

14a above — a very rarely seen by Digital Subtraction Angiography, but much more commonly with Cone Beam / Flat Panel CT, tiny vessel or vessels arising from the “hypophyseal” segment of the internal carotid artery — a proximal intradural segment also known as supraclinoid, paraophthalmic, etc. See ICA page for details of this semantic disorder.
The artery arises from the medial carotid wall — pituitary is medial to the carotid — and supplies the hypophysis, by definition — the pituitary — usually anterior hypophysis and pituitary stalk. The inferior hypophyseal arteries (from the MHT) are usually much bigger and supply the posterior pituitary.
The “hypophyseal aneurysm” — a medially or inferiorly projecting aneurysm from the hypophyseal segment — is thought to be related to this branch — at least by those who believe that aneurysms must arise from branch points. Aneurysms, of course, don’t care for our opinions, but we are right more often than not.
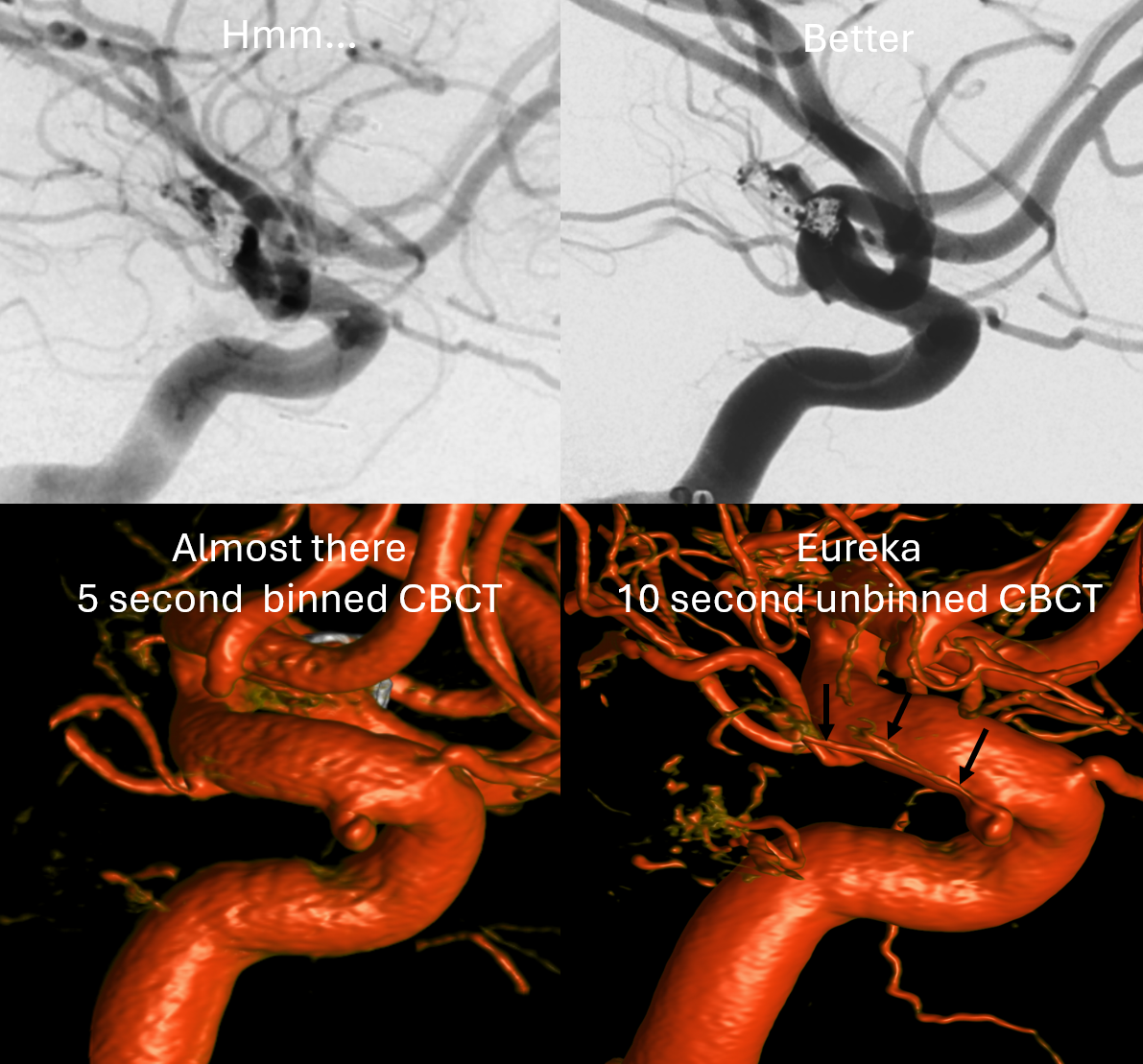
If you want to see hypophyseal arteries, do some high res DYNA of VASO imaging. Because of superimposition over the carotid in lateral views, again, its hard to see. Below is an example of why this artery, always there (always, yes! — occlusion is pathologic always such as athero) depends on technique
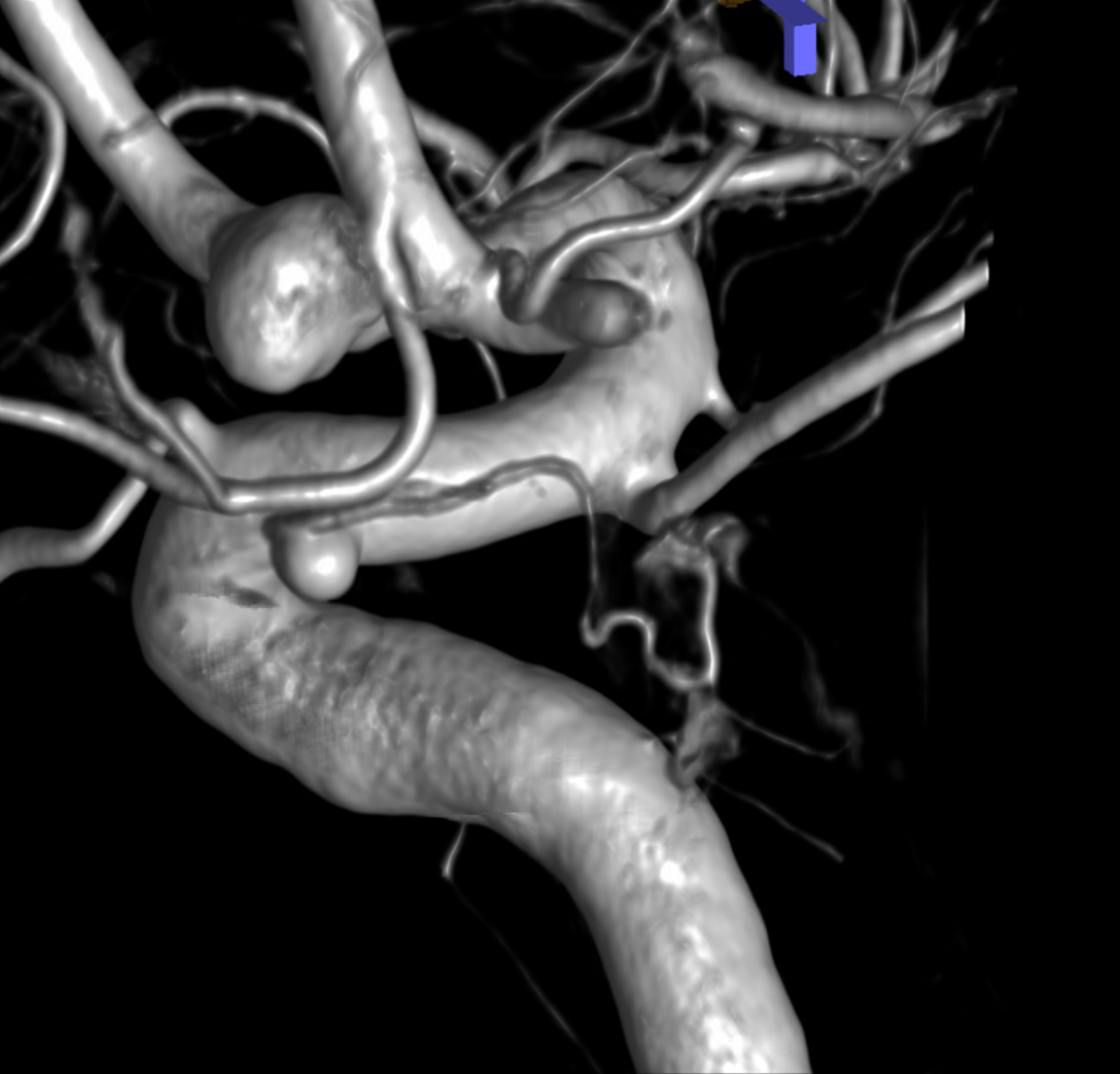
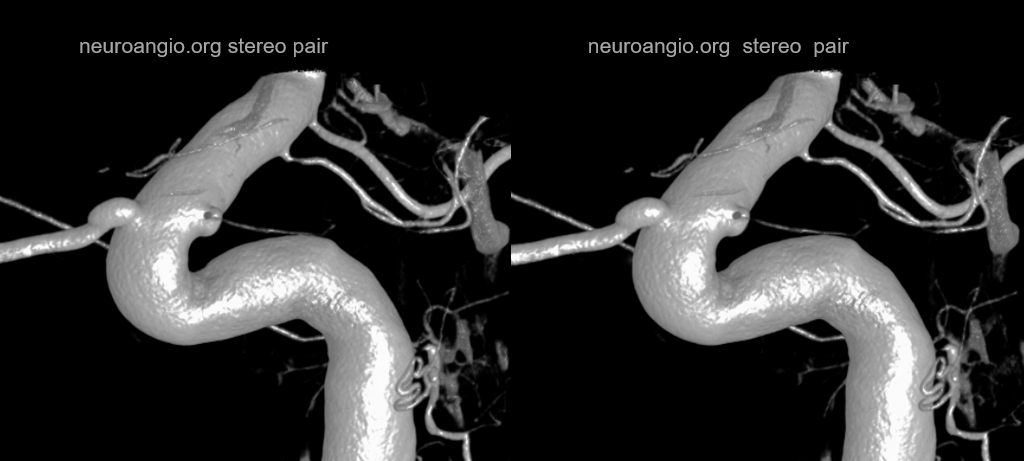
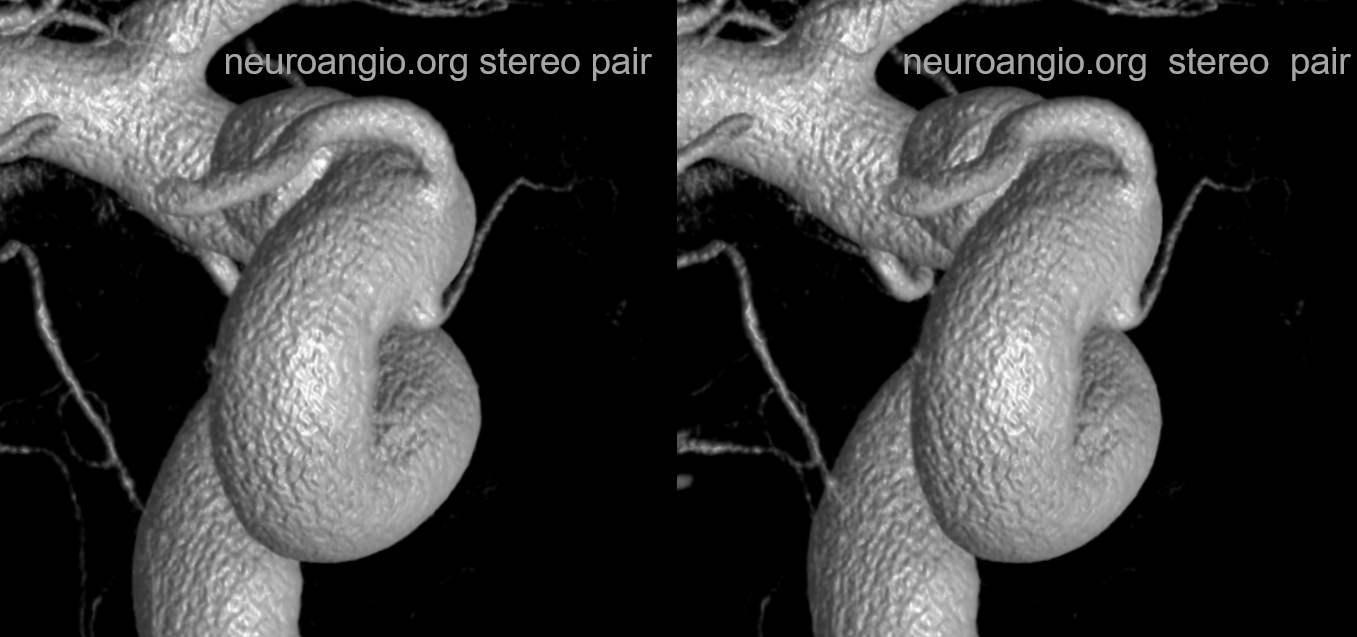
Stereos and MIPs. Both superior and inferior hypophyseals are well seen. The superior hypophyseal, despite being invisible on standard issue views, is quite large, even having two branches to the hypophysis.
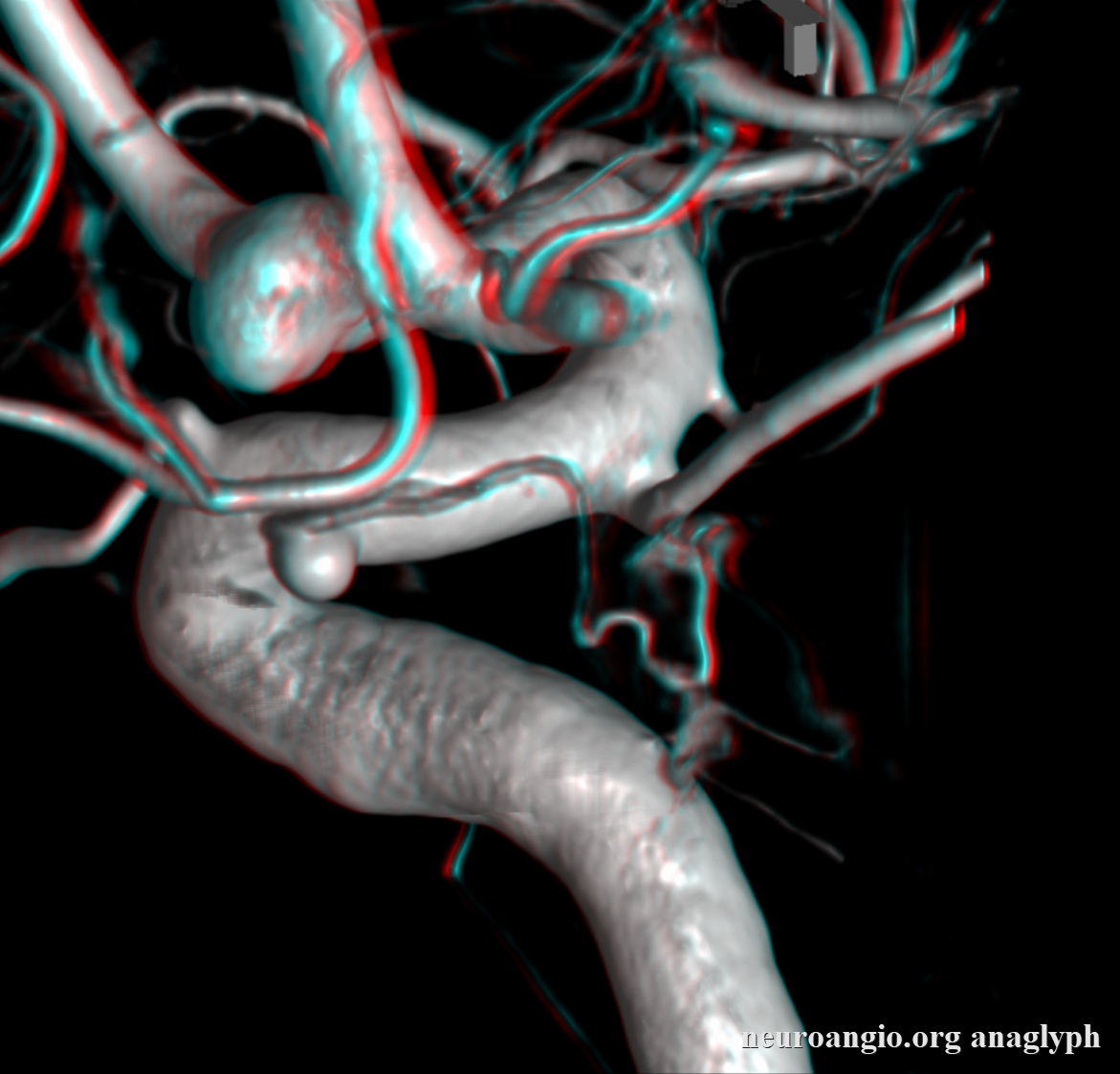
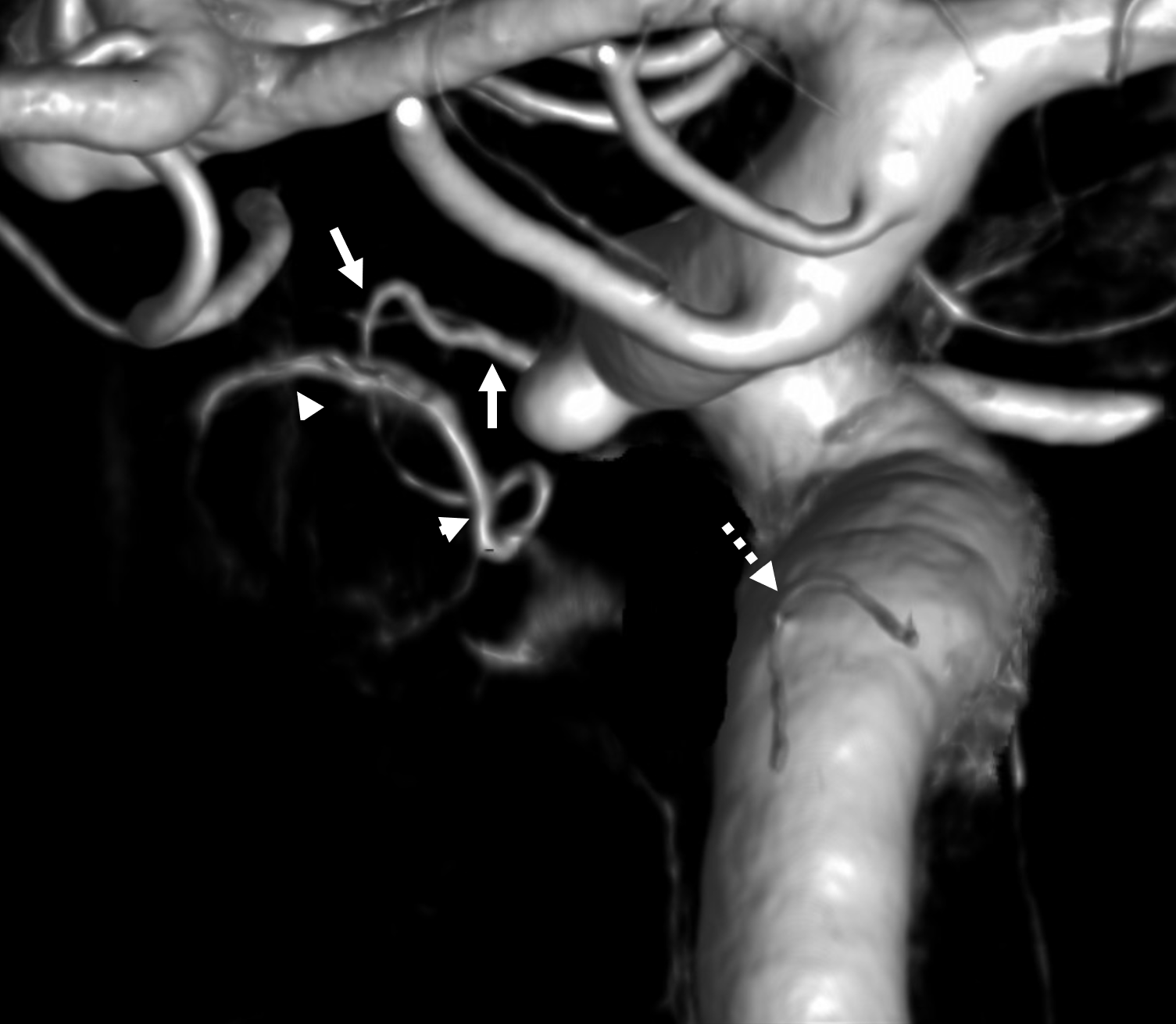
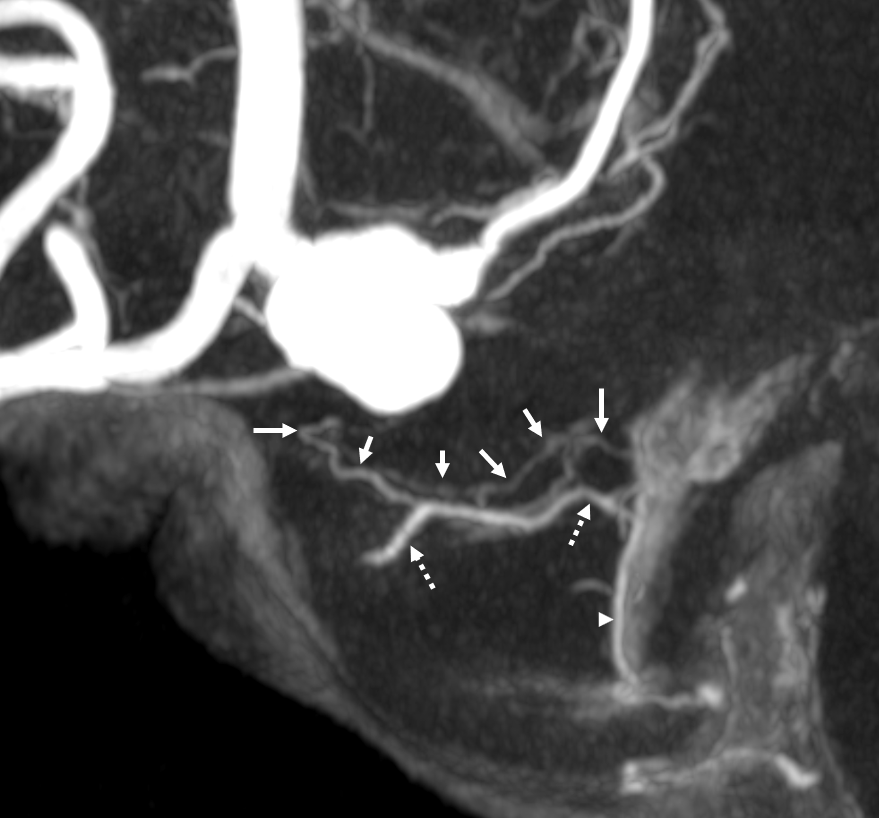
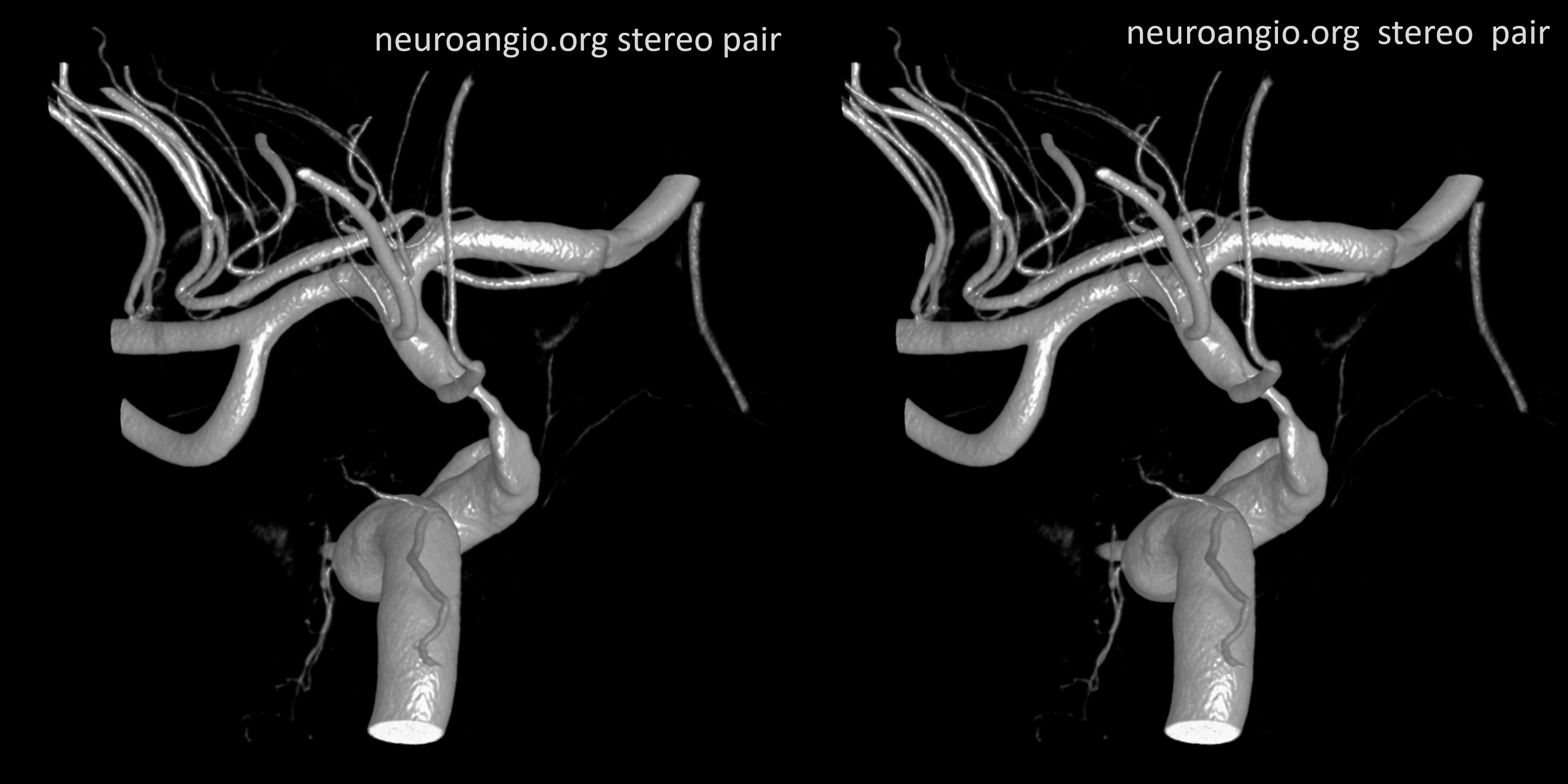
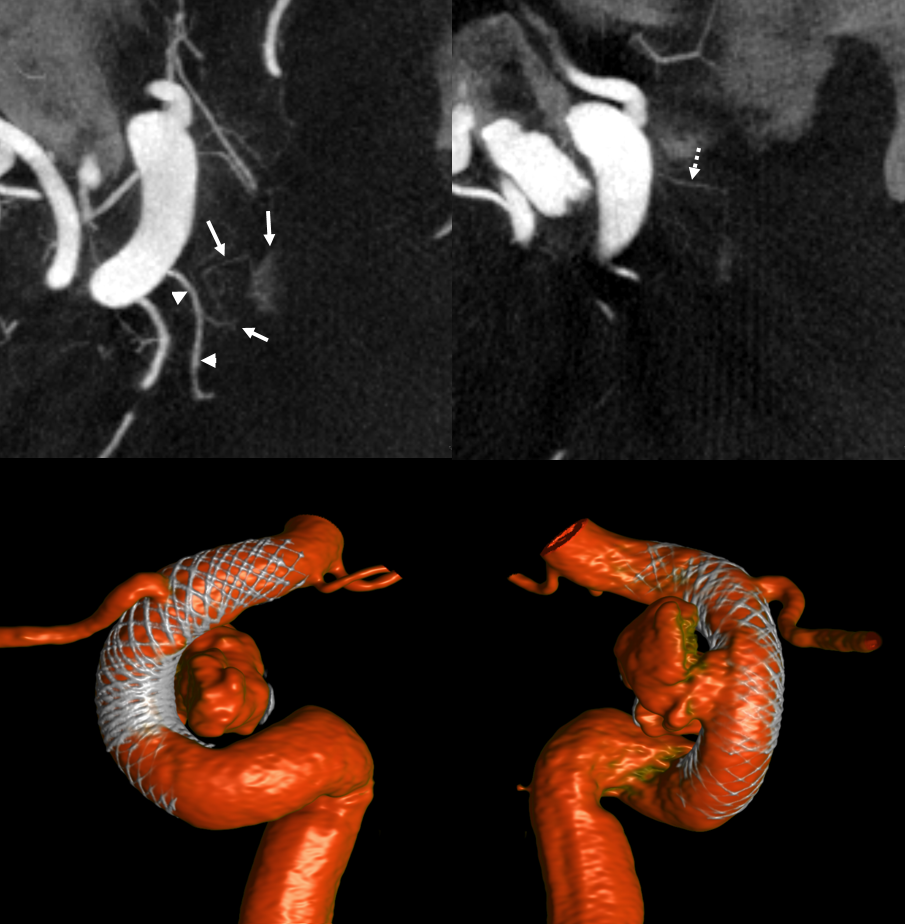
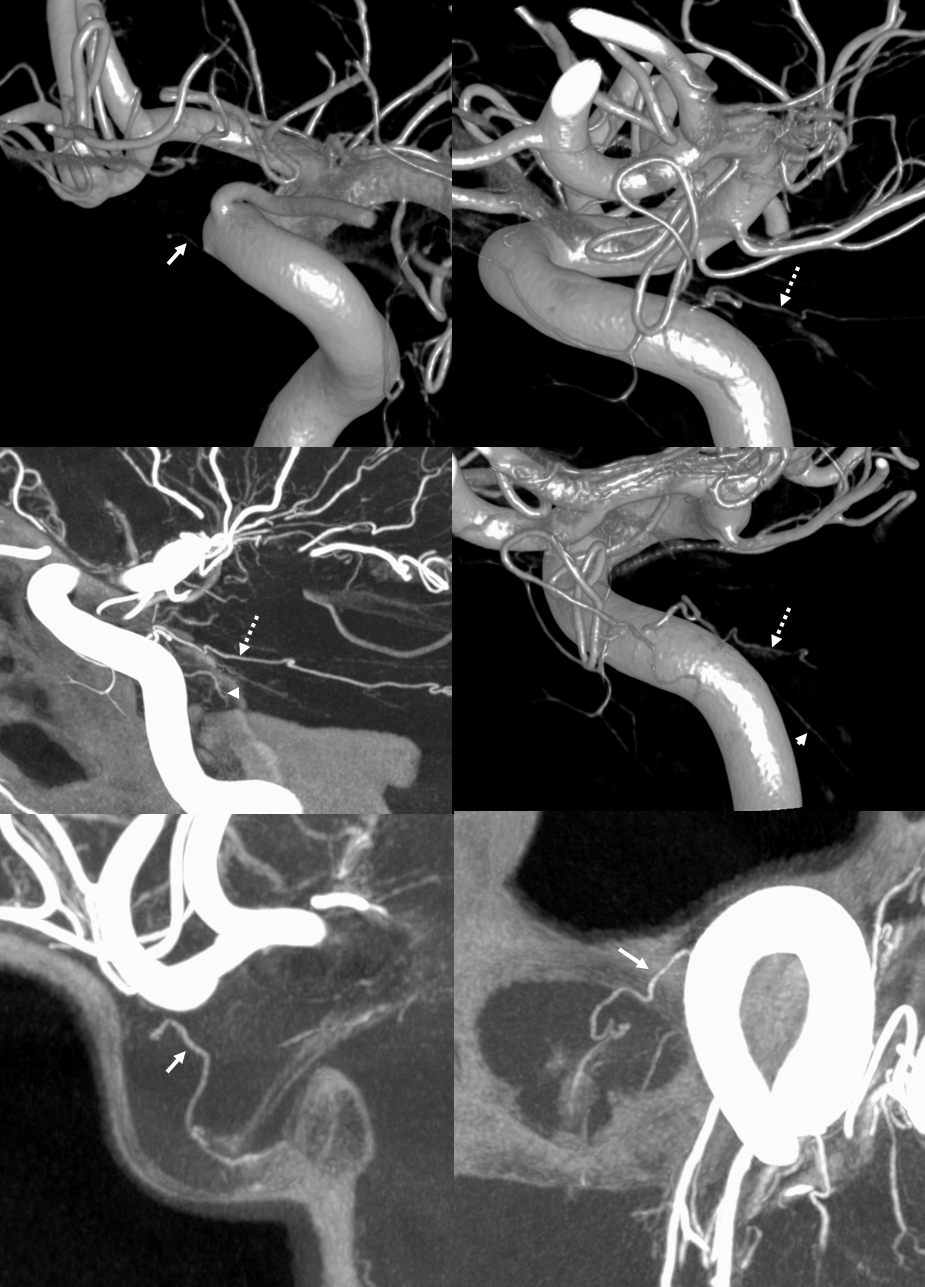
Case courtesy Dr. Eytan Raz — here is a beautiful example of a very dominant superior hypophyseal artery (arrow) supplying the posterior hypophysis (arrowhead), with a correspondingly small inferior hypophyseal contribution from the MHT (dashed arrow)
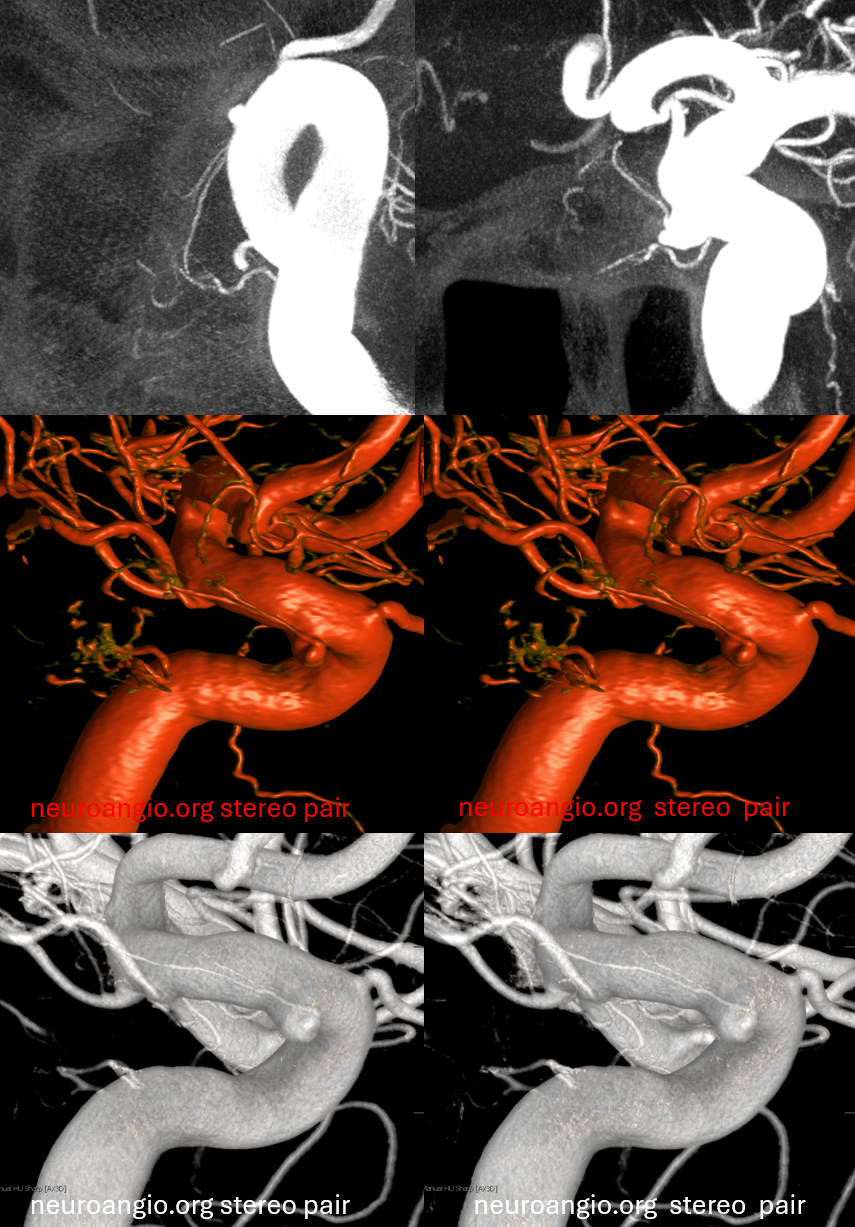
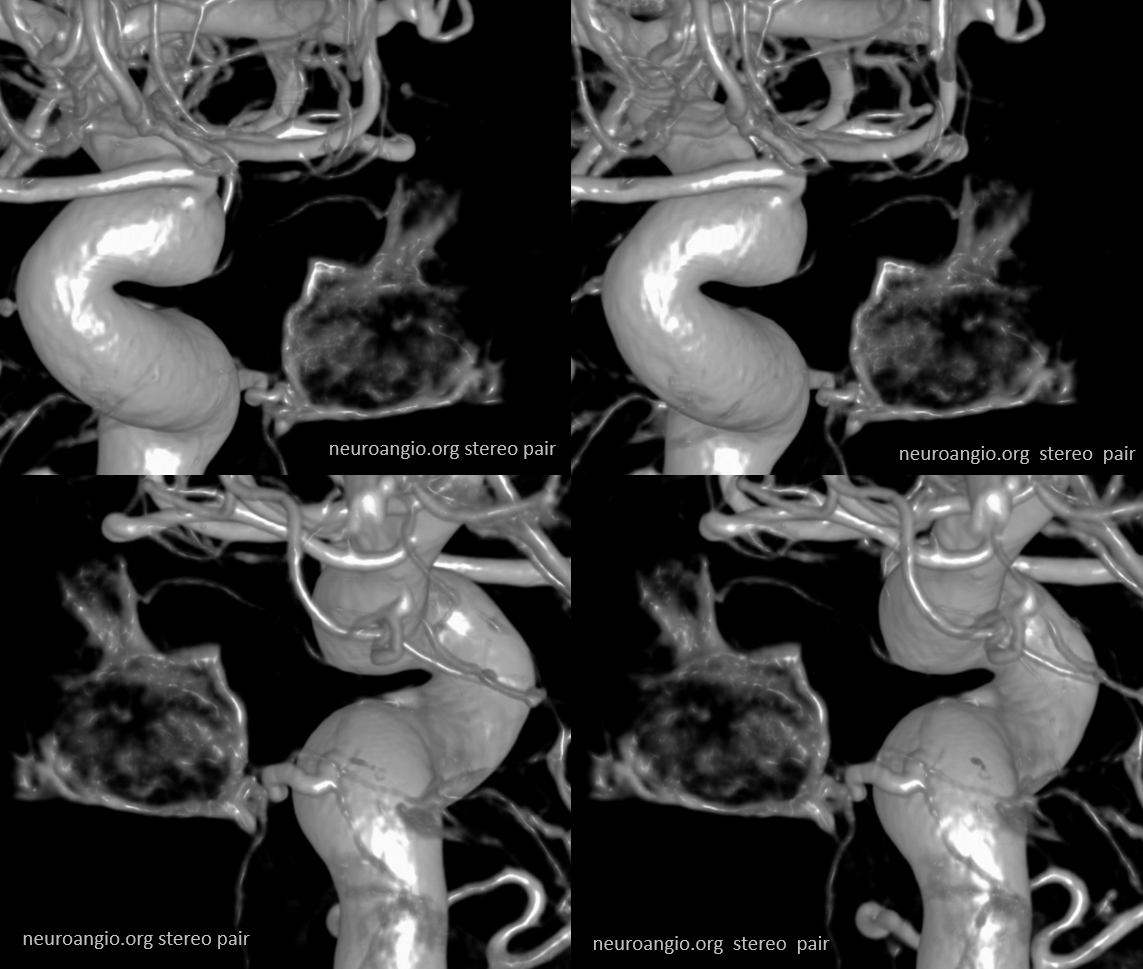
Cross eye stereo
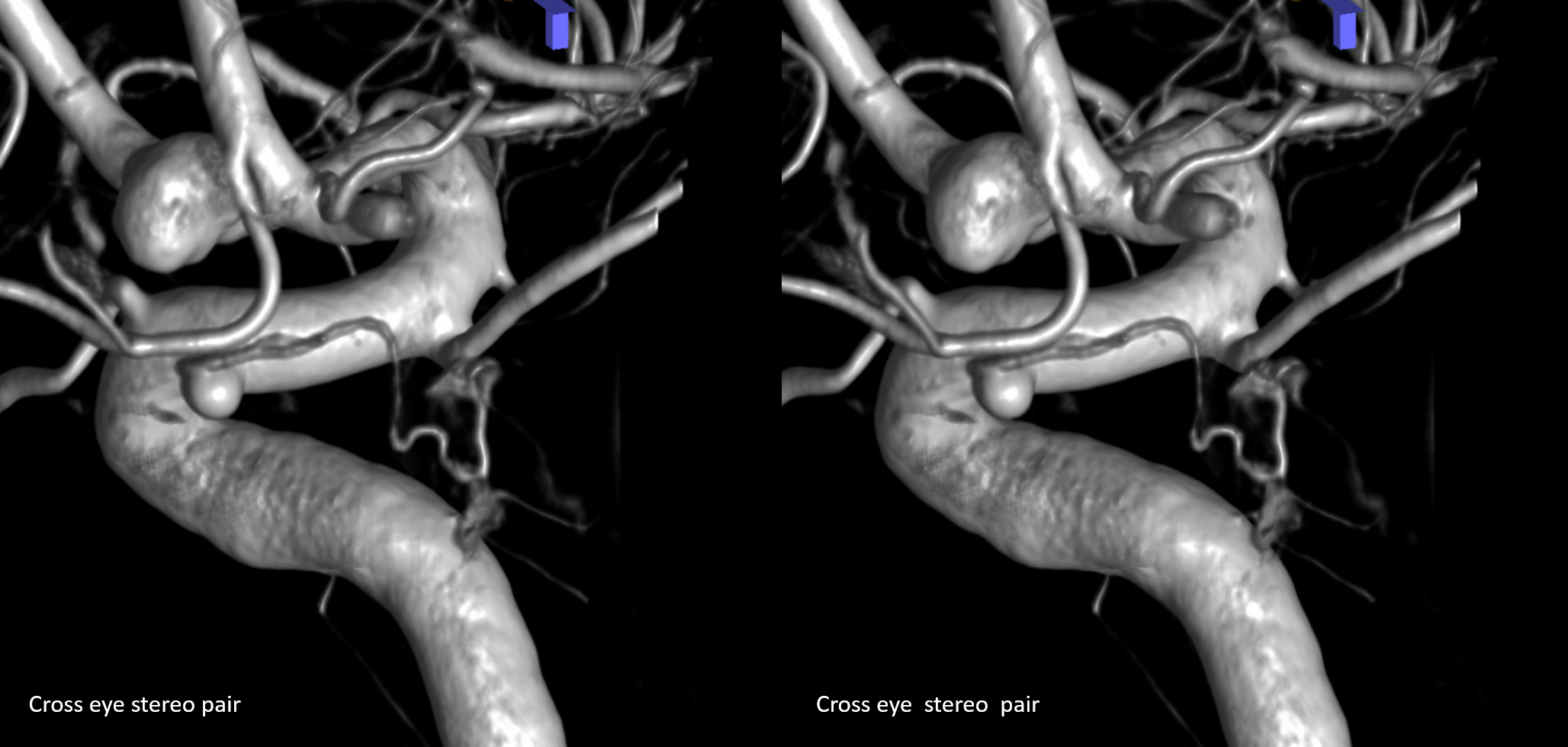
View from the back — again small inferior hypophyseal, big superior hypophyseal — balance again… See the beautiful vascular ring of the posterior pituitary — the connecting it with the contralateral side
Cross-eye stereo

