
A sinus dural fistula need not become high-grade because of entire sinus occlusion. Because the sinuses frequently have compartments, it is possible for a sinus dural fistula to have exclusive cortical drainage if the compartment it is draining into becomes isolated from the rest of the sinus system. This fistula also beautifully shows how arterial supply is frequently derived from arteries in the walls of dural sinuses (see MMA , meningeal vascular network pages)
Patient presents with pulsatile tinnitus. MRI shows enlarged left MMA (yellow arrows). There is a vessel traversing the undersurface of the temporal lobe towards the galen (pink)
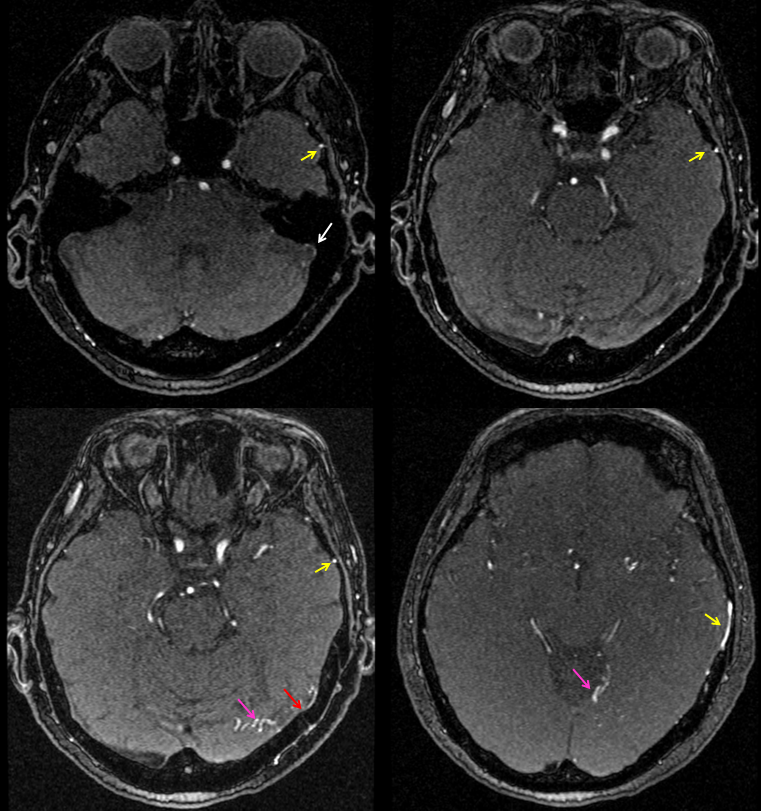
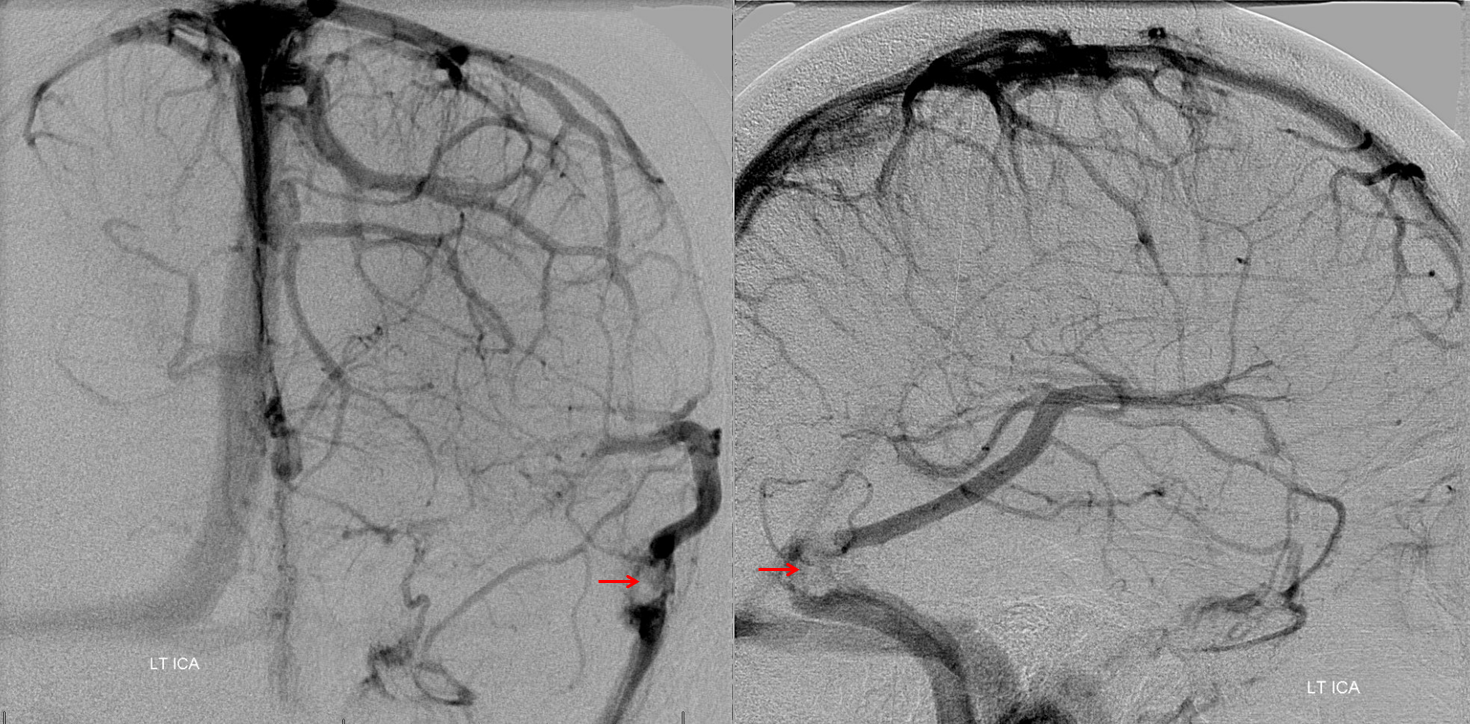
Angio venous phase shows giant vein of Labbe with some kind of filling defect at the ostium (red arrows)
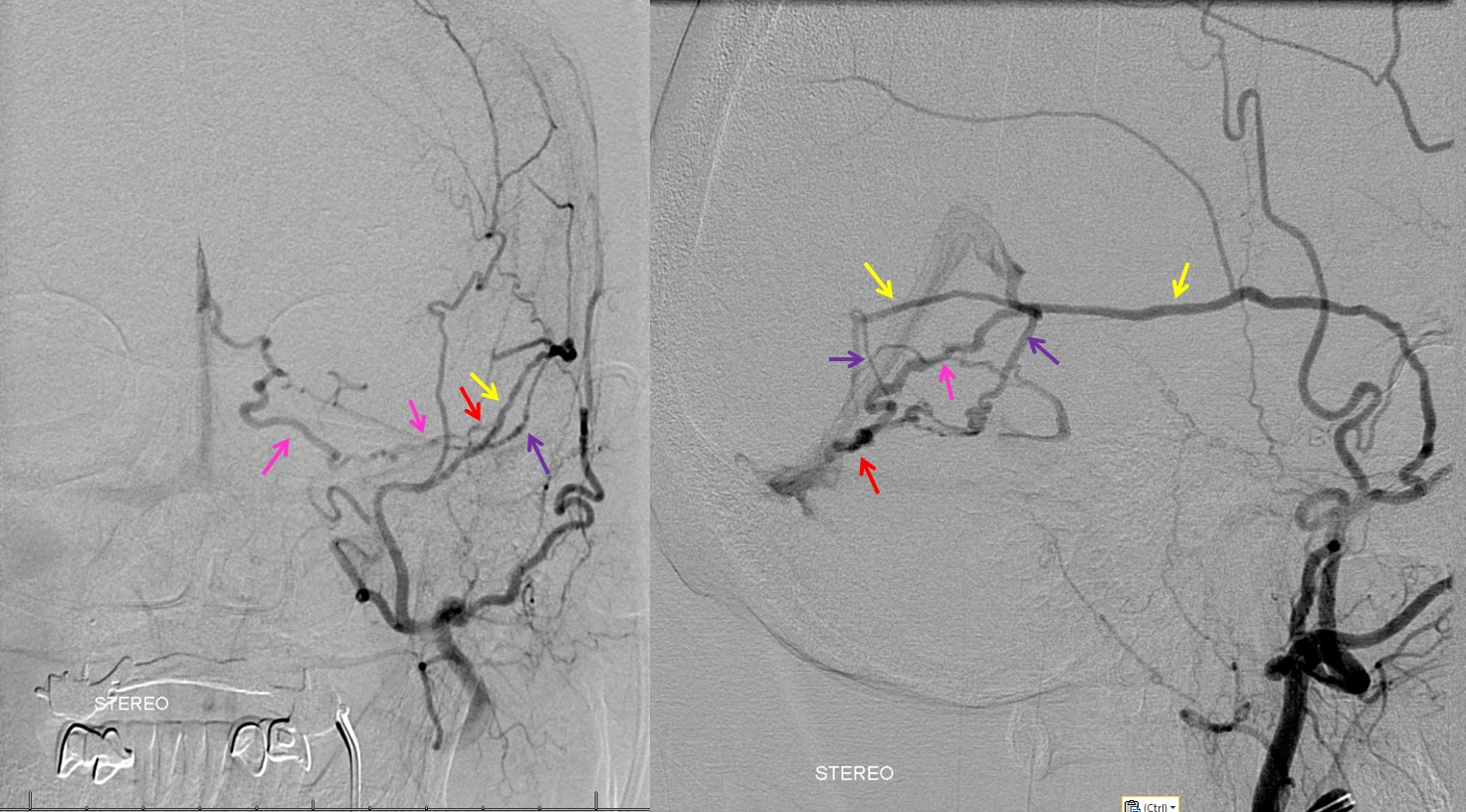
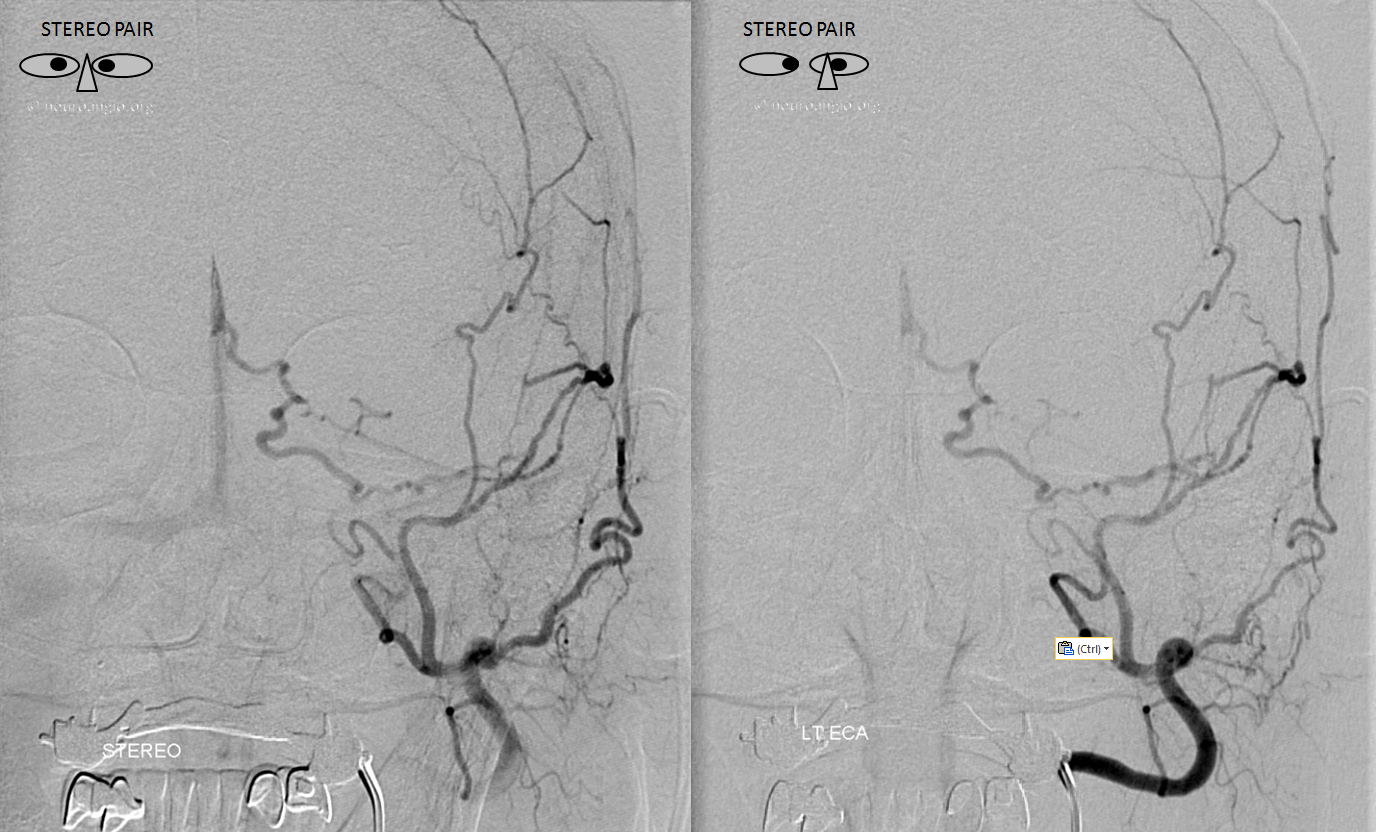
Distal external injection. MMA petrosquamosal branch – yellow. Several petrosquamosal branch pedicles (purple) extend inferiorly towards a common channel (red), and then into the vein seen on the MRI (pink) draining ultimately into the Galen.
