
Here we show how to obtain highest quality DYNA CTs of the Pipeline Device and, if desired, use fusion methods to create a “superDYNA” — combining excellent resolution of noncontrast DYNA of the deployed Pipeline and the pre-deployment high-resolution full contrast DYNA of the vessels
The patient presents with extensive subarachnoid hemorrhage. CTA and 2D DSA are negative

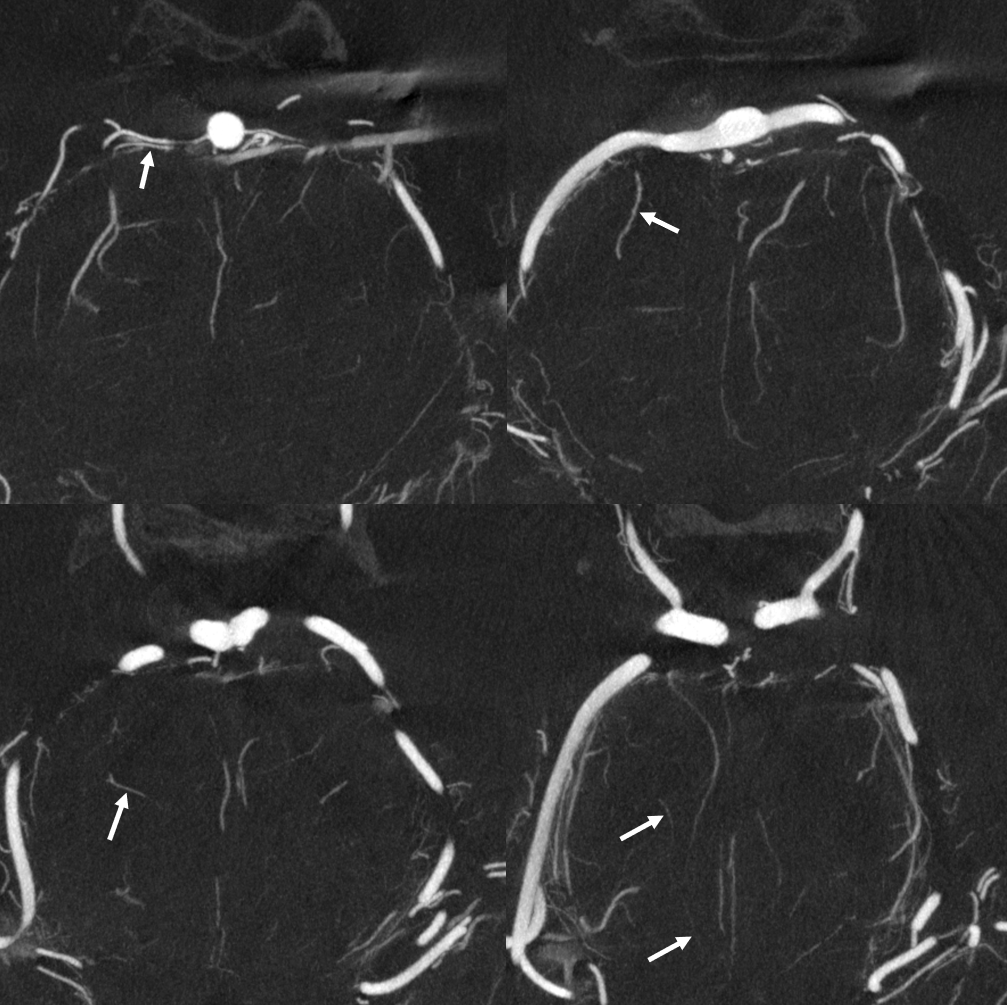
DYNA CT shows a basilar perforator aneurysm. It is small but very real and is the cause of the SAH
This is a Siemens Q 20 second DYNA CT 22 FOV non-binned “micro DYNA”. Injection rate is 3.5 cc/sec for 77 ccs and 2 sec delay, with secondary reconstruction

Ten days later, repeat DYNA CT (not as good an injection due to spasm), it is clear that the aneurysm (open arrow) is larger. ALso note inflow from the left PCOM (ball arrow), suboptimal opacification of the basilar artery due to inflow from the right vert (dashed arrows) with poor opacification of the left SCA (arrows)

After further 3 weeks, the aneurysm persists, which is extremely unusual — likely persisting due to the large size of the perforator supplying a large portion of the midbrain (arrows).
Decision is made to treat with Pipeline Device. The 2D-DSA shows persistent mild spasm more than 6 weeks post hemorrhage, as is typical if you look carefully. Verapamil or similar is typically given by us before Pipeline to make sure we do not undersize or change later

A 20 second DYNA CT is obtained — 22 cm FOV micro dyna unbinned acquisition. To ensure highest quality, put the region of interest in the center. GA, pharmacologic paralysis, and apnea are mandatory for highest quality images. Injection must reflux into the other vert to result in homogeneous opacification (not like what you saw above). Rate = 3 cc/sec for 66 ccs, 2 sec delay
This is the primary reconstruction
Its pretty good, but much better can be done — secondary reconstruction — small FOV, “sharp” mode. The result is much better. The aneurysm persists and is very real.
Stereo views (top row) and MIP images. Plan is to deploy the Pipe below the SCAs, as the origin of the branch is about 1.7 mm below them.
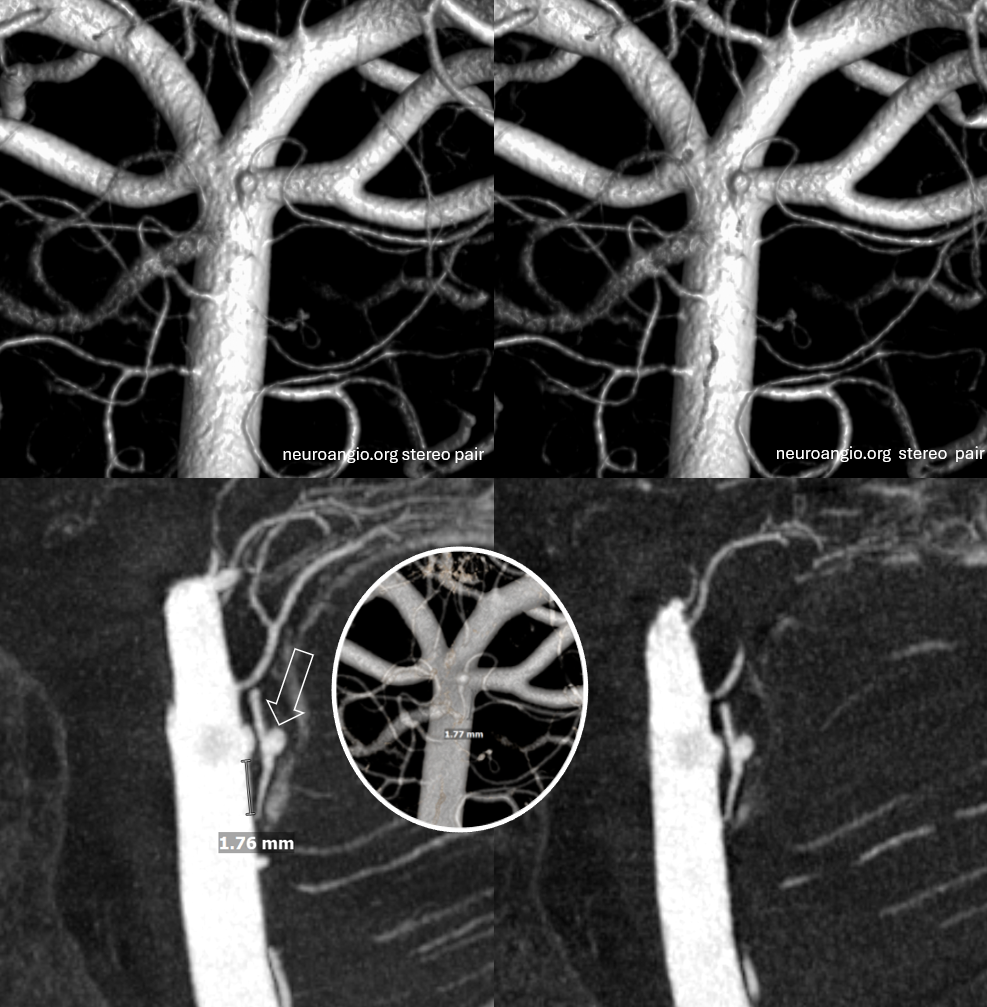
“Cinematic Rendering”
Post PED. Tools: Shuttle 5F 90 cm; Catalyst 5F 132 cm (maximum ID in 5F system to allow for injections through the CAT during PED deployment), Phenom 27, Aristotle 14 standard, Pipeline Shield 3×10.