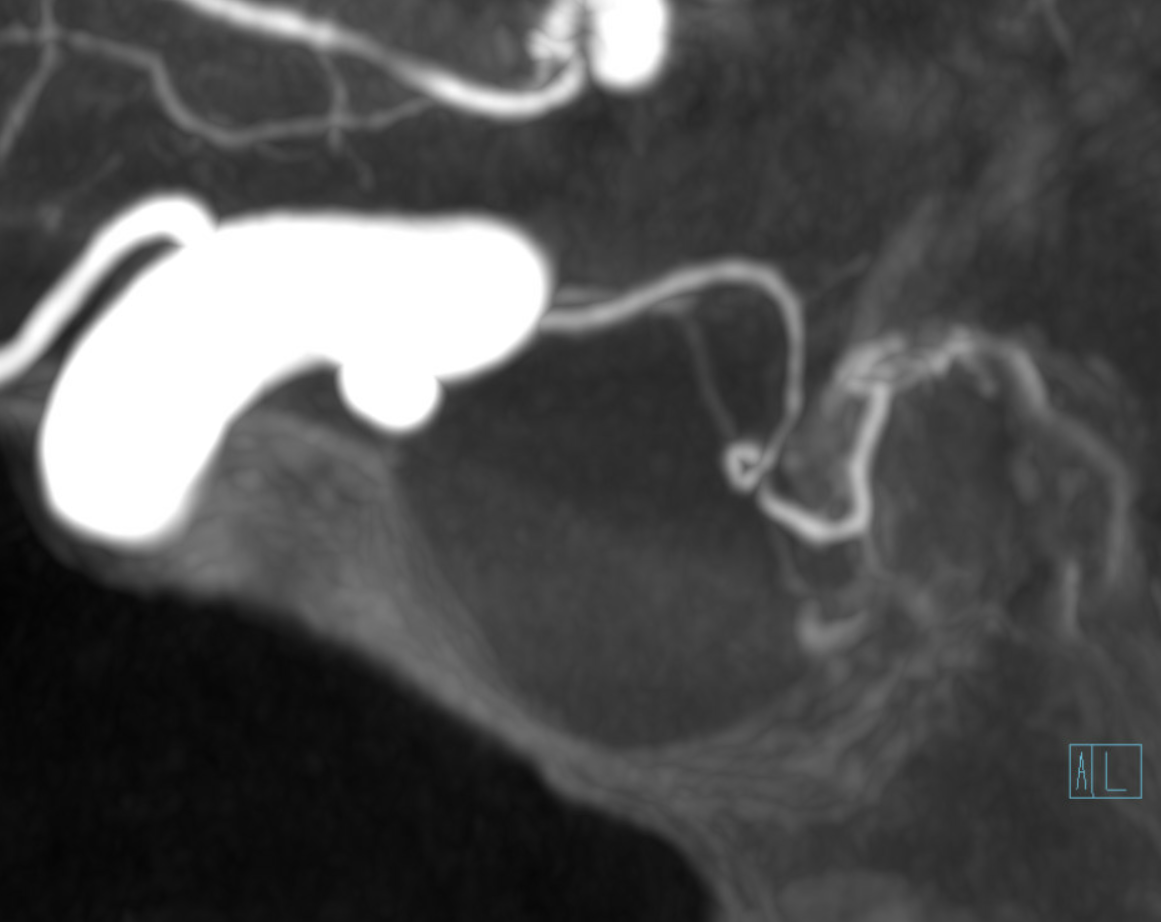
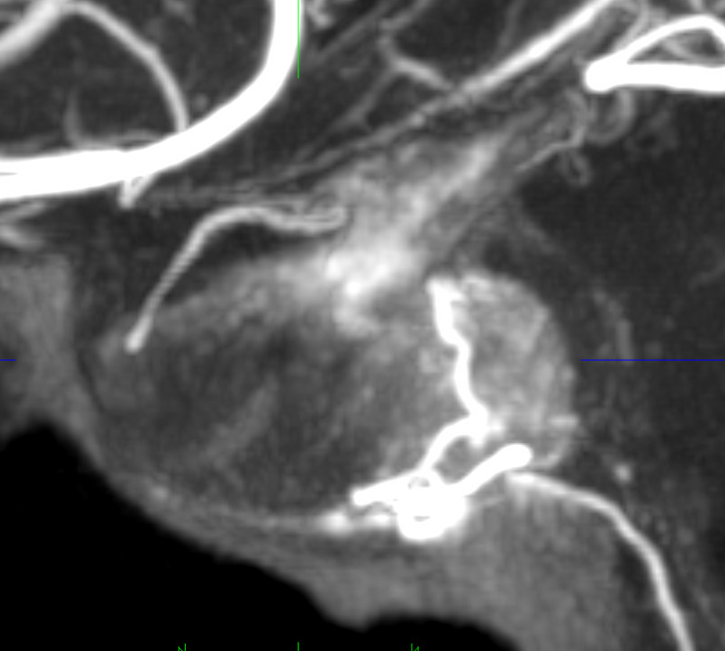
MIP image shows the sella nicely — and helps prove its posterior pituitary
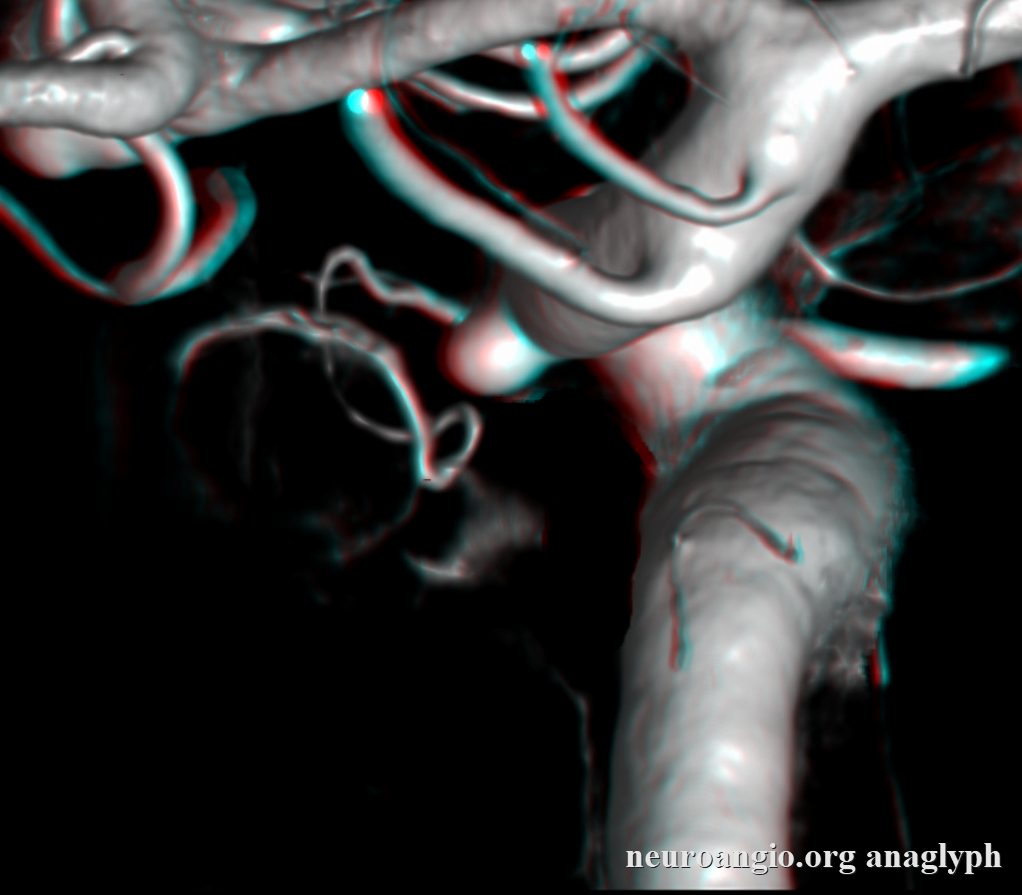
Pure arrowless images — easier to steal…

