

Number 41. A meningeal connection between the proximal intraorbital or canalicular ophthalmic artery and the intracranial compartment. A key route for communication between orbital and intracranial compartments, aside from the ophthalmic artery itself — again… As such it’s both a dangerous and useful anastomosis. The picture above tells the story. This deep recurrent meningeal artery can connect with the sphenoid ridge branch of the MMA and, when the spinosum part of MMA is hypoplastic, this ophthalmic-recurrent meningeal connection becomes the source of MMA territory supply. Usually limited to frontal MMA branch, more rarely the whole MMA. A very nice example of balance between ophthalmic and MMA systems. Aside from the MMA, the recurrent branch can connect with the marginal tentorial artery and supply the free margin — including various lesions there — meningiomas, dural fistulas etc. Finally, can connect to the anteromedial branch of ILT.
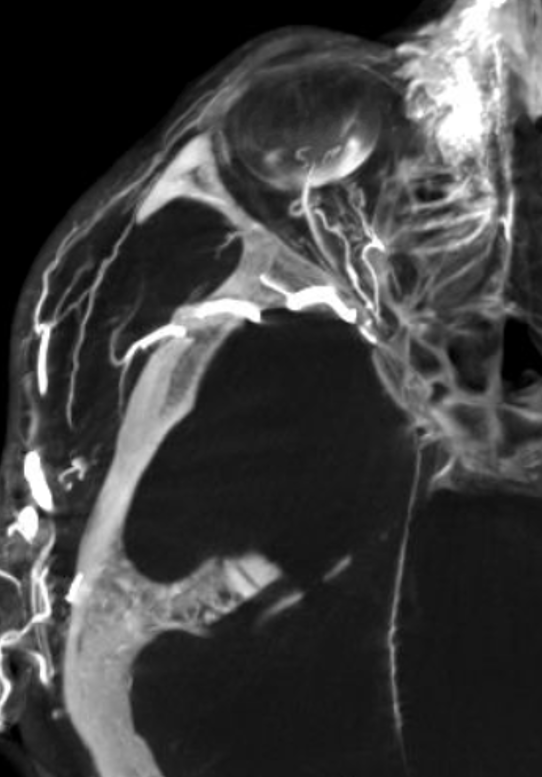
Angiographic evaluation is not so great often unless part of recurrent meningeal supply to MMA. High resolution Cone Beam CT is much better.
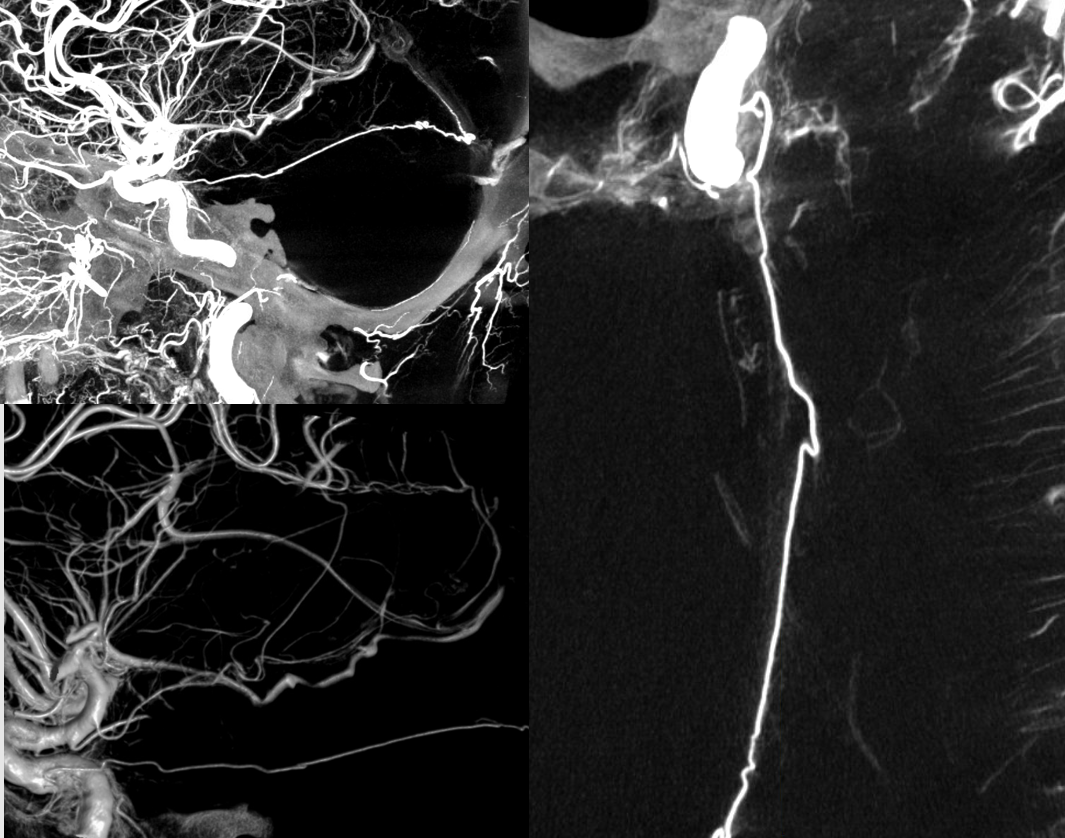
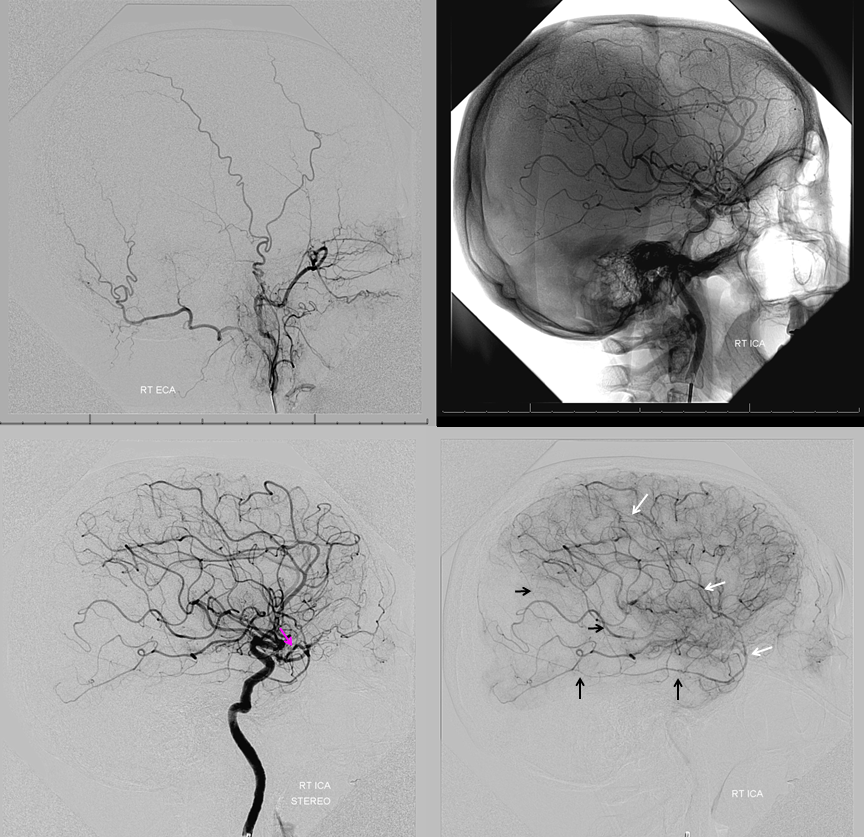
Below is recurrent meningeal supply of marginal tentorial arcade.
