Occlusion of Labbe group of veins is a rare but potentially very serious complication of stenting, leading to venous infarction. One advantage of braided stents is that they are resheatheable — hence the possibility to partially deploy them, check for Labbe patency, and if you are not happy, reposition or remove the stent. Below is an example
PT on LEFT
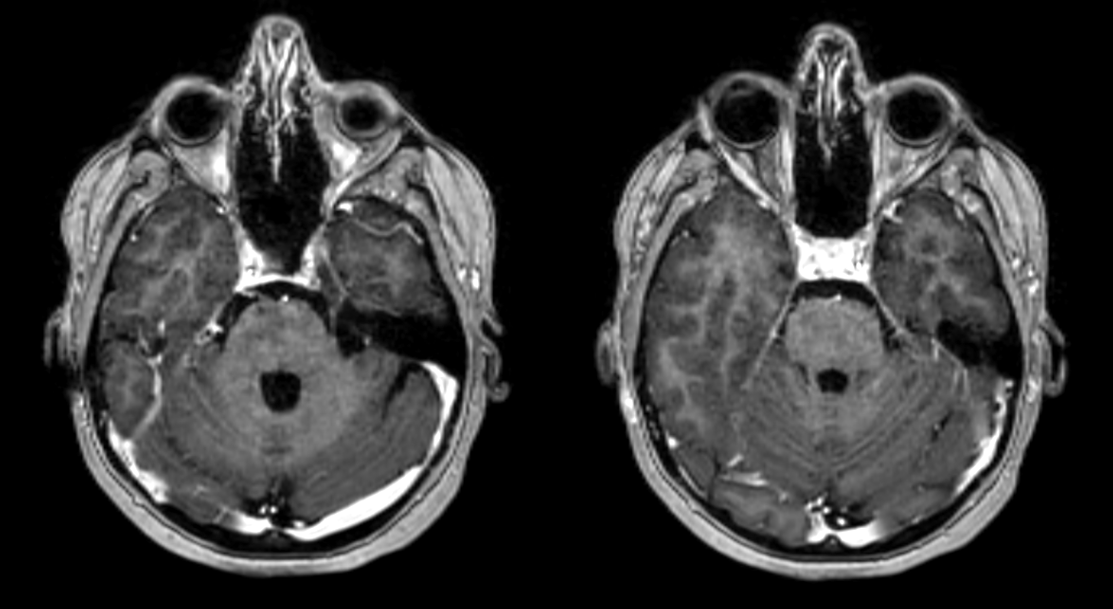
Arterial Access is important
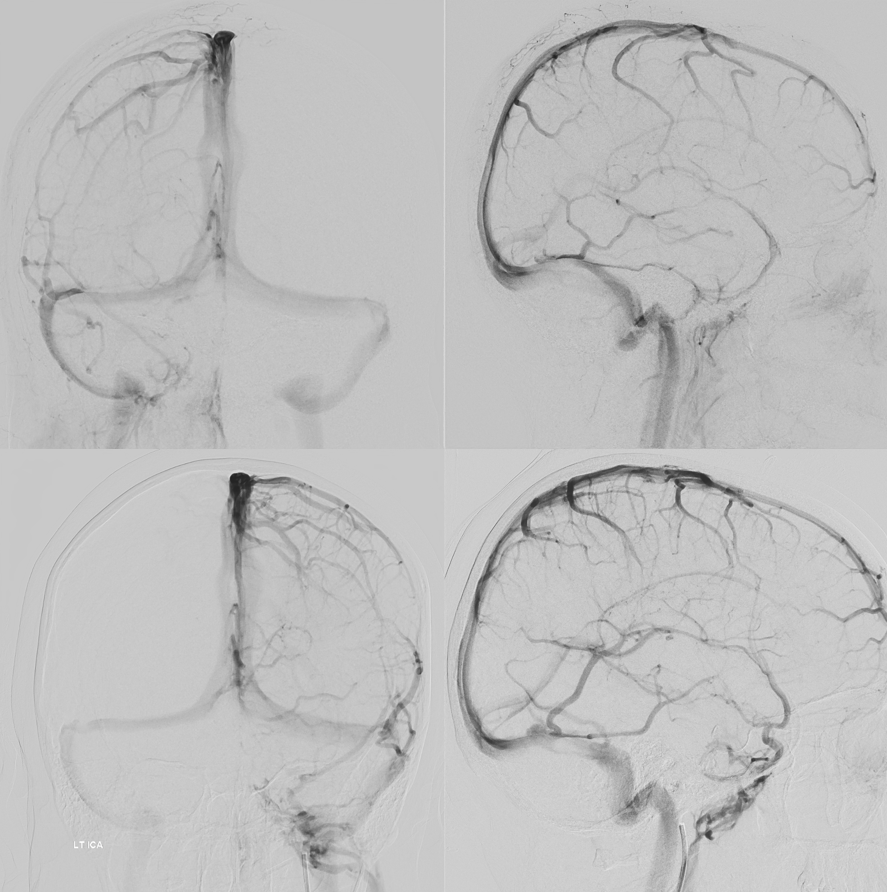
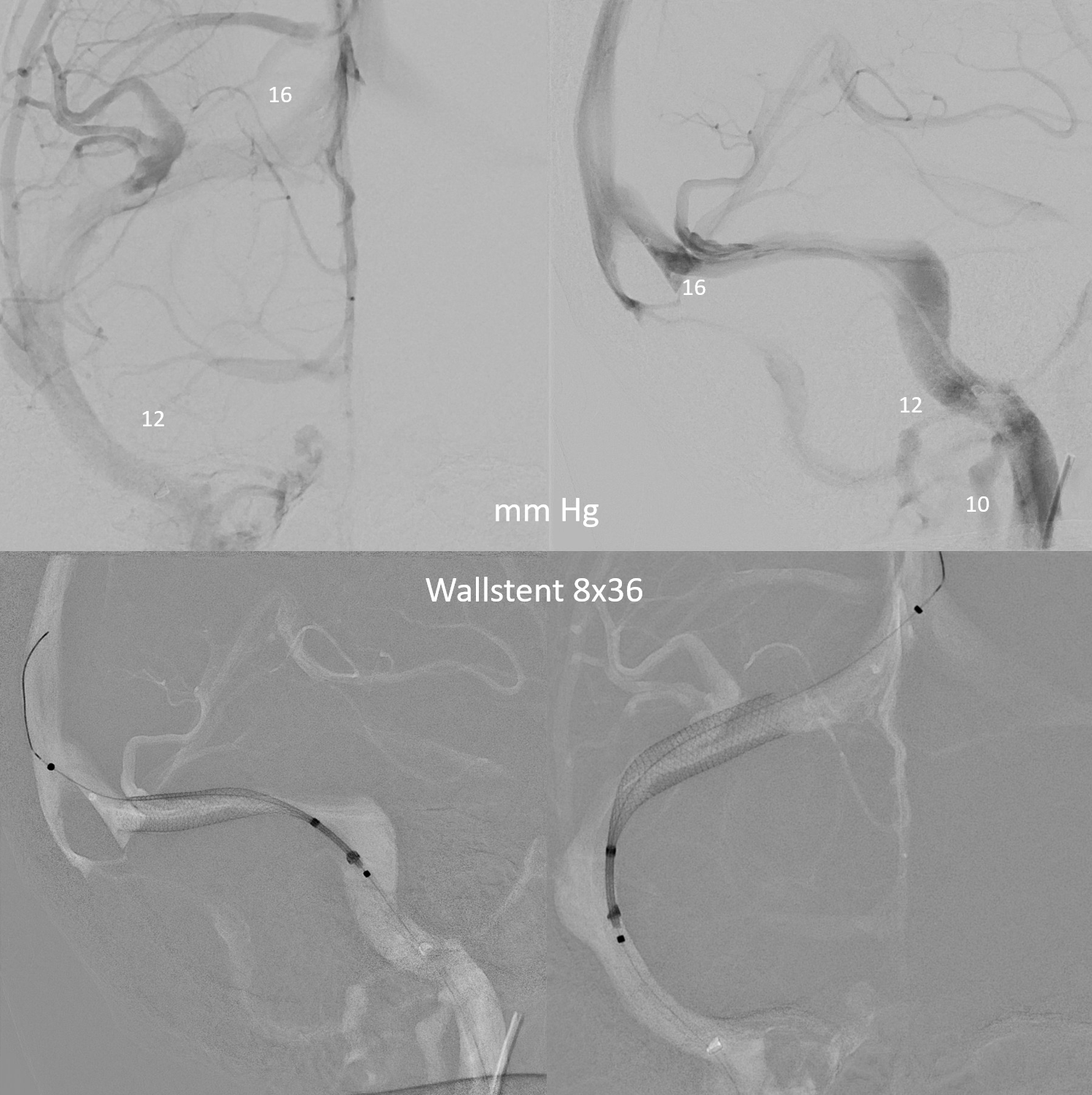
Venous phases RT and LT ICAs. Note large left ICA Labbe and inferior temporal veins
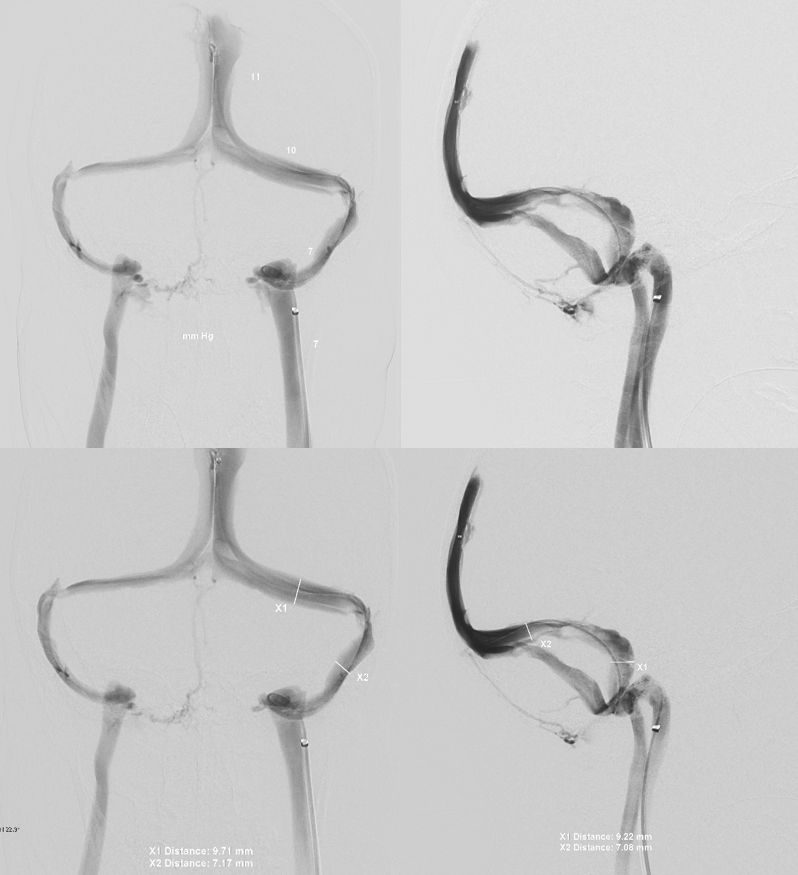