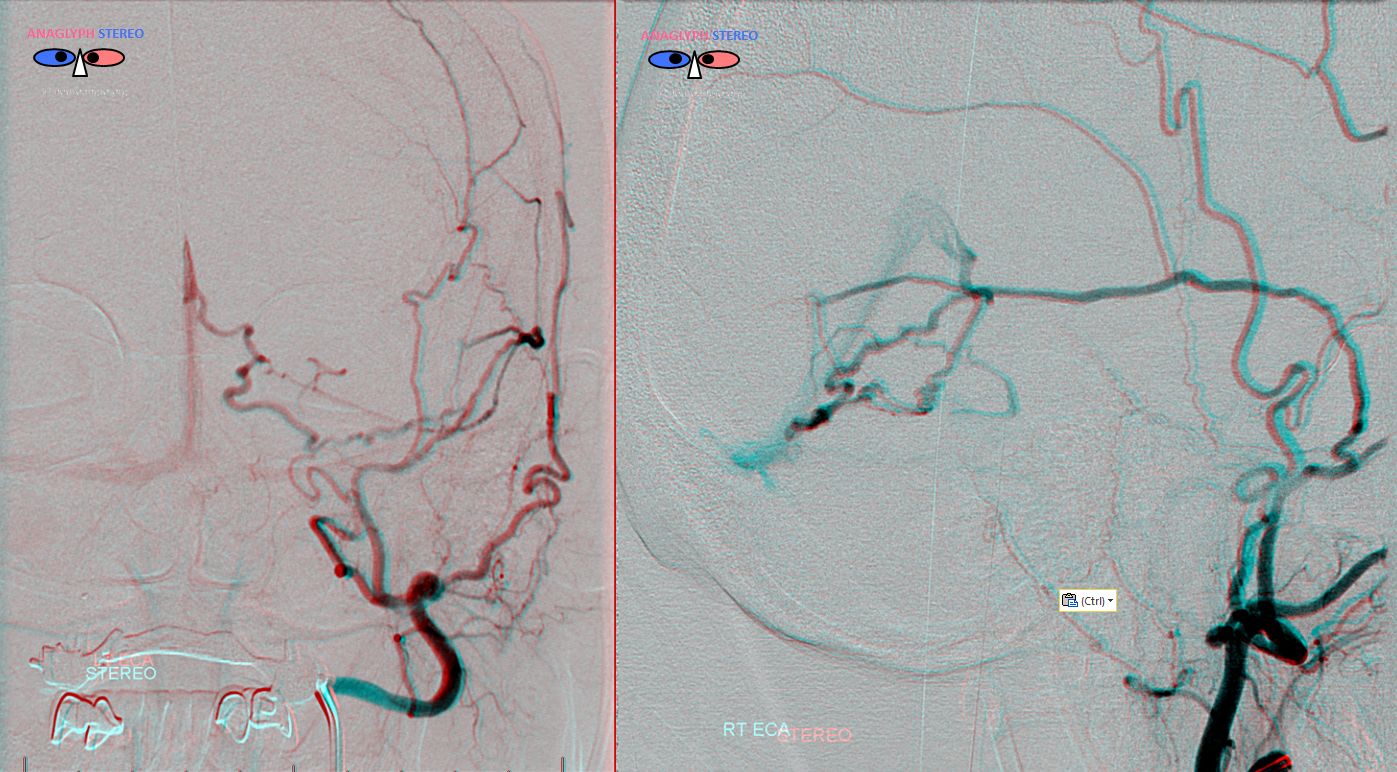
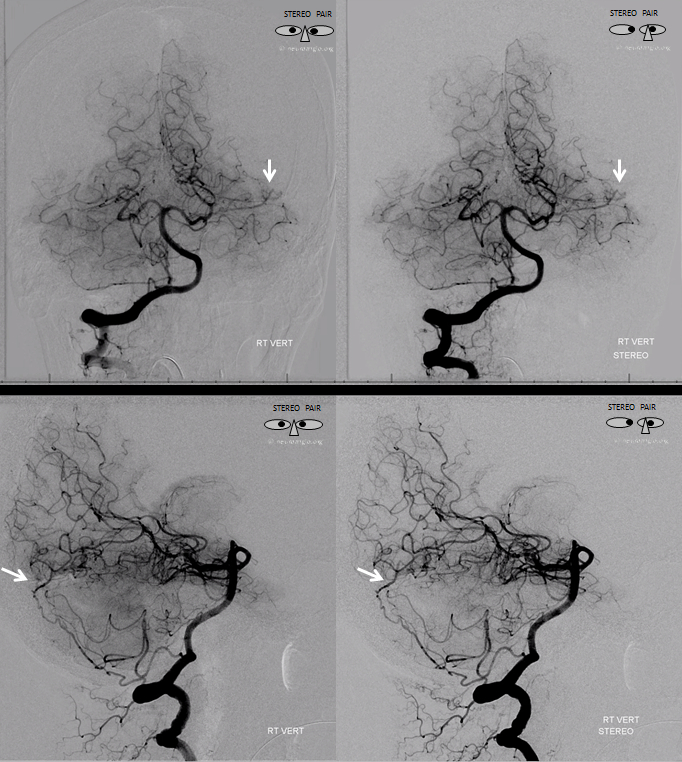
Stereo Pair

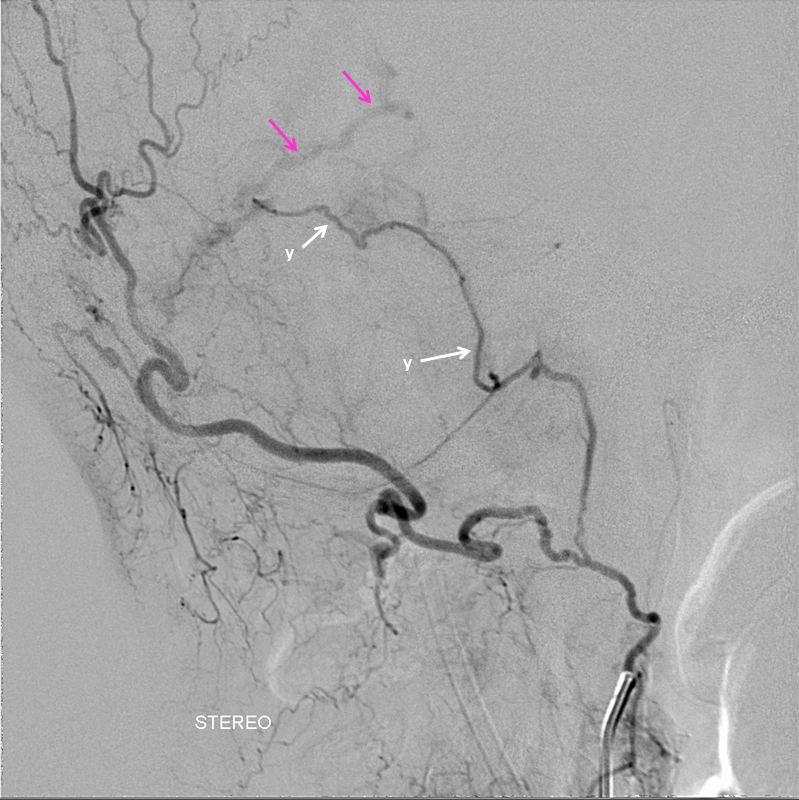
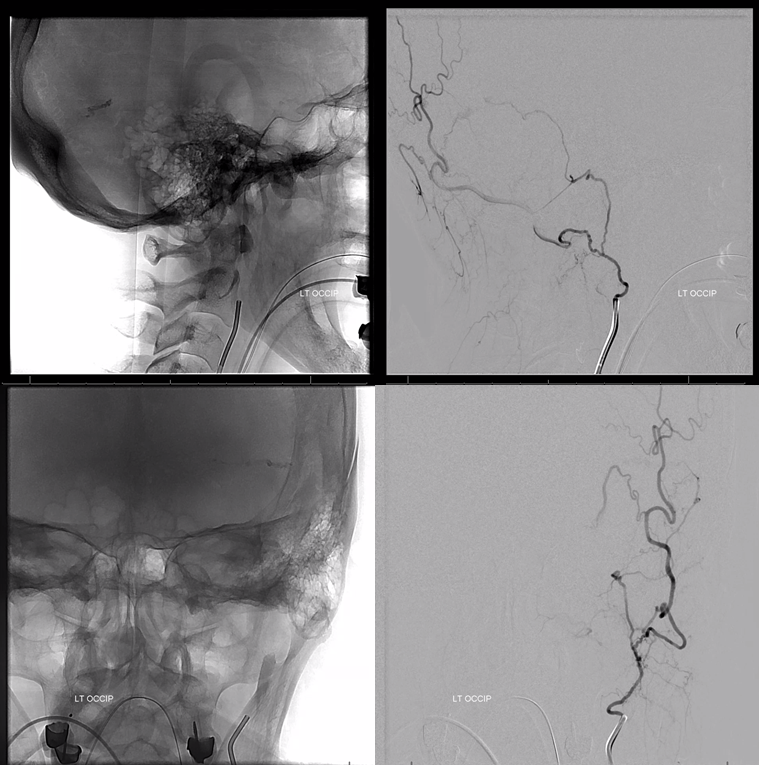
Not done yet. Injection of the pharyngo-occipital trunk (common origin occipital and ascending pharyngeal artery) shows