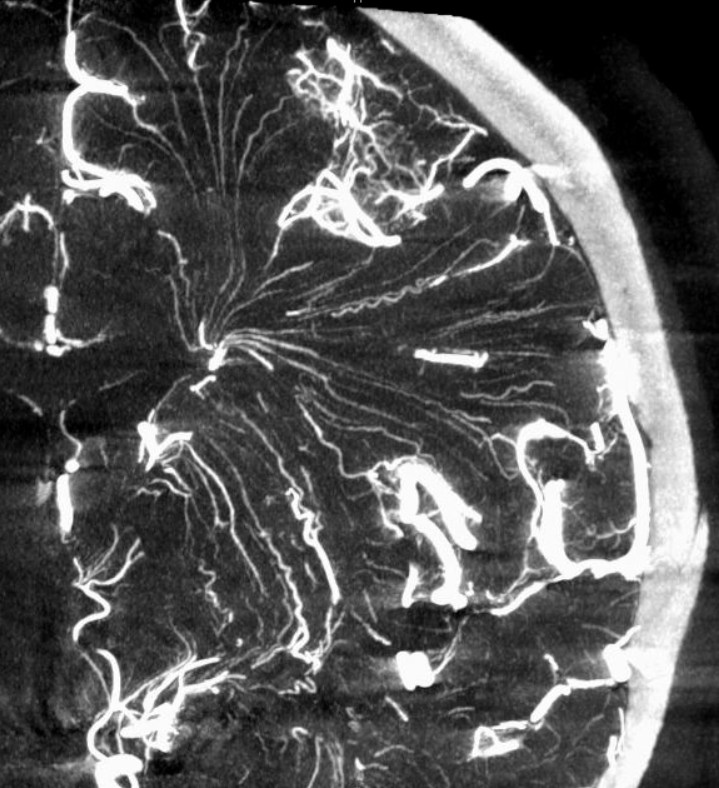
There are several ways to appreciate role of deep veins in balance. Here is a great example of transverse and longitudinal veins, courtesy Dr. Gopi Nayak. There is hypoplasia of the Superior Sagittal Sinus.
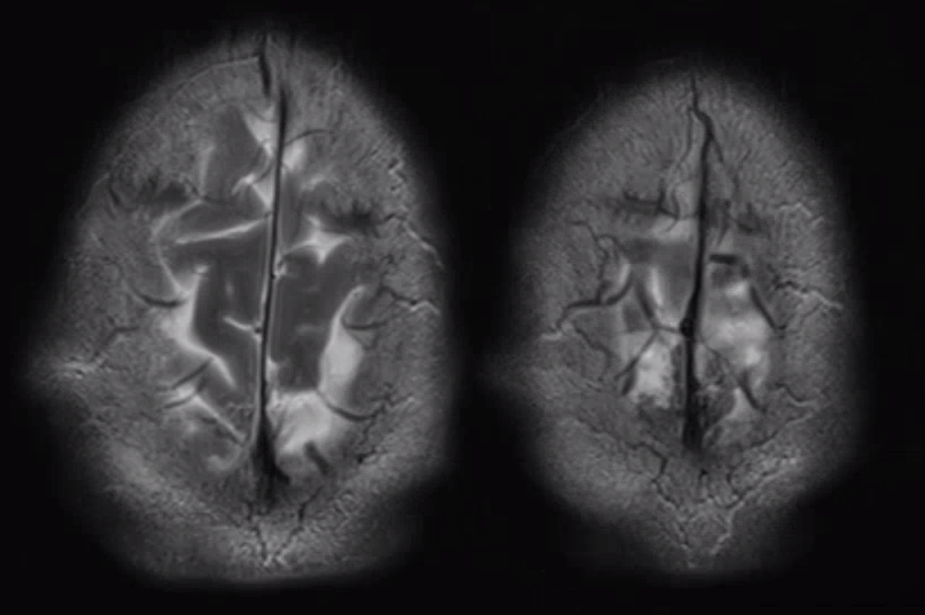
As one way of compensation for this superficial venous system deficiency, there is more venous drainage routed to the deep system. Amazing images of deep medullary/transverse venous prominence — completely nonpathologic, simply reflecting a shift of drainage equilibrium towards the deep venous system
Some arrows. Open white arrows — septal veins on the medial aspect of frontal horn. Thick white arrows — longitudinal caudate venous arcade. Black arrow — direct lateral vein, prominent because of hypoplasia of the posterior segment of the left longitudinal caudate vein. Thin white arrows are transverse/ medullary veins
Here is a diagrammatic way of showing the same thing
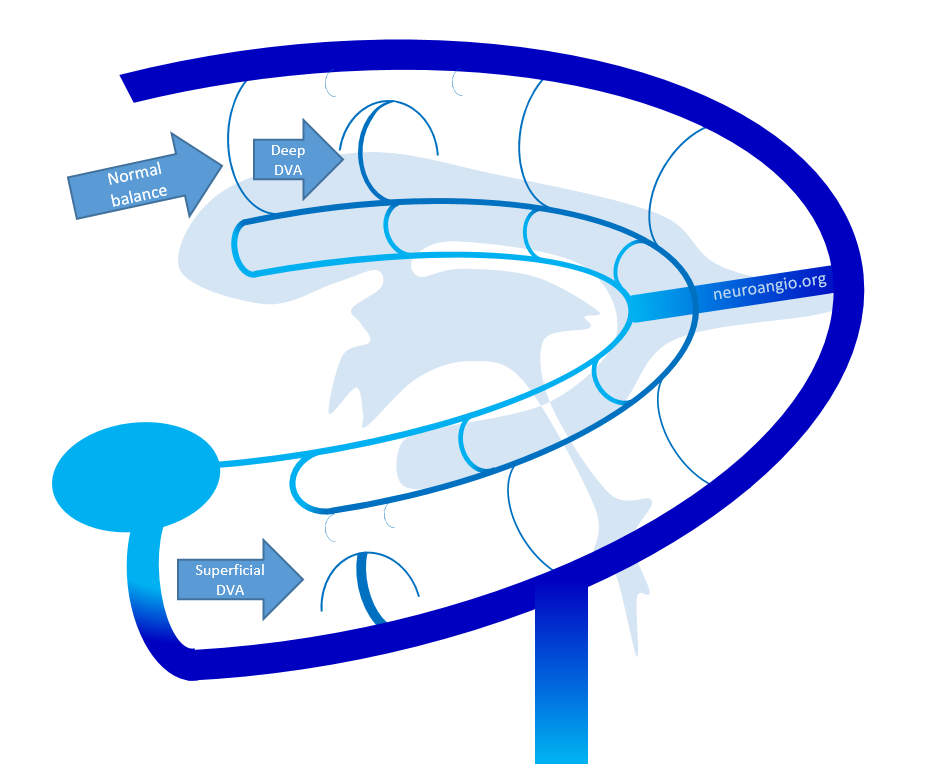
Developmental Venous Anomaly
Another great way to understand the grid-like longitudinal/transverse arrangement of veins is to study the Developmental Venous Anomaly, also known as DVA, or as (more appropriately but unfortunately relegated to obscurity) called by Yun Peng Huang the Medullary Venous Malformation. See dedicated page of this topic here.
Essentially, DVA represents a developmental drainage balance shift, where one transverse / medullary vein acts as a collector of adjacent medullary deep or superficial territory, secondary to developmental hypoplasia of superficial or deep component. The convergence of local/regional longitudinal veins onto this prominent transverse collector is the “caput medusa”. Below are some illustrations of this by Y.P. Huang. This is a diagram of normal disposition.