Venogram. Gradients can be small with venous PT. The key is ability to stop sound with jugular compression
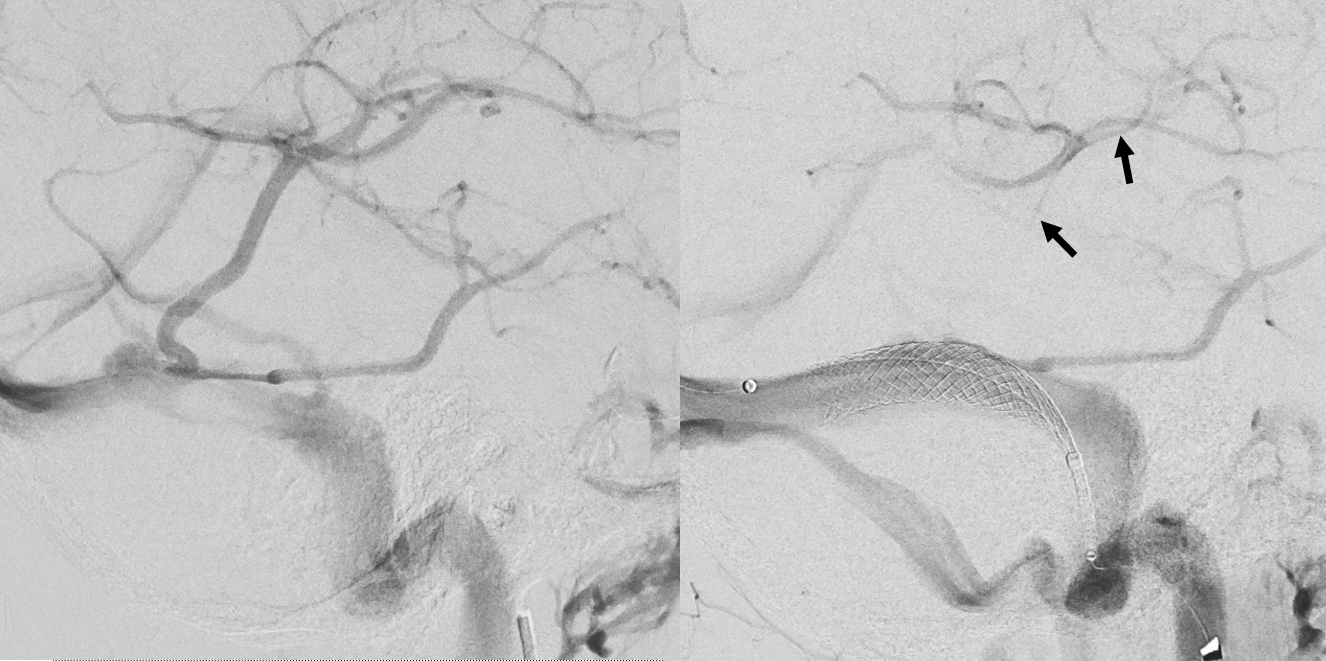
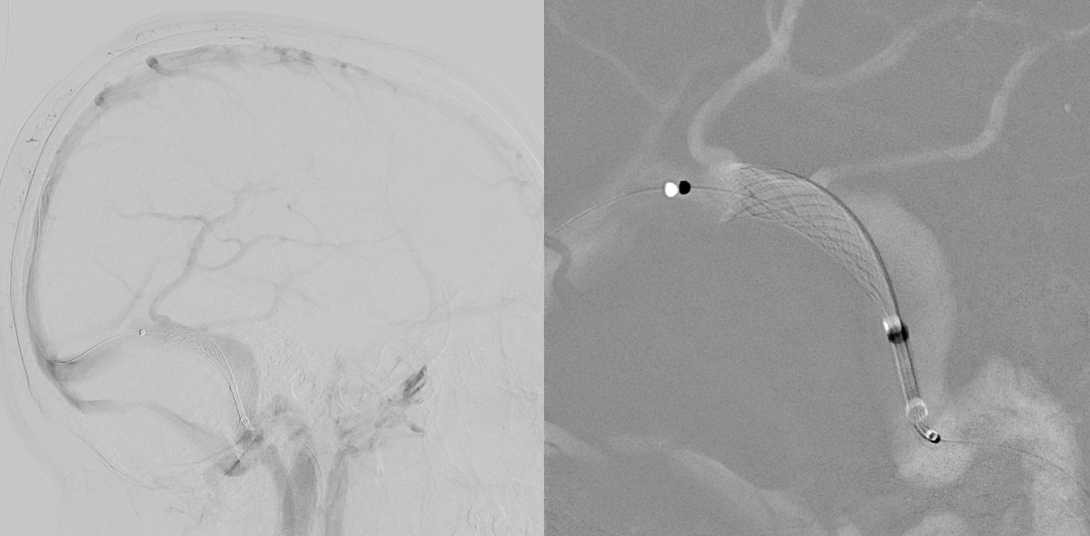
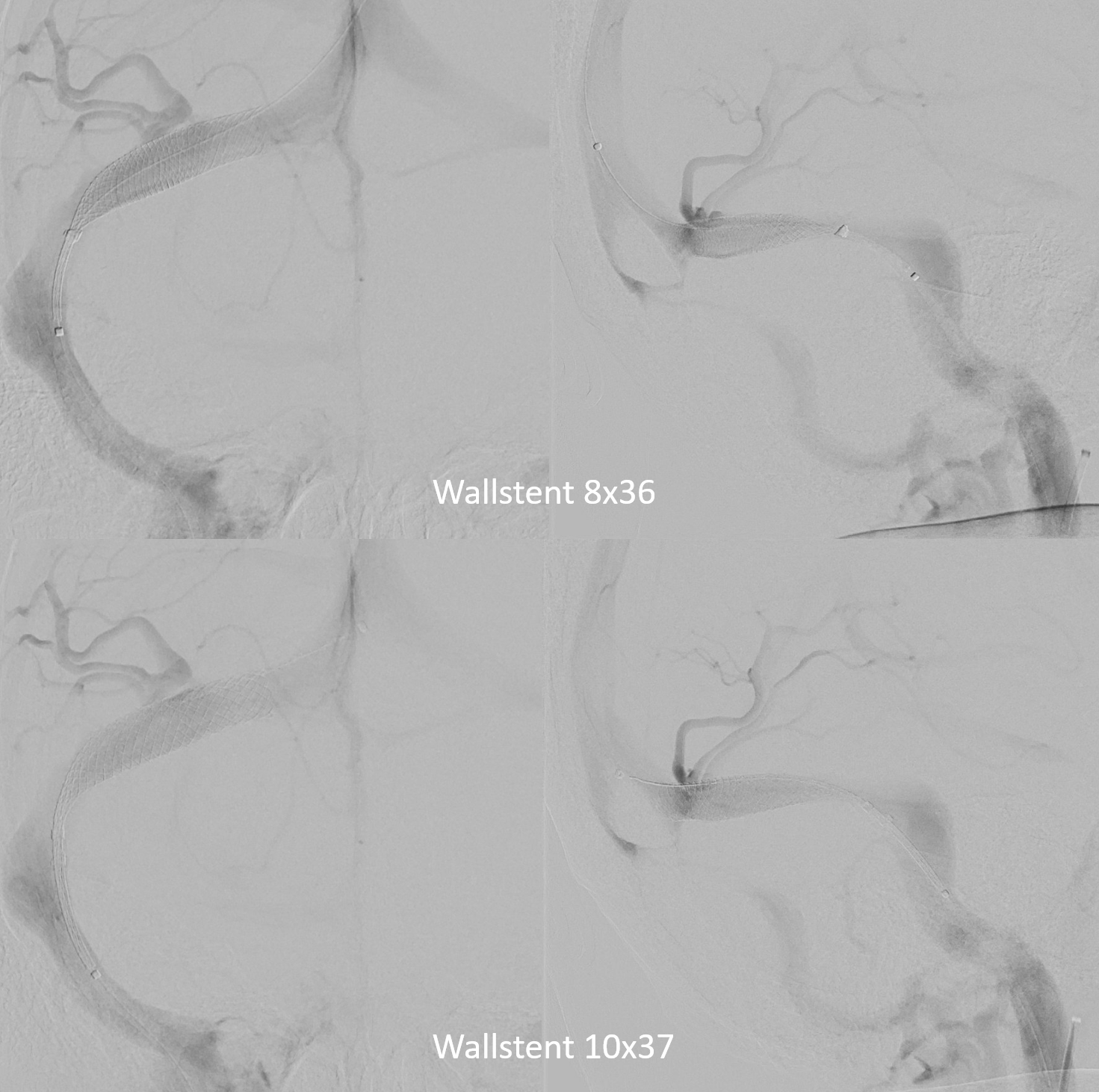
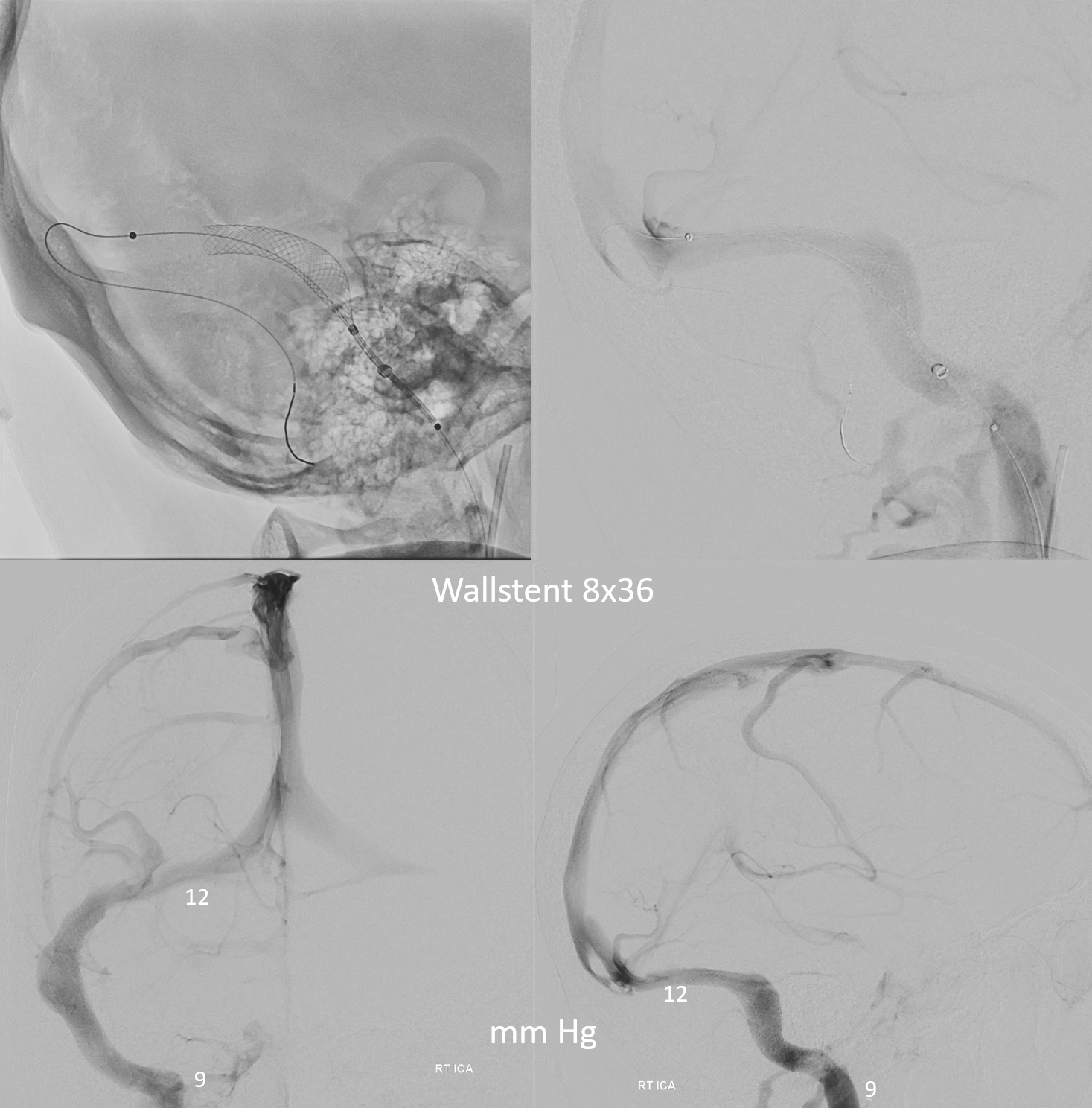
A 10×31 wallstent, partially deployed. Image on left before. Image on right with partial deployment and complete Labbe Occlusion. Unlike laser-cut stents, braided stents should not be undersized or they will foreshorten and create very dense meshes. This sinus measured slightly more than 8 mm in diameter by conventional averaging.
