
These “collaterals” form the basis of brain’s response to proximal occlusion. Volumes have been written about ischemic response, penumbra, reperfusion, etc etc. In the end, I believe, fundamental concepts are simple concepts. If an MCA branch is occluded, for the affected territory to survive there must be macroscopic compensatory “retrograde” flow by physical connections between the distal MCA territory and its potential saviors — either the PCA or the ACA. The connections are a priori present more in some than others on genetic basis. They can be augmented by flow demand in progressive ischemic conditions. However, for embolic occlusions, we each have what we have.
The other two factors are pressure and vasodilatation, however no amount of pressure or vasodilatation can compensate for absence of actual physical anastomoses.
These can be seen in vivo with Cone Beam CT
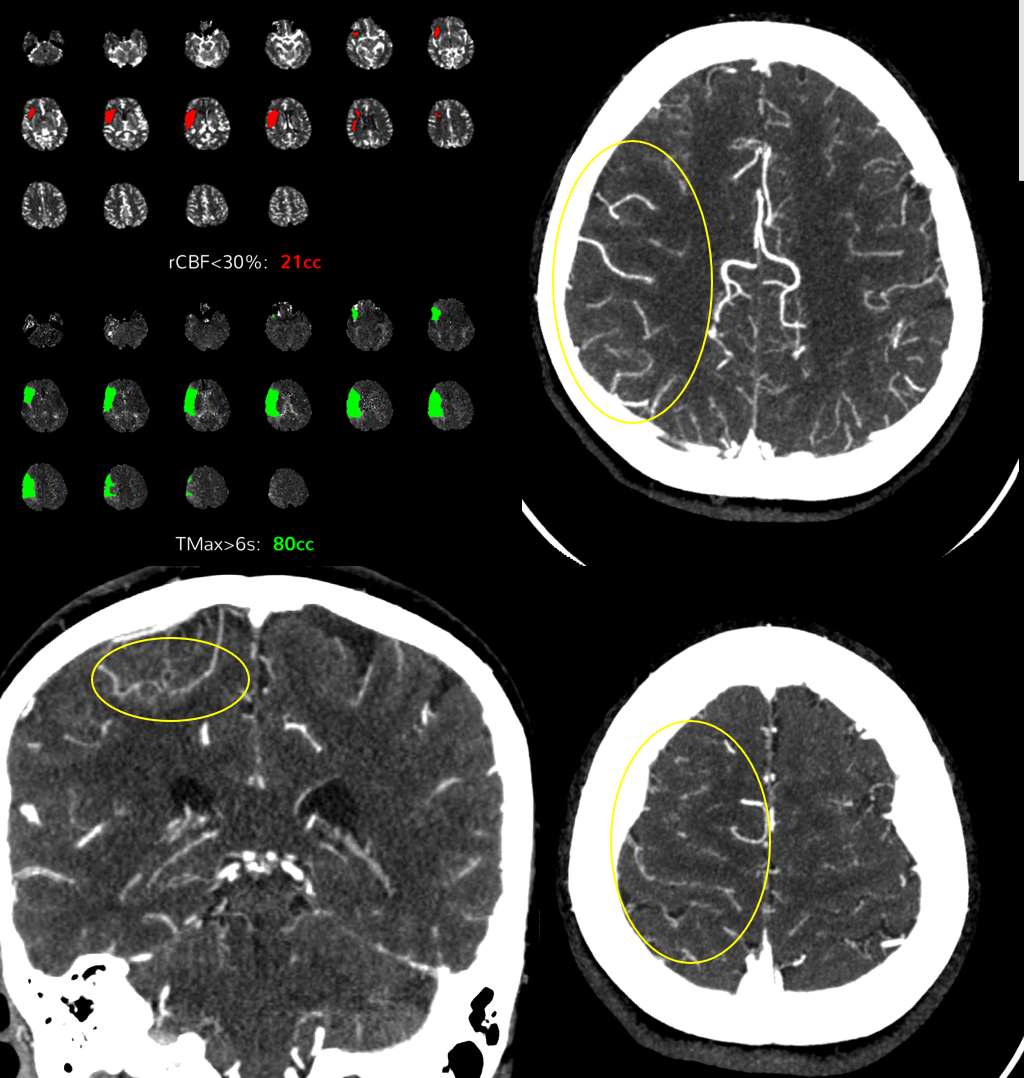
Patient presents with NIHSS = 2. You can see backfilling of MCA on the axial CTA. Note prominence of vessels in the sulci at the physiologic MCA–ACA watershed territory (yellow ovals)
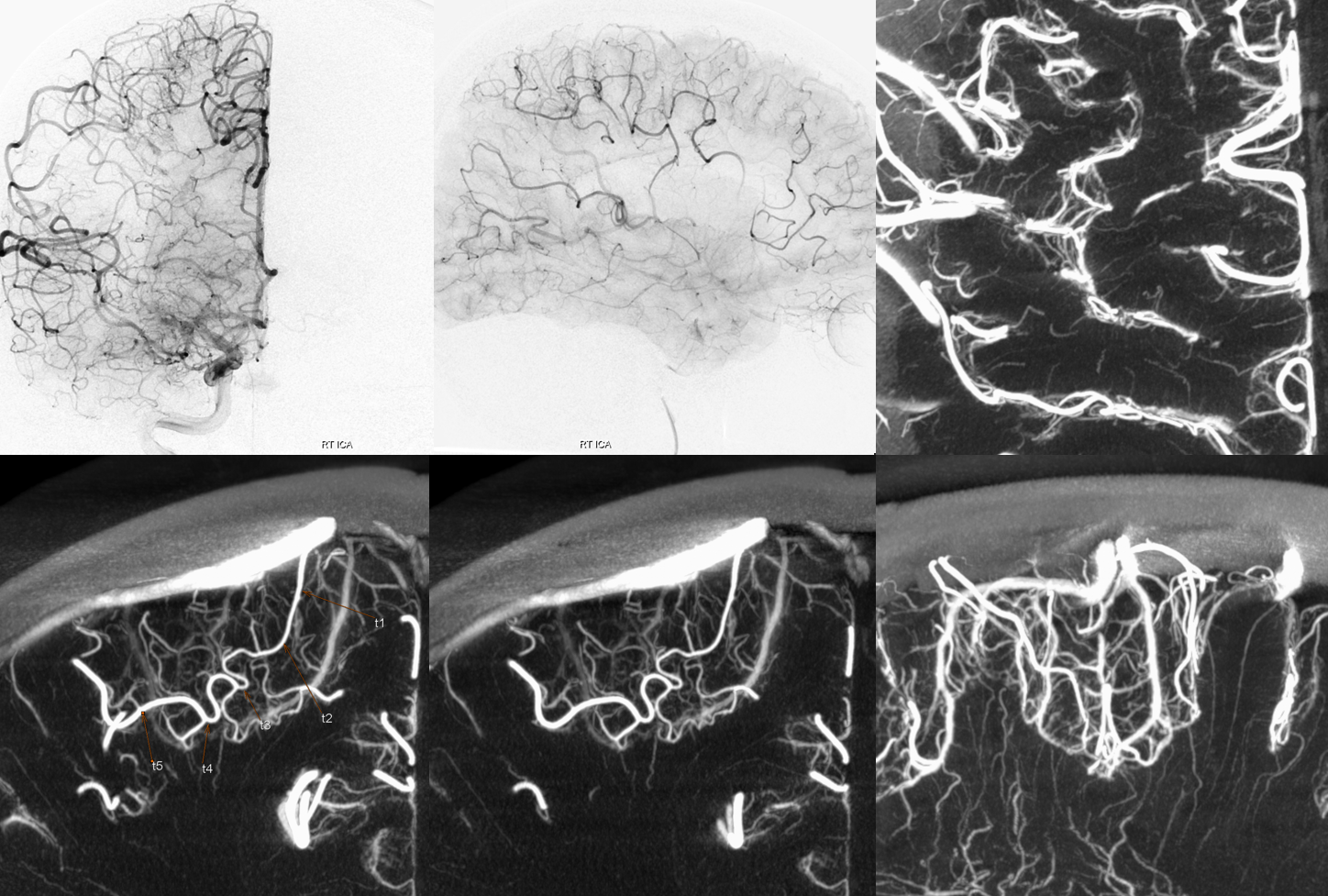
2-D angiographic correlation of excellent “collaterals”.
