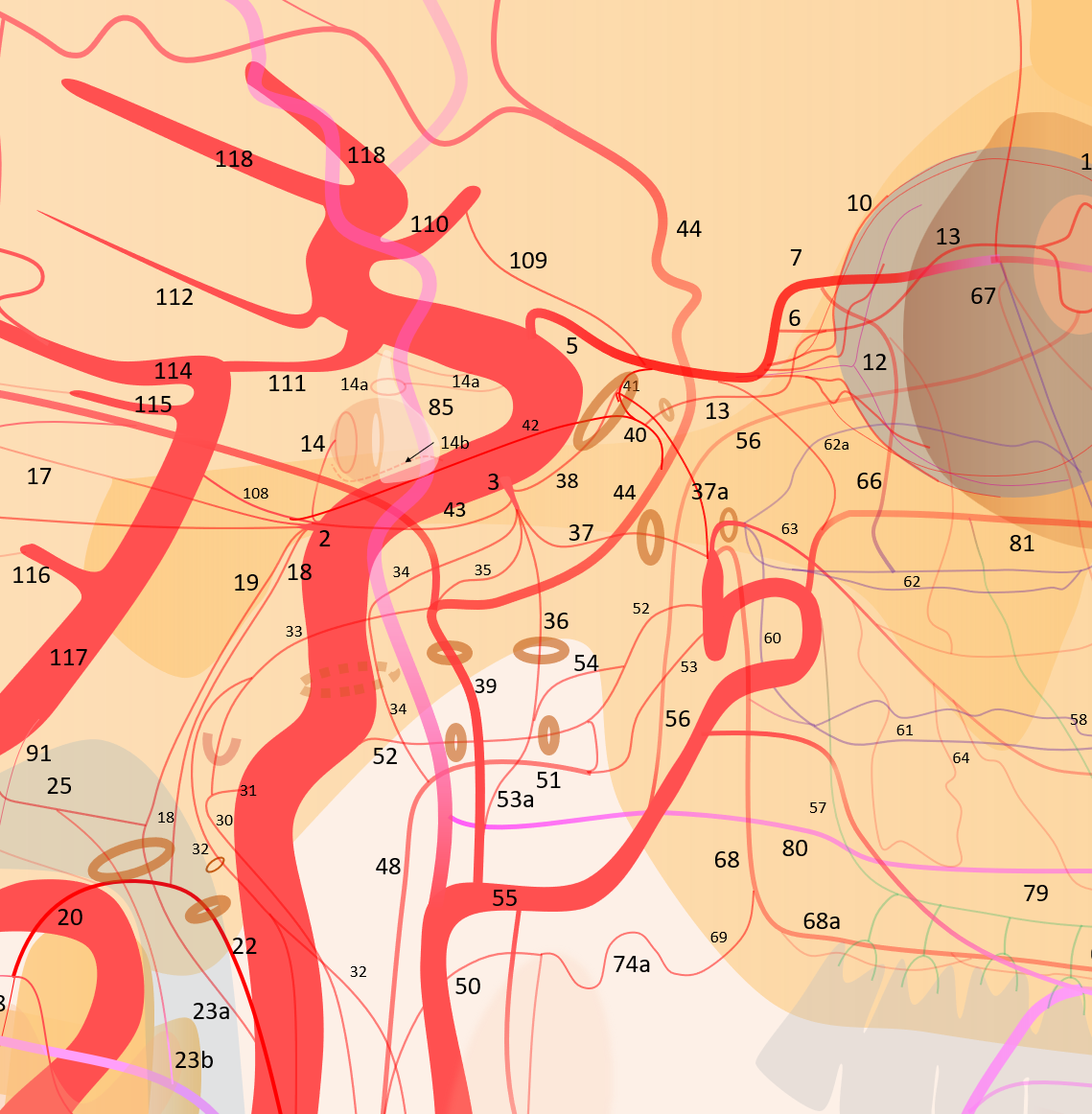
34 — Artery of Foramen Lacerum or Carotid Branch of the Ascending Pharyngeal Artery
Typically very small branch, extending between the superior division of the pharyngeal trunk of the ascending pharyngeal artery (51) and the cavernous ICA. Classically connects to the ILT (2). Usual supply is from the ascending pharyngeal, however as we always say it is a network, so supply can be visualized from either AP or ICA.
