Anterior Choroidal Artery
Embryology (abbreviated)
For a fuller discussion, see dedicated neuroembryology section. For a masterful description, consult Lasjaunias and Berenstein’s work “Surgical Neuroembryology”, either 1st edition volume 3 or 2nd edition volume 1.
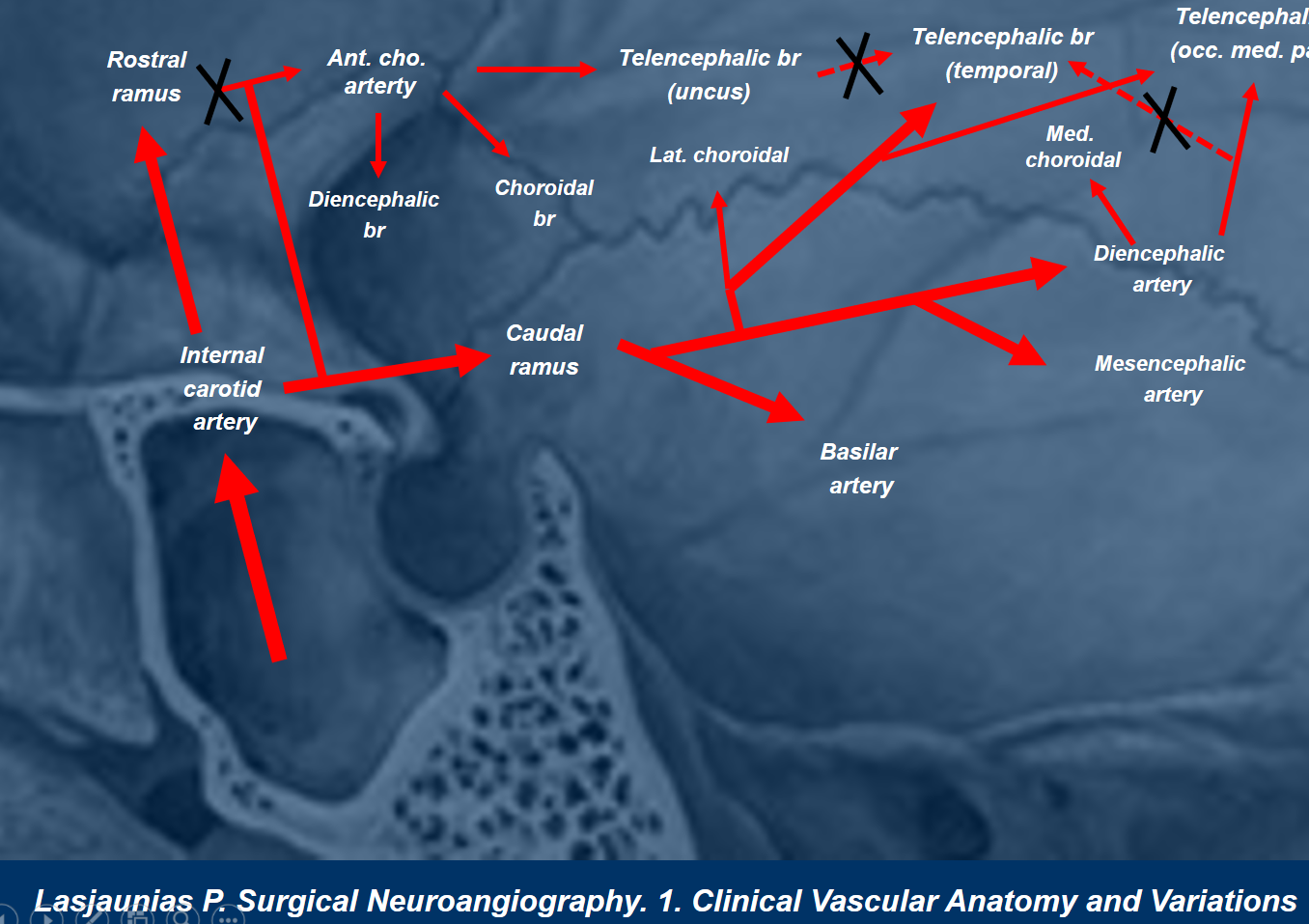
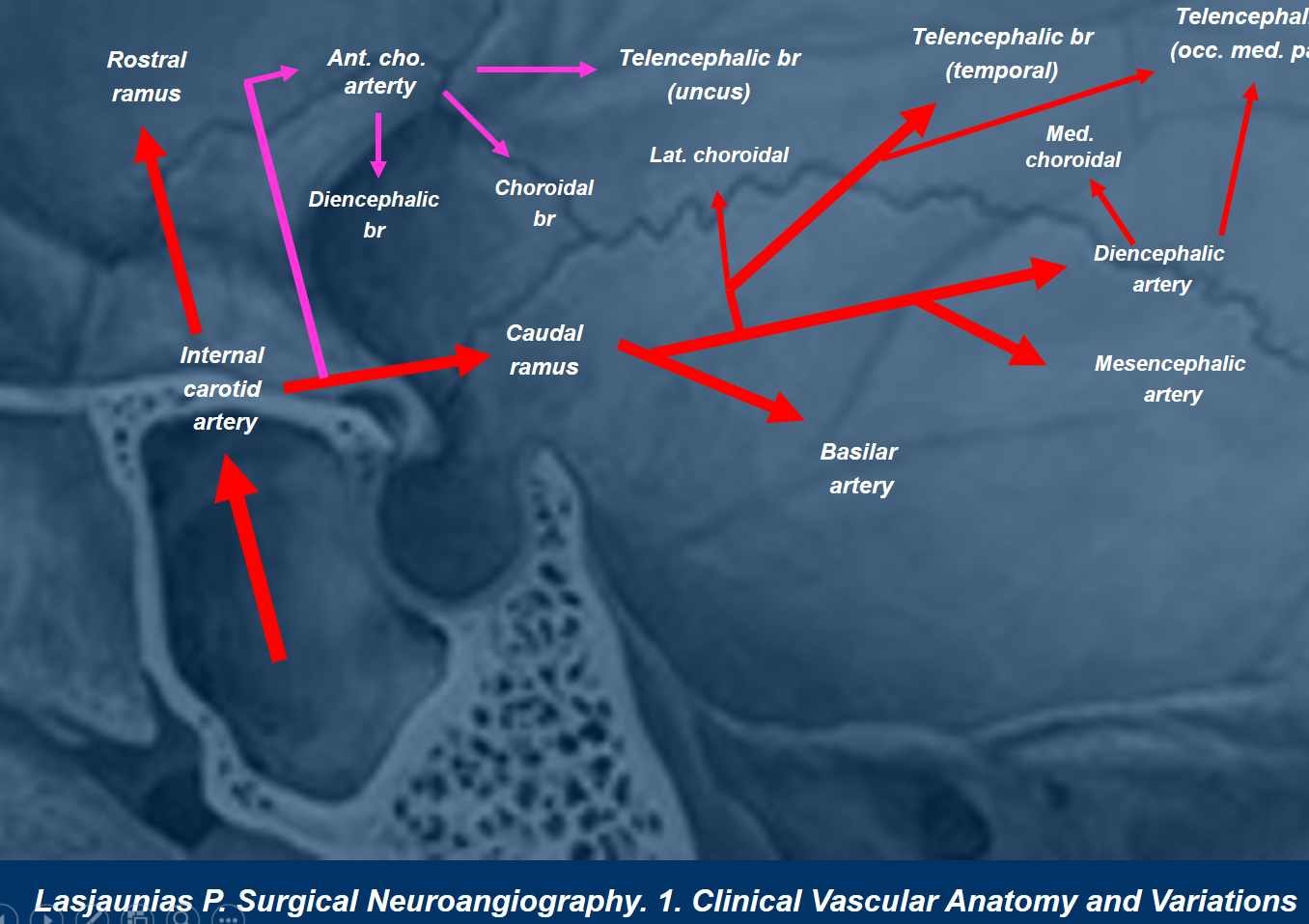
The anterior choroidal artery is almost as old as hills. Phylogenetically, its homologs (recorded under various confusing names in dissections of “lower” species) are already well developed in fishes and continue into amphibians and mammals. In these species, it supplies the ever enlarging posterior hemispheres, in effect vascularizing the territory of the posterior cerebral artery in the human. This is because the posterior circulation does not begin to supply “supratentorial brain” until late in evolution when (probably) growing volume of the brain places increasing demand on additional vascular supply sources. As the posterior cerebral artery is annexed by the vertebrobasilar system in relatively advanced mammals, the role of the anterior choroidal artery in hemispheric supply diminishes.
In the human embryo, the anterior choroidal is quite prominent at the “choroidal” stage of development (roughly 5 weeks or so) when the vertebrobasilar system has not yet come to be and the carotid artery supplies almost the entire brain, including upper brainstem. As the hemispheres grow, the volume of brain supplied by the anterior choroidal diminishes in favor of the posterior cerebral artery. This explains why in some individuals the anterior choroidal artery retains portions of cortical PCA territory (see below). This has led to numerous erroneous angiographic and surgical reports of “duplicated PCA” based on appearance of two large vessels coming off the distal ICA. Likewise, perforator vessels can come from either proximal choroidal or just distal to it, from the ICA proper. It is critical to understand that this, too, is an error — there is only one PCOM, and only one anterior choroidal possible — choroidal being the vessel that supplies choroid plexus. However, even in its “normal” relatively small state, the anterior choroidal enjoys importance far out of proportion to its size.
