
Another example of how having anterior spinal supply from a given level does not preclude an embolization from the same level, if understanding of anatomy leads to a rational strategy
Patient presents for a hemangioma embolization
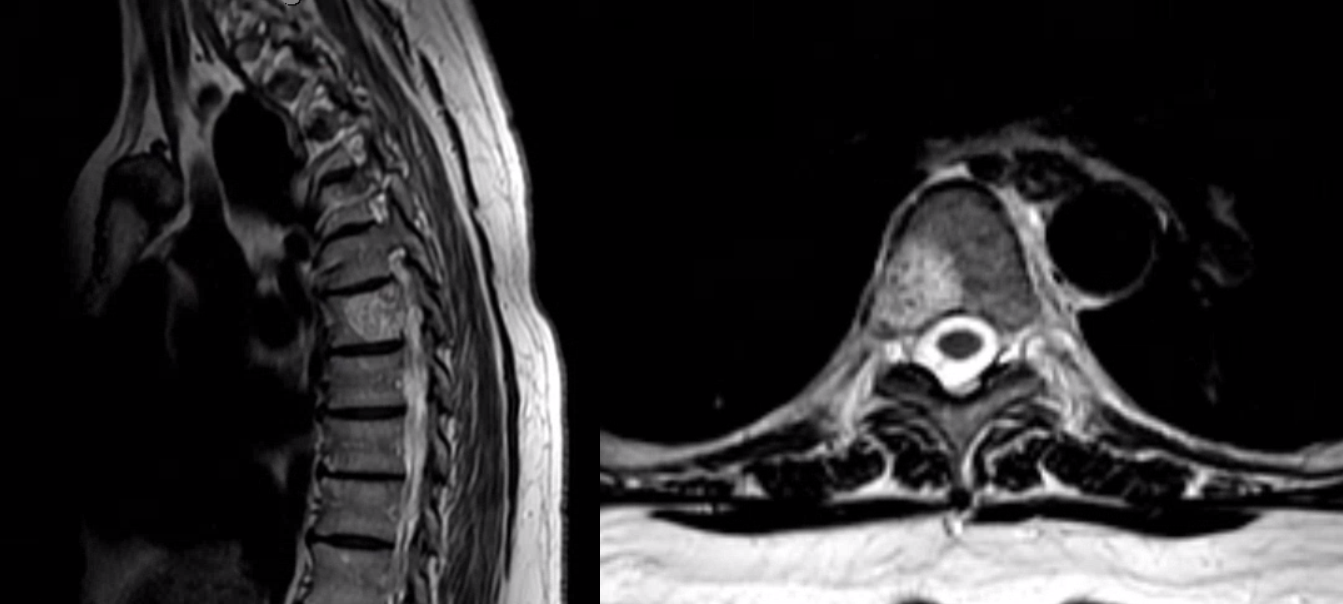
Not very vascular. Target level
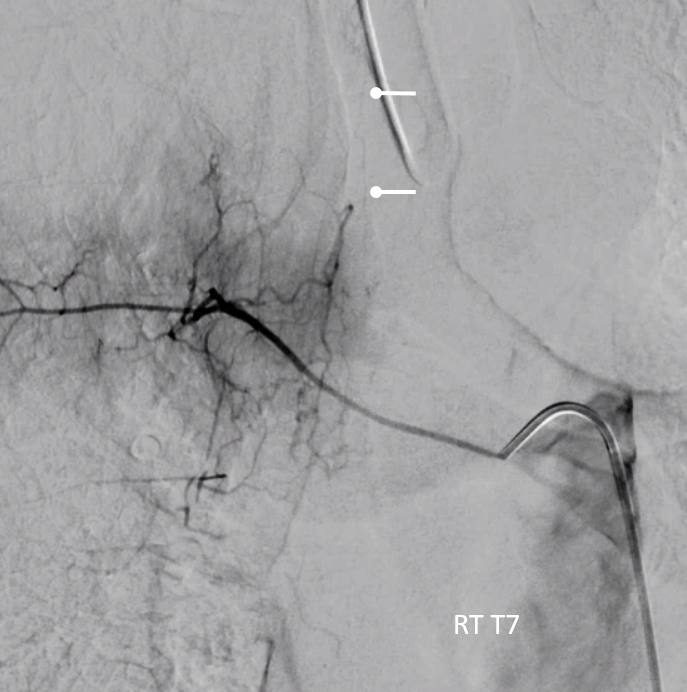
There is contribution to asa (ball arrows) from adjacent Rt T7 level, but no supply to hemangioma