Of course, there is an aneurysm here — the branch point camp would point out how this larger than usual branch is a setup for aneurysmal formation. Naturally…
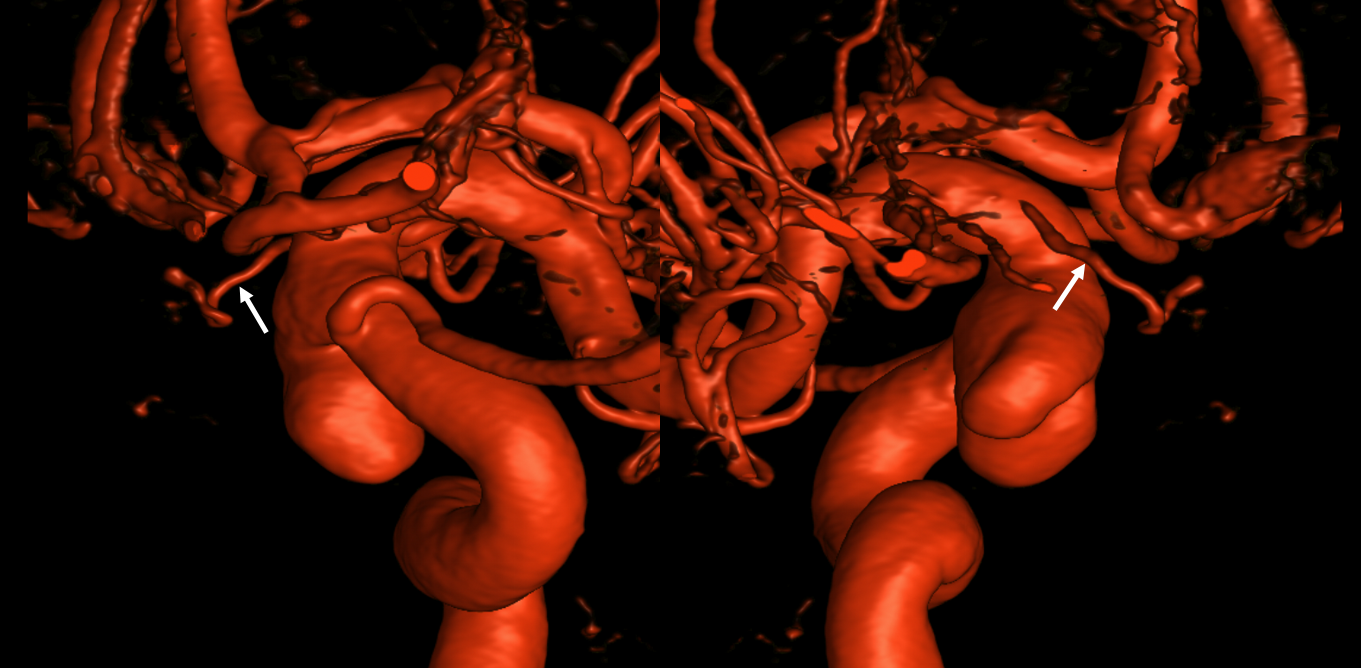
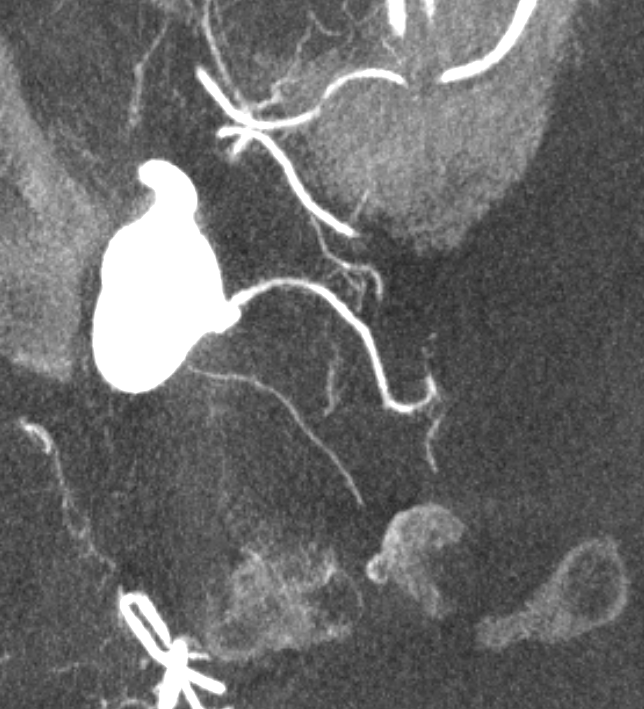
Below is a Volume Rendered typical arrangement — a slender (but still large by its own standards) superior hypophyseal supplies the stalk (and anterior pituitary), while inferior hypophyseal from MHT supply the posterior pituitary.
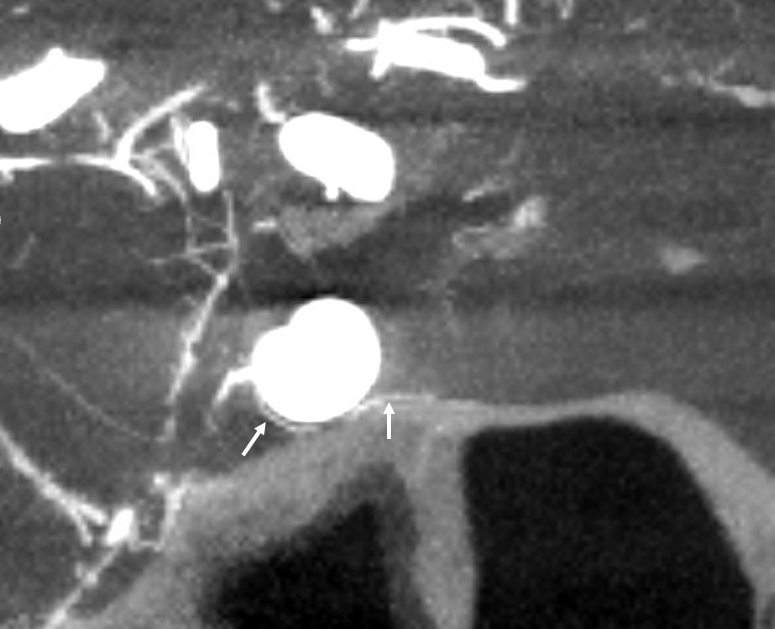
Sagittal MIP of the pituitary
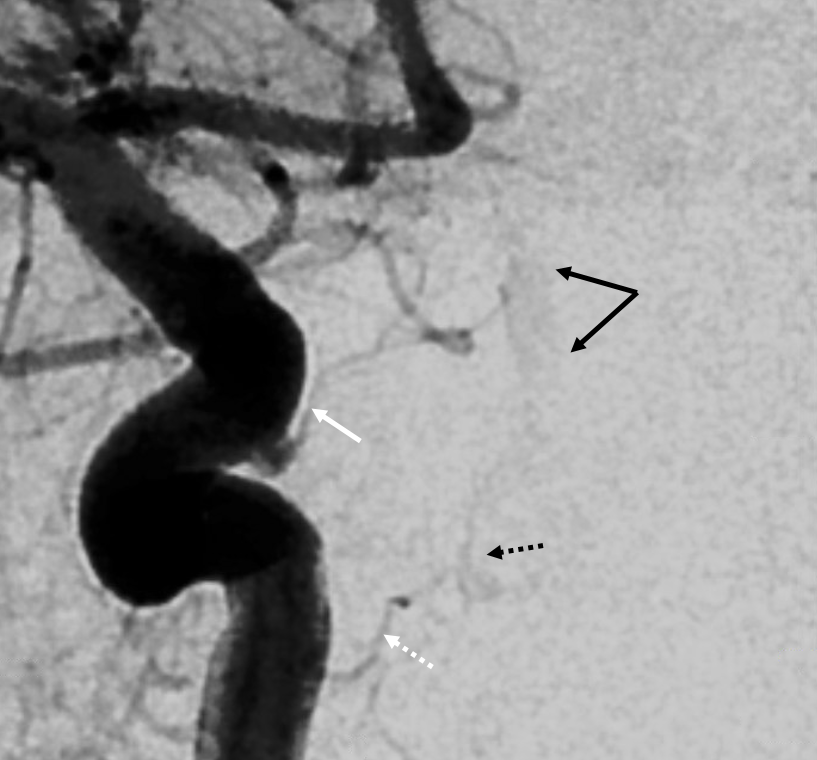
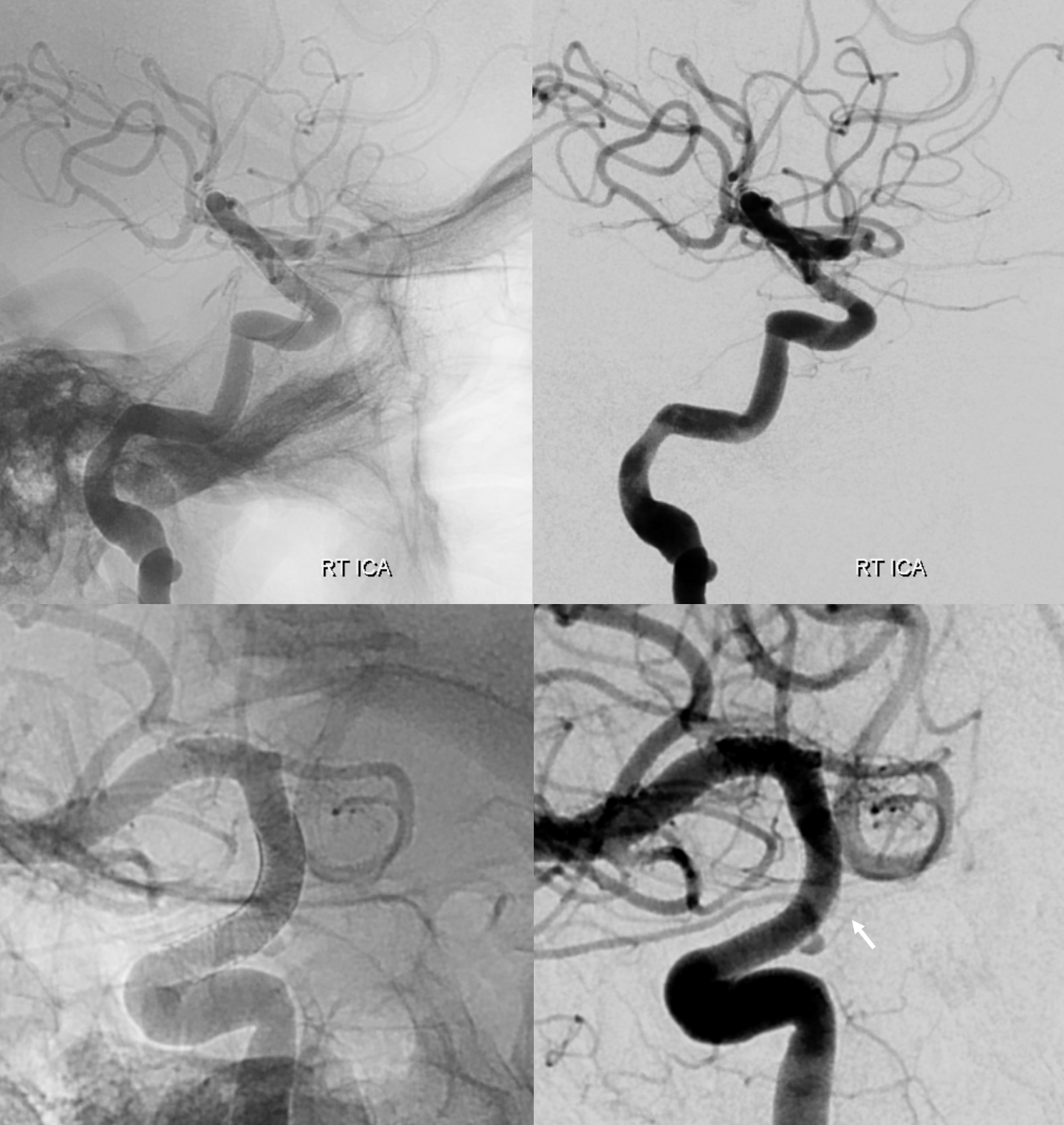
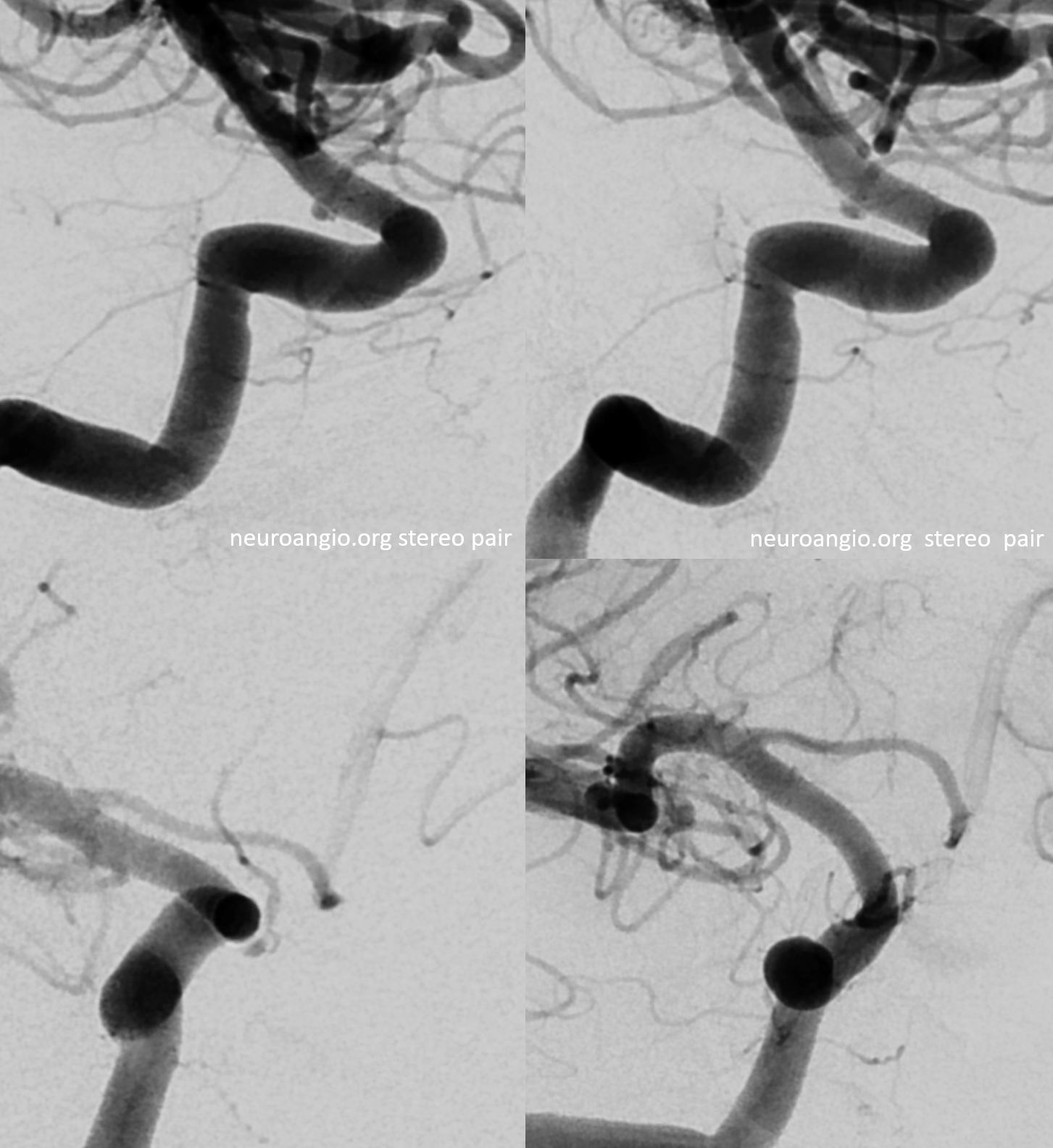
DSA — yes, they do exist on DSA also. A slight contralateral oblique is probably best — to throw them off other vessels. Here, an LAO of right ICA injection shows a farily promenent superior hypophyseal (white arrow, with an infundibulum), supplying the pituitary stalk (black arrwos). Also seen is inferior hypophyseal (dashed white arrow) supply of the posterior pituitary (dashed black arrow)
Supply of the Hypophysis and Balance
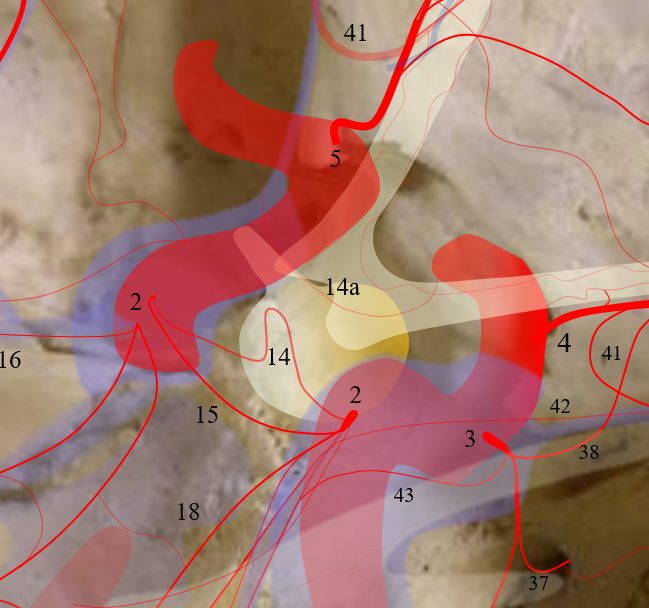
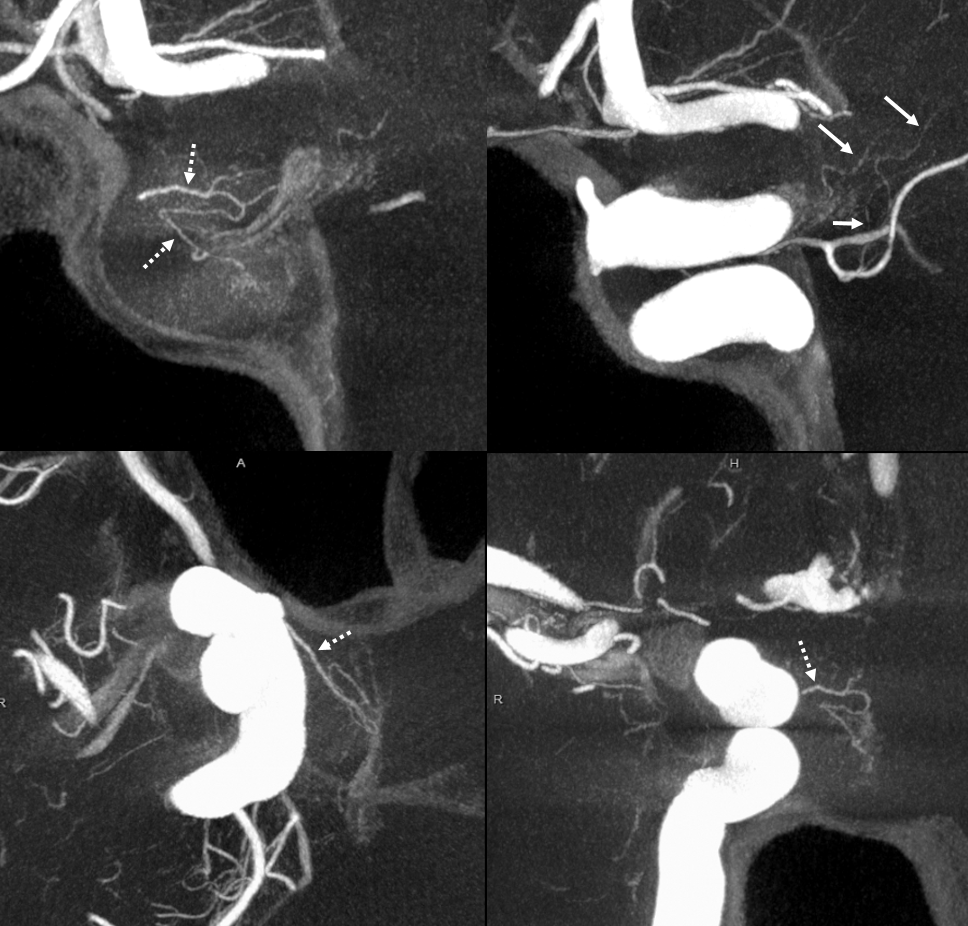
As always neuroangio is about balance. There may be one or more superior hypophyseal arteries. Usually one is visible by cone beam/flat panel CT. Sometimes more than two. Here there are 3. Nicely shown is supply of the stalk (open arrow). There is also likely contribution to the optic chiasm, which is of course very important. The inferior hypophyseal branches (dashed arrow) from the MHT support the posterior pituitary. The ILT is hypoplastic, with lateral branches of the MHT (white arrowhead) heading towards the meckel cave and the recurrent branch along the tentorial edge (black arrowhead) supplying territory normally done by the ILT