Here is a diagram of a DVA on right image
Another one of YPHs diagrams — in this case the superficial system “takes over” drainage of the deep system via the medullary venous system
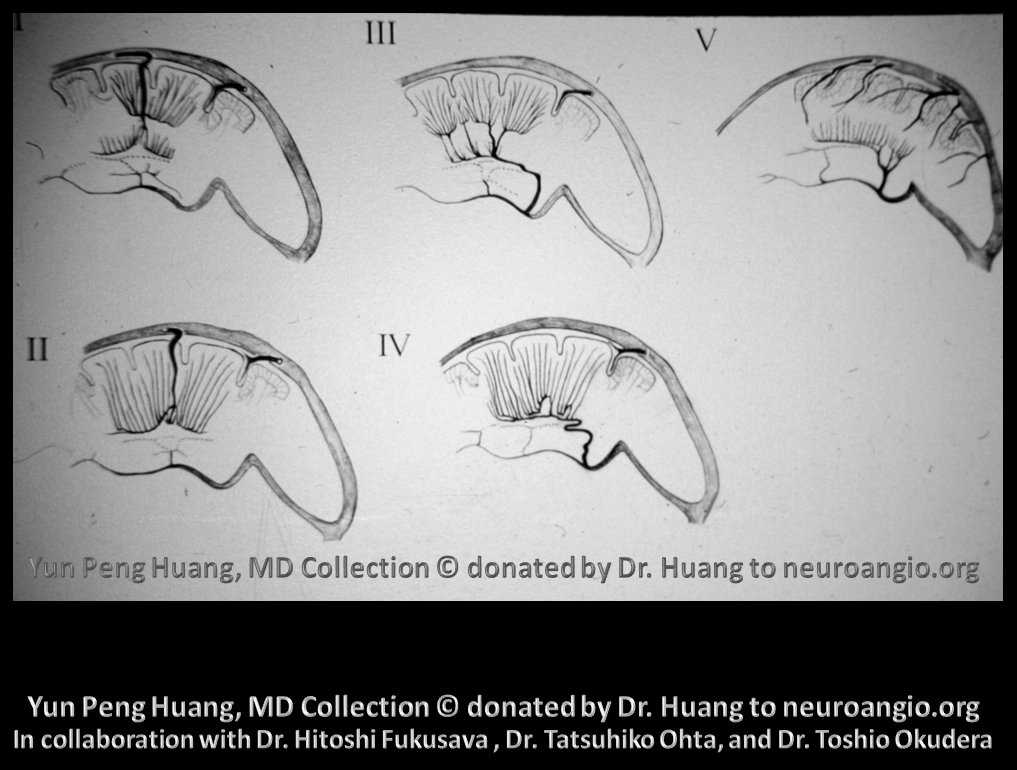
Here is the idea for both superficial and deep DVAs illustrated in another way
Here is a diagram by YPH and colleagues, of various DVAs illustrating deep/superficial balance — look at it from the transverse (medullary) and longitudinal venous perspective
Here are some examples from YPH library. A DVA of the direct lateral vein
A similar image to the case of SSS hypoplasia we showed on MRI — here we see SSS hypoplasia and consequent shift of drainage into the internal cerebral vein system on subtraction angiography
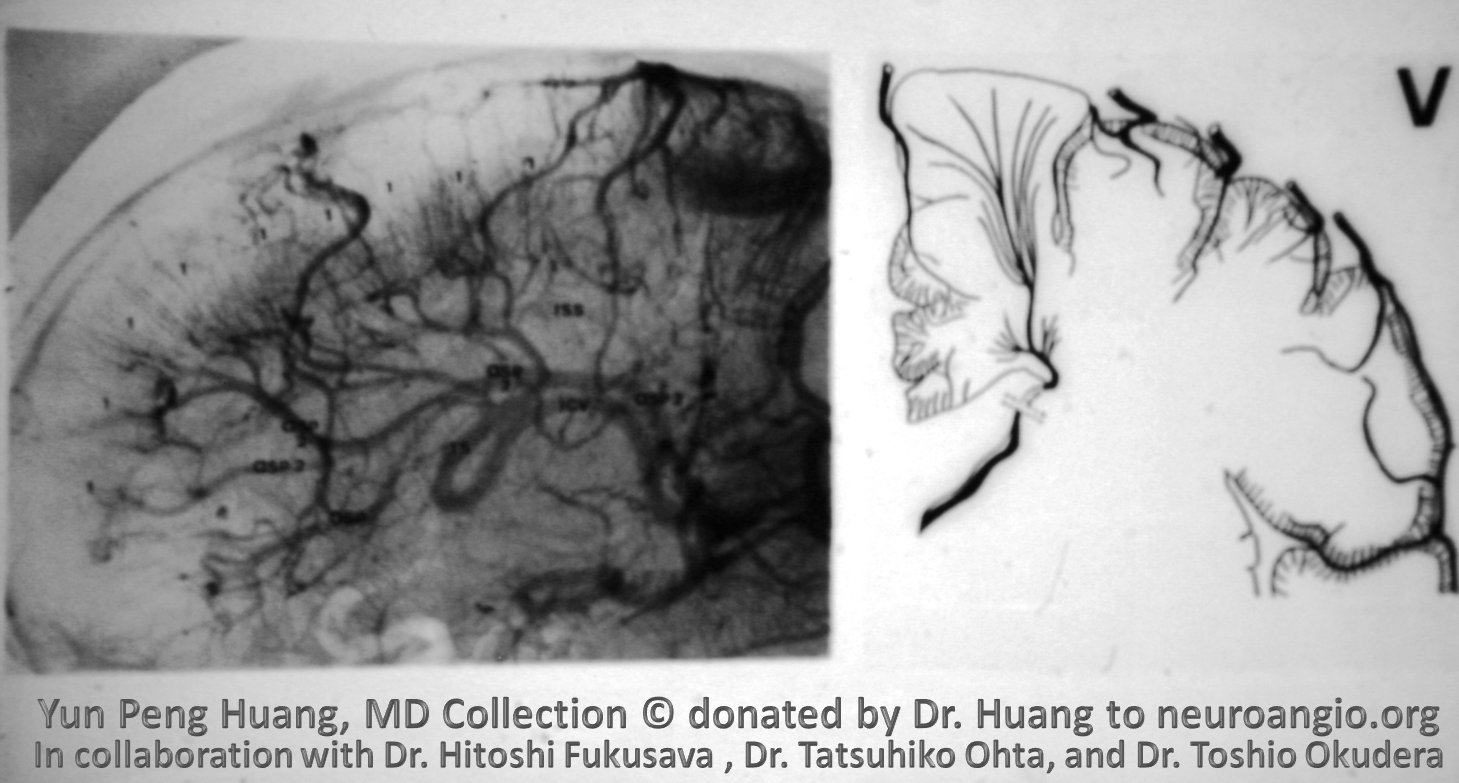
An absolutely insane DVA, with no visible internal cerebral vein (except for the most proximal part draining the lateral direct vein (9). Everything else is draining into the Rosenthal. Developmentally speaking, an absent internal cerebral vein, without Vein of Galen malformation, is extremely rare. Perhaps the most proximal internal cerebral vein-like remnant is actually the vein of Markowski. We dont have the other side. And who knows anyway?