Sequence
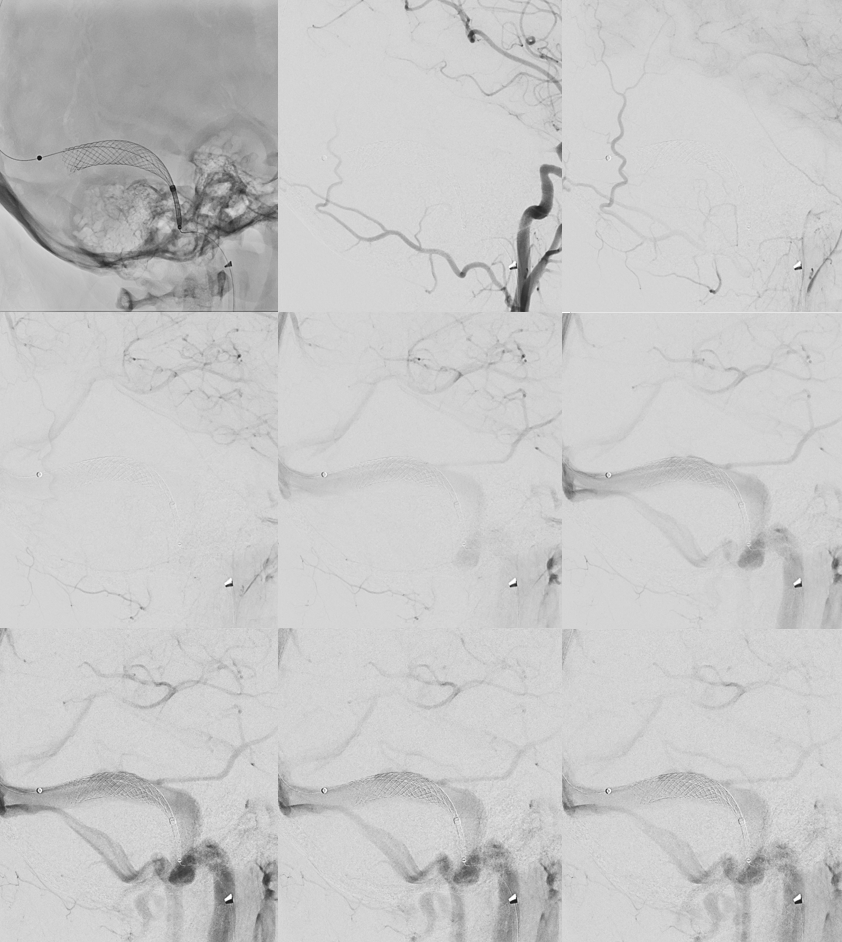
Resheathing the stent reopens the Labbe (bottom left). Re-opening in a slightly different position again leads to problem (bottom right)
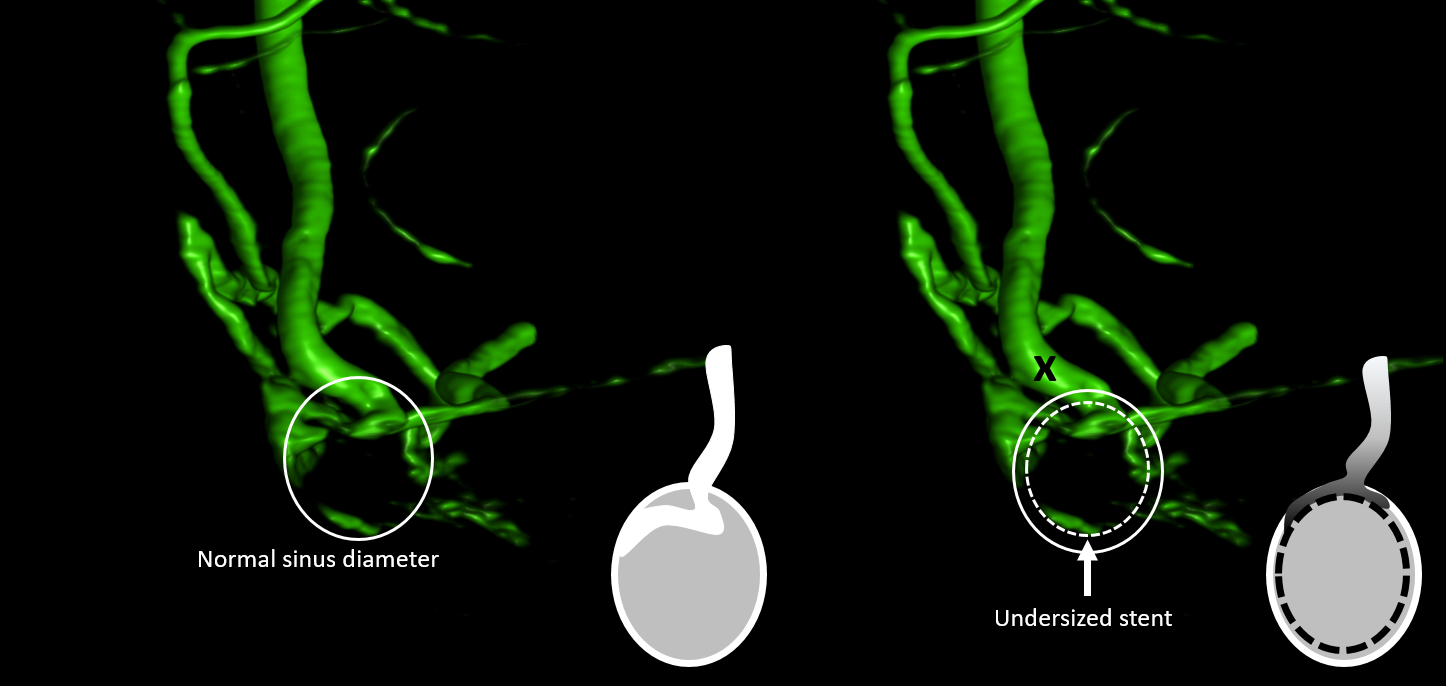
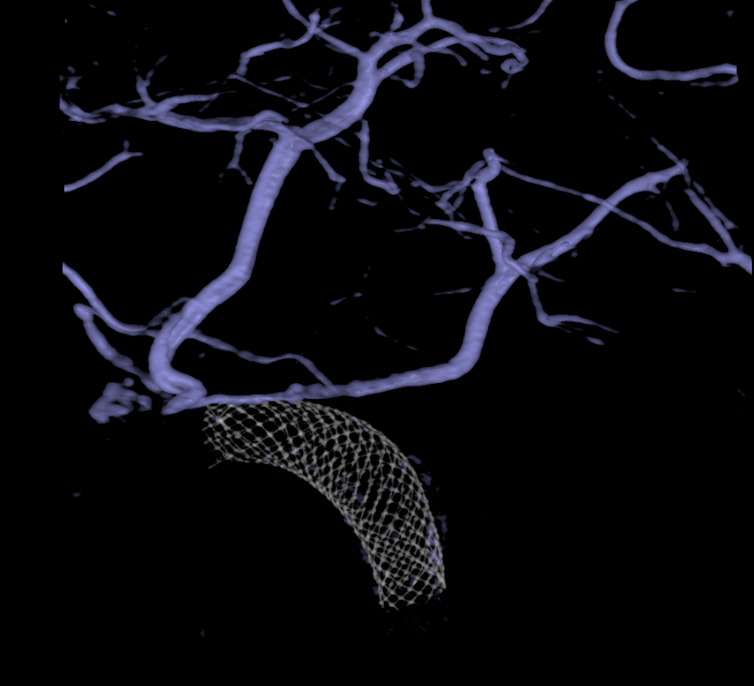
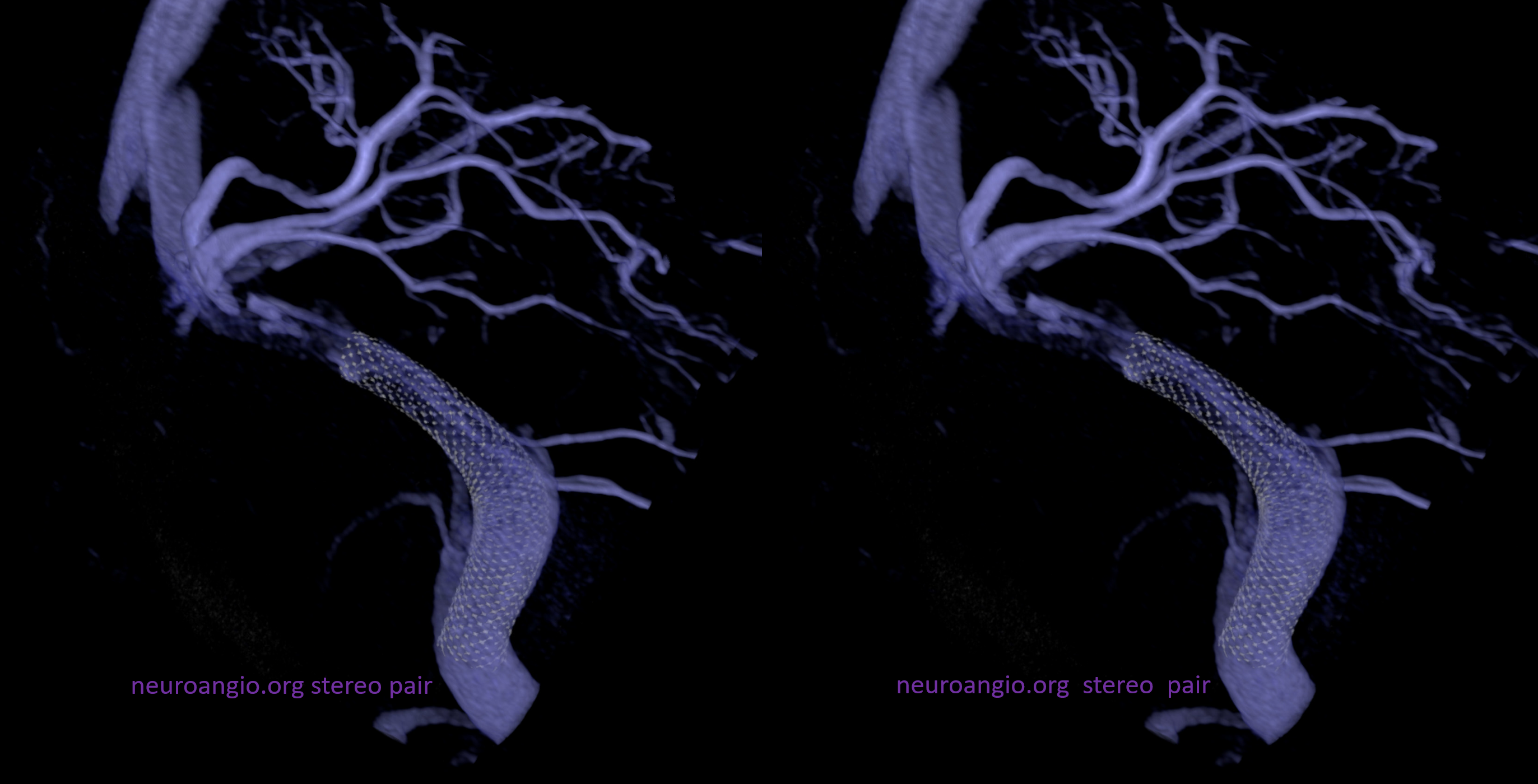
What is the issue? The answer is in high-res DYNA CBCT imaging. The configuration schematic is below. Because Labbe ostium dips into the narrowed sinus, even an undersized stent would have likely caused a problem.
What to do? There are several options. First is to try an 8 mm wallstent. Second is to deploy a 10 mm just proximal to the Labbe. Third, and by far the worst, is to try an (undersized) laser-cut stent and hope for the best. There is no way to remove the laser-cut stent once it is deployed. Dragging it down might be possible, but tearing the sinus/labbe is a possibility.