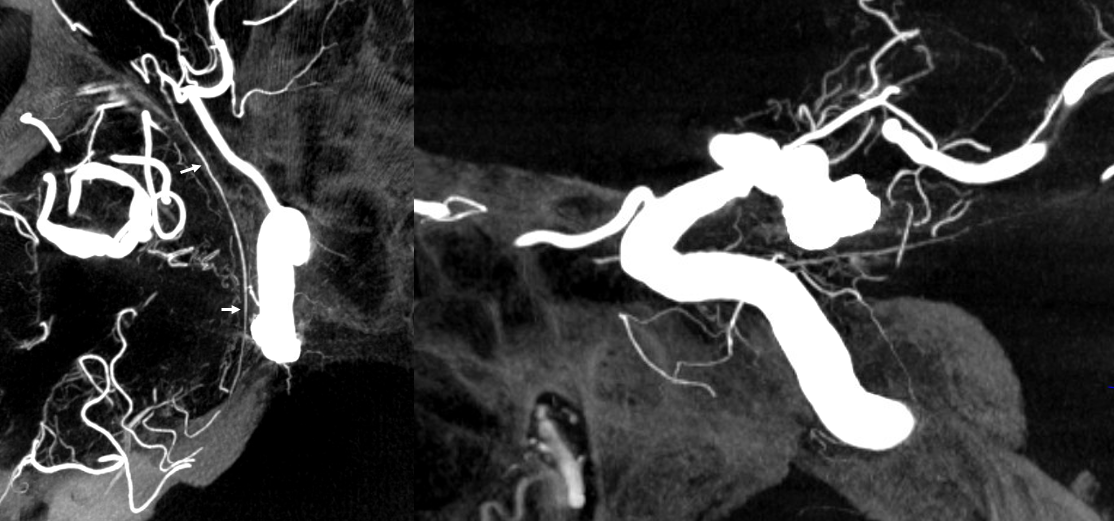
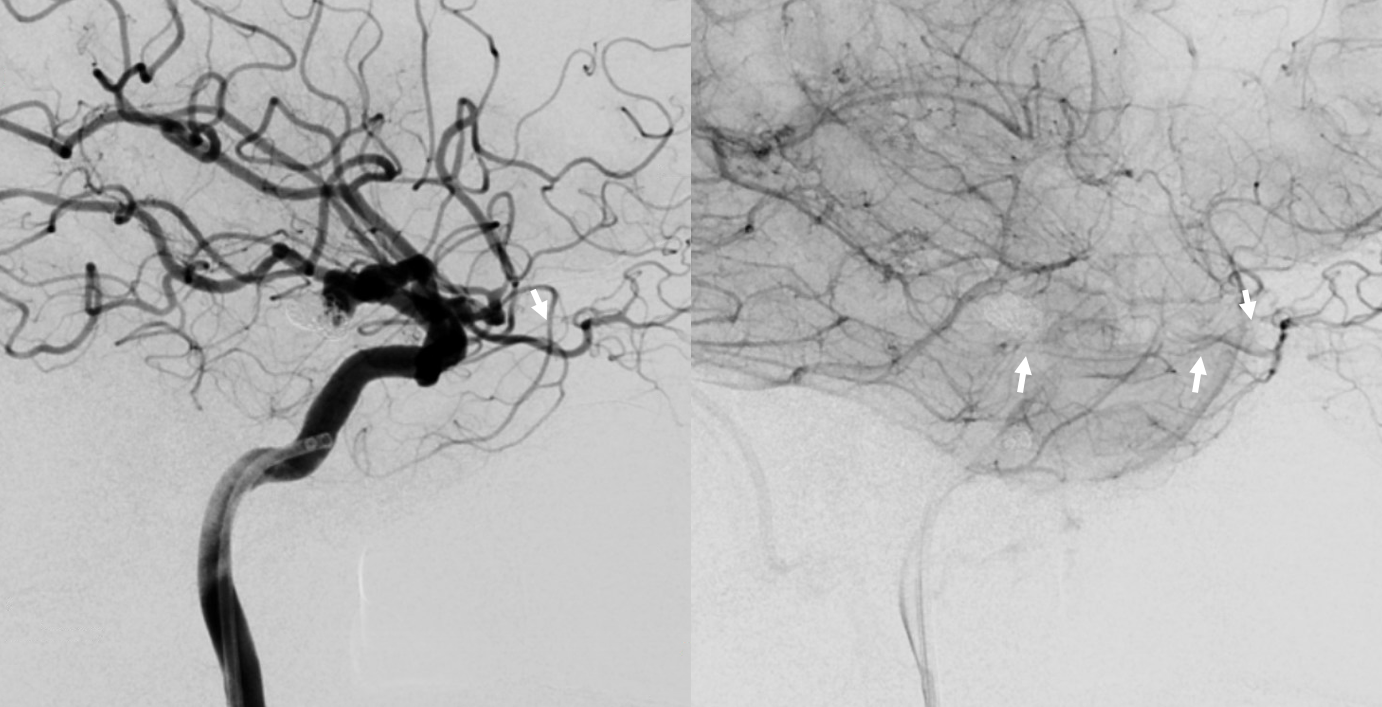
Same on 2D DSA — nearly impossible to see without benefit of Cone Beam CT knowledge
Note that ILT is hypoplastic here. Best seen on the below video. MHT supplies much of ILT territory, except for marginal tentorial which is fed by recurrent meningeal
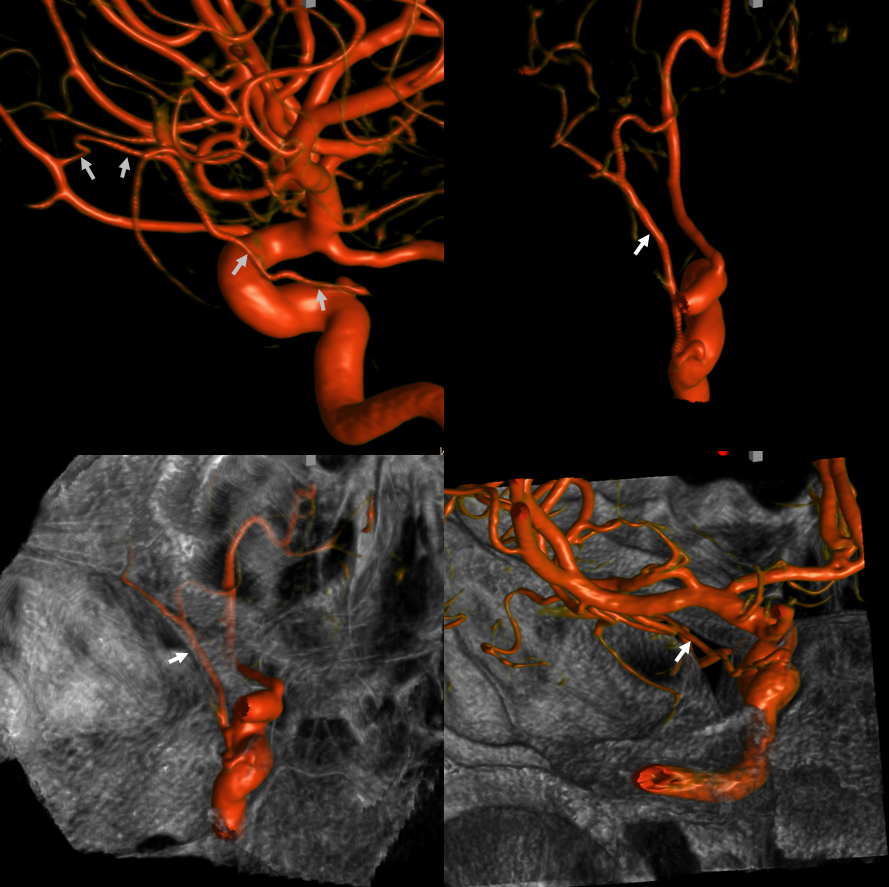
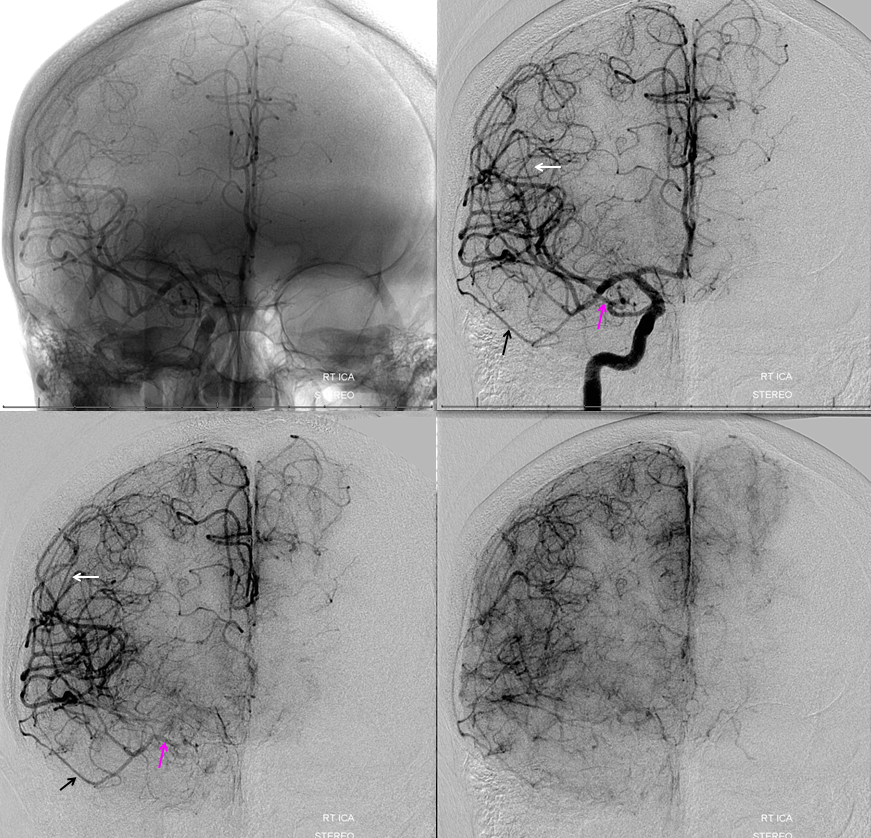
MHT — Ophthalmic Balance via recurrent meningeal
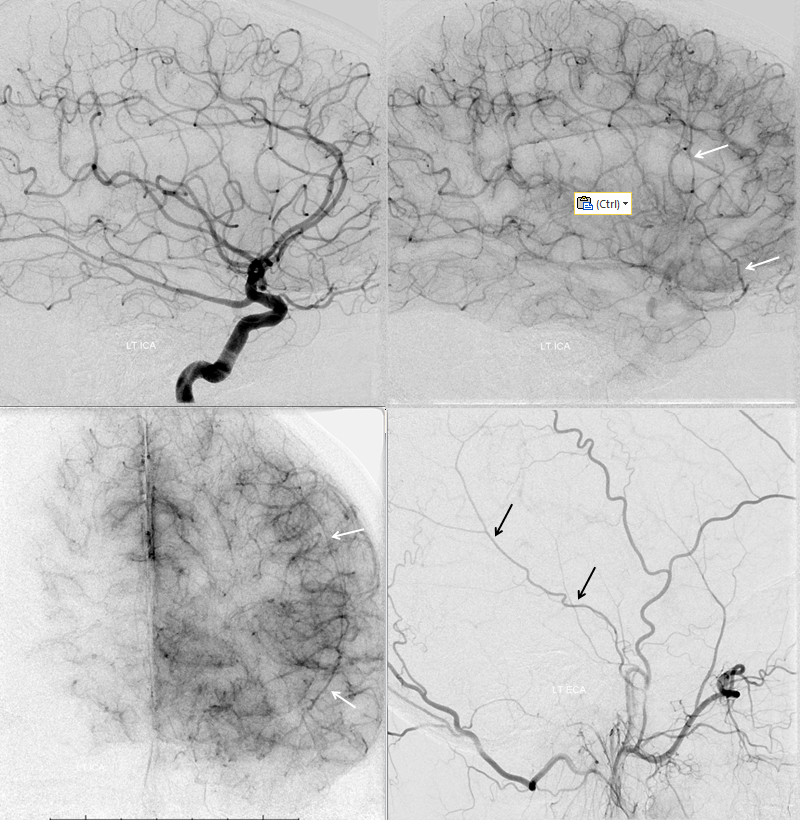
A more extreme (and therefore rare) version of balance between MHT and ILT. Remember we showed above how MHT can reconstitute ILT territory extending into foramen rotundum? The balance principle is that progressively greater takeover of one territory by another is correspondingly rarer. For example, ILT can occasionally contribute to supply of the ophthalmic via the “Dorsal Ophthalmic Artery” — the same vessel as the anteromedial branch of the ILT. So, you can now imagine that if an ILT were hypoplastic, and its territory supplied by the MHT as we saw above, it might happen that this supply could possibly extend into the orbit by the same “anteromedial branch” route also involving the recurrent meningeal in the orbit. Below is an example of this
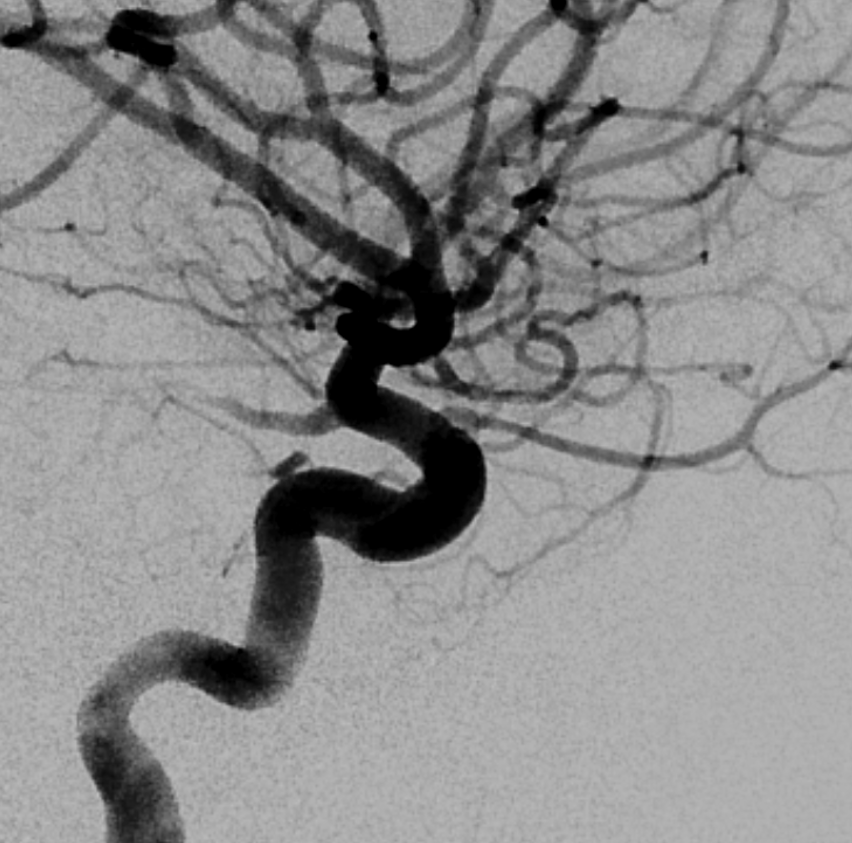