Did we do well? Time will tell, but placement is good
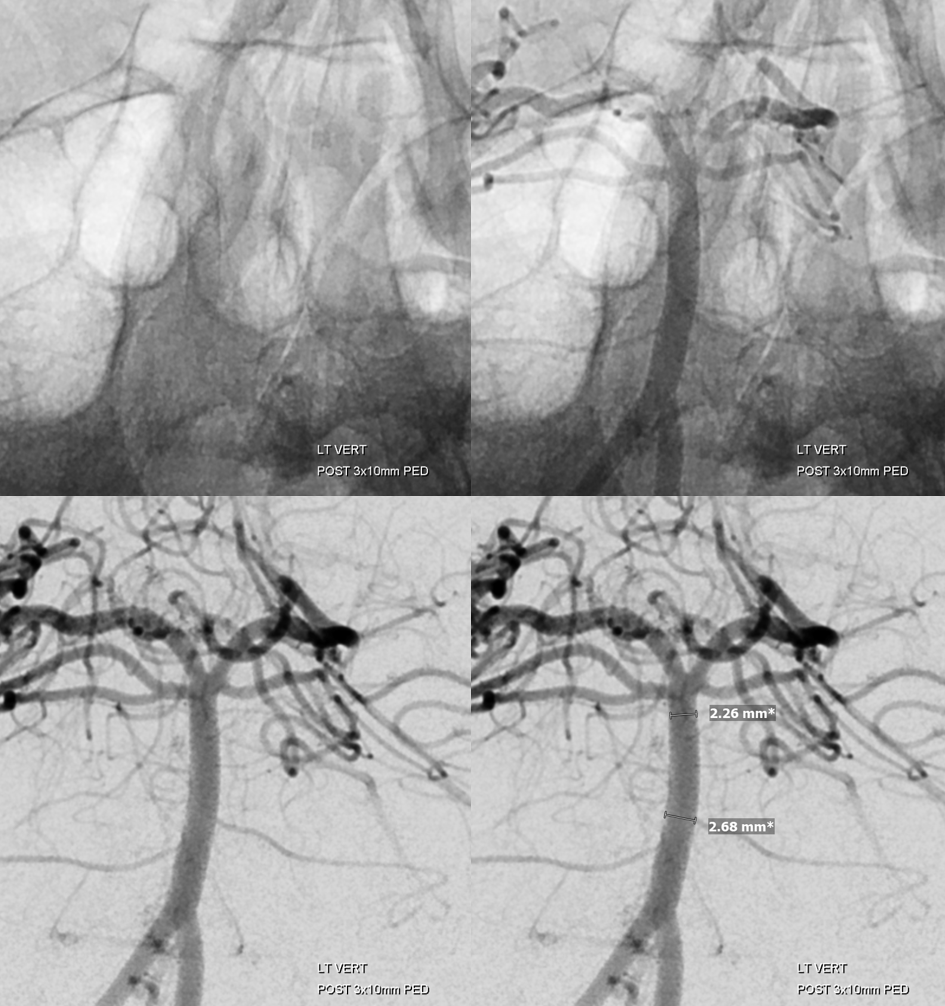
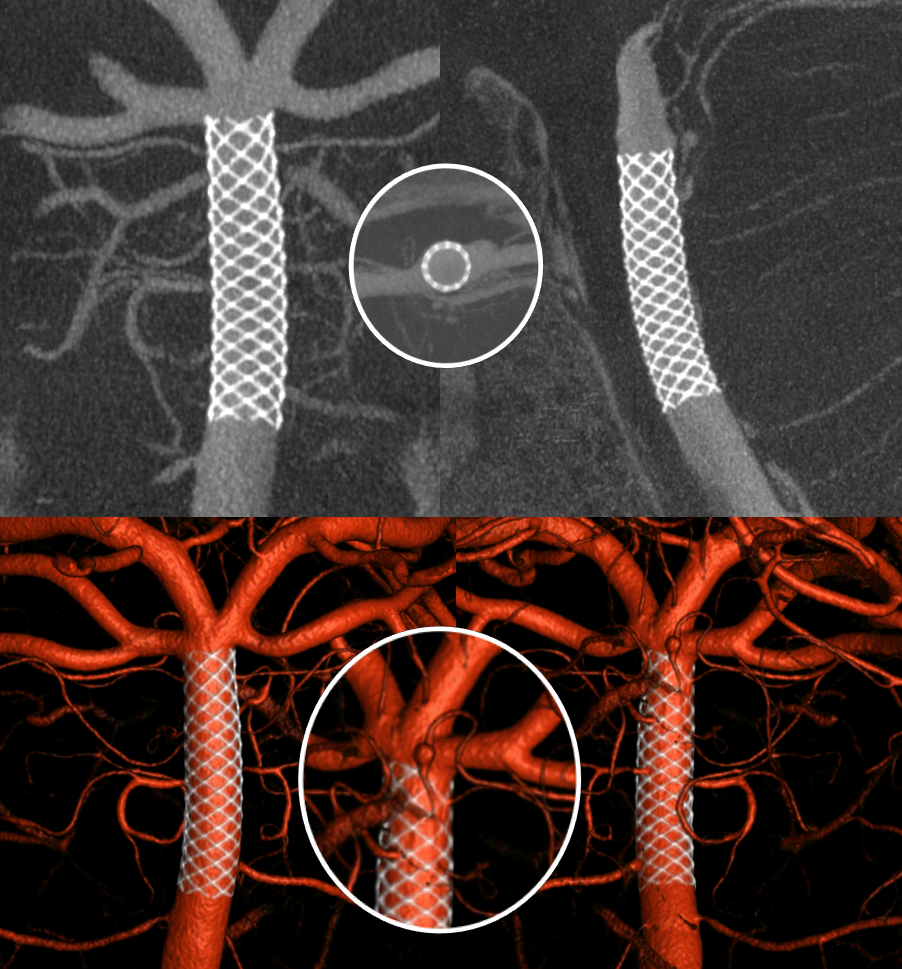
The classic post-Pipeline DYNA is with dilute contrast to check for wall apposition. That’s good for large branches like the SCA. We prefer “superdyna” (see below), but if you want to go classic, fine. This is a 20 second DYNA CT acquisition with 22 FOV (microdyna no binning) with 