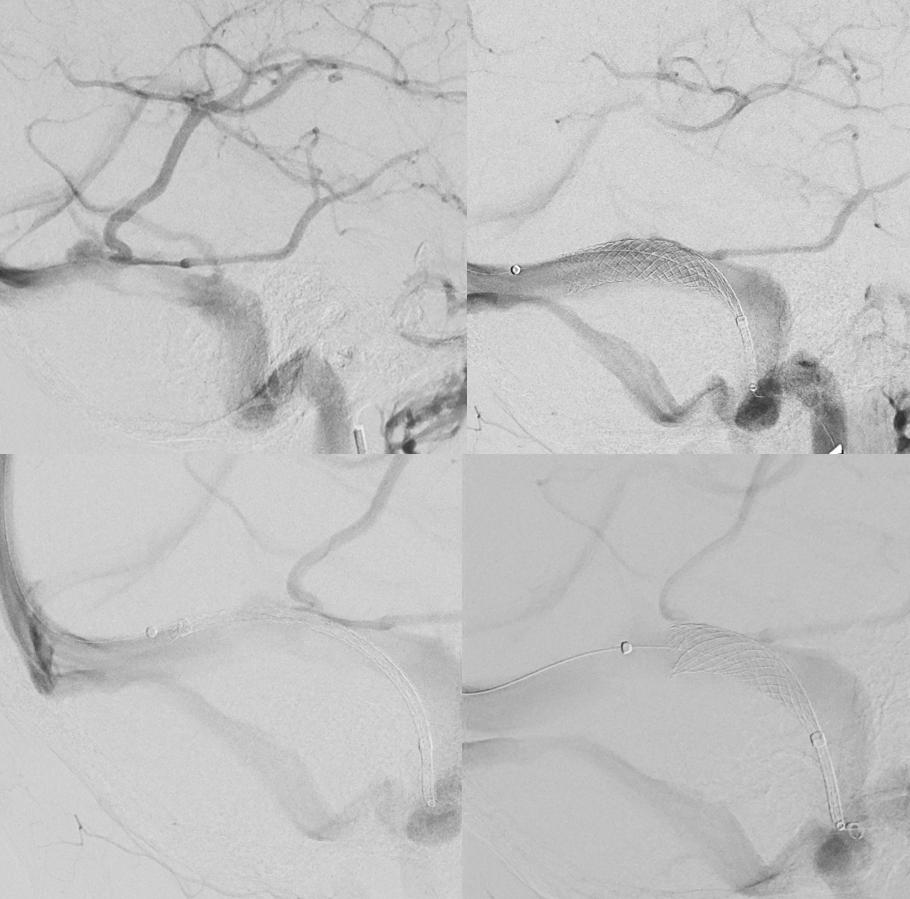
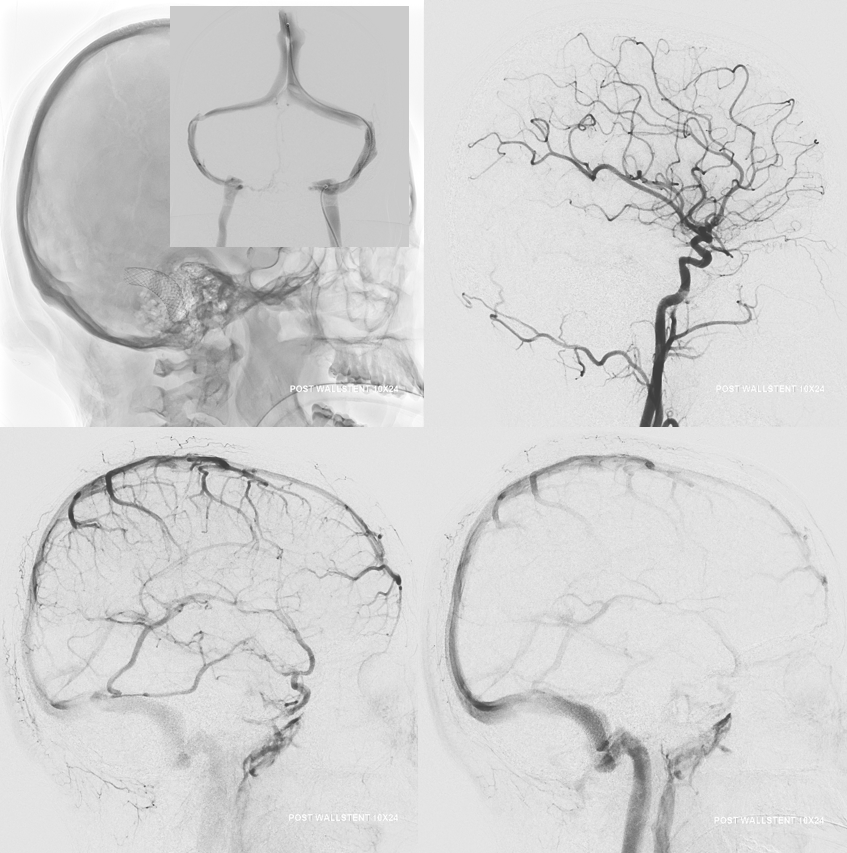
We go with choice 2 — Wallstent 10×24, deployed just proximal to Labbe — below are the images. Labbe is draining now (left image). we actually repositioned the stent even a bit more proximal after these images, as the labbe was a touch late here.
Post deployment image below. The Labbe is open.
