
Case with Vera Sharashidze, MD.

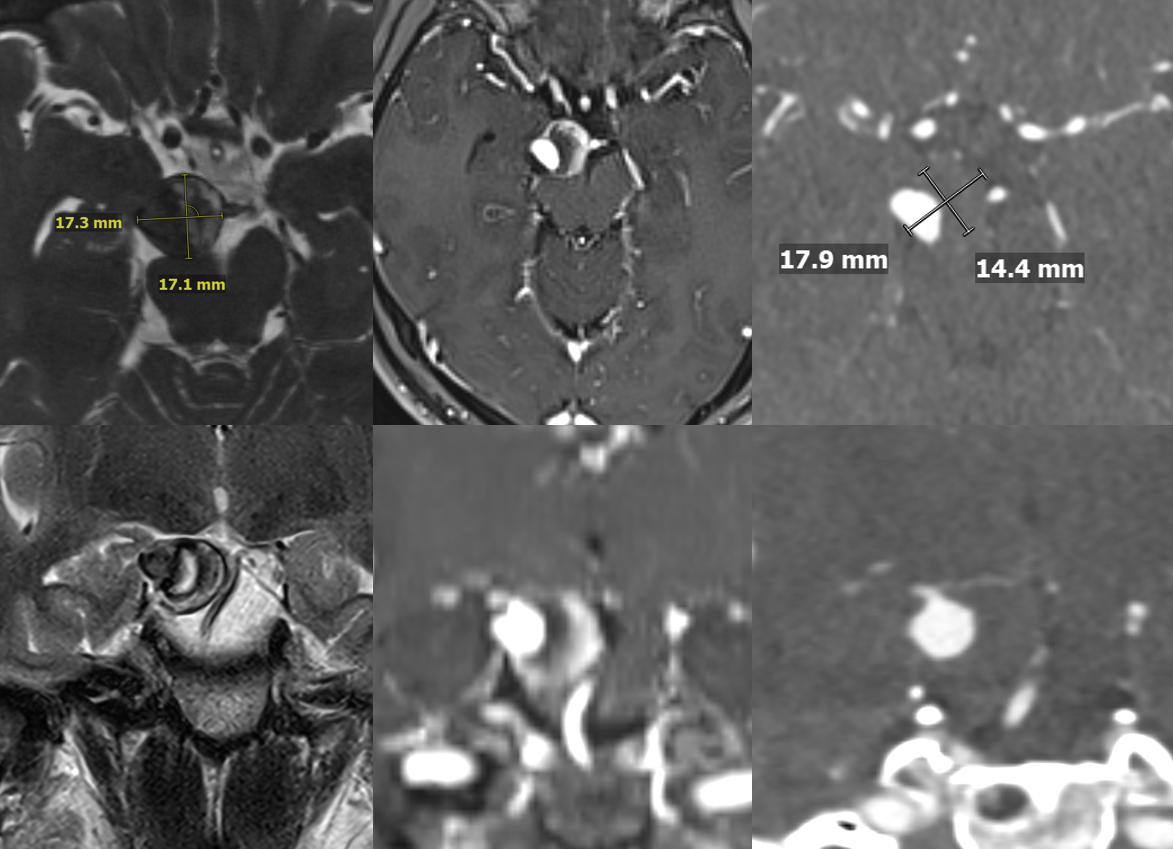
History is progressively severe headaches
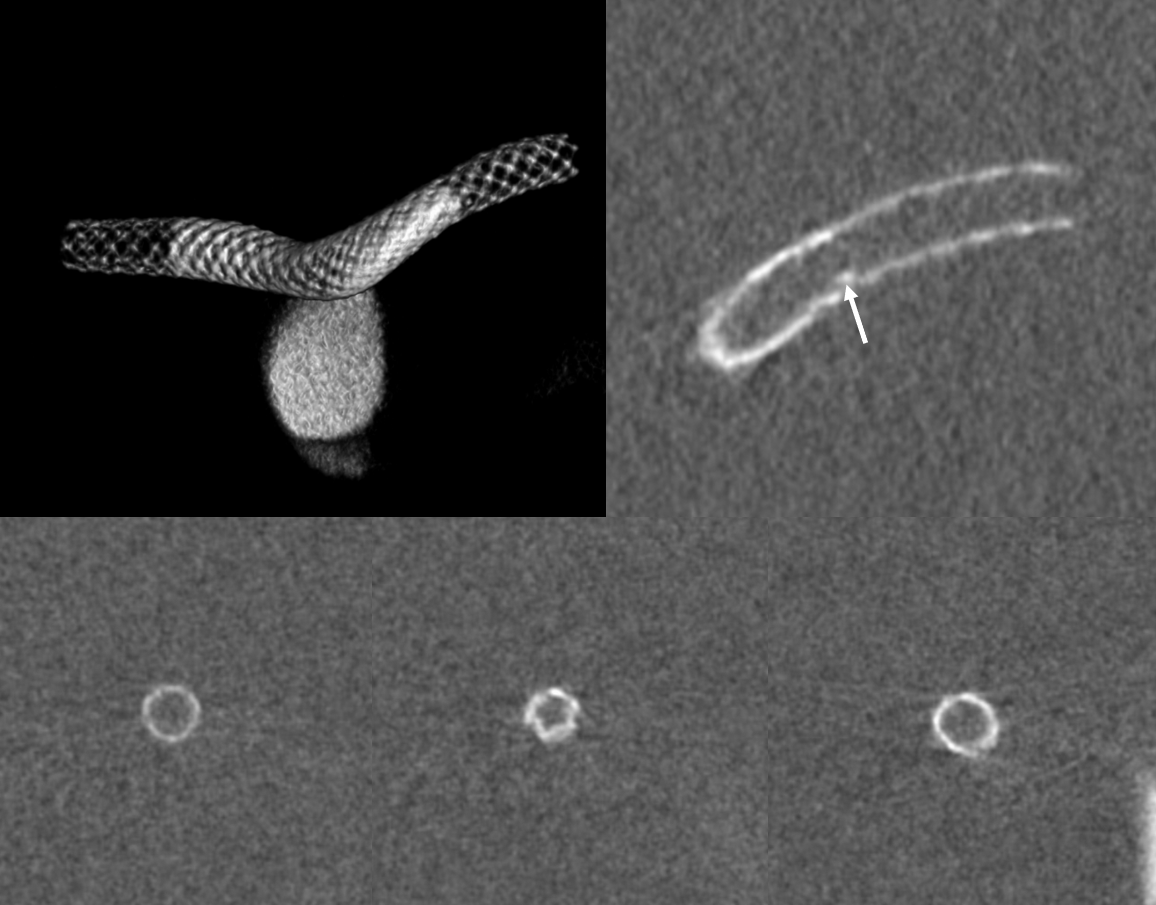
Stereo pairs below. Arrow on the medial choroidal branch
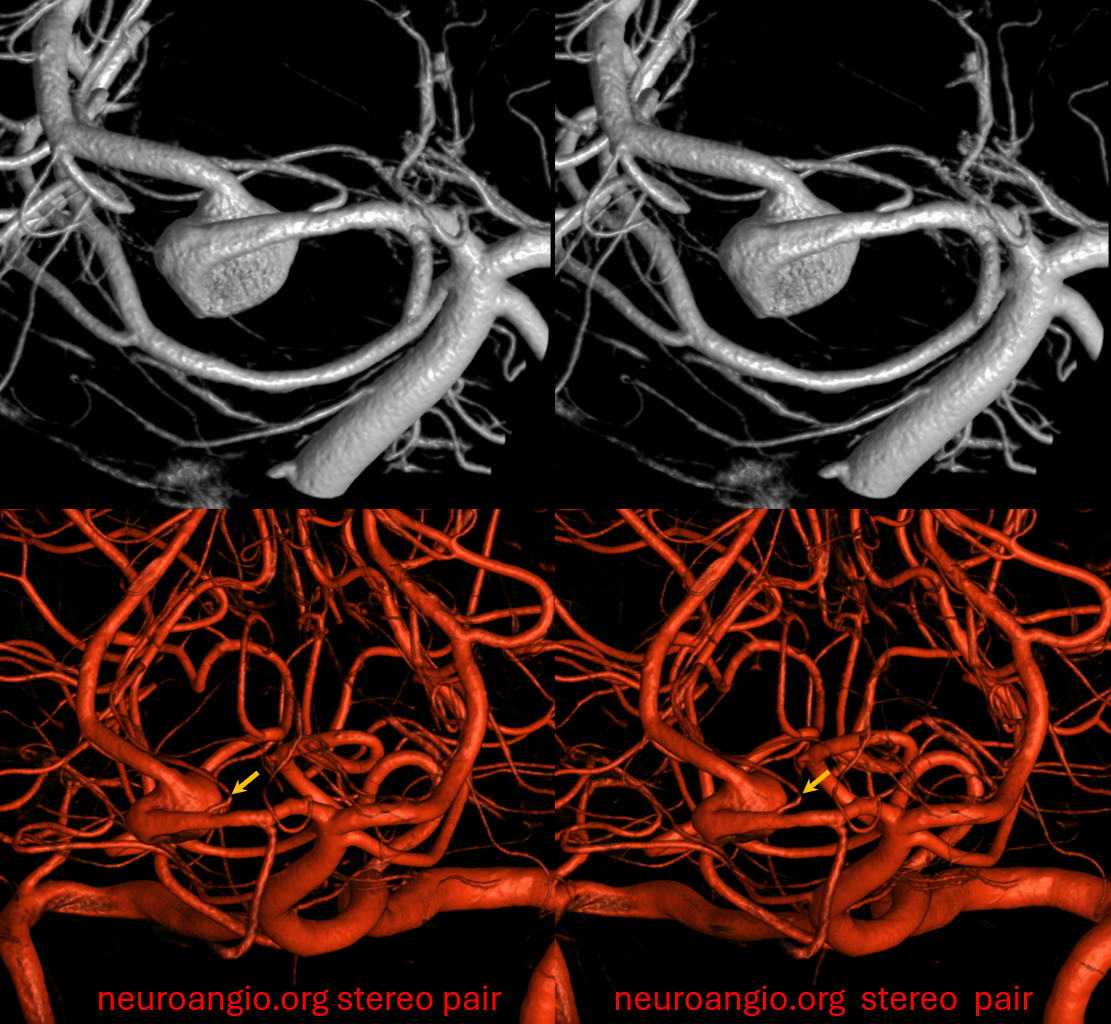
Bonus — can u also recognize the long collicular branch — distinct from medial choroidal? Where is its origin?
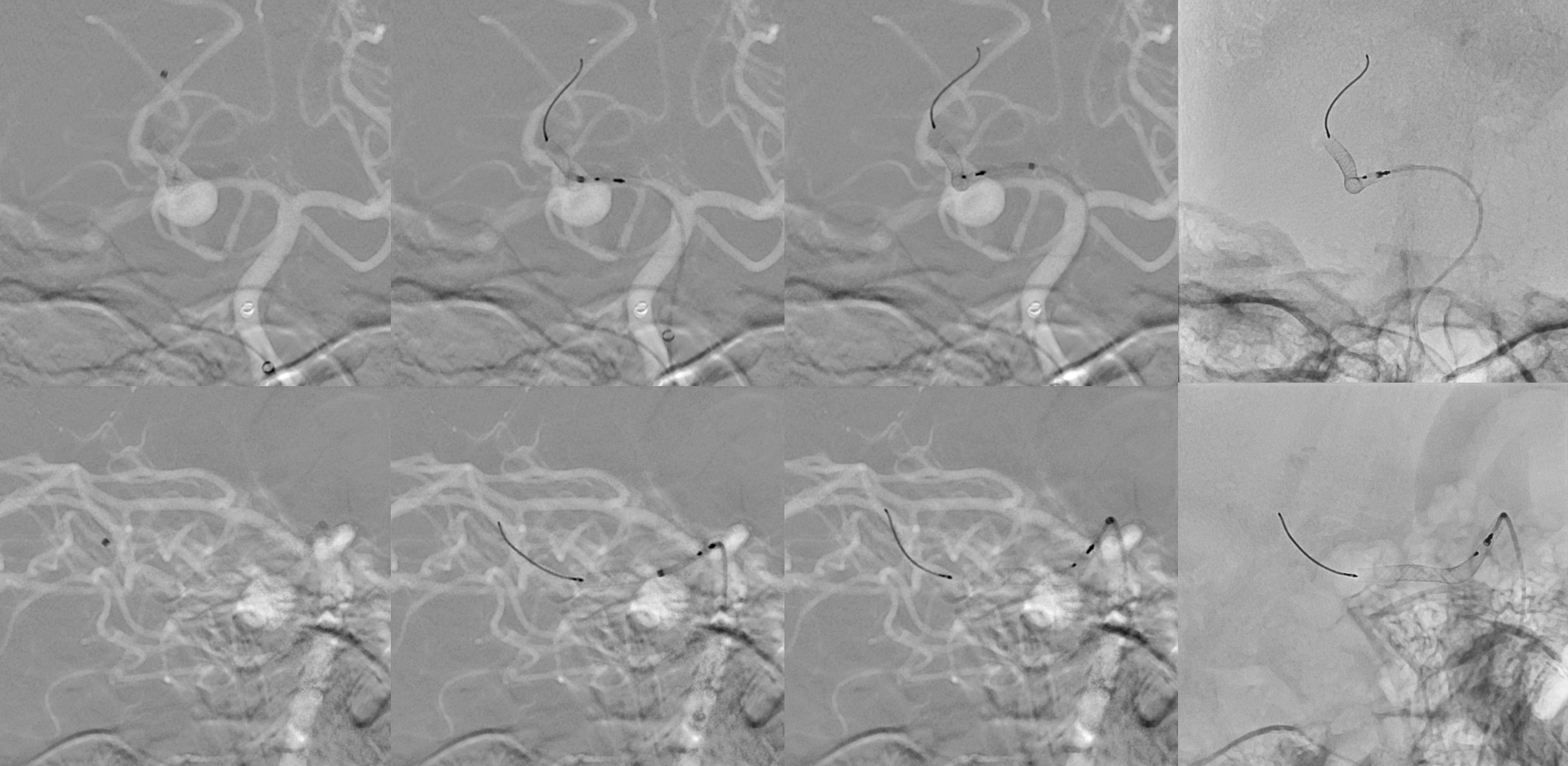
Before we treat this aneurysm, some good anatomy. On the left, the lateral (arrows) and medial (dashed arrows) choroidal branches originate from the same pedicle — P2 segment origin. Usually this is the origin of the lateral choroidal, which in this case supplies medial choroidal territory also. On the right side, the usual anatomy, with medial choroidal origin more proximally (ball arrow).