Is one of the “dangerous EC-IC anastomoses”. Very tiny usually and so rarely a problem.
Can be often involved in supply of JNA — Juvenile Nasopharyngeal Angiofibroma — an extremely vascular tumor that is essentially unresectable without a good preoperative embolization
Here is one (34, master diagram) supplying a JNA — as you can see it is seen from ICA injection, and does not extent to the ILT — they dont read books. Full JNA embo case here.

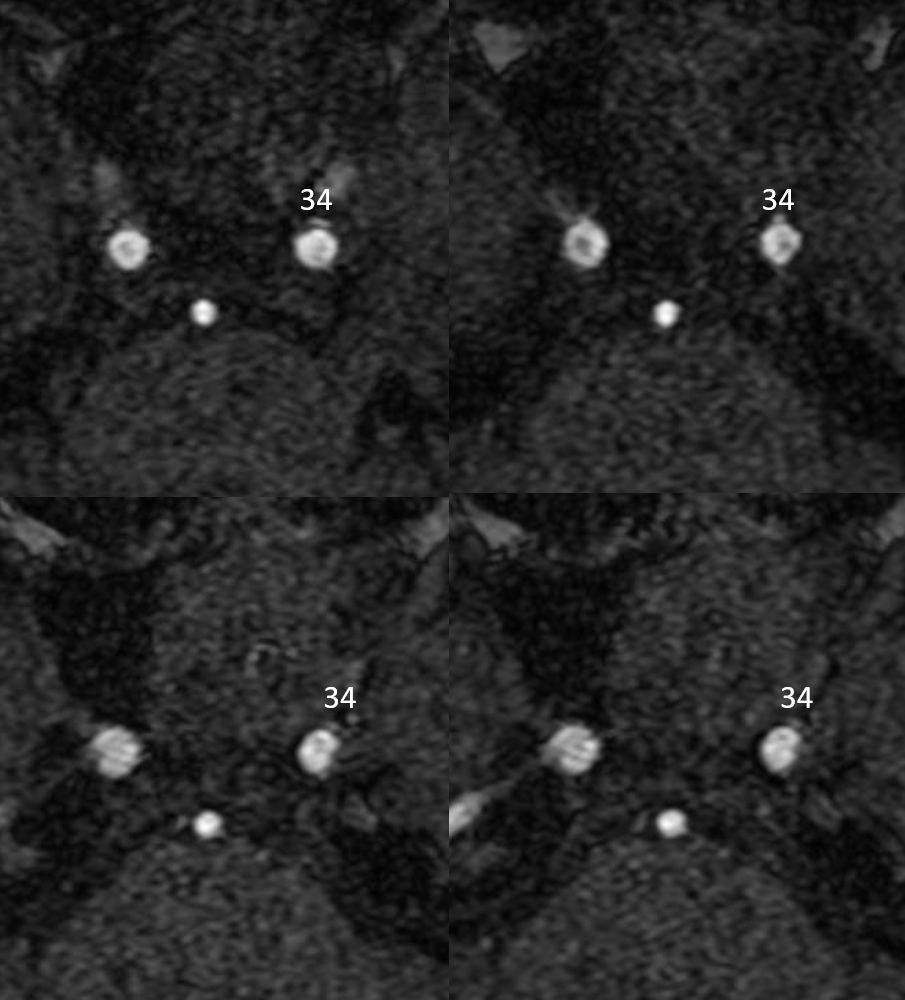
Remarkably it can be seen on the MRA as well
Another example off the Ascending Pharyngeal master page
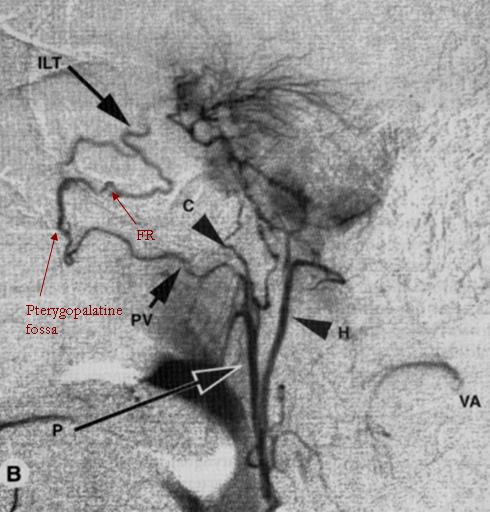
This remarkable lateral angiogram demonstrates multiple extracranial-to-intracranial anastomoses of the pharyngeal division. A pterygovaginal (Vidian) anastomosis of the AP artery leading to the pterygopalatine fossa, from where the artery of foramen rotundum (FR) re-enters the cranium to supply a meningioma and collateralizes with the Inferolateral trunk of the cavernous ICA. The carotid branch (C) a.k.a. artery of foramen lacerum is also nicely visible. The hypoglossal division (H) contributes extensively to supply of the meningioma. Muscular collaterals to the vertebral artery are also present (VA) Image taken from Lasjaunias and Berenstein, first edition.