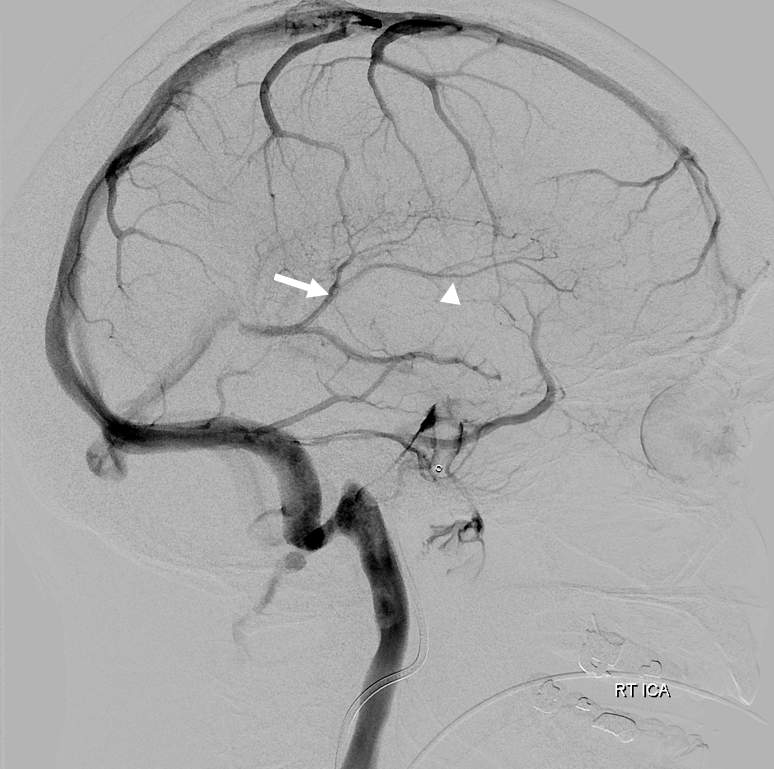
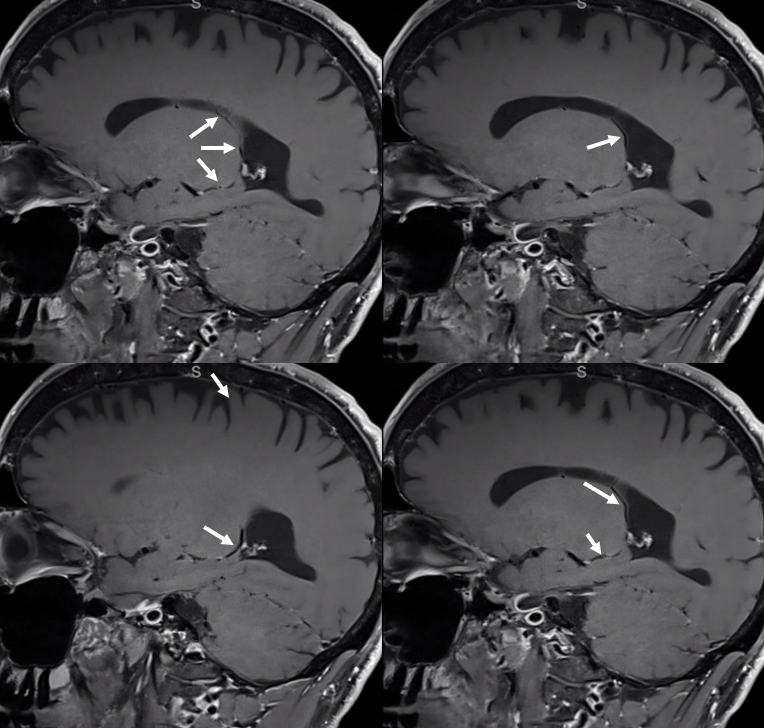
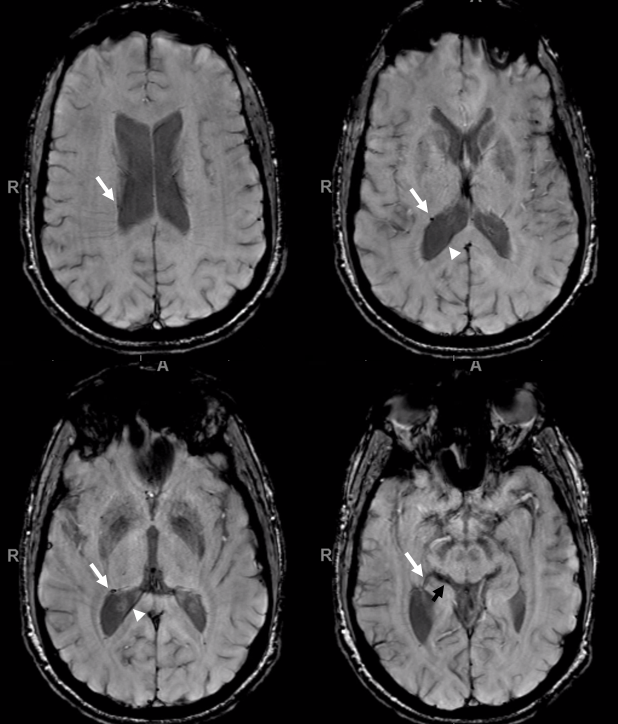
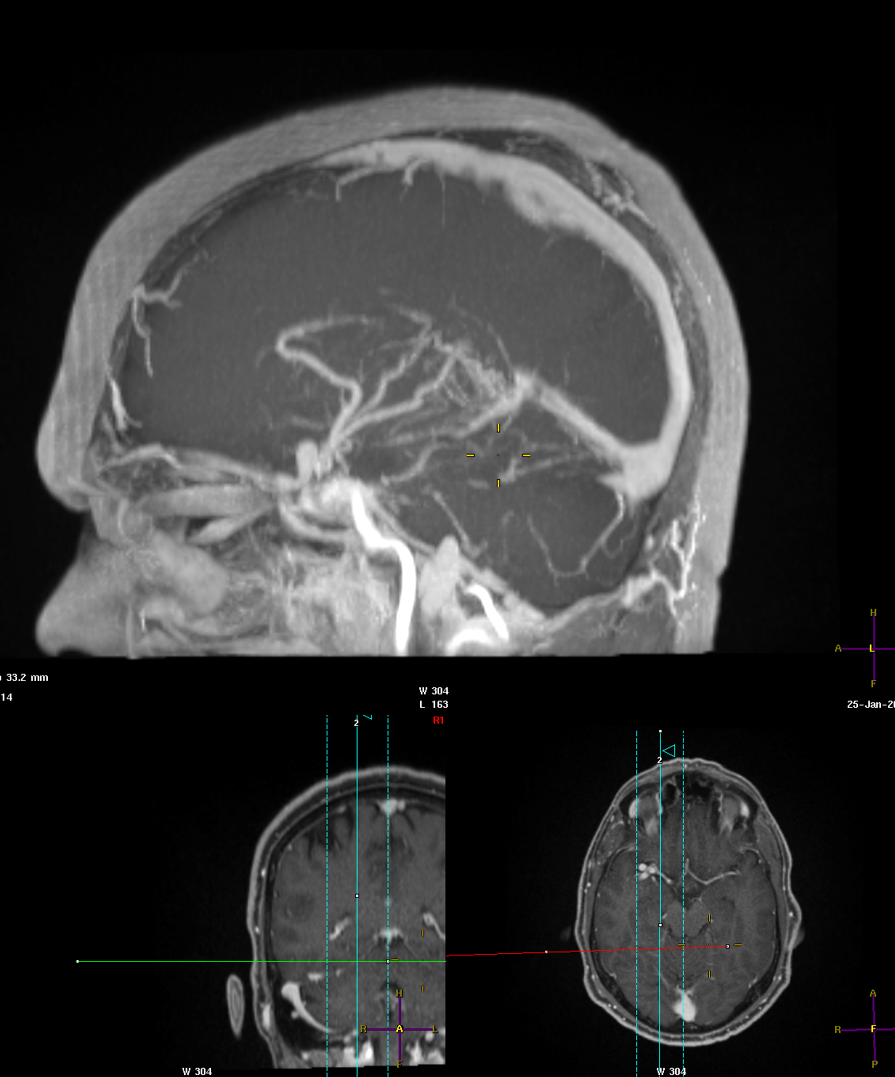
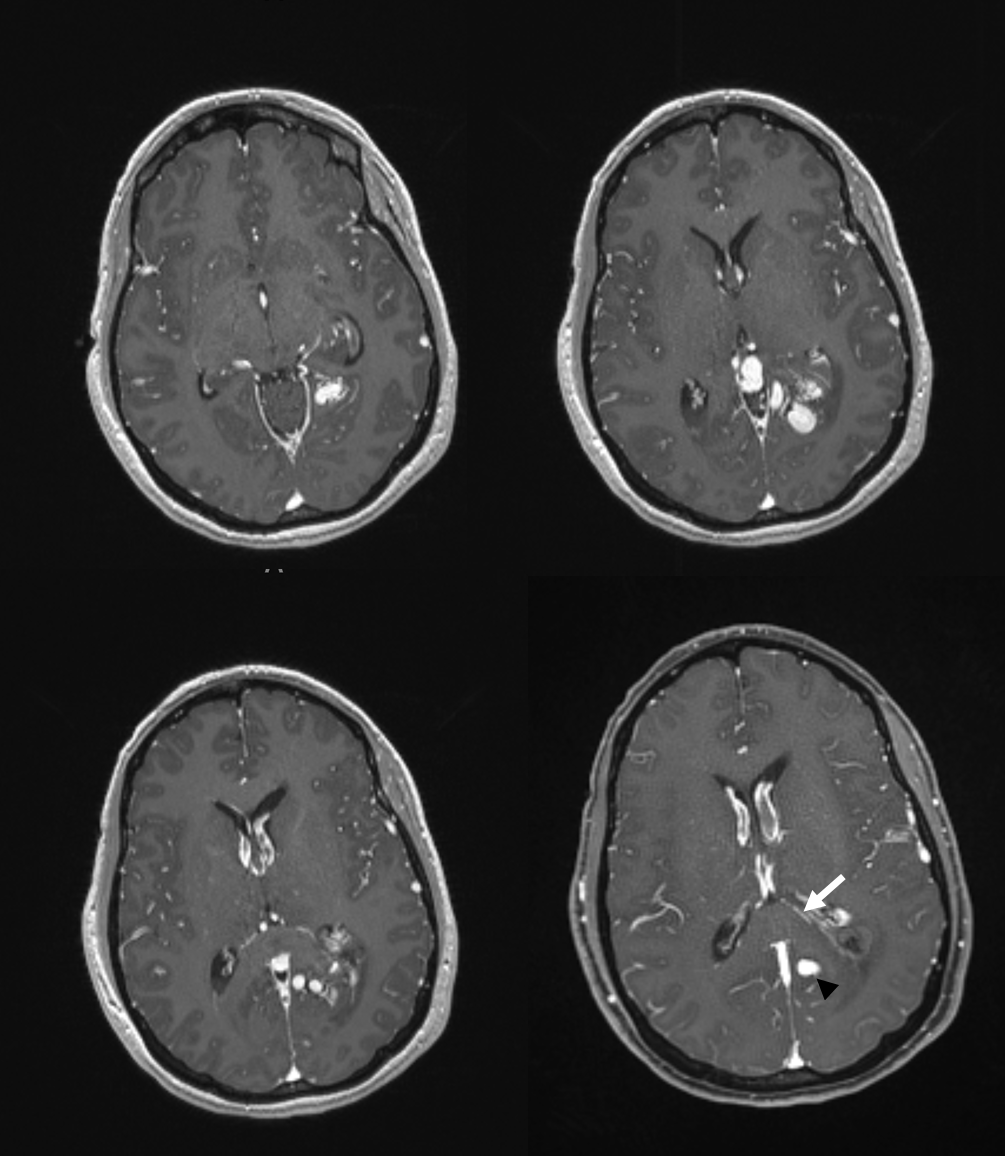
Here is a more recent MRI example, case courtesy Dr. Gopi Nayak. Huge DVA draining basically entire internal cerebral vein territory via lenticulostriate / inferior ventricular veins towards the laterocavernous sinus. And, again, the right internal cerebral vein (black arrow) is tiny — its drainage is basically limited to the medial (septal) territory. Normal left ICV is white arrow. I must say, Huang’s angio still looks cooler. But our MRI DVA is even bigger.
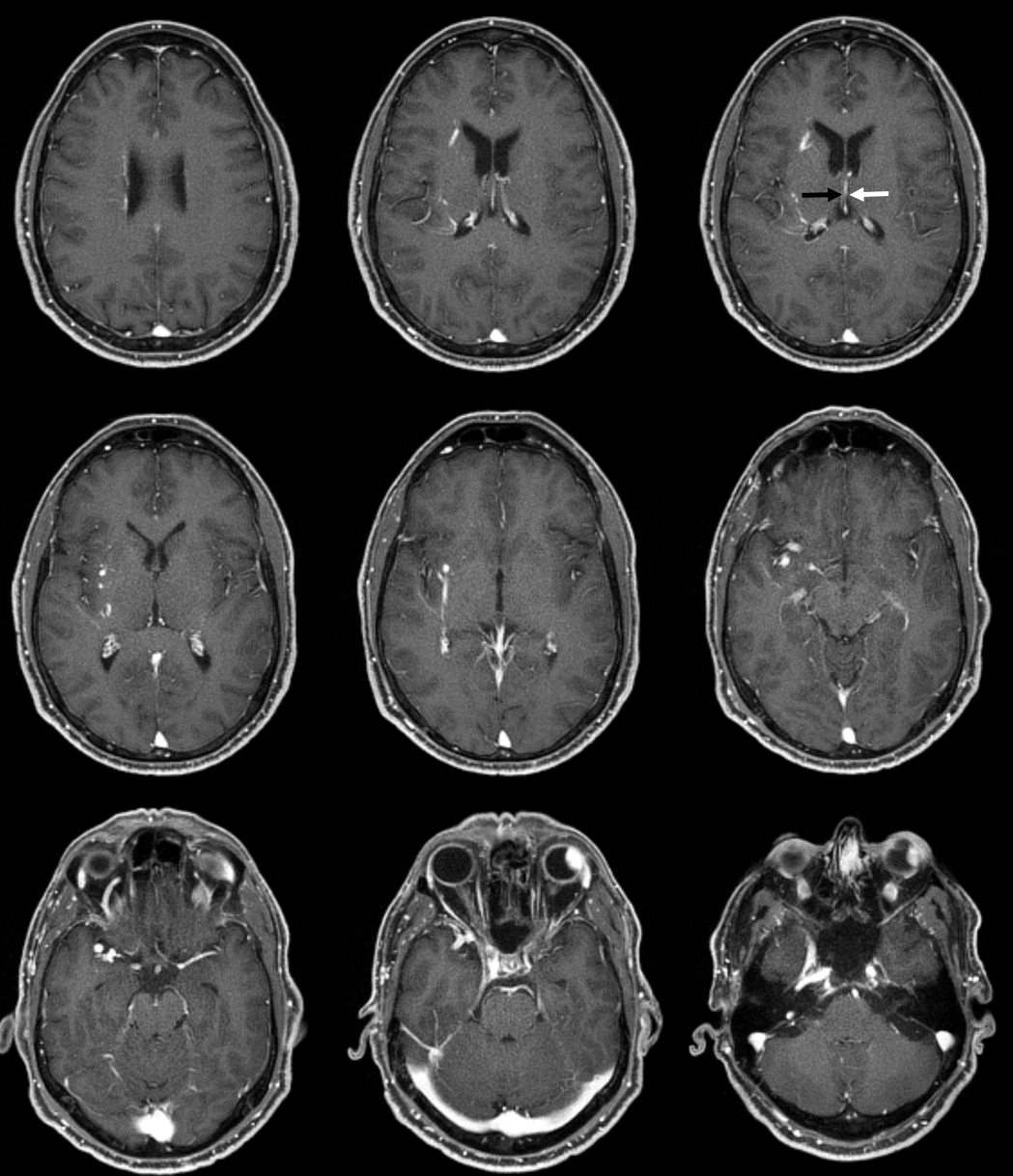