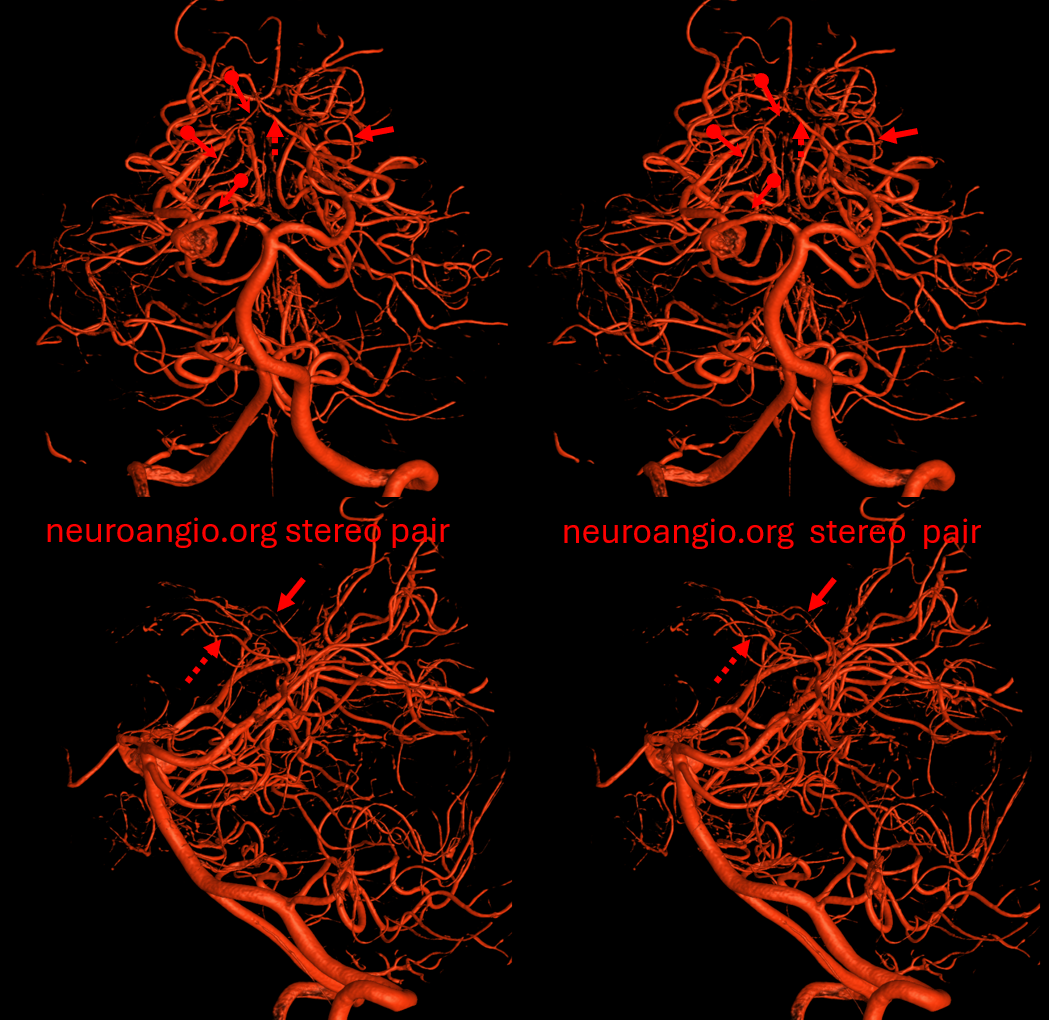
Similar to the anterior choroidal, the posterior choroidals have pre-plexal and post-plexal segments. The pre-plexal segments are variably eloquent, and may supply parts of thalamus / epithalamus, internal cerebral peduncle, and periventricular tissues in general. It’s generally not a good idea to close them proximally.