Cross-sectional Imaging
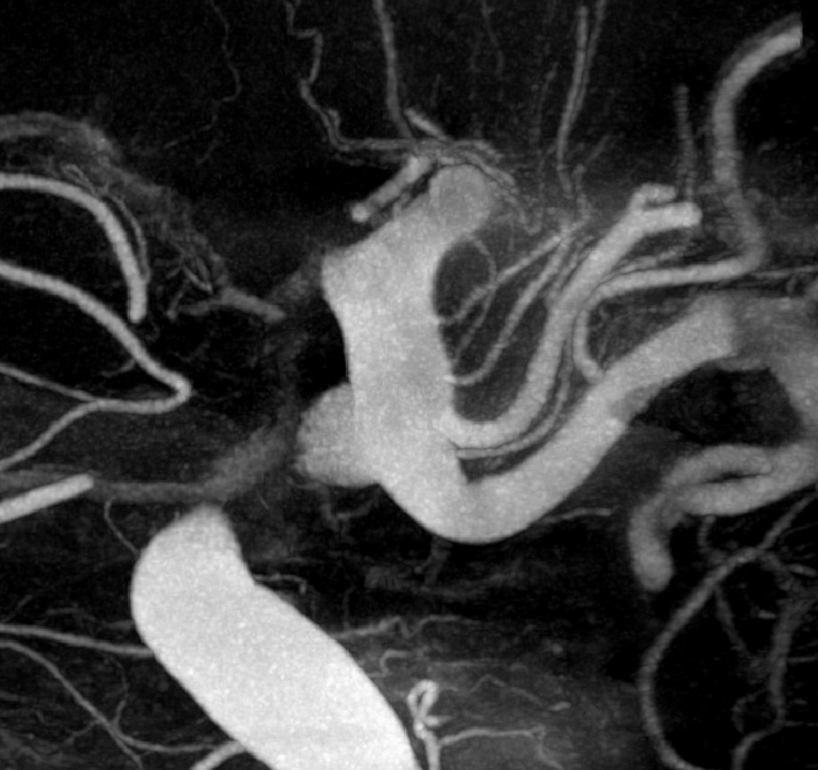
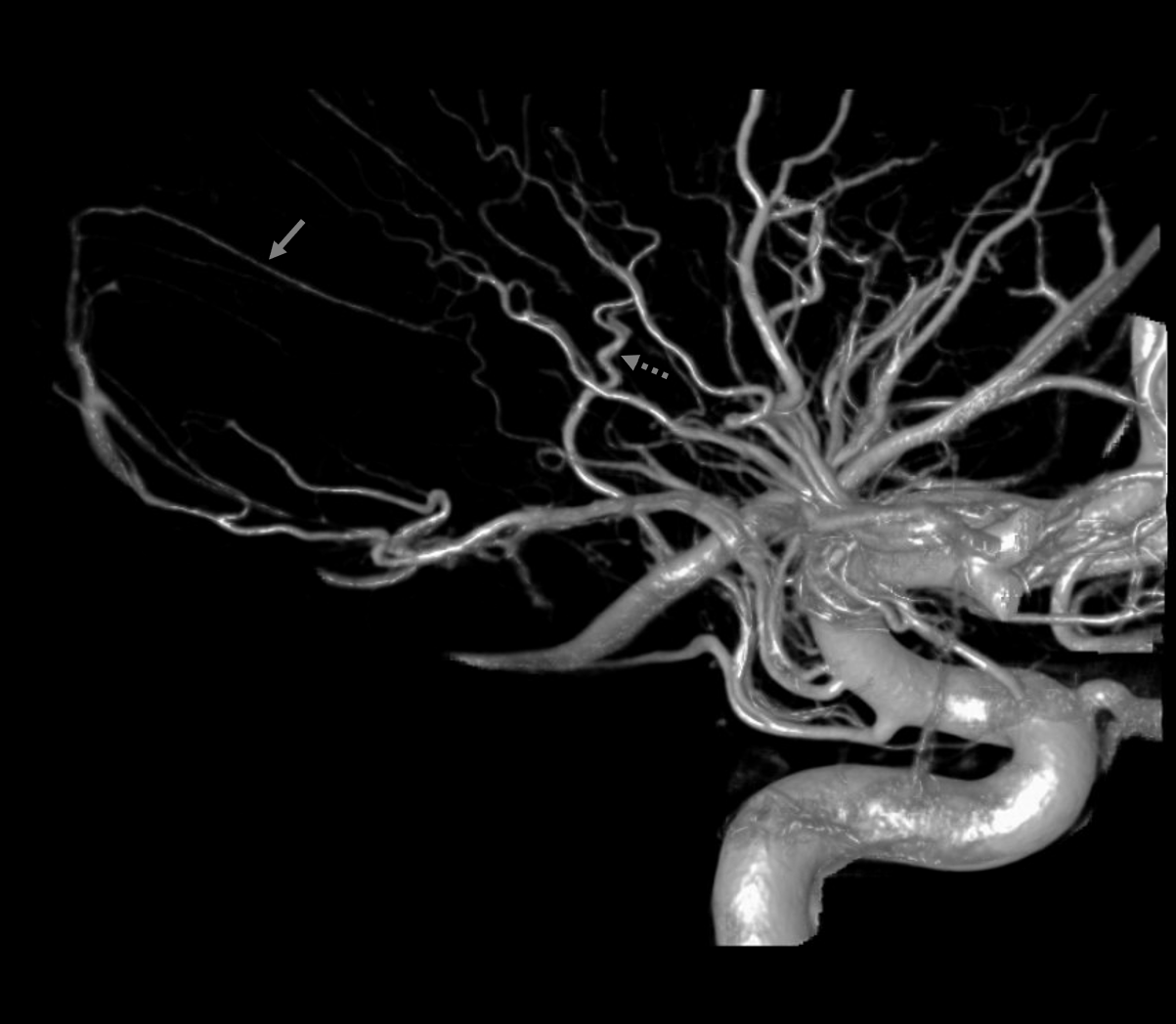
The A. Chor. ostium is usually seen on 1.5T MRA, but the rest of the vessel is seldom visualized unless significant pathology exists to enlarge it. In contrast, both cisternal and choroidal portions of normal-size anterior choroidal arteries are nearly always on 3T MRA. All of these studies have to be of high quality.
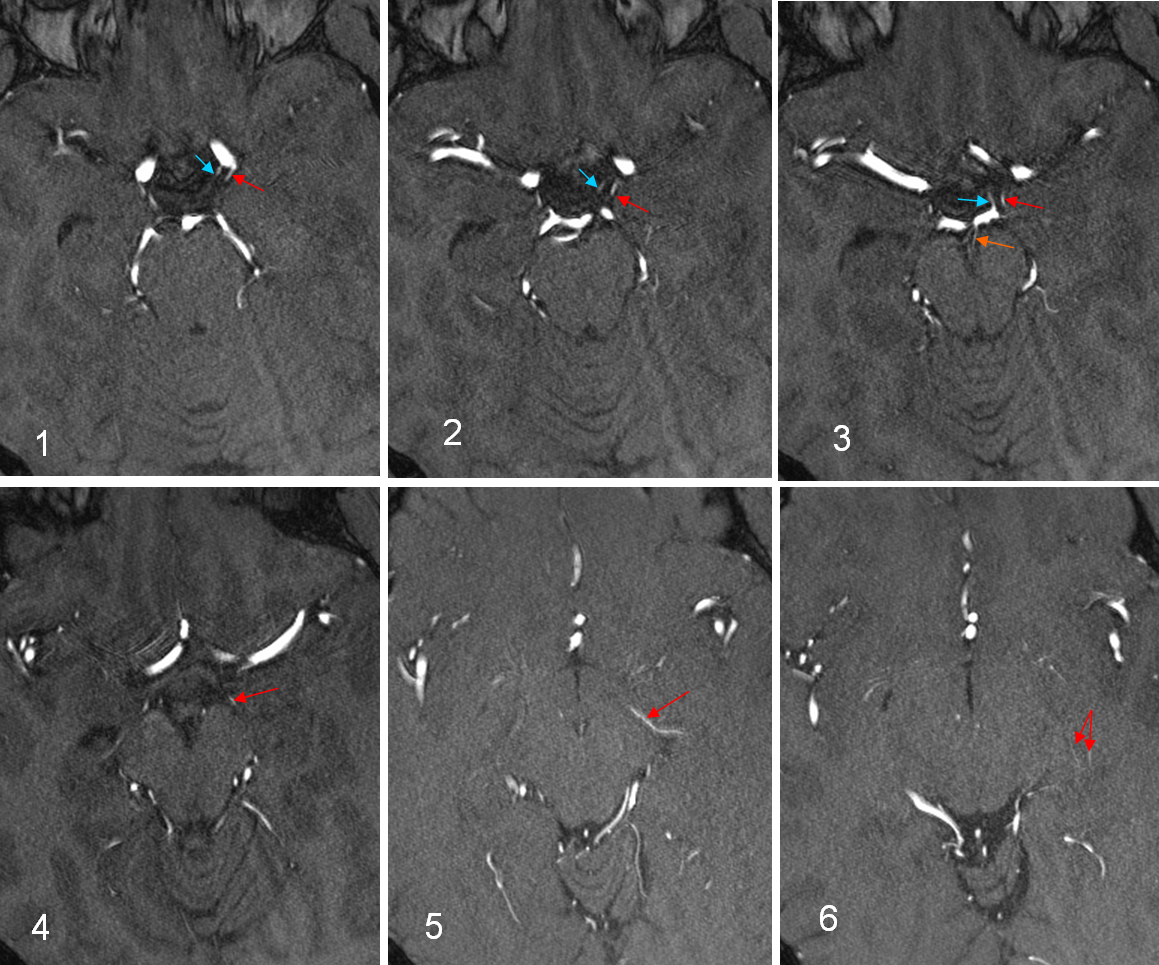
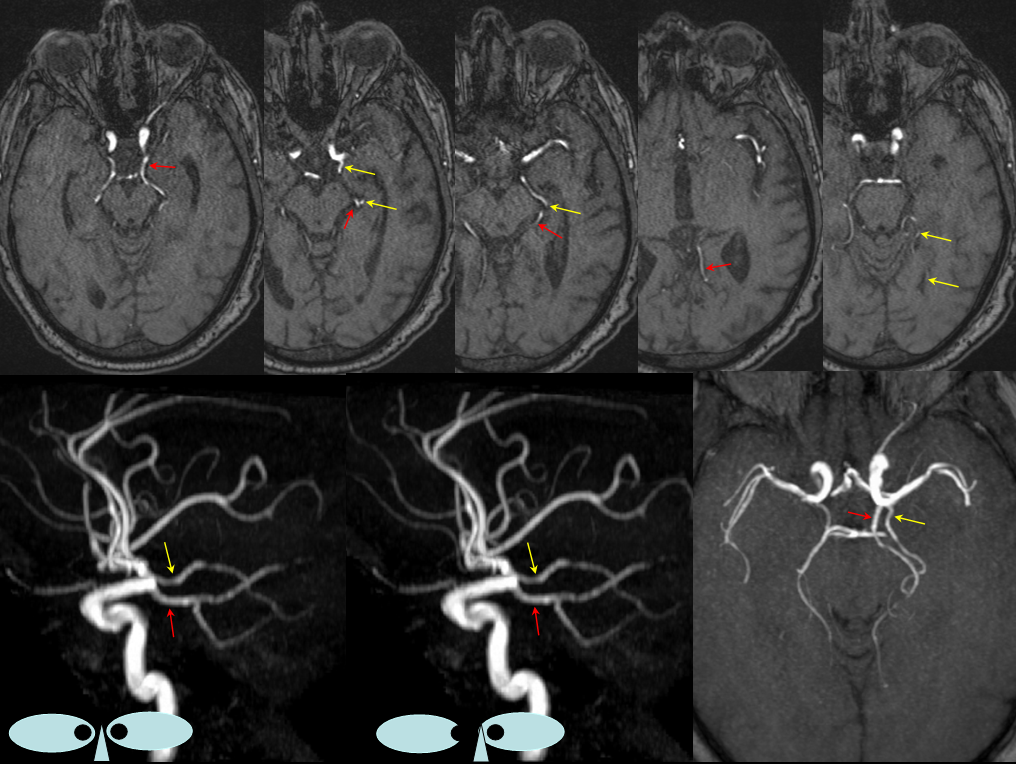
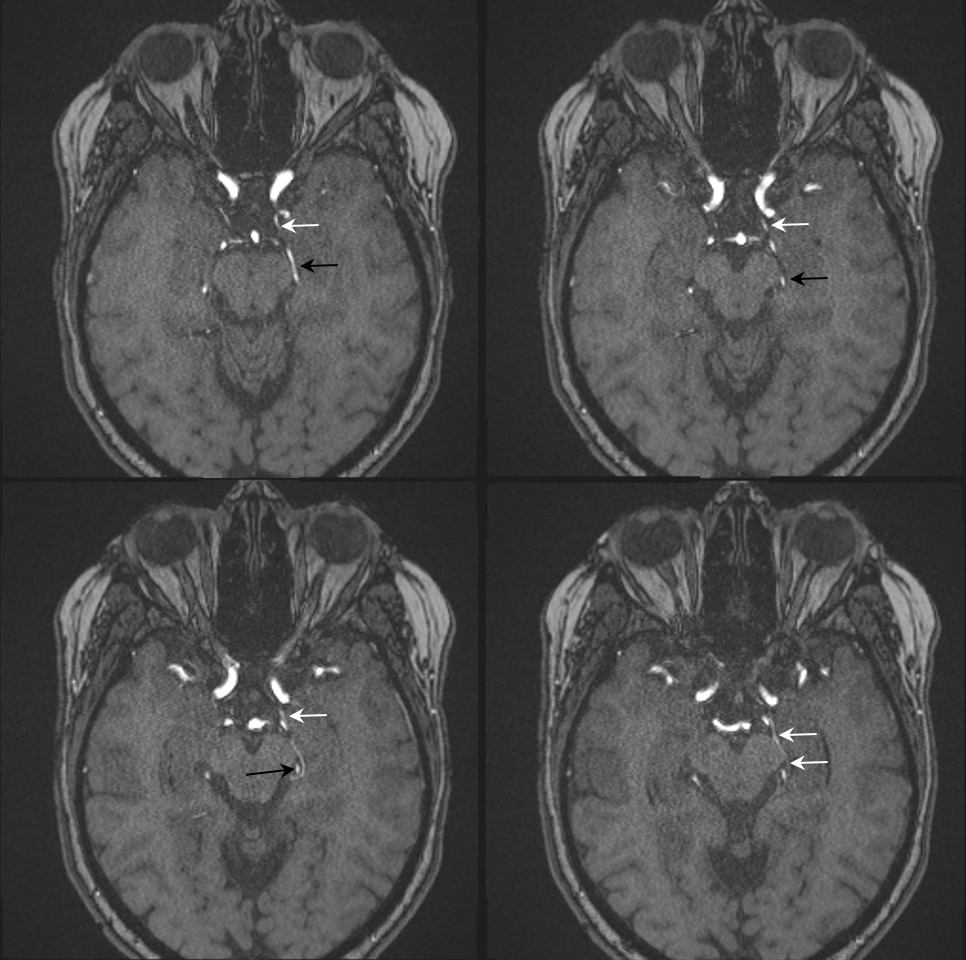
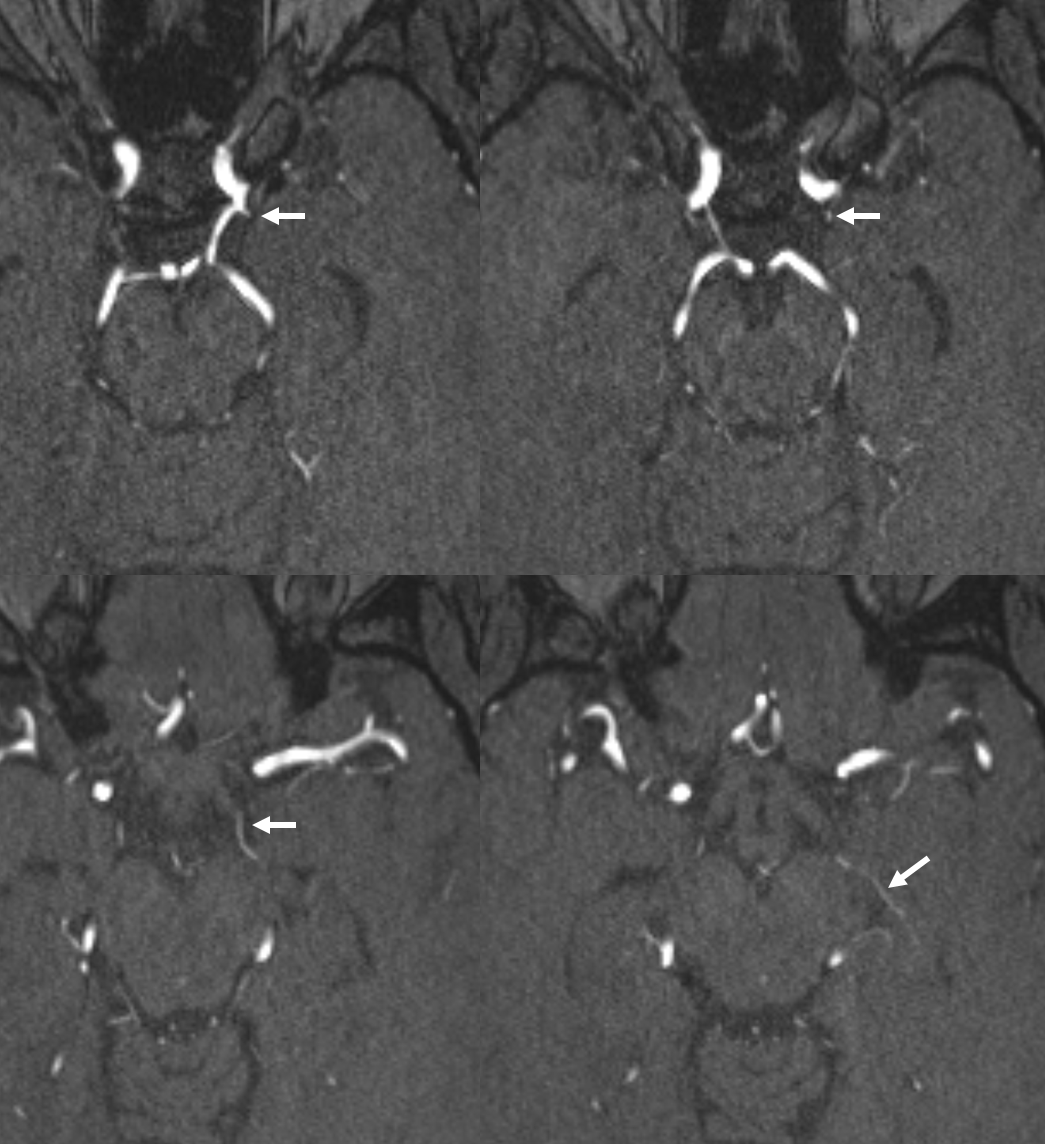
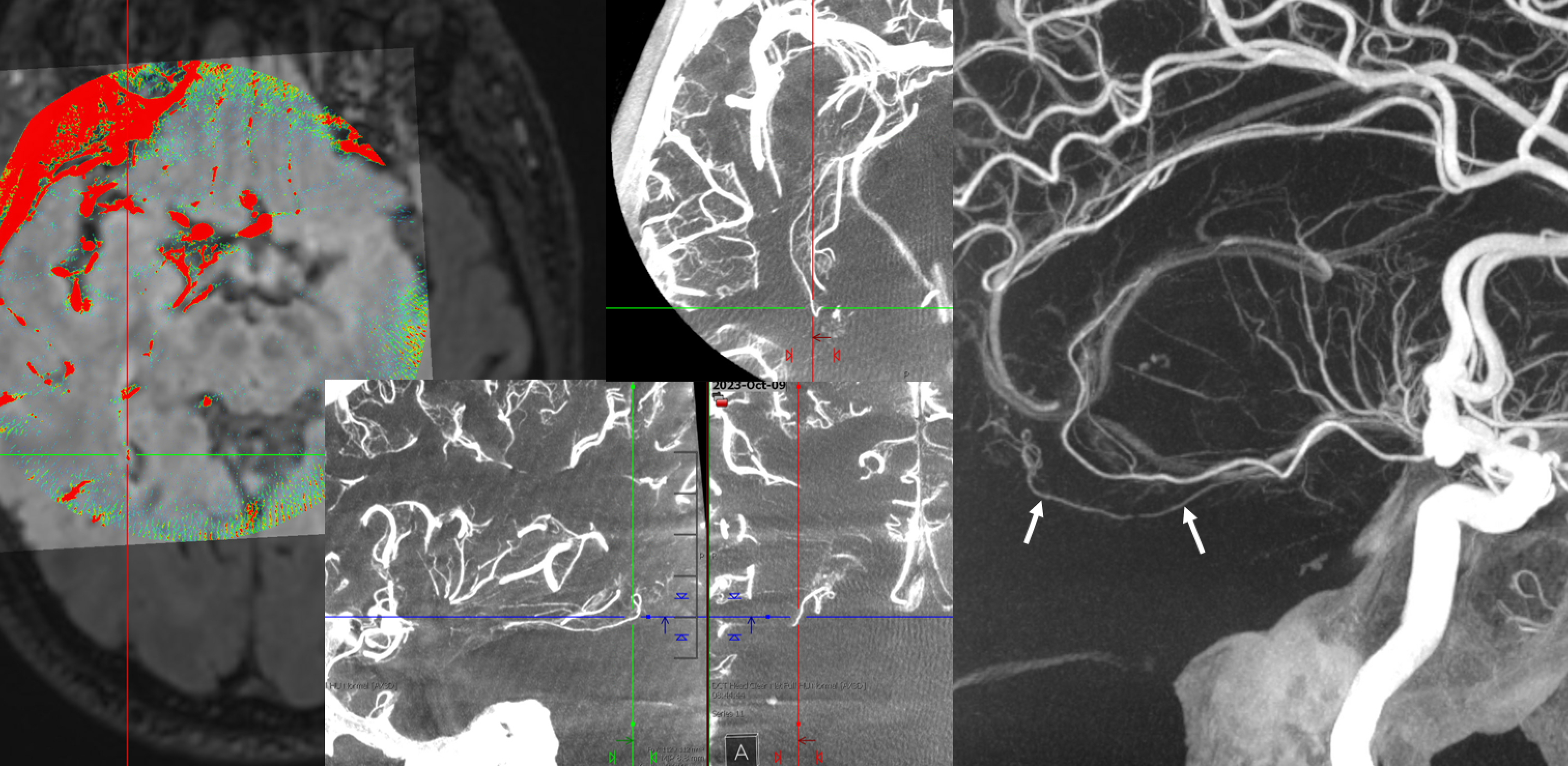
3-Tesla MRA of normal anterior choroidal arteries (red)
1) Ostium of the A Choroidal artery lateral and distal to the PCOM (blue)
2) Cisternal portion of the A Chor.
3) Lateral course in the perimesencephalic cistern at level of PCOM / PCA confluence. Even medial choroidal artery (orange) can be seen on a 3-T
4) Entrance into the choroidal fissure
5) In the choroidal fissure, in plane of scan
6) Branching to feed choroid plexus
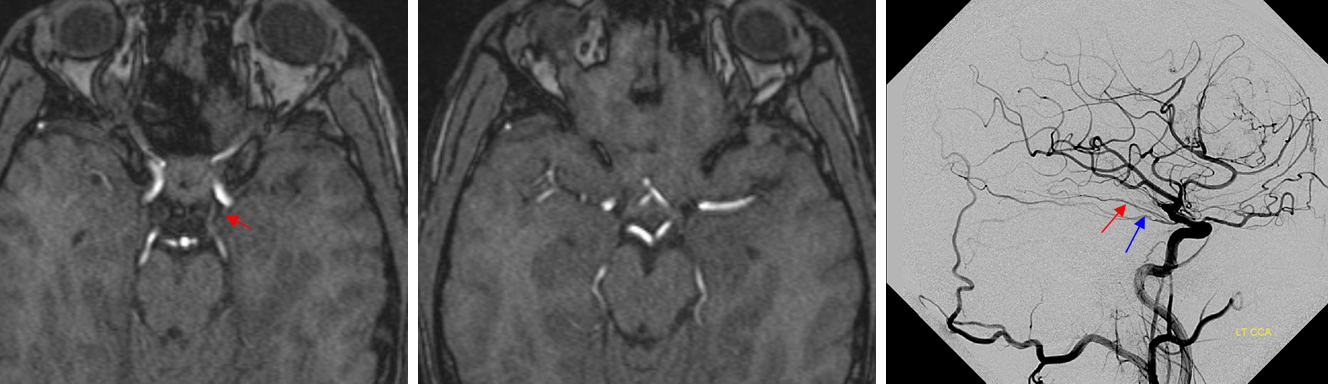
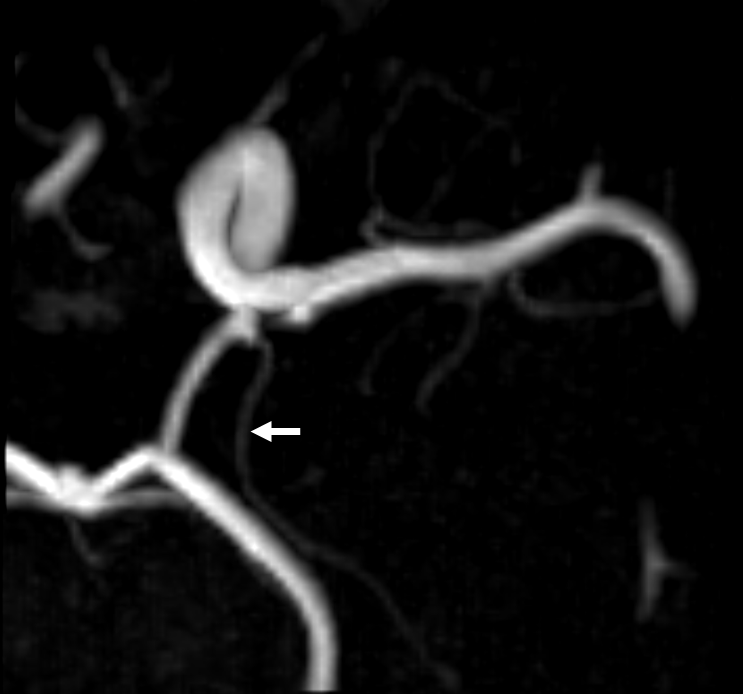
In contrast to 3T, the 1.5T MRA below only shows an ostium of what is in fact a very prominent anterior choroidal artery (red), as seen on angio of the same patient. Poor visualization is to some extent related to direction of Anterior Choroidal flow, which can be close to plane of MRA slab.
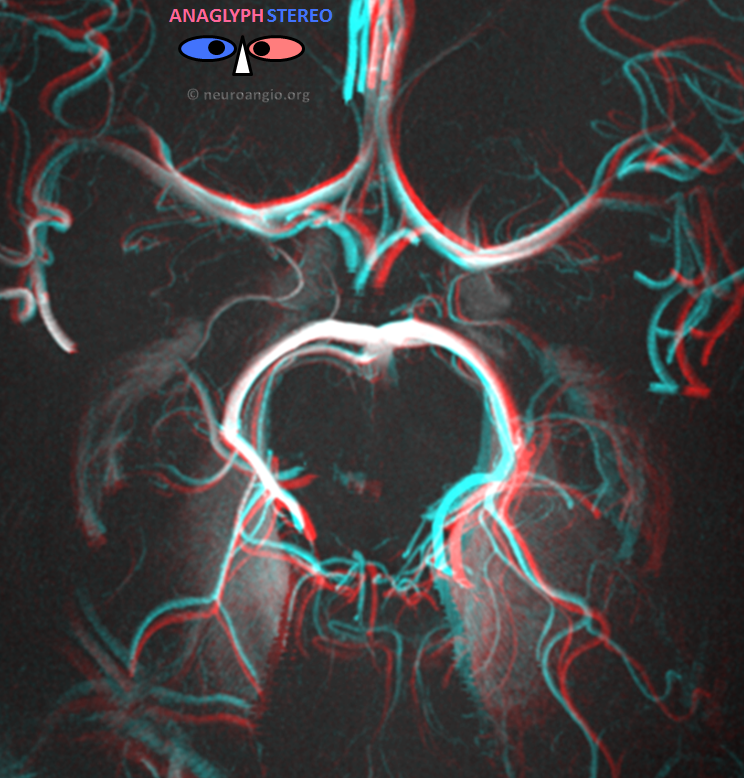
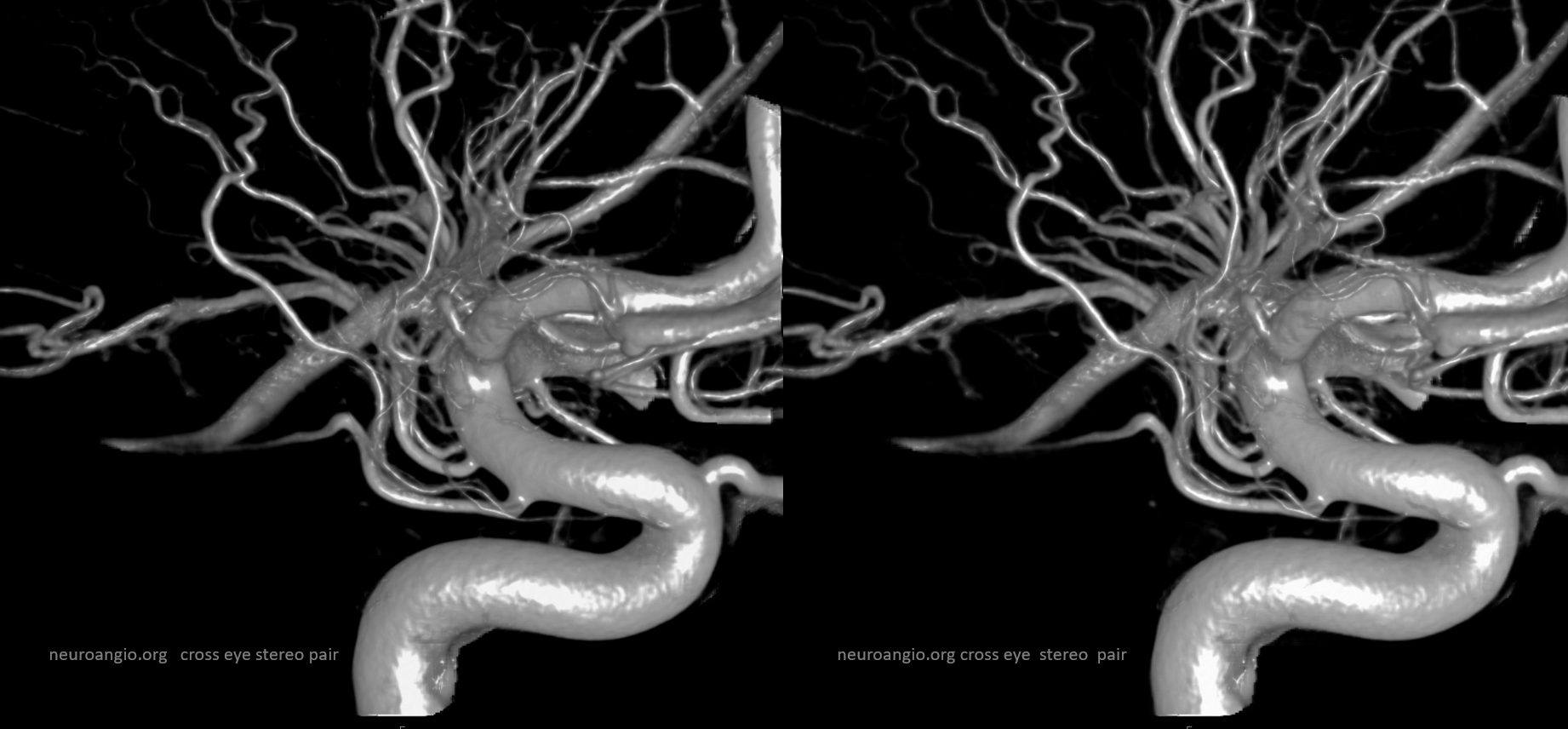
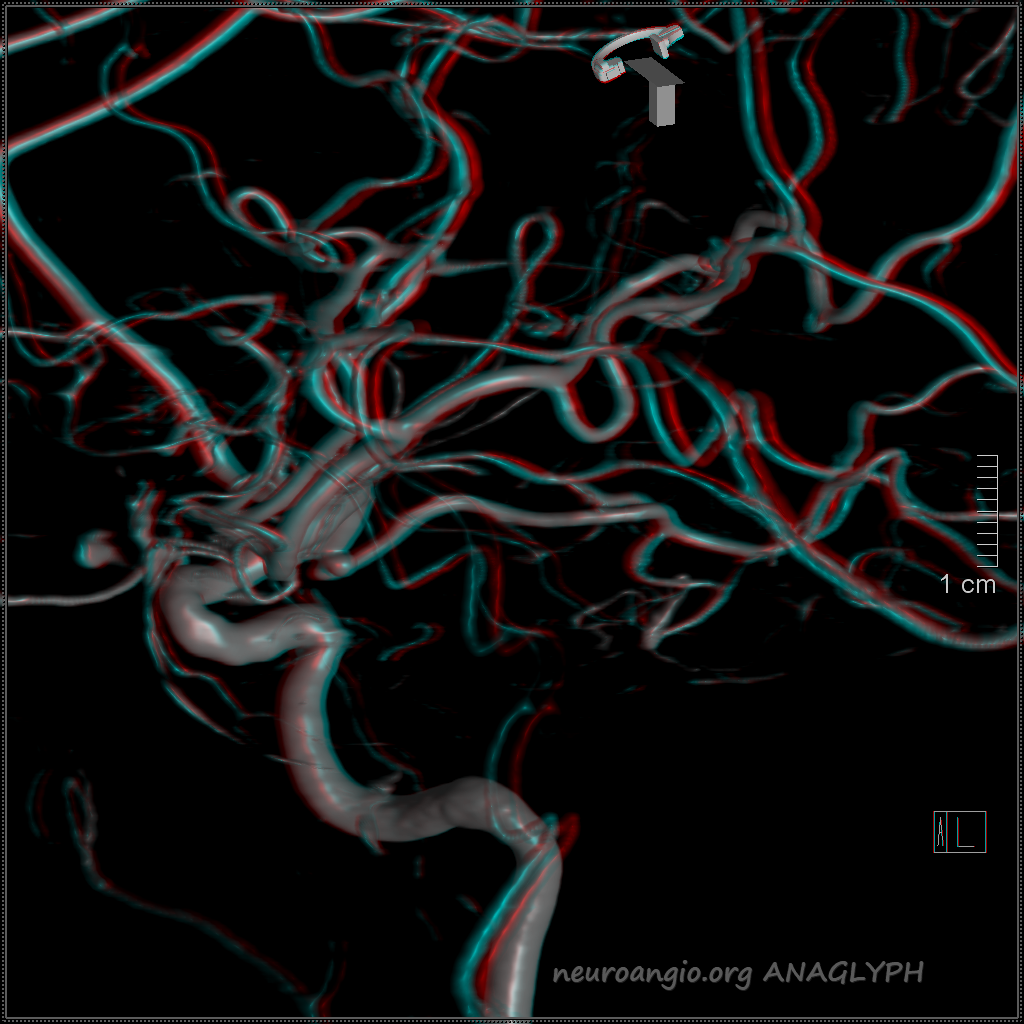
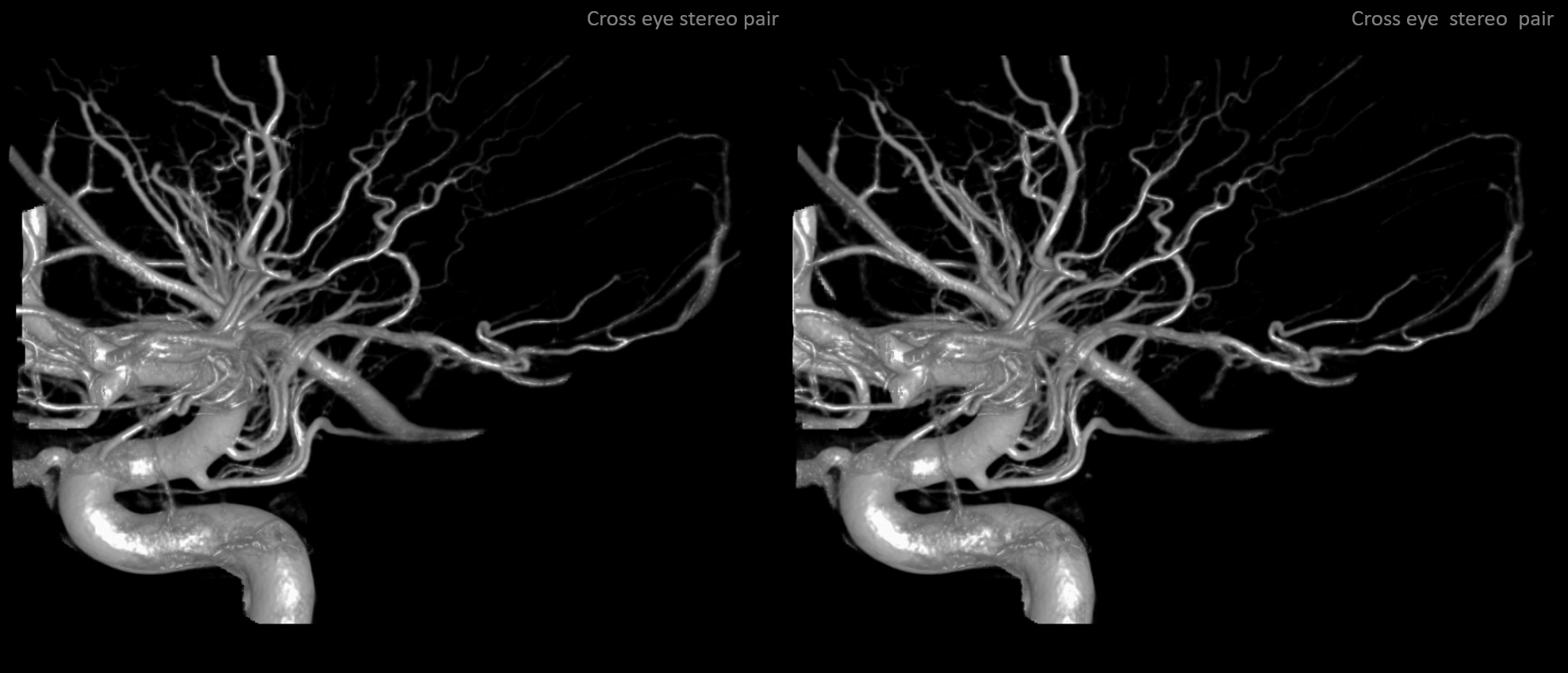
However, we do not stop there. Here’s what 7T can produce. Pretty stunning. The Anterior Choroidal (light blue) can be traced perfectly well towards the choroid plexus (dark red). Gadolinium contrast was administered prior to the scan, which explains some venous structures in there (not labeled). Notice amazing views of the lateral lenticulostriates (black), thalamogeniculate (dark blue double-sided arrow), as well as posterior choroidal (white), posterior inferior temporal (green) and middle inferior temporal (pink). The tentorium cerebelli enhancement (yellow) is also very helpful, as best seen in stereo