20% contrast dilution. Probably 15% is better but we went with a bit more
This is the primary reconstruction. Its good enough to see that the Pipe is well placed. But we can do much better. Lets create a secondary reconstruction
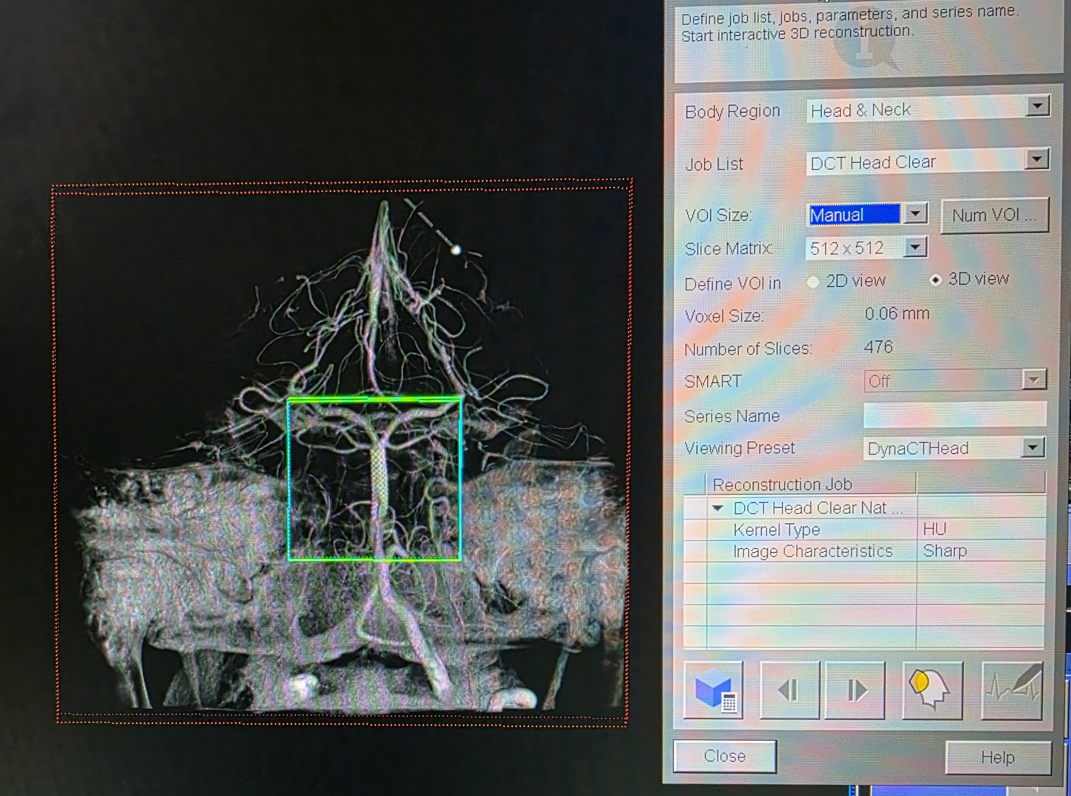
Small FOV and “sharp” image characteristics
Better
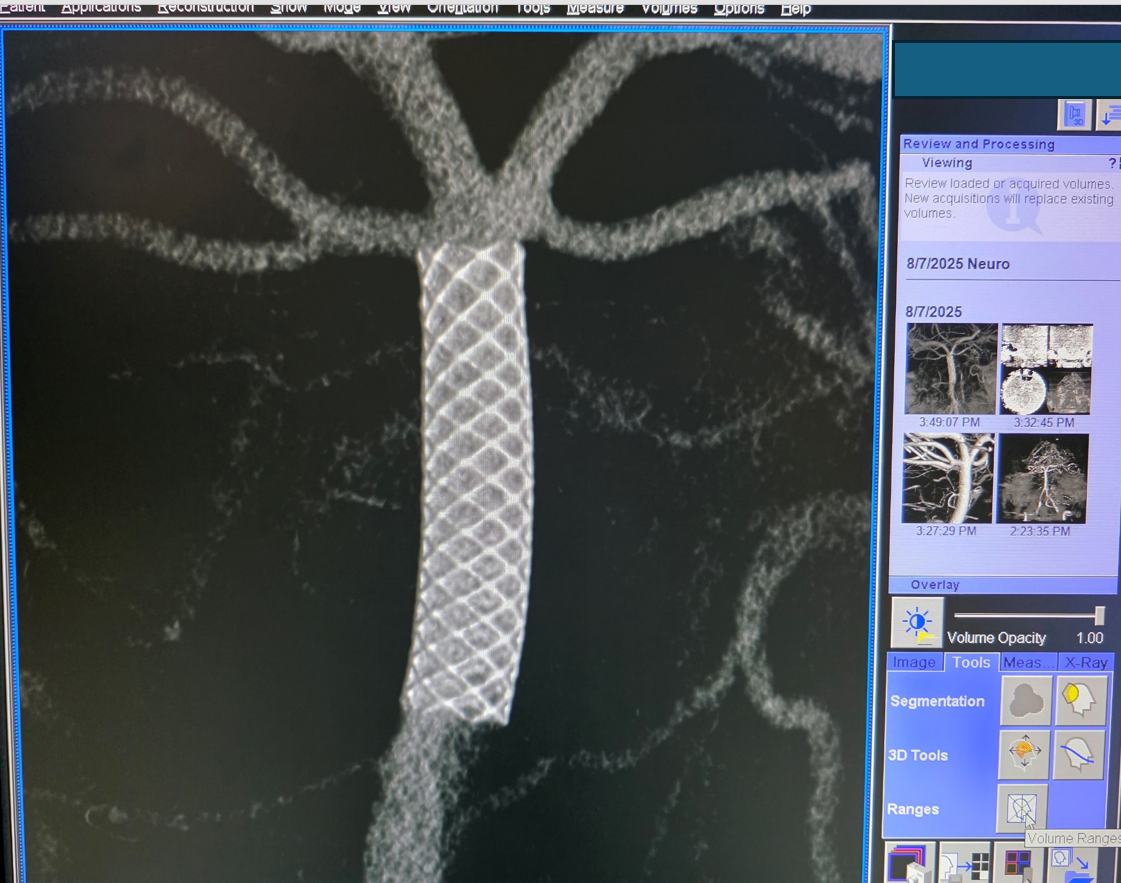
We can check to make sure apposition is good etc