Sagittal — no internal cerebral vein is visible – -there is a tiny one in fact seen on the axials above
Coronal
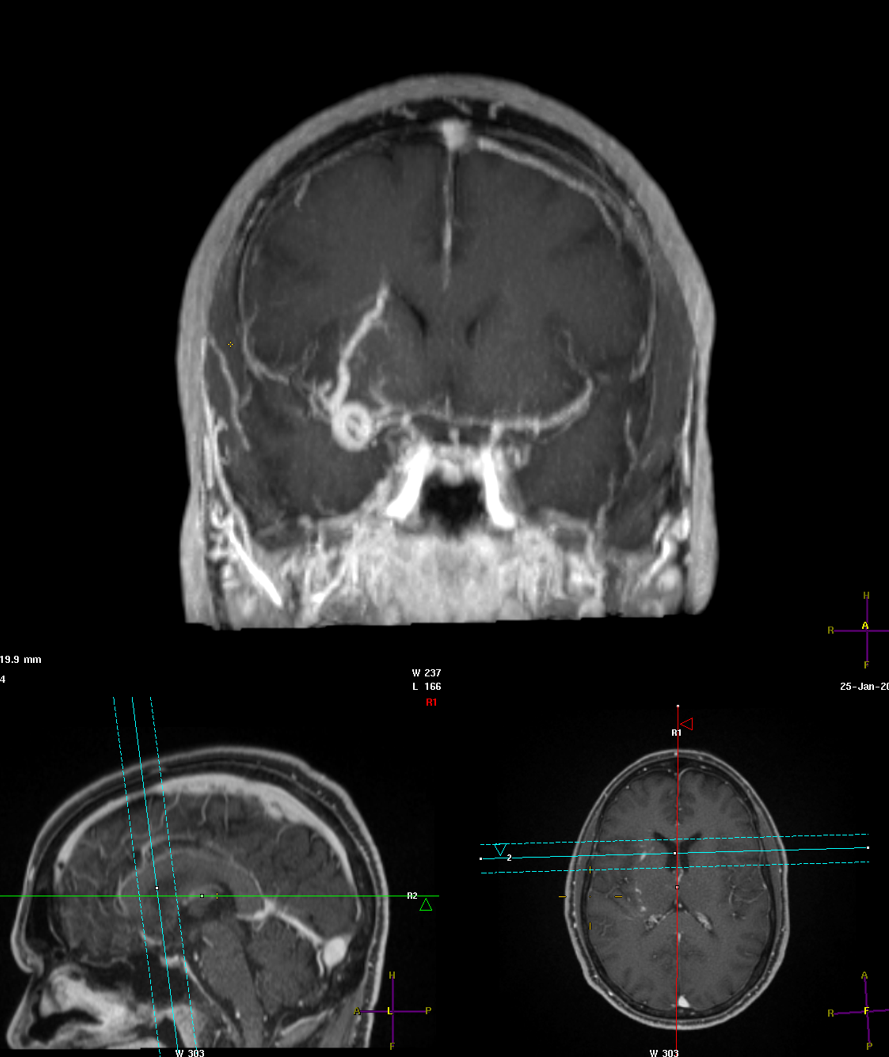
Normal looking ICV on the left side
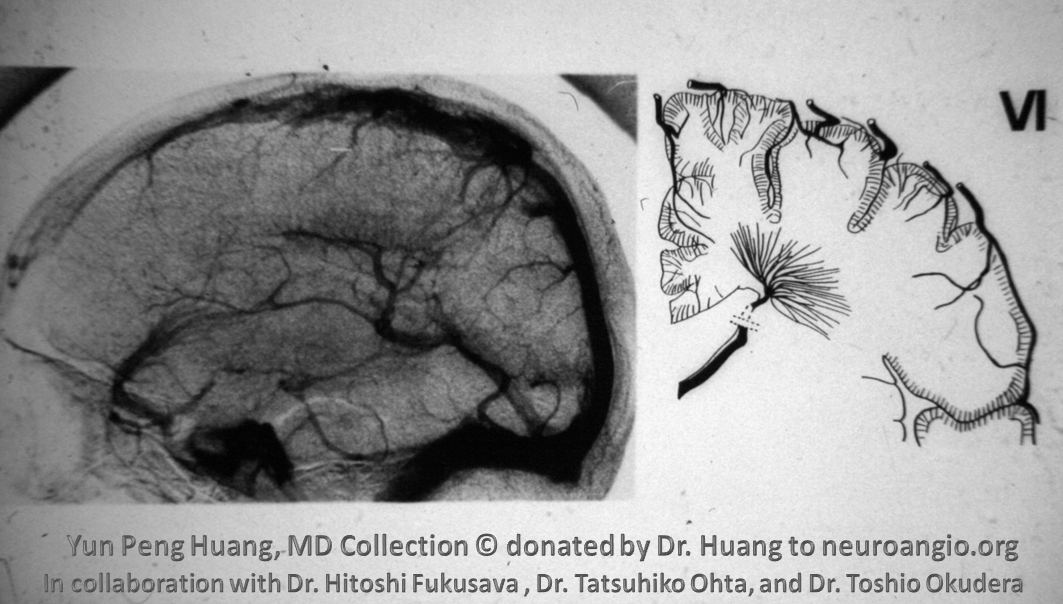
But wait — there is even more! The ultimate angiographic winner — a Yun Peng Huang DVA of course. And a perfect illustration of logitudinal and transverse caudate veins. And again, no internal cerebral vein to be seen…
Another one — this looks kind of unhealthy though. Congested — not sure this is a DVA. Plus the opening into the anterior cranial fossa venous system (*) Perhaps Sturge-Weber?