2D angio of the same case — can you recognize the connection? Not easy. We got the Cone Beam CT because MHT origin looked so weird
Of course its all about balance. Marginal tentorial usually arises from the ILT (see below)
Ophthalmic-Middle Meningeal Relationship
Guess what? Good job — its a spectrum! The whole thing about variants like meningolacrimal, meningo-ophthalmic, recurrent meningeal, — its all part of a continuum in balance between ophthalmic and middle meningeal territories. The same kind of analysis as we did for origins of ophthalmic artery above will apply here also. Below is a figure from our MMA publication, where this idea was first shown. Its a busy slide, we will dissect it below.
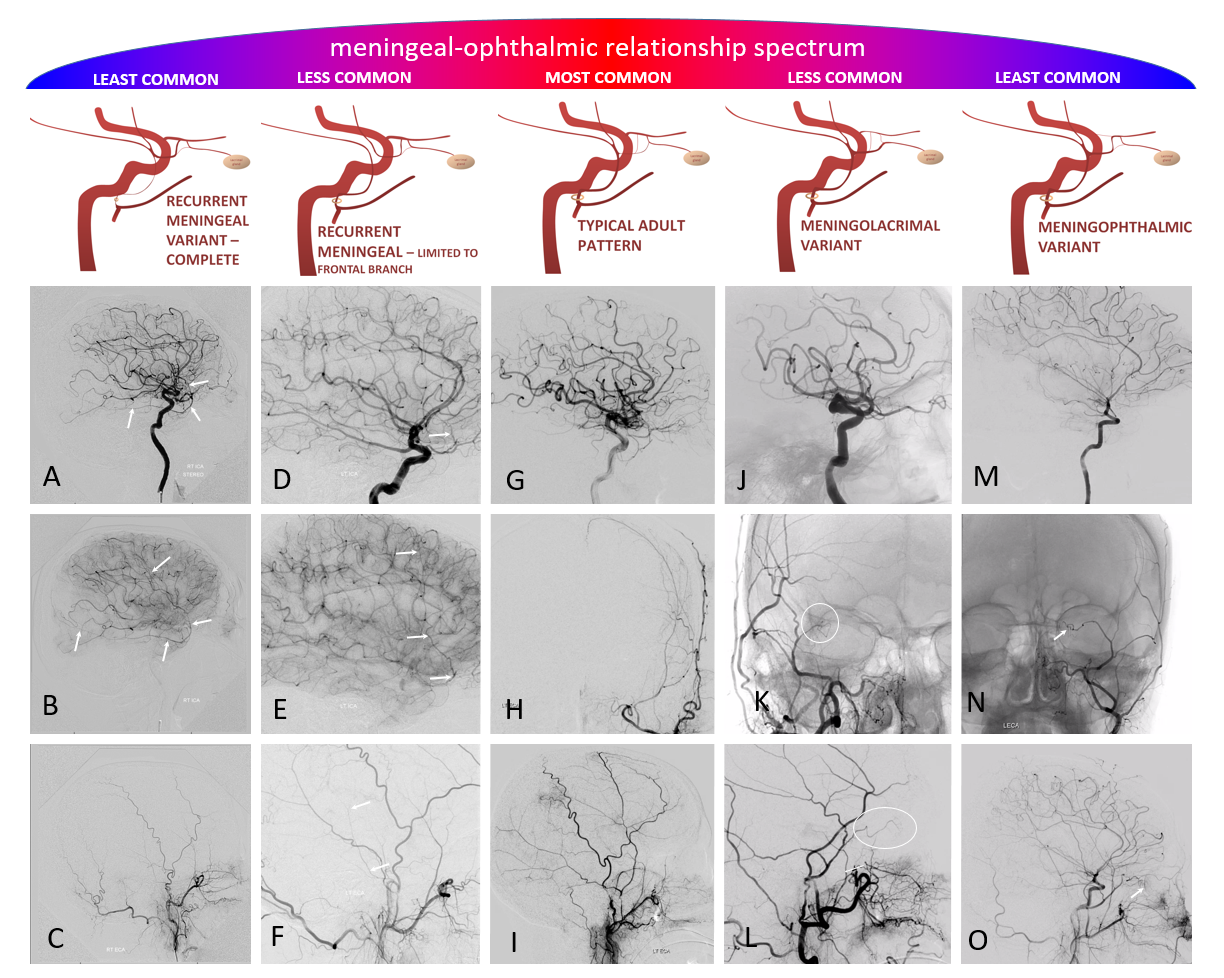
In a most common, “classic” scenario, the ophthalmic supplies the orbit, and MMA the meninges. However, these territories are in balance. Not infrequently, one may encroach on territory of another. The partial, and thus relatively common, orbital supply of MMA is known as the classic meningolactrimal variant. The reverse is partial ophthalmic supply of the convexity meninges, limited to anterior branch. More rare is “complete” MMA supply of orbit — the meningo-ophthalmic variant. Correspondingly rare is complete ophthalmic supply of convexity meninges – both anterior and posterior branches. This simple idea unites the two types of MMA /ophthalmic relationships.