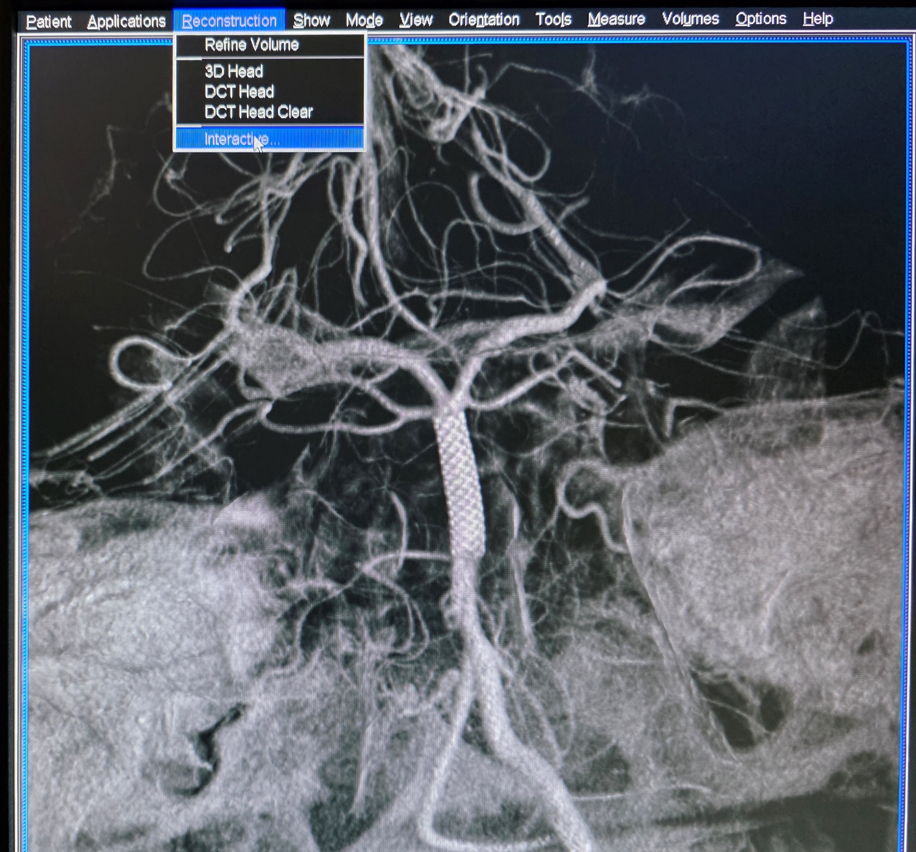
Finally, we create a rotational VR set
Now this could be all you need. However, lets say you want to combine the Pipeline device resolution of the post-deployment 20 sec dilute contrast scan you just got with the superior depiction of the vessels you can get with undiluted contrast — the one below
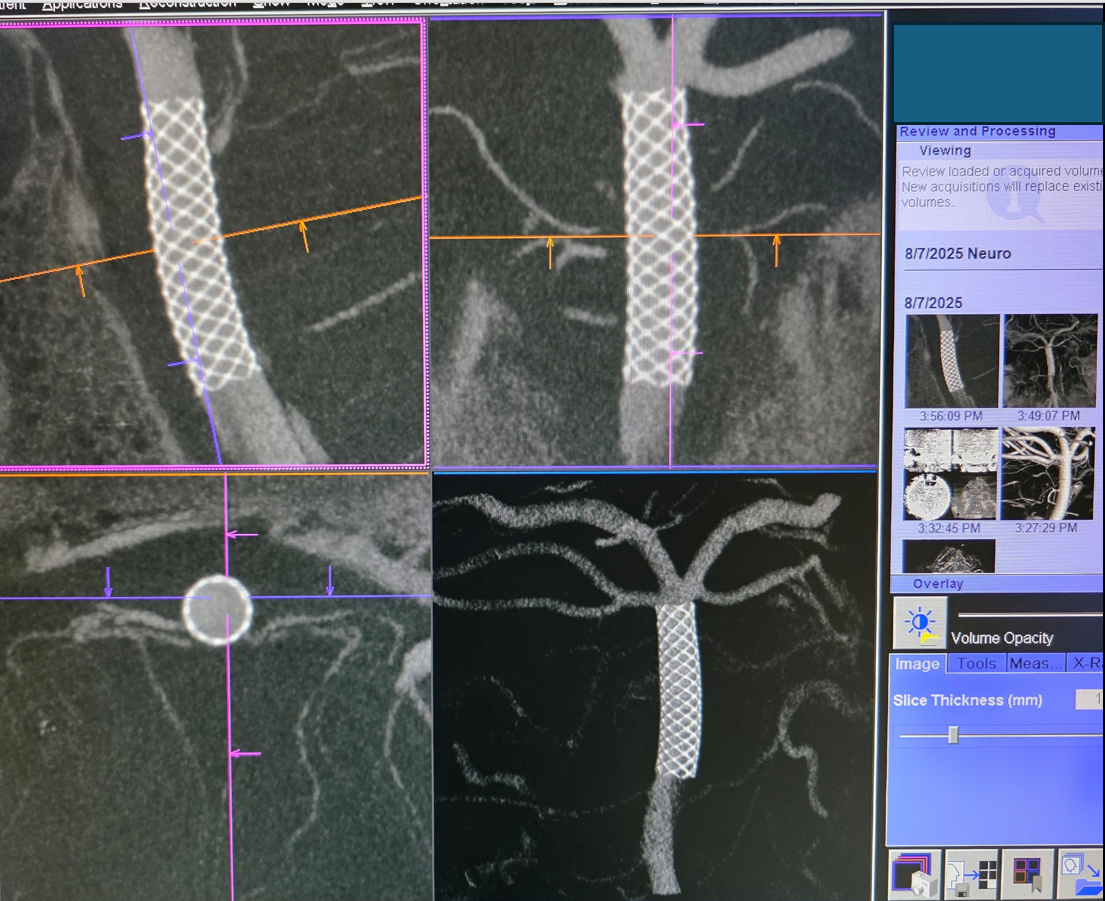