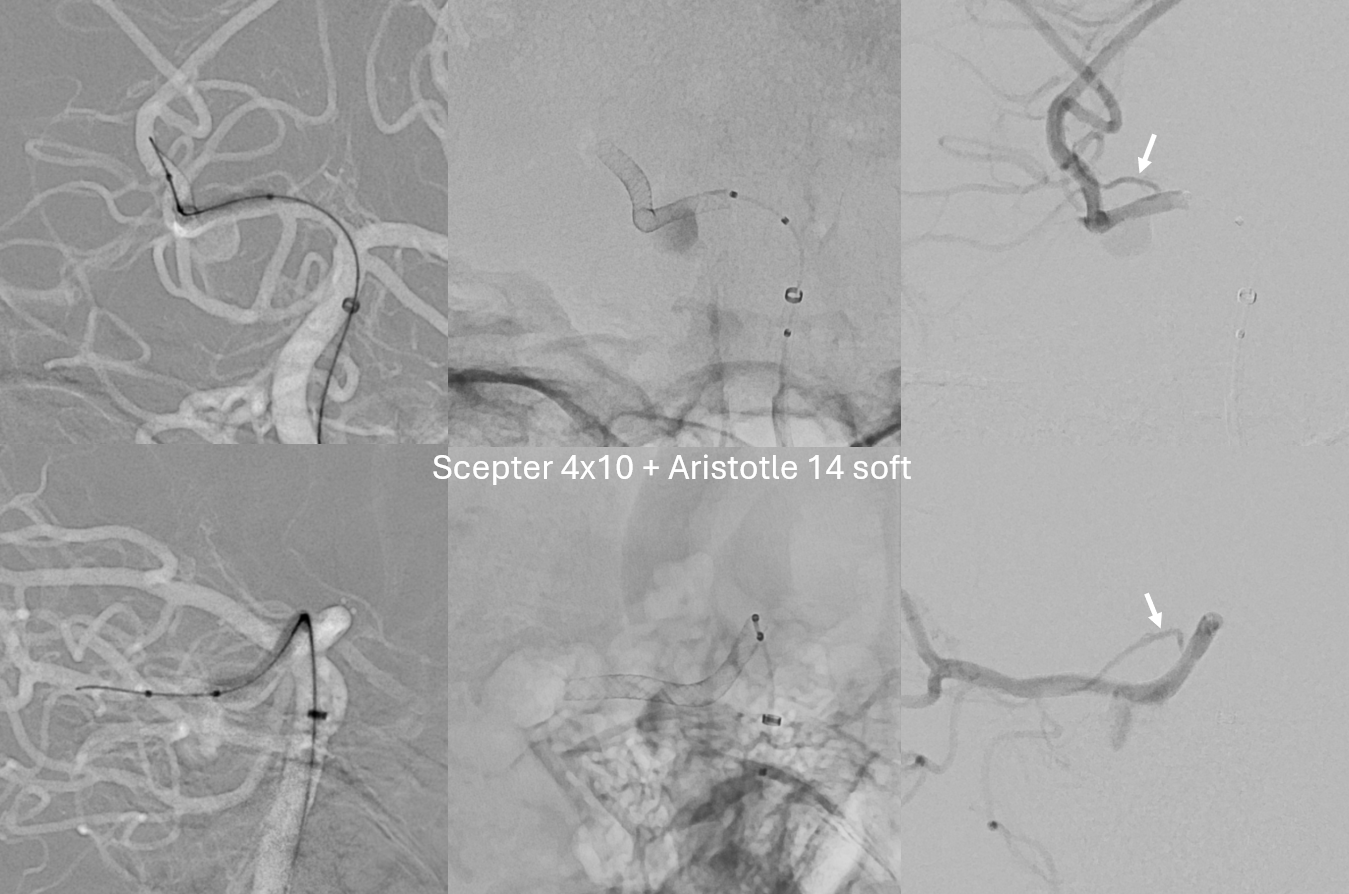
Loop-to-loop / around the world is the only way to go. Having an Aristotle 24 helps a ton with a 27 catheter.
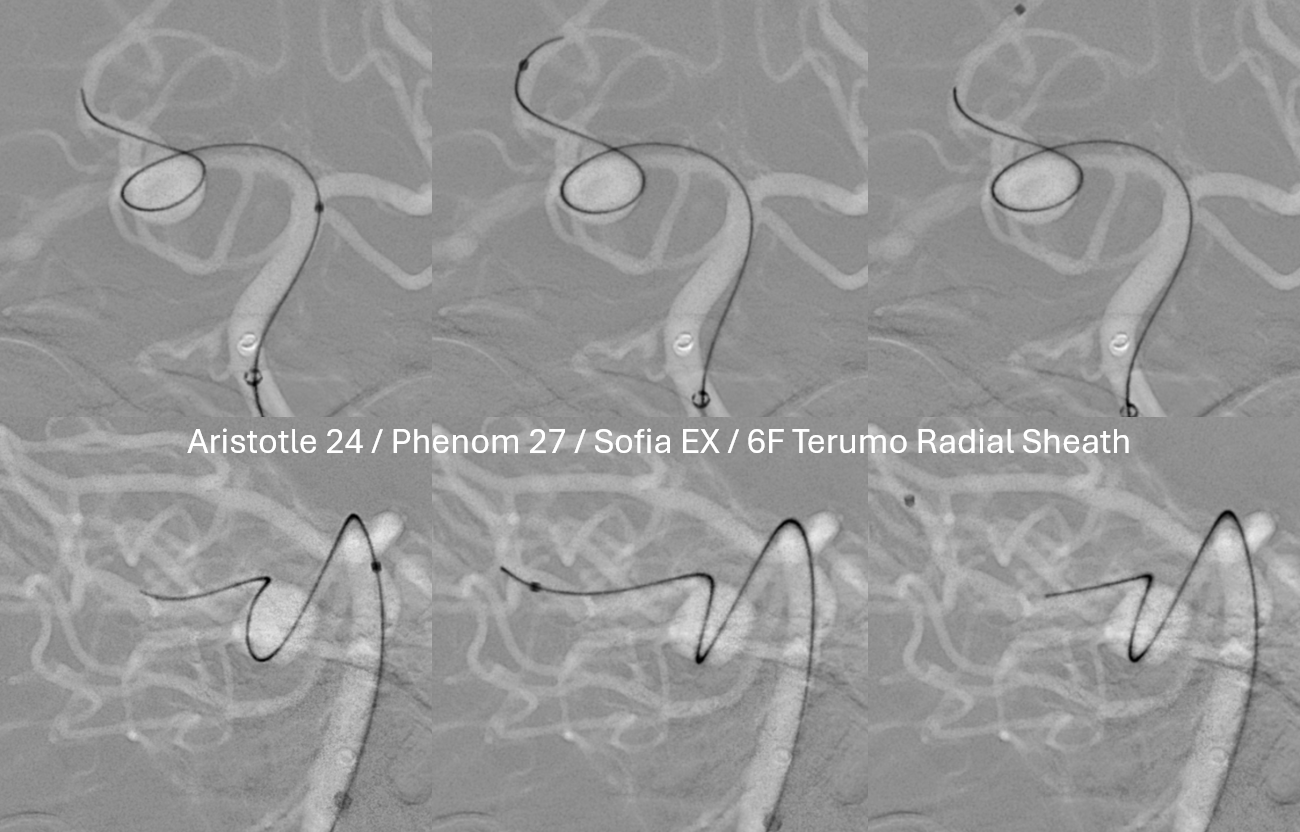
It is sure easier to do this with a 21 or 18 system. But, we believe, PED Shield is the best choice here — for our part.