Also important is to understand that none of these dispositions are discrete. The “meningolacrimal” is not just MMA supply of lacrimal gland — it can be also superior rectus, inferior orbit, etc. Or MMA can supply almost the entire orbit, except for central retinal / ciliary territories. Its all part of spectrum and balance. Below are detailed examples
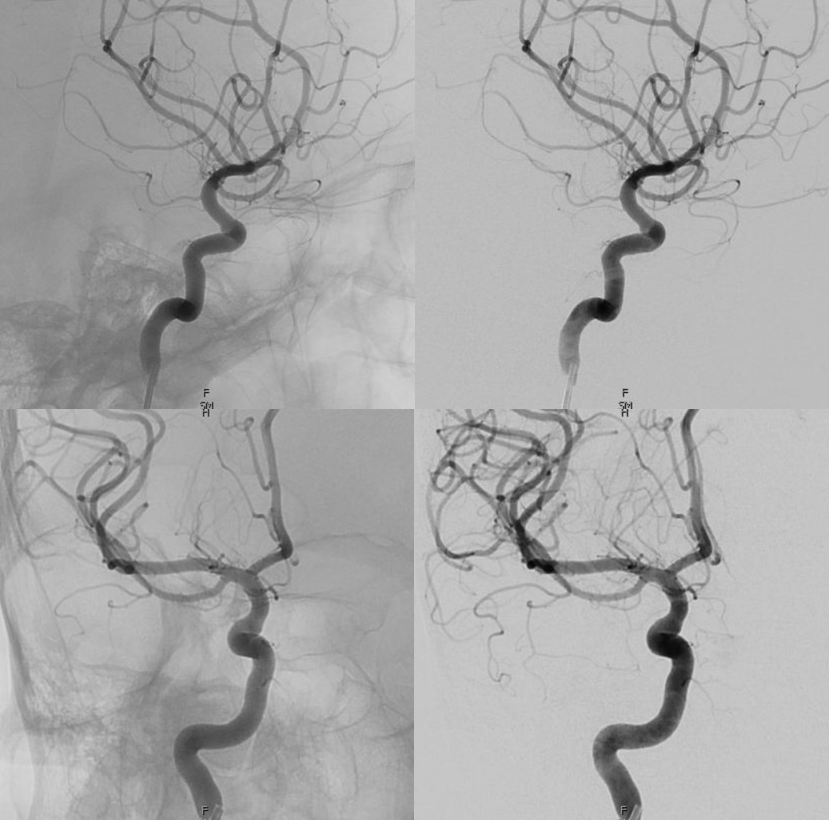
The proximal connection between MMA and ophthalmic is via the deep recurrent meningeal. Below is a classic recurrent meningeal artery with supply limited to frontal MMA territory (white arrows). The parietal or posterior part still supplied from the IMAX (black arrows)
Older example ICA injection
Complete Recurrent Meningeal — less common. Anterior (white) and posterior (black) mma branches. Deep recurrent meningeal is pink.
Meningo-opthalmic