How to do that? One way is to do another 20 sec DYNA full contrast injection and combine them. Another is to overlay the secondary reconstruction of the post-treatment Pipe dataset on the pre-treatment 20 sec DYNA of the vessels. It works only if the vessels do not move post Pipe placement, which they sometimes do. Here, in the straight basilar, we expect no movement. So, we now add the secondary reconstruction of the pre-treatment 20 sec DYNA
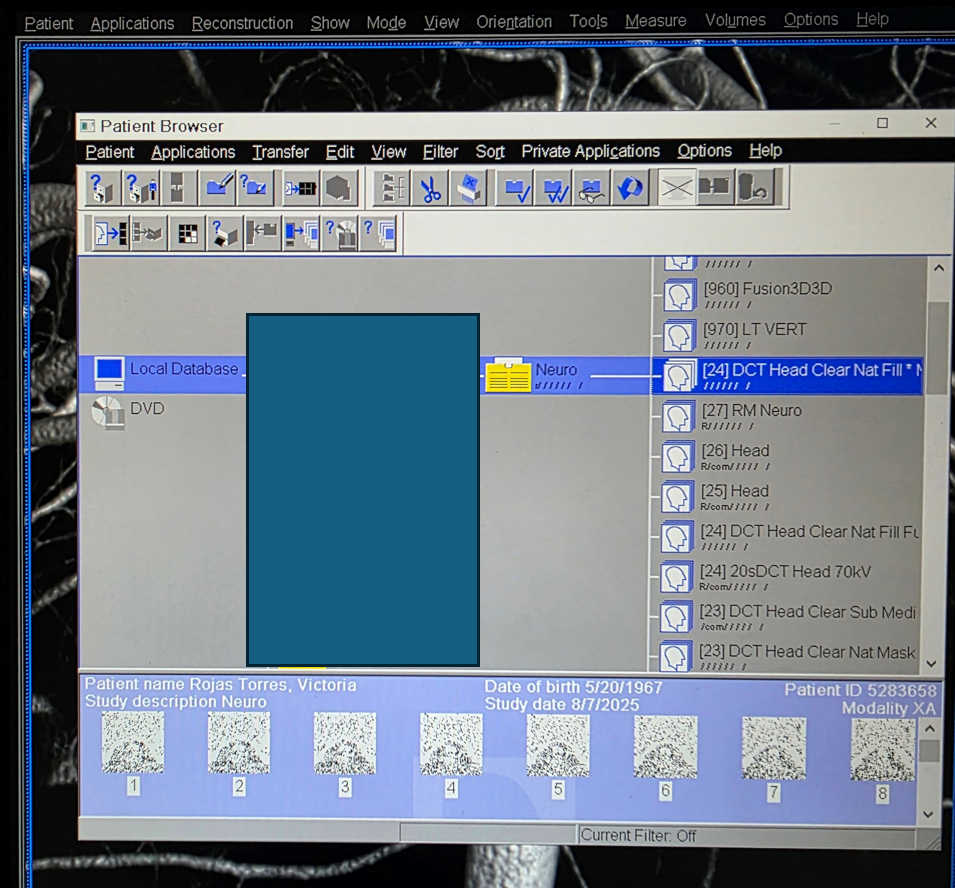