another vessel (white arrows, label “y”) supplying the fistula, with pink arrows on same draining vein
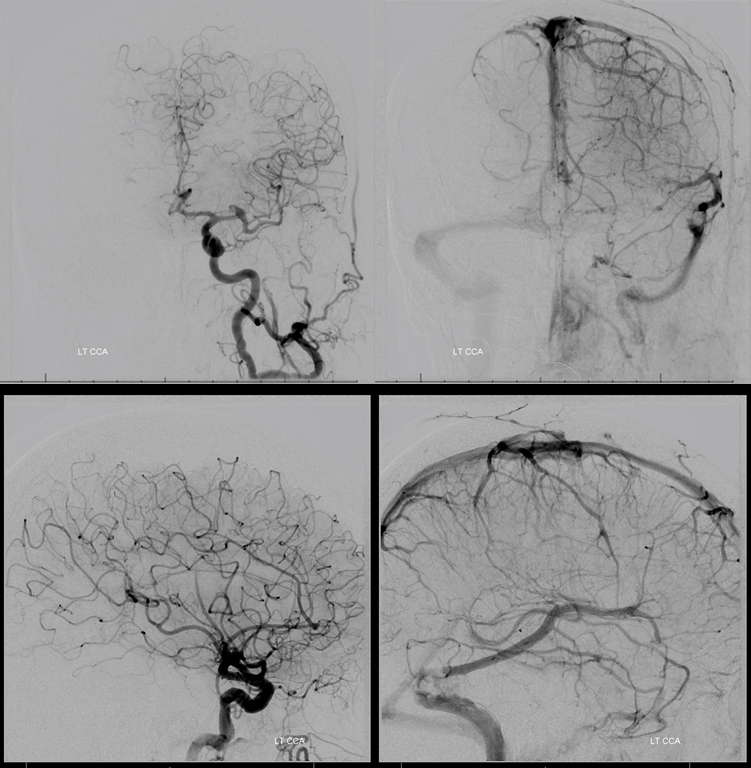
Now, below we see injection of left common carotid artery, with arterial phase mask image (white). What do we see? How to put it all together?