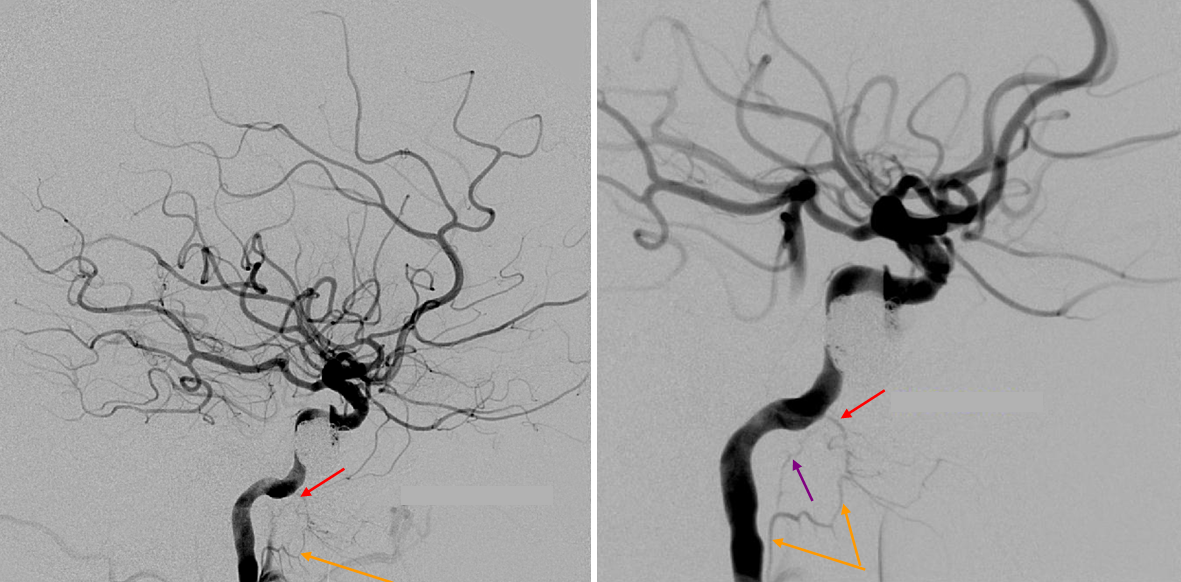
Another example — two lateral views of internal carotid injection demonstrating a mandibulovidian artery (52) (red) collateralizing with superior division of the ascending pharyngeal (orange). The foramen lacerum branch (purple) is also visible
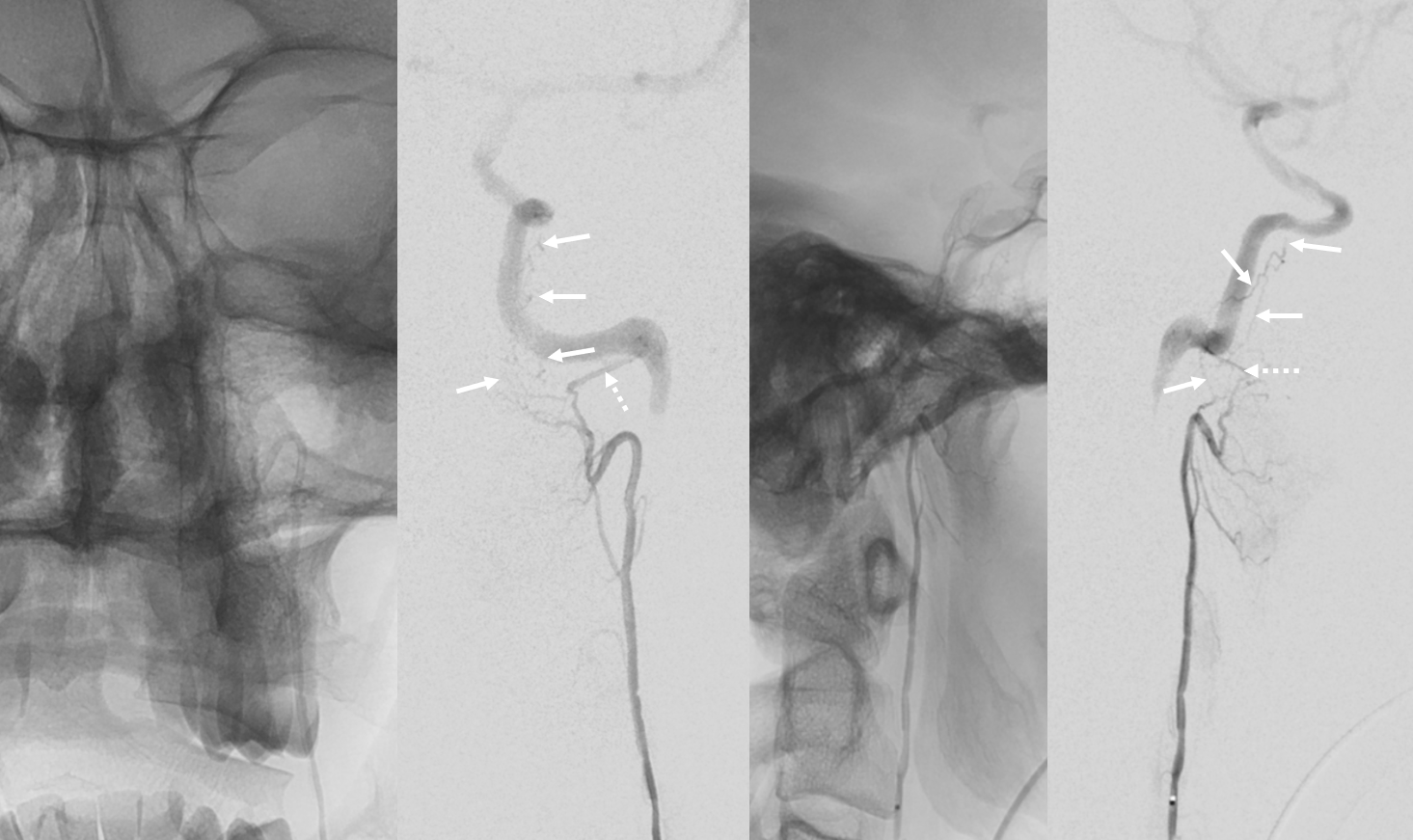
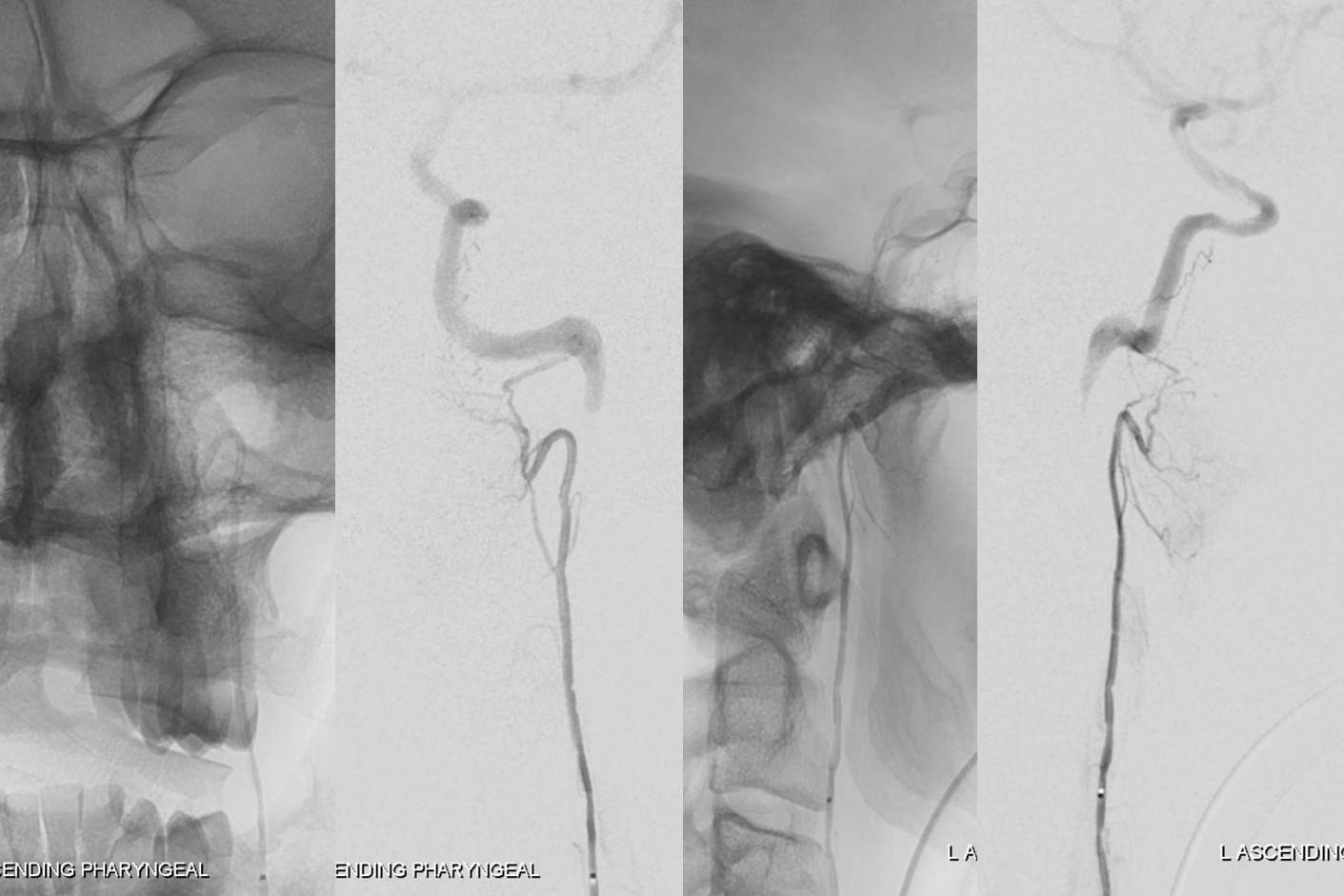
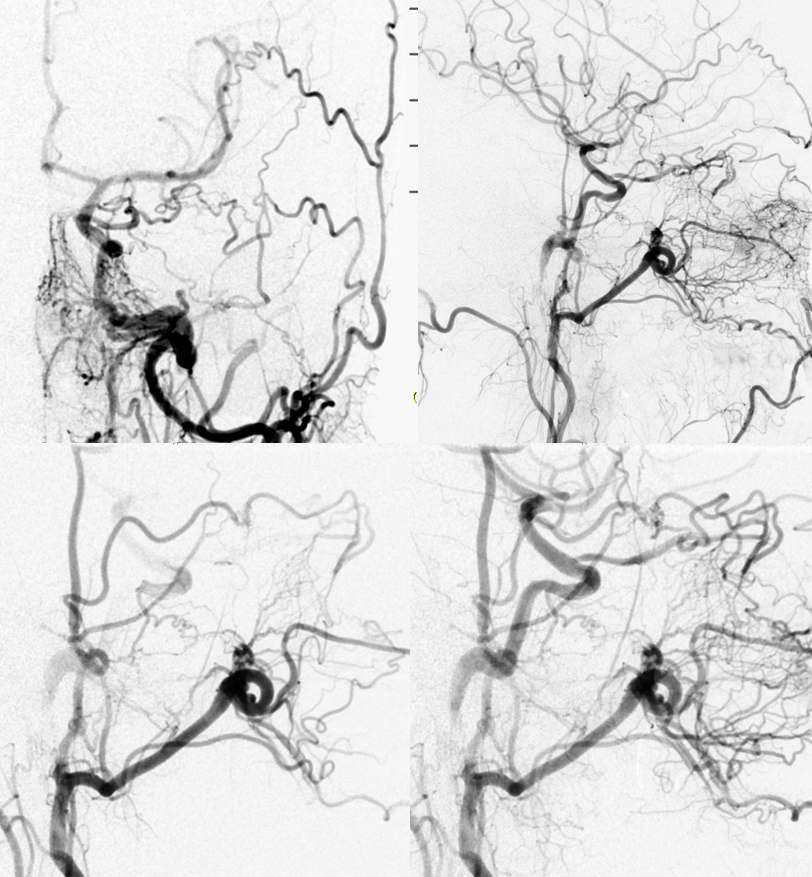