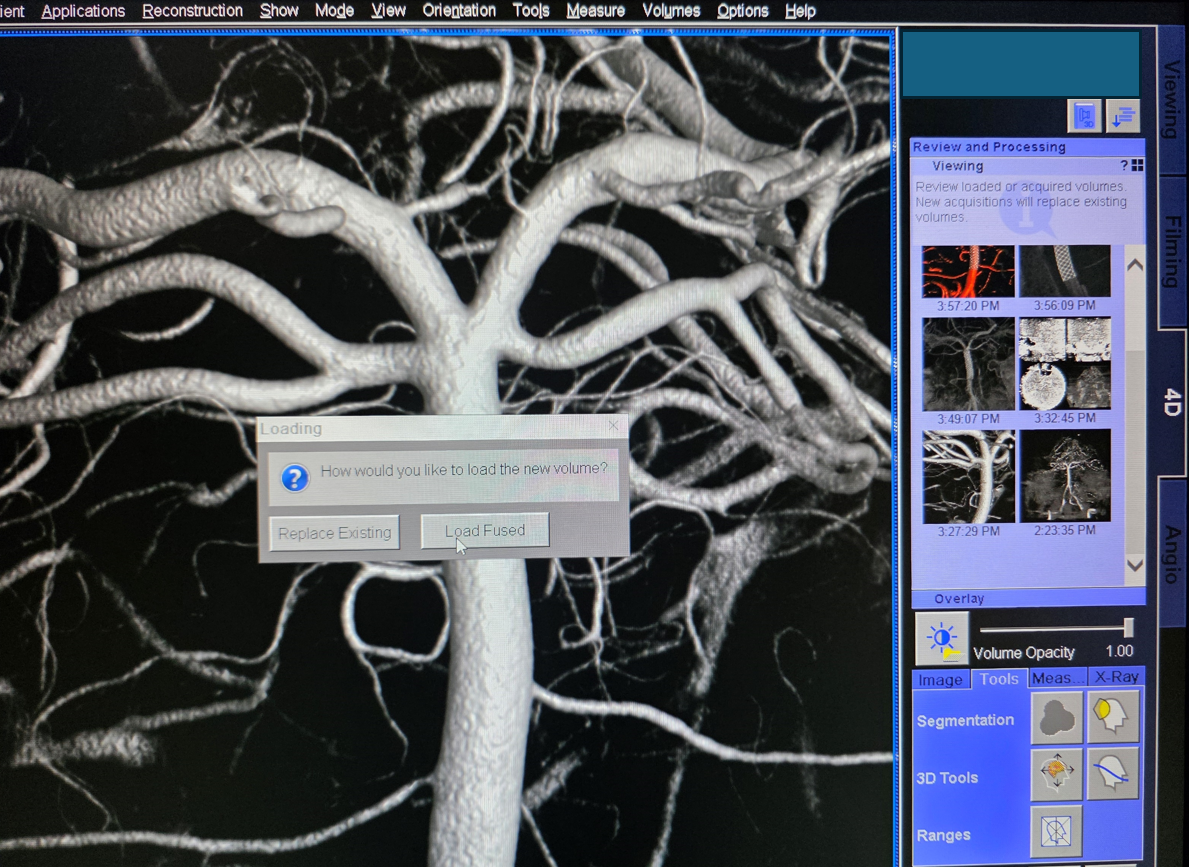
Load fused
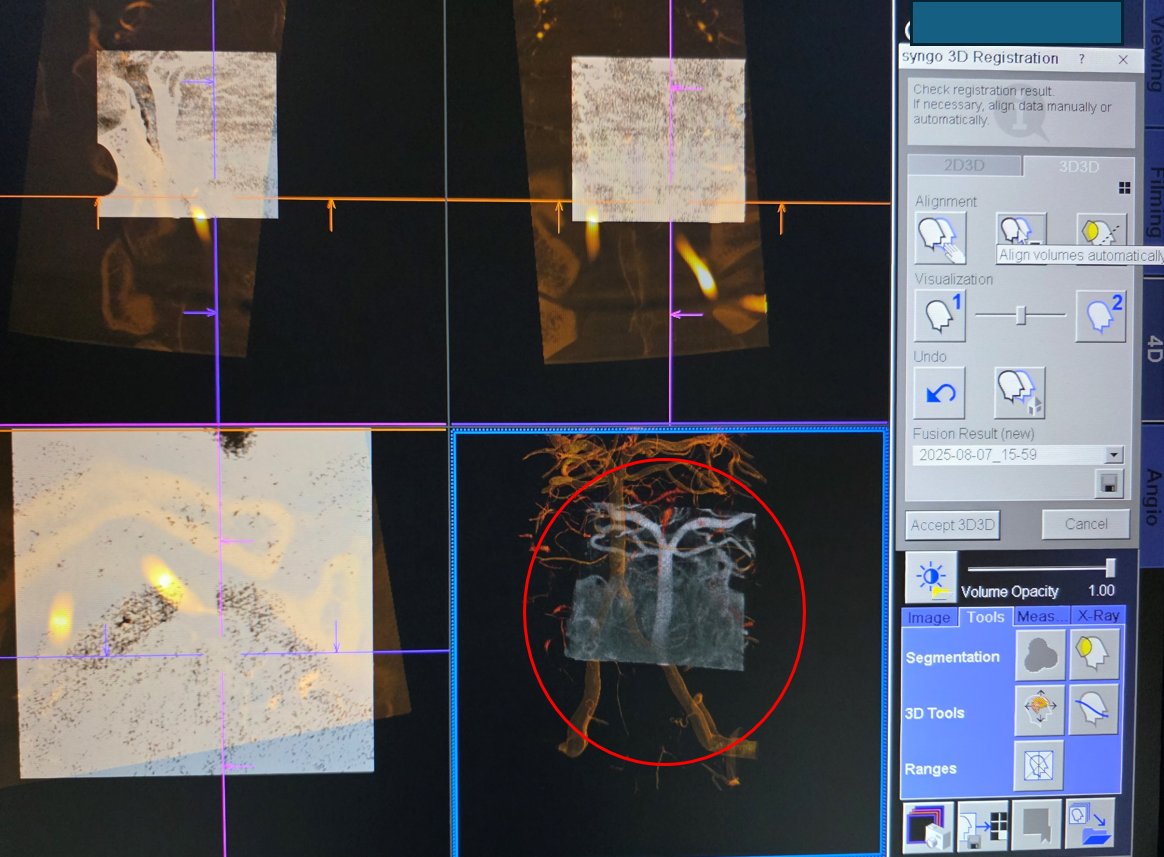
The datasets are not perfectly aligned — and they have to be. Try automatic volume alignment. it usually works well on the Q, and terribly on Icono
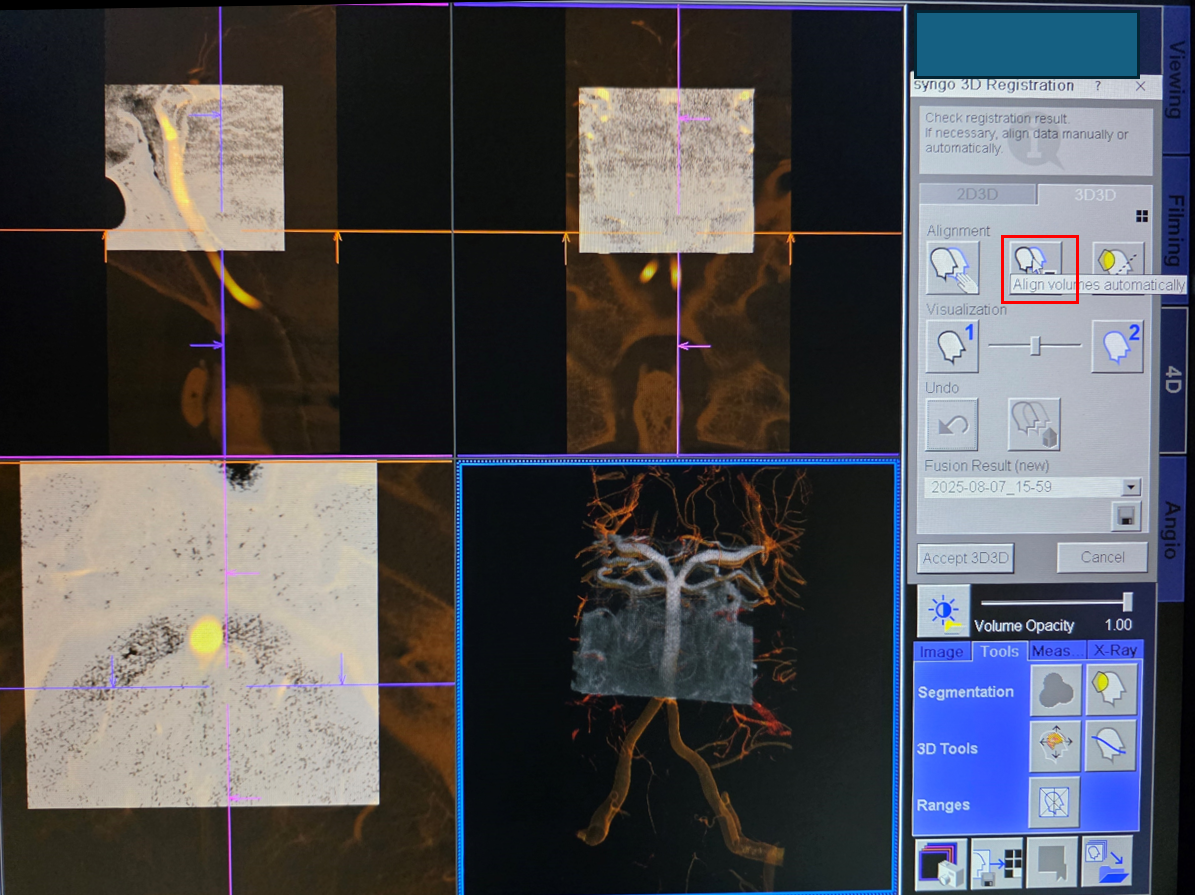
We tried – it did not work
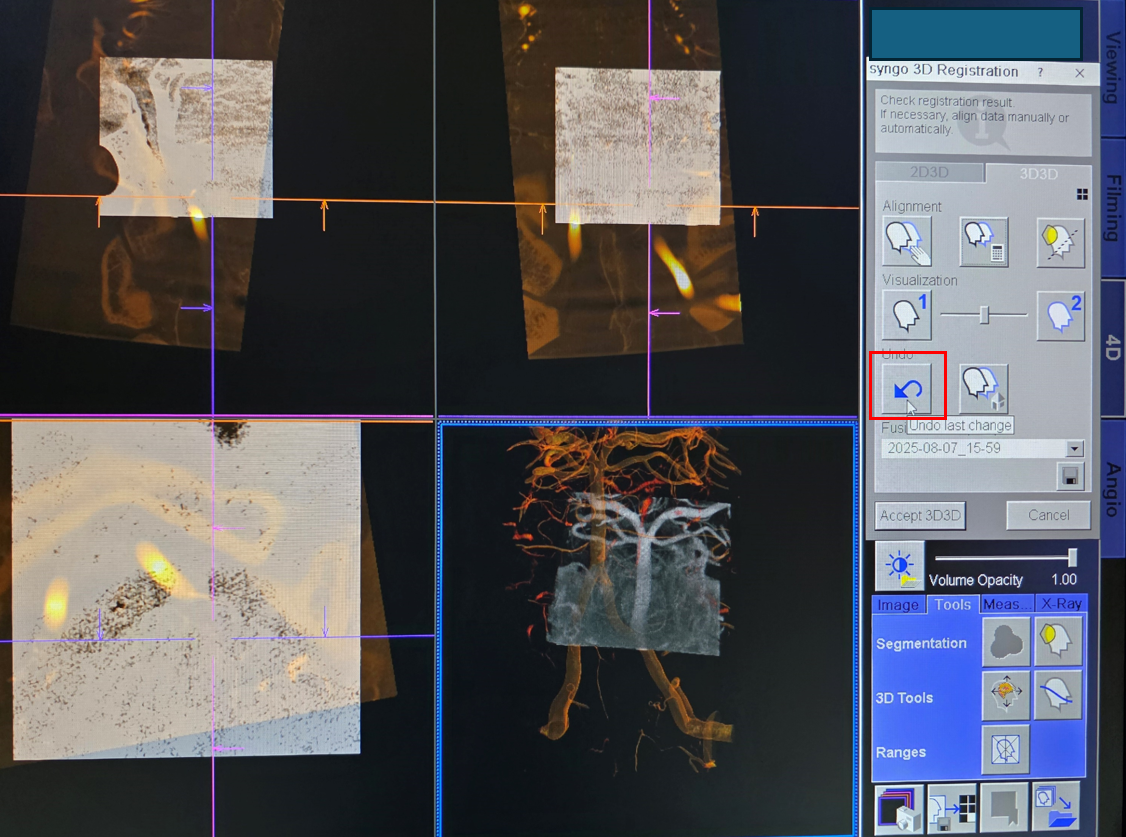
So, click “undo”
And align manually. How to do that — painfully.