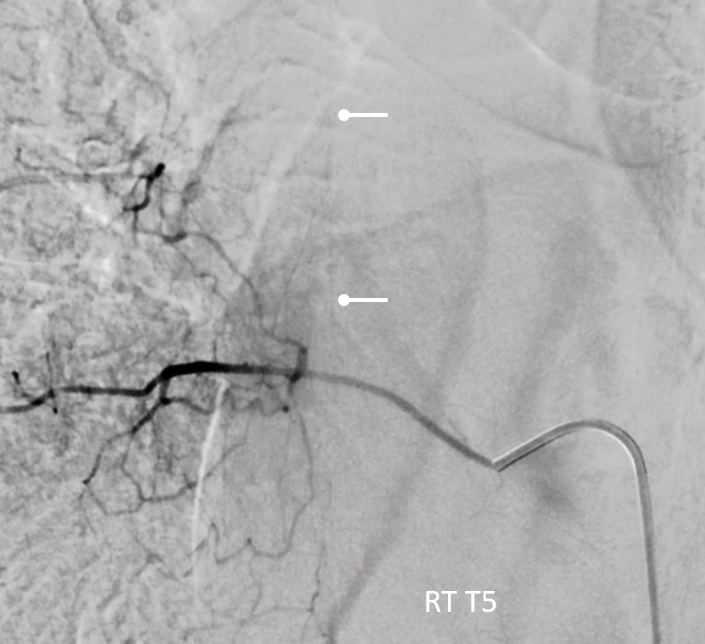
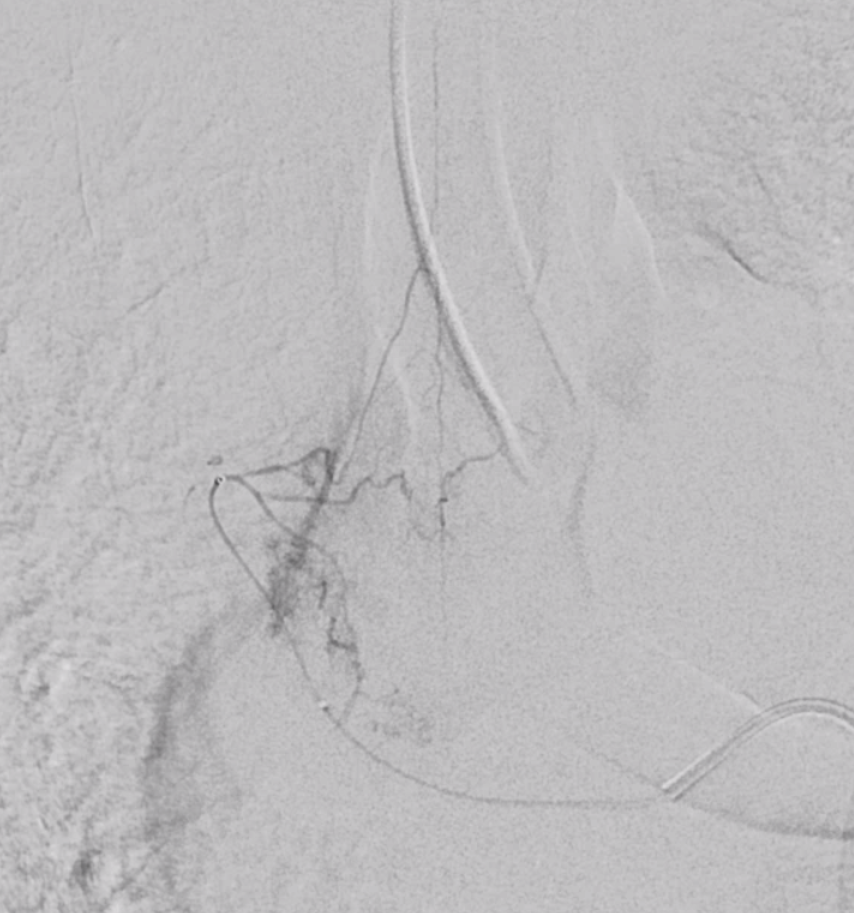
From right T5, there is another radiculomedullary artery contribution to the ASA (ball arrows), as well as supply to the hemangioma via the lateral dural artery
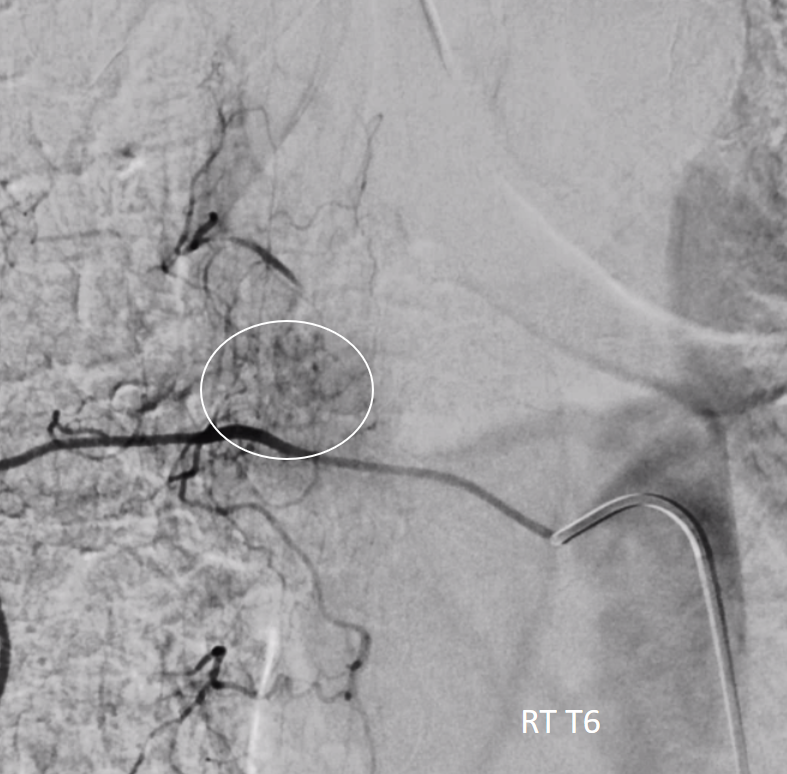
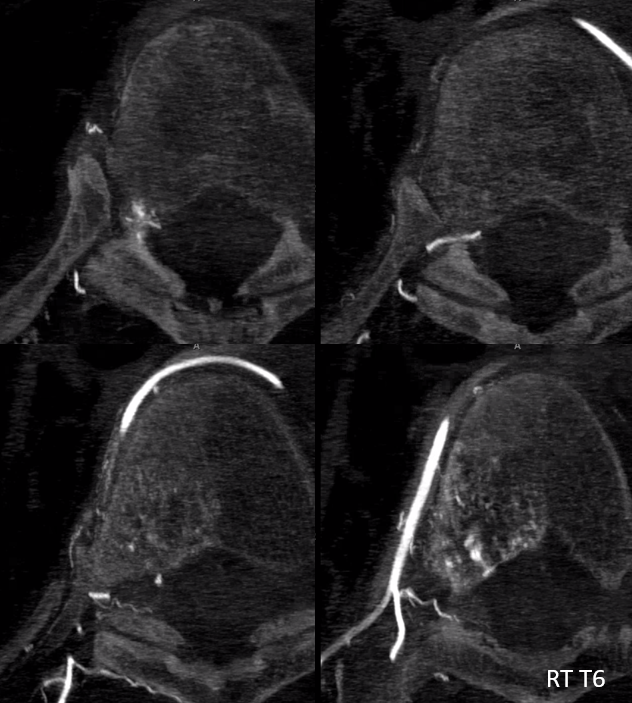
Dyna of RT T6 — most supply is derived from the radiculodural branch