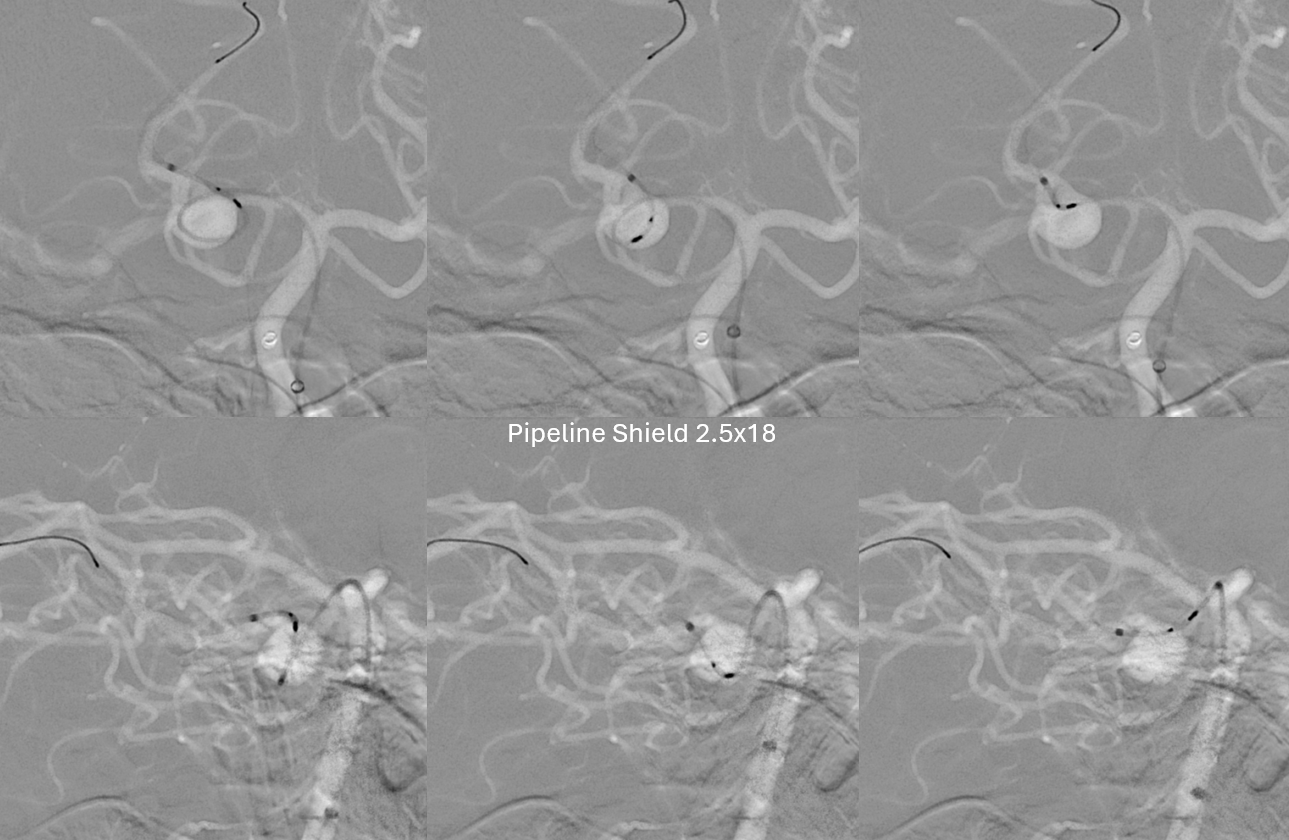
The Phenom did not reduce by pulling on its own. It did reduce with partial deployment of the Pipeline. We prefer this method to stent-triever — less steps and less vessel injury.
Some videos for you, in-depth step by step stuff. Real time speed — so relax and enjoy
In the video below, do u see a twist in the Pipeline part that’s still inside the Phenom 27? That’s what happens when the catheter is “reduced”. Resheathing may get rid of the twist — especially with smaller diameter Pipes.
Now that the Phenom is reduced and loop removed, we can resheath and pull the PED more proximally. Of course one has to be careful not to pull too much etc.