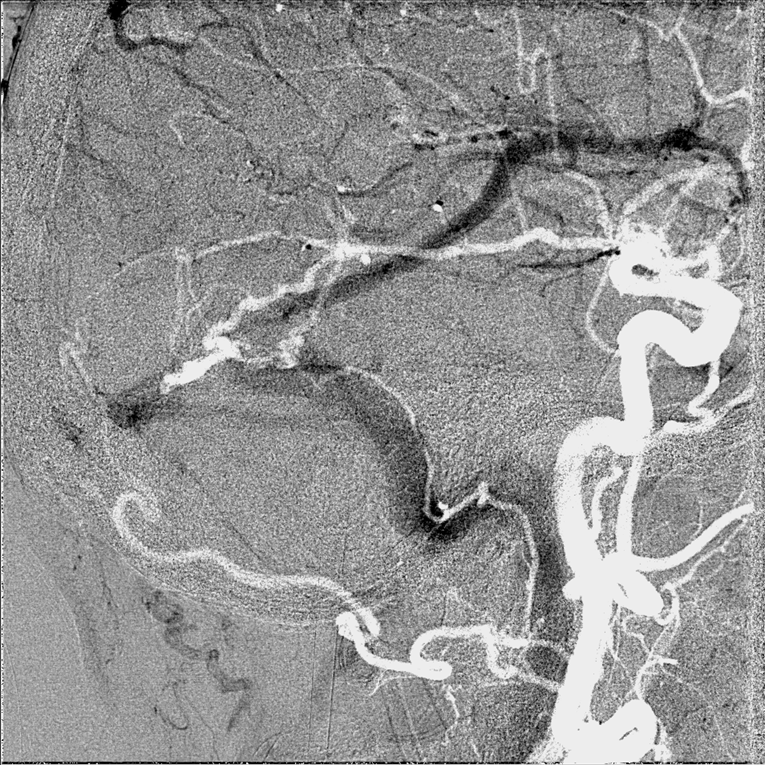
See how the ascending pharyngeal branch is overlying the jugular bulb and sigmoid sinus? Why? Because it is an artery in the wall of the sinus, labeled “y” in the diagram above. This “sigmoid sinus” branch is a continuation of the jugular division of the ascending pharyngeal artery — jugular division being the branch which traverses the jugular foramen and supplies CN IX, X, and XI there. See ascending pharyngeal artery page for more details. In this case, it contributes to the fistula via the sigmoid sinus branch. Also notice how the fistula point overlies the filling defect seen on the venous phase of at the foot of the Labbe.
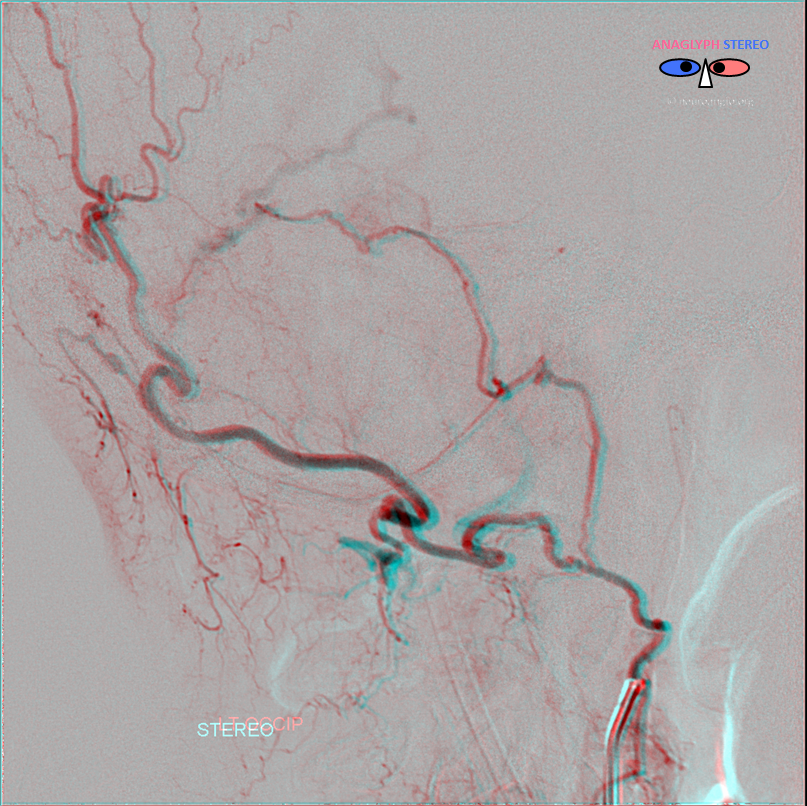
This is not all however. Look again at images below — there is wash in seen in the posterior-most pedicle of the MMA, implying that another source of inflow is present. Stereo views of the right vert show the tentorium cerebelli artery connecting with the transverse sinus artery branch (white arrows) supplying the fistula as well.
The anaglyph below puts the whole picture together
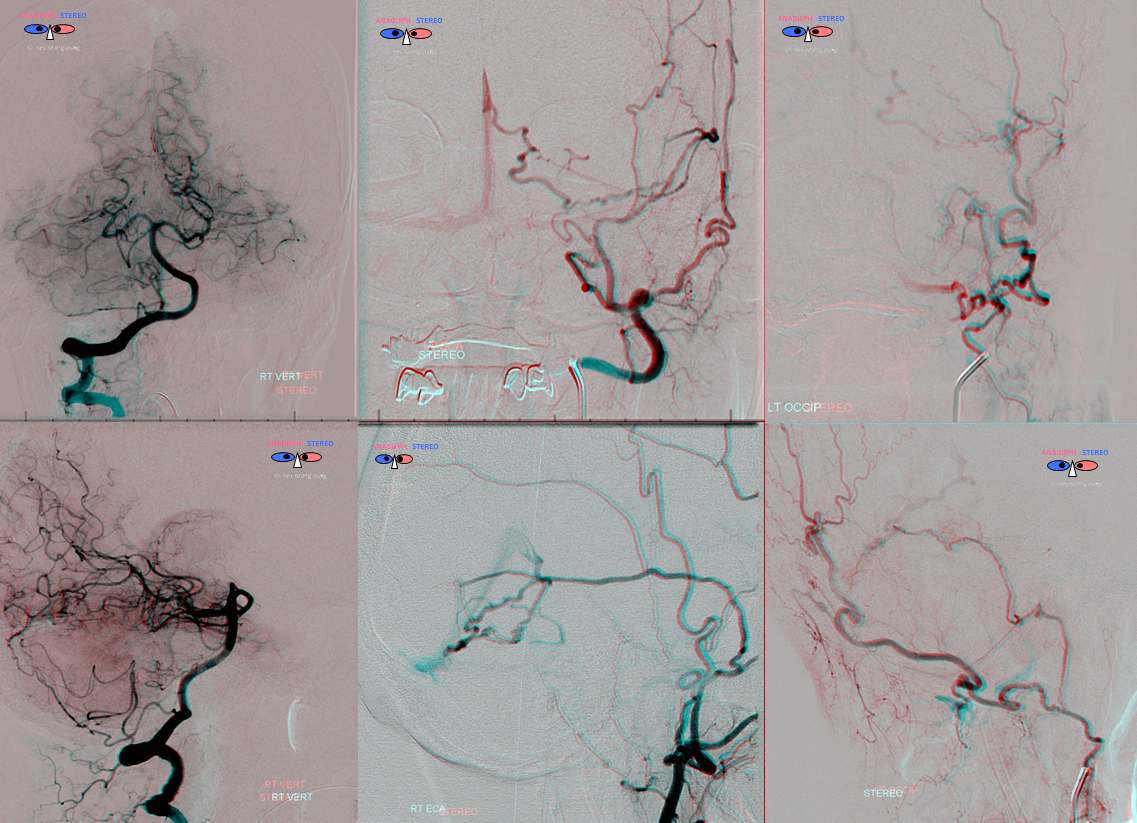
Synthesis: this is a sigmoid sinus fistula, localized to a compartment of the sinus which has no access to the rest of the sinus. The main sinus is patent, and drains the Labbe in antegrade fashion, perfectly well. The fistula however, having no access to the sinus system, drains via a subtemporal cortical vein, between the temporal lobe undersurface and the tentorium, into the Galen. Thus, it is an example of how a fistula can be high grade (Cognard IV, Borden III) and still be associated with a preserved sinus.