The same image in cross-eye stereo. Notice the graceful fall of the tentorium cerebelli, separating branches of the PCA and the SCA. Can you see the junction of the medial septal and thalamostriate veins?

Anterior Choroidal Artery Anatomy and Landmarks
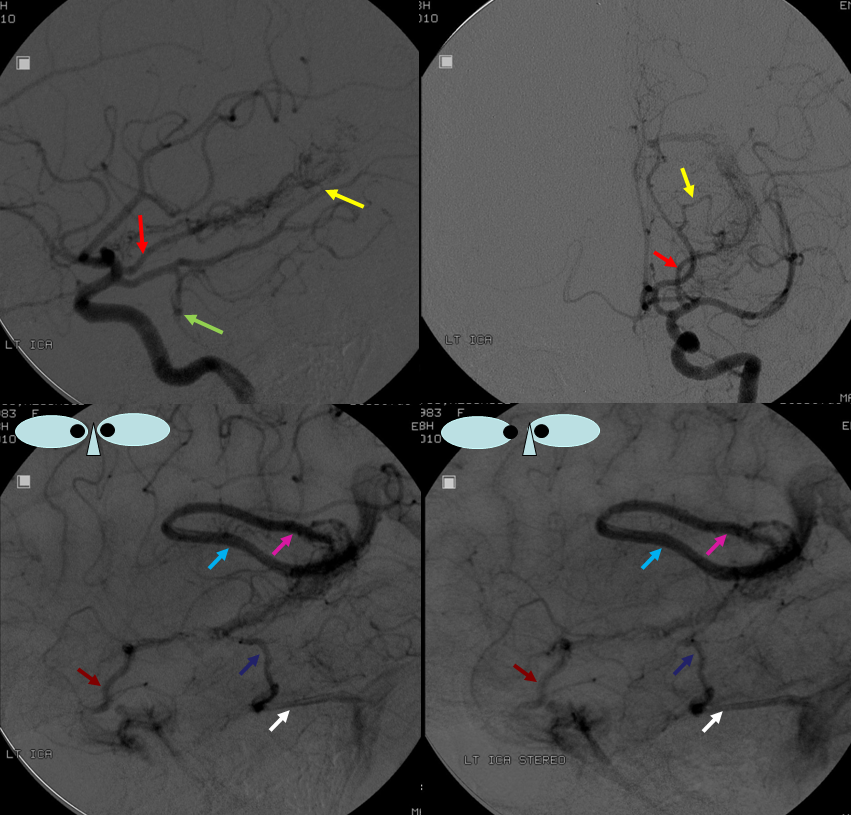
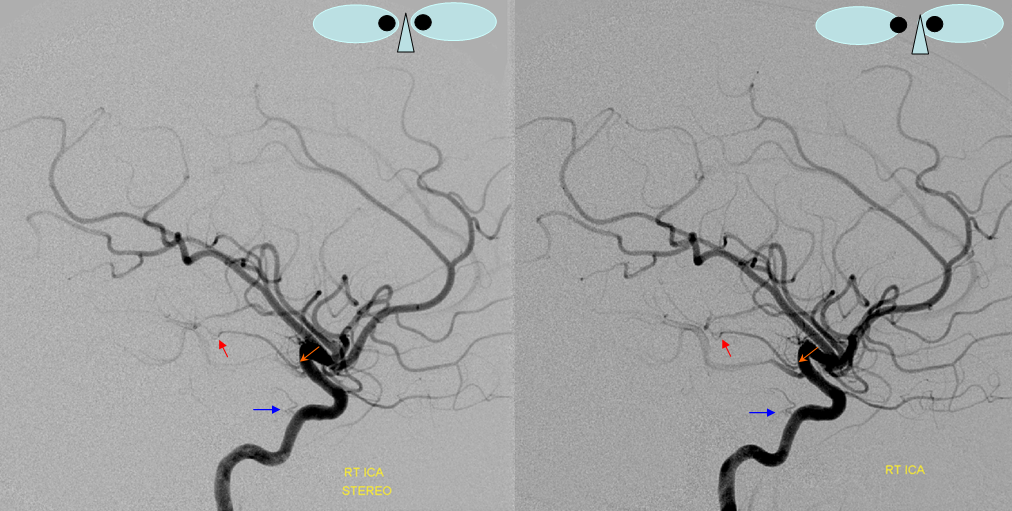
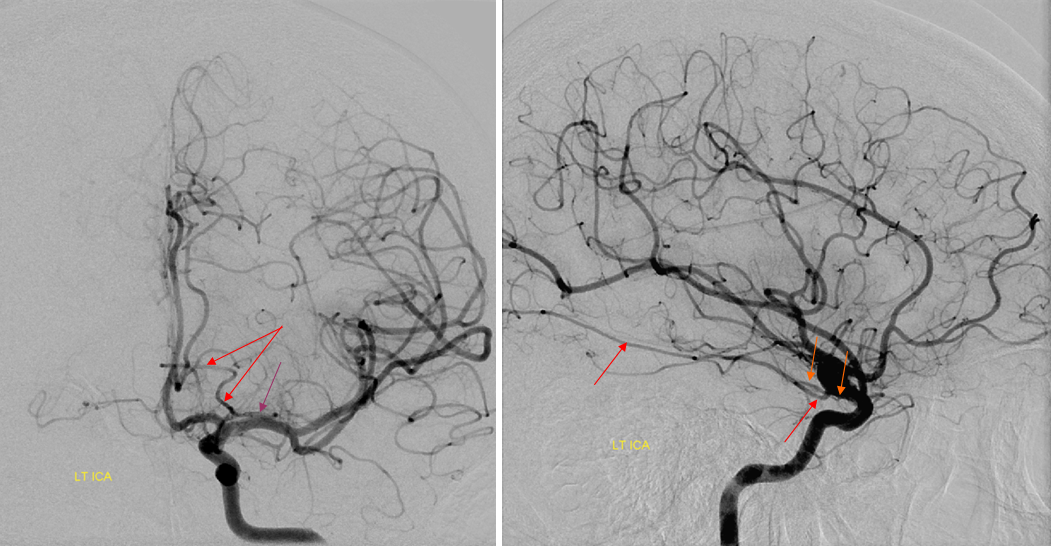
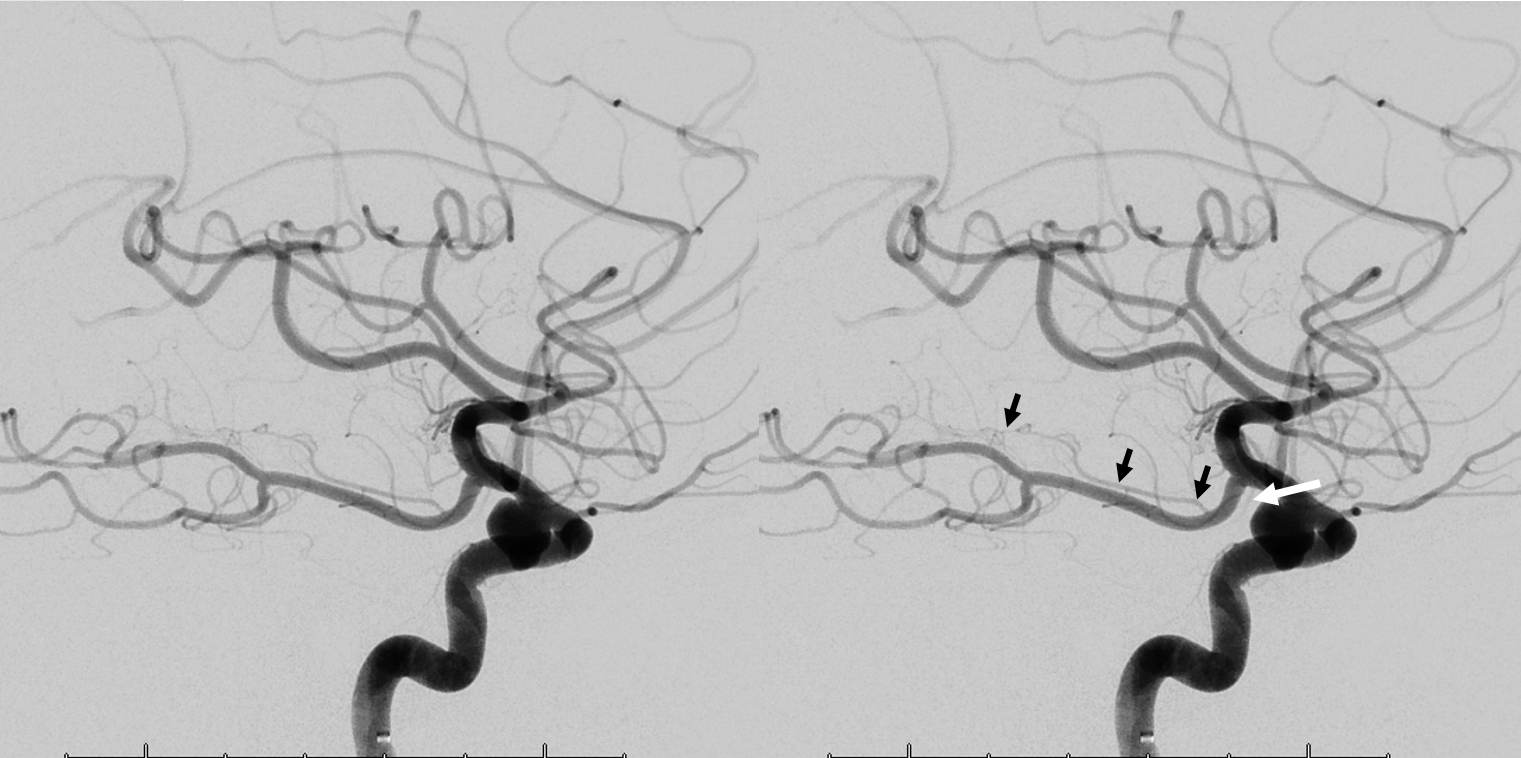
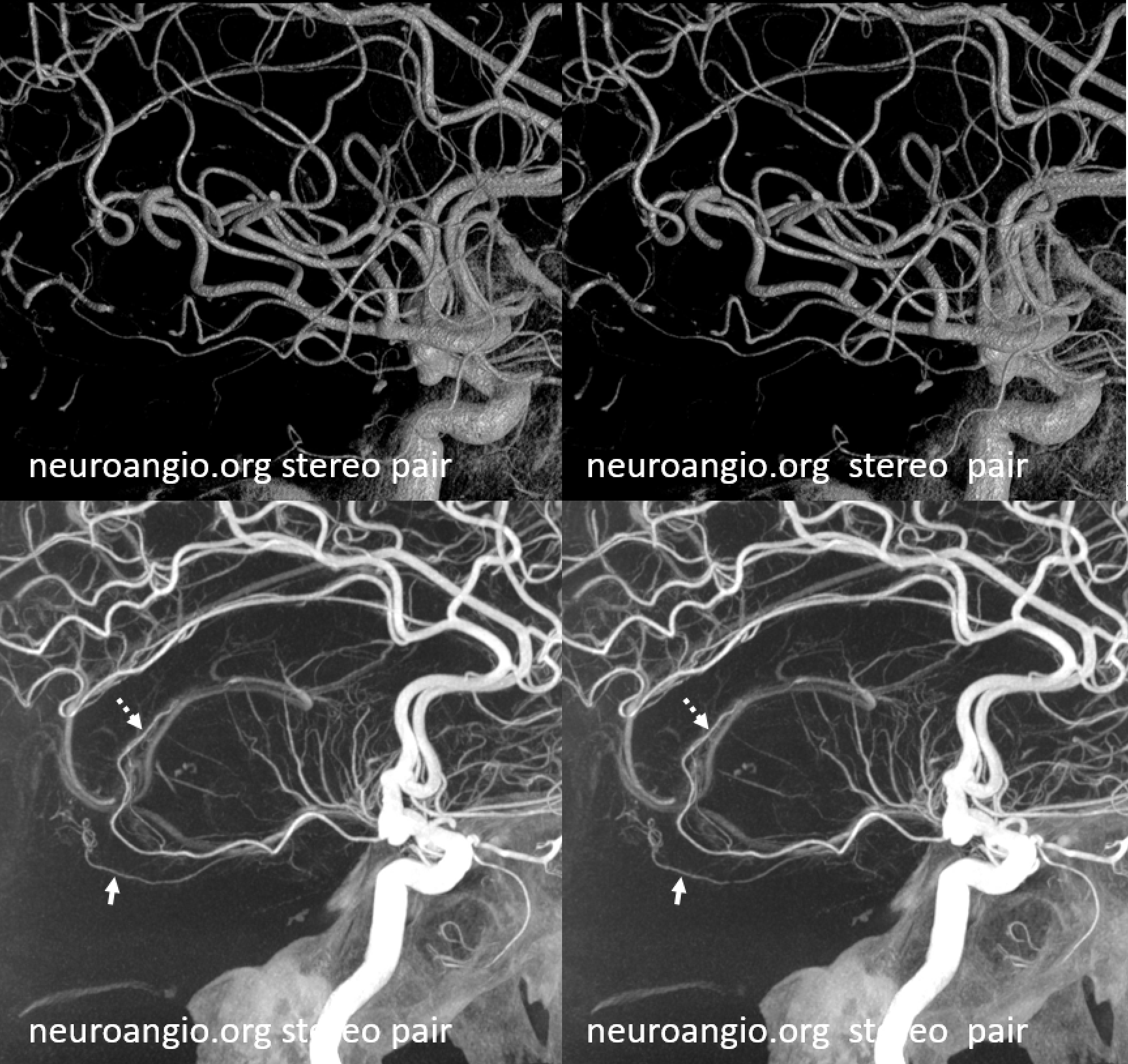
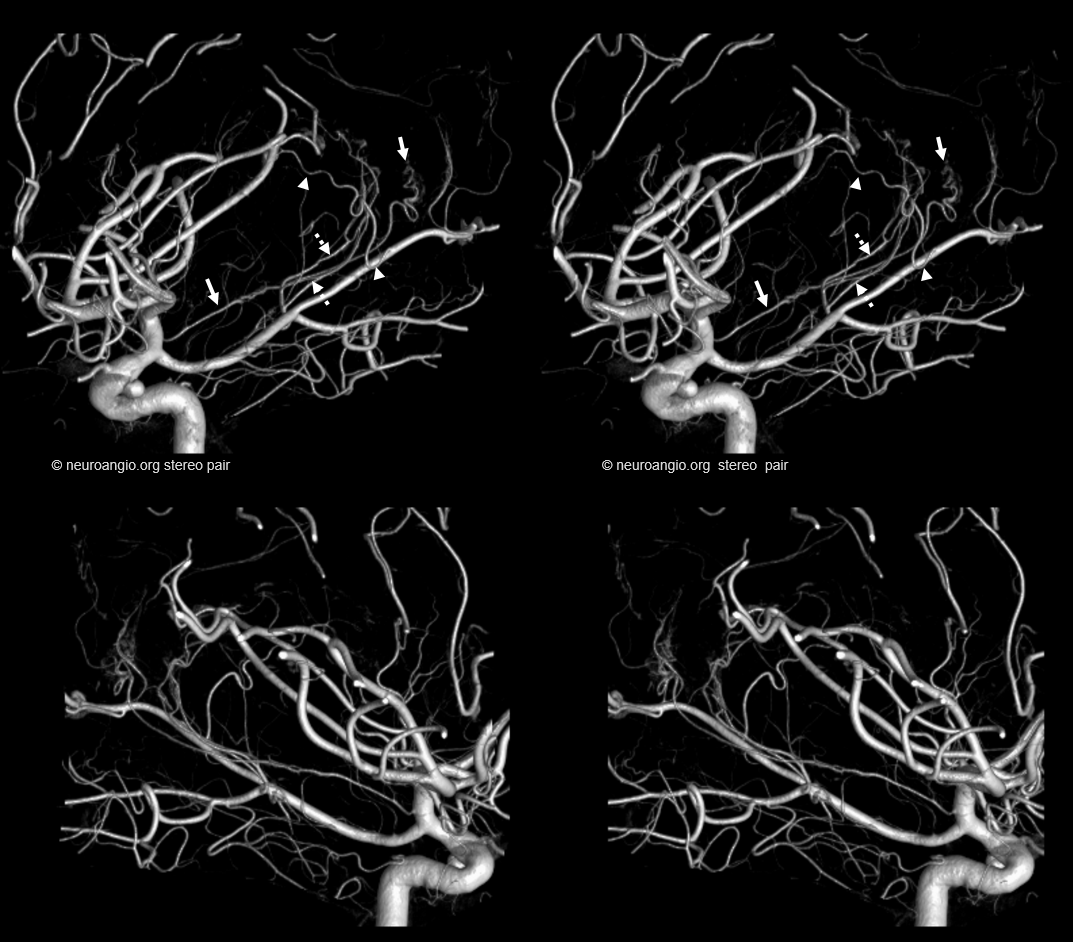
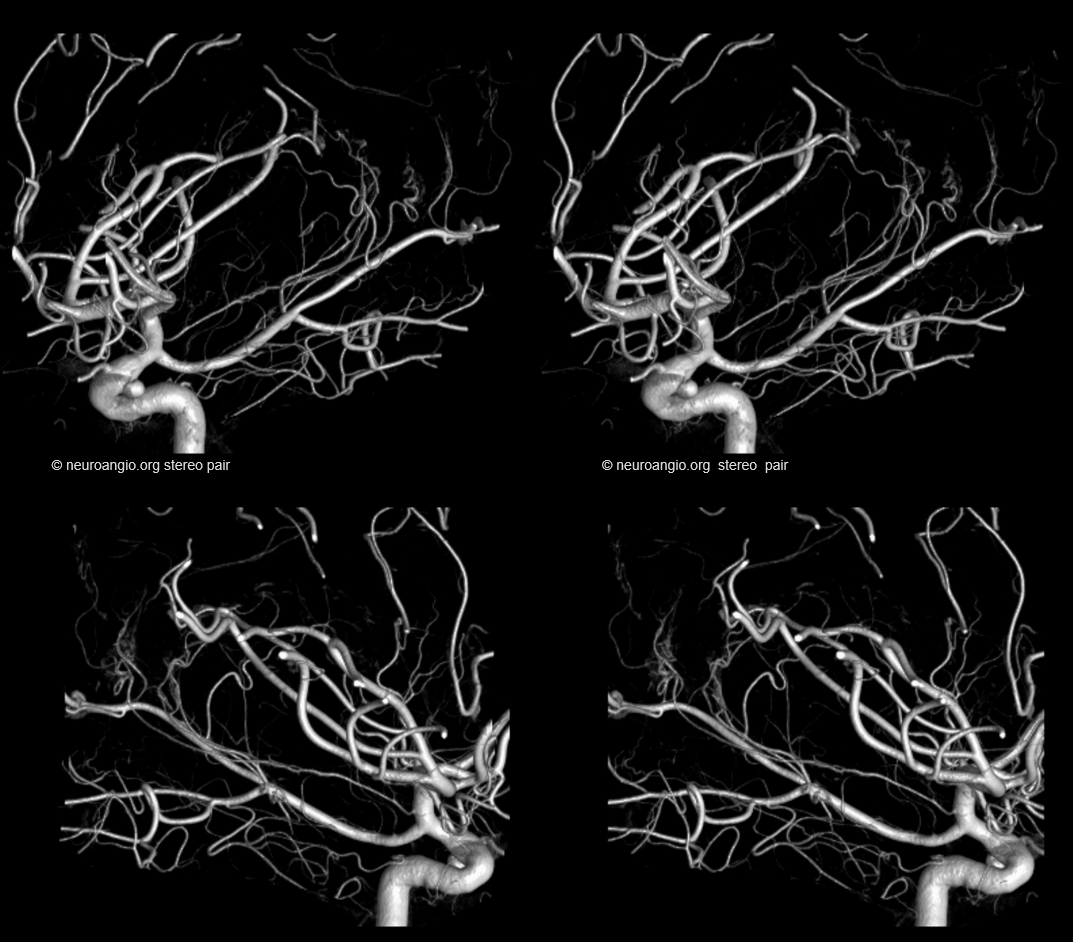
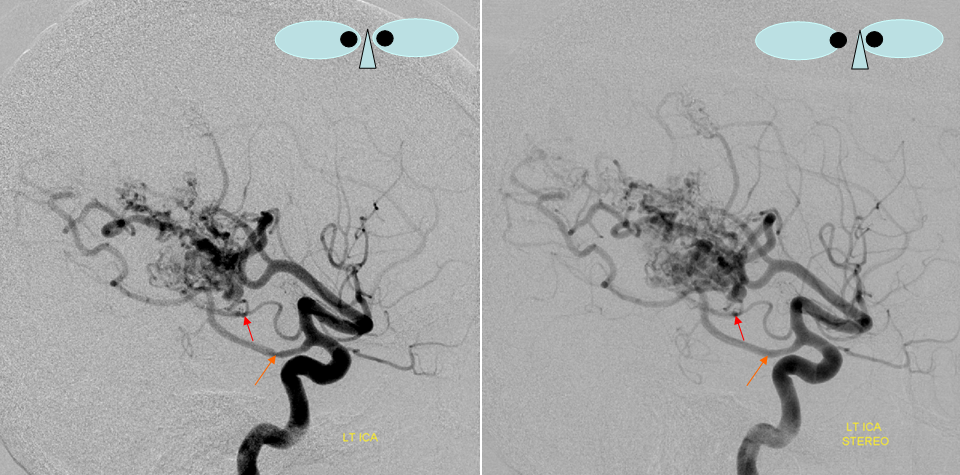
The course of anterior choroidal artery cisternal segment in the paramesencephalic cistern (around the cerebral peduncles) is superimposed angiographically upon the middle segment of the basal vein of Rosenthal. This can be demonstrated on a single image by selecting the arterial phase of the injection to be the “mask” of a later venous phase
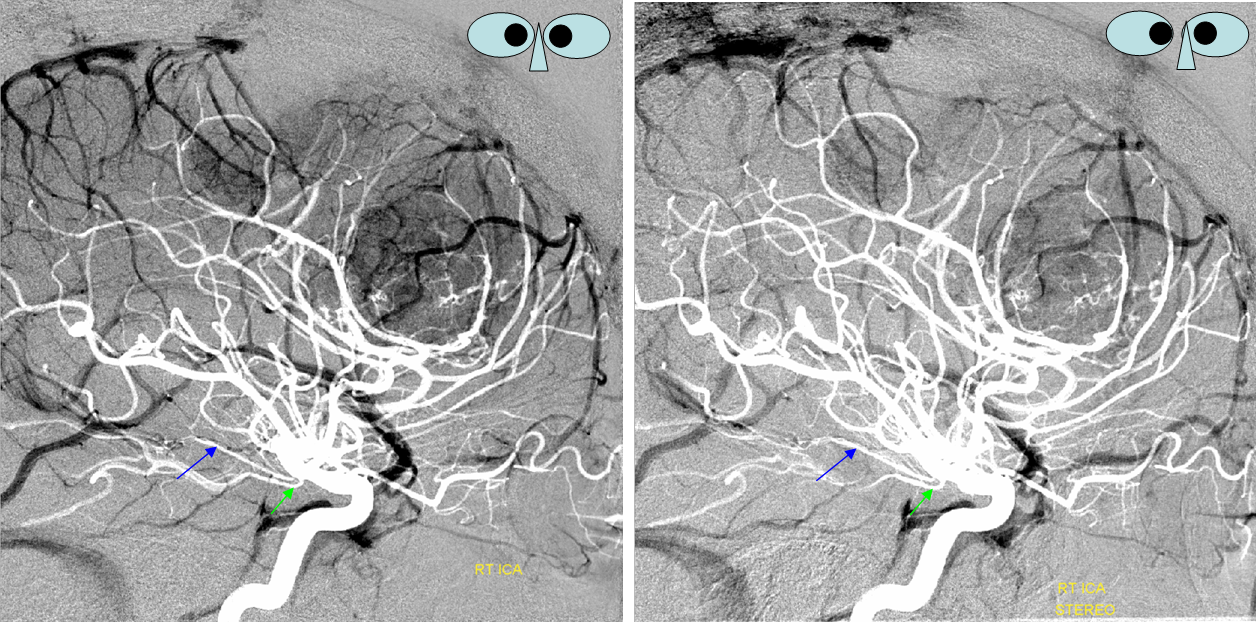
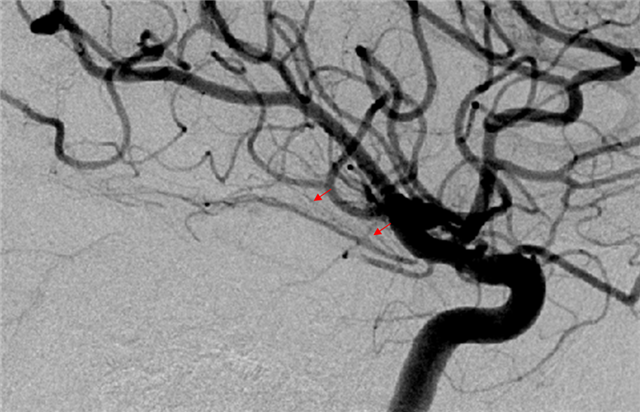
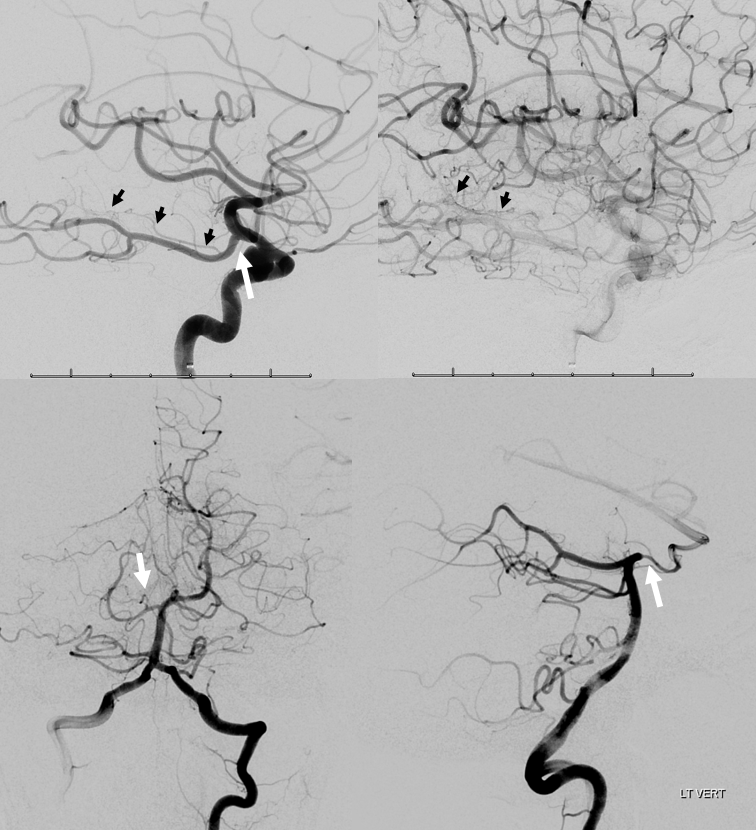
In the stereo projections above, where “mask” arteries appear white, a prominent Ant. Chor. artery is superimposed upon the basal vein. The patient suffers from NFII with multiple meningiomas. Notice many tiny branches (red arrows) coursing superiorly from the Anterior Choroidal artery (best seen in the “normal” image below marked with red arrows).
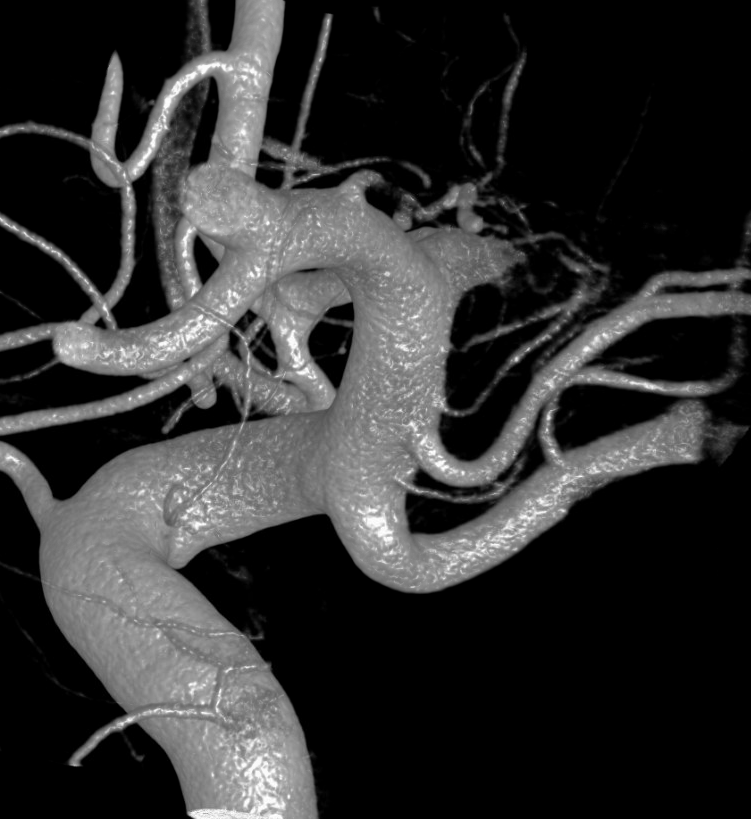
Anterior Choroidal perforators 2
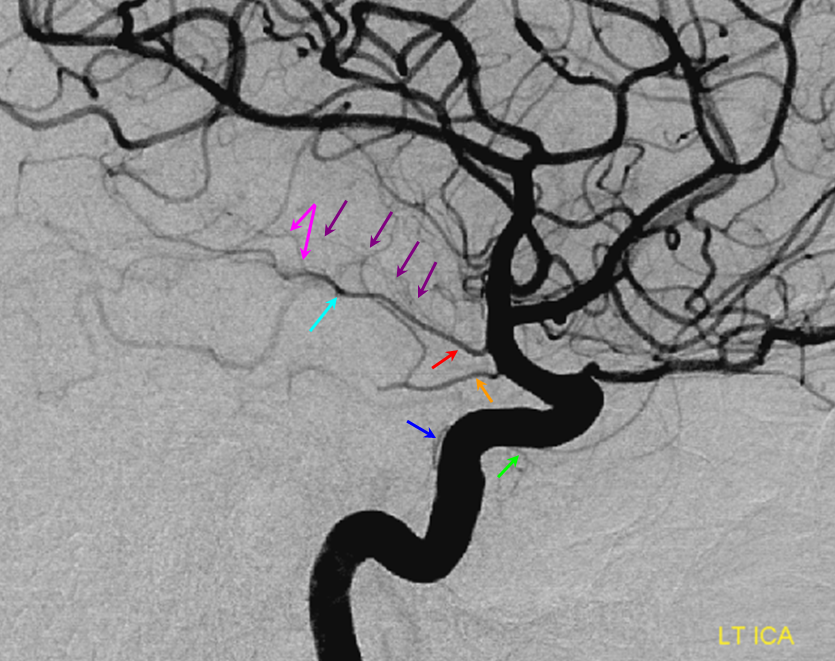
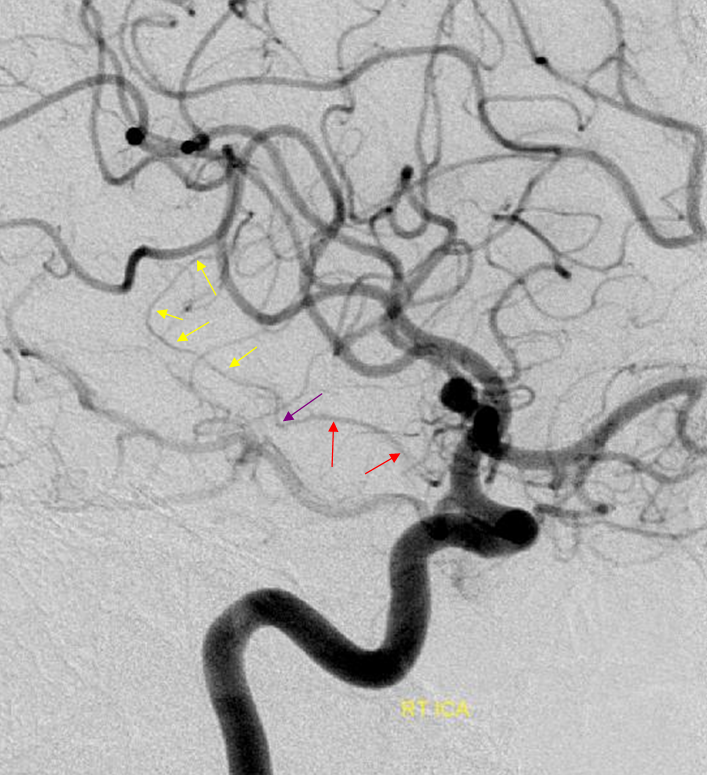
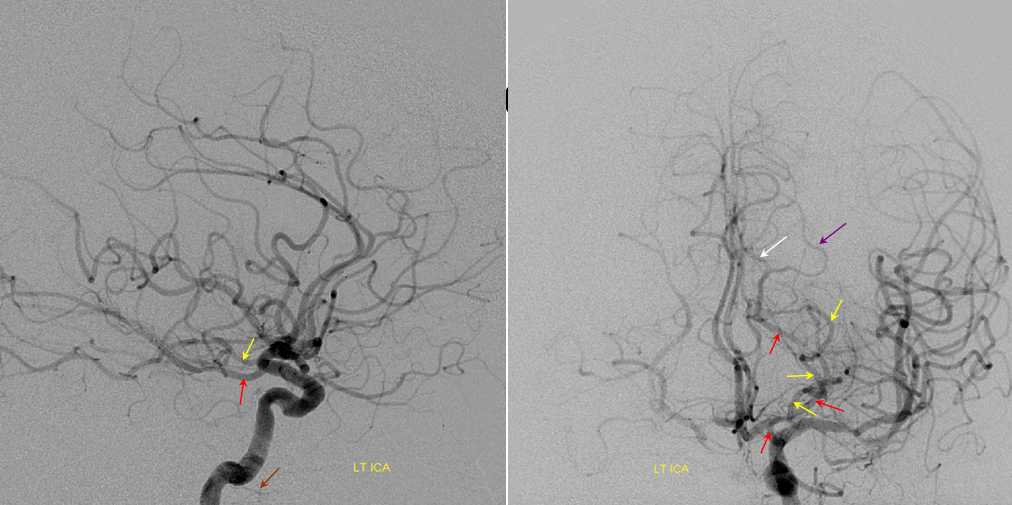
Another illustration of anterior choroidal perforators (purple) coming off the main trunk (red) prior to the plexal point (light blue). A branch to the choroid distal to the plexal point may be present also (pink). The PCOM is orange (with a large thalamic branch of its own). MHT (dark blue) and ILT (green) branches are also visible.
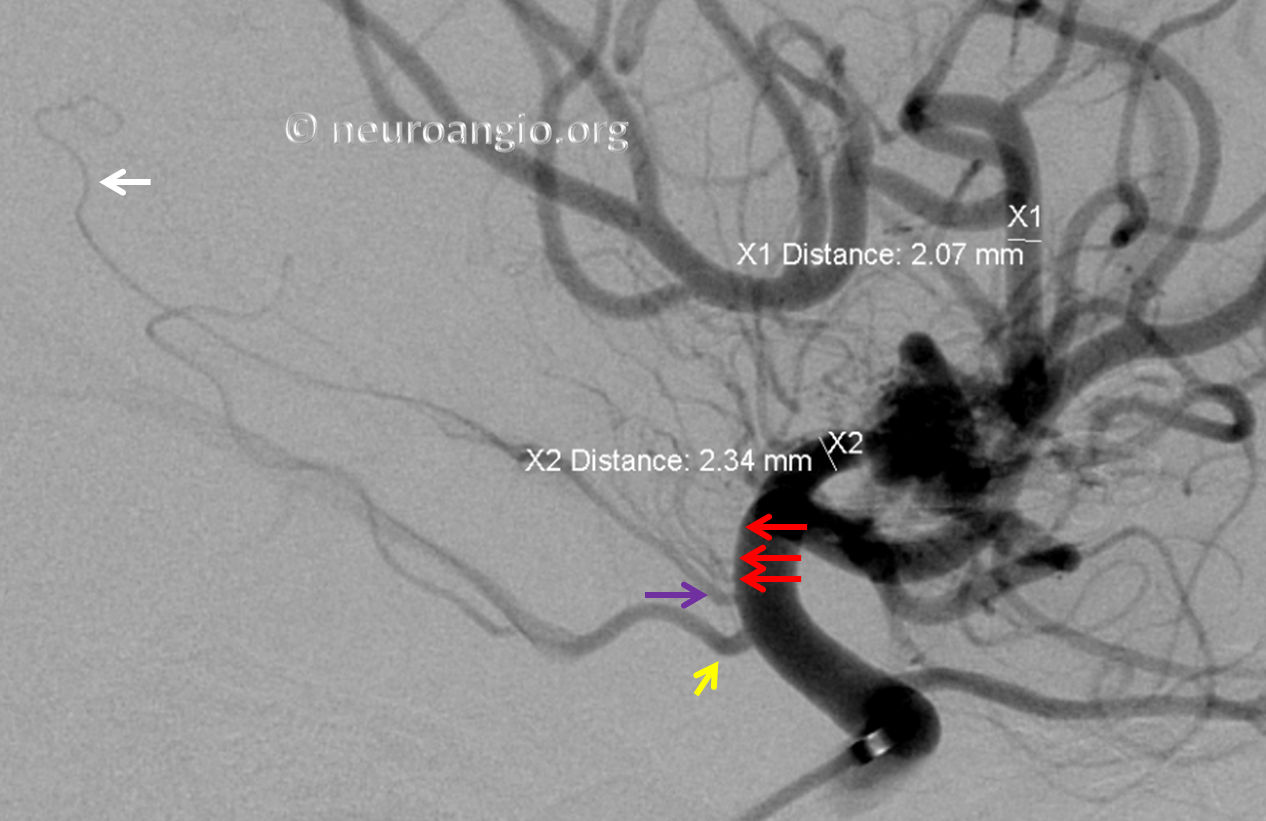
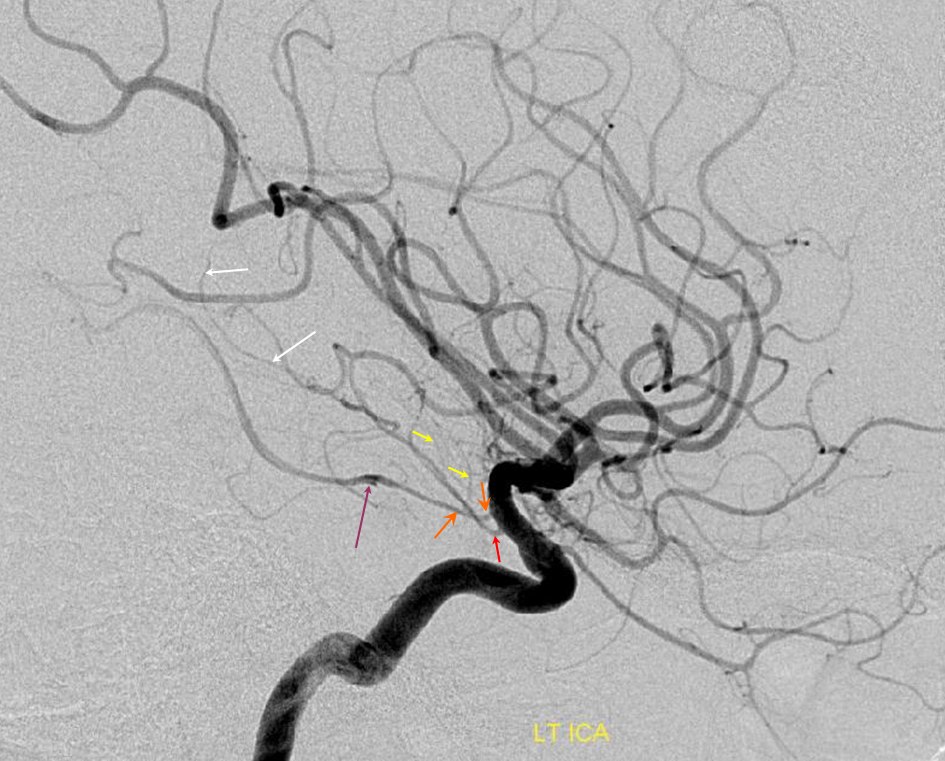
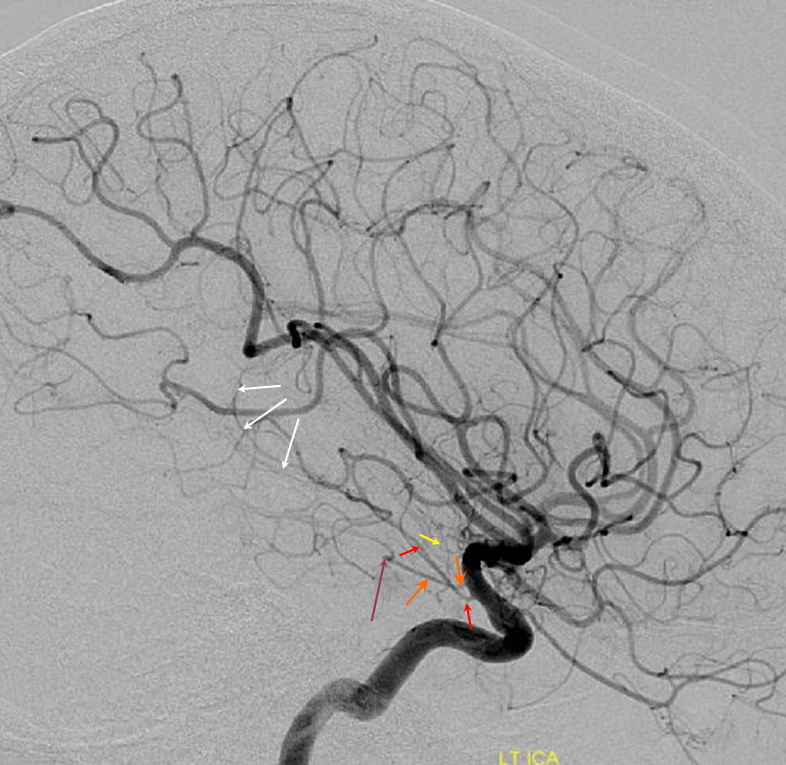
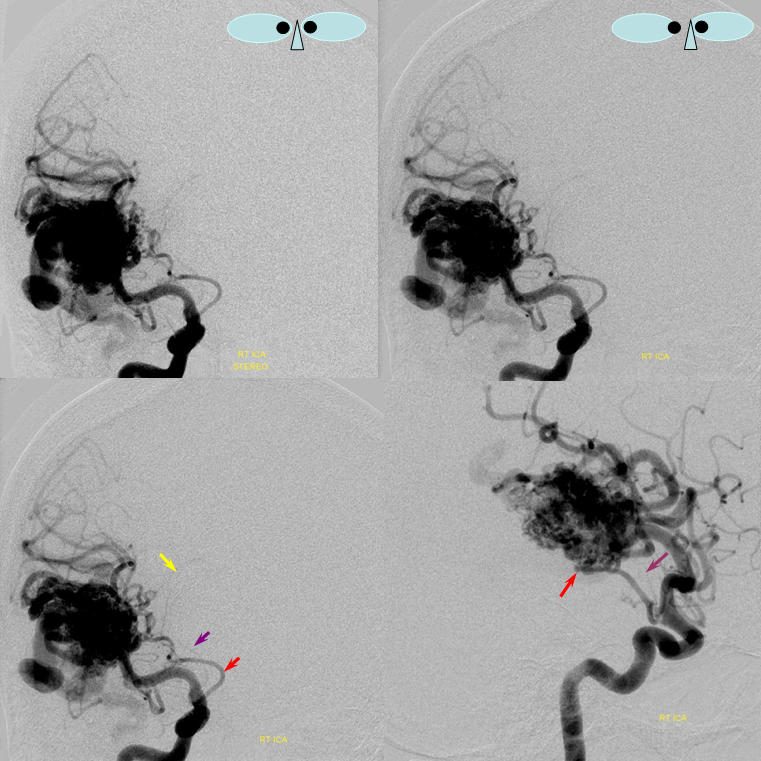
If you talk to an open vascular surgeon, they will tell you about duplicated or multiple choroidal arteries. Essentially what they are seeing are several vessels arising distal to the PCOM and looking like they are heading into choroidal territory. While it is certainly a correct observation that more than one vessel can be seen in the choroidal region, there is only one choroidal artery — the artery supplying the choroid plexus. What is really going on is that perforator vessels which normally arise from the cisternal (proximal) portion of the anterior choroidal artery frequently originate directly from the adjacent internal carotid artery. These distal vessels are pretty much all