DYNA CT — 10 second DSA DCT (dual volume) acquisition. FOV = 42 cm (binned) 100% contrast. Injection 3 cc/sec for 39 cc, 3.5 sec delay. You need longer delay to fill the anastomoses well. The connections are usually in the depth of the sulci, not on the surface, as often drawn in cartoons. See the density of sulcal vessels axial view top right. Bottom row — macroscopic connection between ACA and MCA branches. Lower right view is a coronal profile of a sulcus with multiple anastomoses
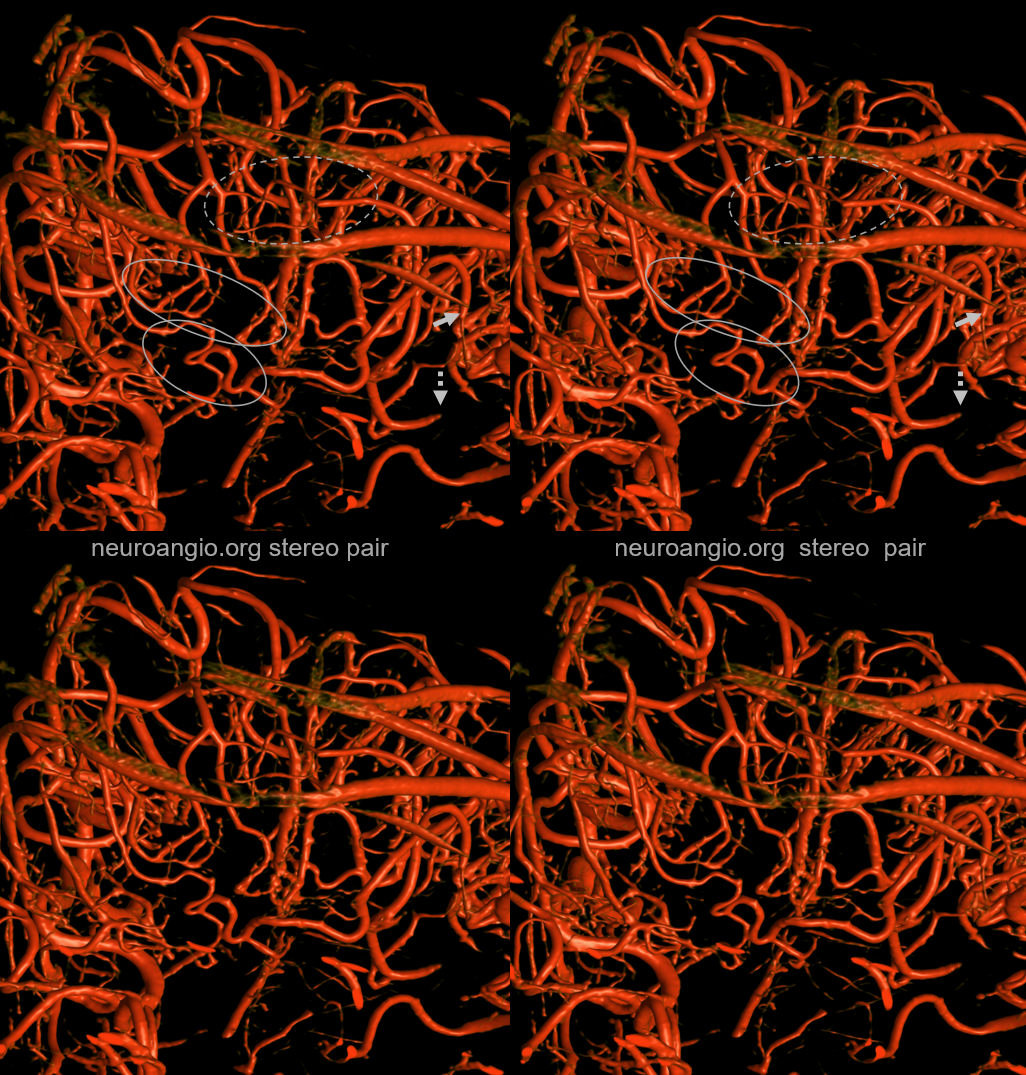
Beautiful volume-rendered stereoscopic views of the above DYNA CT. The two anastomoses outlined by ovals are located in adjacent sulci (ovals). The more macroscopic anastomosis is closer to us, and is supplying a branch which remains occluded at M4 level (arrows) following a TICI 2C M2 thrombectomy. A more anterior (deeper to us) M4 residual occlusion is supplied by a less prominent sulcal anastomosis (dashed ovals). Amazing information like this exists in countless stroke cases.