Treatment
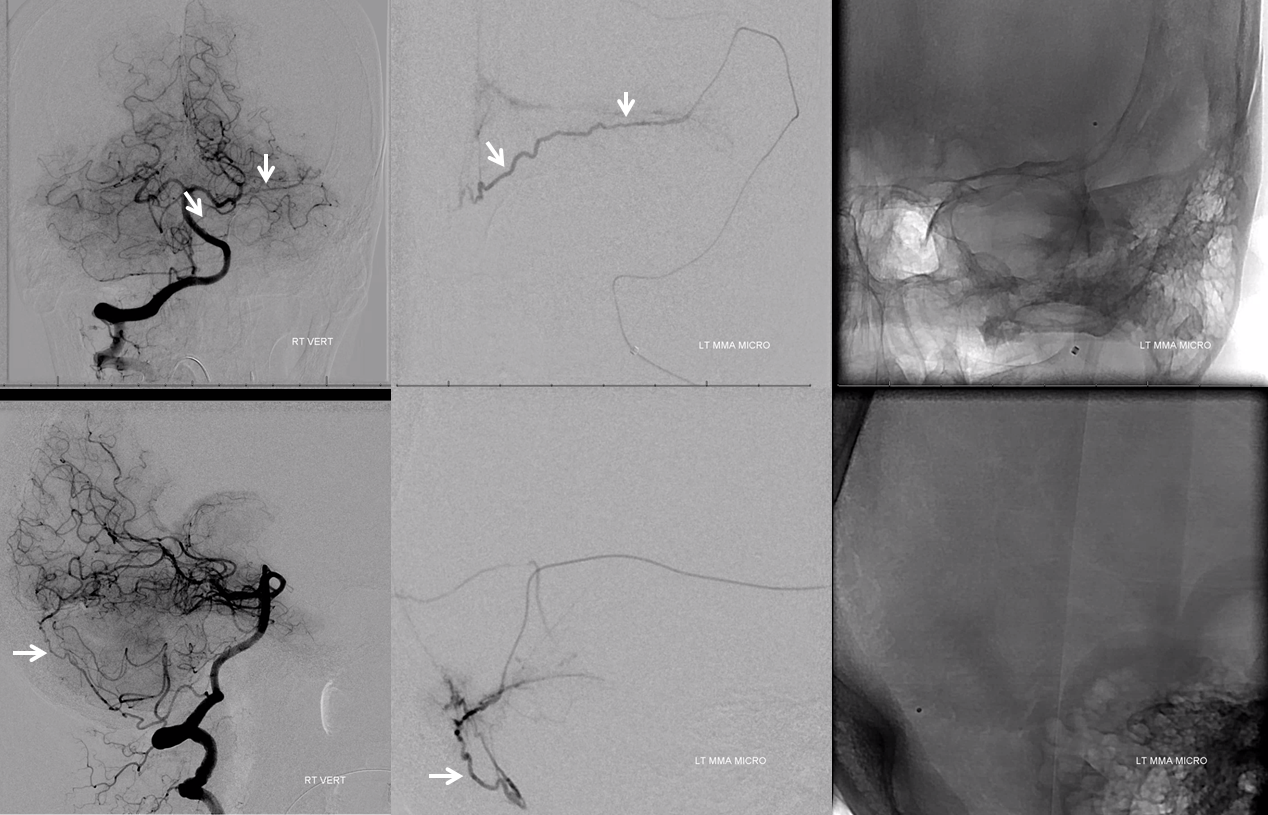
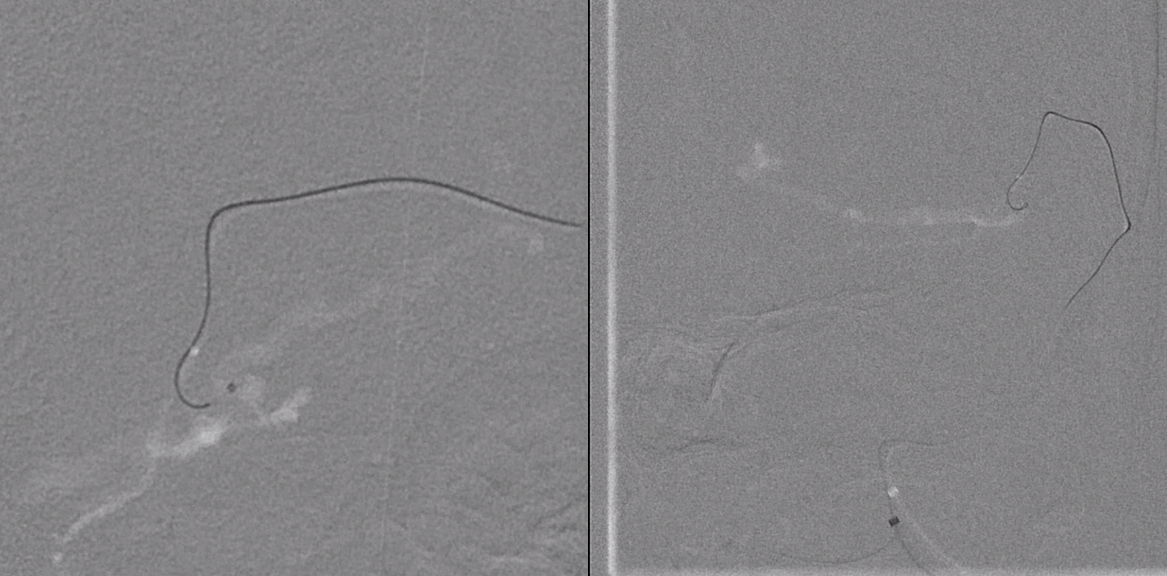
Headway duo in the distal MMA. Again see change in caliber in the posterior-most pedicle on lateral view due to supply from right vert
Retrograde injection of transverse sinus artery branch down to the falx cerebelli, same branch shown with white arrows on prior right vert injection
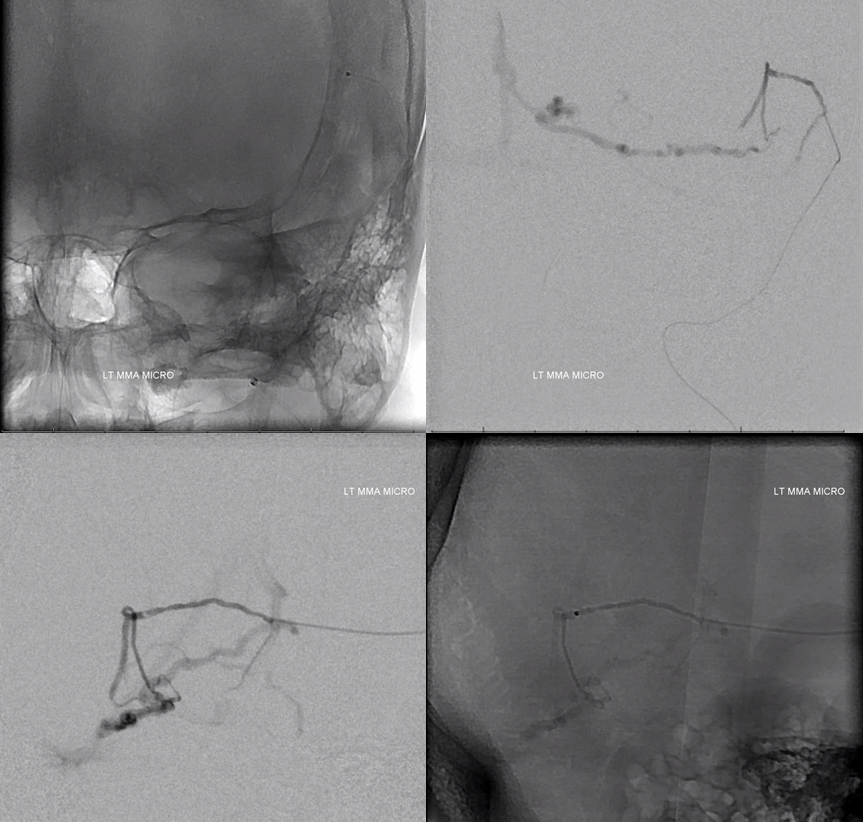