Reverse — supply of the ophthalmic via the MMA — also through the deep recurrent meningeal — reverse of the MMA recurrent meningeal disposition. No ophthalmic from ICA below
Complete supply via MMA — via the deep recurrent meningeal
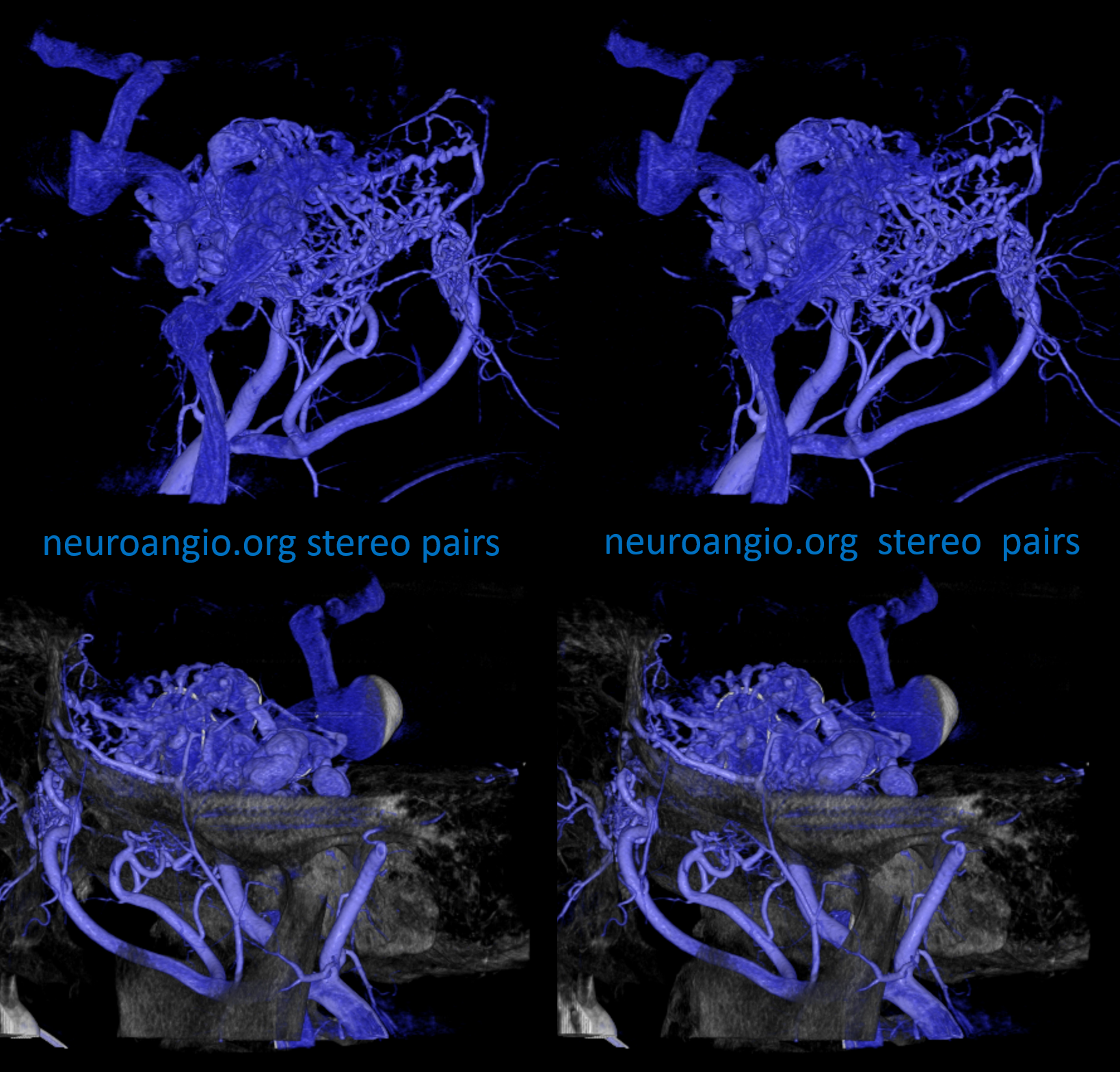
Same on MIP images — the meningo-ophthalmic also extends into the marginal tentorial
Pathology
Multiple Dural Fistulas
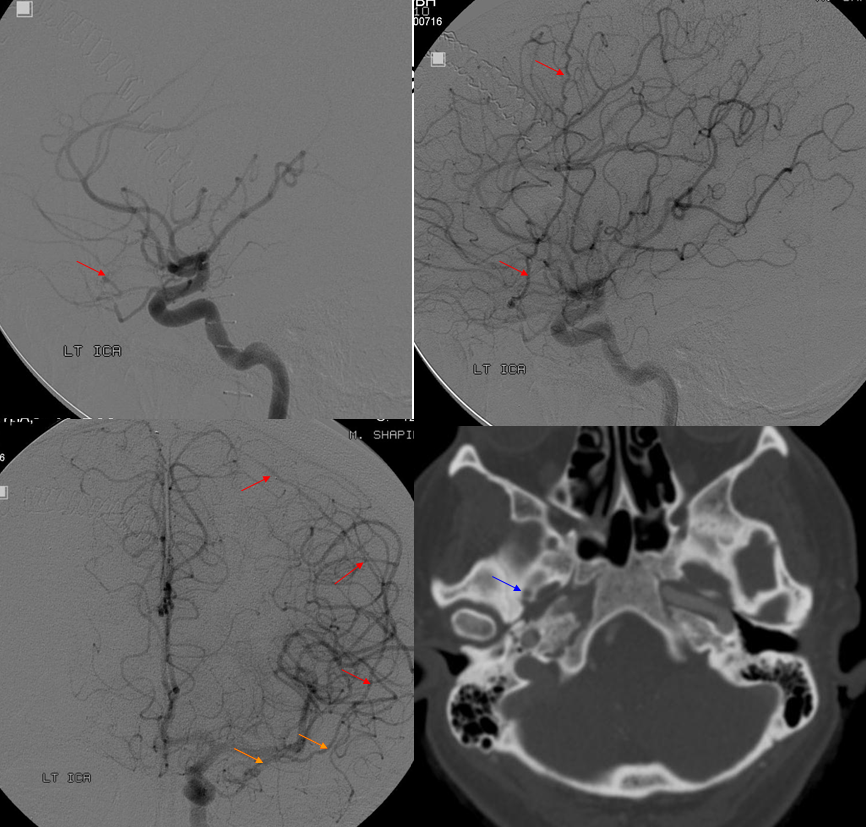
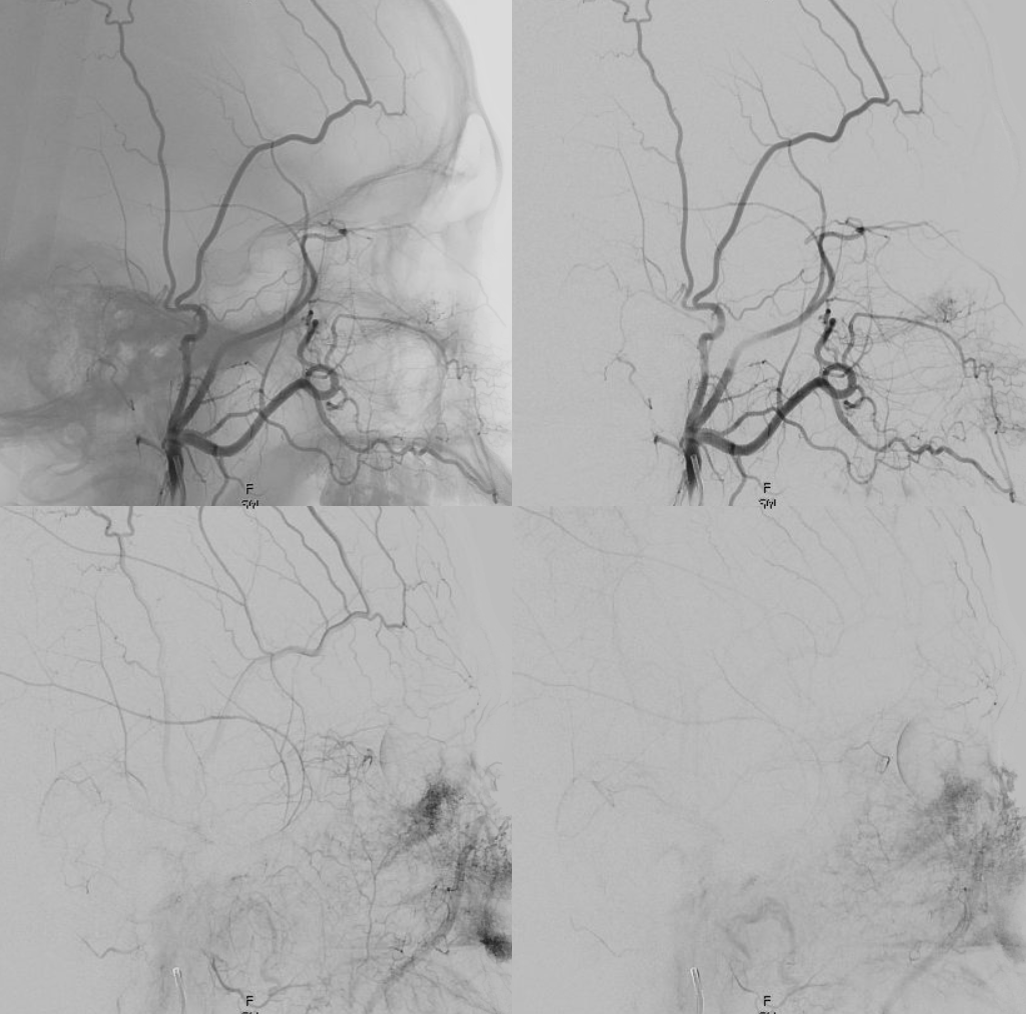
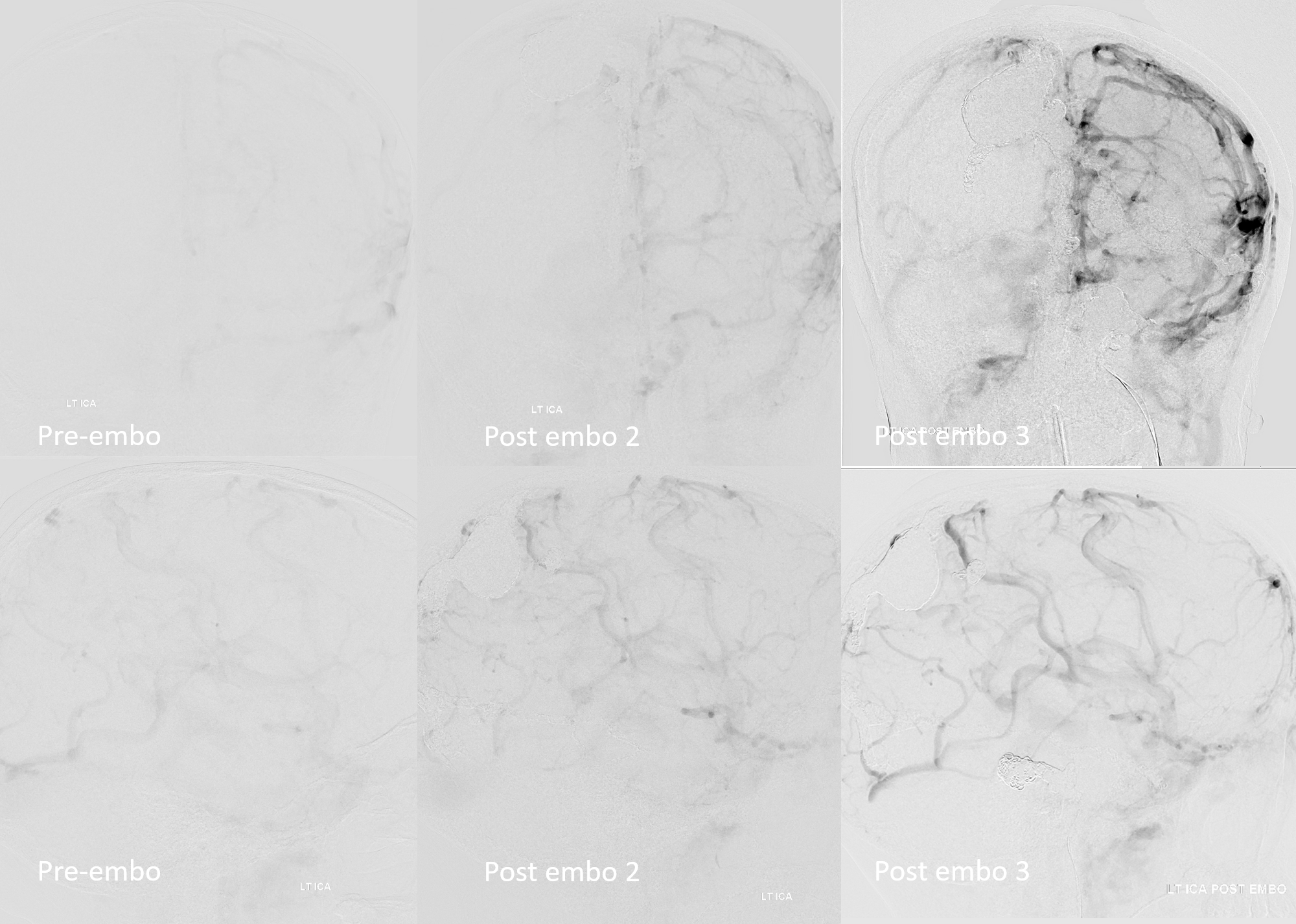
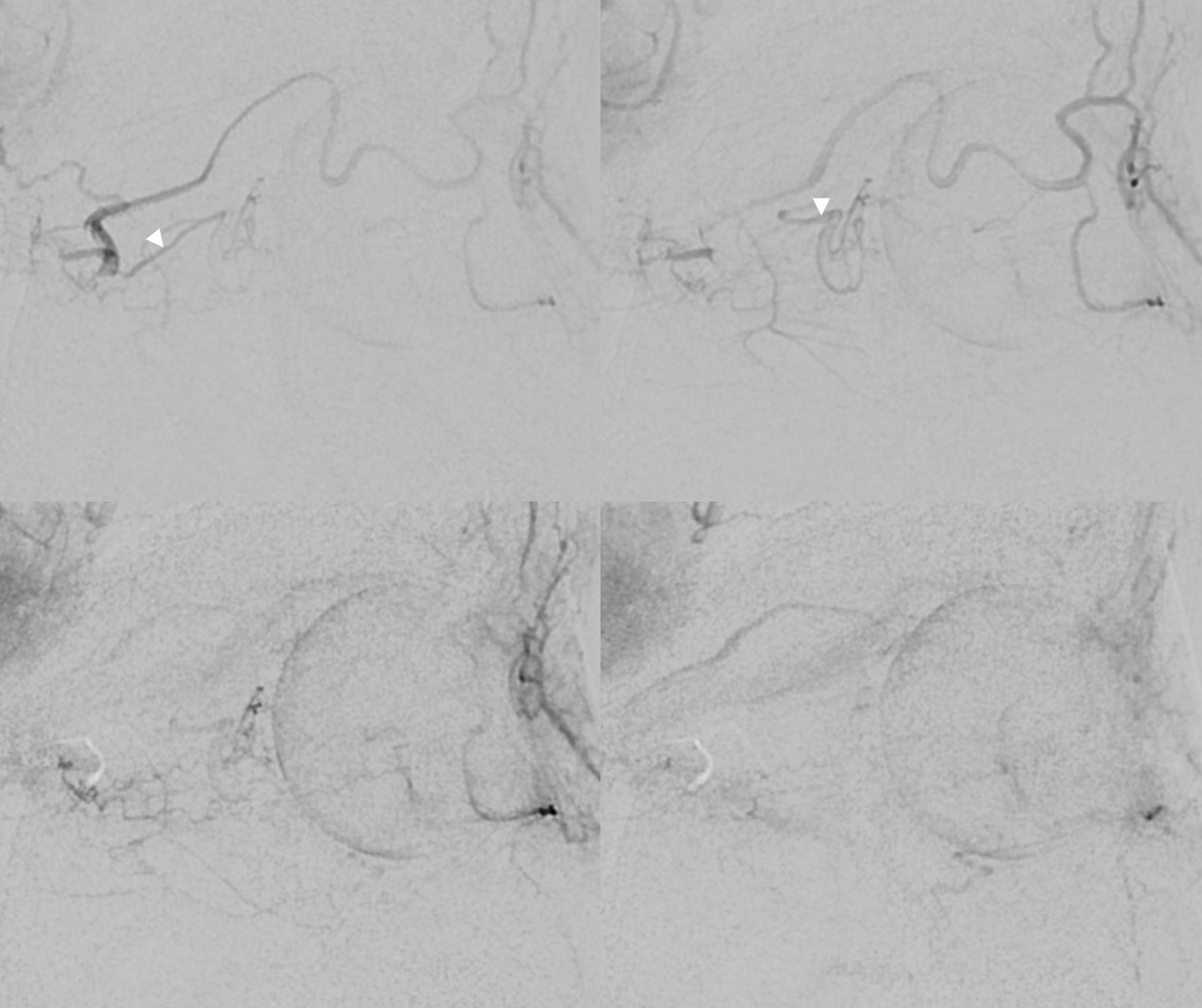
Very large cavernous sinus fistula — one of many fistulas in this patient. The ILT and MHT are hypoplastic (likely) or secondarily occluded (much less likely — usually such connections proliferate in setting of fistulas, not regress). The MHT and ILT territories were supplied via the deep recurrent meningeal (arrow), rotundum, MMA, and accessory meningeal arteries — which have now enlarged massively to supply the shunt. This is actually fortunate.