Most commonly this branch is seen in setting of AP to ICA collaterals due to cervical ICA occlusion. Much more frequently, the superior division of pharyngeal trunk connects with the ICA via the vidian branch (dashed arrows). This is NOT the carotid branch, although it is frequently mistaken for it. On 2D-DSA, the characteristic thing about the carotid branch is that it really runs parallel to the ICA, just below it (dashed arrows). Best seen though on Cone Beam CT — definitively in the carotid canal etc. Most commonly seen as a collateral in cervical ICA occlusion, as in case below. Even for a rarely seen branch such as this, there is really a network rather than single vessel — best seen in frontal view. Underscores how much more there is than seen by the eye
without arrows
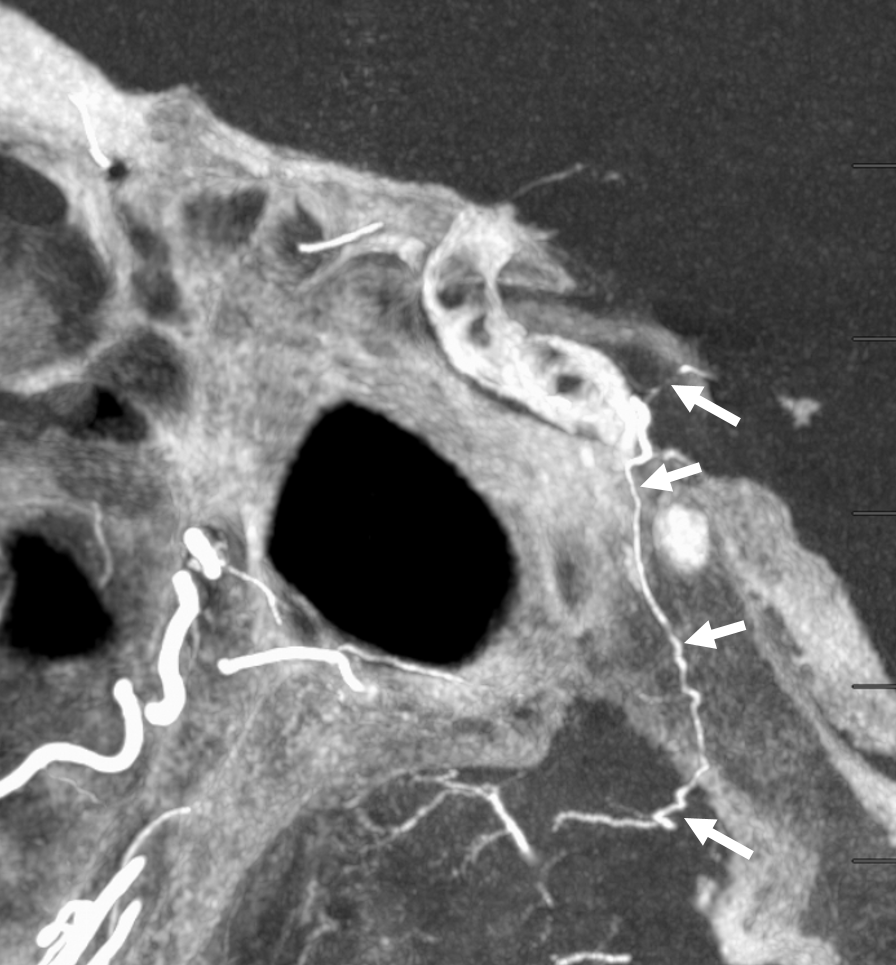