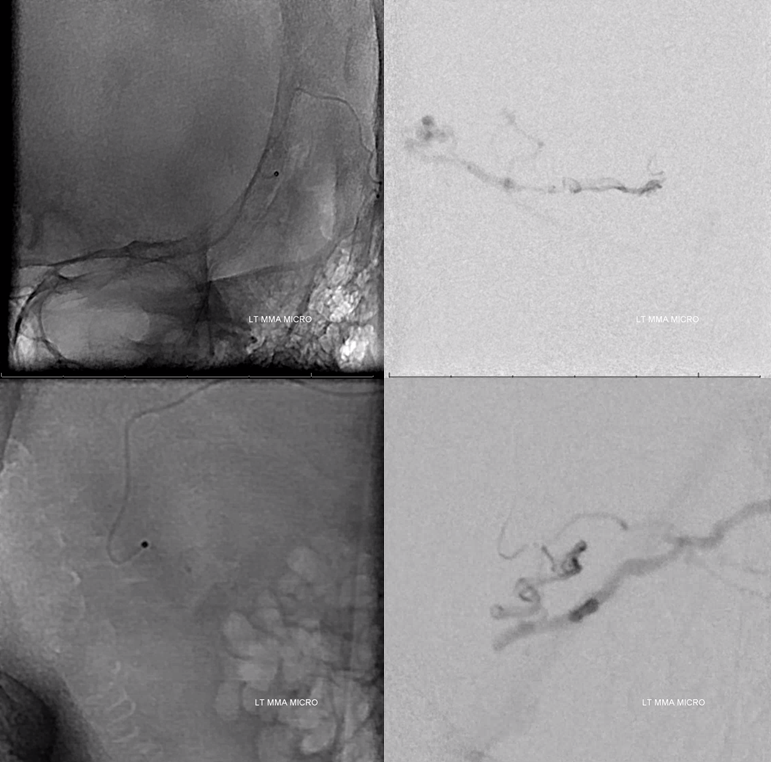
Now we turn anterior into one of the small pedicles that is supplying the fistula in a relatively direct manner
Micro injection in “wedge” glue position
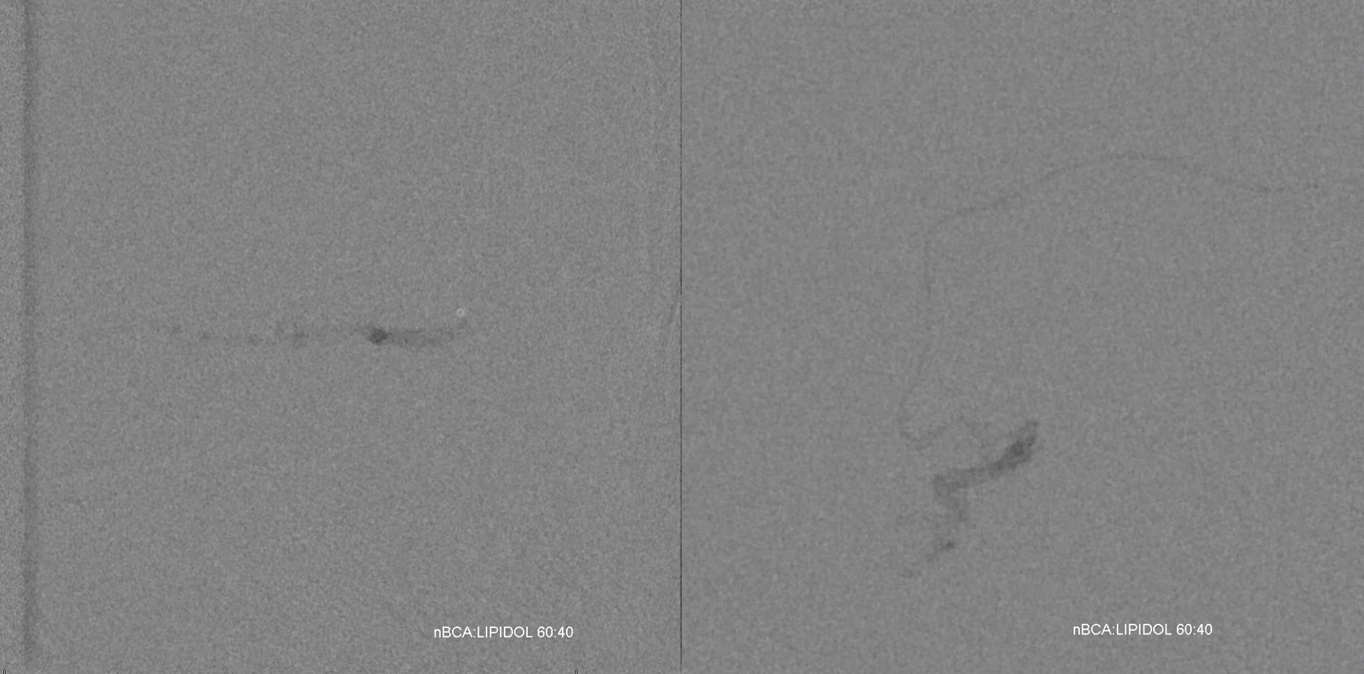
Glue cast (nBCA:Lipidol 60:40). A higher glue concentration given washin from other pedicles means we want glue to polymerize faster