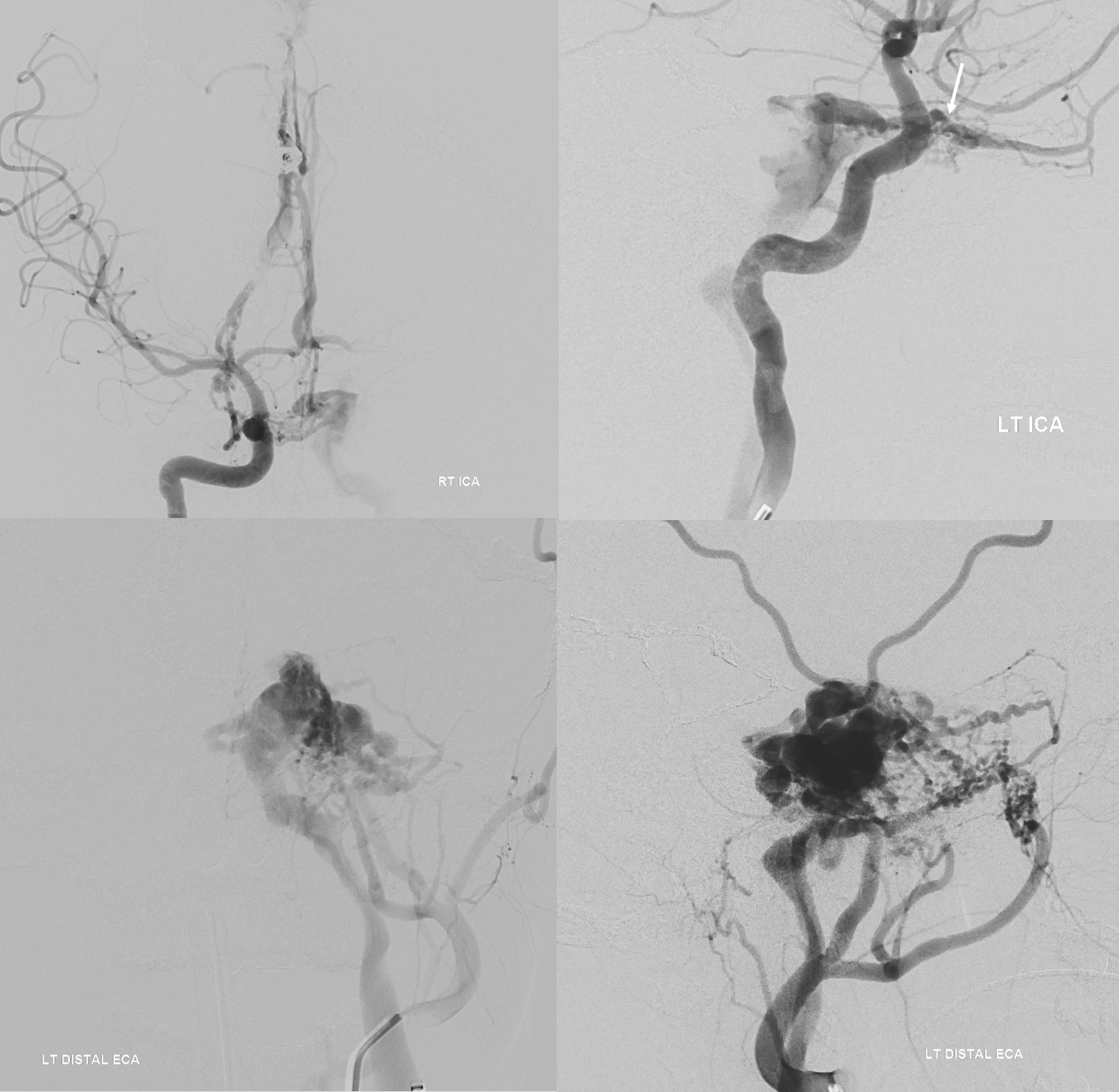
The fact that MHT and ILT are hypoplastic is actually fortunate. During closure of the cavernous sinus, it will become impossible to see them. Thus, transvenous onyx injection into the sinus risks spillage into the ICA — except that risk is very small with hypoplastic MHT and ILT. The deep recurrent meningeal is much easier to see, since it is anterior to the sinus.
A total of 4 microcatheters were placed into the cavernous sinus. Location in key areas — lateral mesencephalic vein, common ophthalmic vein, top of sinus — were verified with DYNA (not shown). Below image is during embo — starting with coils in the lateral mesencephalic, and proceeding with onyx, then other catheter etc…
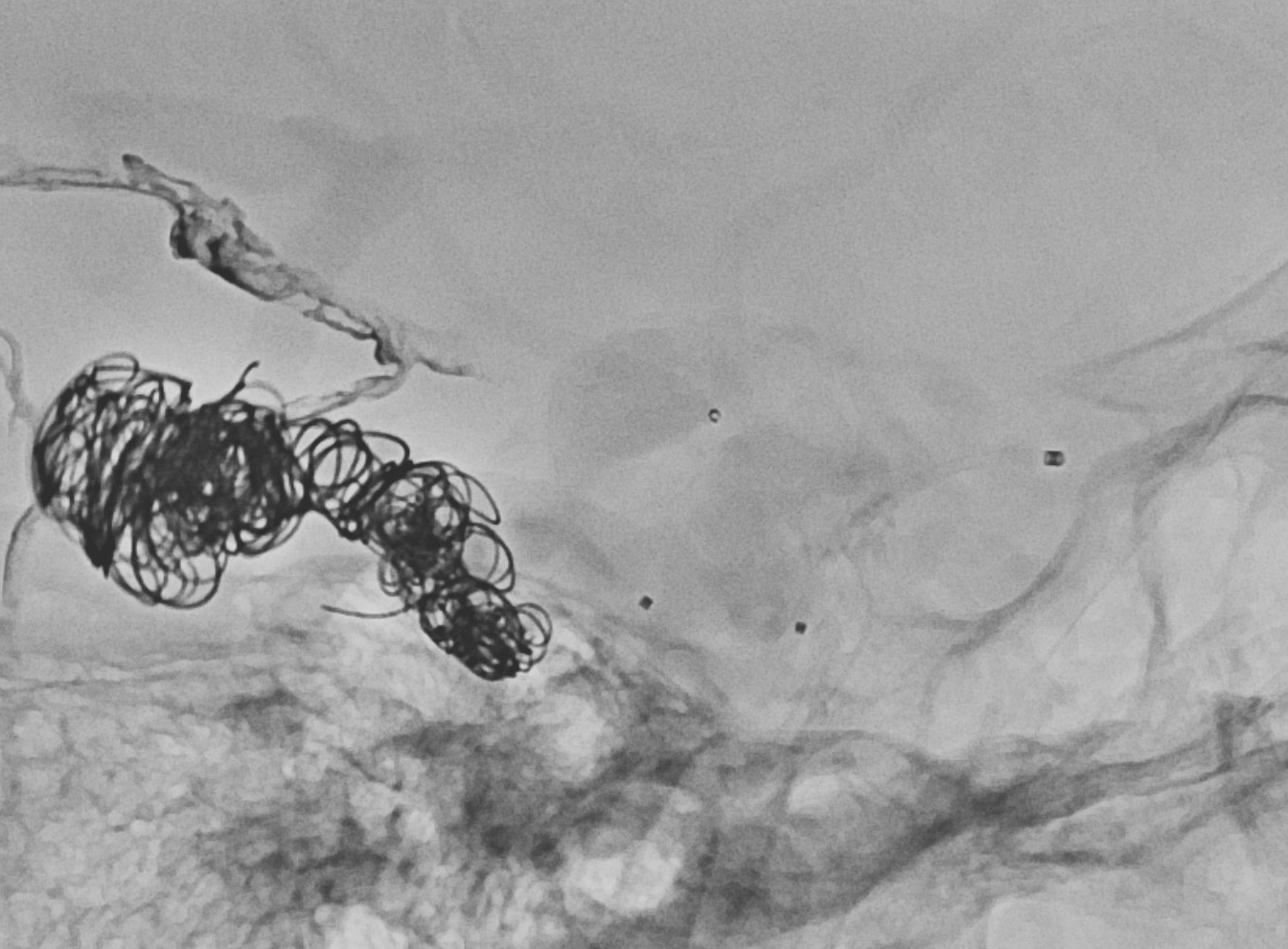
Post embo — note that the recurrent meningeal supply is gone also. Other embos were done before…