eloquent. They are also the same vessels that hypertrophy as anastomoses between the choroidal perforator system and the lenticulostriate vessels in Moya-Moya or other steno-occlusive proximal MCA disease. Here is an example of multiple normally proximal choroidal artery perforators arising as a variant directly from the ICA. Perforators are marked by red arrows. Choroidal artery proper is purple, including its choroidal segment (white). PCOM is yellow. Case courtesy Dr. David Gordon
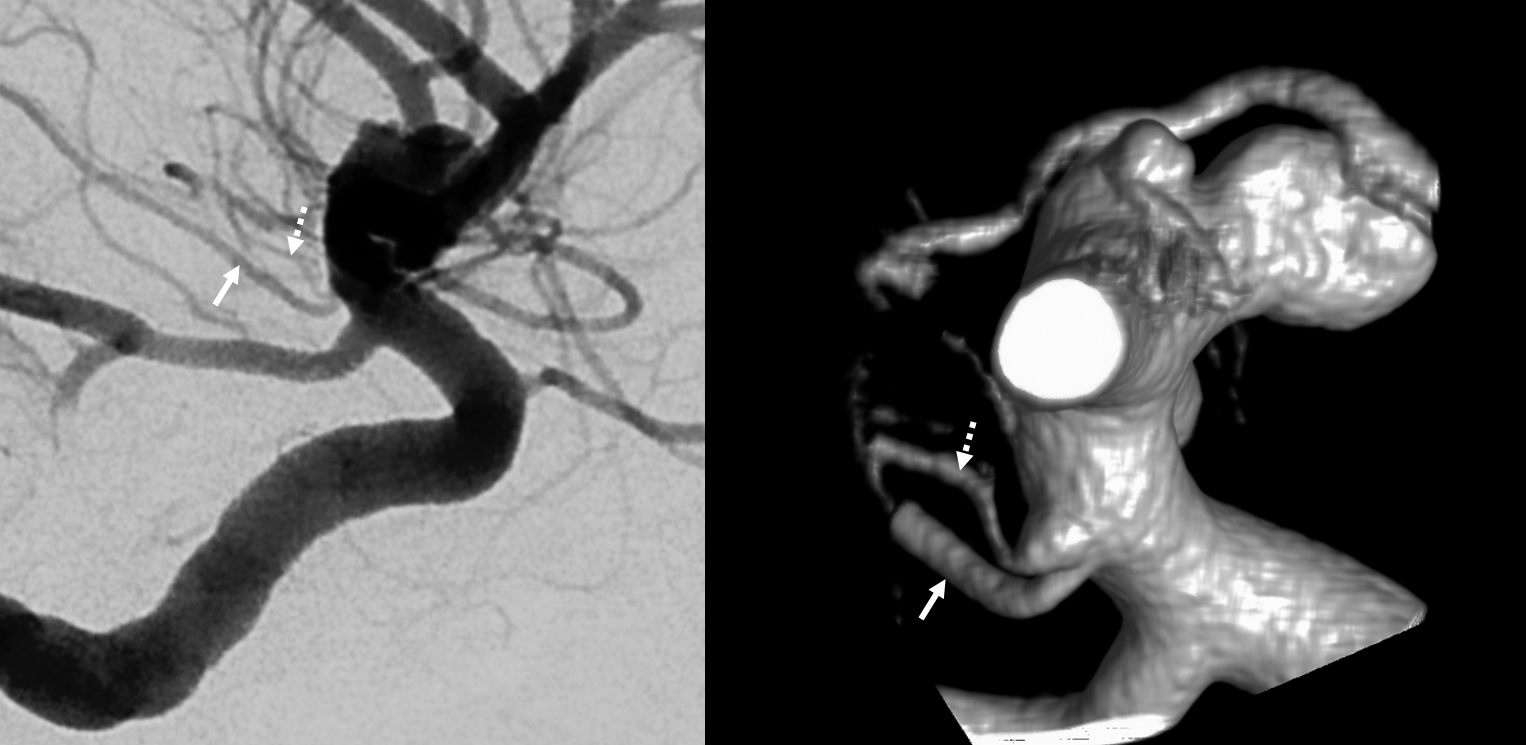
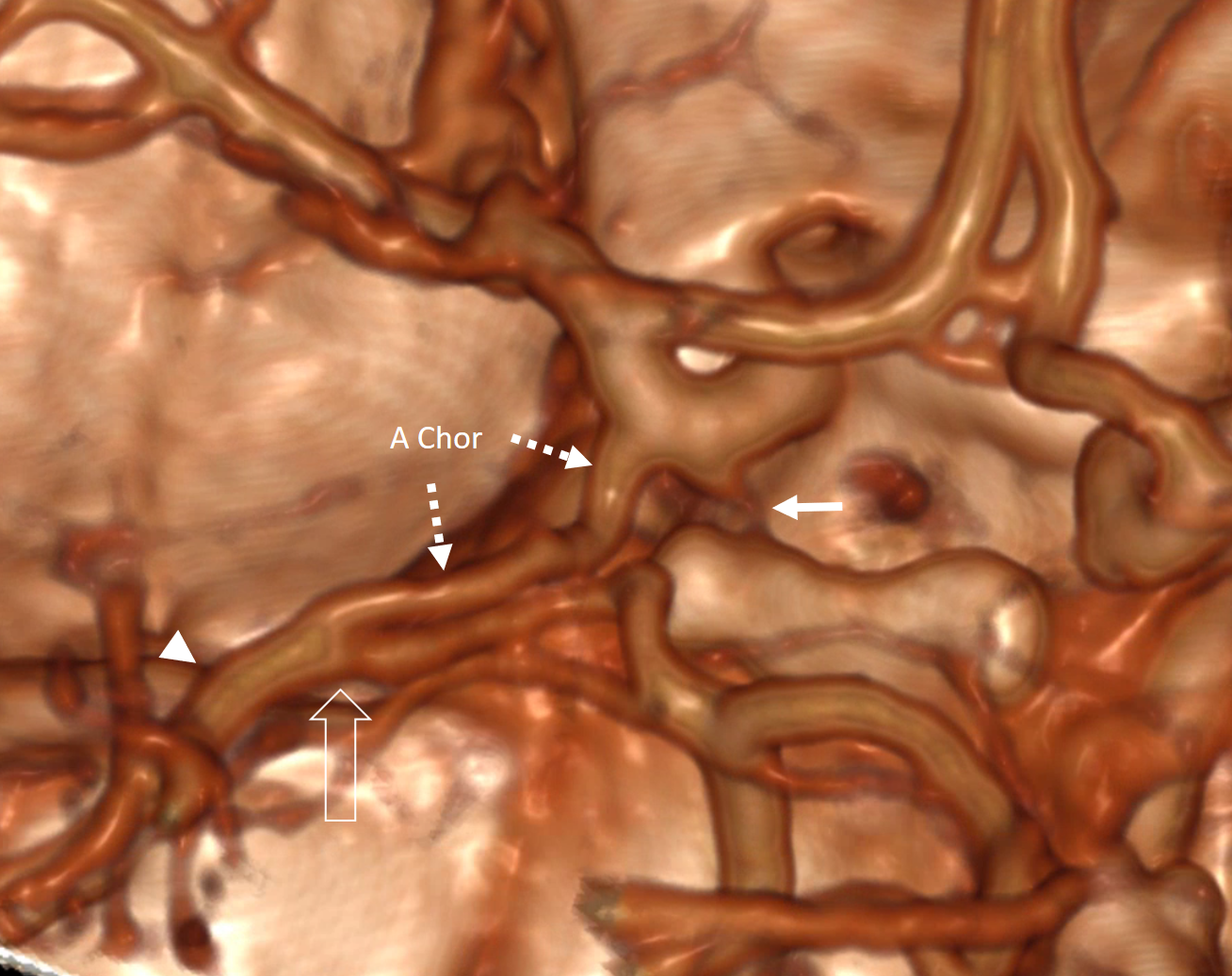
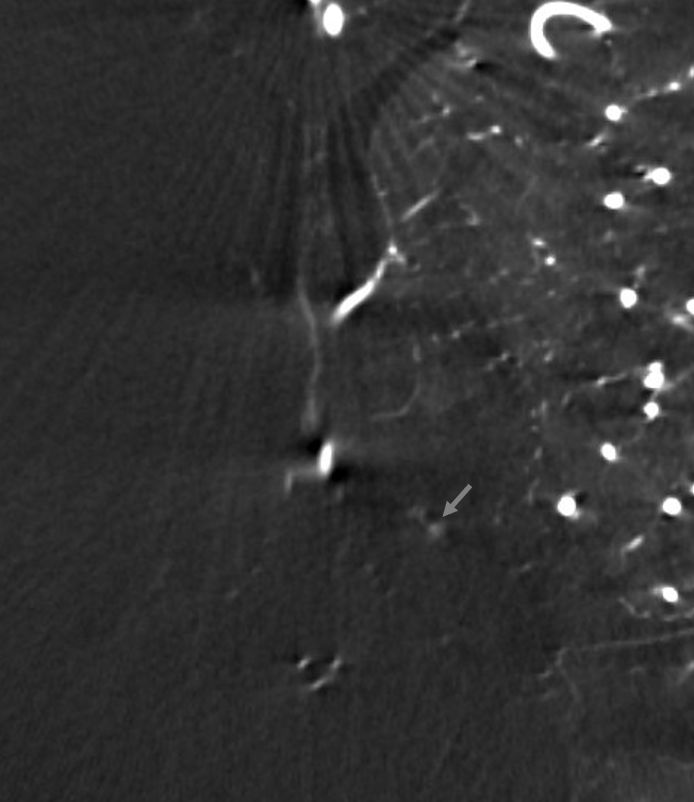
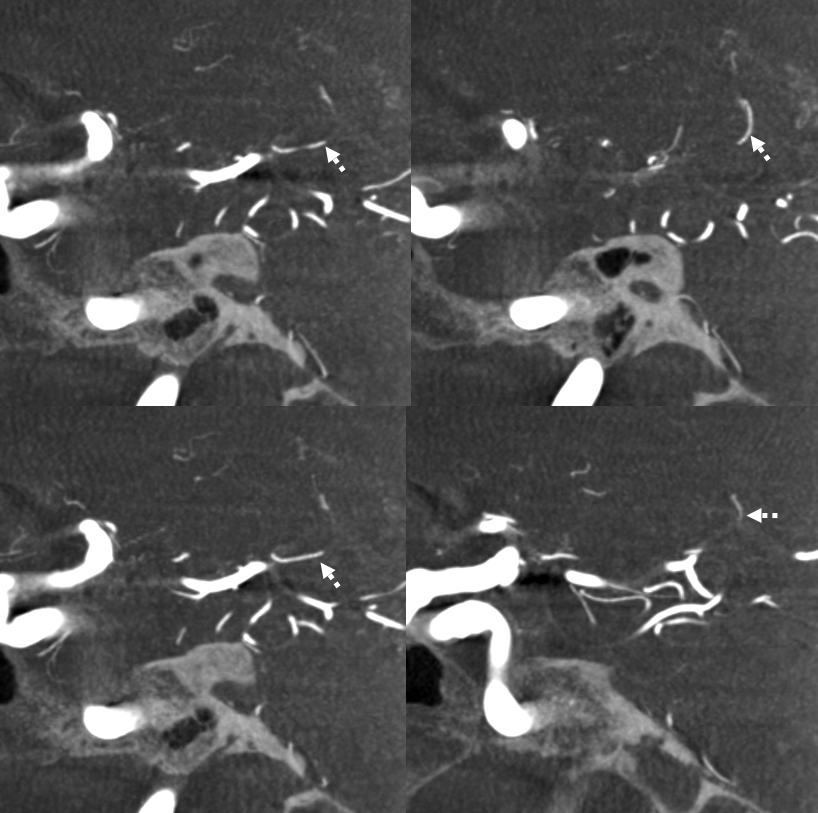
The reason these “extra” vessels are not seen as often on angio as surgically is that they are often very small. DYNA CT helps a lot. Below is an example — not much can be said conclusively on the DSA — however DYNA shows clearly an anterior perforated substance destination vessel (dashed arrow) just distal to choroidal (arrow) origin — with its own infundibulum
Like everything else, there is a spectrum of variability in where the vessels are located relative to each other, etc. The distances between anterior choroidal and PCOM and ICA terminus are all variable. In the example below, the PCOM and choroidal origins are nearly “fused”. Nothing wrong with that.
The same can be well-illustrated in cone beam CT. The choroidal artery — by definition one supplying the choroid plexus — is always most proximal to the perforators. The more perforators are associated with ICA the less will be on choroidal itself
Angio of same patient
Here is another example by Dr. Raz. Importantly, there is this notion that no vessels can be found between the PCOM and the choroidal. That’s usually true — the direct origin perforators are typically distal to choroidal artery proper (defined as artery which supplies the choroid plexus). The below case is an exception — see the little one between fetal PCOM and big Anterior Choroidal? MIP image of DYNA CT
VR same patient
M1 reconstitution
Differential diagnosis includes Moya-Moya, twig MCA (whatever this is), “rete MCA” (whatever this is), sequela of dissection, or athero. Demographics help with ordering these, but generally if you ask 5 people you will get 10 answers. What is clear is that proximal choroidal perforators (to the mesial temporal lobe, optic tracts, anterior limb), whether arising from the choroidal itself of the ICA, will play a role in many of the observed reconstitutions (Moya-Moya as a rule).
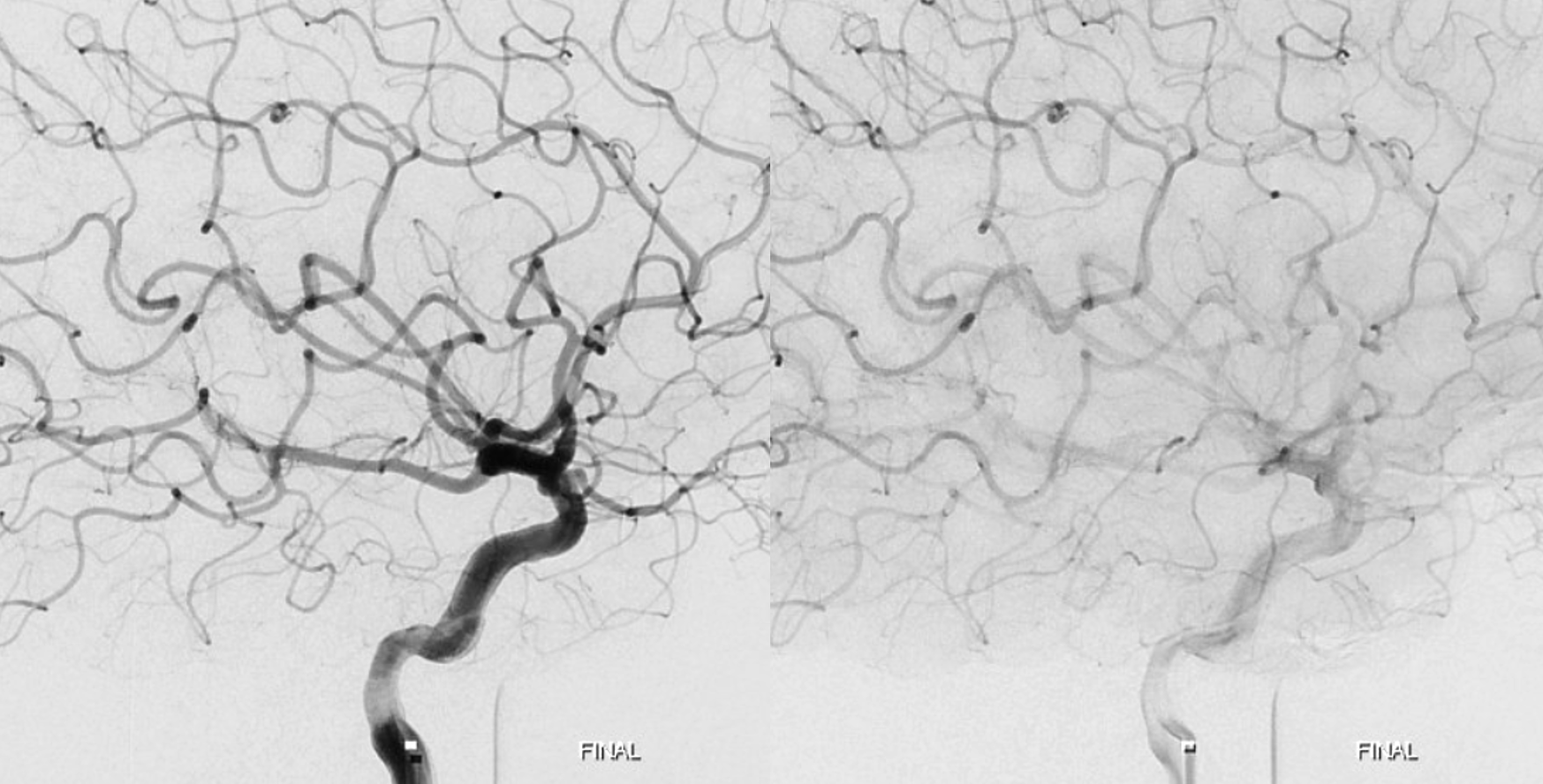
Below is an example, where a kind of smoke puff can be seen at the terminus, although most of the reconstitution is leptomeningeal
DYNA CT shows well proximal choroidal perforator role in MCA resupply (stereo pairs, without and with arrows)