Below is the rotational angiogram of this acquisition
The original reconstruction is below
A “secondary” reconstruction with 0.17 voxel volume field of view (medium size) and “sharp” image characteristics in the below raw dataset is the basis for all of the above images
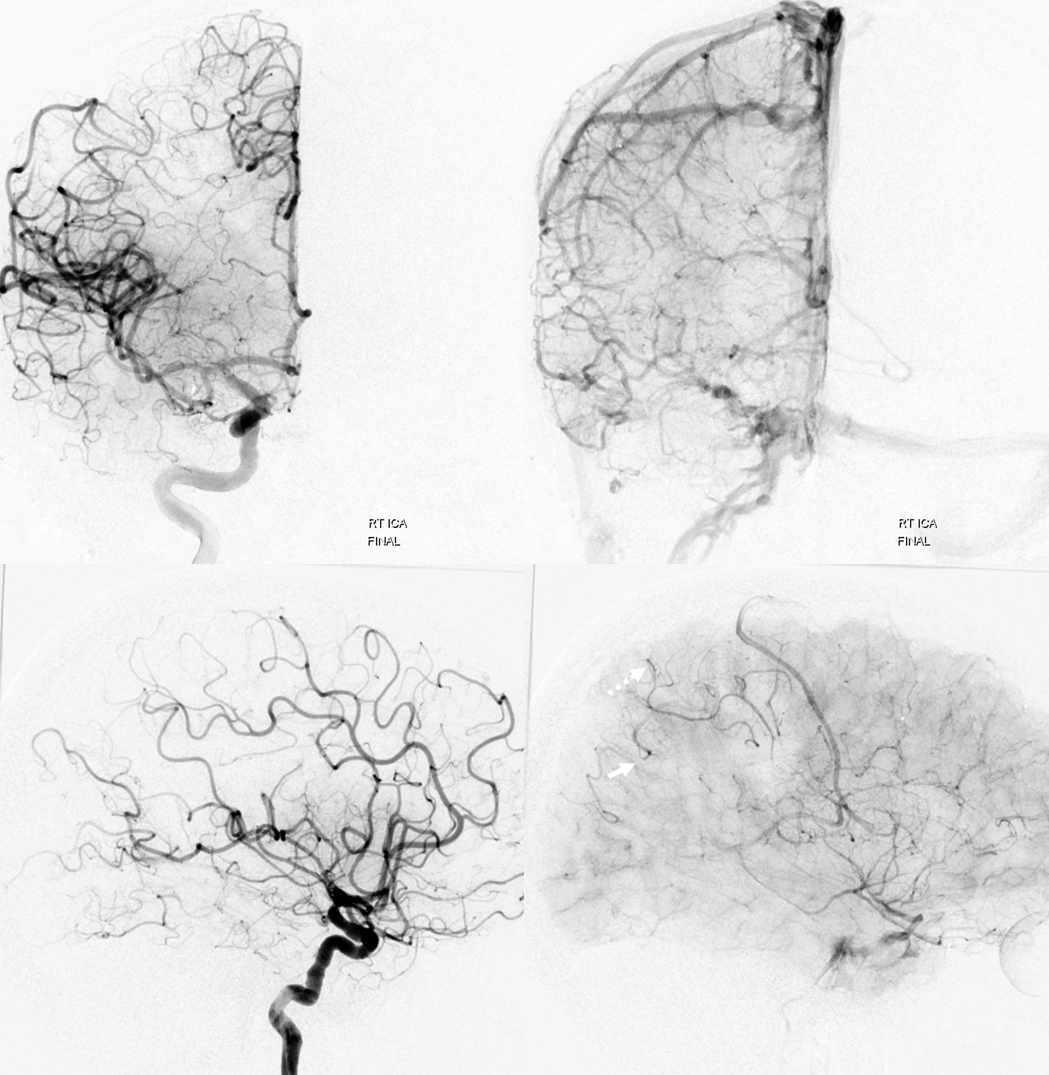
Just to prove that we reopened the artery… The arrow points to the residual occlusion branch associated with the macroscopic anastomosis seen above. A few smaller M4 parietal branches are also retrogradely reconstituted, one of which (dashed arrow) corresponds to the dashed ovals in the VR stereo image
Cone Beam CT — its not all about AVMs and aneurysms and dural fistulas.
Back to Principles of CBCT Page