Progressive improvement in venous congestion — venous phases of left ICA injections
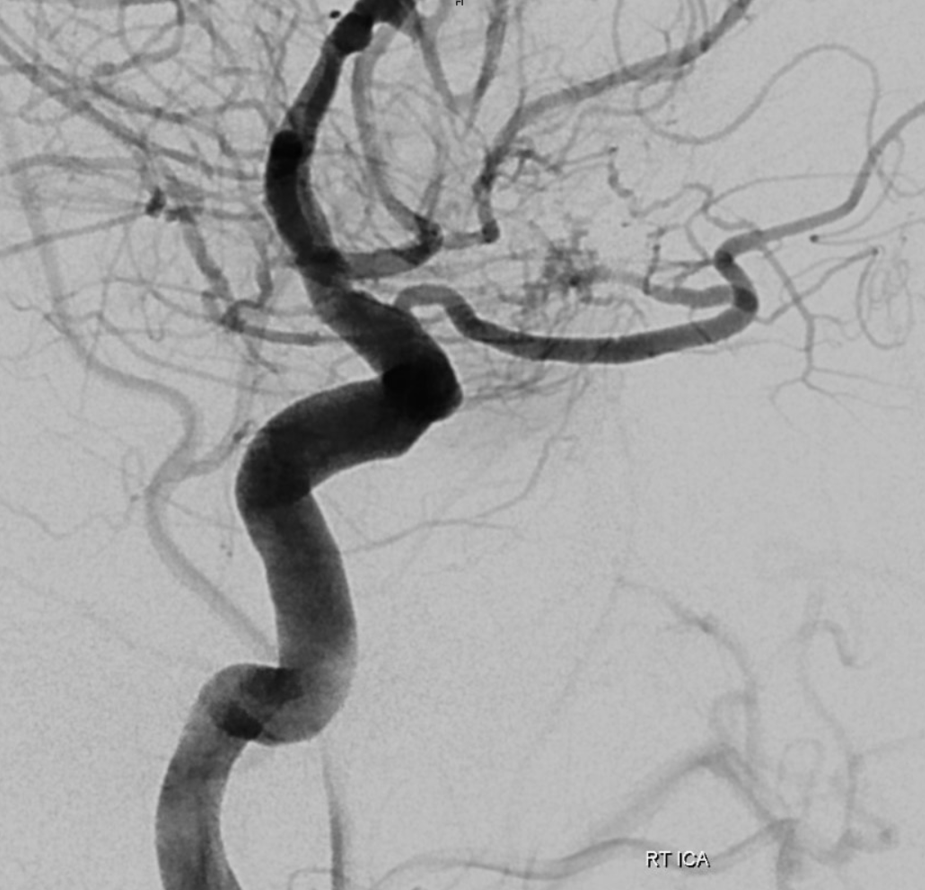
Meningioma ophthalmic supply embolization
Link to full case above. Supply to sphenoid wing or petroclival meningiomas will come from whatever arterial network exists there before tumor arises — just as it is for fistulas. It will vary on case-by-case basis. In a case where ILT for example is hypoplastic and MHT is dominant, that will be the supply recruited by tumor also. So, if there is a deep recurrent meningeal artery present — say to supply the tentorial margin — that will feed the tumor. Below is an example
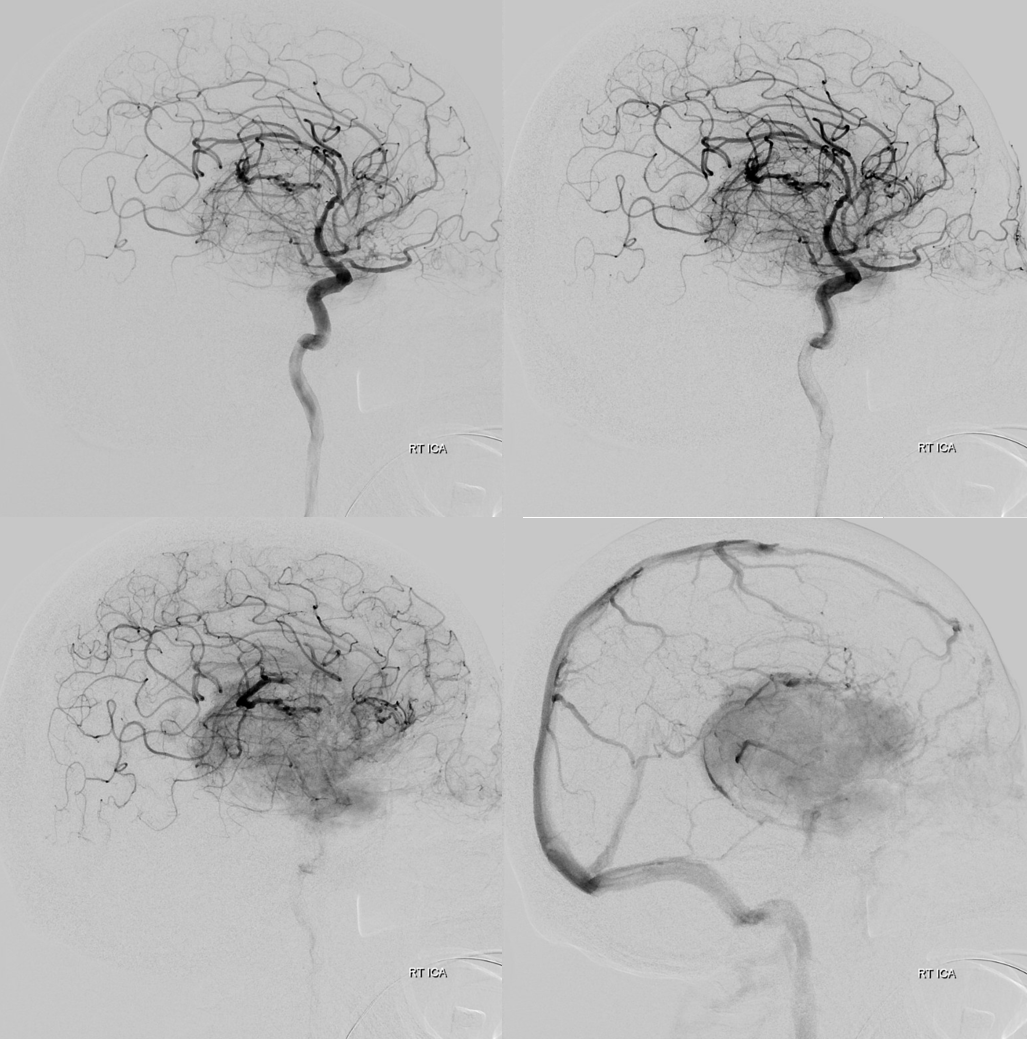
Detail
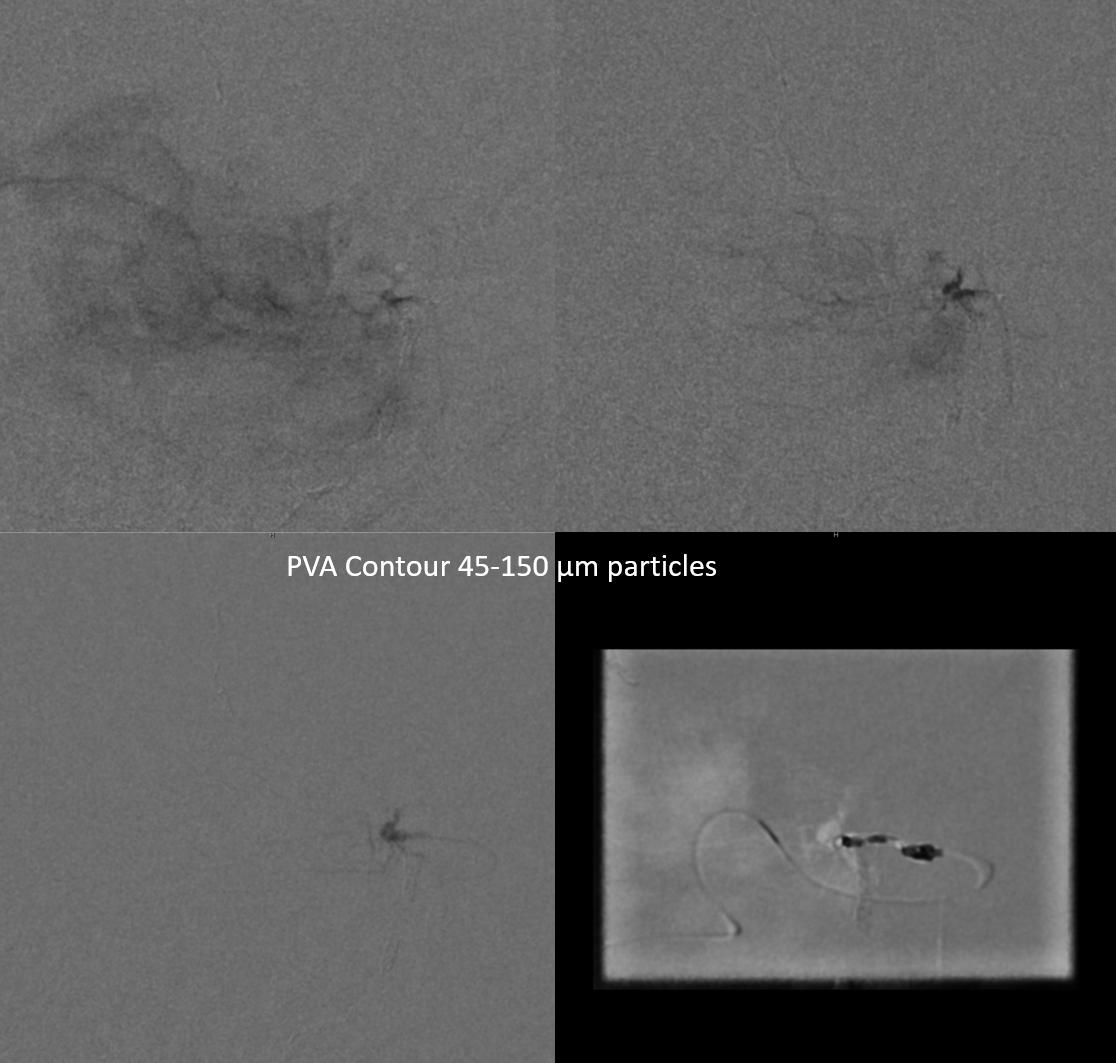
Embolization is possible — we prefer particles — but it is extremely important not to reflux. Liquid embolics work also but in our practice the control during withdrawal of catheter is less certain than with particles.