Without labels
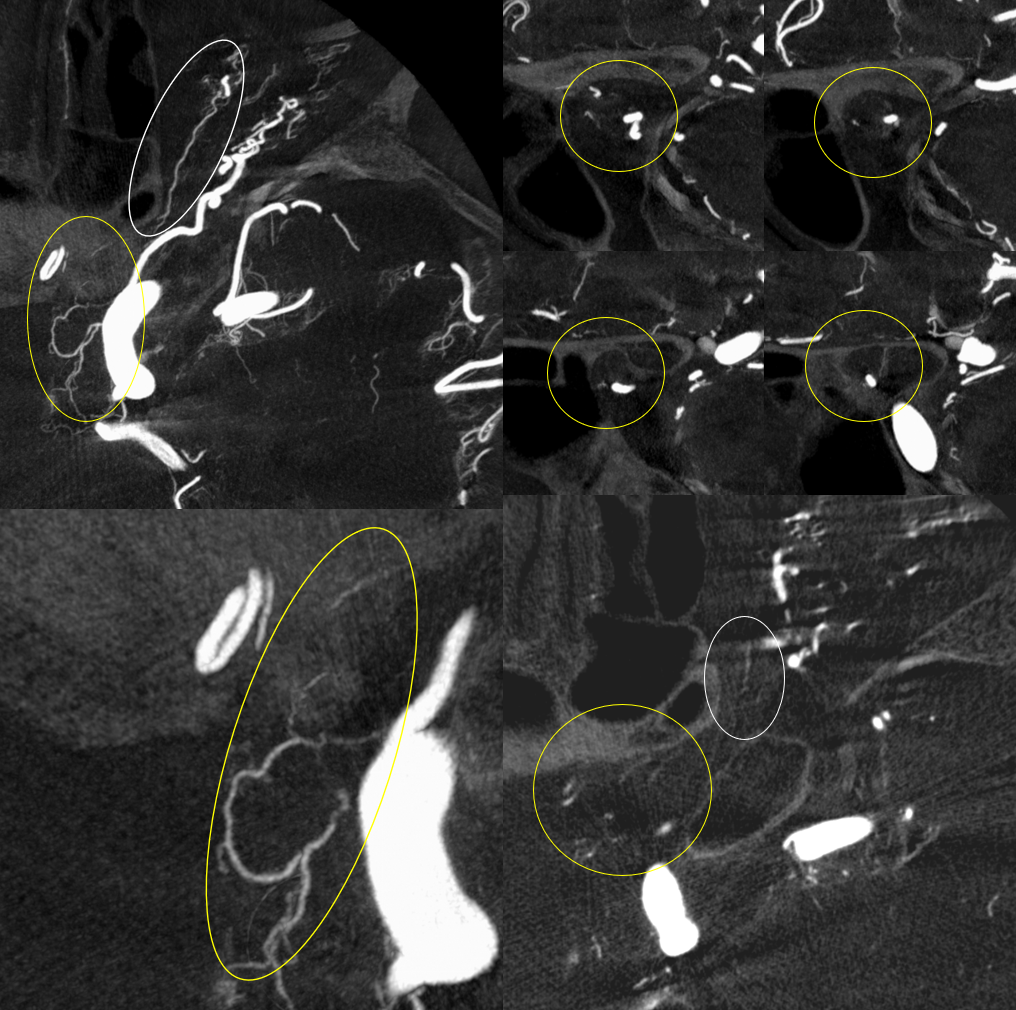
The image below is from an Ophthalmic Artery case page. The superior hypophyseal branches supplying the stalk are dashed white arrows. Inside the oval are vessels related to the optic nerve and chiasm — possibly in part supplied by the superior hypophyseal branches also, but not sure.
Axial source data movie — pause and scroll
Optic Nerve Supply
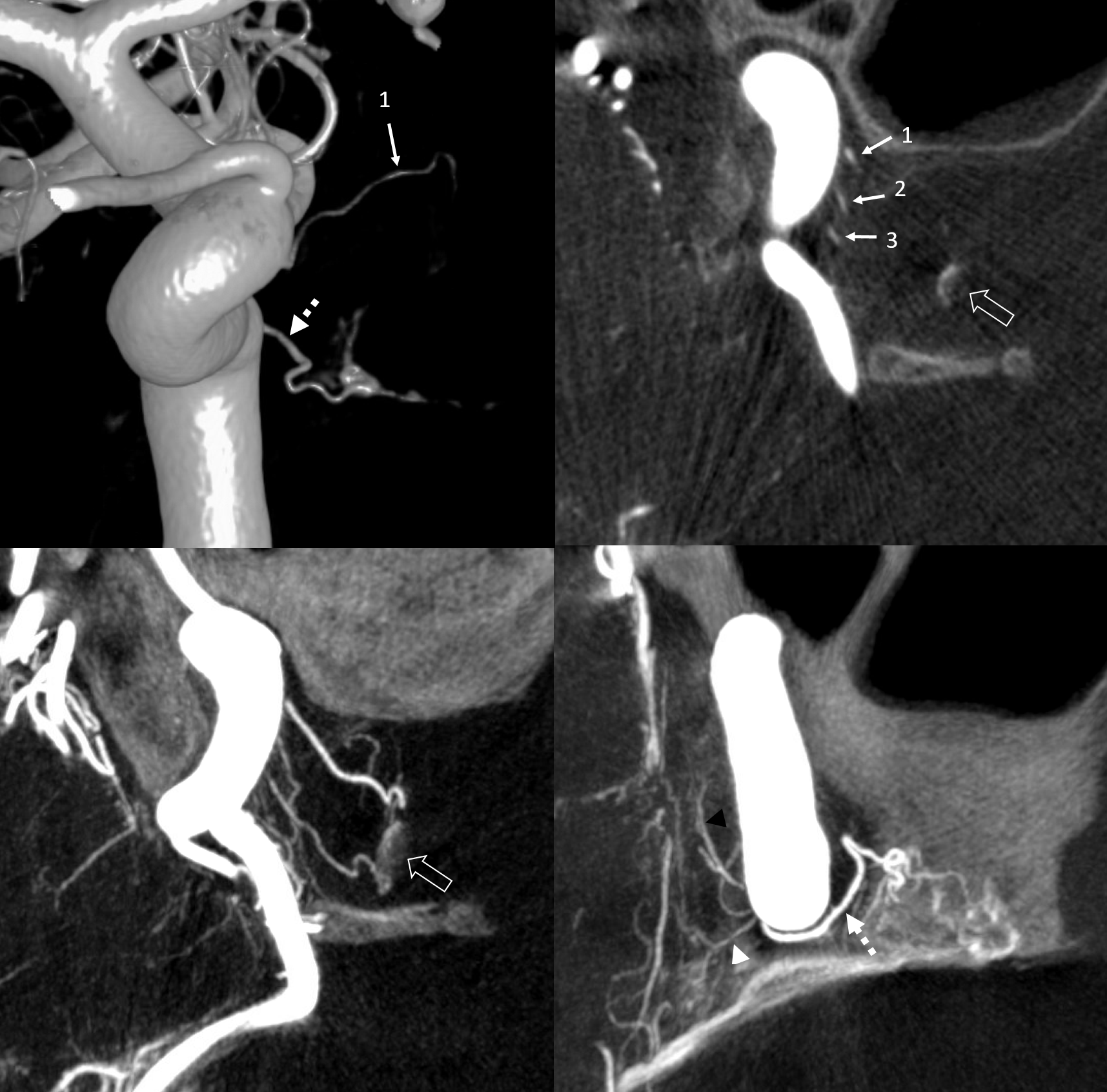
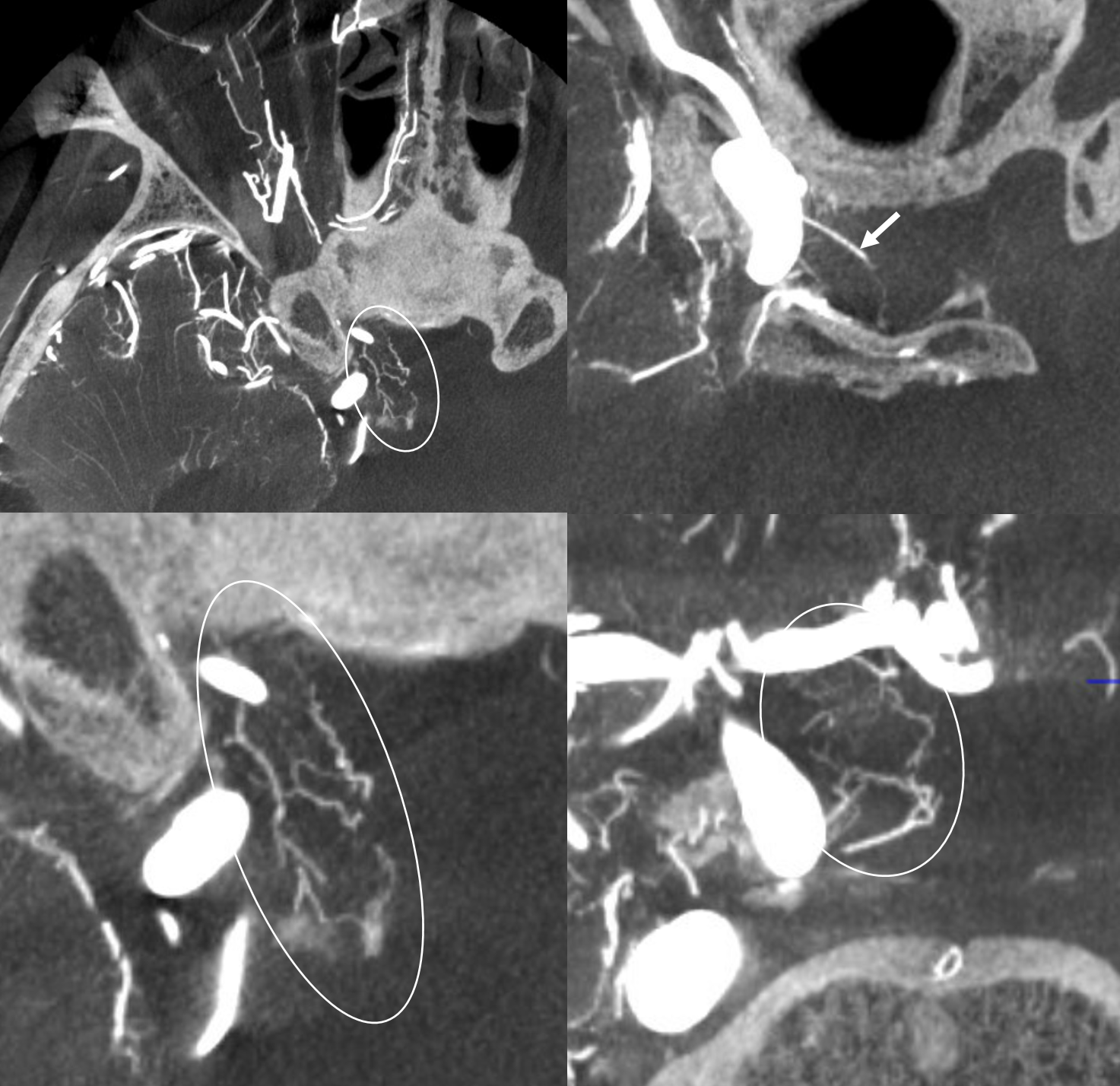
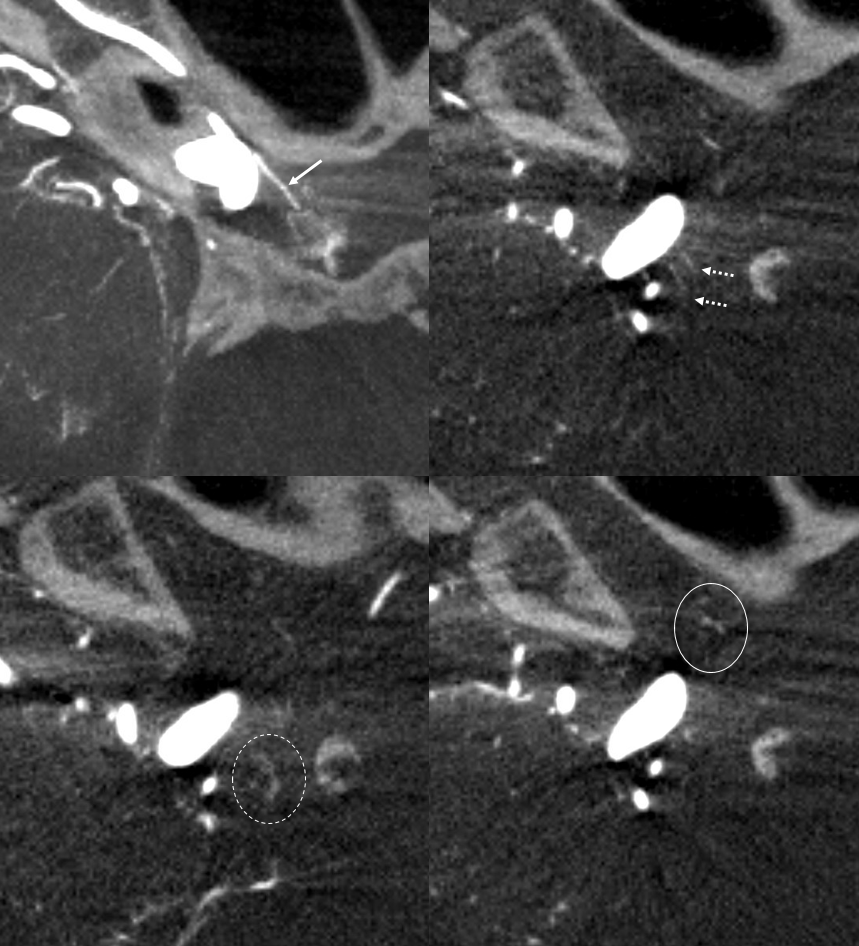
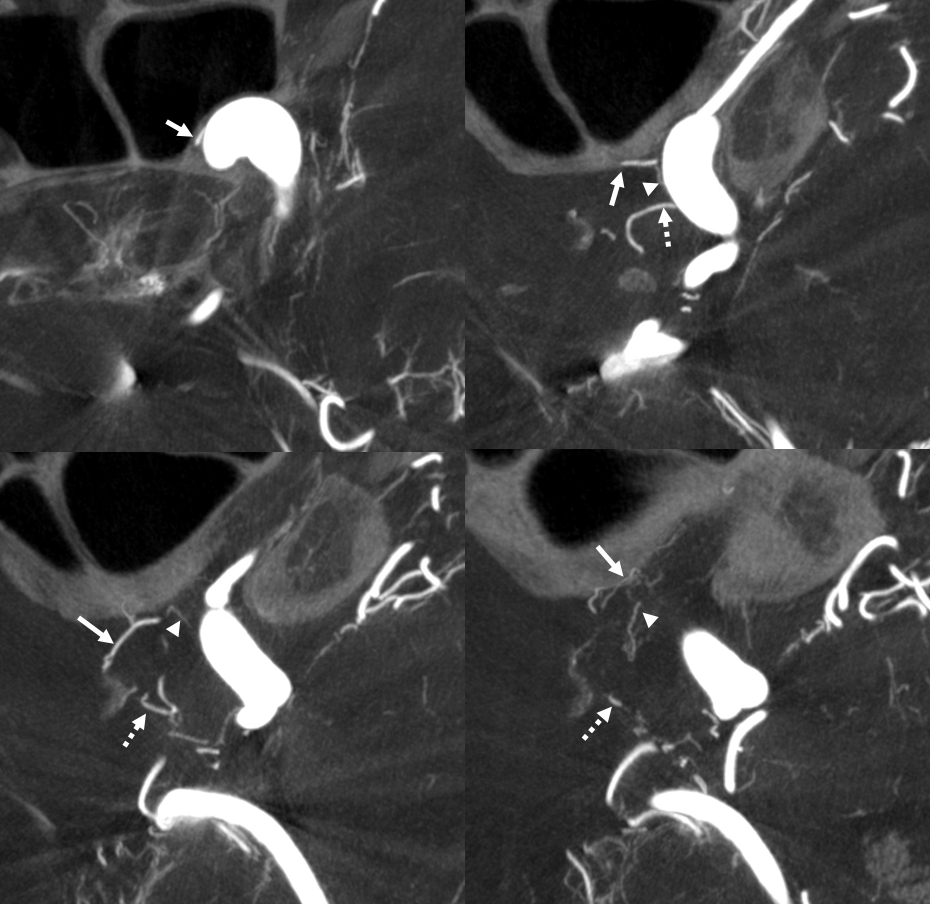
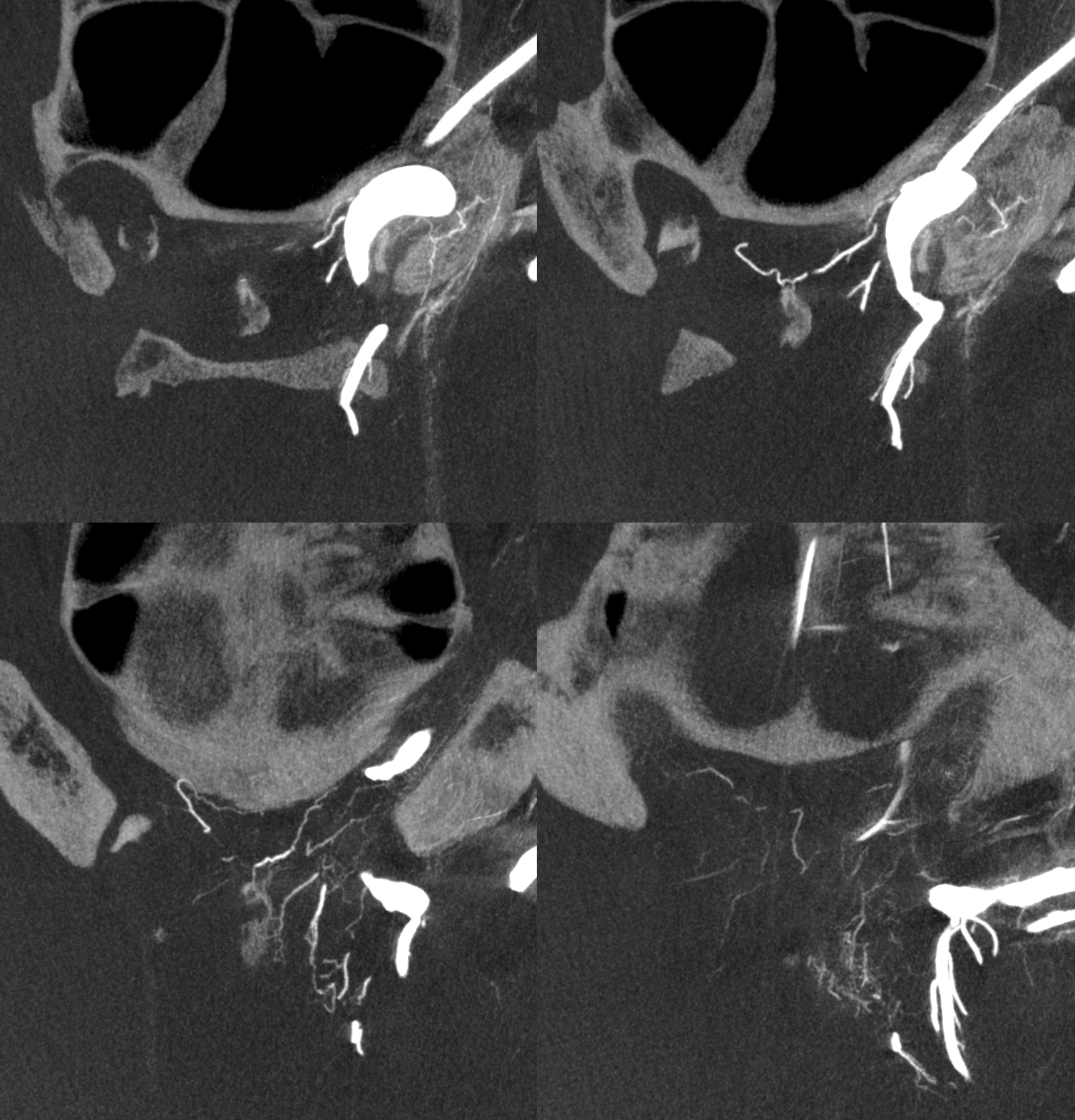
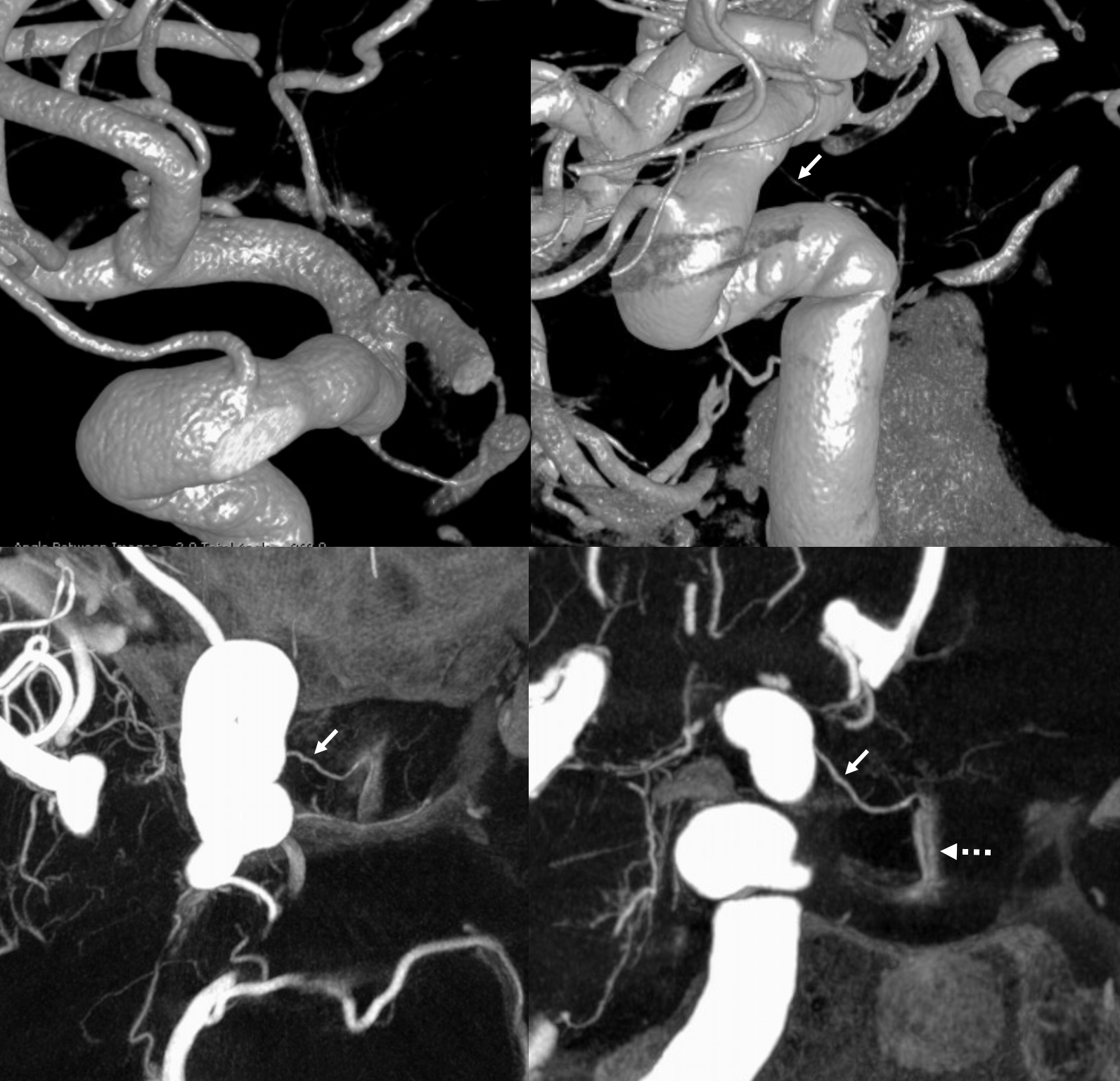
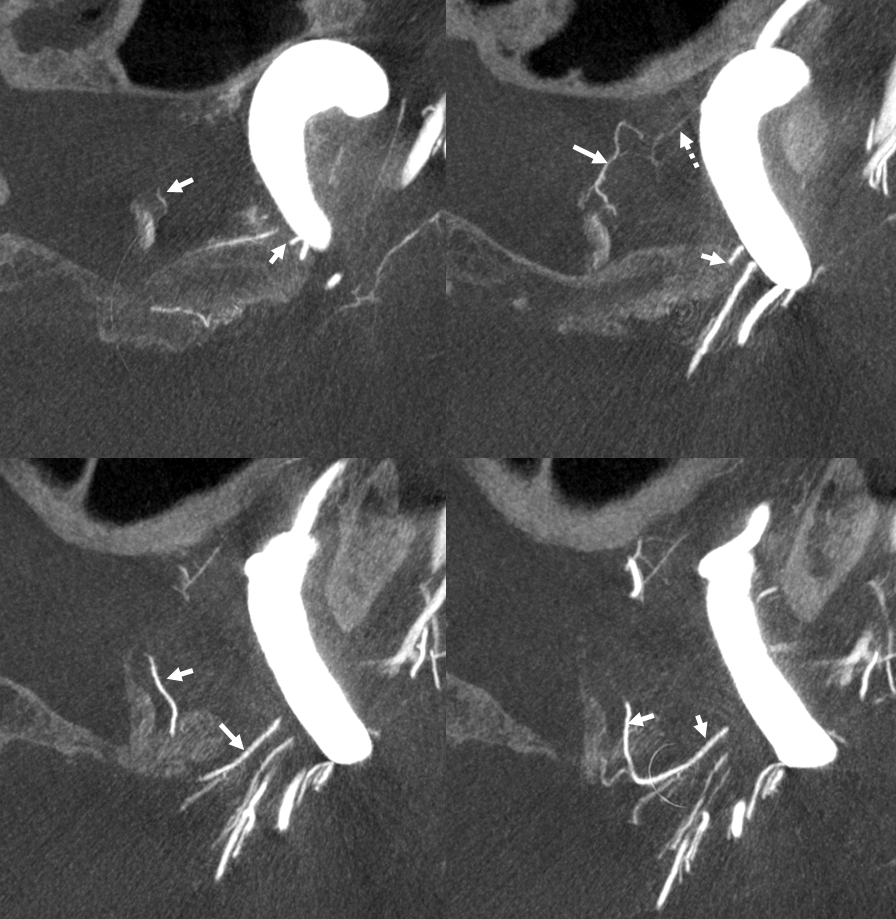
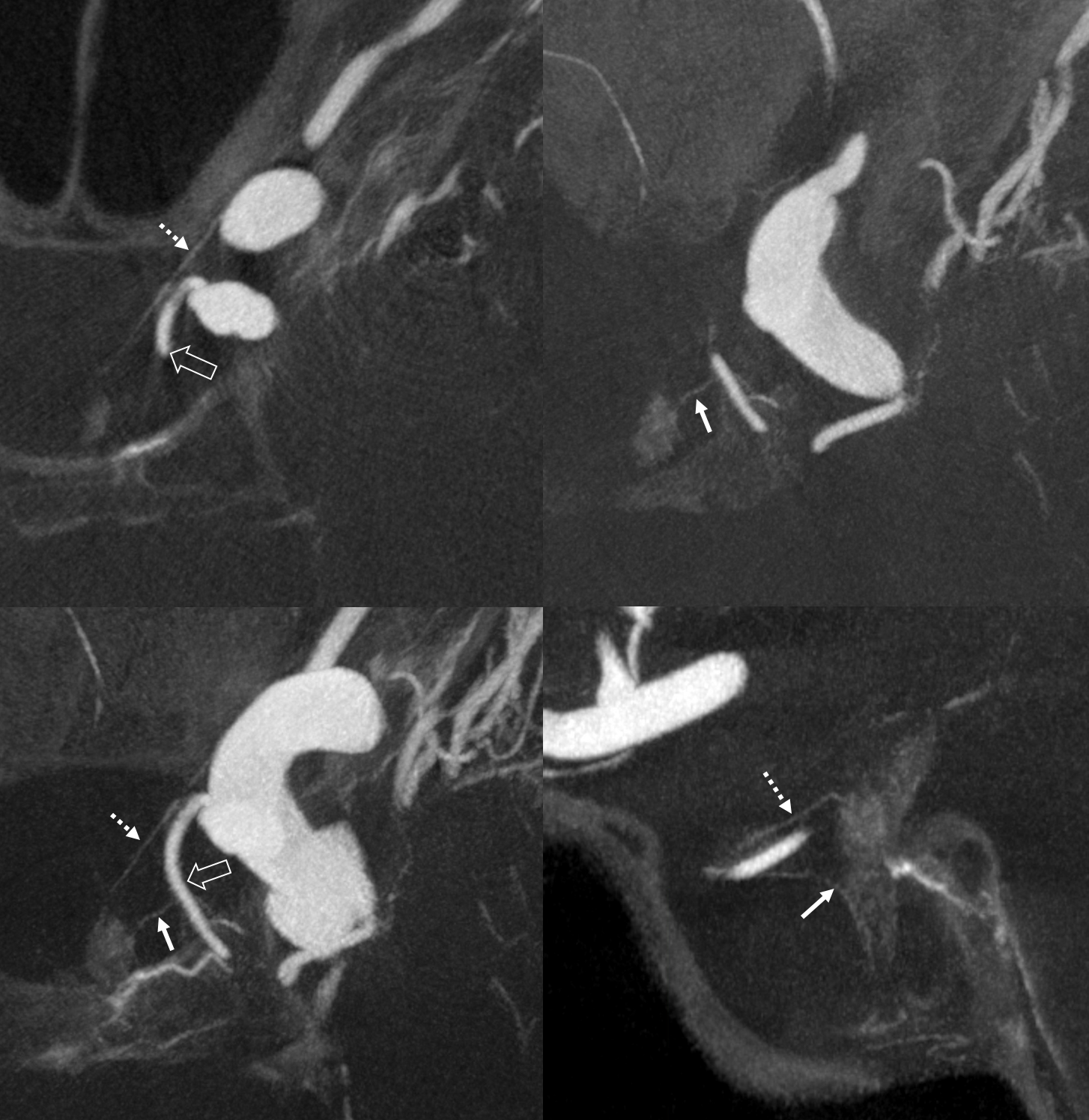
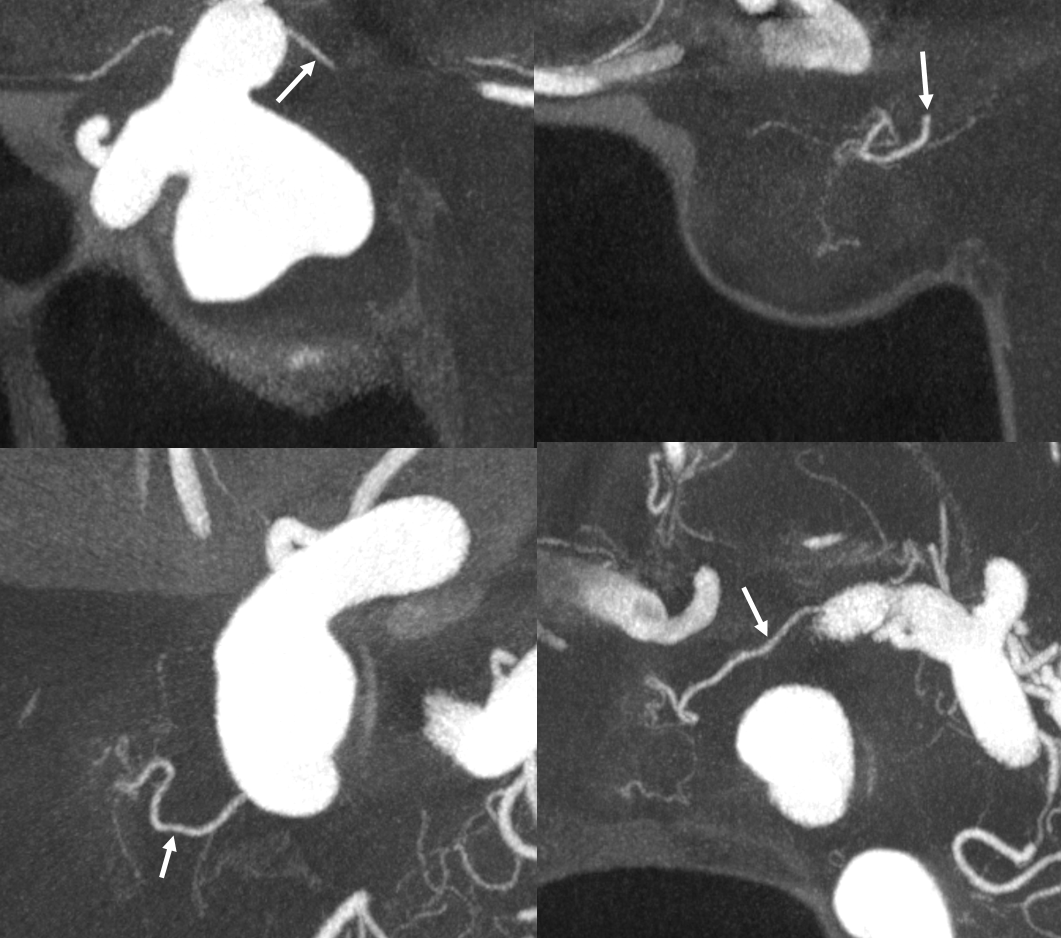
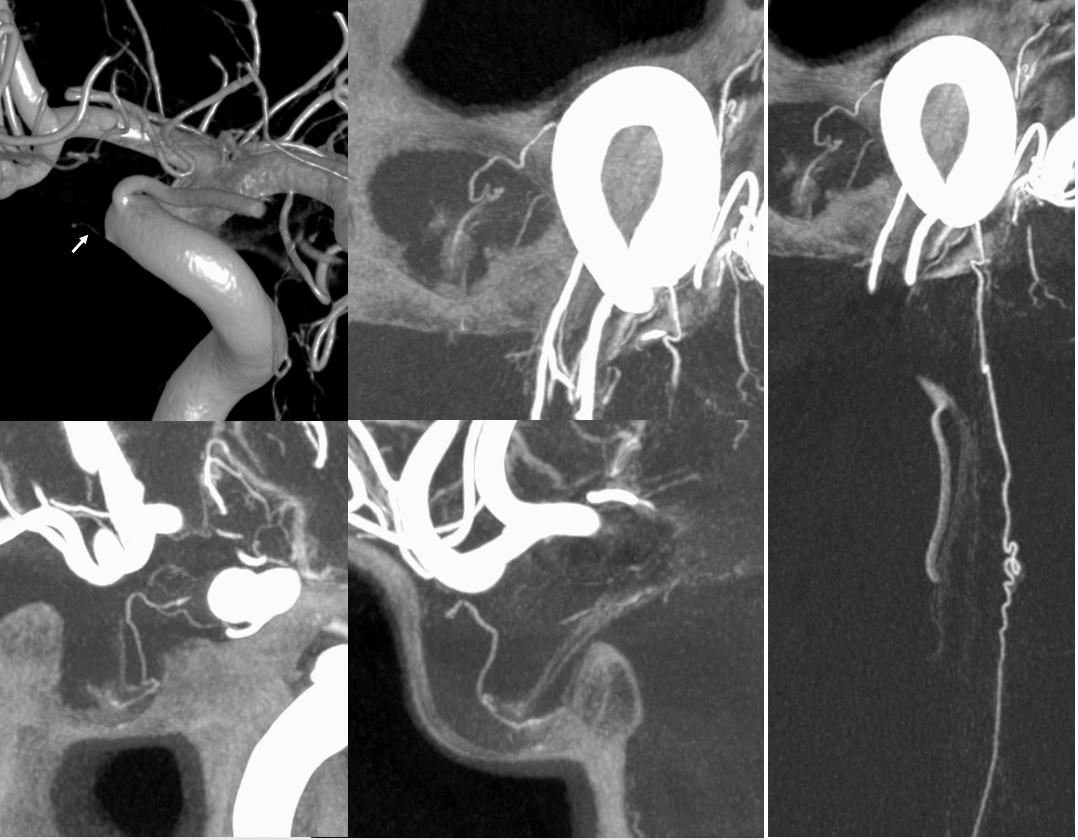
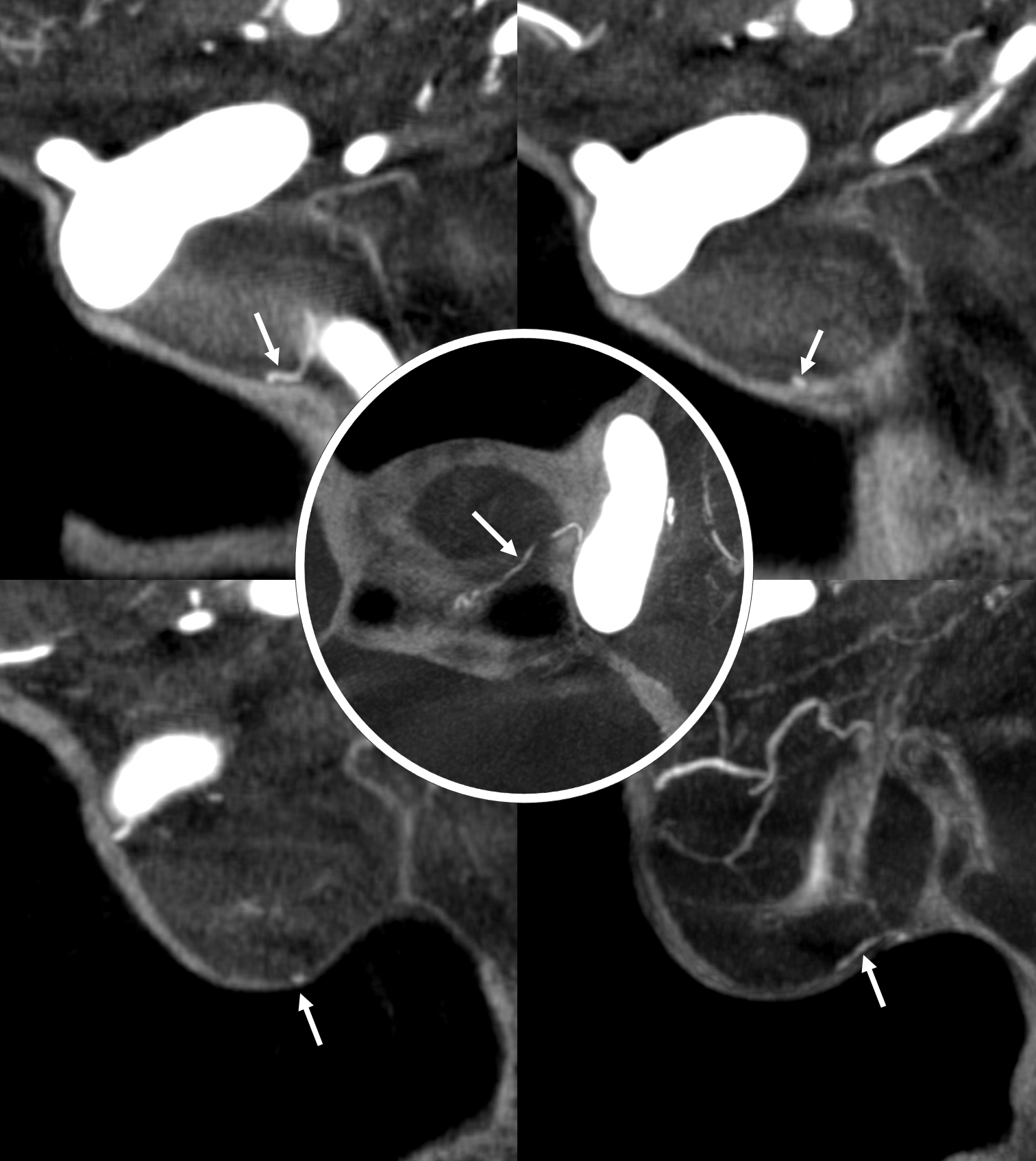
What supplies the bulk of optic nerve? Central Retinal artery is for the distal portion of nerve and retina. What about the rest — intracranial, intracanalicular, proximal intraconal segments? The answer is not clear (let me know if you do), but i believe the bulk of it comes from the superior hypophyseals. It is probably in balance with the recurrent branch of the central retinal artery. Below is an example of an especially prominent proximal-most superior hypophyseal (arrows) supplying the pituitary stalks and optic nerve in the canalicular and