Now, the embryology of this is a bit intem resting. We believe that ICVs form early — prior to the expansion of the cortex. DVAs like the ones above must somehow form after the whole germinal layer migration phase takes place. Somehow all of those subependymal veins have lost access to the ICV afterward. Let me know if you have any good ideas — neuroangio@neuroangio.org
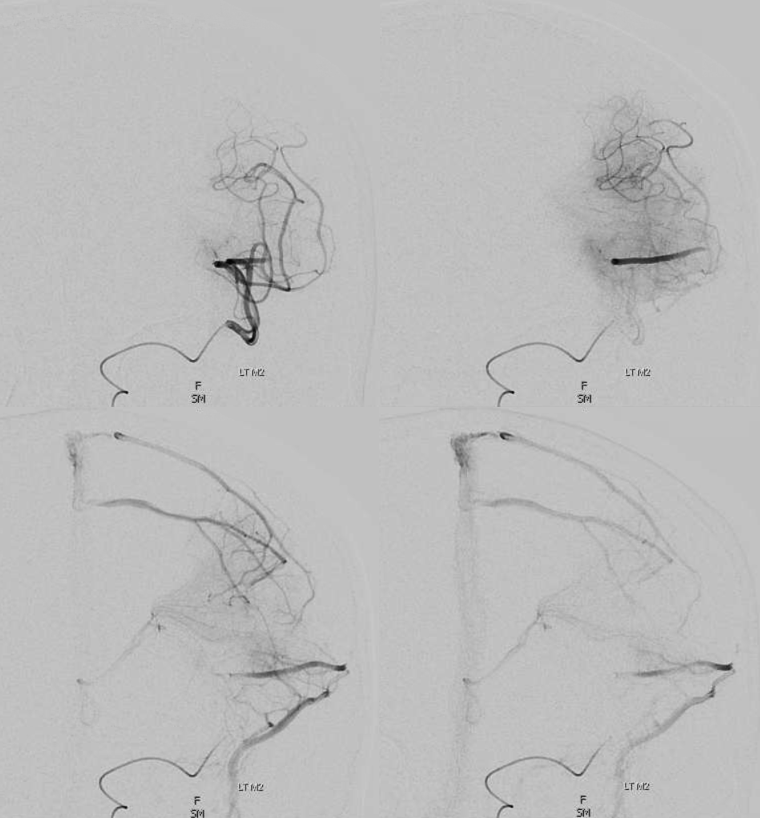
Deep drainage of superficial arterial system
Look at this one — M2/3 junction injection — well beyond the lenticulostriates. These apparently superficial arteries drain partially into deep venous system — relevant to understanding AVMs — see example lower down. This image was made in preparation for distal thrombectomy – full case here
Bithalamic drainage — DVA?