DYNA in embo position — the concern is actually not the central retinal artery — its proximal to the recurrent meningeal in this ophthalmic artery configuration — see ophthalmic artery page for details of over / under course and implications for central retinal artery origin. The concern is what supplies the optic nerve. Its practically impossible to see these branches, and if any supplies comes from the recurrent meningeal, well… Fortunately, that is not the embryologic way, as we understand it. So, with the DYNA not lighting up the optic nerve, i think its good to go.
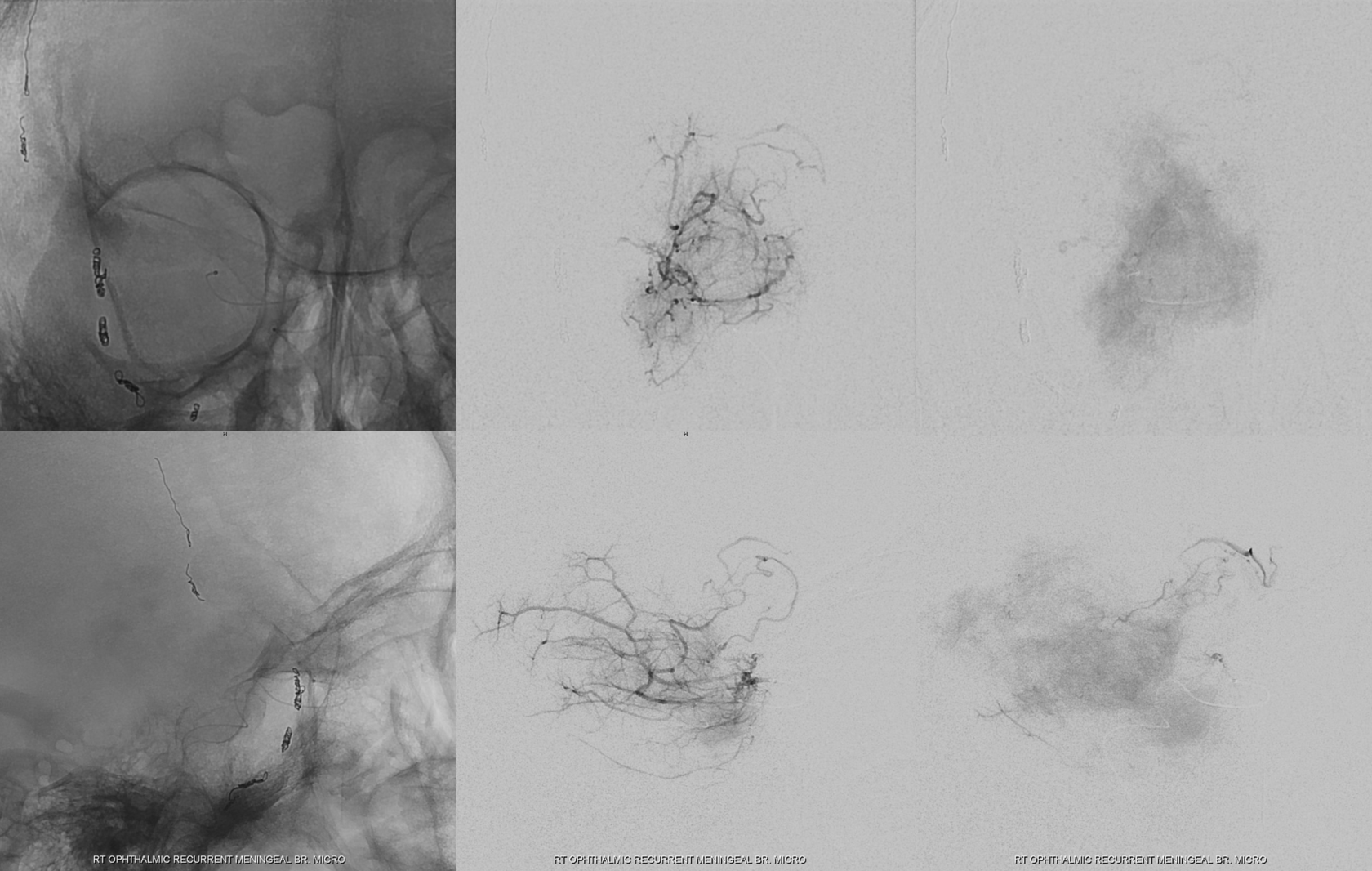
Particles are safest, in our opinion. Pretty much the only concern is reflux. There is no “pull” at the end, no chance of dragging glue or onyx on the tip, no need to build plugs or seek wedge positions. Particles and a coil or two at the end. If you are worried about bubbles that always come out with coils, don’t do them.
Amazing post embo DYNA distal to origin of the central retinal artery — see selective contribution of the ciliary arteries to the choroid — and no CRA in the middle of the nerve
DSA from the same position — a perfect demonstration that one can have a very nice choroid blush with no central retinal artery. Arrowheads on ciliary arteries.
More proximal post-embo DYNA shows the CRA also — see its proximal origin CRA = solid arrows. Central Retinal Vein = dashed ones
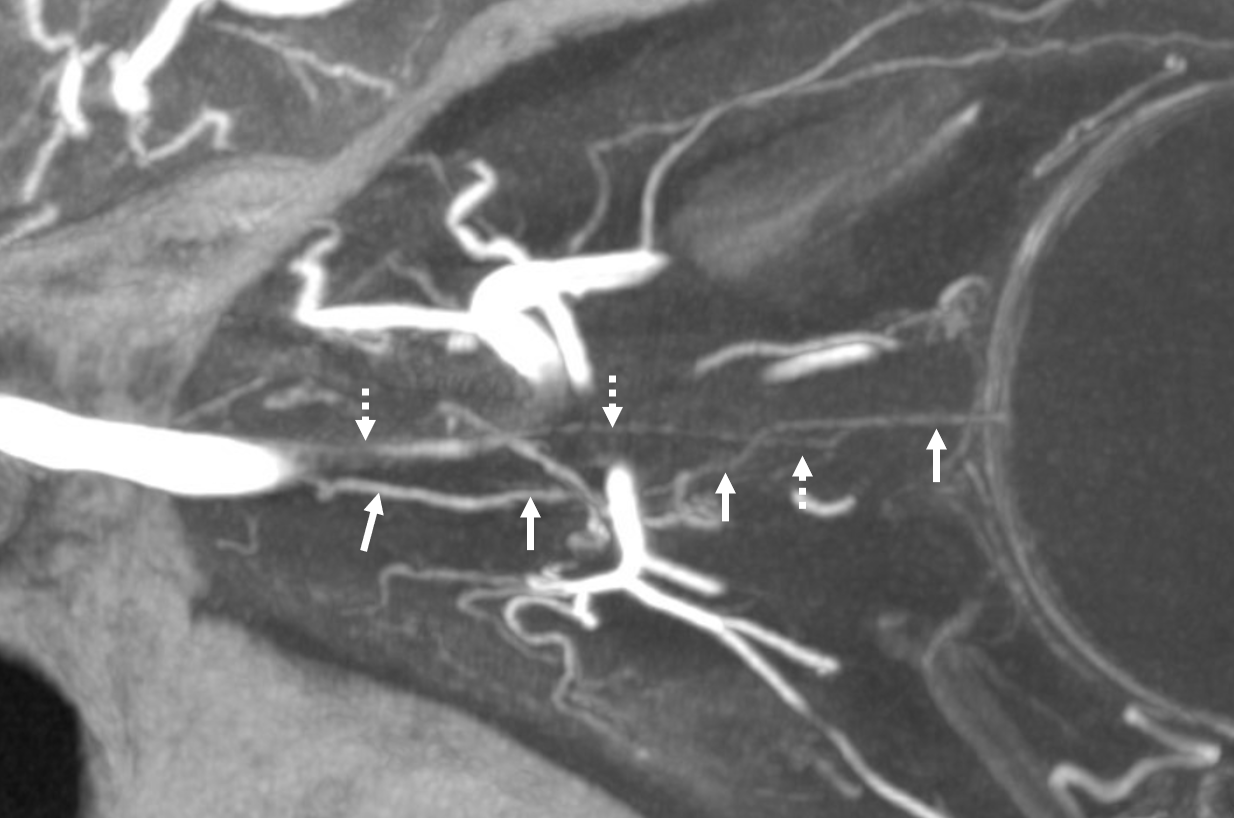
CRA = arrows; ciliary artery = arrowheads.

More to follow…