intracranial locations. Note how well one can see the branch in coronal view (bottom left image). In this case there are two large superior hypophyseals — the more distal one (dashed arrows) supplies predominantly the pituitary stalk. The inferior hypophyseal artery is marked by arrowhead. Lower right image is coronal.
Movie is the best way
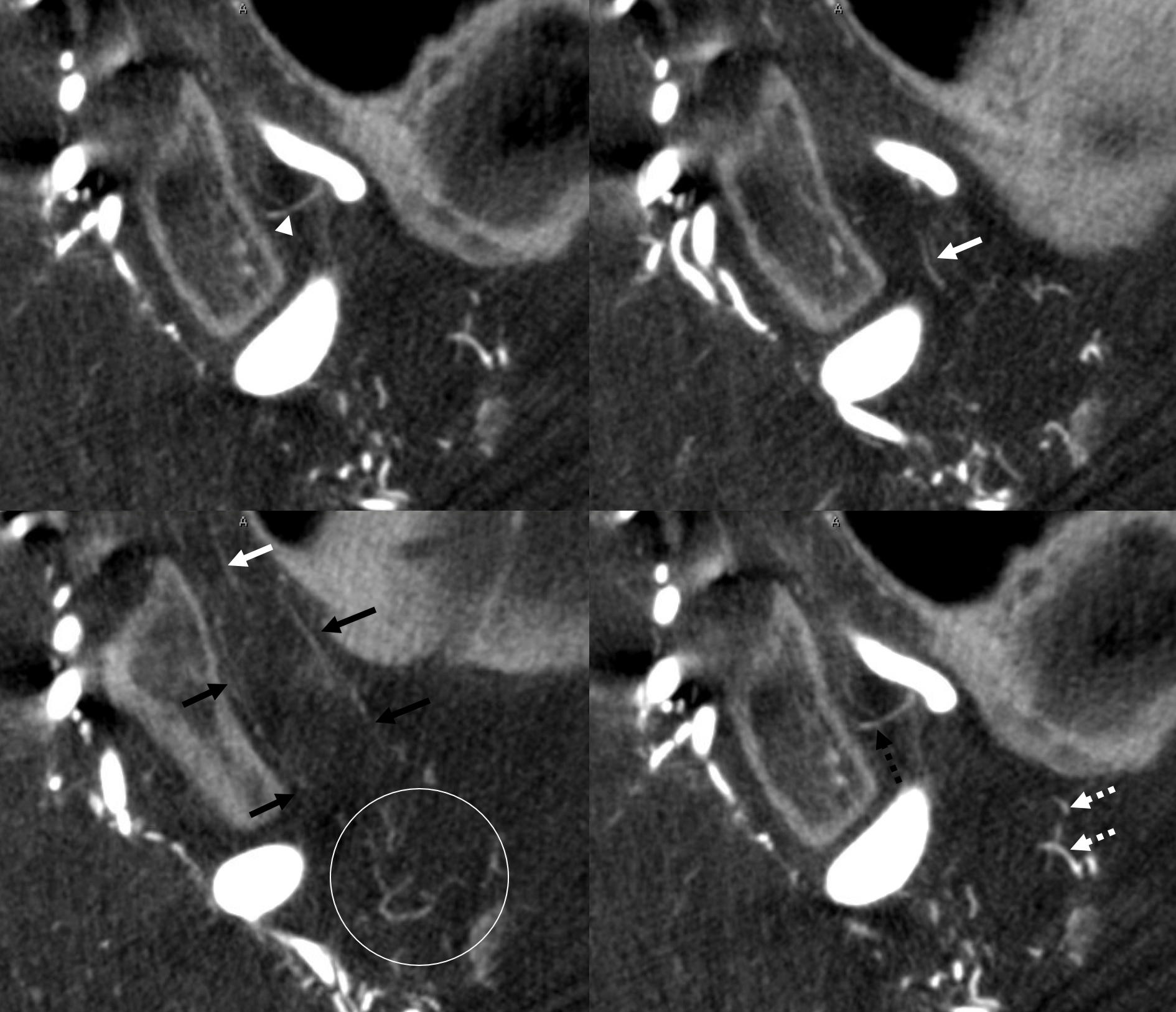
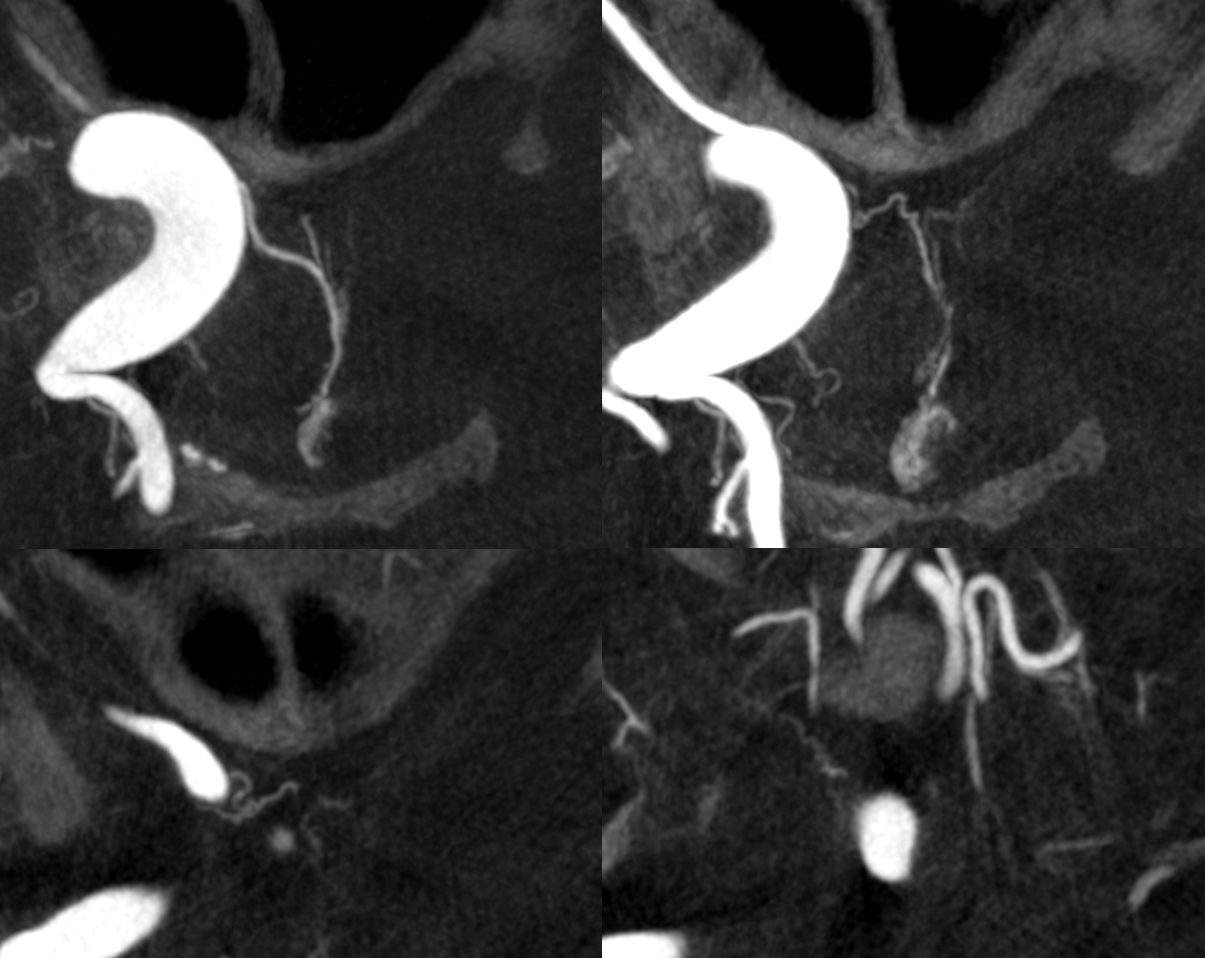
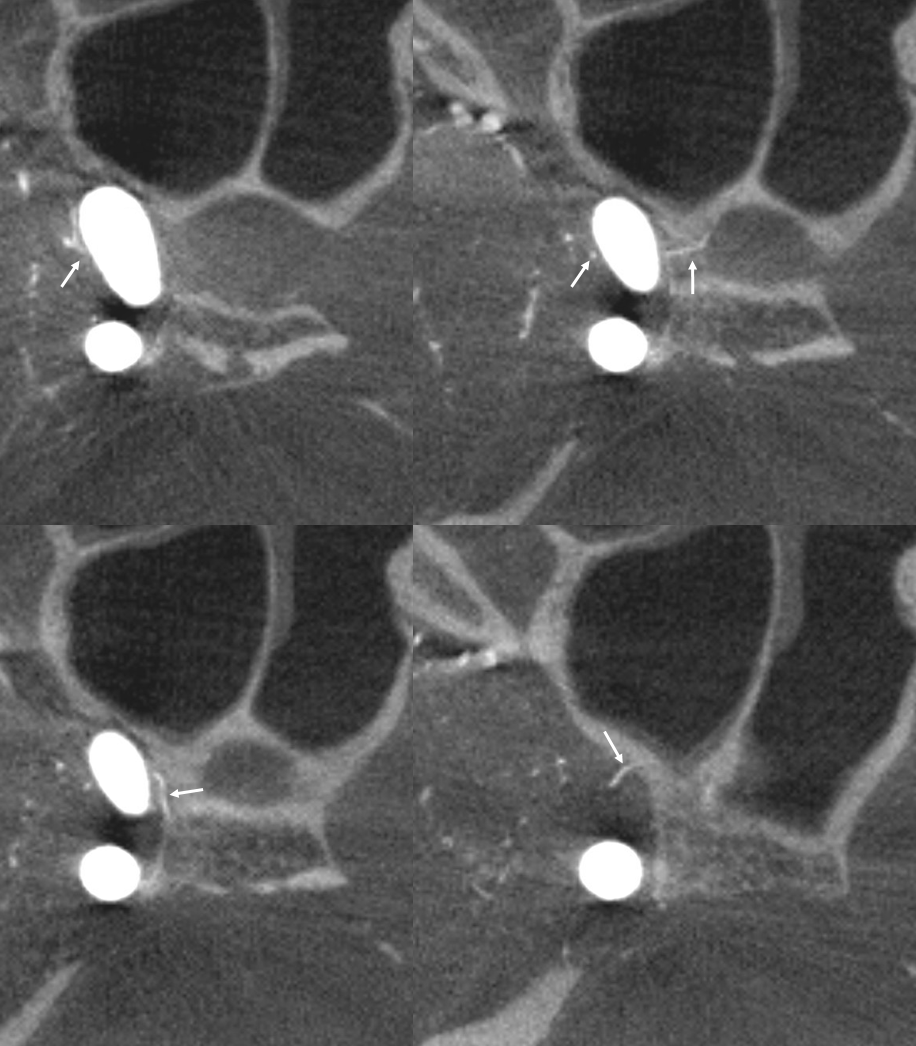
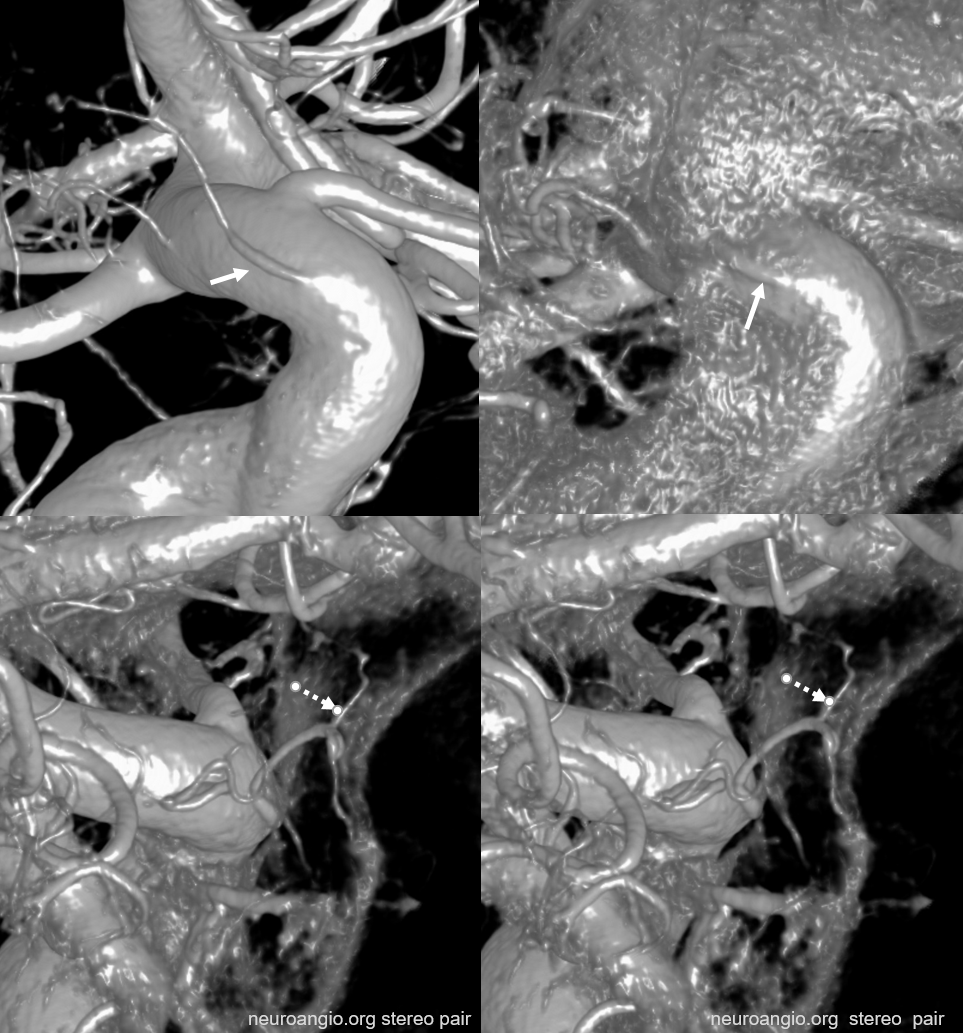
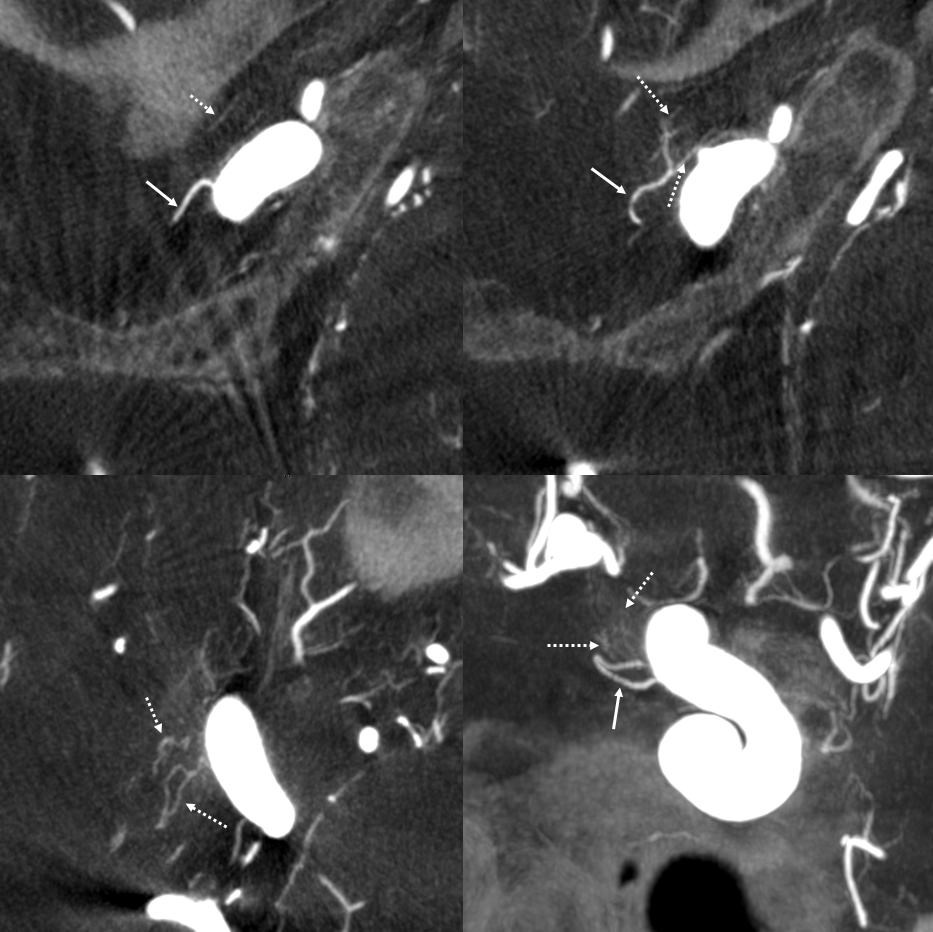
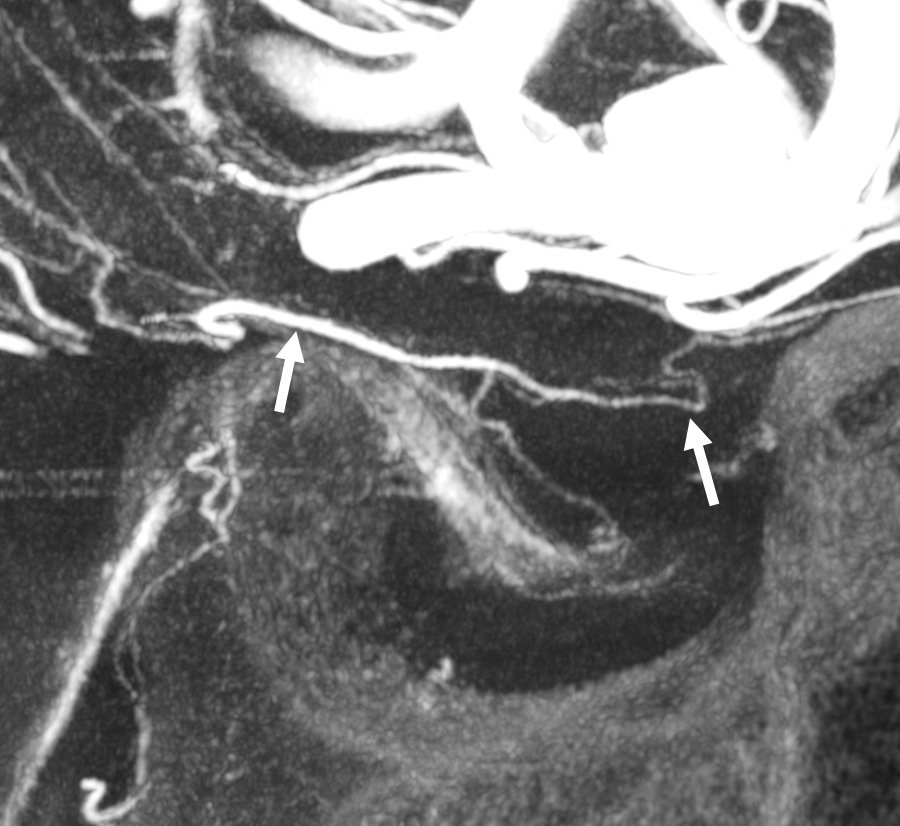
Here too superior hypophyseal (arrow) supply of the intracranial optic nerve (oval) and possibly chiasm is shown definitively (lower right image is coronal)
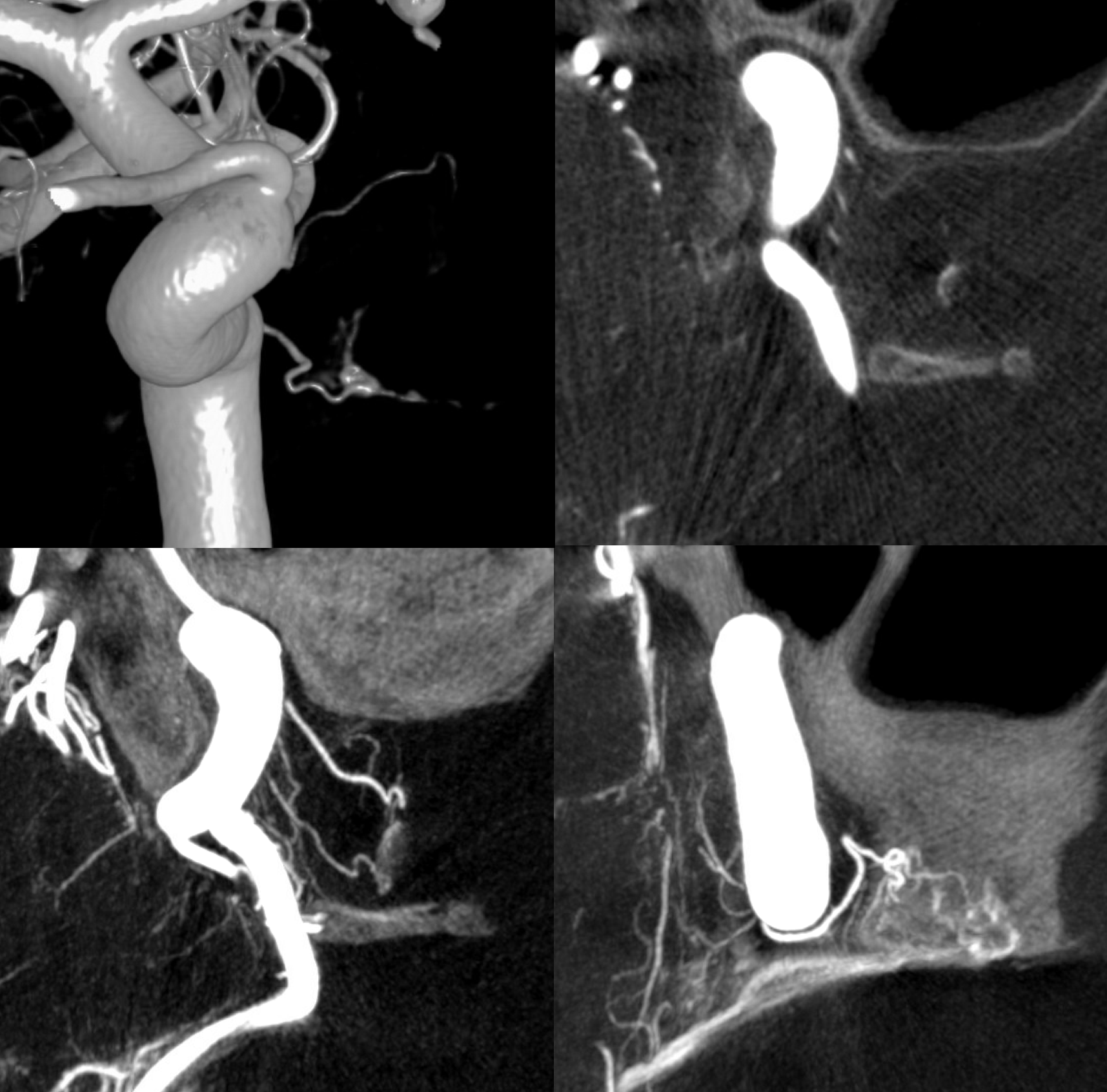
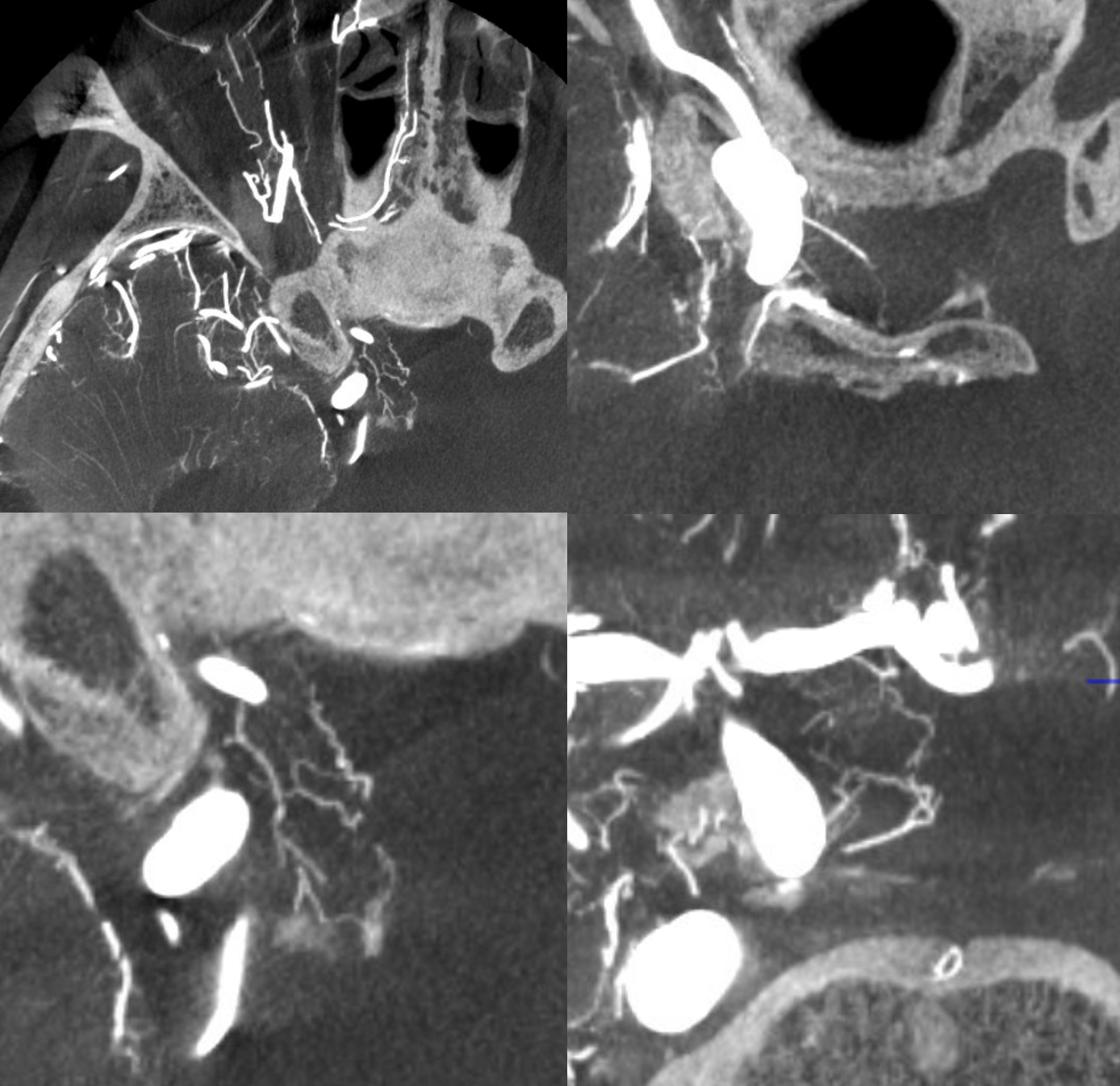
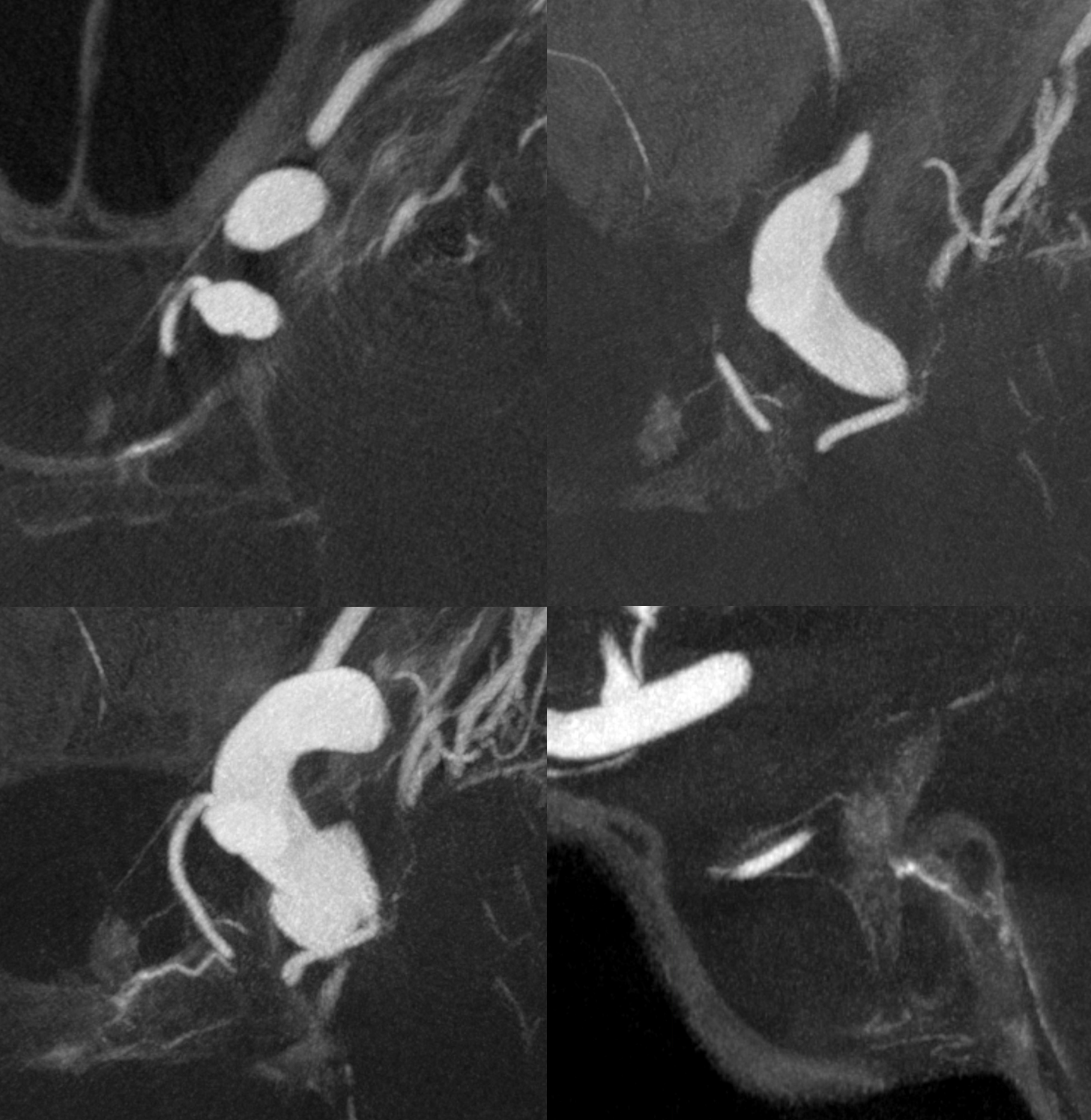
No annotations
Best seen in this movie (pause to scroll)
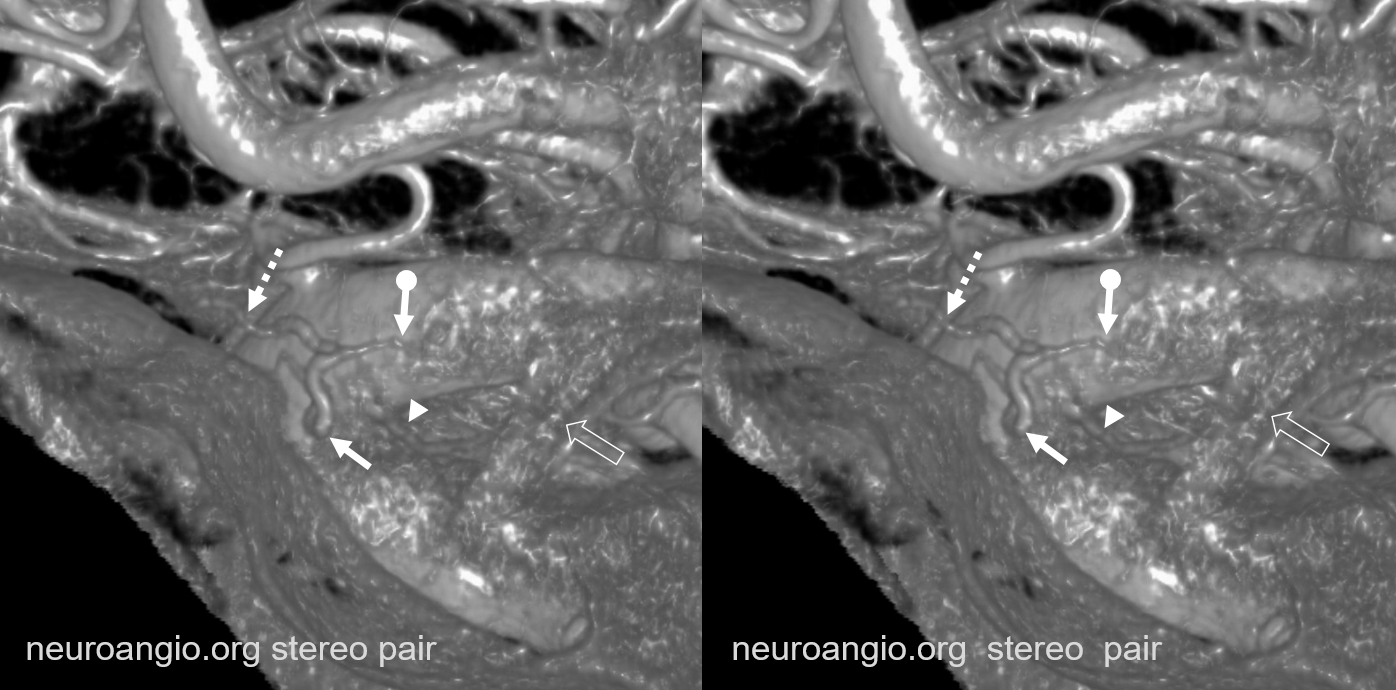
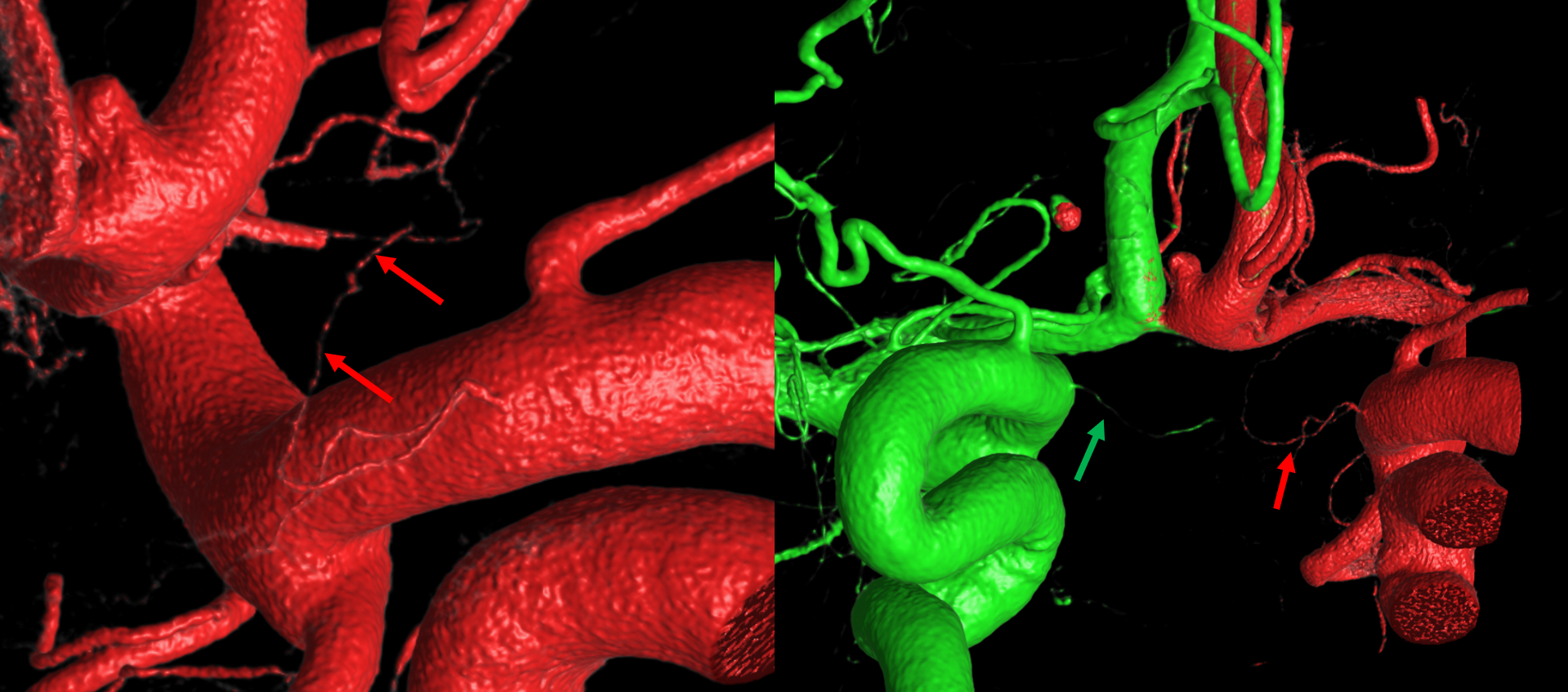
Relationship between Ophthalmic, Superior Hypophyseal Arteries, the hypophysis, and optic nerve supply — all in one — complements Dr. Erez Nossek
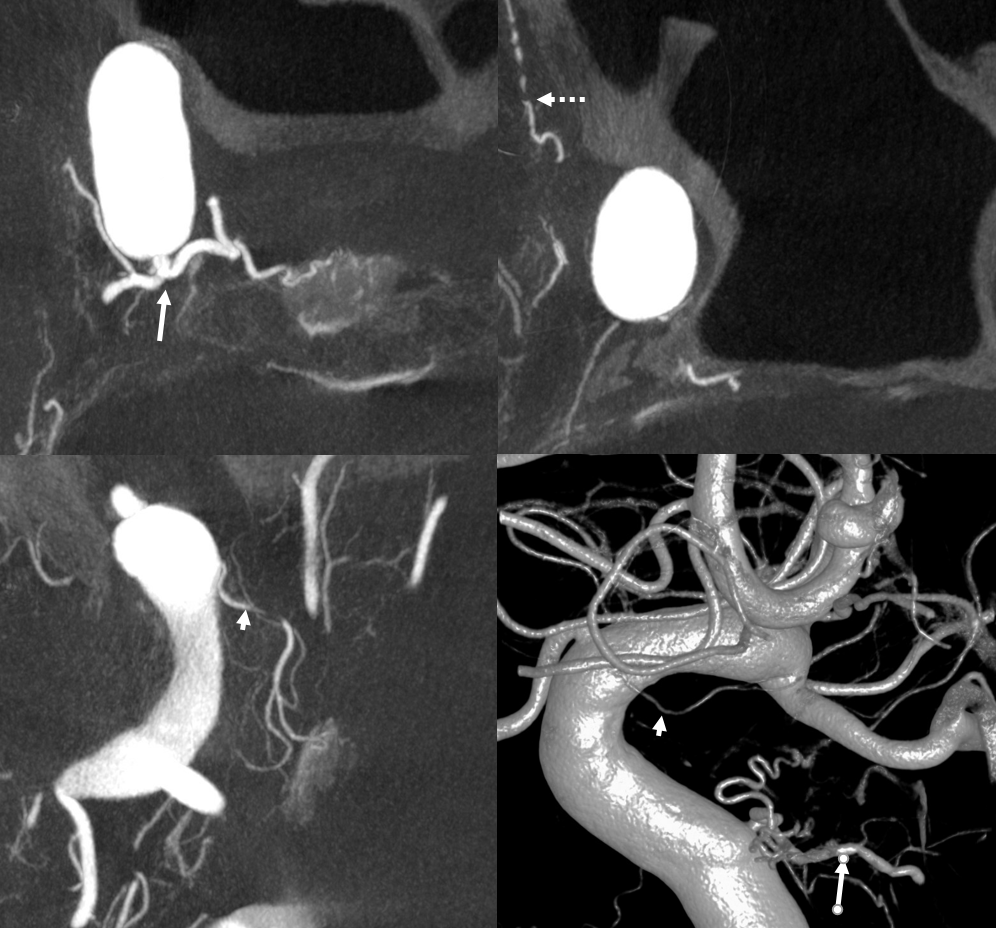
Great connections — the superior hypophyseal artery (dashed arrow) supplies the anterior pituitary, but there is much more. A network of vessels (arrows), at least one of which is connected to the proximal ophthalmic artery and the more distal superior hypophyseal near the midline, supplies both proximal optic nerves. The ophthalmic/ superior hypophyseal connection is discussed from an embryologic perspective below.