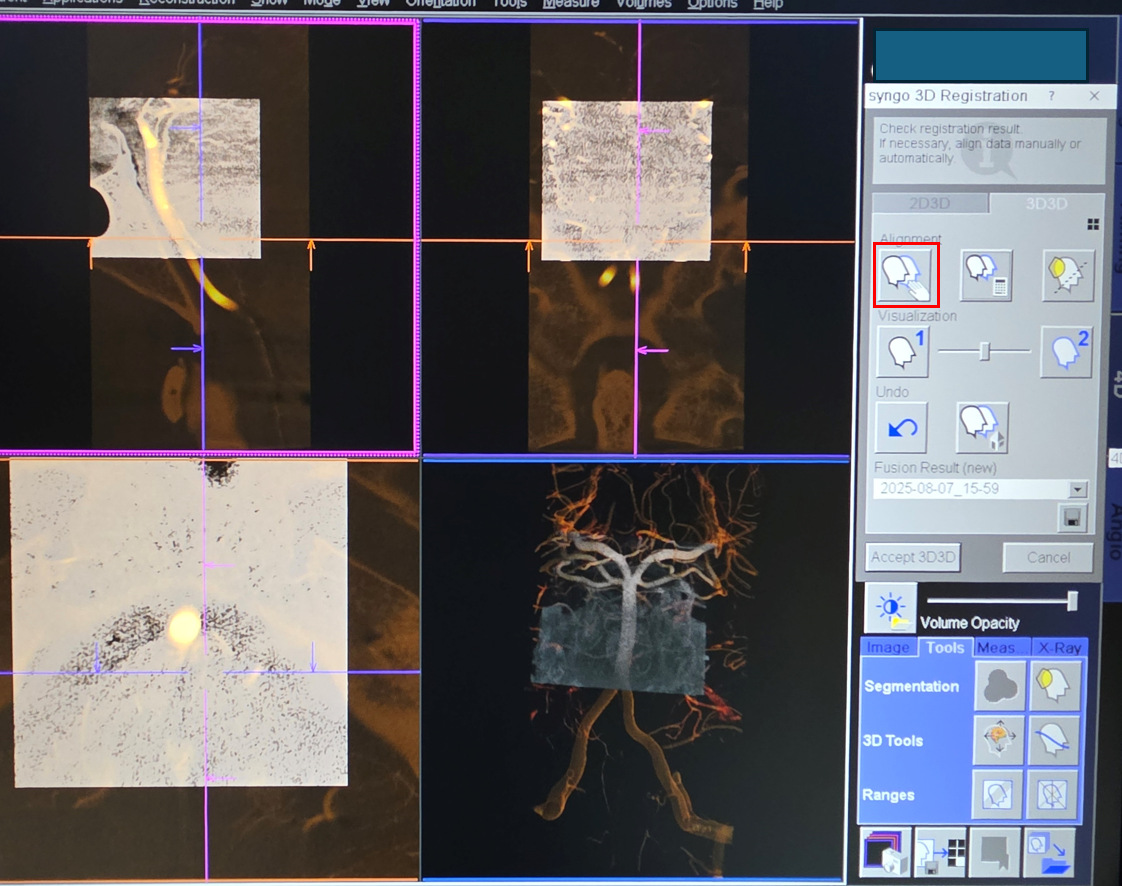
After manual alignment, try automatic again to make it perfect. it usually works in the Q and almost never in Icono. Latest is not greatest.
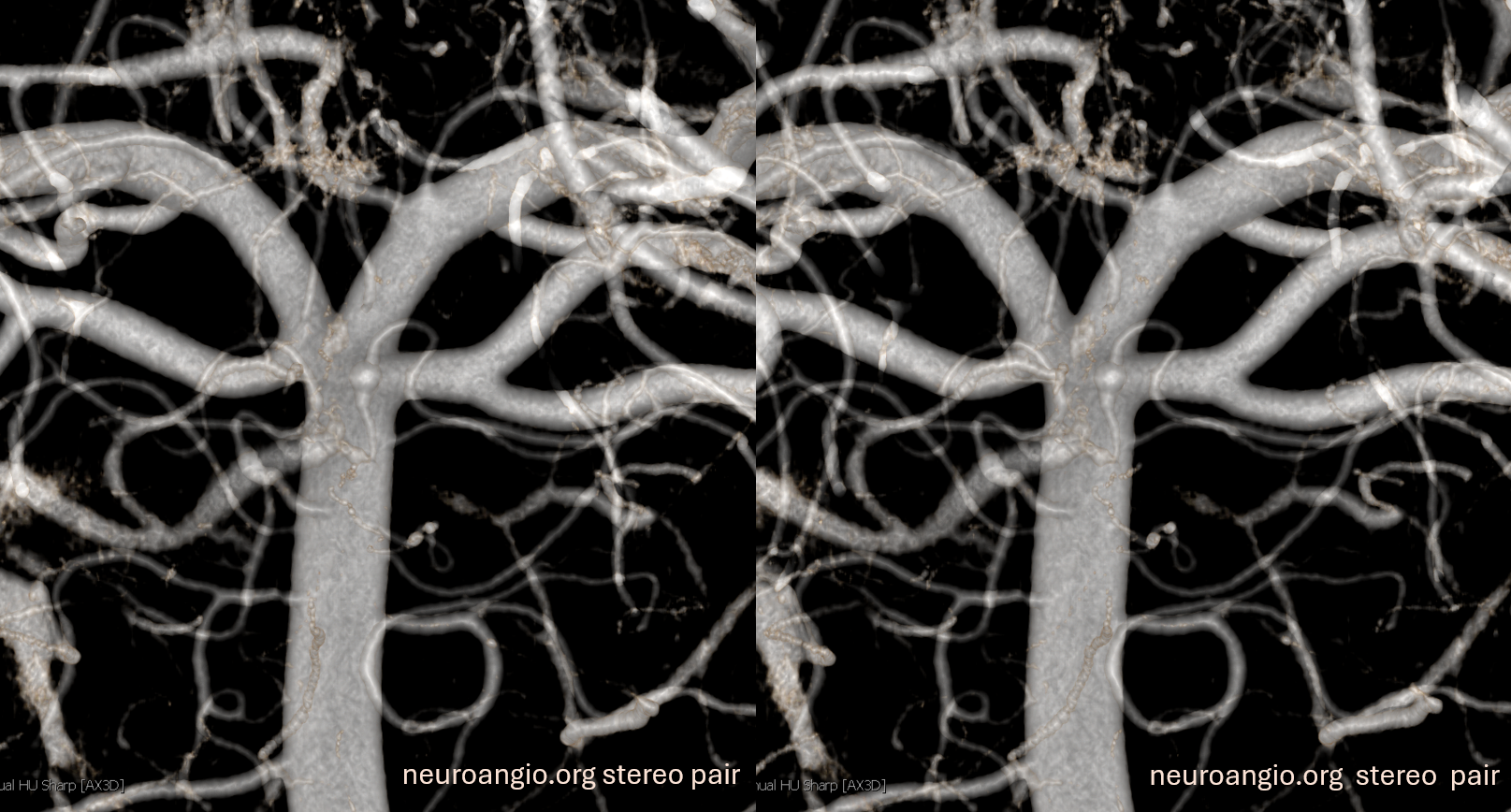
Below is the result — now we just need to change colors
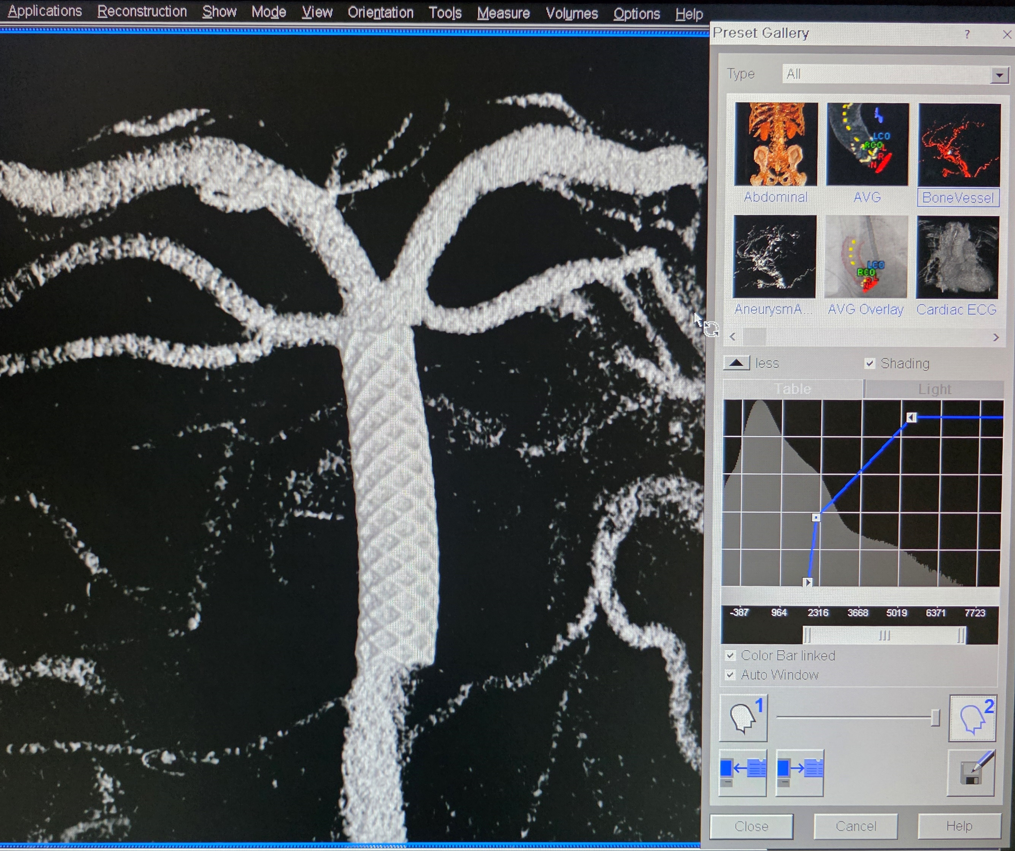
Move blending bar to see both datasets