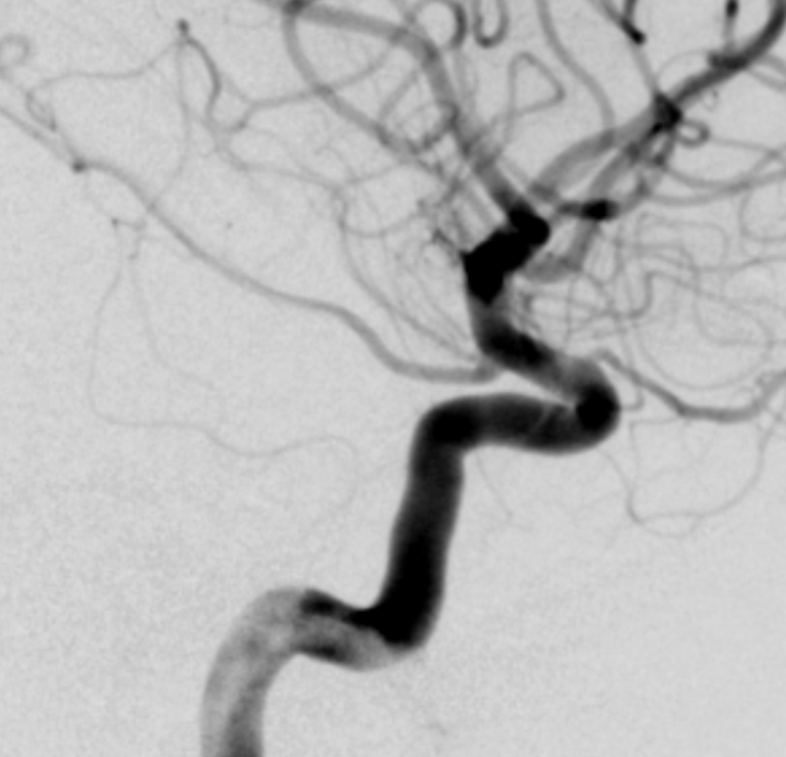
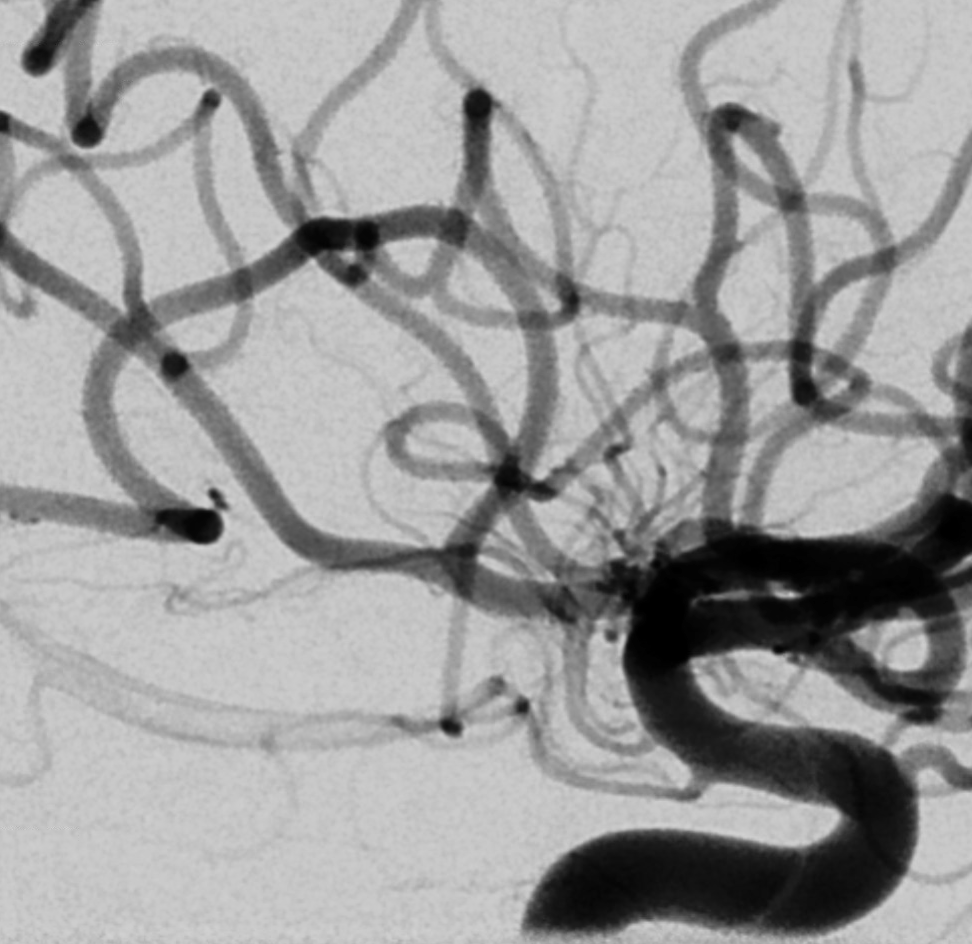
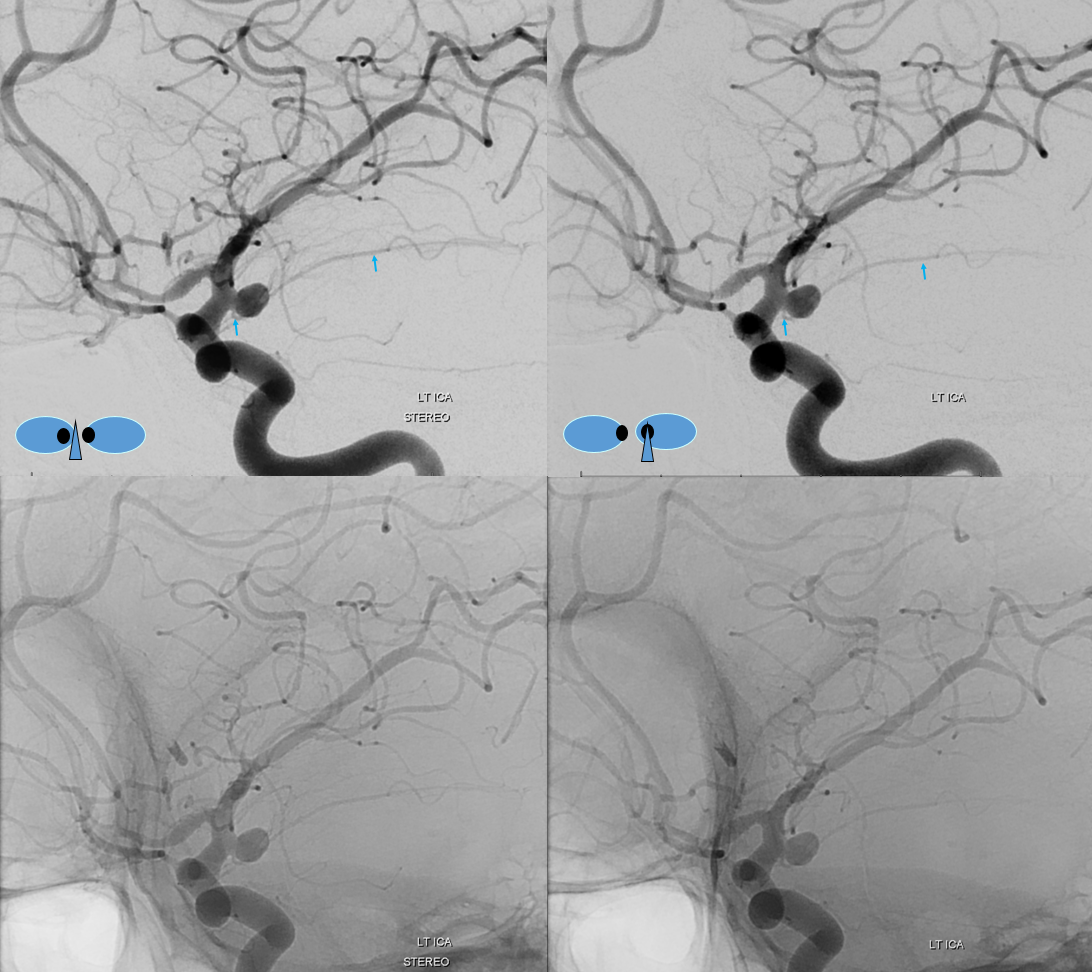
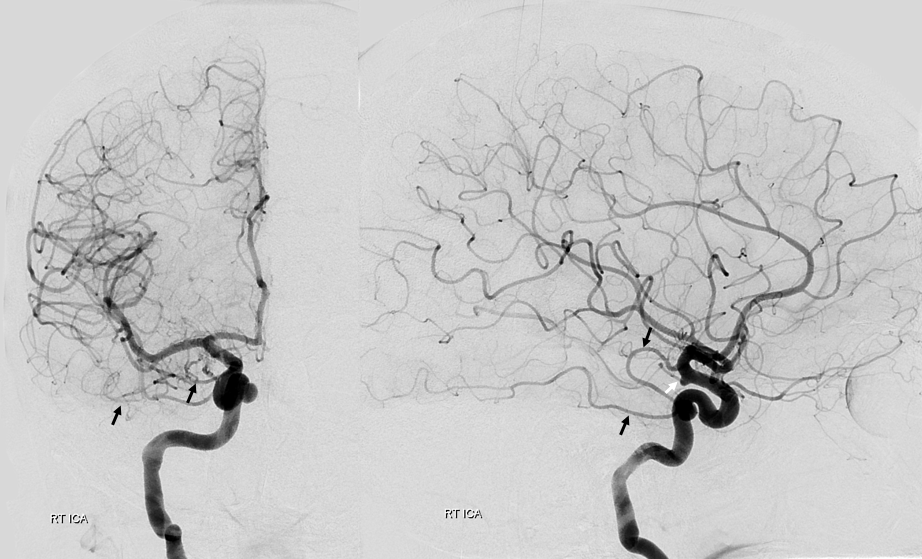
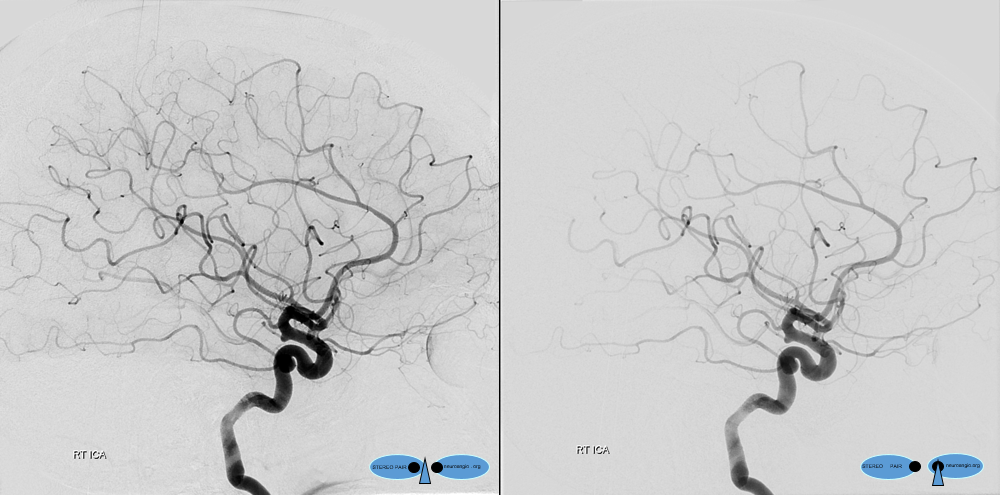
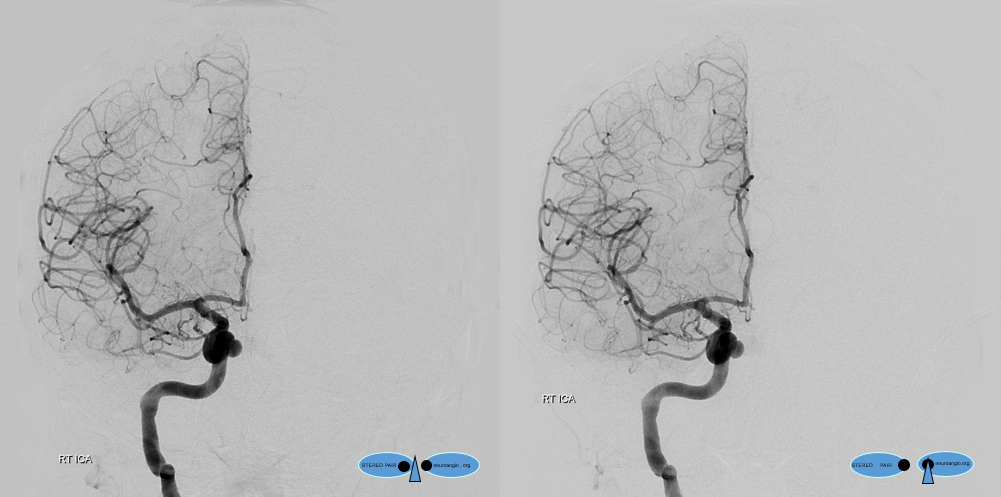
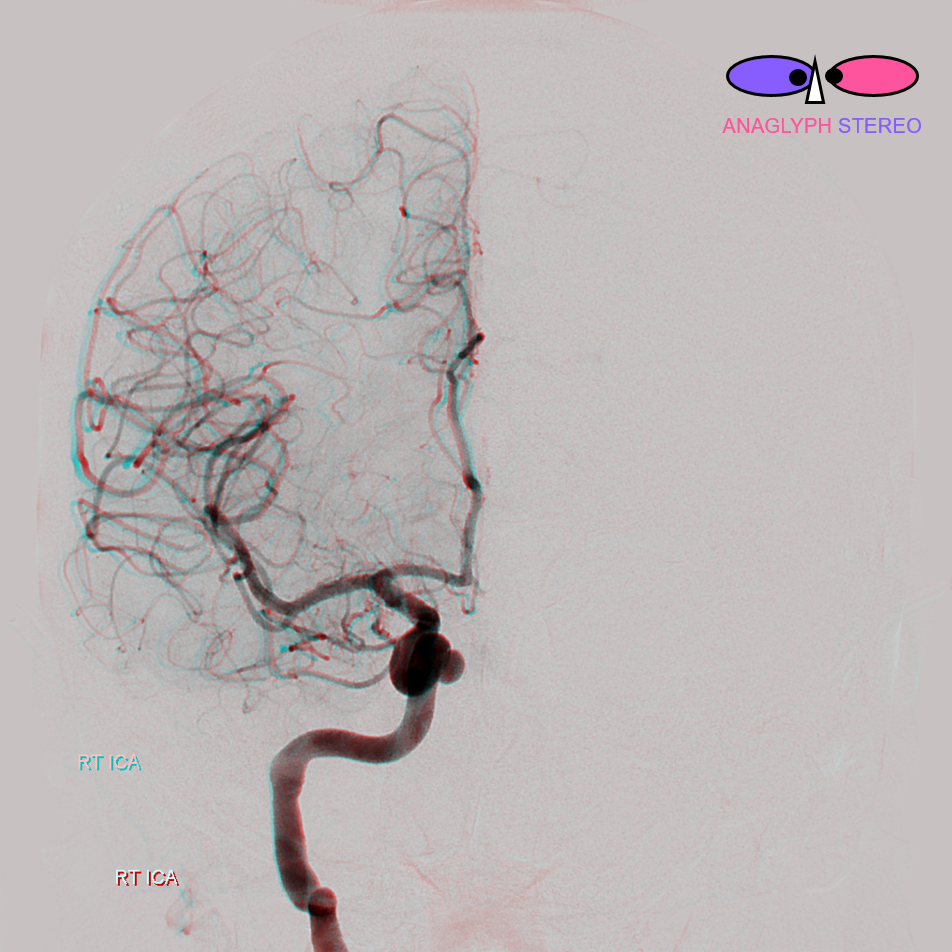
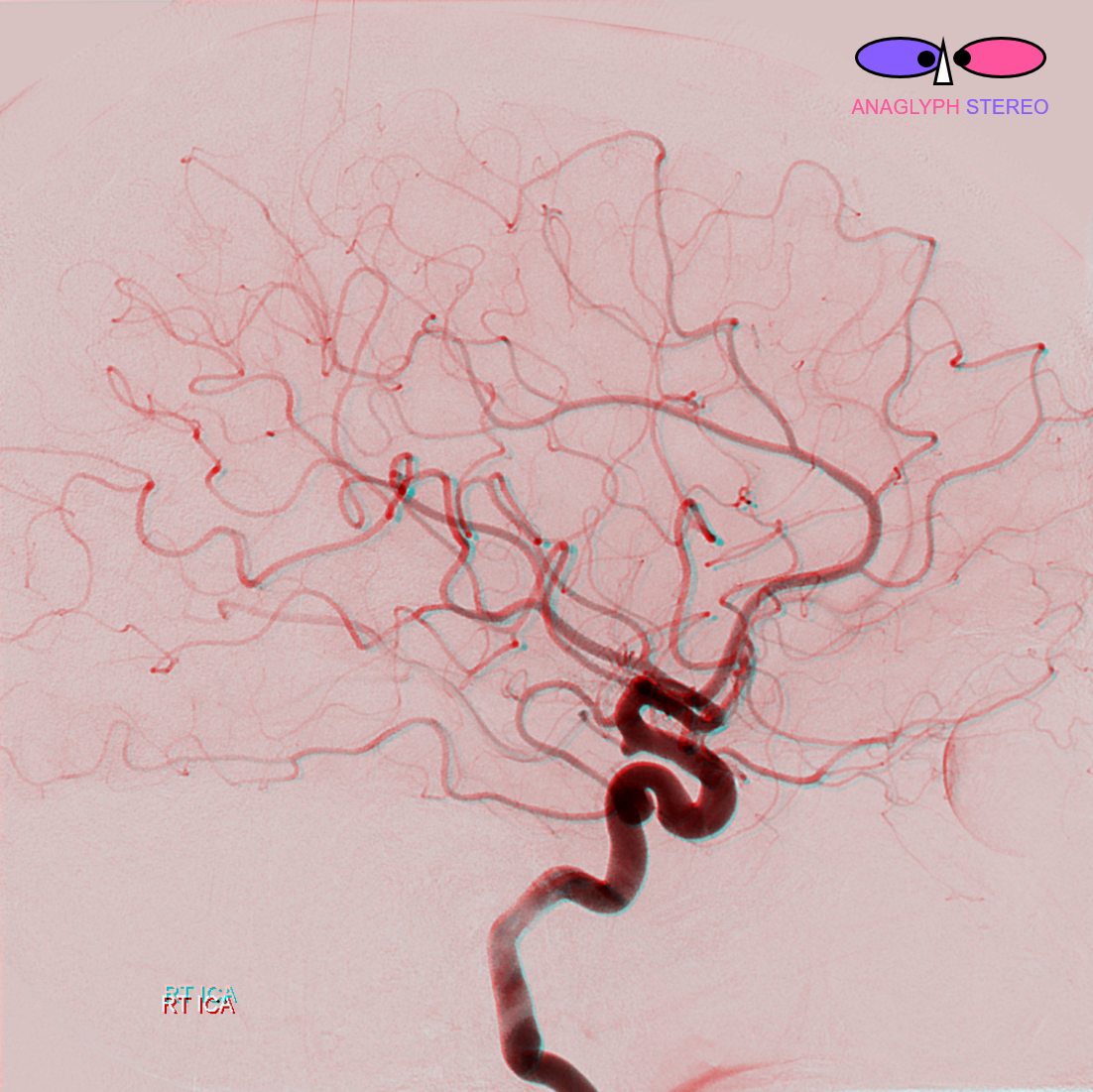
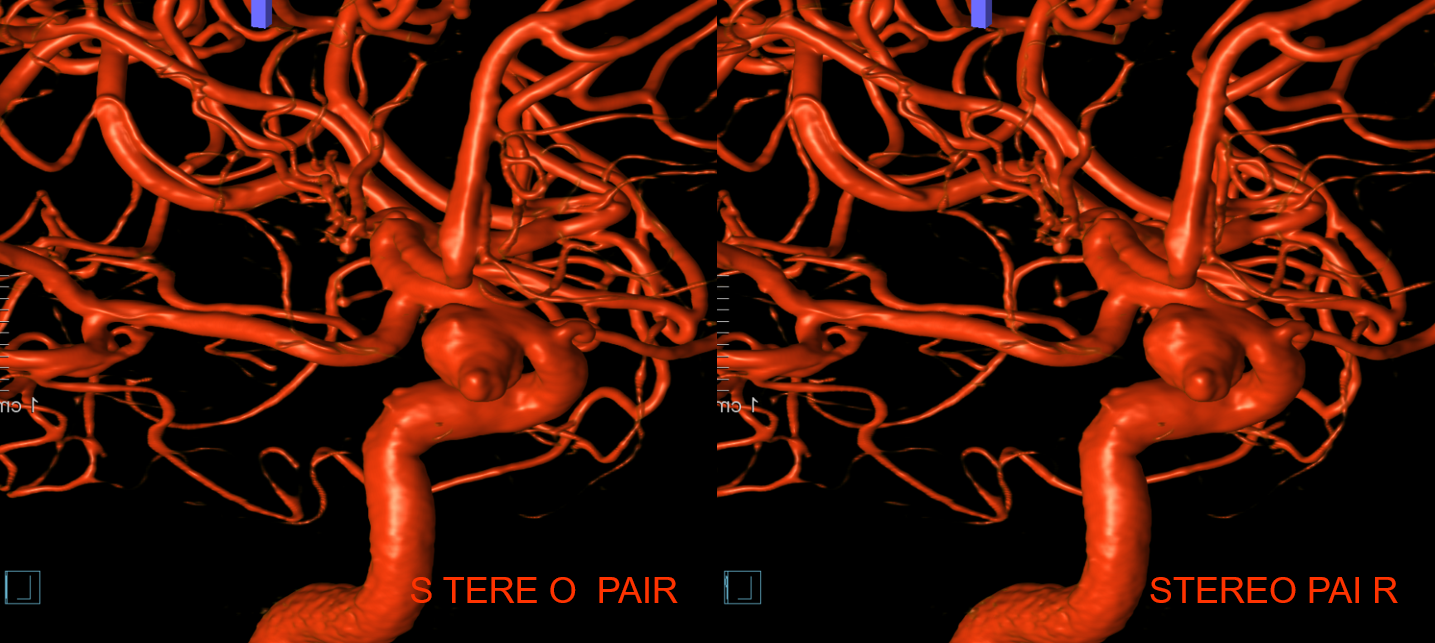
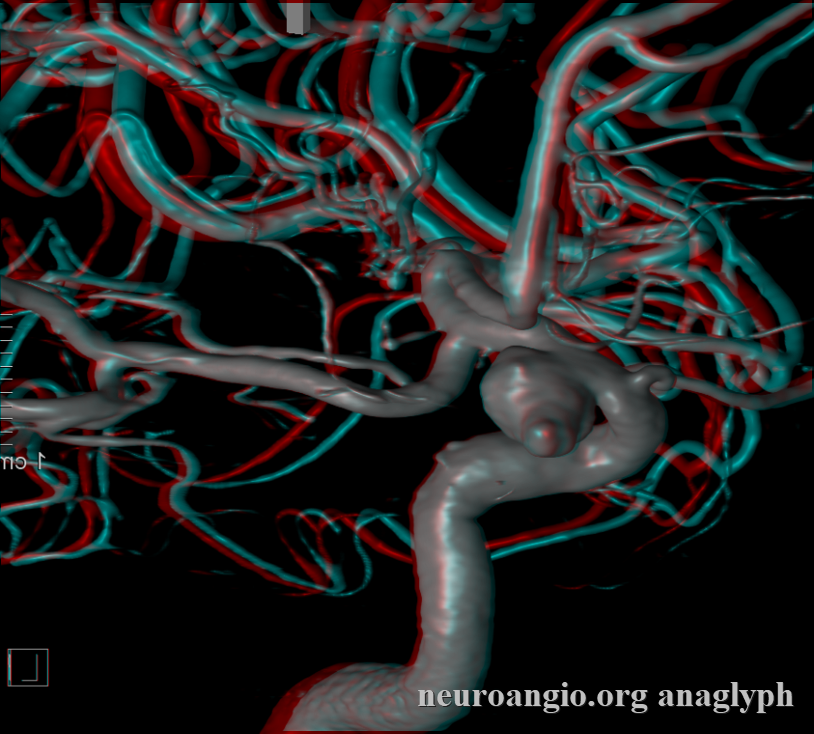
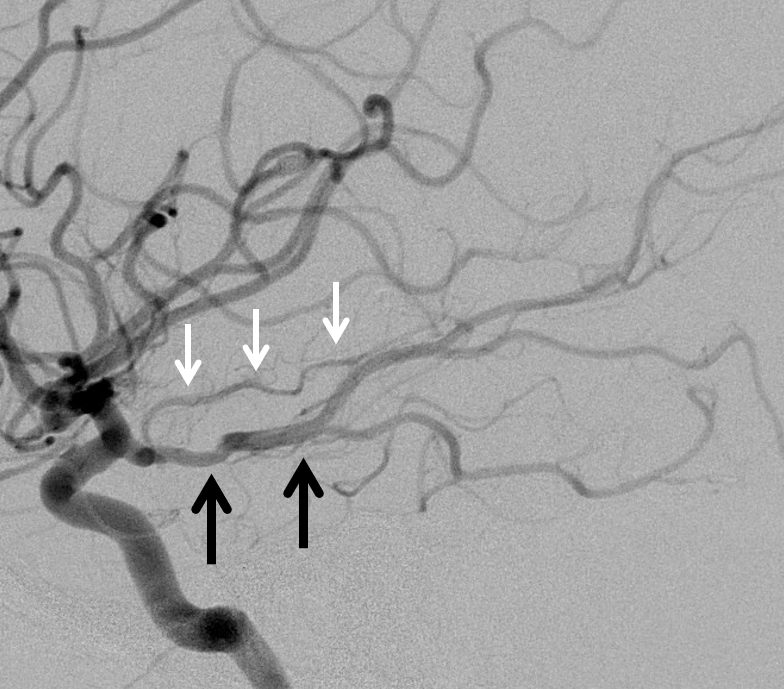
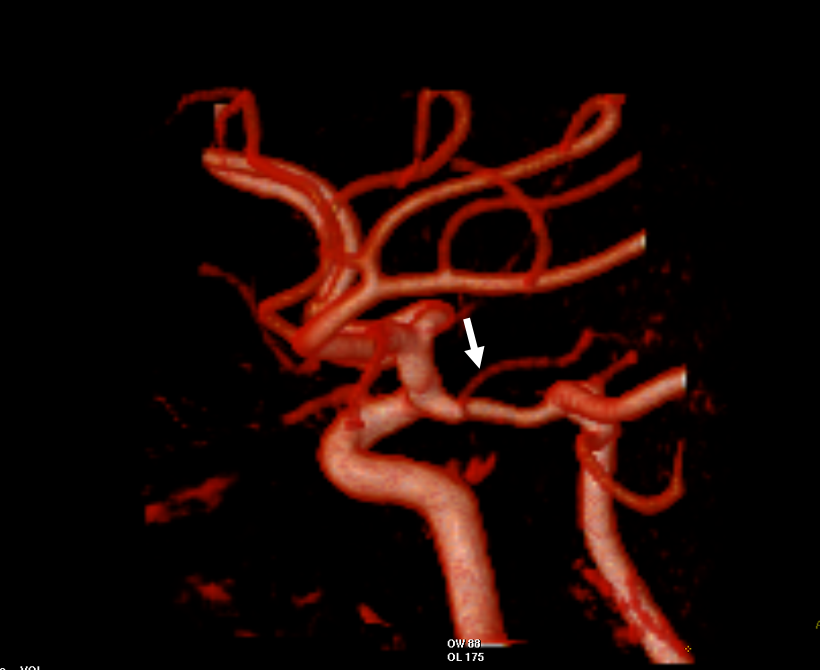
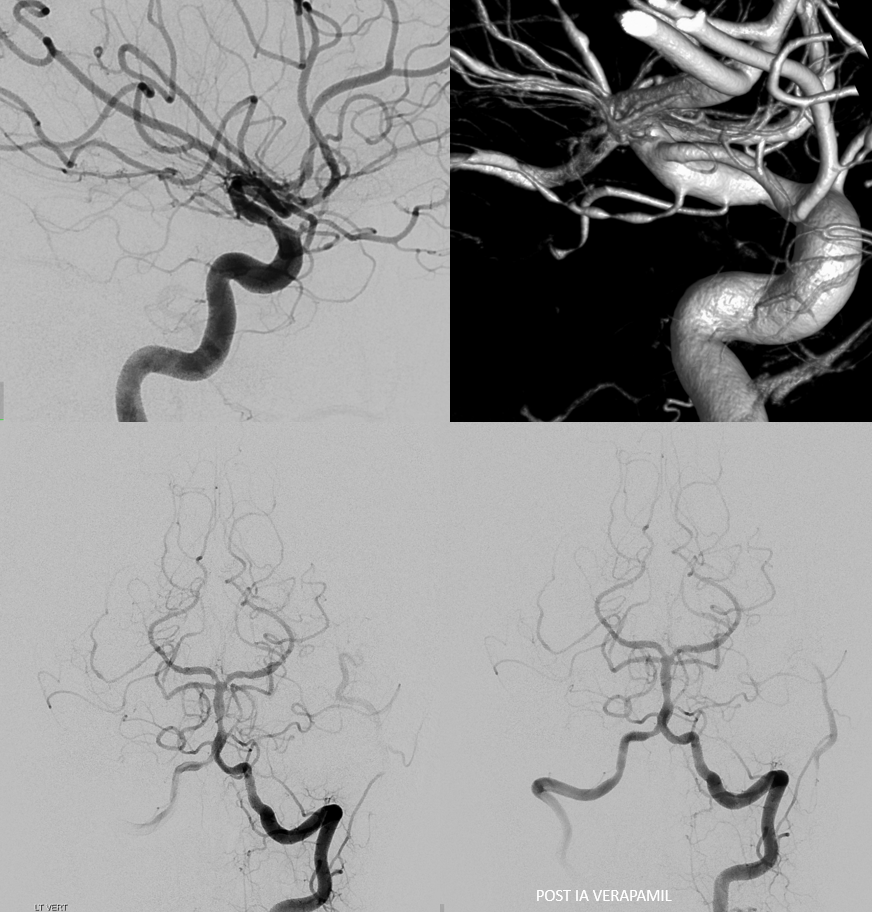
Typical DSA appearance of an anterior choroidal artery in stereo.
Typical appearance of the anterior choroidal artery (red). The red arrow marks the plexal point where the artery enters the choroidal fissure. A small artery distal to the anterior choroidal is present also (orange) These arteries ascend thru the anterior perforated substance and may supply areas of hypothalamus or optic tract — these are the arteries which hypertrophy in the Moya-Moya condition. An MHT branch is also present (blue)
Anterior Choroidal Projection — RAO projection (about 80-60 degrees RAO) of the RIGHT Anterior choroidal artery usually elevates the MCA branches away from the choroidal.
Frontal projection — the best projection for choroidal aneurysm is usually an ipsilateral oblique and somewhat submental. It is particularly good for visualizing choroidal artery origin when associated with an aneurysm. For example, in this case the optimal coiling view of this left choroidal aneurysm is a steep left anterior oblique, somewhat Waters.
Red=A. Chor; Purple=plexal point; Yellow=choroidal segment
Territory
Balance and spectrum, as always. There are, broadly speaking, two choroidal territories — parenchymal and intraventricular/choroidal. Below we are talking about the parenchymal one.
It is basic knowledge that infarcts of the anterior choroidal artery can lead to hemiplegia, due to its participation in supply of the posterior limb of the internal capsule. Other potential deficits include various homonymous field cuts (optic tracts, lateral geniculate), hemisensory deficits (lateral thalamus), non-primary motor movement changes, such as relief of rigidity and less often tremor from classic surgical ligations of the choroidal artery in patients with Parkinson’s disease (globus pallidus interna and ansa reticularis).
As with other vessels, the clinical syndrome of anterior choroidal artery occlusion will be determined by 1) size of territory supplied by the choroidal in each individual case, which is highly variable and 2) availability of collateral support. There is definite value to memorizing the structures which could be potentially supplied by the artery, but it is silly to expect choroidal occlusions to produce a particular deficit related to one of these areas. Some choroidal occlusions are nearly asymptomatic, while others can be devastating, for the above reasons. More details on choroidal artery distribution can be seen below, including examples of when the choroidal persists in supply of the posterior temporal territory that is normally annexed by the PCA.
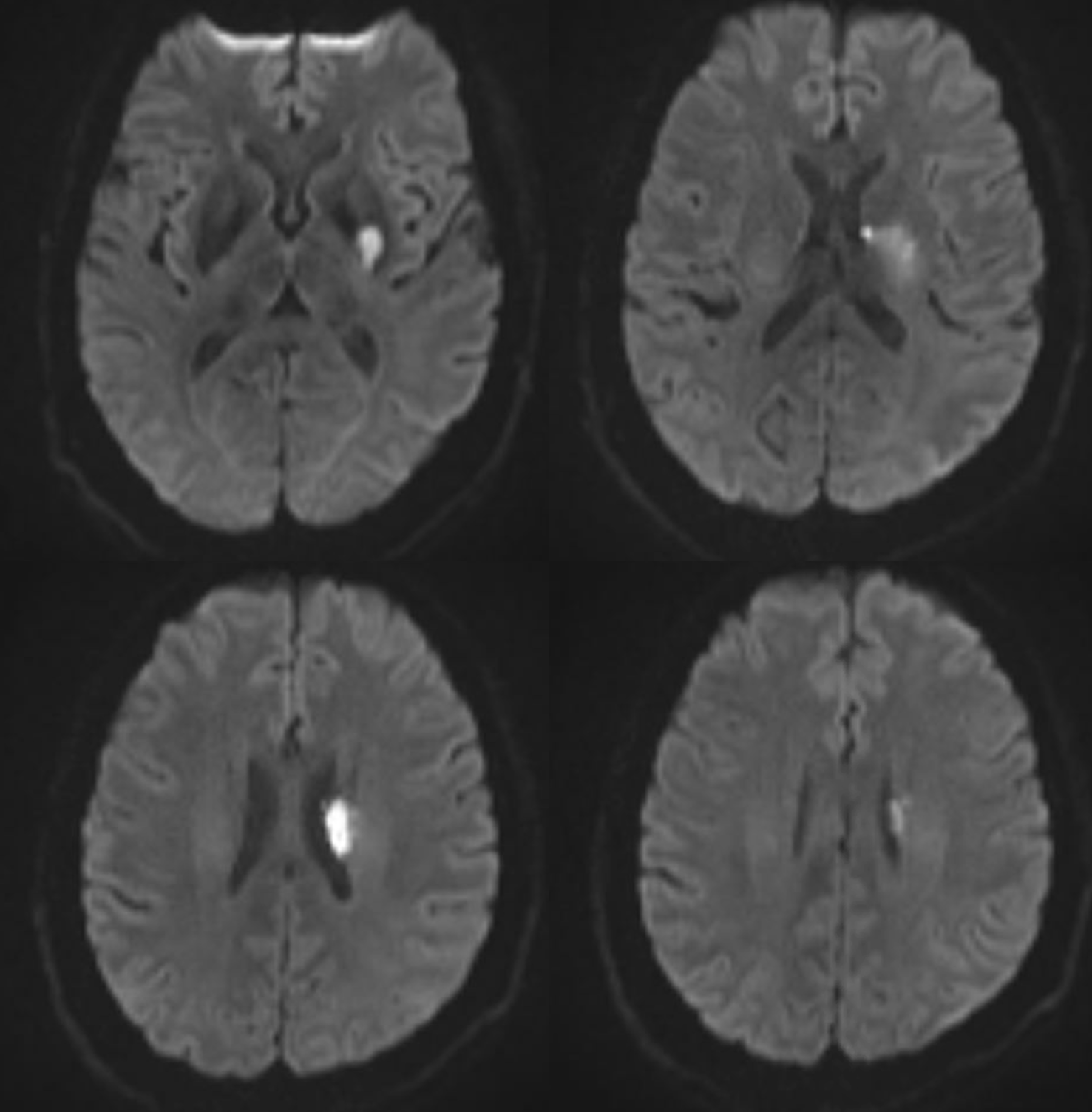
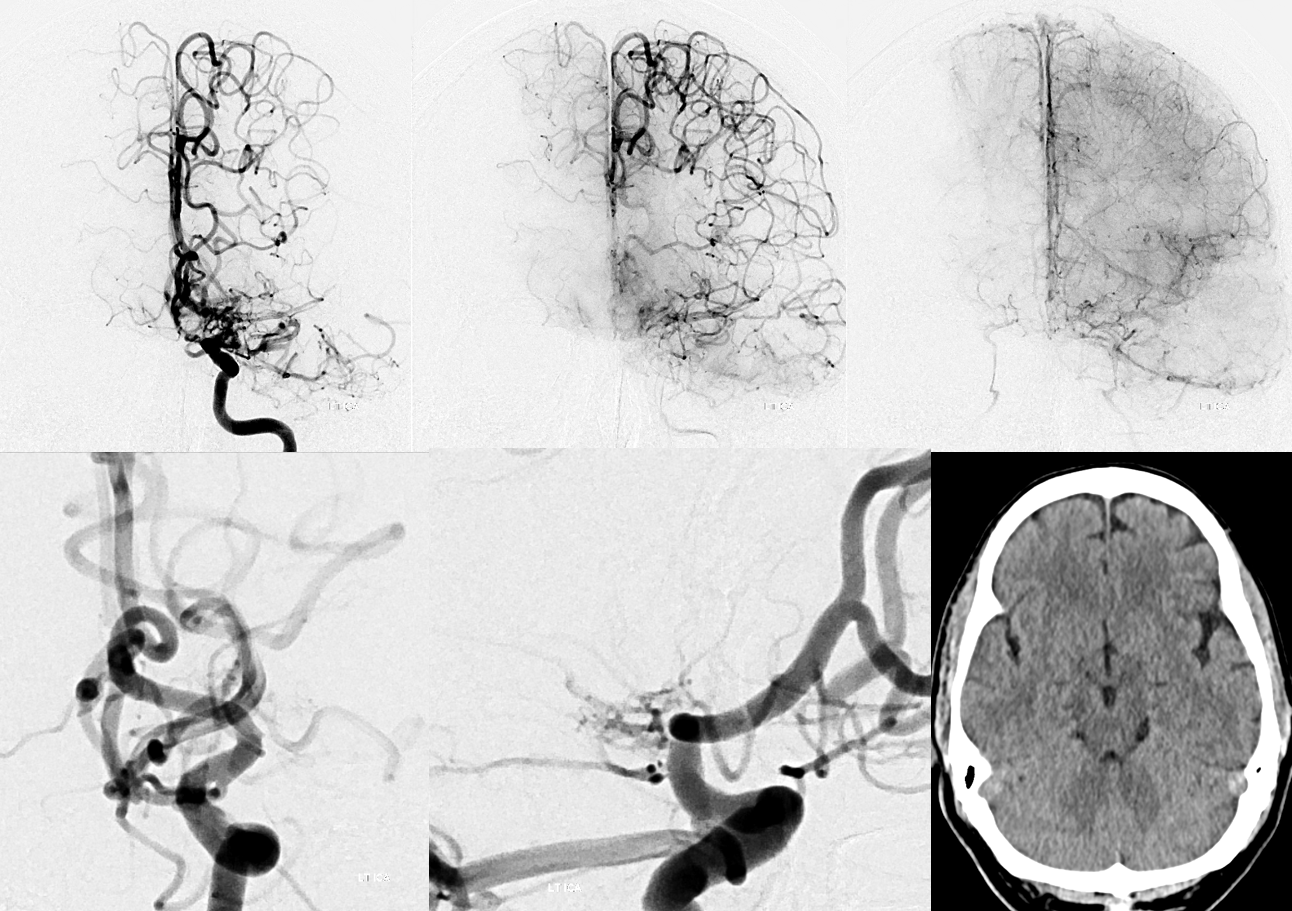
For the above reasons, trying to establish the definitive choroidal territory is not a project prompted by wisdom. What is important is to recognize the reverse — when you see an infarct pattern — think of what single vessel it might be. Below is a “classic” choroidal infarct. The point is not that they all will look like that — but if you see this pattern, think choroidal
In the following patient with a ruptured perinidal choroidal aneurysm, global and microcatheter injections demonstrate the more typical course of the distal choroidal artery, just proximal to its plexal point, through the expected region of the posterior limb of the internal capsule.