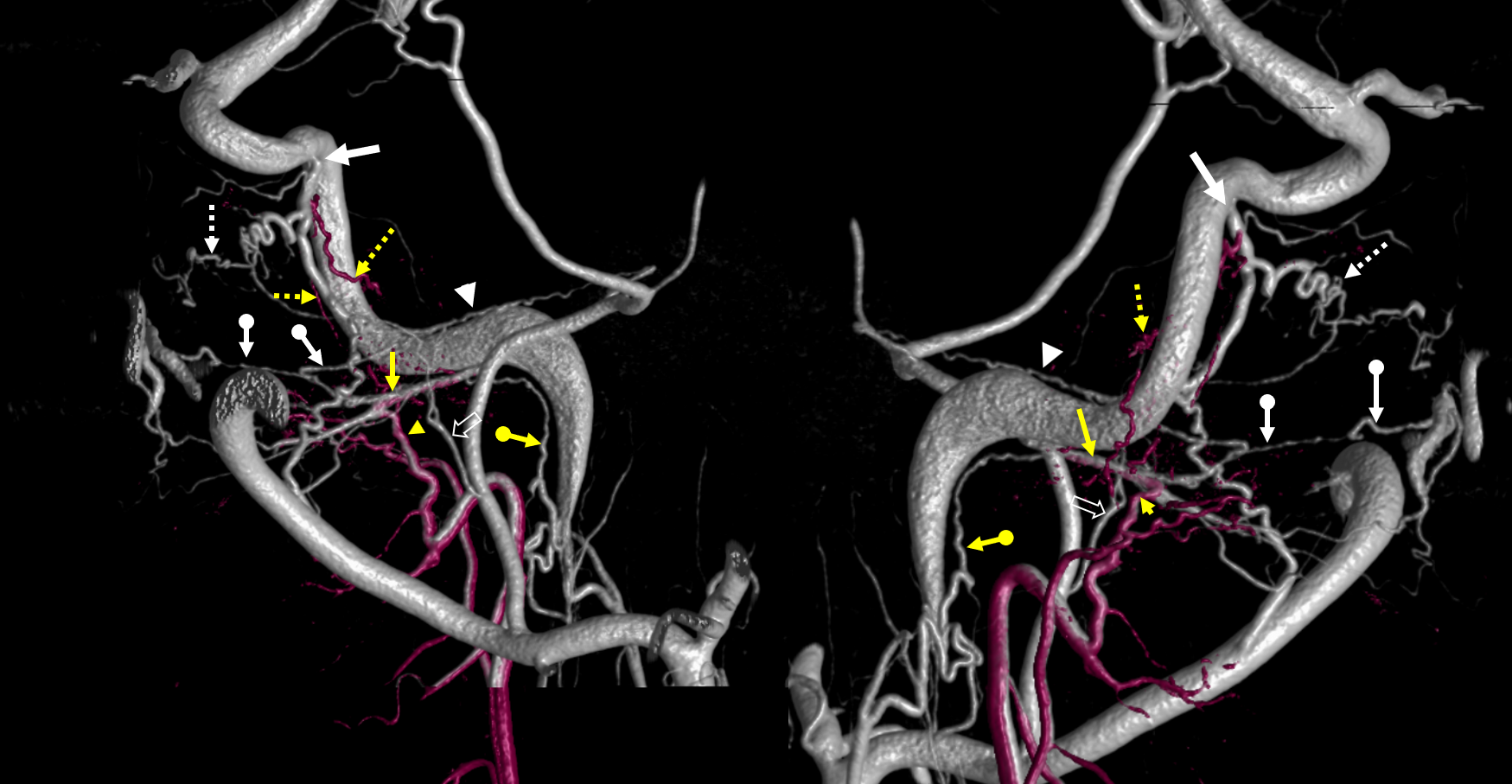
Cone beam fusion of pharyngeal division hand injection (purple) and ECA global injection. Superior division AP = yellow arrowheads; vidian = yellow arrows; Carotid AP branches = dashed yellow arrows; ILT = white arrow; Foramen rotundum branches = dashed white arrows; palatovaginal / pterygovaginal = ball white arrows; neuromeningeal trunk lacerum anastomosis with the vidian = ball