Case courtesy Dr. Eytan Raz — left thalamus (arrow) drains to the right via a really rare vein in the interthalamic adhesion (dashed arrow). The inferior left thalamus also drains to the right (thin arrow), collecting into a common vein (open arrow) which receives right thalamic drainage as well (ball arrow) and empties into the Galen. The basal vein is hypoplastic on the right. Probably the whole thing is a bithalamic DVA
I hope u get the big idea. Now to the details…
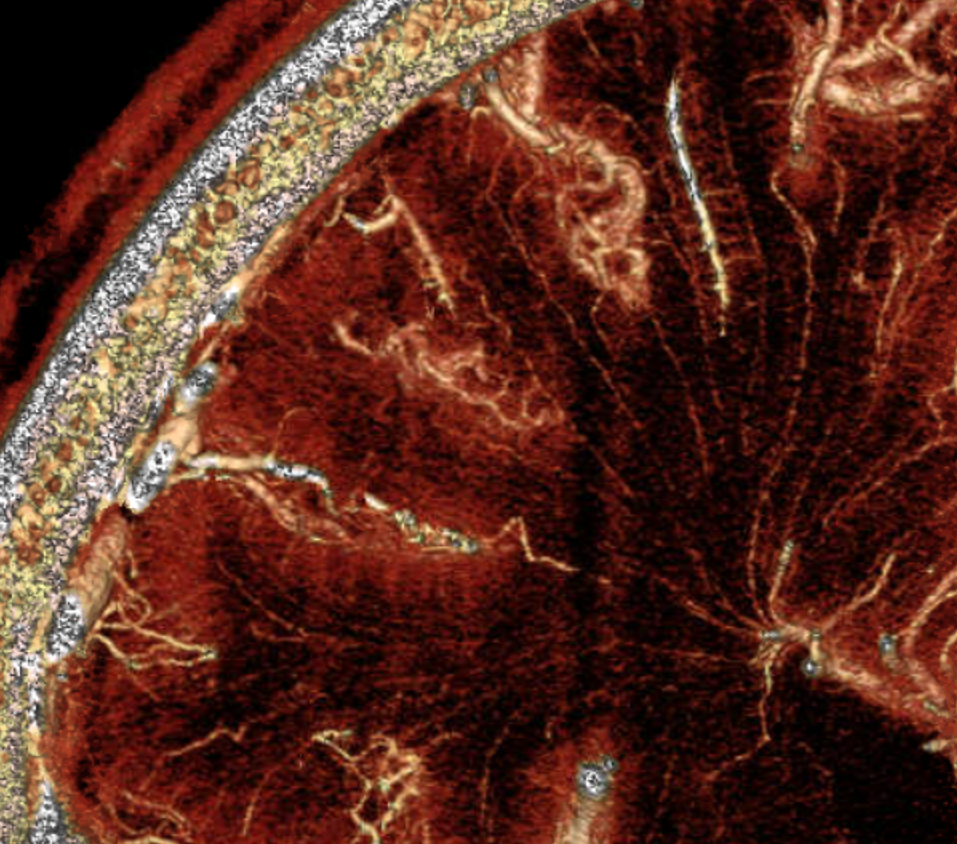
White Matter Venous System by DYNA CT
Stunning detail can now be obtained. Here are some examples — the drainage of white matter is predominantly into the internal cerebral venous system
Cross-sectional tutorial
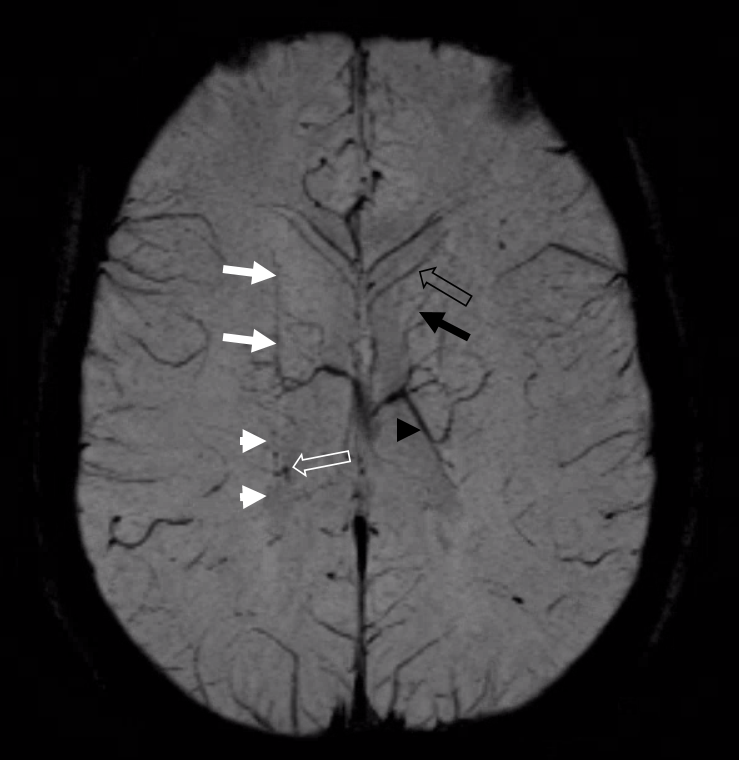
Didn’t we say that we should study cross-sectional imaging? Fine, here it is. SWI. Typical stuff. Open white arrow – septal vein, along medial aspect of frontal horn — not really in the septum, but still called septal by most people. White arrow — septal vein in the actual septum. Black open arrow — thalamostriate vein. White arrowhead — direct lateral vein, aka lateral direct vein, aka direct atrial vein — good luck with learning this stuff. Black arrows — medial atrial veins — one of the most consistent tributaries of the internal cerbebral vein.
More cross-sectional correlation — boring but instructive. Do this at home on your own dataset –its much more engaging.
On the left there are “double thalamostriate” veins (black, white arrows) opening into the ICV — another variant you should be able to explain by now. Also present is a large anterior caudate vein (dashed black arrow, lateral group)
Schematic of above variant — double opening of longitudinal caudate veins into the ICV
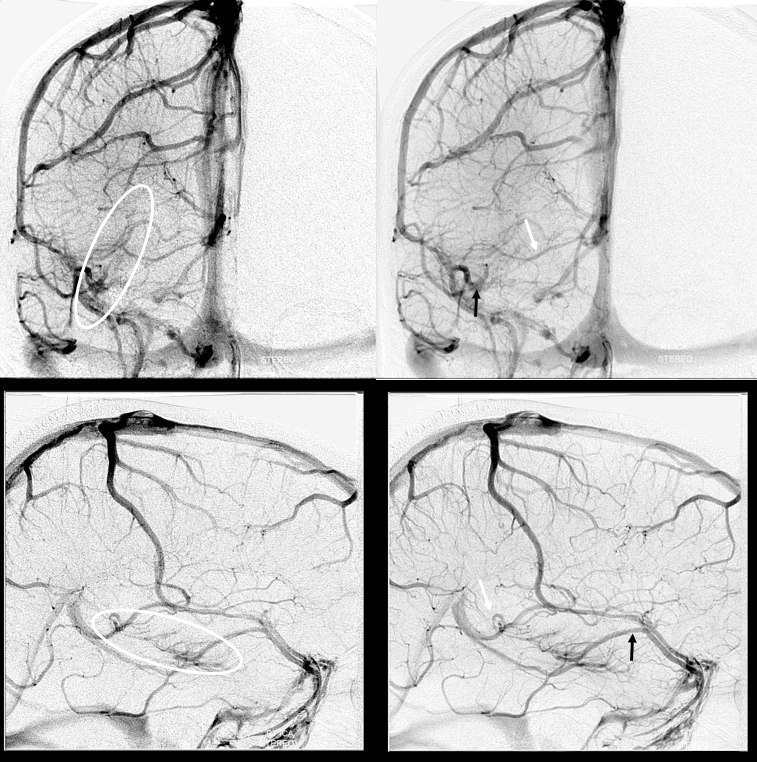
On the right, there is a DVA (white oval), part of which drains via the inferior ventricular vein (white arrow) into the Rosenthal, and another part into the supefficial sylvian venous system (black arrow)
Stereo pairs
Vessel wall imaging — serial orthogonal thin MIPs, from front to back
Finally, something really unusual — double septal veins!