Notice that there is narrowing in the pipe at the neck — the configuration of the vessel has changed because of the reduction of the loop. The pipe needs to be “loaded” or pushed to help open it there. This is where there is a difference between 27 pipe and 21 vantage or smaller devices — they will not open here the same way — smaller chronic outward force. Another option is to keep the loop and deploy flow diverter around the world but we don’t like that.
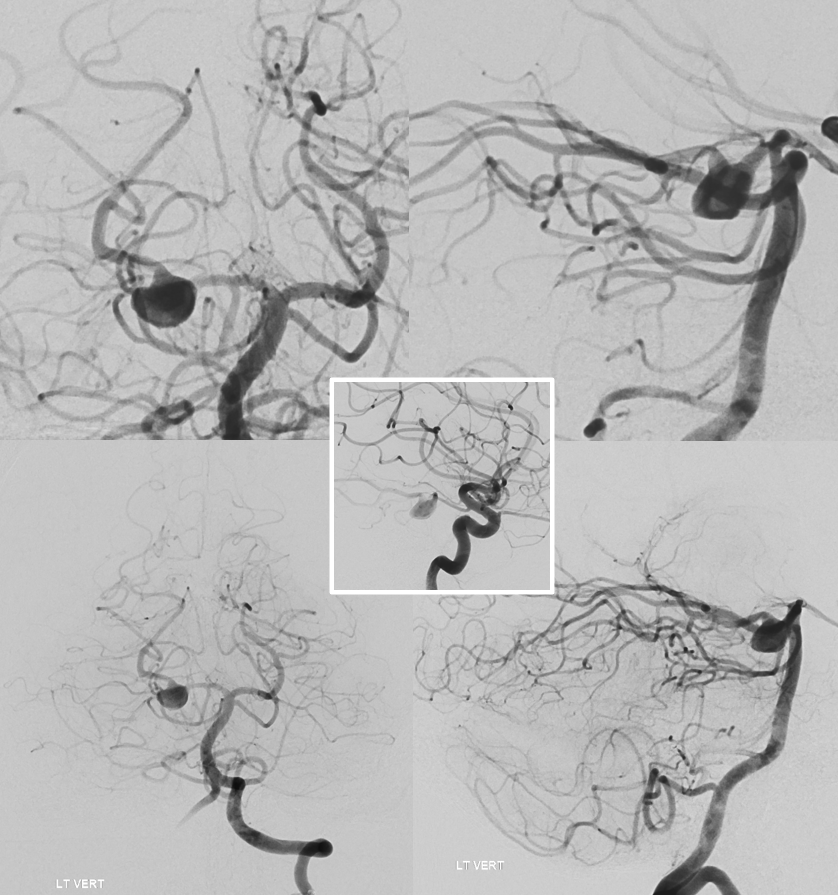
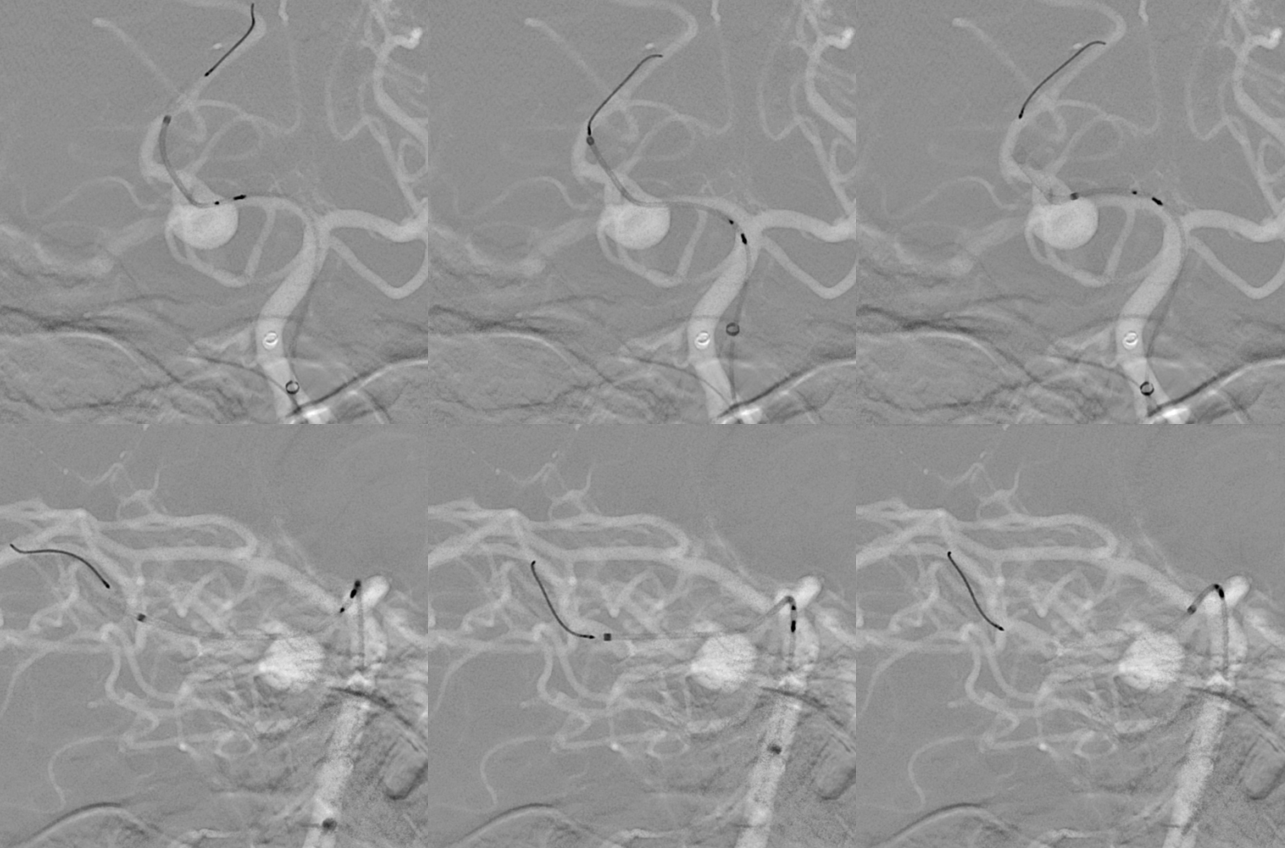
Now in static images
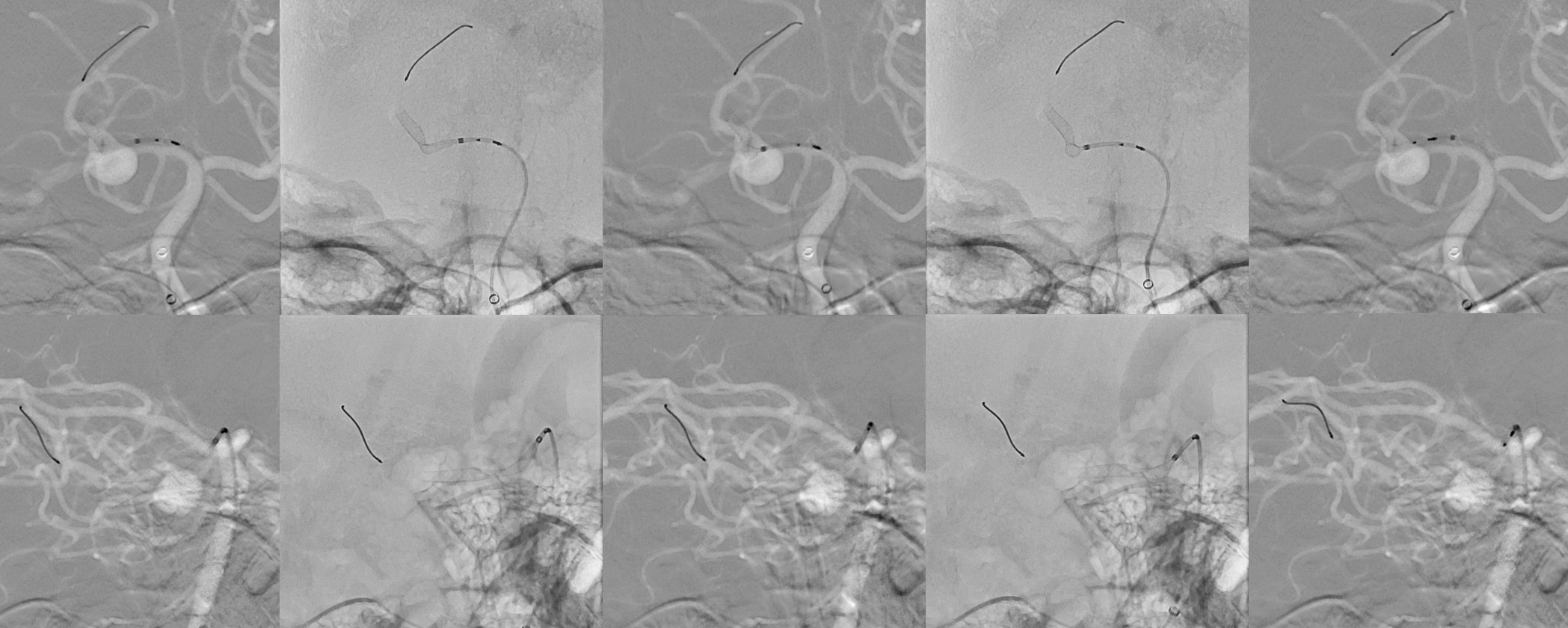
What’s very, very wrong with this picture? What are the possibilities? Look here before going to next one.