yellow arrows; cavernous branch of the MMA = white arrowheads; Accessory Meningeal = white open arrows
Stereos

Cone Beam CT axial MIP — Pharyngeal division micro – Siemens ICONO 10 second dual volume non-binned FOV 22, hand injection 100% contrast, with “secondary reconstruction”
Same dataset with fusion of ECA and above AP injections
ECA injection — multiple anastomoses with the ophthalmic artery also
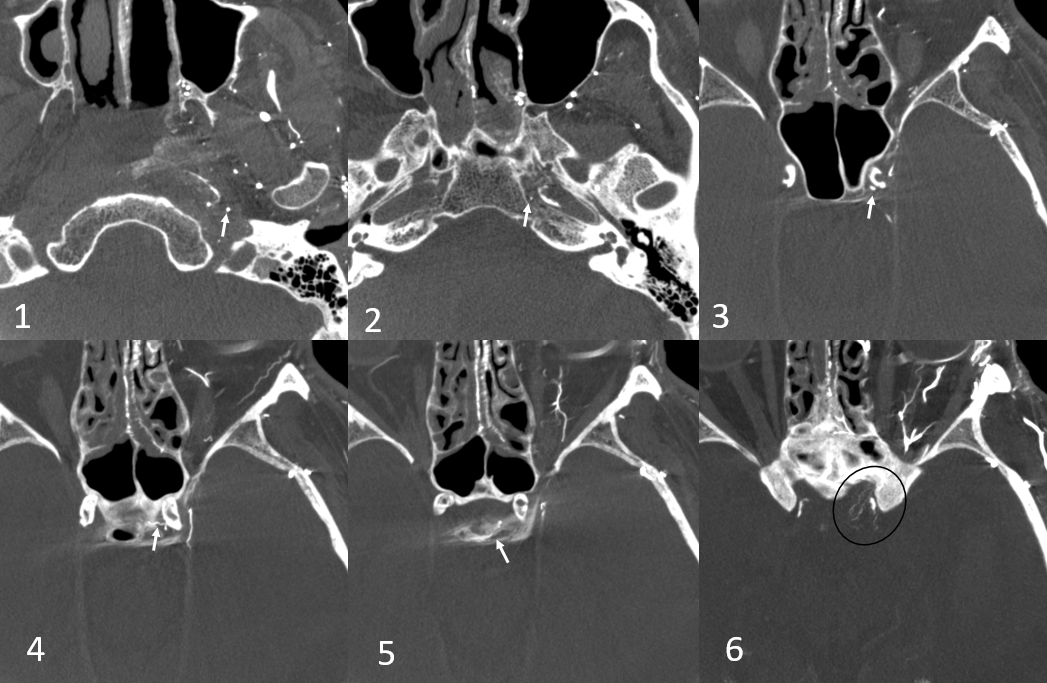
Carotid Branch Supply of Posterior Pituitary
Anything is possible. Here is a carotid occlusion case. The AP carotid branch (arrows) traverses the lacerum, ultimately supplying the posterior hypophysis (the carotid is occluded from cervical bifurcation, and MHT is apparently out our hypoplastic also). Note optic nerve network (black oval) that is often prominent when ICA is closed