There is a residual smaller stenosis. However, this is not an IIH case — its PT. Even small decrease in stenosis can help PT a lot. In this case, the sound is gone
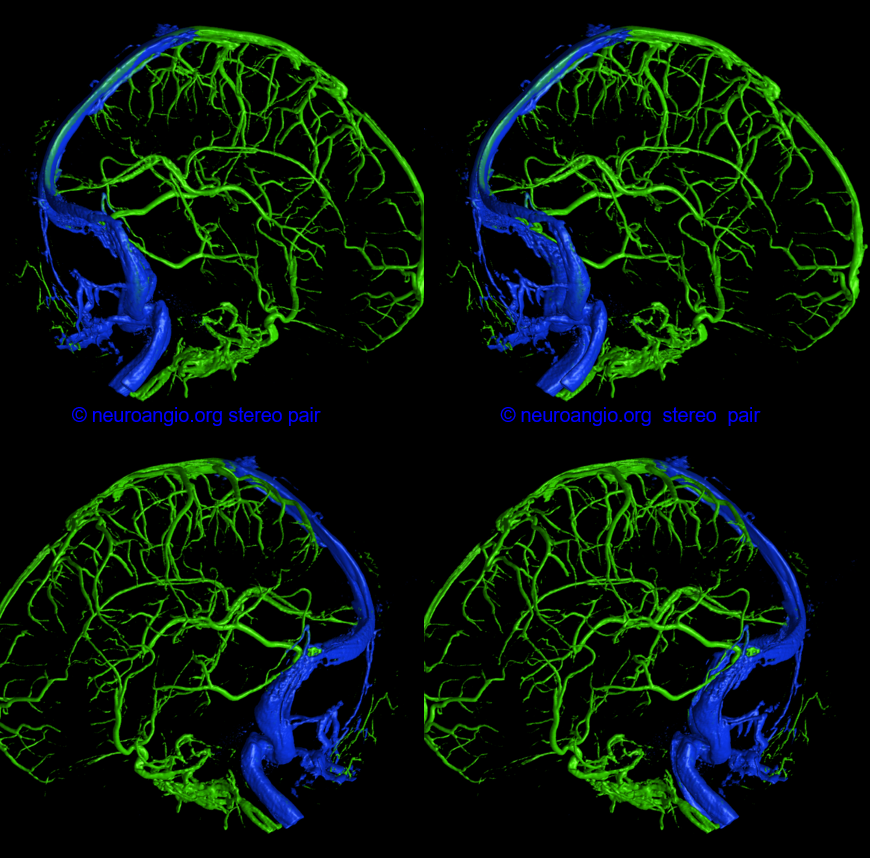
And, below, are some beautiful images, too
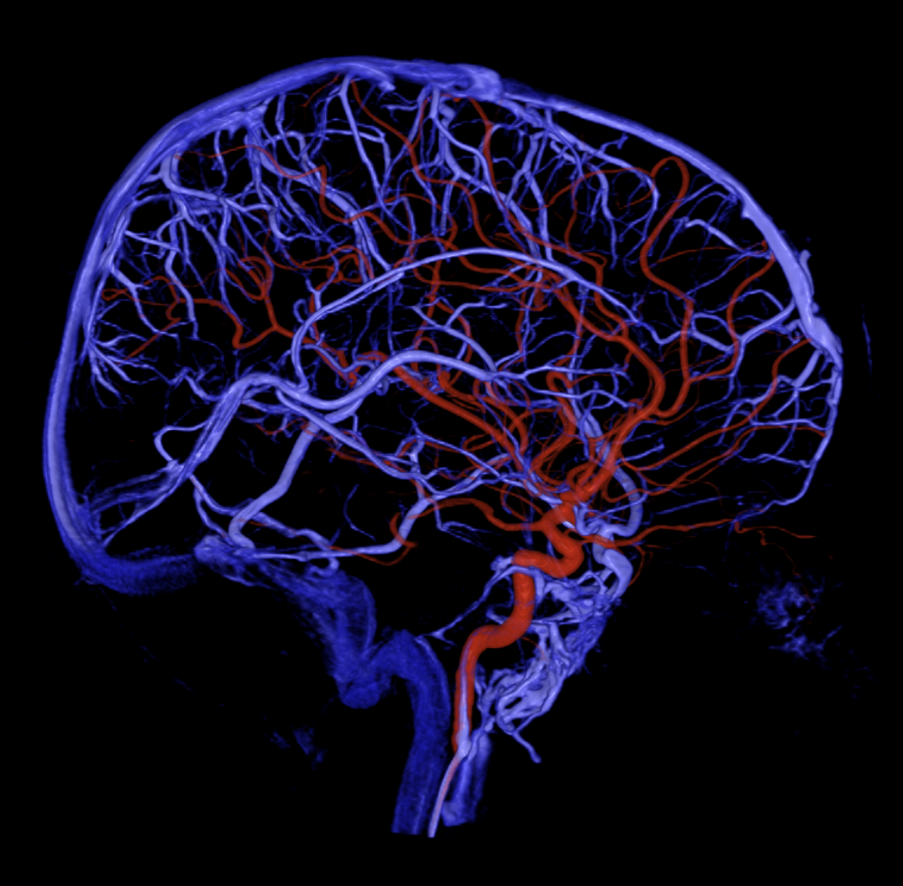
Venous phase arterial injection and venogram overlays
Conclusion — Labbe occlusion is likely a rare thing — less than 1%. However, this one would have gone to venous infarct for sure, since Labbe had no alternative outflow. This is an important point to consider when choosing stents.
SO, not as rare as one might think — another case below
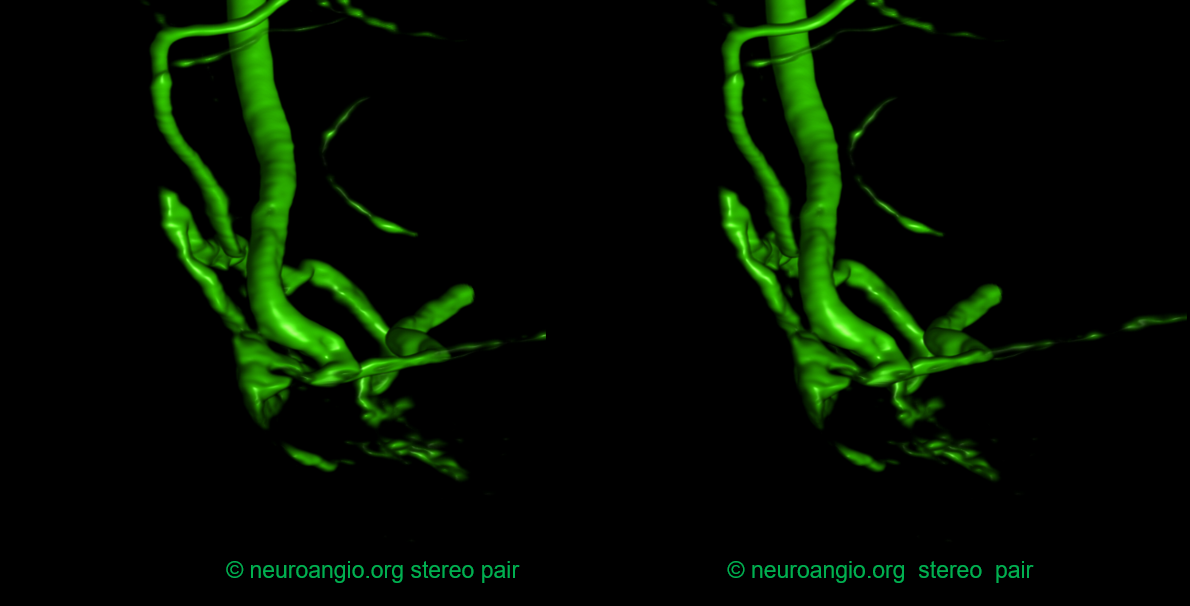
VR
Same case — before sent