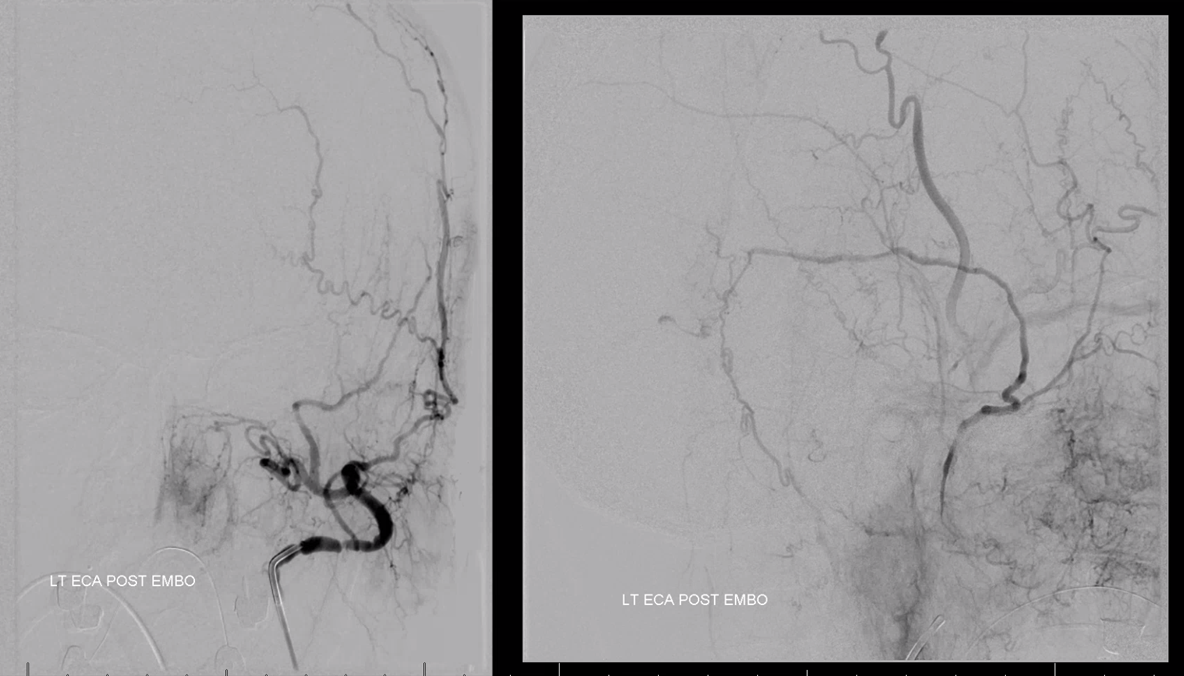
Post ECA
Post pharyngo-occipital
Post left CCA with preserved Labbe
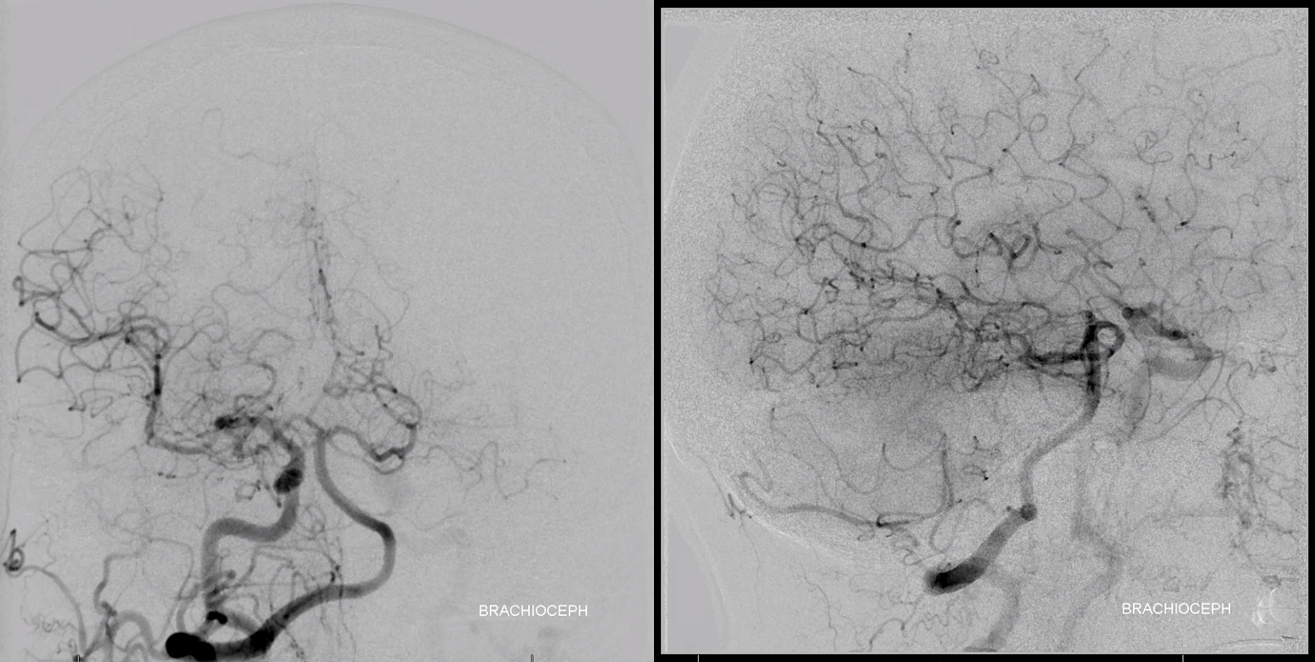
Post right brachiocephalic
Conclusion
Another example of superselective embolization. See other cases here: 1, 2, 3, 4
Another example of dural arterial channels in walls of sinuses, such as sigmoid and transverse sinus artery. See “Meningeal Arteries” page for more info