Here is a rare case of double septal veins
No! Its a fakeout. Remember — you only see veins of the arterial territories you had injected. This patient has a dominant right A1 segment. Therefore, both ACA territories are opacified, resulting in visualization of bilateral septal veins. The internal cerebral veins are superimposed on the lateral images, but both sets of septal veins and ICVs (lower set of white arrows on bottom right image) are separated on frontal views
Practical Applications
Falcotentorial Dural Fistula — Congestion of ICV results in gradual development of effective transmedullary collateral
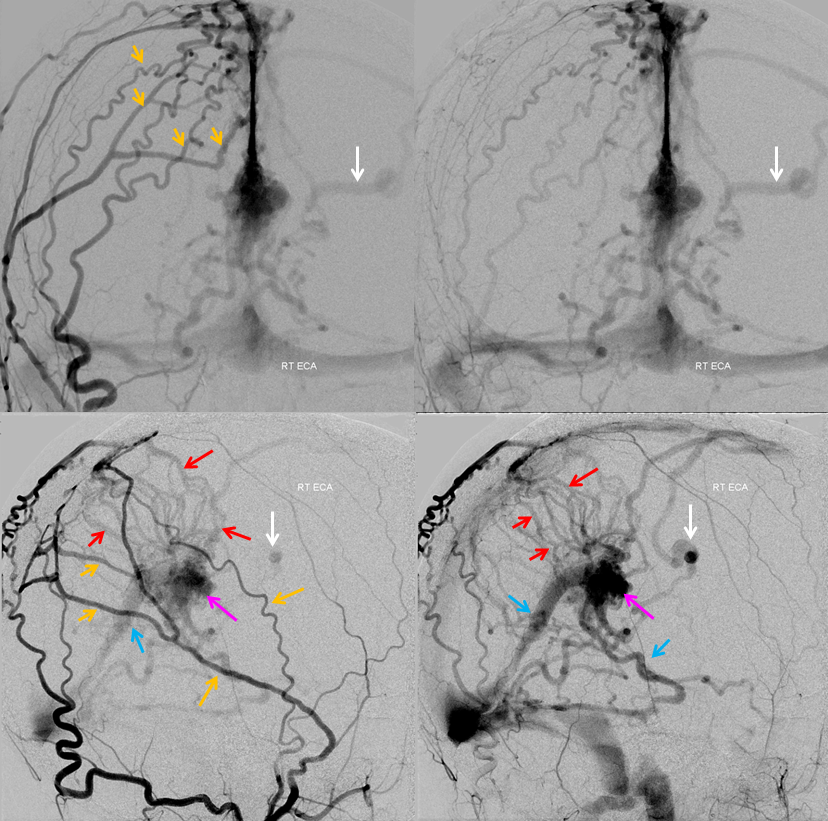
One of the best conditions to understand the deep venous system is a “falcontenorial dural fistula” — a super interesting fistula that often has extensive “Davidoff-Schechter” supply but predominantly still is fed by dural branches of the MMA and extradural carotid. These fistulas drain into the Galen/straight sinus junction region and thus are strategically positioned to compromise the internal cerebral venous system. With larger fistulas and more outflow restriction the internal cerebral venous system is forced to look for other sources of outflow. The basal vein is one natural outlet, however when this is unavailable the solutions are usually very interesting — transmedullary veins, lenticulostriate veins for example. Below is an example of one fistula that results in hypertrophy of a transmedullary vein (white arrows) draining the internal cerebral venous system. The full case can be seen here:
The same vein is also used by the fistula, which means that even at this stage the internal cerebral system has to compete