A post-nBCA CT scan confirms the course of the vessel through the posterior limb, with the index hemorrhage

Anterior Choroidal-PCOM confusion
One of the more embarrassing and potentially hemiparetic misidentifications is to mistake the anterior choroidal for a PCOM. This is especially critical in surgical cases, where a PCOM aneurysm may be treated by sacrifice of the PCOM (unless it turns out to be the anterior choroidal)
The anterior choroidal is labeled in red, whereas a small PCOM, arising more proximally, is marked with orange arrows. On the AP, you can see the hemispheric portion of the A Chor in red, and the choroidal portion in purple.
Anterior Choroidal Artery capturing PCA cortical territory
As a consequence of embryonic participation of the choroidal artery in supply of cortical territory in many mammal species, there is occasionally encountered a variant whereby the choroidal artery supplies the territory typically served by the Posterior Cerebral Artery.
As we always do on neuroangio.org — think spectrum of variation. There will be a spectrum of PCA takeover by the choroidal. The more common instances of this uncommon variant will be partial takeovers — most commonly the inferior temporal branches. The progressively larger territory takeover will be correspondingly rarer still. The least common is complete takeover — see below.
The most commonly encountered variant captures territory of the inferior temporal branch, which supplies the undersurface of the temporal lobe. The parieto-occipital and calcarine branches typically originate from their “usual” positions. It is important not to confuse this variant with by thinking of it as a “duplicated PCOM, or duplicated choroidal”. There can be only one PCOM and one choroidal. Here are MRA and angio examples from same patient
Red=PCOM/PCA; Yellow=Anterior Choroidal Artery
Another example, courtesy Dr. Howard A. Riina, with temporal branch labeled with black arrows
Cross-eye stereo lateral
Frontal cross-eye stereo
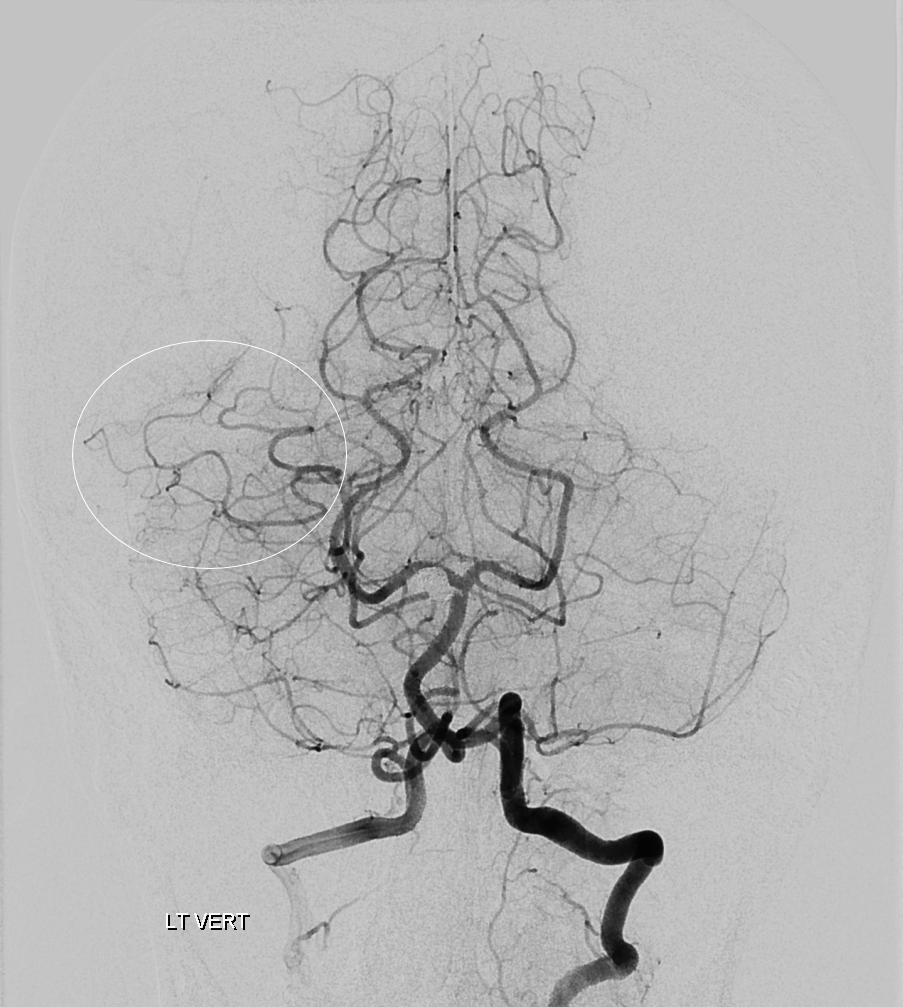
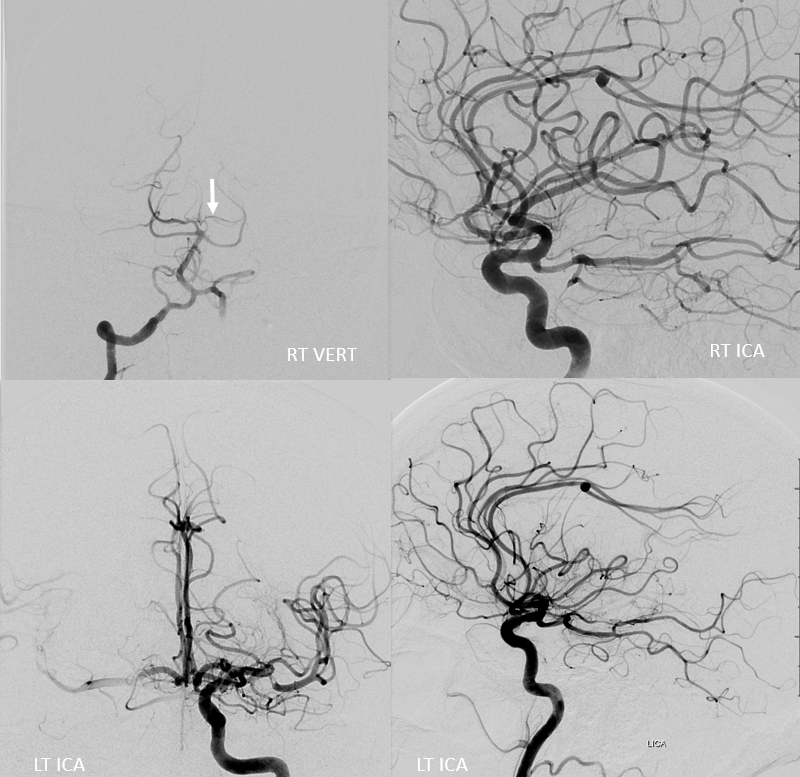
Vertebral artery injection shows lack of inferior temporal branch on right, which is present on the left (black arrow)

Another example, with an aneurysm. It is critical not to mistake this choroidal aneurysm for a PCOM — surgical or endovascular sacrifice of PCOM ostium with a good P1 backfilling it is very well tolerated. Choroidal sacrifice is a different story. There are plenty of examples of the latter.
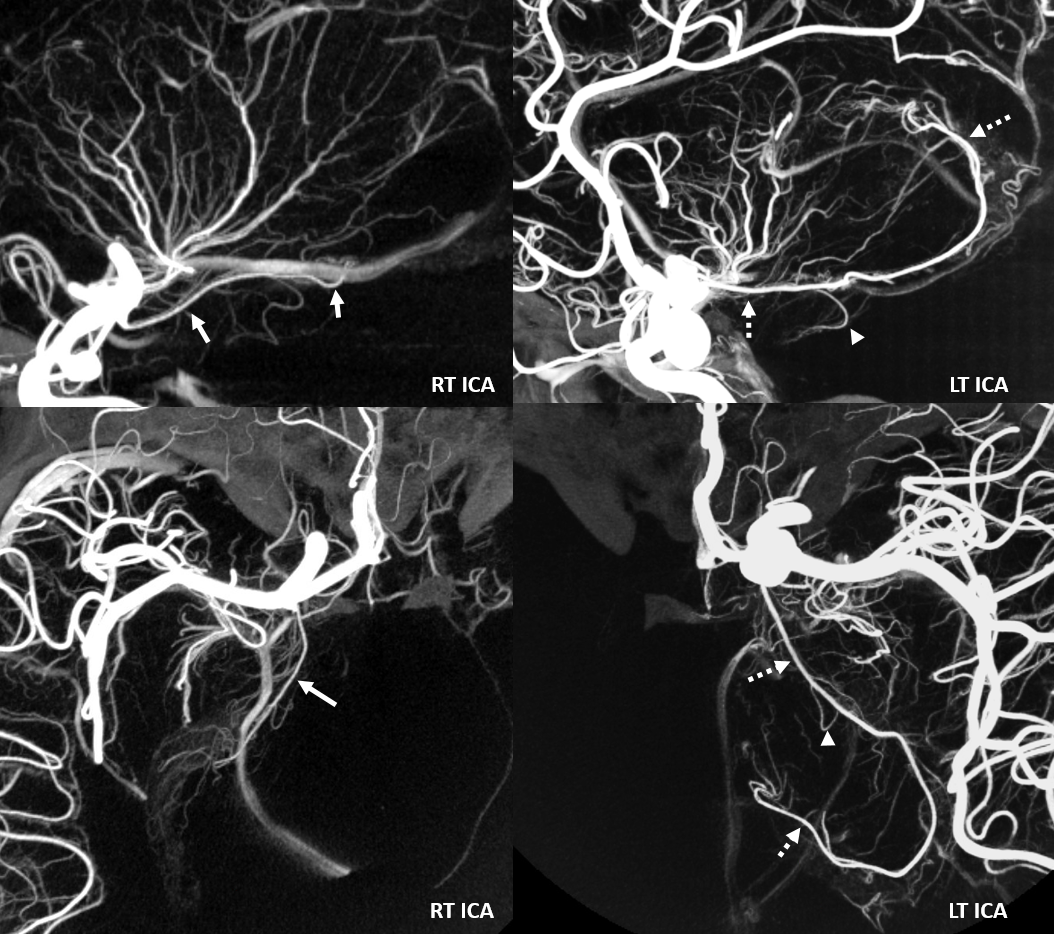
Here is a vert injection — notice that inferior temporal branches are missing on the left (normal ones inside oval on right)
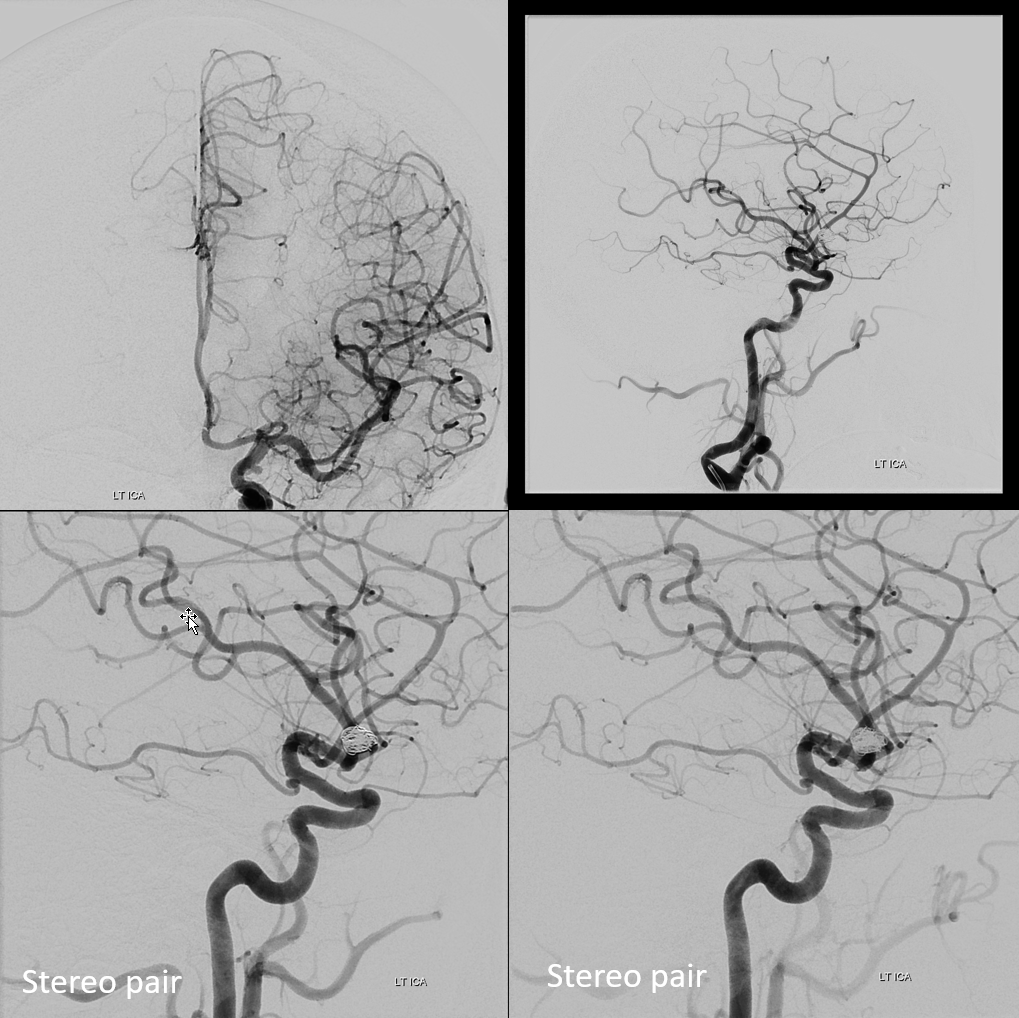
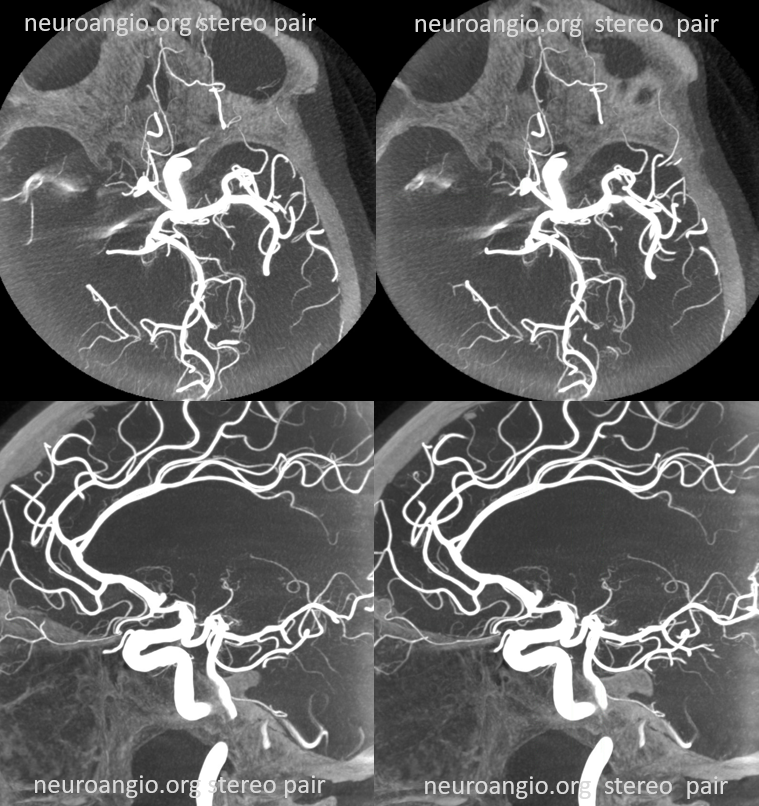
Global frontal and lateral views on top, cross-eye stereos on bottom
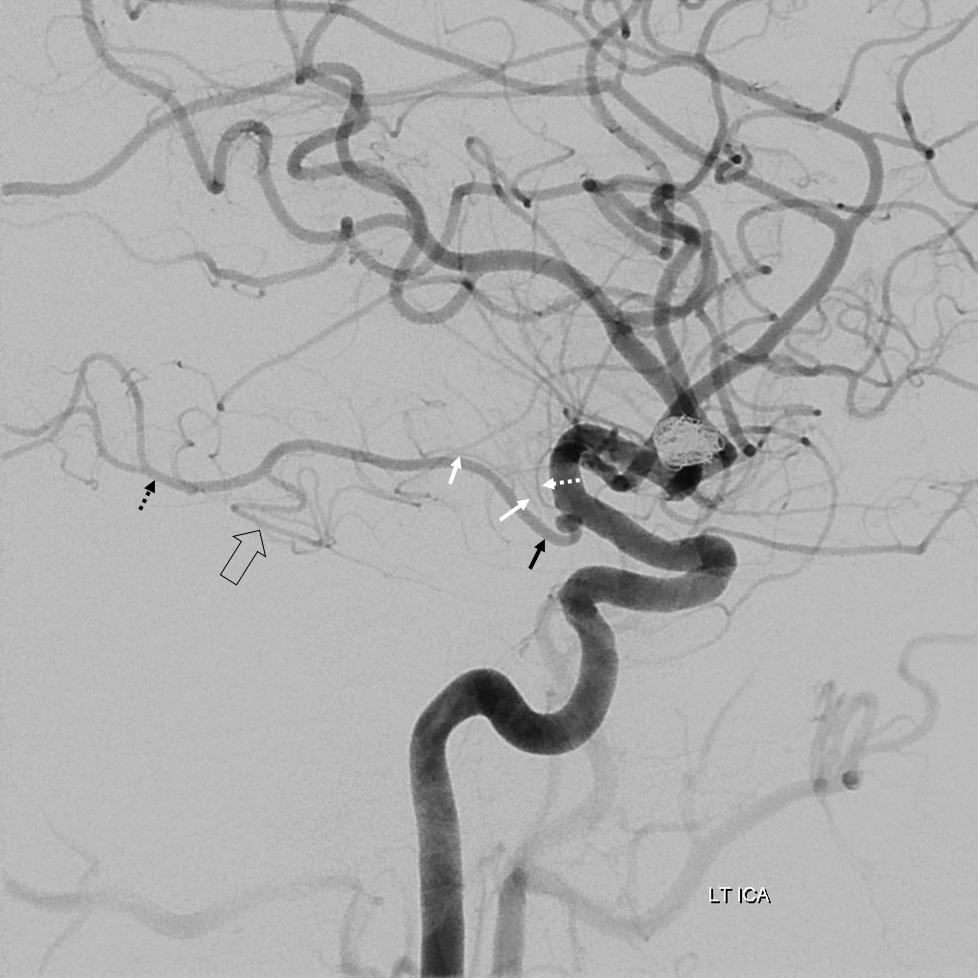
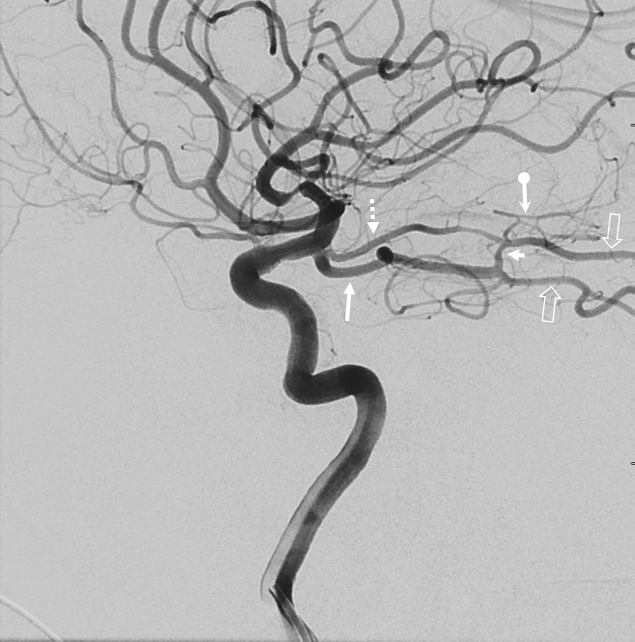
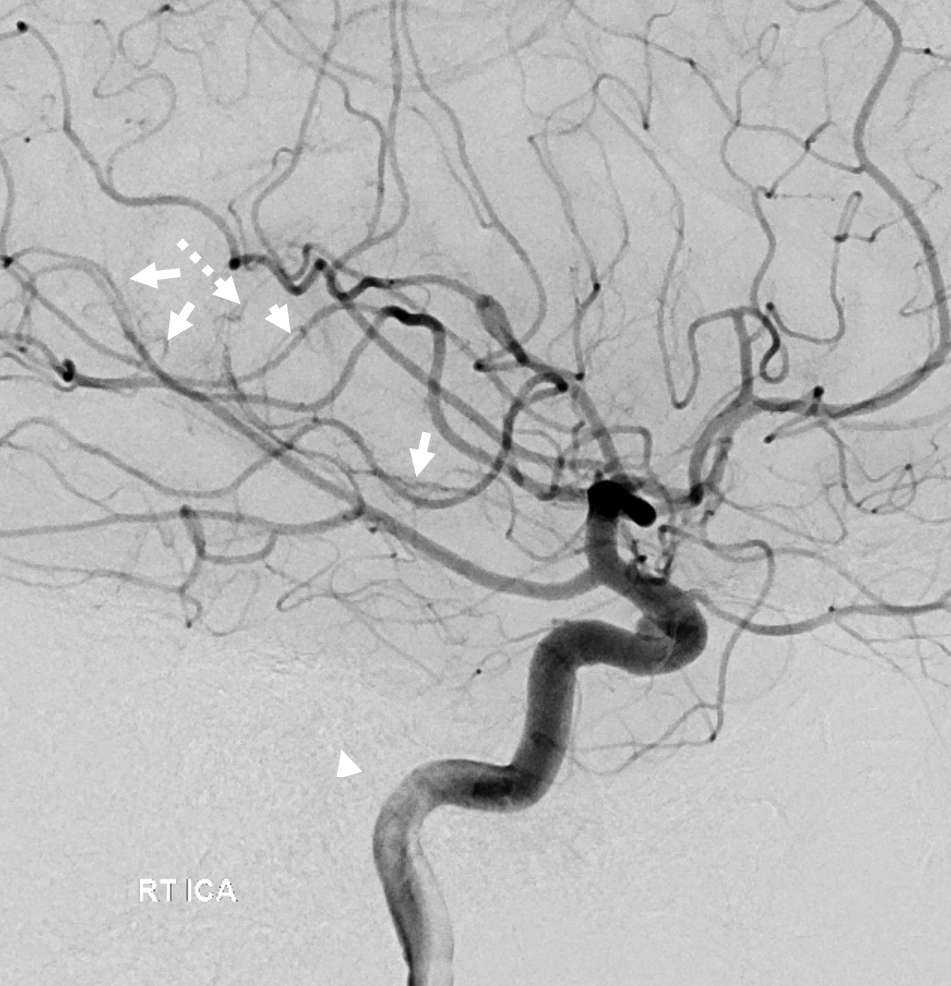
Lateral oblique. Typical course of the choroidal artery (black arrow). There is no “wash-in” from P1 segment — tells you that that either this should be a fetal PCOM, or that this is a choroidal. Several perforators are seen coming off choroidal (white arrows) and one separately from the more distal ICA (dashed white arrow). Do not confuse this for “duplicated anterior choroidal artery” — there is no such thing . By definition a choroidal artery is one that goes to choroid plexus — the rest are perforators off ICA — they may be eloquent, but they are not the choroidal artery. The posterior inferior temporal branch is marked by dashed black arrow. Middle inferior branch by open black arrow.
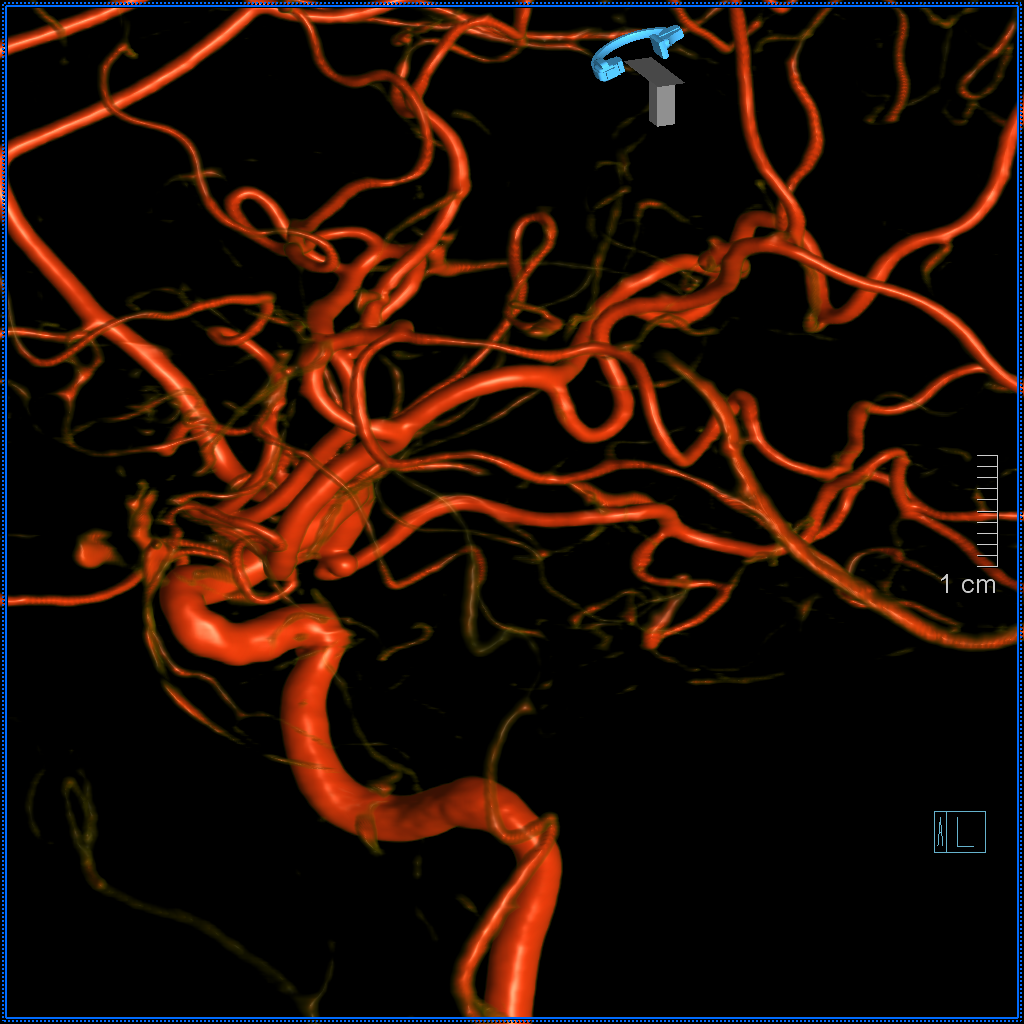
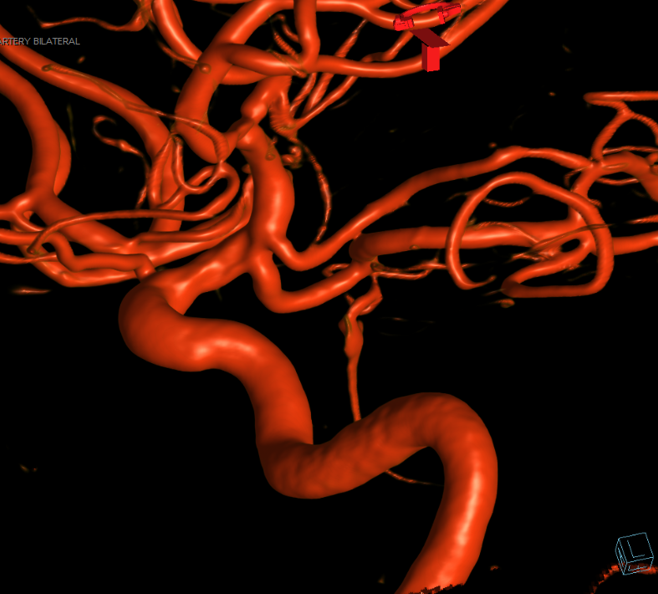
VR
Anaglyph VR stereo
Hard to figure out on MRA prospectively, but it is there, separate PCA (black) and choroidal (white). No PCOM
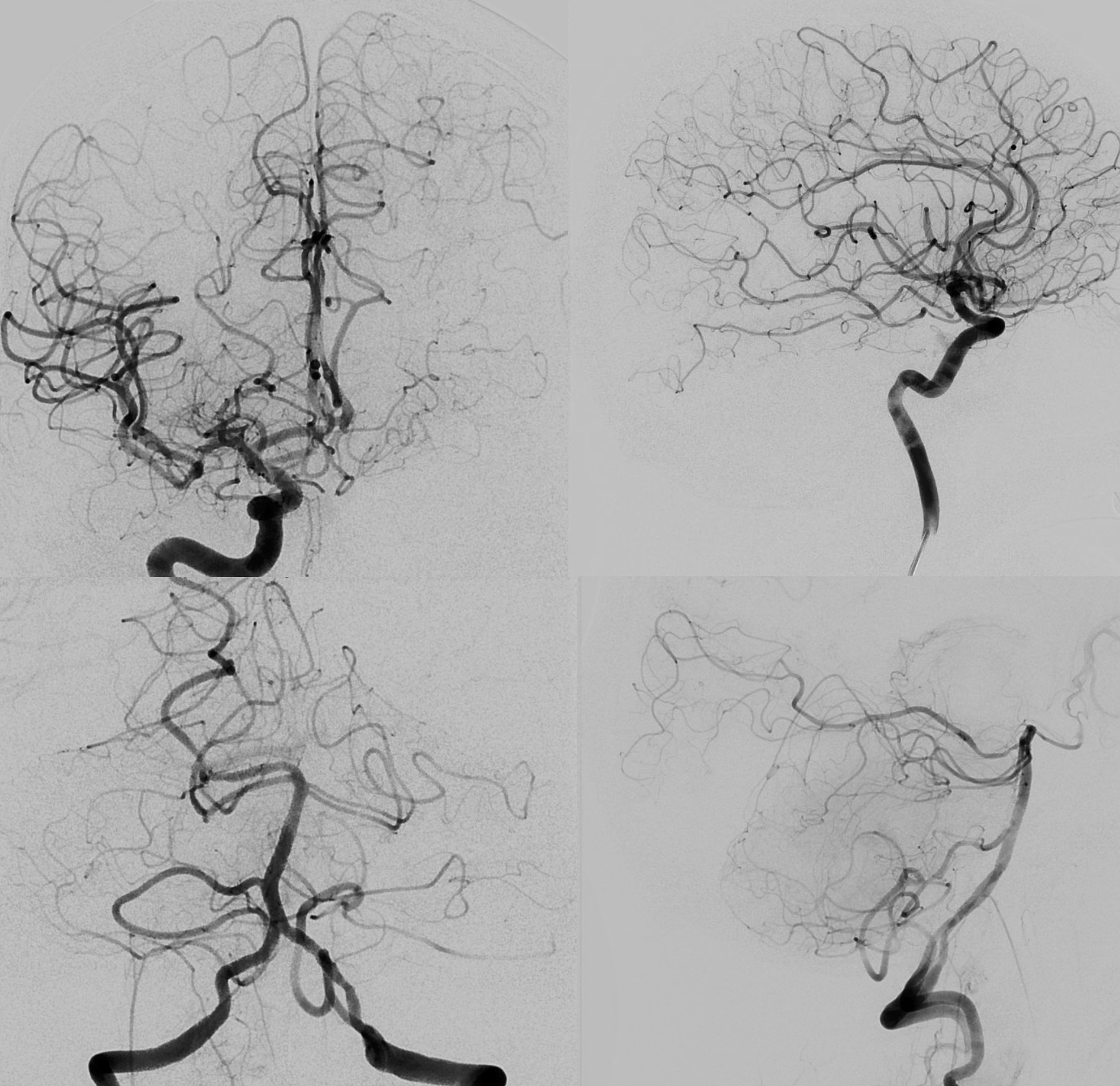
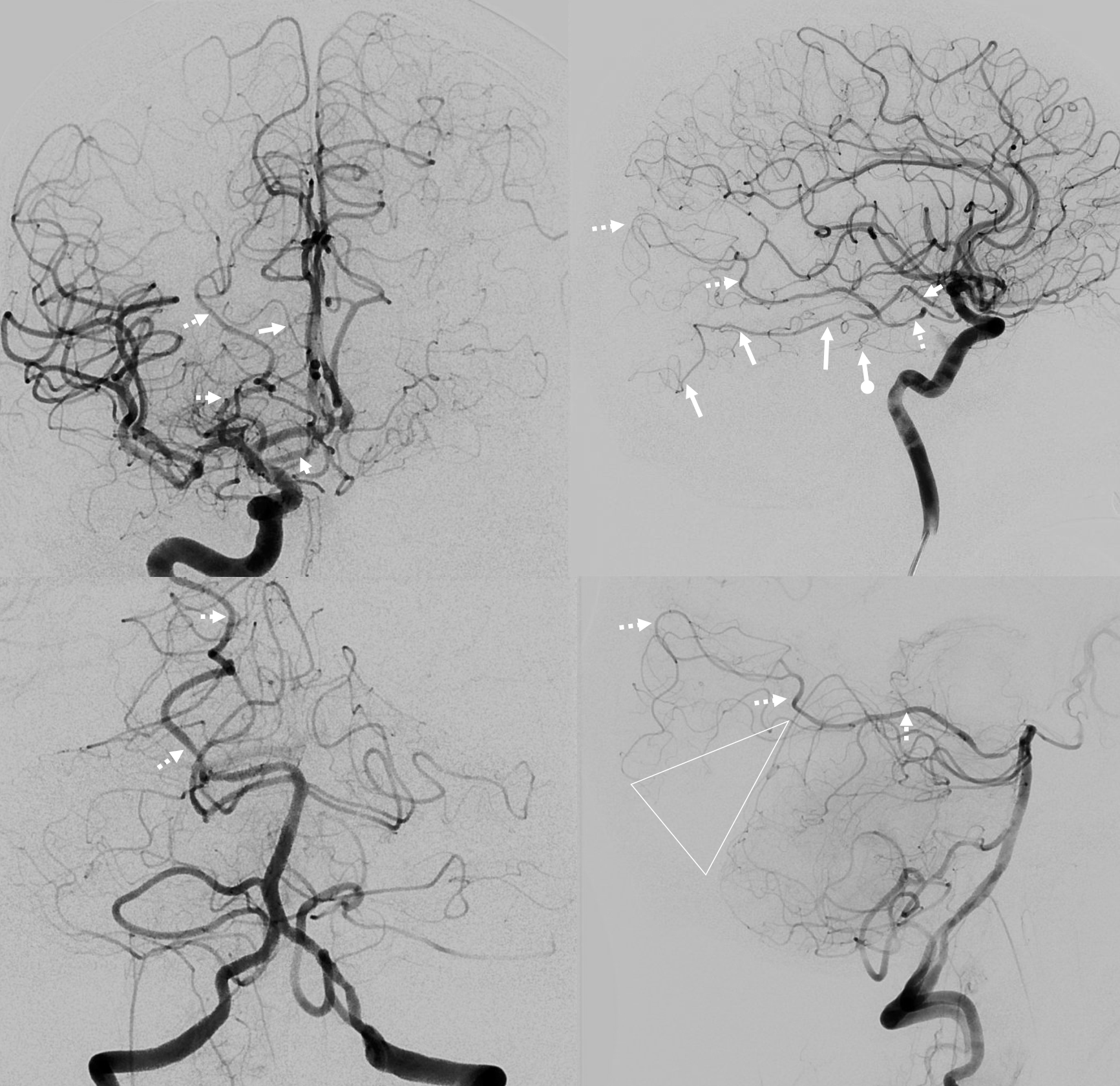
Choroidal supply of Calcarine and Inferior temporal territories — case of Eytan Raz MD PhD
A lot less common than inferior temporal takeover — see spectrum idea above. This is not exact science. Recognized cases number in single or double digits. The full takeover (below) is also extremely rare. This is just a general idea of how to think about it.
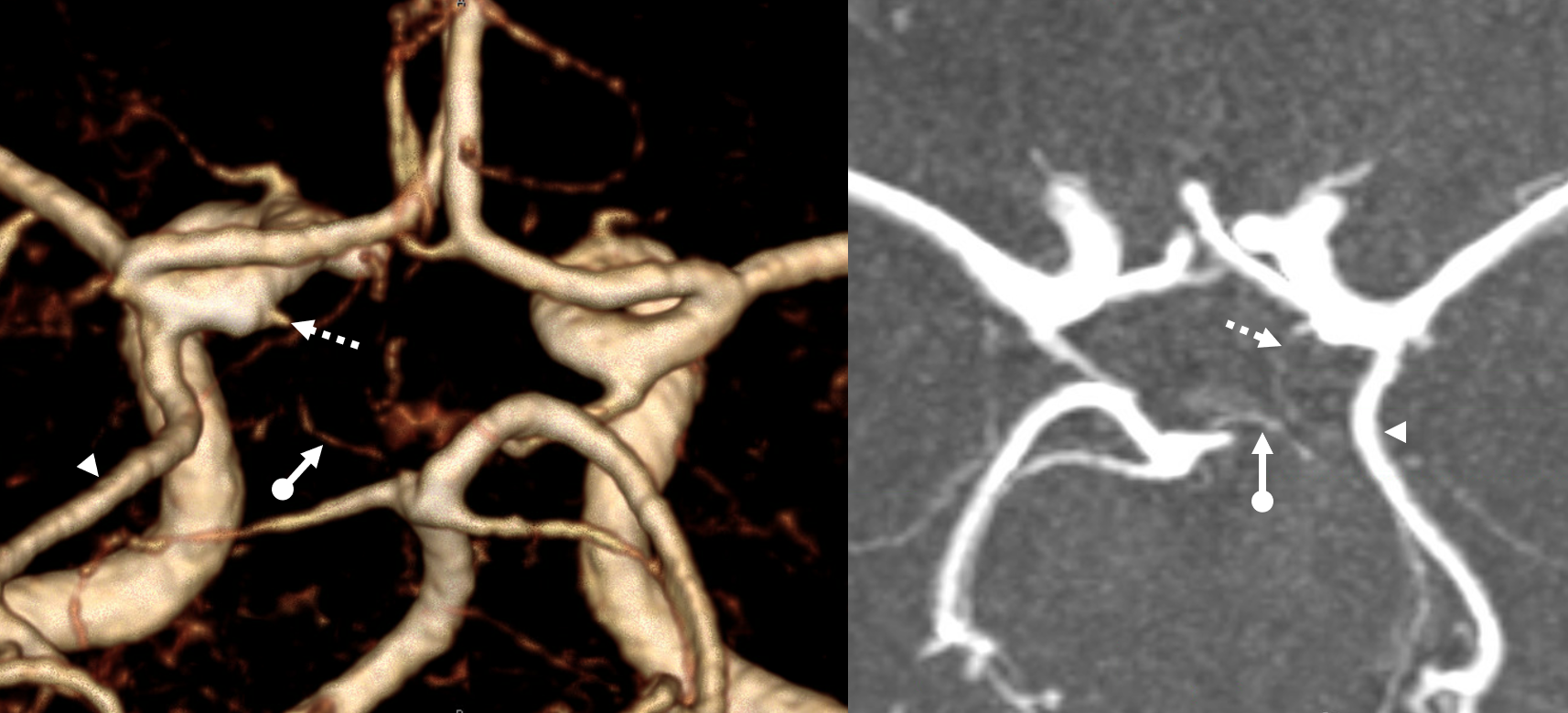
Without labels
With labels — choroidal = arrowhead; calcarine = arrows; inferior temporal = ball arrow; PCOM / P1 dual supply parieto-occipital branch = dashed arrows. Extremely rare
Full Choroidal takeover of PCA territory
Much rarer than partial choroidal supply of inferior temporal PCA branch only. Again, as we often say, there is a spectrum here — partial takeovers are more common than complete ones. Not easy to recognize this one sometimes — that choroidal looks very much like a fetal PCOM. But very important. Here is an example — image on left is without labels, and might just look like a fetal PCOM. Its not. On right image, small true PCOM (white arrow) and “choroidal artery” (black arrows) — the whole trunk is choroidal though — with full choroidal supply of PCA
Vert injections label the same PCOM (white arrows). Images on top are same carotid injection in early and late phases — with more choroidal blush in upper right image
Cross eye stereo pair
Anaglyph stereo
Post Pipeline stereo — very nice! Choroidal not covered

