

The same principles apply to brain and spine. Angiography, both 2D and 3D/Cone Beam CT, is an art. You must be an artist if you want to create images both beautiful and useful. It is a lame excuse, and a catch 22, to say that one does not need images of high quality, that all you need to know is visible on whatever quality one believes is good enough. Could one argue that an operating microscope is not necessary to clip aneurysms because it sees too much or because one is experienced enough to no longer need it?
Without good imaging, one simply doesn’t know what one doesn’t know. Yes, many times we can get away with suboptimal work or compensate for deficient imaging. Generally, though, the more we see the more successful our operations are. This is particularly important in spine, where technique makes a huge difference in both diagnosis and treatment.
Good technique starts with 2D imaging. The vast majority of spine imaging is best done under general anesthesia. However, there are many ways to administer GA. For spine, pharmacologic paralysis and breathold are important. So is bowel paralysis in some cases — achieved with administration of glucagon. Metallic artifacts — EKG leads, wires, etc should be out of the field. Imaging should be long enough to detect slow shunts. All of the above produce optimal 2D DSA images of the spine, without which Cone Beam CT imaging is impossible.
See case here for illustration of above
Cone Beam CT Spine
Arm elevation
For thoracic and lumbar spine images, elevating arms above head makes a big difference. You have to be careful about brachial palsy with over-stretching, and making sure arms are secure. There is no free lunch — you want good results, you have to invest. GA, pharmacologic paralysis, breathold are all essential. Below are examples of the same patient — rotational angiography and reconstructed MIPs — arms down and arms up. The difference is obvious.
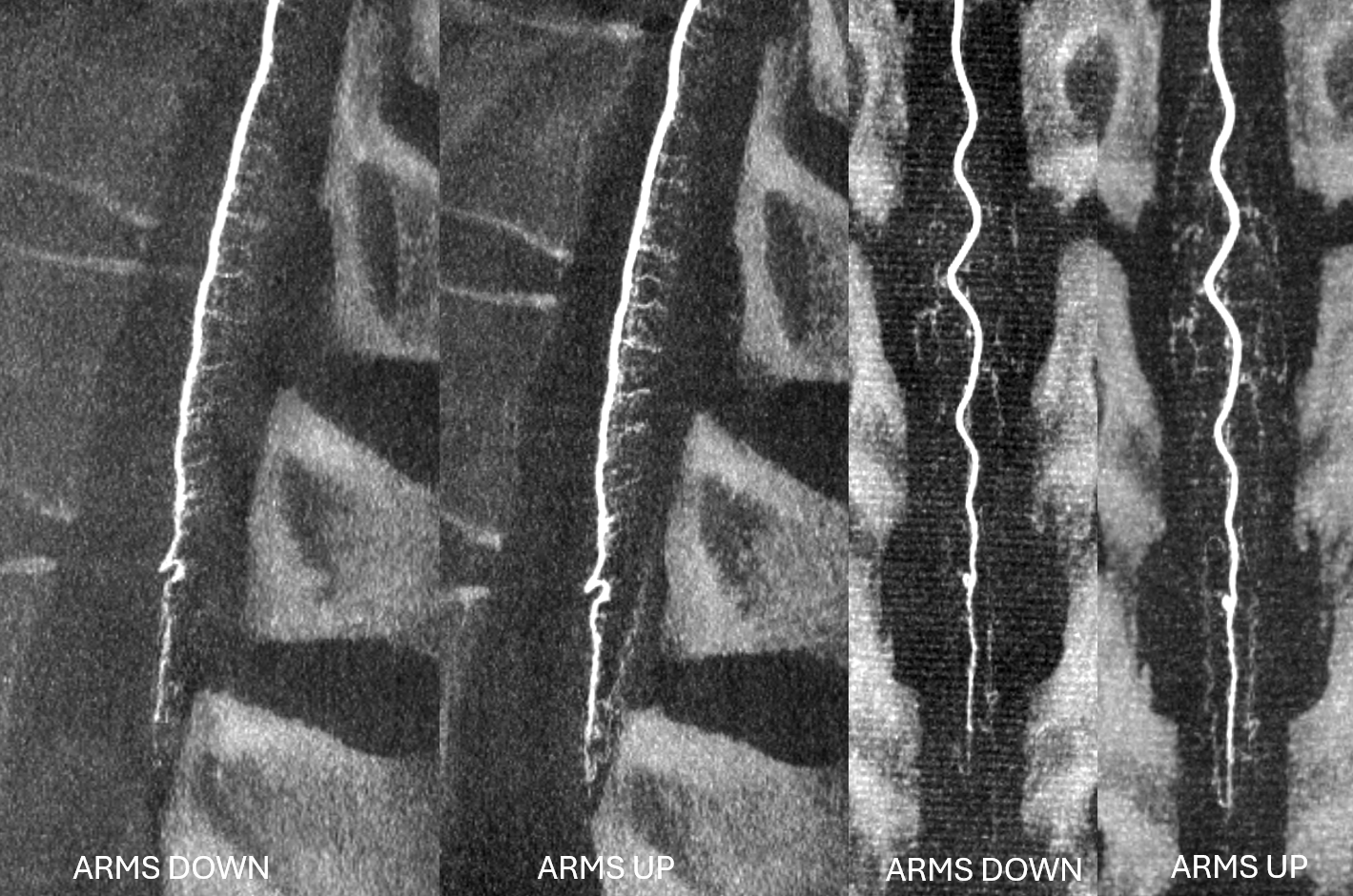
Arms down, arterial phase. Siemens Icono, 7 second micro dyna single volume, 1 cc/sec for 9 seconds, 2 second delay. The thickness is very heterogeneous — too thick with arms in lateral view (dark) and too thin in frontal view (light)
Arms UP, arterial phase. Siemens Icono, 7 second micro dyna single volume, 1 cc/sec for 9 seconds, 2 second delay.
MIPS
The difference is even more striking in venous phase. Selecting venous delay is key. The delay is chosen based on the time between the END of arterial opacification and beginning of venous one
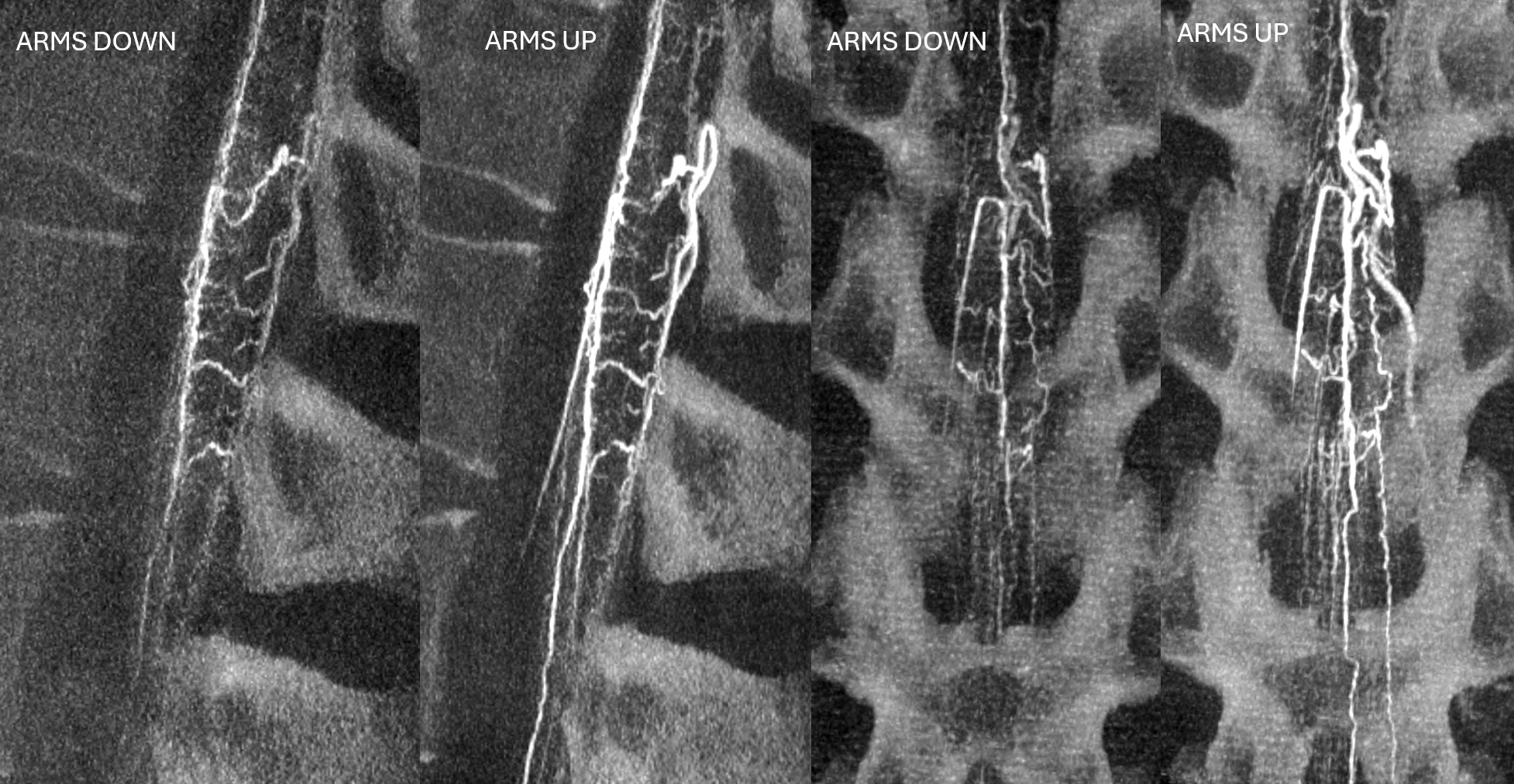
Arms DOWN, arterial phase. Siemens Icono, 7 second micro dyna single volume, 1 cc/sec for 8 seconds, 13 second delay.