The answer is below
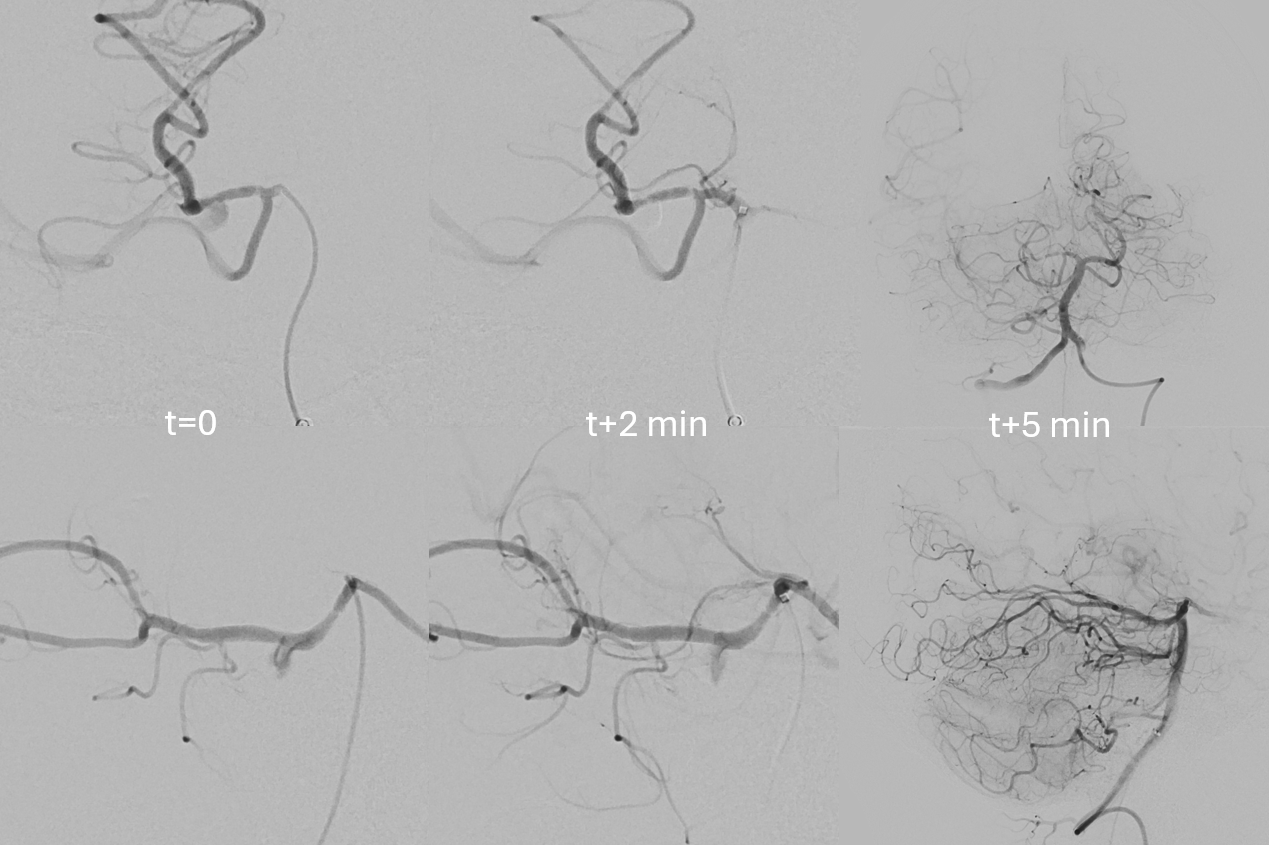
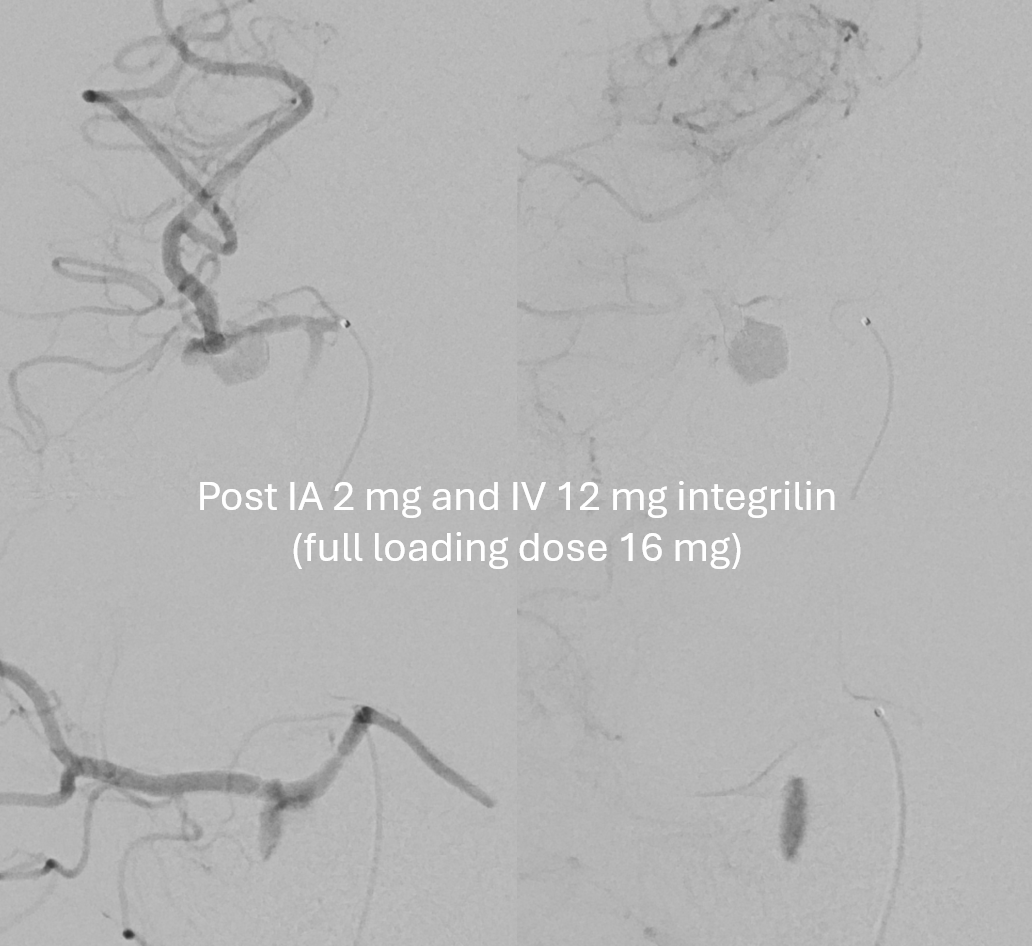
Post IA verapamil, IA and IV integrilin. Without integrilin or similar how to do this? It doesn’t matter what antiplatelets they are on — all have some resistance.