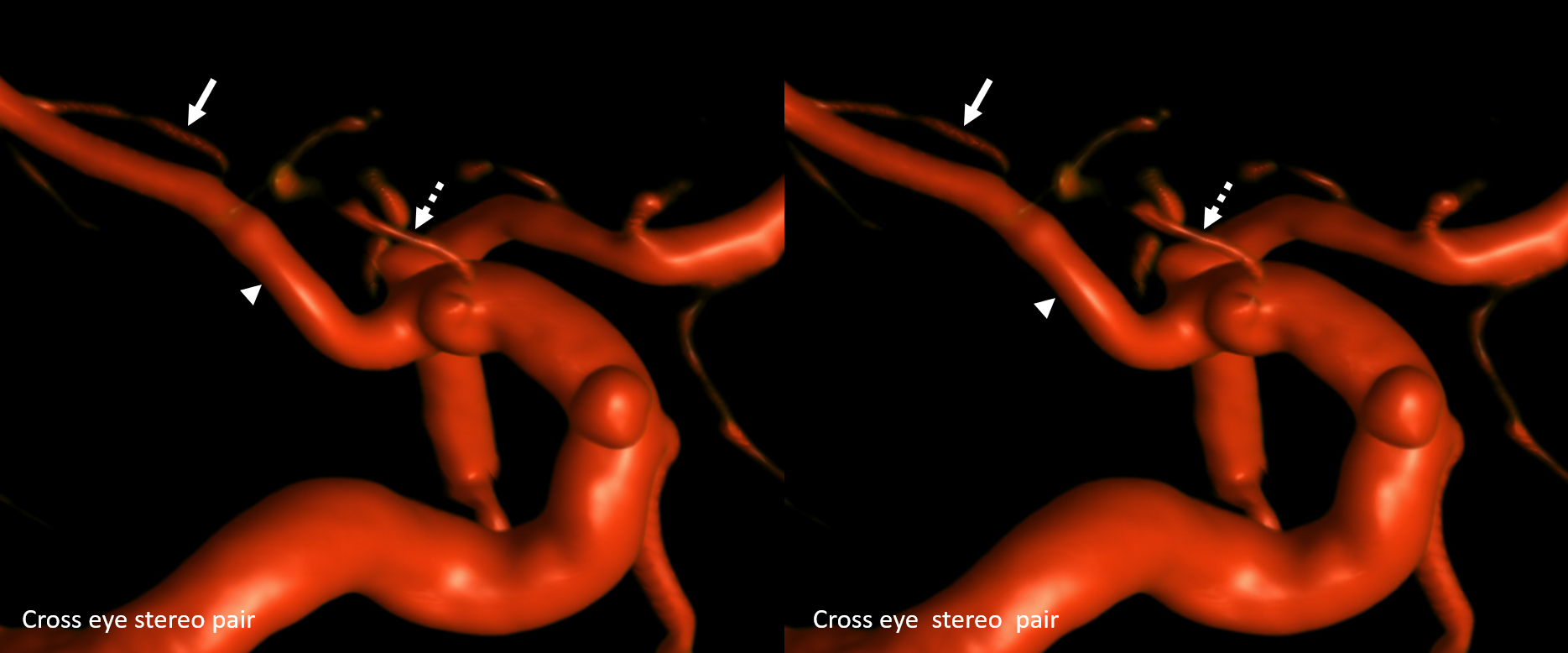
Another example — hard to recognize, especially without good projections. In this case only standard projections are available, and there is no vert injection. Hard to say on this lateral view:
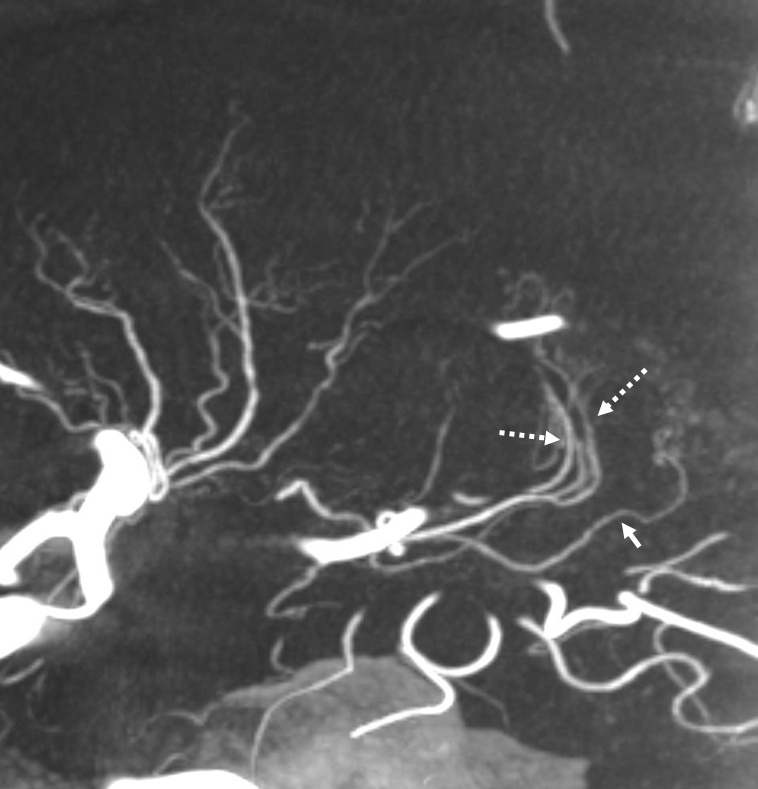
Fortunately, the VR images are common now. Here, we see a small PCOM-like vessel — limited to its thalamic supply likely (dashed arrow), while the large vessel (arrowhead) is the choroidal supplying whole PCA. The choroidal branch to the plexus is shown by solid arrow.
Magnified lateral projection — the proximal nature of the PCOM anterior thalamic vessel is lost here
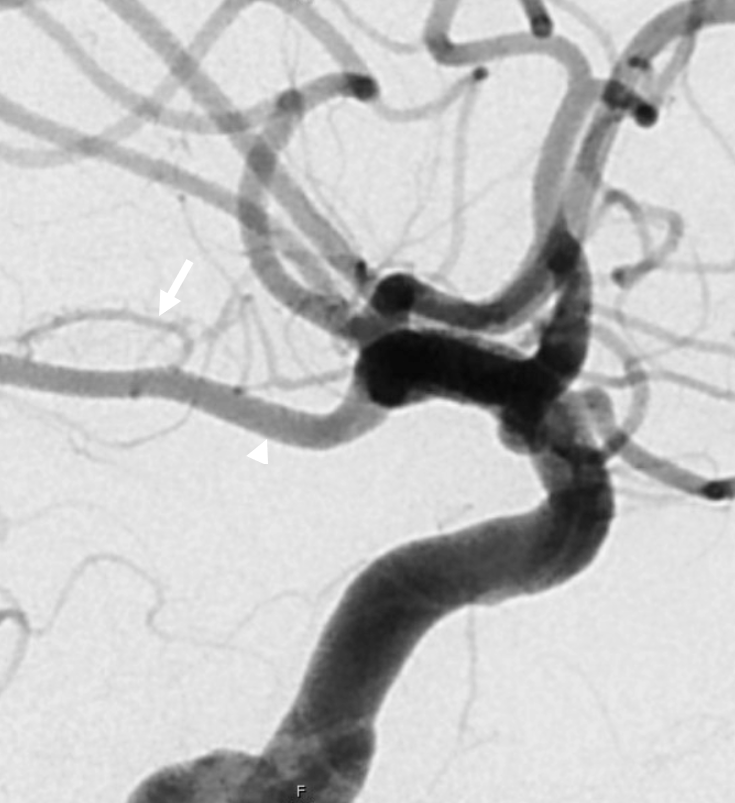
Some information may be gleaned from MRA — there is a stump of PCOM origin and a small probably circumcullicular branch (ball arrow)
Moral is look carefully…
Common trunk PCOM and Anterior Choroidal
Super rare. But very real. And can be extremely clinically important as well — again, not to mistake an anterior thalamoperforator for choroidal artery — both are eloquent of course but in very different ways.
Here is a case courtesy Drs. Frédéric Clarençon and Eimad Shotar, Department of Neuroradiology, Pitié-Salpêtrière Hospital, Paris, France
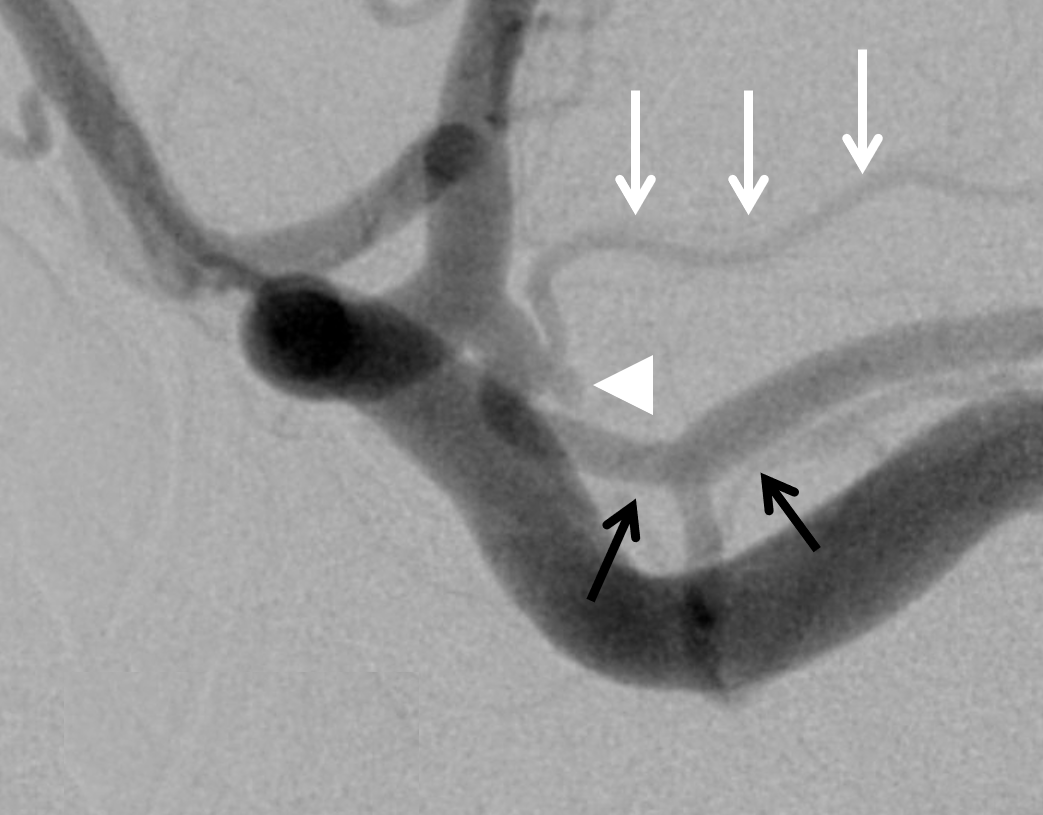
Presentation is SAH. Cause is a tiny aneurysm at the bifurcation of common origin PCOM (black arrows) and choroidal (white arrows). Don’t see the aneurysm — its very tiny indeed and superimposed on the PCOM in this straight lateral
Here it is (white arrowhead), in an oblique view. Pretty neat diagnosis, huh?