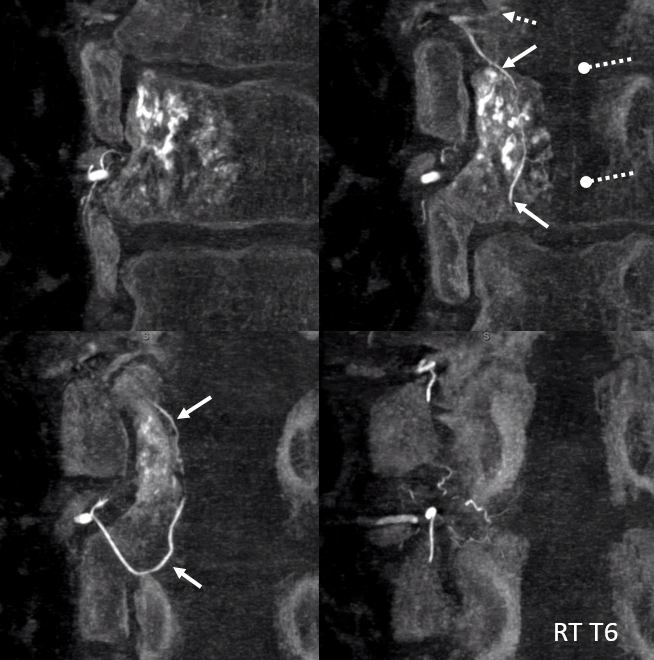
Coronal images of Rt T6 injection show faint opacification of the ASA (ball dashed arrows) — implying that there is an anastomosis somewhere. We know there are asa contributions from both adjacent levels — Rt T5 and Rt T7. So have to be careful. The likely connection is via the lateral dural artery (white arrows) a longitudinal intradural anastomosis between adjacent radiculodural arteries