No arrows
In sagittal also seen is the artery of the pituitary stalk (arrowhead)
DYNA Movie
Pattern of optic apparatus supply and unusual hypophyseal ILT vessel
VR — the anterior-most branch of the superior hypophyseals is usually the largest (arrow). The others are too small to see on a VR image

MIPS. The anterior, proximal-most branch (arrow) tends to supply the optic nerve (white oval), while the more posterior branches (dashed arrows), when present, supply more posterior structures such as chiasm and tract (dashed oval)
A highly unusual branch originating from ILT region swings underneath the cavernous ICA and supplies the floor of the pituitary fossa. Yet unknown, as far as i know
More Optic Nerve Supply — its easier to see on MIPS, but with the right windowing, and stereo, VR imaging is also possible. Here, there are 3 superior hypophyseals seen. The anterior-most (arrow) is usually the largest, suppling the optic nerve (dashed arrow) and chiasm (ball arrow). The middle and posterior hypophyseals (arrowheads) supply the stalk.

Stereo of VR image. Same arrows. The stalk is open arrow.
Another patient — also 3 arteries. Cave origin of the anterior-most (arrows) one. The middle one (arrowheads) also supplies the optic nerve. The posterior one (dashed arrows) is for the stalk.
VR images (stereo pair on bottom). The cave origin of the anterior branch is most beautifully seen in the upper right image.
Here is one more — extensive participation by the left SHA (yellow ovals) and recurrent branch from intraconal ophthalmic (white ovals).

Note lack of any supply to optic apparatus from A1 or ACOM — there never is
Pathology — Optic Apparatus supply in setting of atheromatous disease
Here there is severe supraclinoid stenosis. Whether because of disease on the other side or other issues, there is extensive takeover of the bilateral optic apparatus by various branches of the left superior hypophyseal arteries. Stereo images shows two main superior hypophyseal artery branches — thats pretty big for the hypophyseals
Bilateral optic apparatus supply (left and right proximal optic nerves, chiasm, proximal left tract) are inside the ovals

Without ovals
Moya-Moya — Similar Process of RIGHT Superior Hypophyseal Reconstitution of the ACA territory, while on left the ophthalmic, via ethmoidal piodural anastomoses, reconstitutes the olfactory branch of the ACA. Full case here
Even more info can be gleaned from MIP images — Whereby on the LEFT, small branches from the proximal ophthalmic — superior hypophyseal equivalents — highlighting the homology between the two — are also present, supporting the optic apparatus and frontal base
“Carotid Fenestration” — hypophyseal to PCOM connection
Super case by Dr. Eytan Raz

see that small branch to the anterior hypophysis?