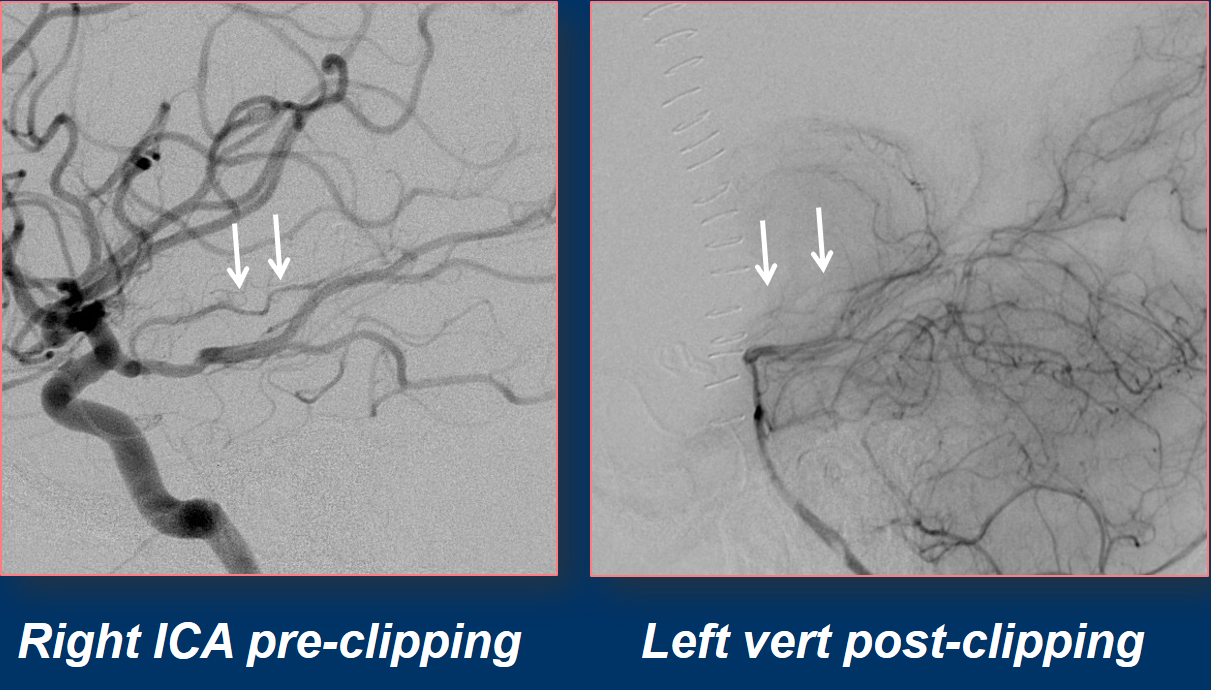
The aneurysm is clipped. Despite best efforts, the choroidal is lost (image on right). However, the patient is asymptomatic 🙂

Why? The choroidal backfills via the posterior lateral choroidal system! Extremely rare for collateral to actually rescue the choroidal — but here it is…

Look at the vessels side by side. What a great case!
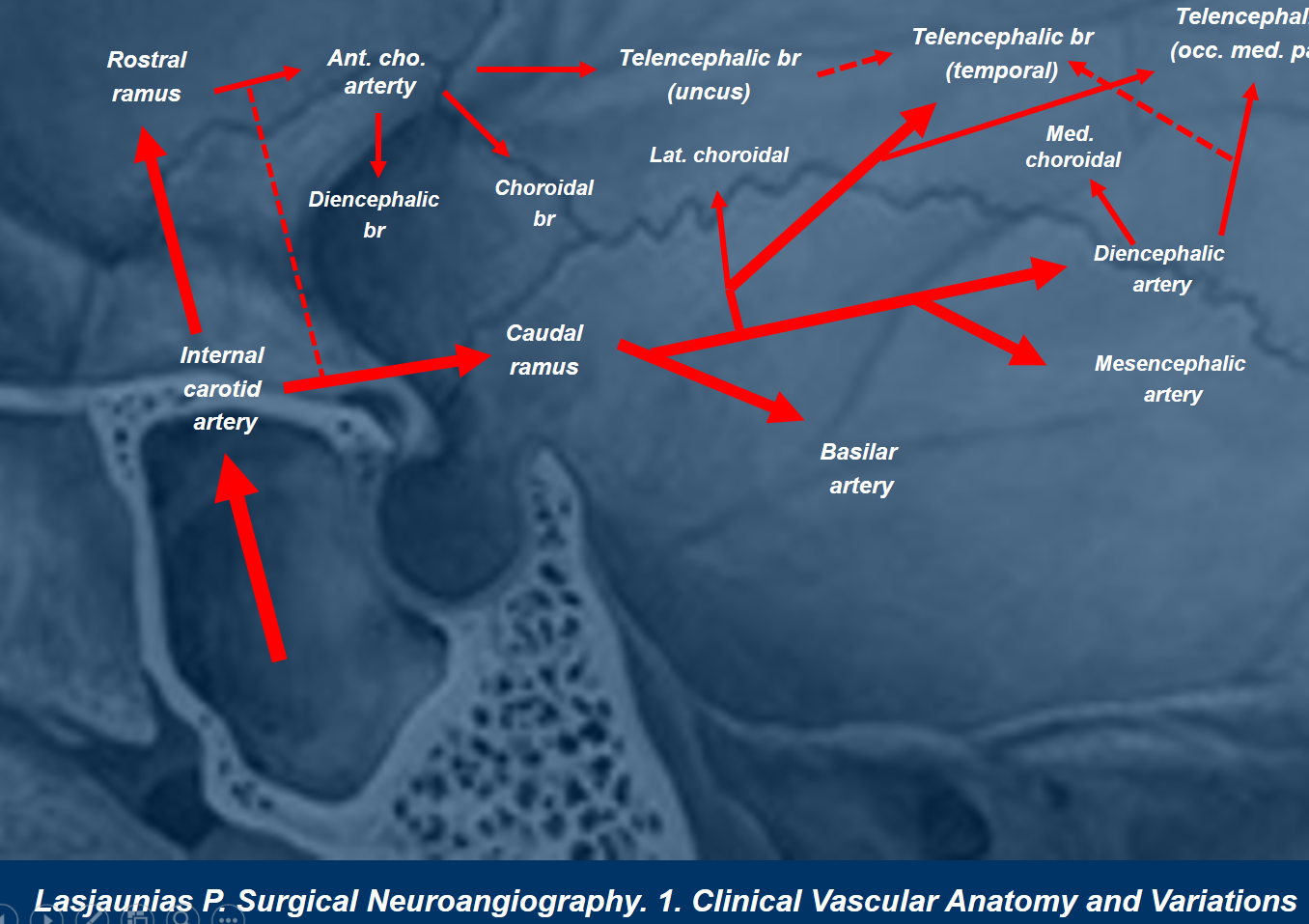
According to Lasjaunias, as illustrated by Dr. Clarencon, the embryologic mechanism responsible for common pcom/choroidal origin is related to persistence of some less typical anastomoses between PCOM and Choroidal vasculature, is as follows:
If you think this is a one-time occurence, of course no. Below is a case courtesy Dr. Caleb Rutledge. Note an additional more cranial small perforator, best seen in lower left image, likely supplying mesial temporal lobe. This one was not covered by the Pipe.

Here is another instance of common PCOM/Anterior Choroidal origin, now on MRA, Dr. John Loh and Dr. Eytan Raz
Choroidal is white arrow
VR
MIP
Choroidal-PCOM fusion
Another super rare variant, also explained by embryology above. Cases below courtesy Dr. Eytan Raz
In this very rare variant, there is a connection between choroidal and PCA at the level of P2. How to think of it? It is on the spectrum of choroidal persistence in supply of PCA territory — part PCA is from choroidal, part from PCOM/P1 — except that there is a connection between the two at P2 segment.
There is a small left P1 (white arrow). The right ICA is “normal”. Left ICA standard projections are also unrevealing
Oblique lateral projection view of left ICA – PCOM is white arrow, proximal choroidal is dashed arrow, distal choroidal is ball arrow, connection between choroidal and PCOM origin PCA is arrowhead. Distal PCA branches are open arrows. Clearly there is a choroidal-PCOM “ring”
Volume rendered image, same case
Another case of same, on CTA, also courtesy Dr. Eytan Raz
PCOM (arrow) and choroidal (dashed arrows) fusion at P2 segment (open arrow) to produce a slightly larger caliber PCA (arrowhead)

Volume Rendered image of same. The PCOM is very faint and thus really cant be seen here. But, there is a nice ACOM fenestration 🙂
QUIZ TIME!!! What is happening on the left side? History is vasculopathy, ultimately requiring stenting. The stents are not the point. The point anatomy of the left ICA reconstitution. Top images are a few months before bottom images

MRA from around the time of top images
Fusion post stenting of left vert and left ICA CBCTs — for the slower ones here
Anterior Choroidal origin proximal to PCOM
According to theory, anterior choroidal artery can never be proximal to the PCOM — the latter being the caudal ramus of the internal carotid artery (see neuroembryology). However, sometimes it just does, like in the example below, right? NO!! Fake! Below is a particularly convincing fakeout.
Loot at this frontal view, and you will understand. The choroidal below is labeled in RED

Proximal Anterior Choroidal=red; Choroidal segment of Ant. Chor = white; Parenchymal Ant. Chor. branches = yellow; PCOM=orange
Choroidal Plexus Supply
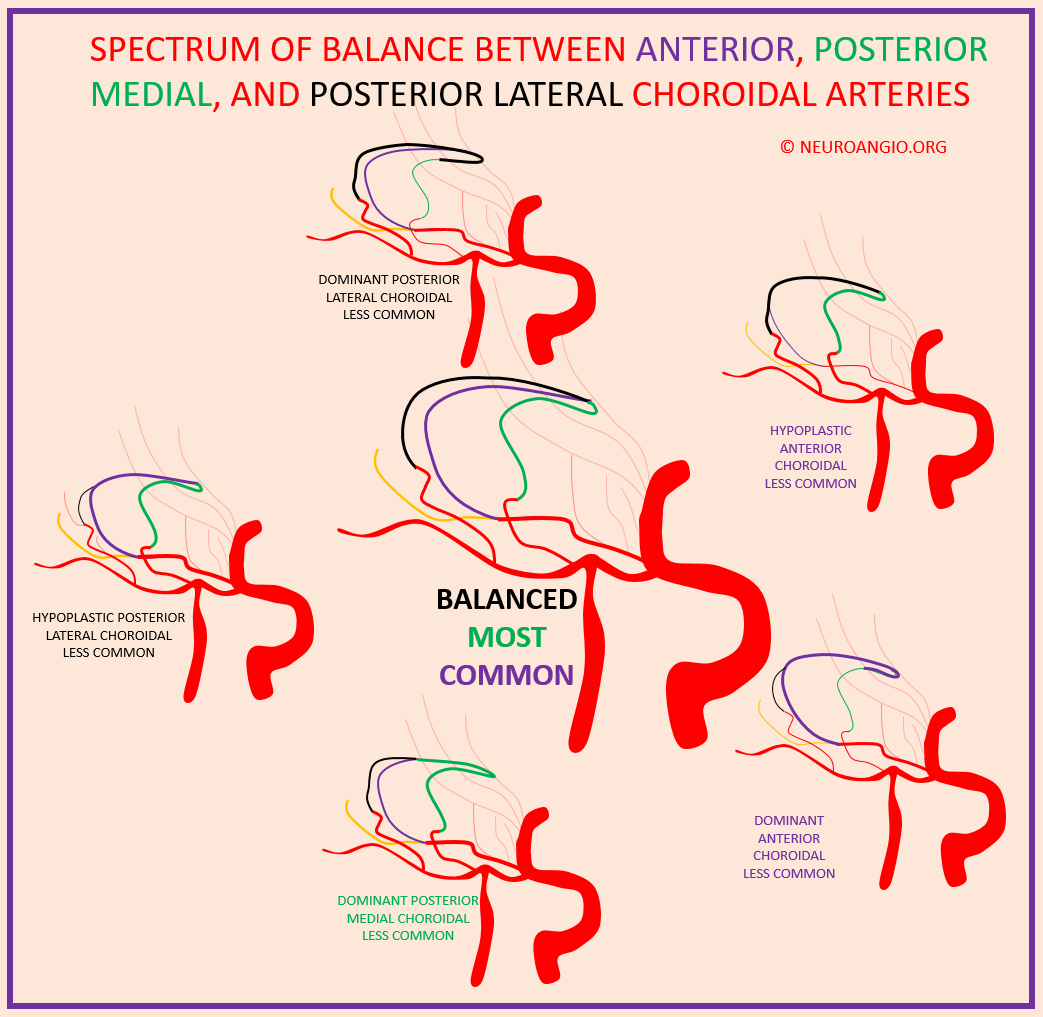
Spectrum and balance, again.
So, now we come to the second major territory of the anterior choroidal artery — the intraventricular one. Supply of choroid plexus. Which means that the balance will be between the other two arteries supplying the choroid — the posterior lateral choroidal (lateral ventricle), and posterior medial choroidal (third ventricle). The anatomical connection between the medial choroidal and anterior / posterior lateral ones is same as for the CSF — foramen of Monroe. The balance here does not have the same implications as parenchymal issues such as stroke. But it does have a role in supply of intraventricular AVMs and hypervascular tumors, for example.
The balance of supply is mostly expressed at the borders / watershed areas if you will, of the territories. Anterior Choroidal is mainly responsible for the temporal horn — it usually keeps that. The posterior lateral choroidal for the atrium. Posterior medial for 3rd ventricular plexus. The anterior choroidal is therefore in balance with the posterior lateral choroidal as both supply lateral ventricle. In practice, the more fluid balance is between the posterior medial and lateral choroidals, while anterior usually keeps is horn territory. Sometimes there are exceptions. For example, below is a large choroidal segment (arrow) extending into the atrium (notice also a large anterior thalamoperforator from PCOM — dashed arrow)
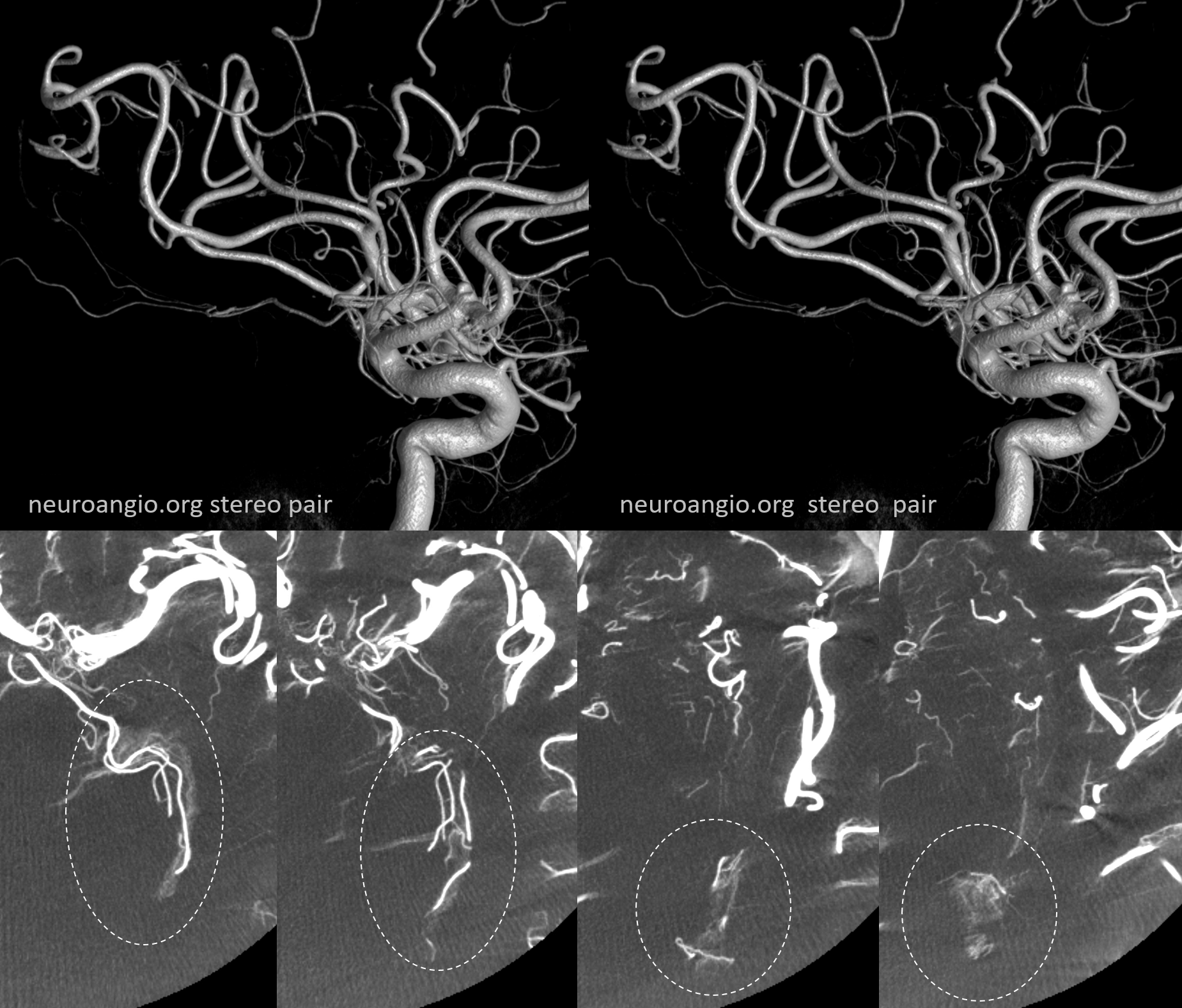
Stereos
Axial MIP showing supply of atrial choroid plexus (arrow)
The corresponding posterior lateral choroidal is hypoplastic (arrow). Note how little of the distal anterior choroidal prominence can be seen on DSA
Another example of choroidal balance
The anterior choroidal contribution to lateral ventricle choroid supply is small (white arrowheads). The corresponding dominance of posterior lateral choroidal (yellow dashed arrows) is present. Also seen is a large posterior medial choroidal (yellow arrowheads). Also balanced are hypoplastic median callosal artery (white arrows) and correspondingly large posterior pericallosal artery (white dashed arrows)

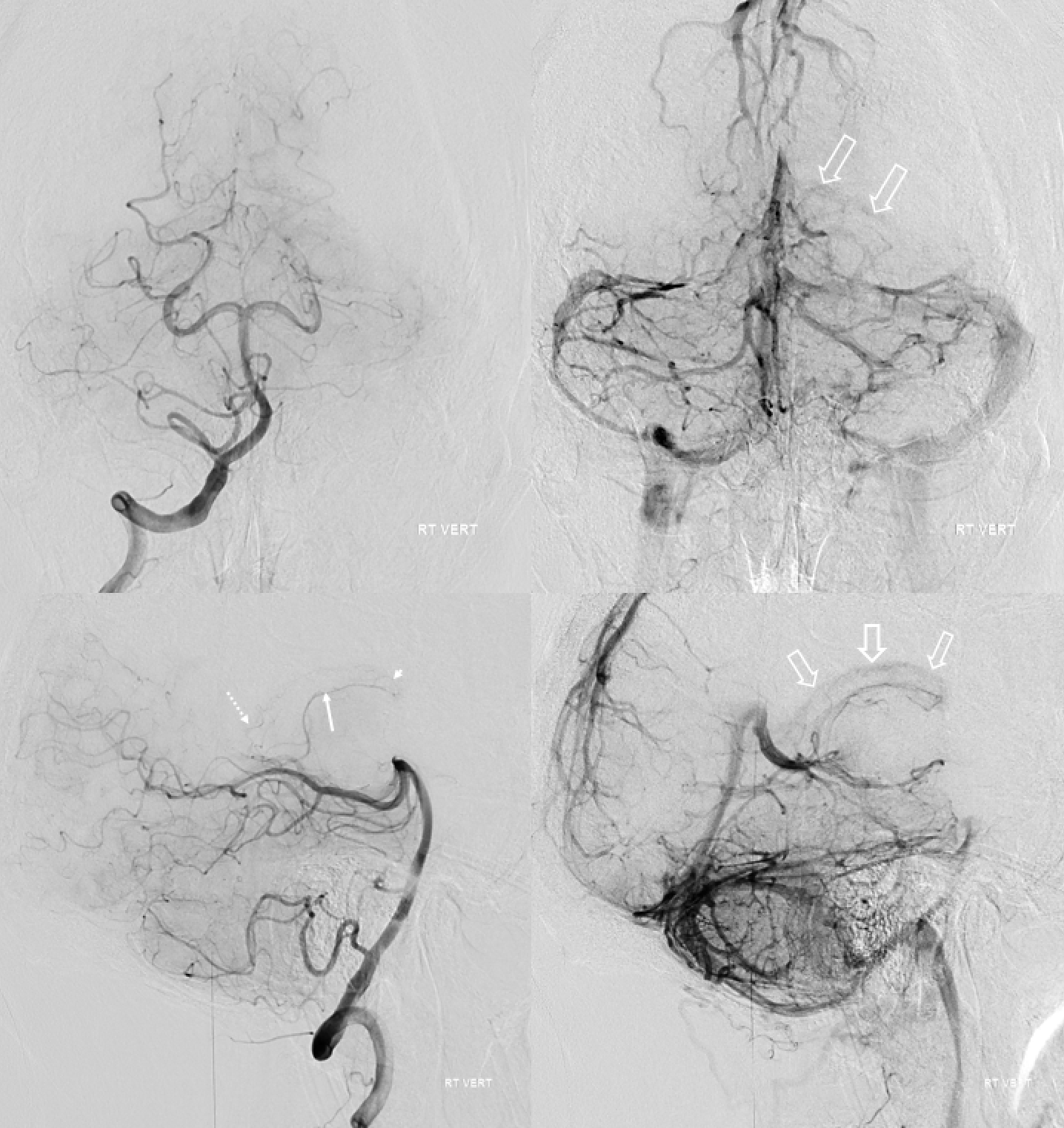
Collateral Supply of the Anterior Choroidal
Infrequently, the intraventricular anastomoses between posterior lateral and anterior choroidal arteries are sufficient enough to allow anterior choroidal resupply in case of latter’s occlusion. This is usually not the case though. Parenchymal branches of the anterior choroidal have very poor collaterals — one similarity with the lenticulostriates.
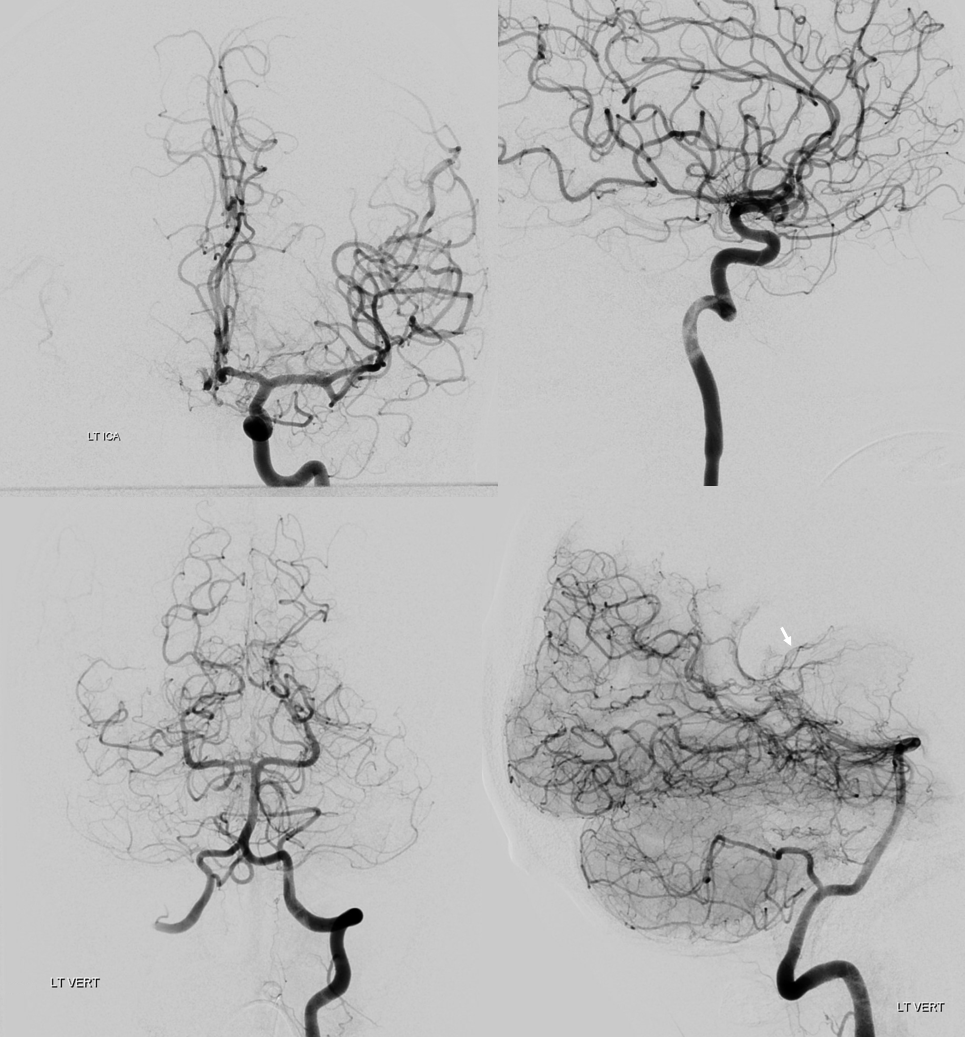
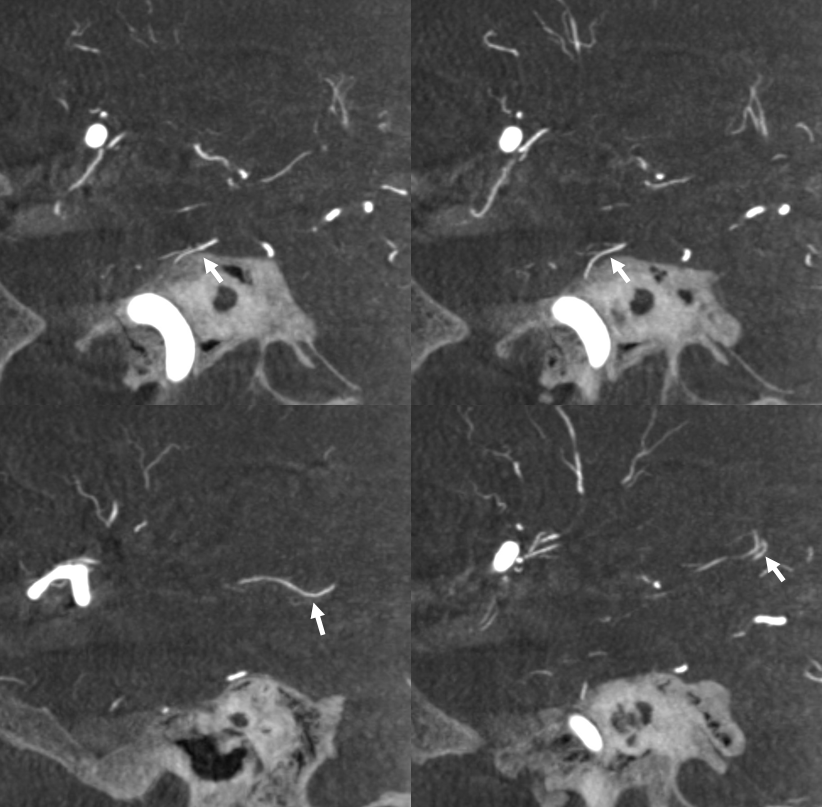
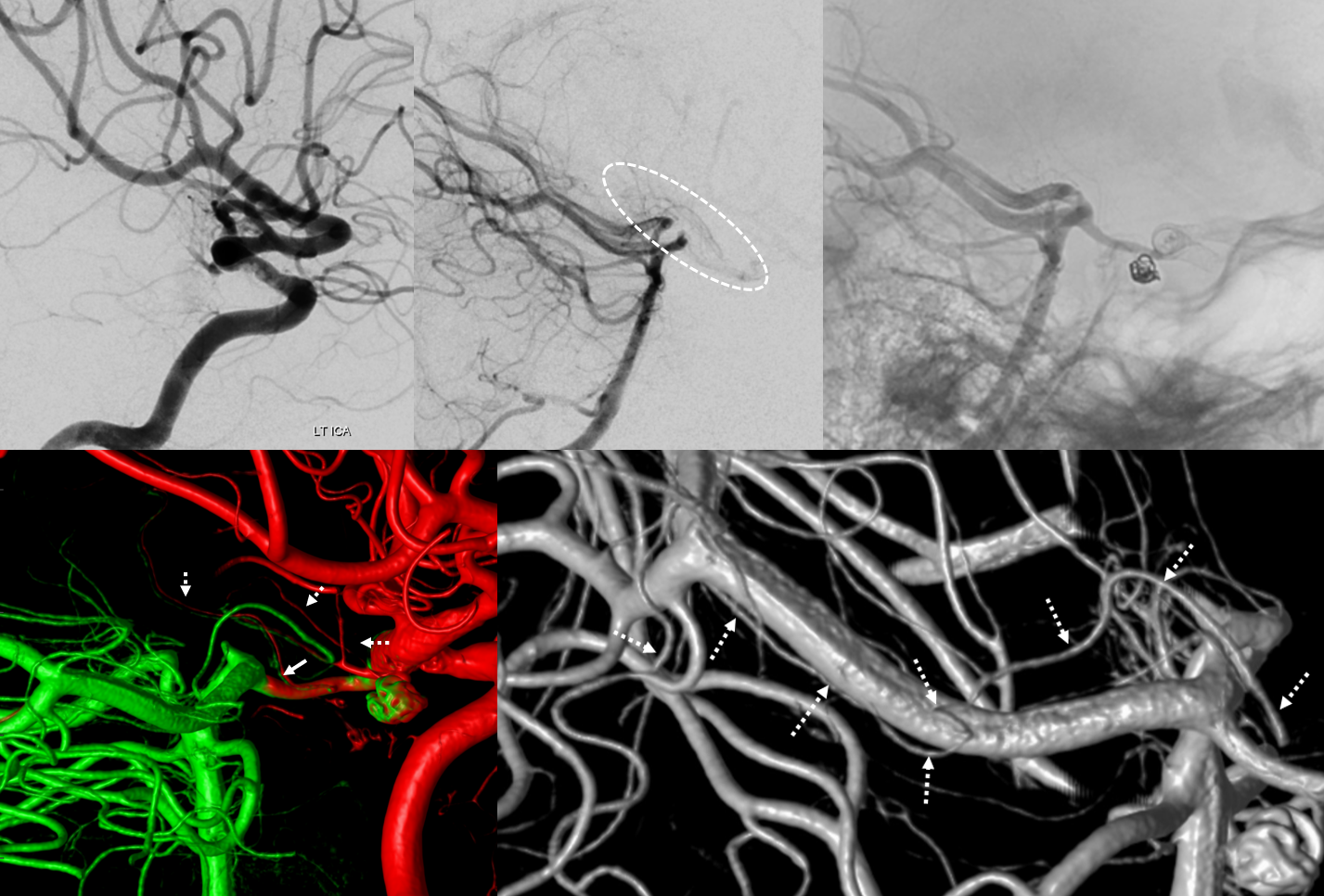
This is an example of posterior lateral choroidal reconstitution of the anterior choroidal artery in setting of treatment. There is thrombus in the ICA. The proximal choroidal is open (left top image). Center top image shows reconstitution of some branches in the PCOM-Choroidal area. Top right image shows retrograde filling of the PCOM. Bottom left image — fusion of HR-CBCTs — the fusion is imperfect, allowing one to see side by side the green of the vertebrobasilar injection and red of the carotid. The anterior choroidal region (dashed arrows) and PCOM thalamoperforator (solid arrow) are seen. Bottom right image traces the course (dashed arrows) of the posterior lateral choroidal reconstituting the anterior choroidal
Plexal Point Dogma and Reality


AP and Lateral views (Stereo pair on top) of a temporal lobe avm with deep anterior choroidal supply component.
Anterior Choroidal – Posterior Lateral Choroidal anastomosis — the anterior choroidal beyond the plexal point supplies the plexus of the temporal horn, where it is in balance with the posterolateral choroidal going to the atrium region. This is elegantly shown in the following case of left choroidal plexus AVM, supplied by both vessels with beautiful illustration of draining veins.
Red=anterior choroidal; yellow = posterolateral choroidal; pink=choroidal vein; light blue=inernal cerebral vein; brown=basal vein to sylvian veins; dark blue = atrial vein; white = superior petrosal sinus; green = midbasilar agenesis