AVMs — another good way to appreciate some IVC anatomy intricacies.
AVM 1
Here is an AVM of the deep left parieto-occipital region. Venous drainage proceeds via the “internal occipital vein” — see Netter above. This is separate from the medial atrial vein which is normal (white arrows). This tells u that AVM is likely to be supplied by the parieto-occipital and calcarine branches, rather than the posterolateral choroidal artery
Angio. The rupture-related pseudoaneurysm is black arrowhead
AVM 2 — thalamic hemorrhage in a child. Vein draining the AVM is a purely parenchymal thalamic vein opening into the proximal ICV
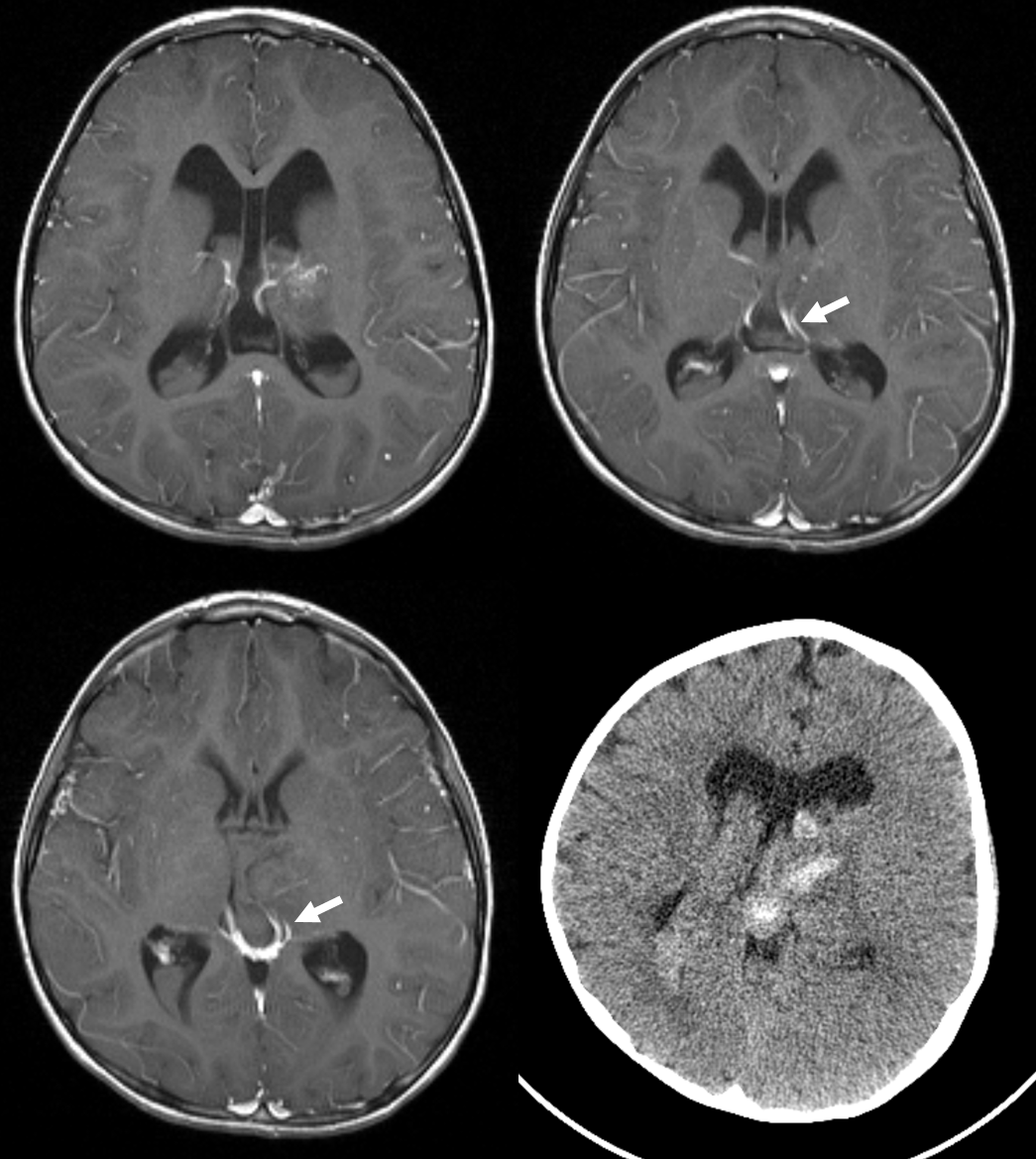
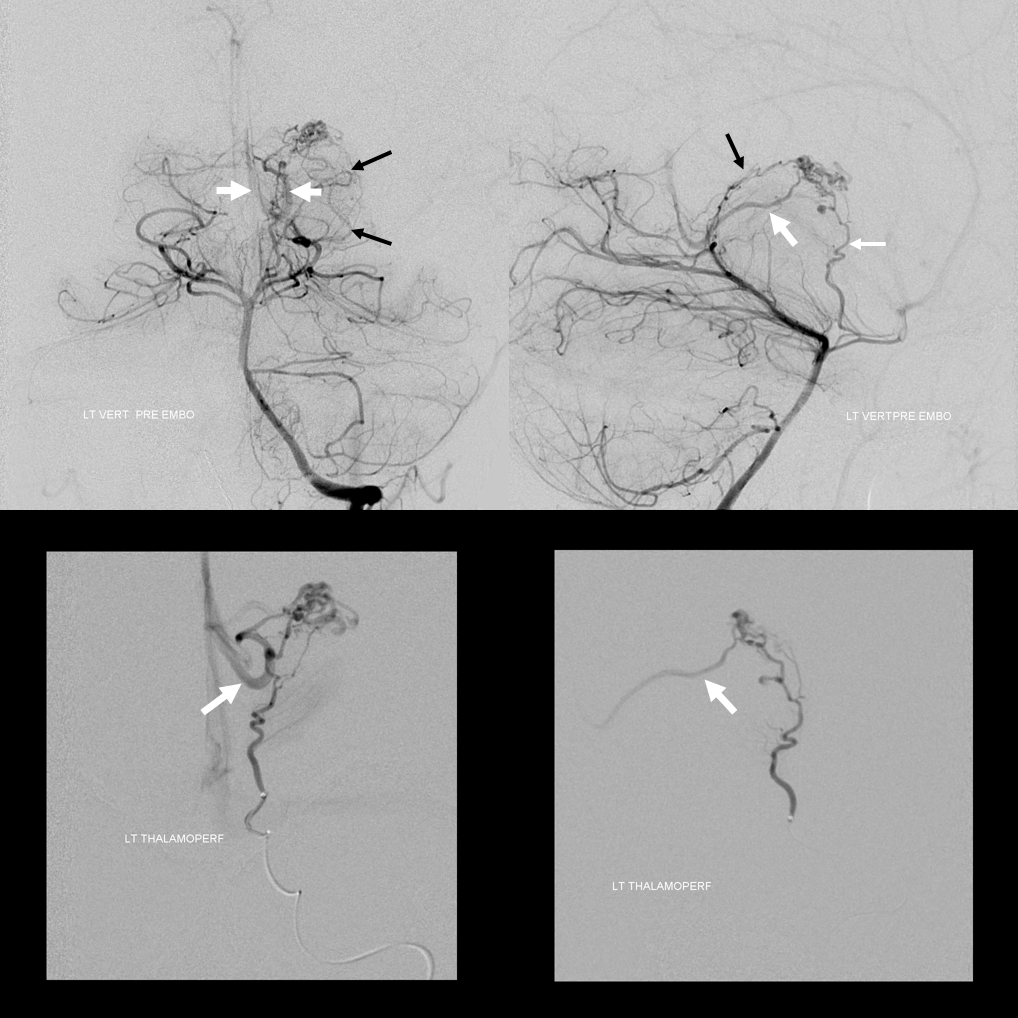
Angio. Supply from anterior thalamoperforator (thin white arrow) and posterolateral choroidal (black arrows) arteries. It should be well appreciated that posteromedial and posterolateral choroidal arteries usually supply parenchyma in addition to choroid plexus. Draining vein is thick white arrows

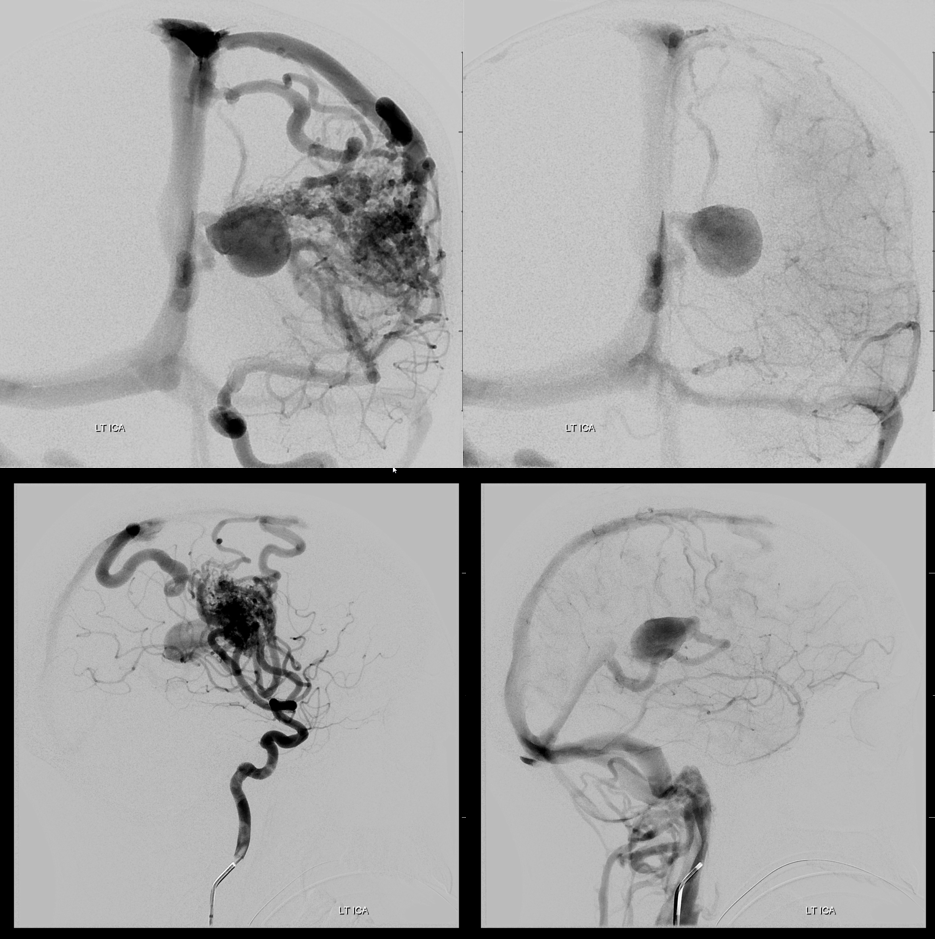
AVM 3 — it is not true that internal cerebral venous drainage requires presence of choroidal or lenticulostriate supply. Look at this huge thalamostriate venous aneurysm in an AVM with no lenticulostriate supply (right ICA injection showed only indirect supply by left convexity leptomeningeal anastomoses)
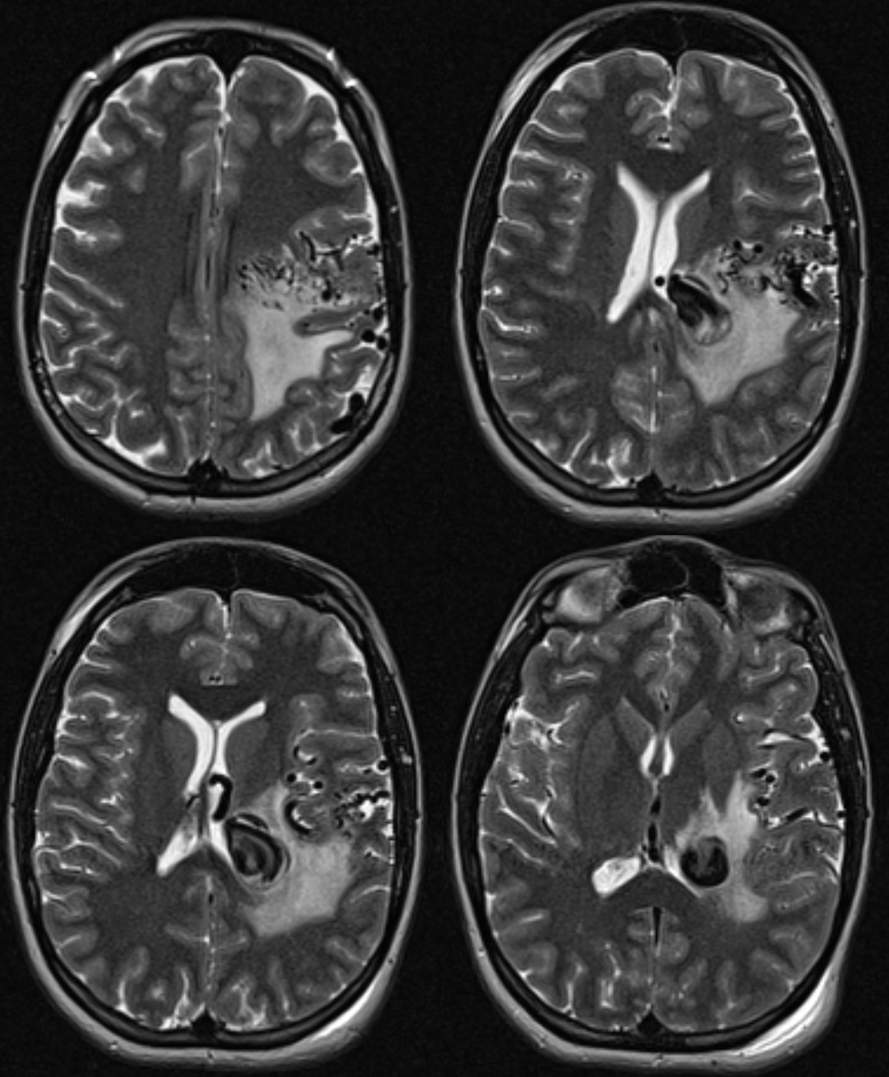
The supply comes from an array of M2/M3 segment penetrating / medullary arteries that form a cone with nidal apex in the supbependymal space
Cross-eye stereo

Anaglyph stereo
Had enough? Of course not. Check out DVA and Deep Venous System Pages