ANOTHER EXAMPLE — Superior-Hypophyseal-PCOM Anastomosis
Lest you think these are super rare — well, probably its one in every 200 or so cases. We have seen 2 and did over 400 DYNAs of the area
This really begs the question of what is the embryologic relationship between the two — and how does that fit into the cranial/caudal ramus theory
MIP — superior hypophyseal – arrow; PCOM — dashed arrow; Anterior Choroidal — open arrow
Stereo VR

Axial MIPs. Same arrows. The anastomotic superior hypophyseal is the more distal one. There is another, more proximal superior hypophyseal (ball arrow) supplying the stalk
Relationship with Ophthalmic Artery
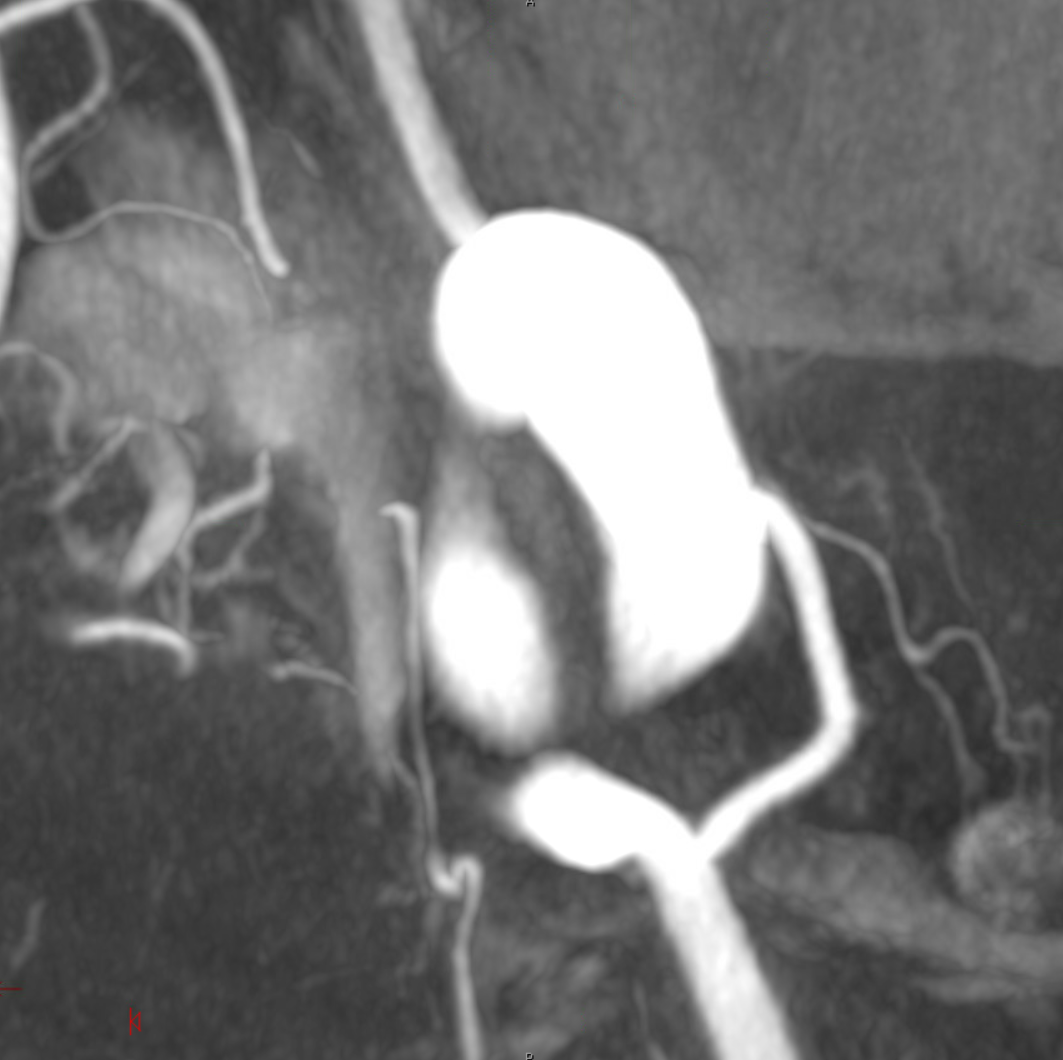
Another interesting topic. Courtesy Eytan Raz MD PhD. Hypophyseal Aneurysm, post PED
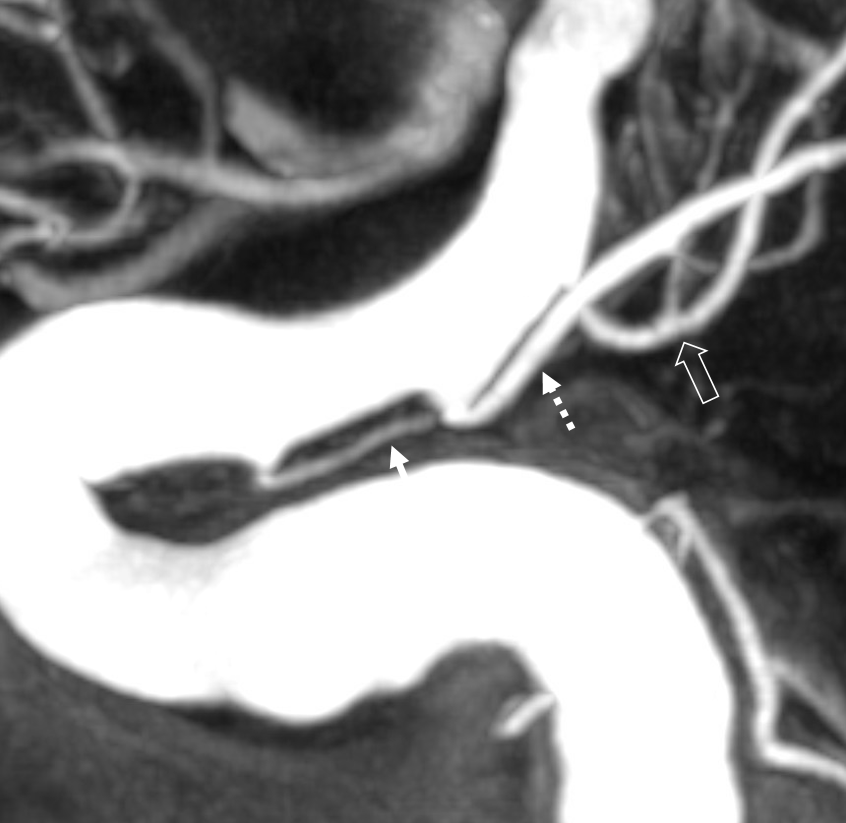
Follow up — notice a “lower” origin of the ophthalmic now, and a small vessel (arrow) from the medial wall, adjacent to the new ophthalmic ostium.
What happened to the ophthalmic origin? See Pipeline Device Properties page for more into. Basically, the Pipeline is not fully apposed to the ophthalmic ostium, creating a secondary communication between the aneurysm and the ophthalmic — essentially incorporating the ophthalmic ostium into the aneurysm. As the aneurysm shrinks, the flow to ophthalmic is reorganized. Other examples are on the Pipeline page.
Fine. But what about the little branch — the superior hypophyseal artery?
Whats interesting is that the superior hypophyseal was part of the aneurysm. Now that the aneurysm has shunk its ostium has come to appose the Pipeline, and its flow is preserved. Other interesting things are there too.
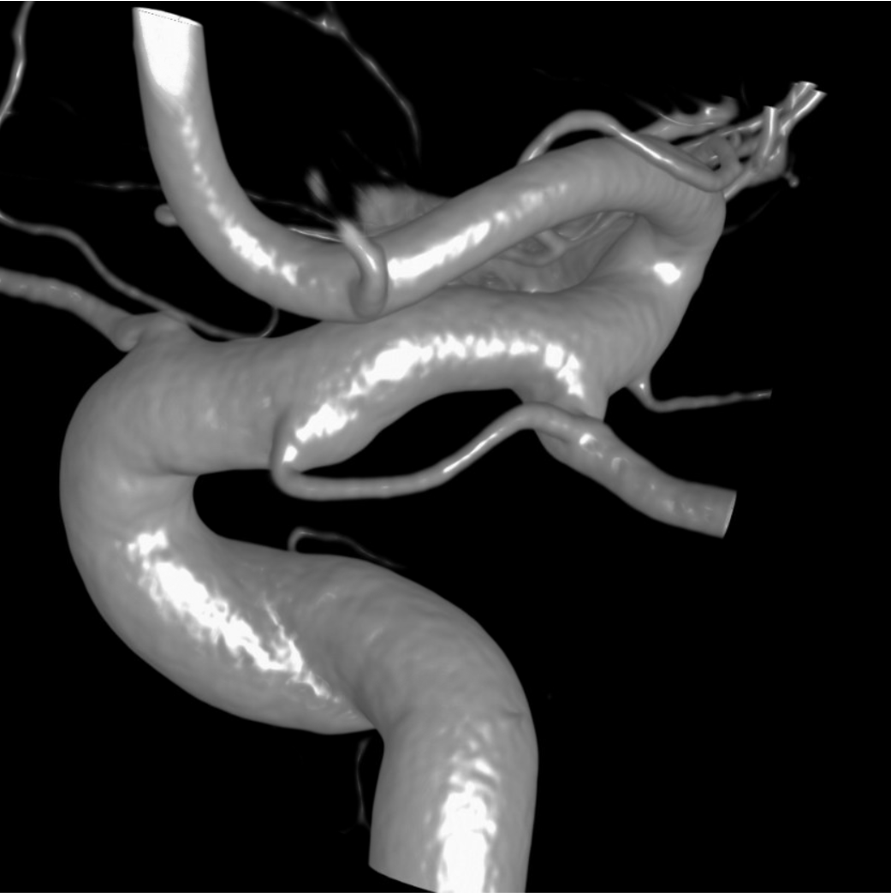
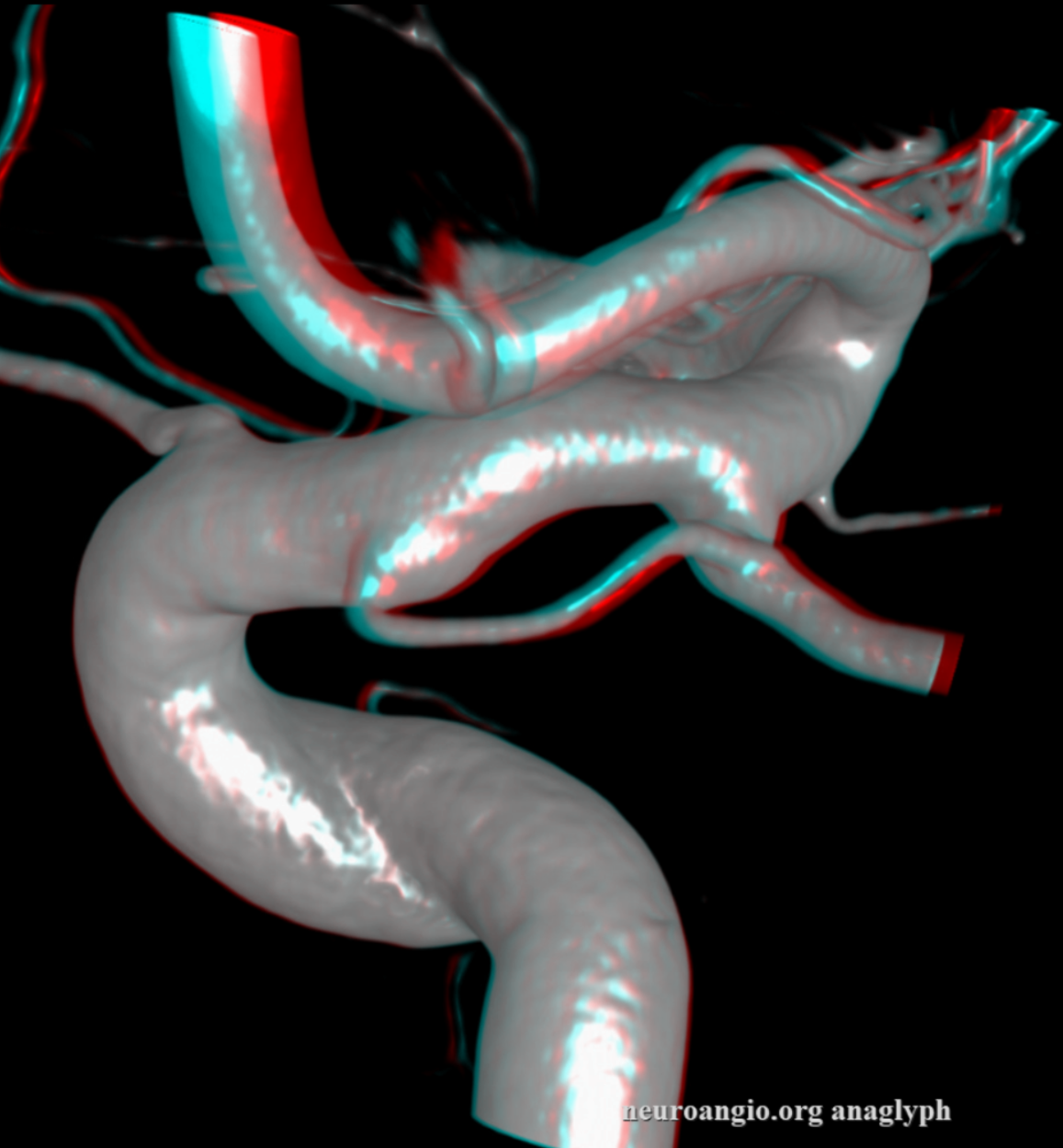
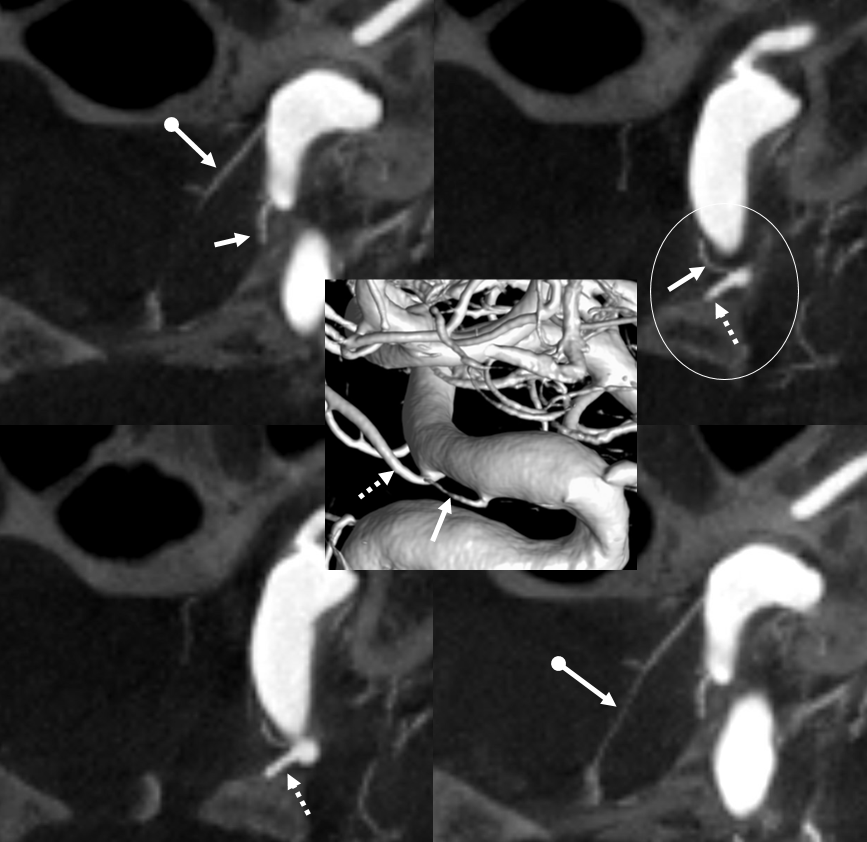
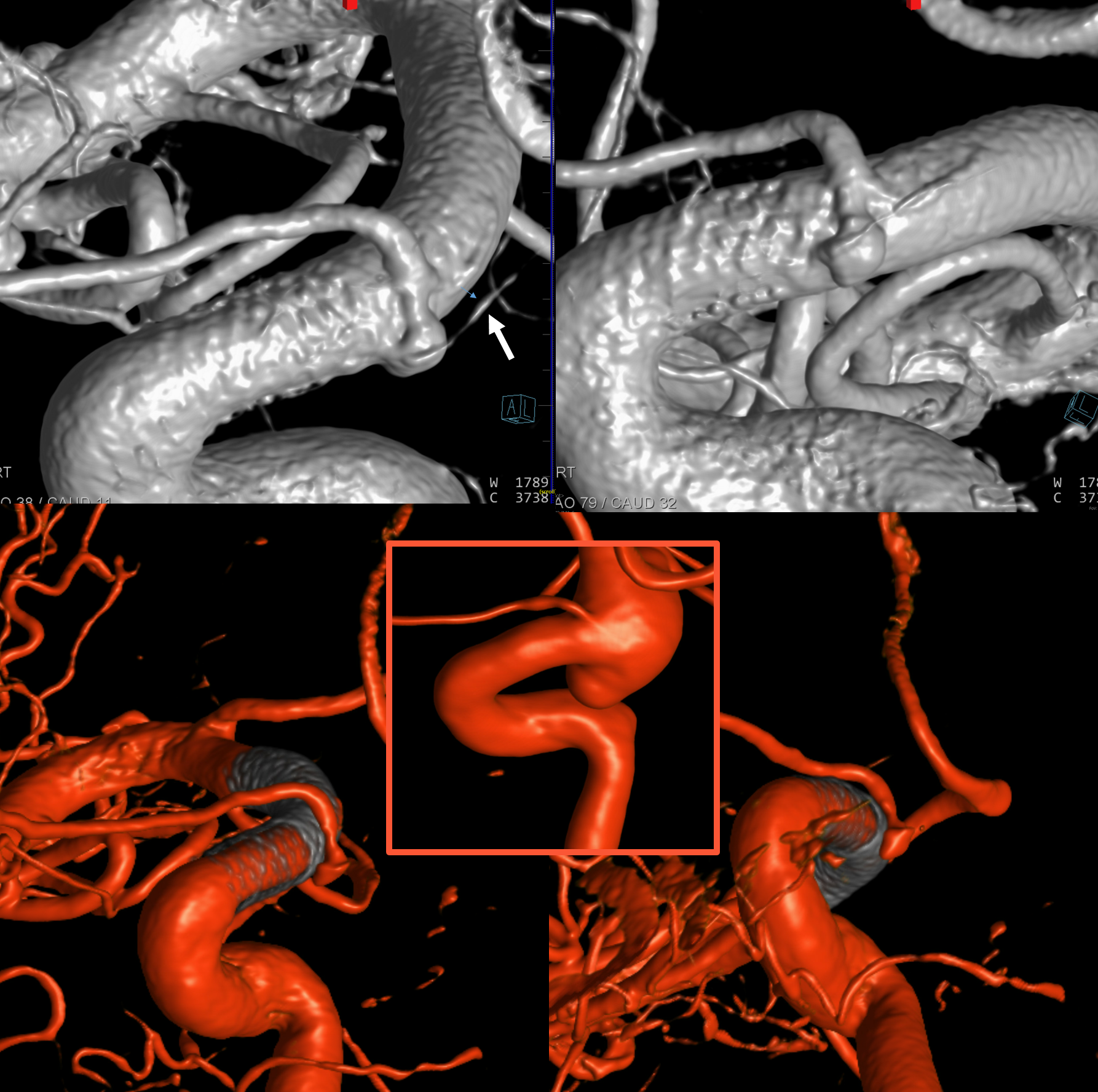
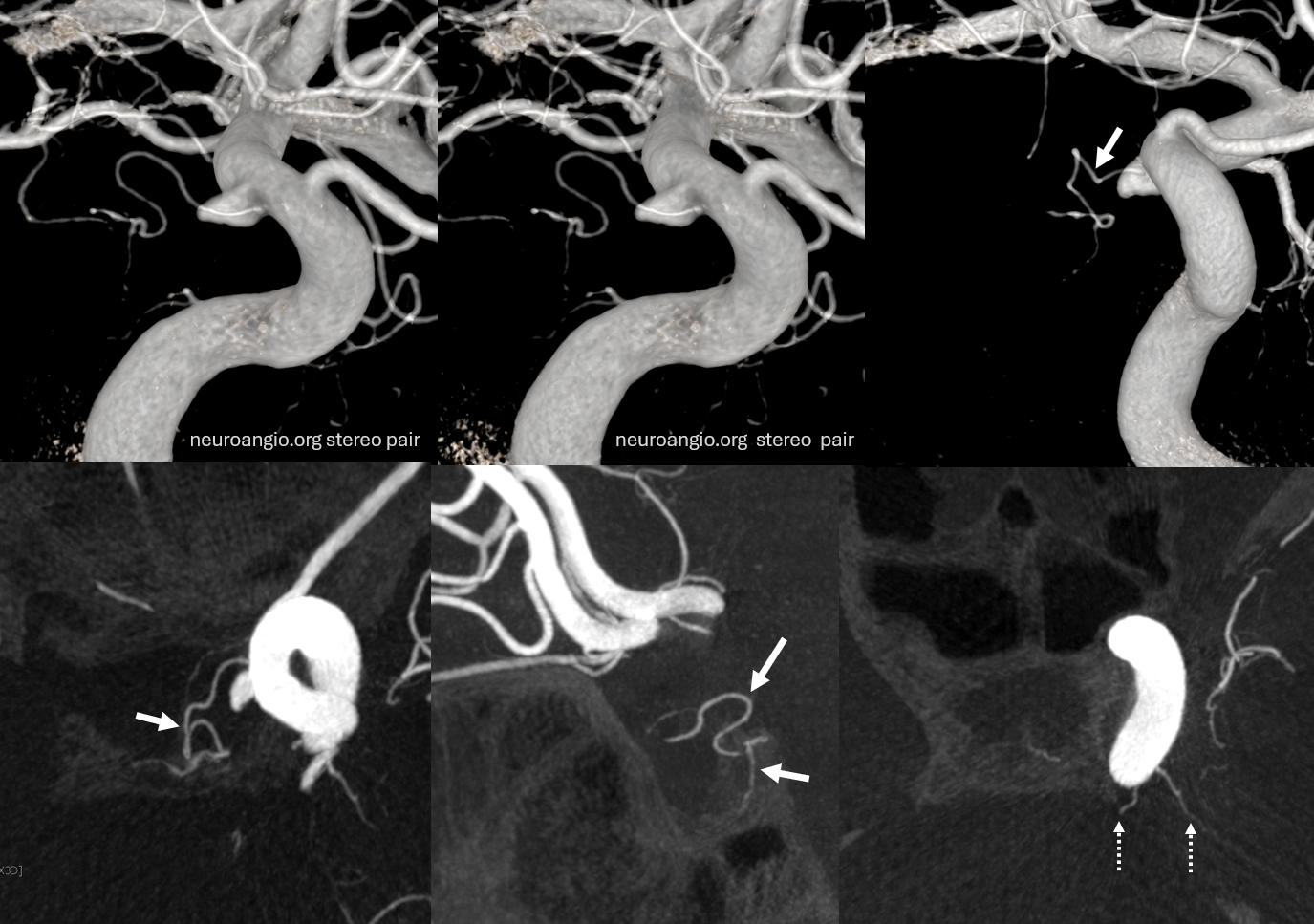
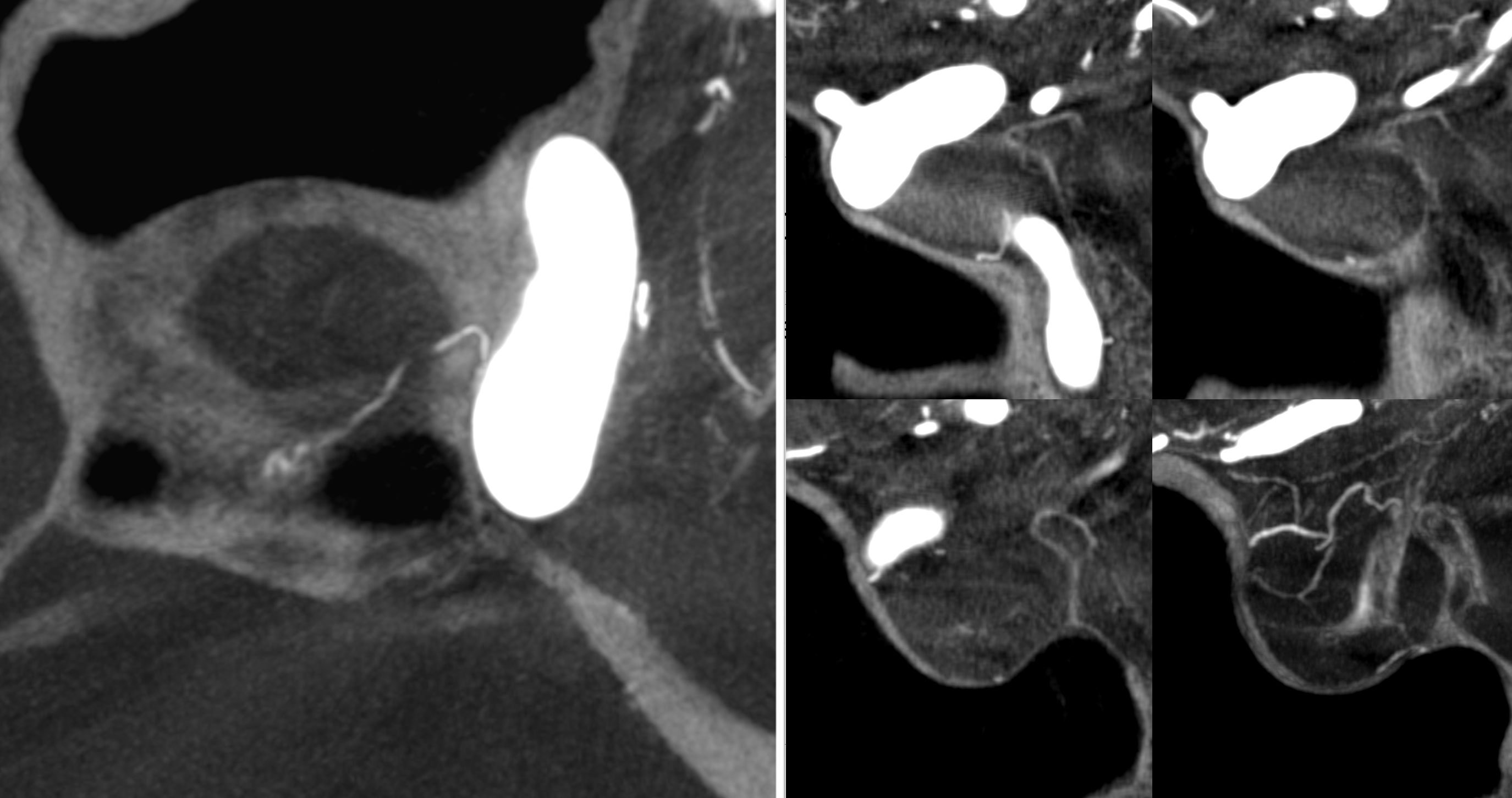
Power of Cone Beam CT imaging
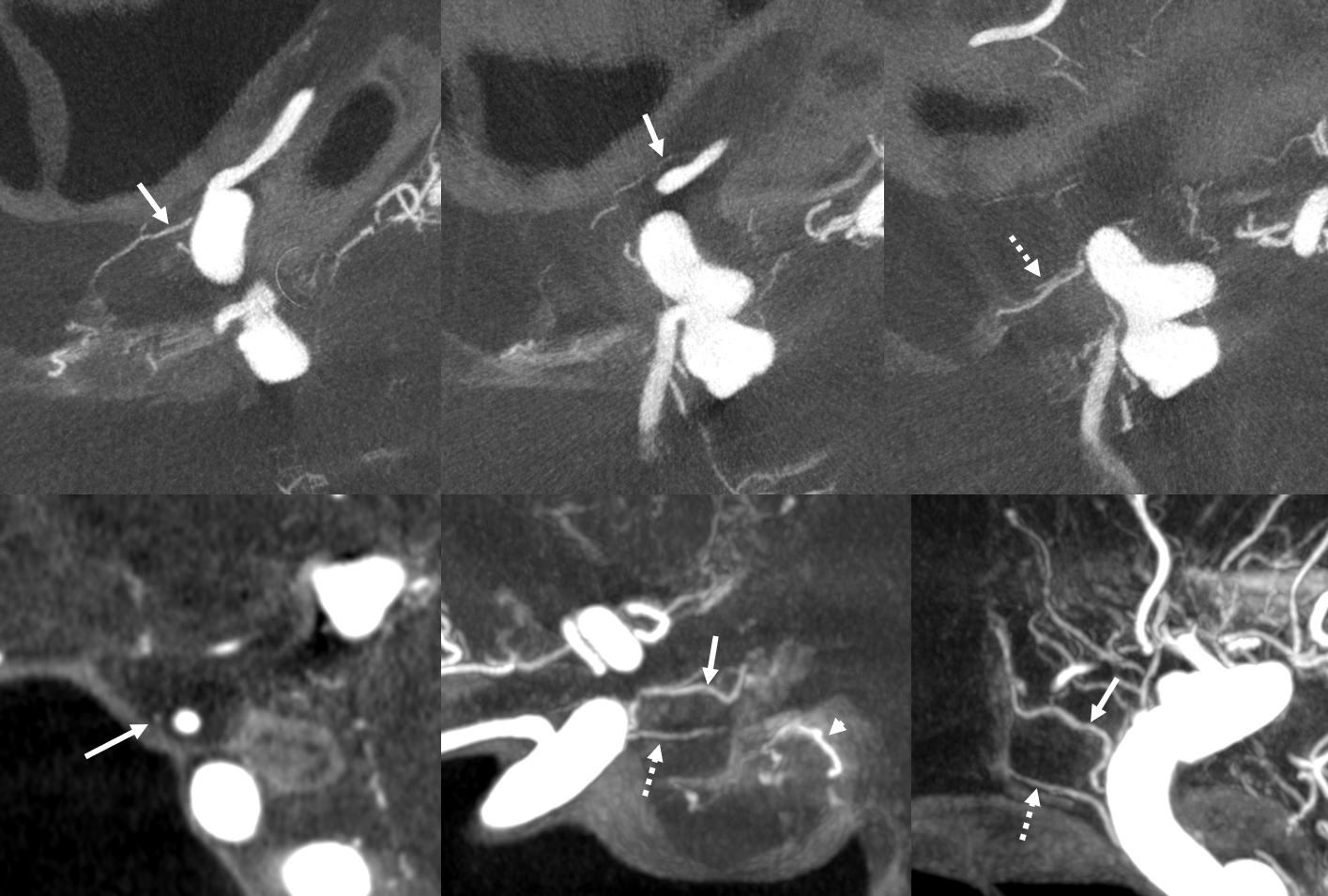
Even the smallest superior hypophyseal arteries can be seen with advanced cone beam CT. Top left is an already high resolution cone beam CT volume rendered image with no apparent Superior Hypophyseal. Windowing to increase sensitivity allows for visualization of a tiny superior hypophyseal (arrow) — top right image. Bottom row are axial (left) and coronal (right) MIP images, showing the same artery, as well as beautifully seen pituitary stalk (dashed arrow)
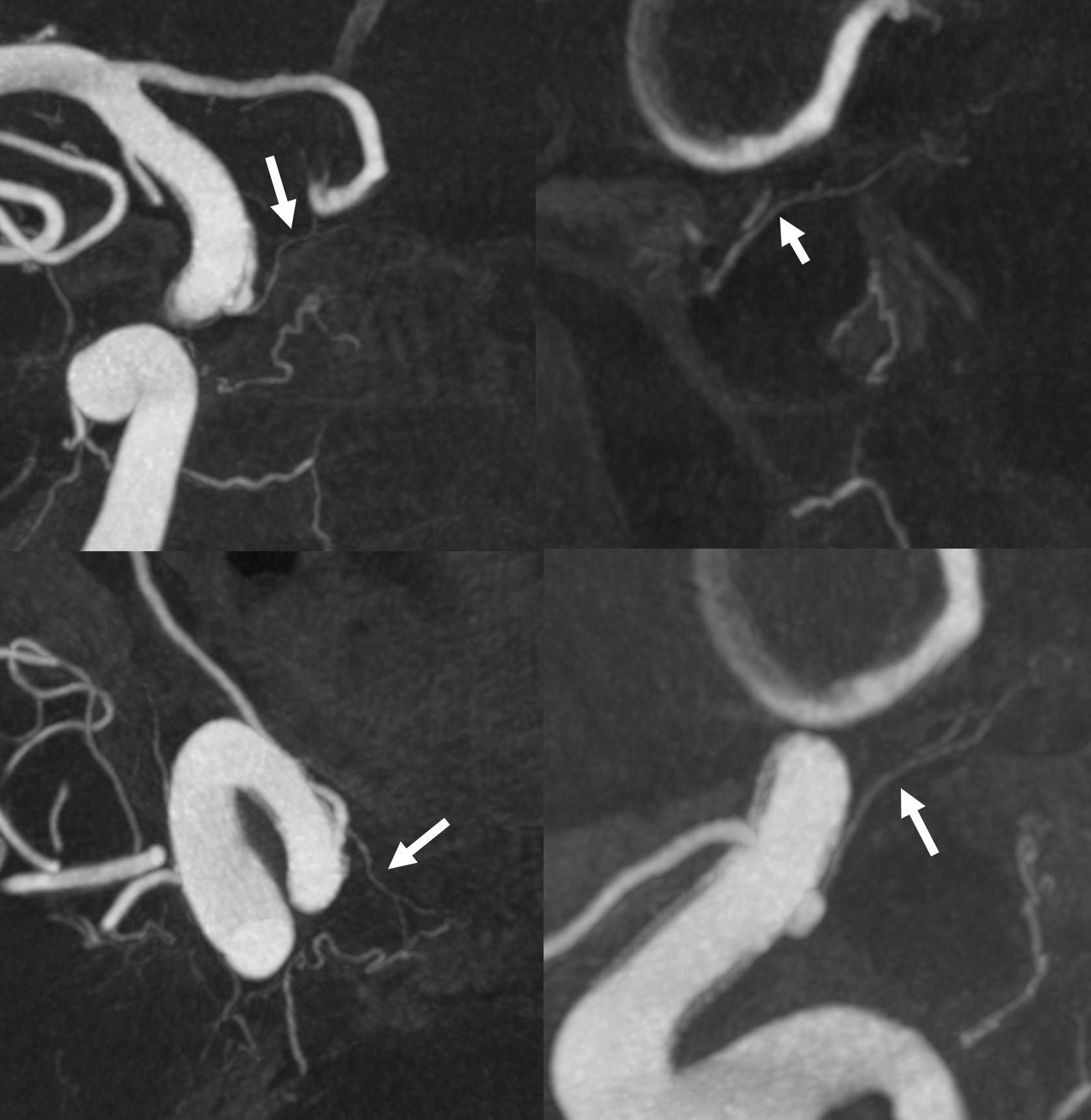
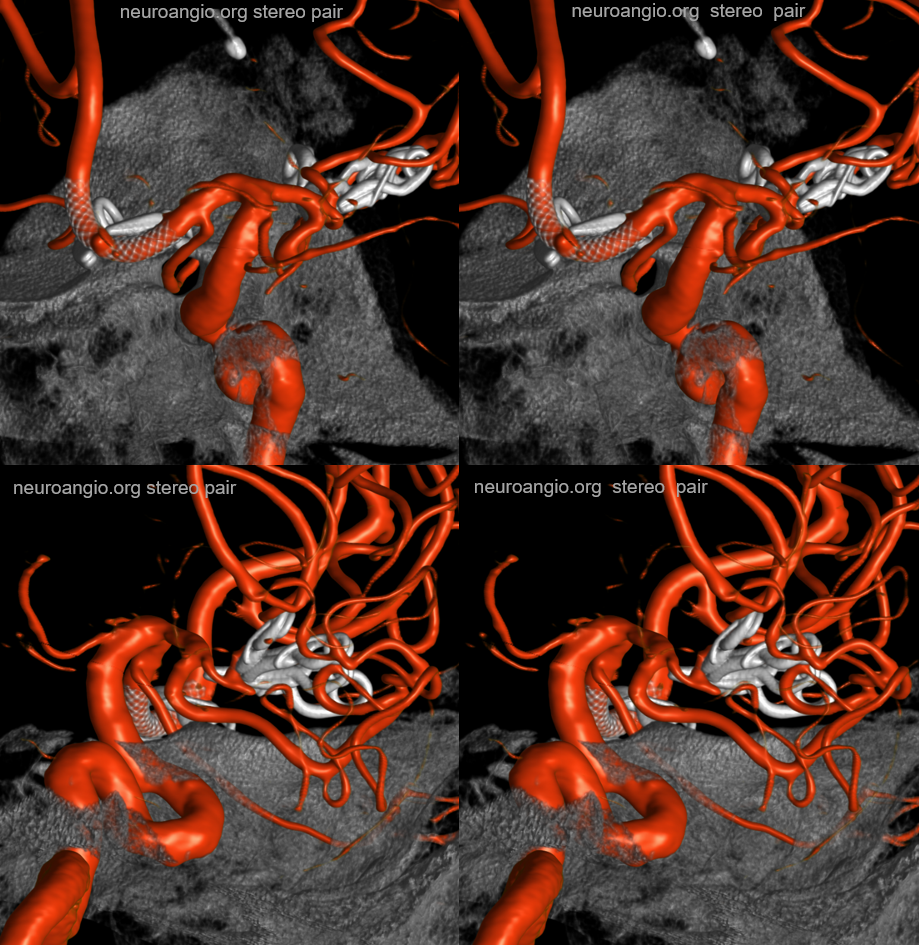
Superior hypophyseal supply of the Optic Nerve
Important point here — since with increasing visualization of this vessel comes possibility of intervention there. Here is an example of superior hypophyseal artery (arrows) supplying the intracranial and optic canal portions of the nerve (dashed arrows). Any ischemia here (posterior ischemic optic neuropathy) would be quite obvious to the patient. Careful now…
Balance — MHT (with inferior hypophyseals) is large (arrow), also supplying anterolateral territory (dashed arrow) of correspondingly hypoplastic ILT. A superior hypophyseal artery is shown by arrowhead
Anterior-posterior balance
Usually the anterior branch is largest. Here, the posterior branch (arrows) is larger, and supplies the hypophysis in a “recurrent” fashion. See PCOM balance below also