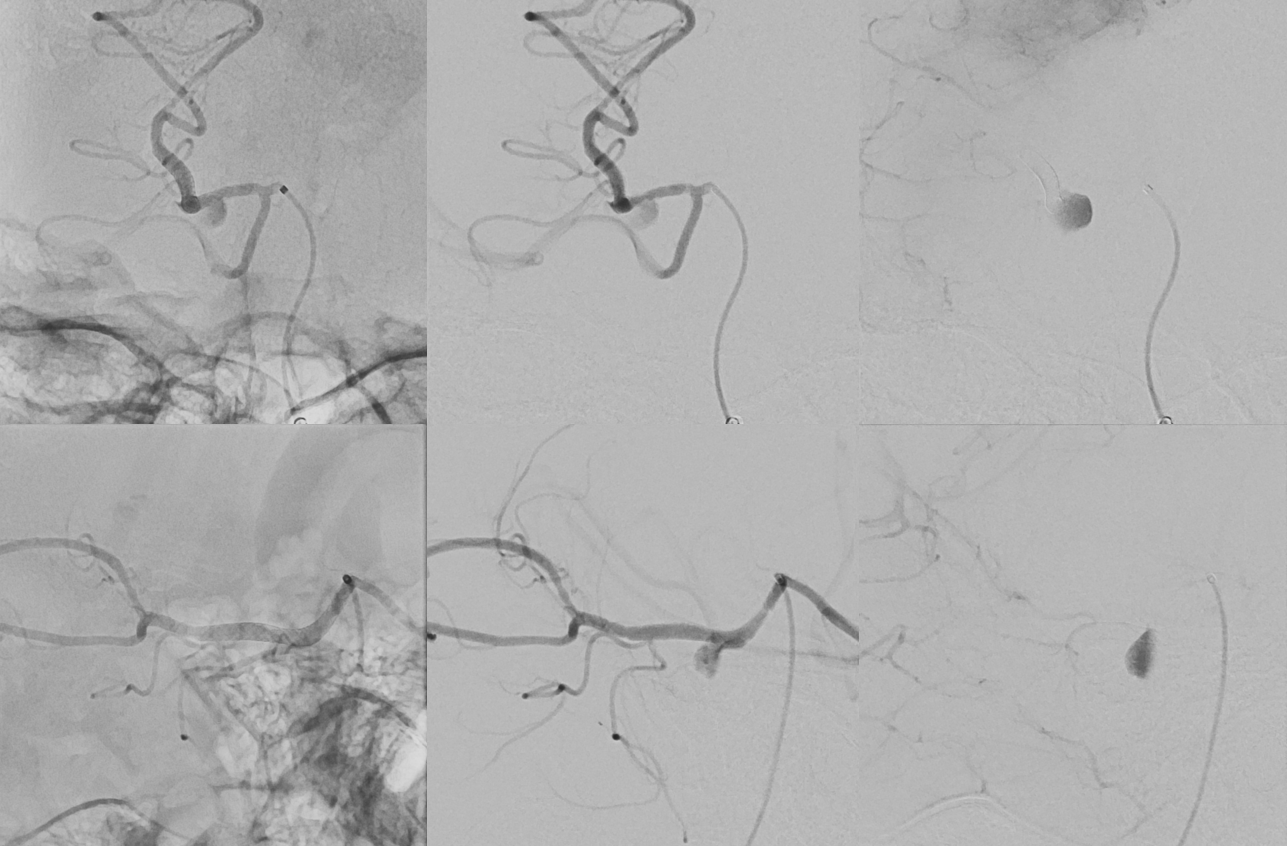
Post deployment of second PED (2.5×10)
Not often that angioplasty can solve this problem — but in this case it does.
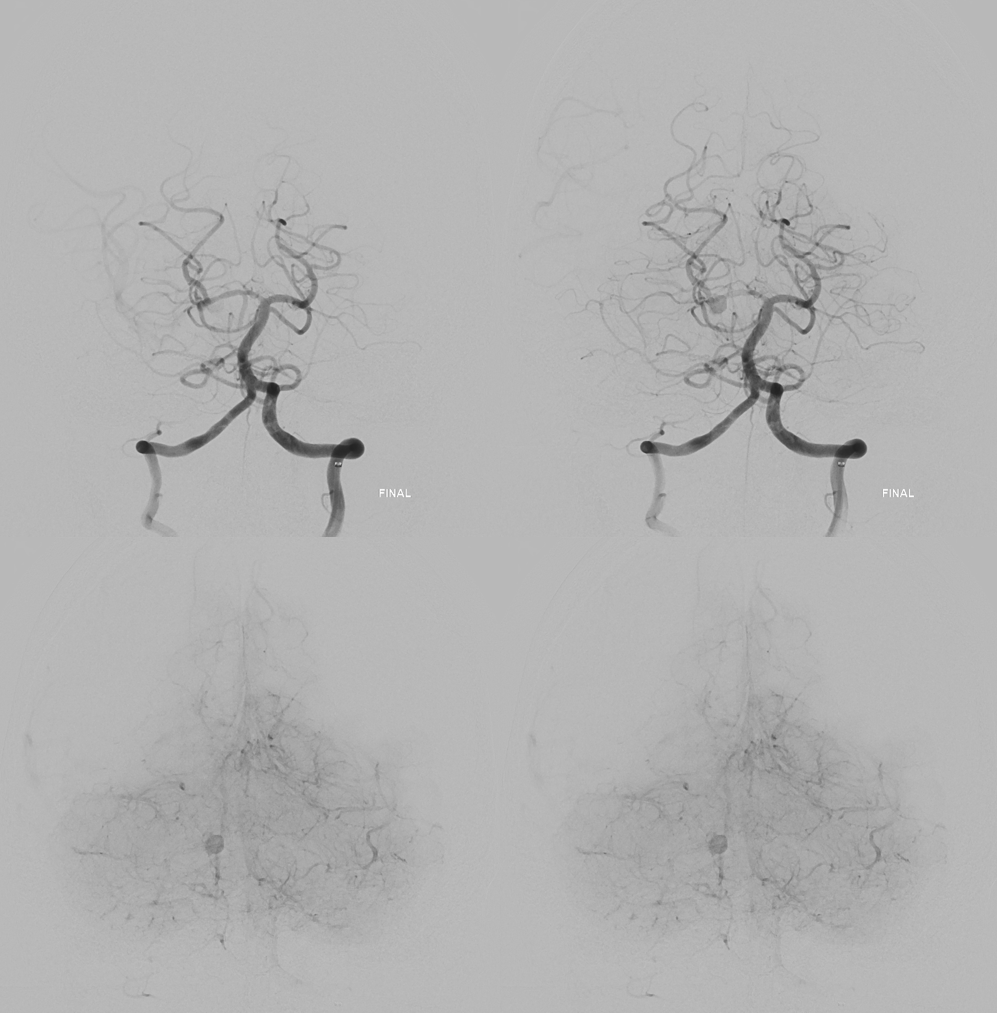
Lets see how to vessel configuration is changed by undoing the loop (middle and lower rows). The lowest is PED superimposed on pre-PED vessel. Note how the medial choroidal origin is also a bit shifted.
Notice precise placement — double coverage of the neck, single coverage of the medial choroidal, and no coverage of the PCOM.