Arms UP, arterial phase. Siemens Icono, 7 second micro dyna single volume, 1 cc/sec for 8 seconds, 13 second delay. It could have been even better if wires and EKG leads were moved.
Venous MIPs
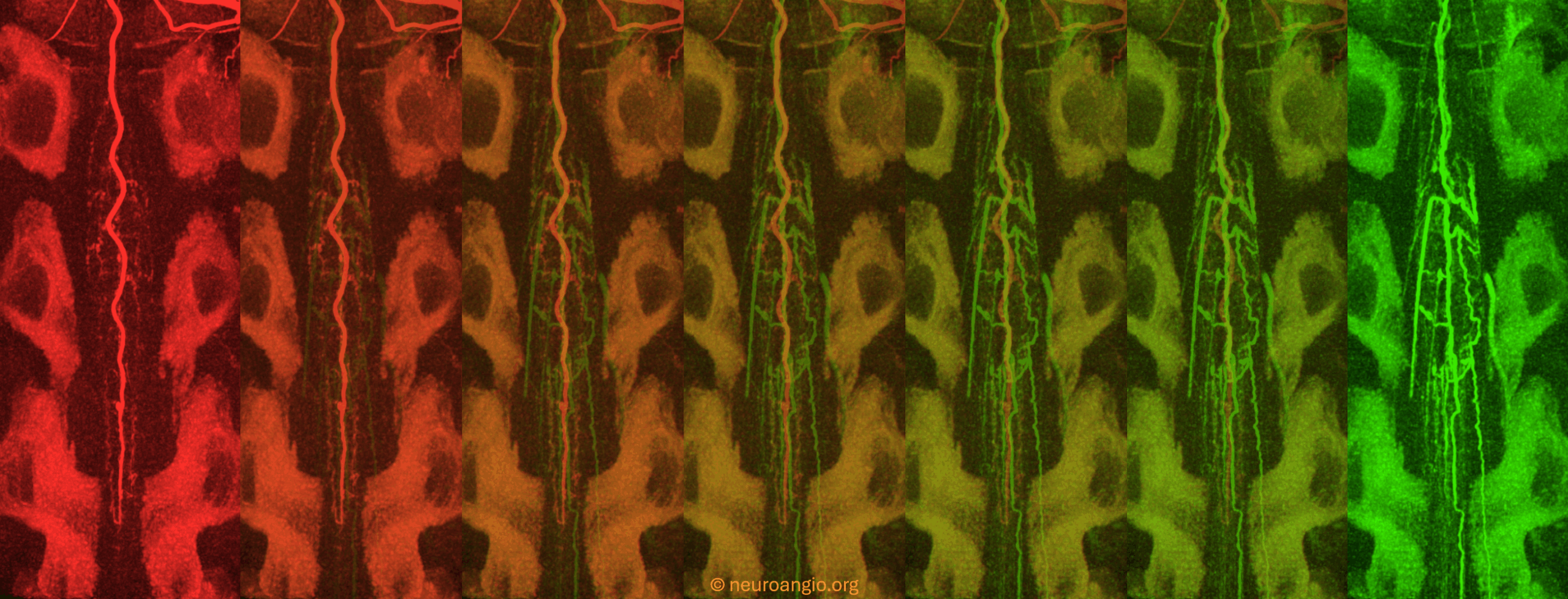
‘”6D” imaging can combine arterial and venous information in one dataset, as below
Movie
A nice case here to show spinal dural fistula pathophysiology and use of CBCT