PCOM– superior hypophyseal balance
The balance between these two is rarely discussed. You saw the anastomoses between the two above? Thats one proof of a relationship. The other is that they share supply to the optic apparatus AND anterior pituitary. Here, superior hypophyseal is markedly hypoplastic (dashed arrow). Supply to pituitary and optic chiasm is via a prominent branch (arrows) from the proximal PCOM

PCOM or Superior Hypophyseal? See below. We have all seen those “proximal PCOMs” Well, maybe not — could that really be a superior hypophyseal? Spectrum? Below is something that would normally be called a PCOM aneurysm

DYNA — dashed arrows point to a more proximal superior hypophyseal supplying the upper stalk. Then comes aneurysm and its bigger branch (open arrows) — a pseudo-PCOM if you will. It also contributes to supply of the lower pituitary stalk (solid arrows). The rest goes to the thalamus — as would a PCOM. There is no obvious connection to the PCA. Which is another curious question — when is a PCOM not a PCOM based on that. If you think these are irrelevant pontifications — they are not. Think of what is the territory at risk if this aneurysm is to be treated. And what is the best method? Coiling? Flow Diversion? Clip? Not so irrelevant anymore…
No labels
Another PCOM supply of pituitary — hypoplastic anterior superior hypophyseal branch (dashed arrow), PCOM (arrowhead) supply of pituitary and optic apparatus (arrows)
Largest PCOM supply — note very small classic location superior hypophyseal (dashed arrow). Large PCOM origin supply to pituitary (arrows). Note aneurysm (superior hypophyseal maybe?) and relatively distal origin of the ophthalmic

Posterior Pituitary Supply — MHT Balance
Excellent example of contralateral balance. On the left, there is a hypoplastic posterior hypophyseal network (part of MHT, arrowhead), and a prominent superior hypophyseal artery (associated with a small aneurysm). On the right, the opposite is true — large inferior hypophyseal arteries (dashed arrows) extending past midline due to contralateral hypoplasia, and a smaller superior hypophyseal, without aneurysm — not visible on these VRs, but seen on subsequent MIP images

MIP images — there is a small right superior hypophyseal artery present
Another example
Spectrum and balance again. Usually, the inferior hypophyseal branches from the MHT supply the posterior pituitary. Here, the MHT is well-developed, but primarily supplies the free margin of the tentorium, while the posterior pituitary is fed by the superior hypophyseal branch (arrow).
Same case MHT — the larger trunk (dashed arrow) is mainly marginal tentorial, smaller one (arrowheads) is clival branches inferiorly towards anastomoses with ascending pharyngeal counterparts
Yet another one — large anterior branch (with infundibulum), no ipsilateral MHT supply
See smaller “middle” hypophyseal as well
Another Infundibulum here –stereo
There is a very real small ophthalmic aneurysm though…
Also see small PCOM contributing to chiasm / tract supply (arrows). A large superior hypophyseal supplies the stalk. The inferior hypophyseal / MHT are hypoplastic
Particularly large superior hypophyseal arrows), supplying both posterior pituitary and bony sella (MHT or McConnell Territory classically). Case courtesy Dr. Vera Sharashidze
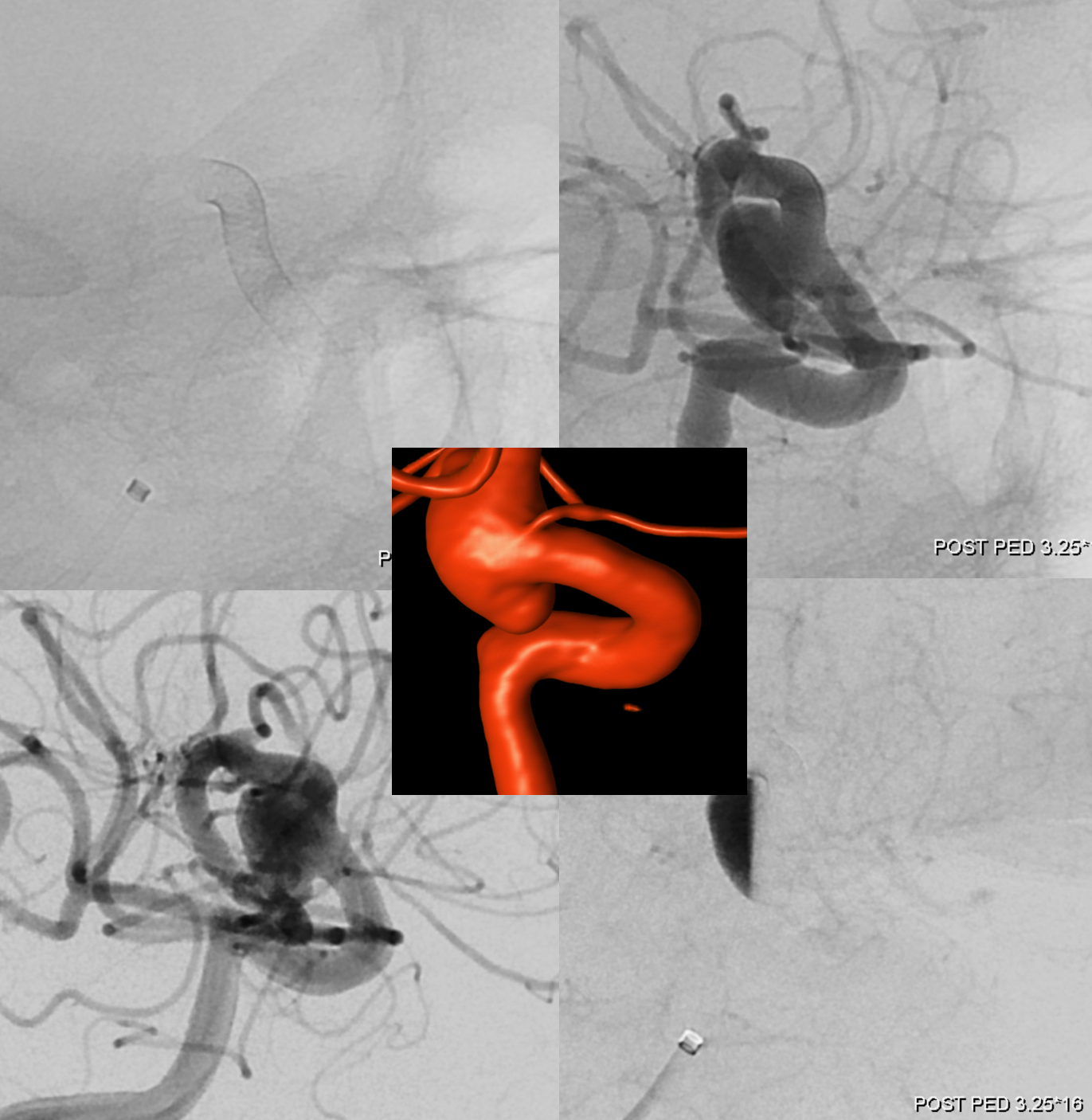
Patent Superior Hypophyseal artery (arrow) post Pipeline Embolization Device placement (6 months post).
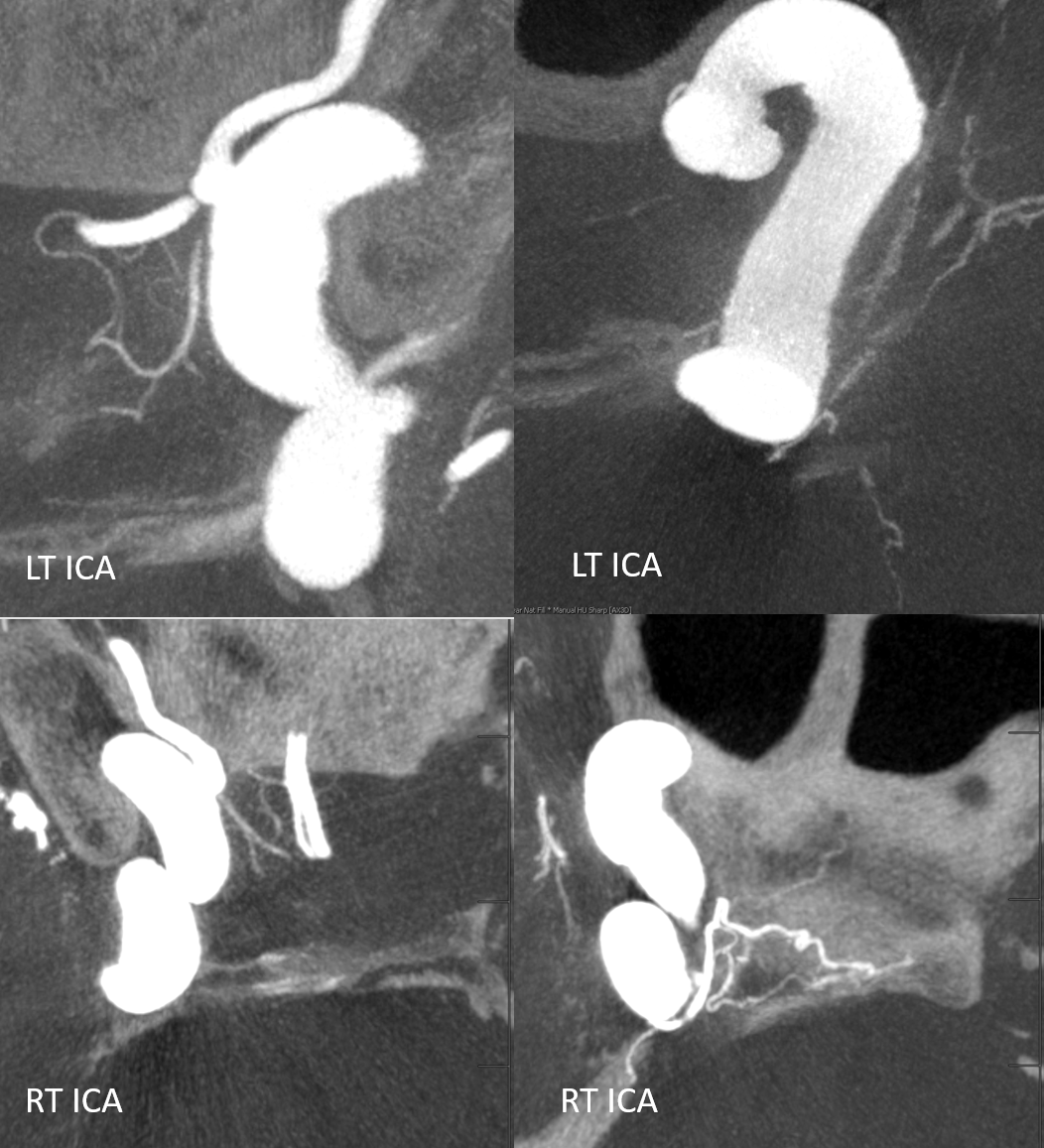
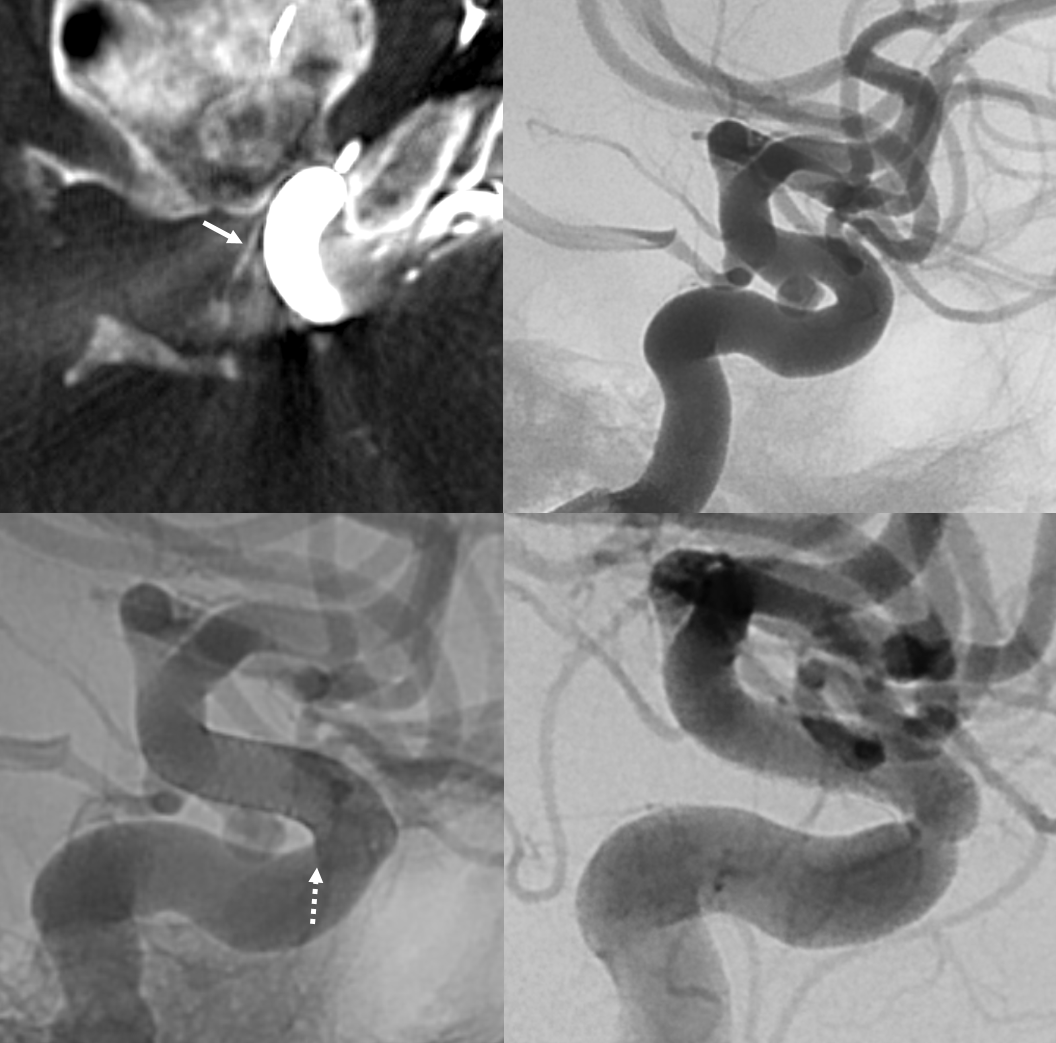
The patency of jailed vessels post technically optimal flow diversion (good wall apposition, good antiplatelet coverage) is principally determined by the collateral potential of the jailed artery. Ophthalmics occlude, asymptomatically in pretty much all cases, because of rich external collateral networks. One way to estimate collaterals is to see what happens to arteries post flow diversion. Below, pre-treatment top row shows two patent superior hypophyseals (arrows) and ophthalmic. Six months later (bottom row), the aneurysms and ophthalmic are closed, while superior hypophyseals remain patent.

Another Example
Note stenosis at the proximal segment of the device due to the proximal edge terminating on the curve of the anterior genu (dashed arrow). This is a kind of T-bone configuration which usually heals with a stenosis.
Another example, in setting of multiple aneurysms. Post clipping of ruptured ACOM and bystander MCA aneurysm, and subsequent Pipeline Shield Embolization of a small ACOM residual. Stereo images show presence of Ventral Ophthalmic Artery origin from proximal A1. The Pipeline is placed distal to its origin, just in case.
Movie
MIPS — great anatomy of the MHT, ILT as well. The MHT is somewhat hypoplastic. ILT supplies bulk of its territory via the recurrent tentorial artery. There are 3 superior hypophyseal arteries, supplying large portions of the optic nerve, chiasm, and probably some proximal tract, together with the PCOM
Capsular Arteries of McConnell
These are different from Superior Hypophyseals, but often come up together. This is because they were described by McConnell in a fantastic manuscript on arterial supply to the hypophysis. The anterior hypophysis is supplied by the aforementioned superior hypophyseals. Posterior by the inferior hypophyseals. The arteries of McConnell supply the dura and bone of the sella turcica. They are considered dural, and do not as a rule supply the hypophysis. Too small for even HR CBCT resolution, they are found in about 1/3 to 1/2 of surgical dissections. Origin is from the MEDIAL aspect of the horizontal cavernous segment (opposite side of ILT). Courses medially towards the bottom of the sella. Below (arrows) is a particularly large one (because it feeds some posterior pituitary for some reason). Note beautiful anterior pituitary / stalk supply on bottom right image.
Without arrows:
Cases of Superior Hypophyseal Artery
There are a myriad cases of SHA involvement in macroadenomas. It is the artery of supreme importance in surgical adenoma resection. We will have some soon.