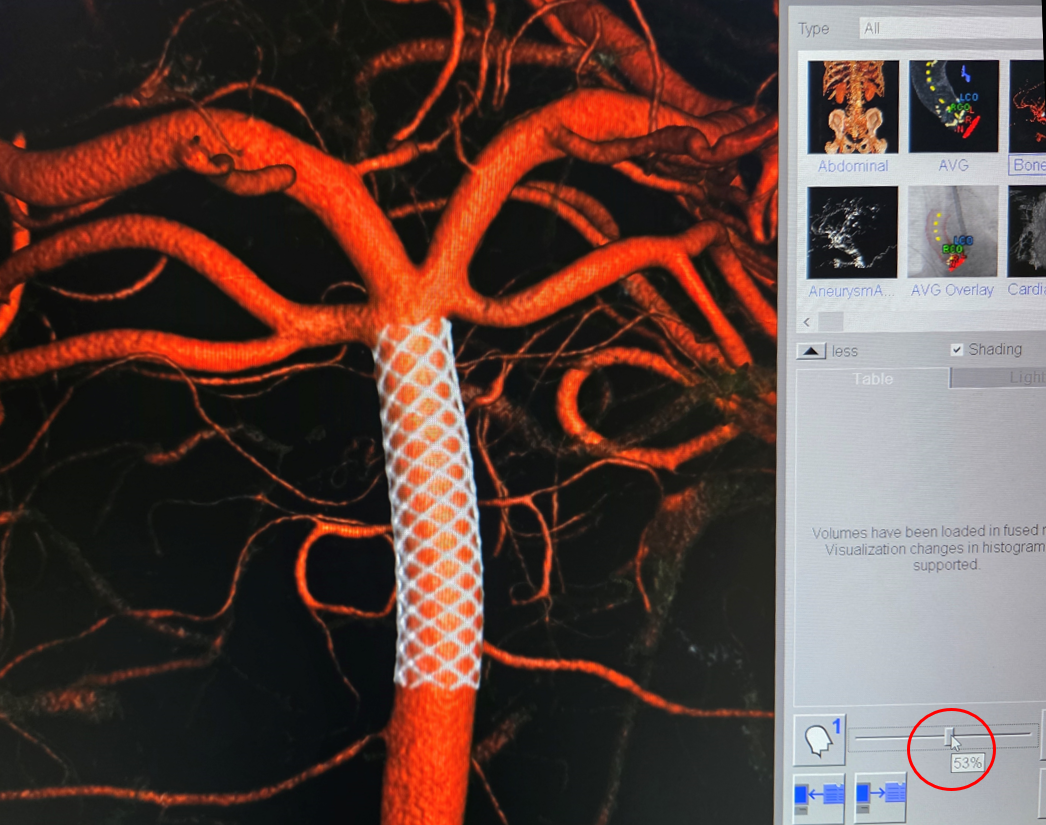
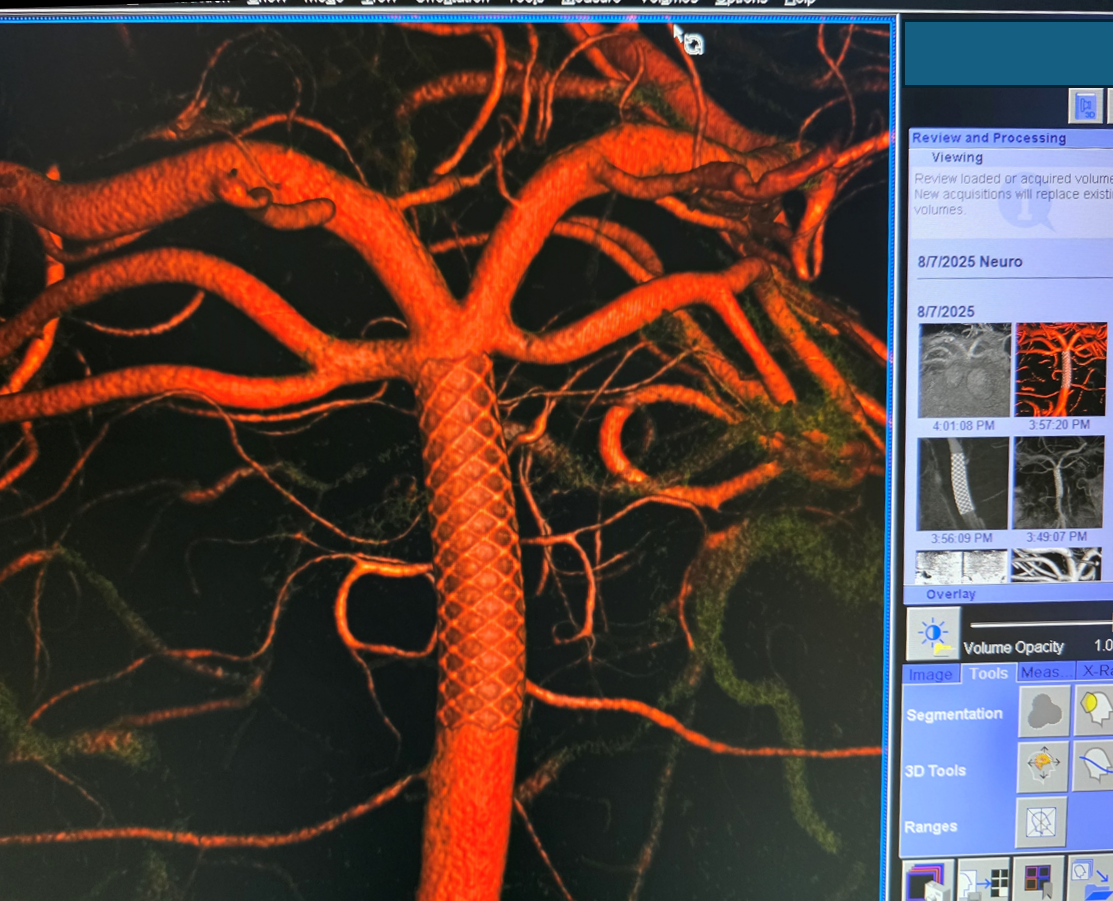
Now you have it
Beautiful
Yes, yes, we get it — pretty much all basilar perforator aneurysms have a benign natural history. We published on that too. Except a few that don’t — rerupture has been documented also. If you see enough of them, you know that never say never is the rule.