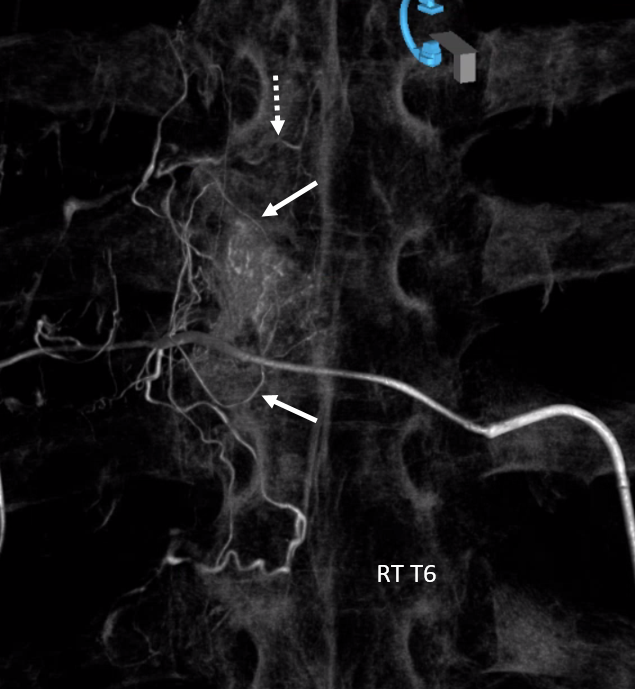
Volume Rendered Image — nice right? The radiculomedullary artery of Right T5 is visualized here (dashed arrow) — either via the lateral dural artery and/or via the prevertebral (extradural) anastomoses (not shown by arrows — if not sure what those are, see Spinal Arterial Anatomy page)
Stereo pair

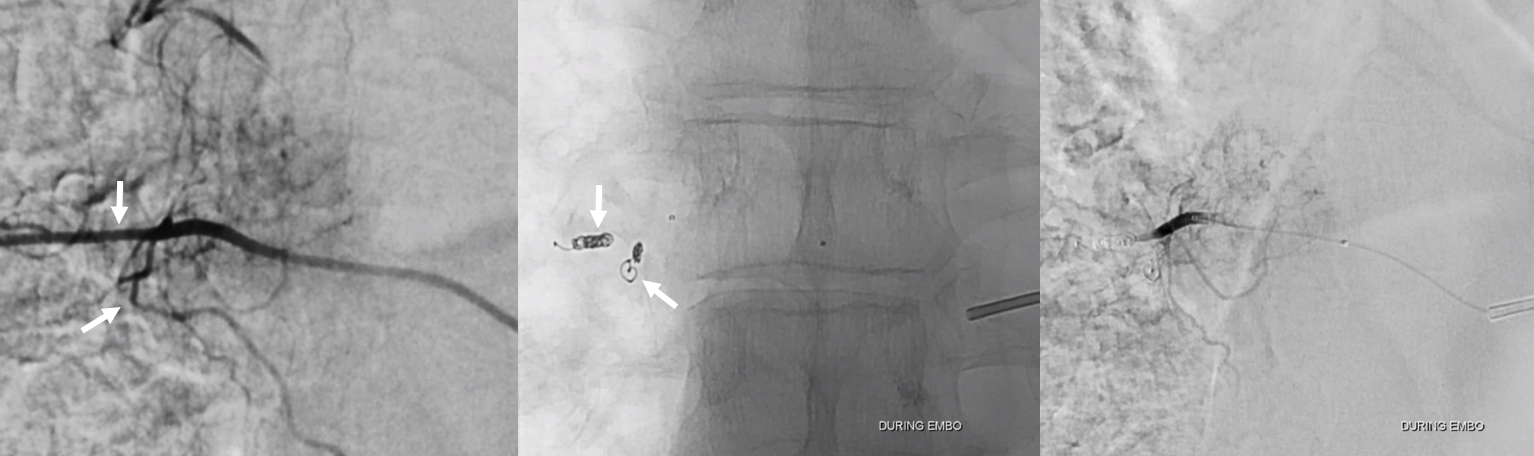
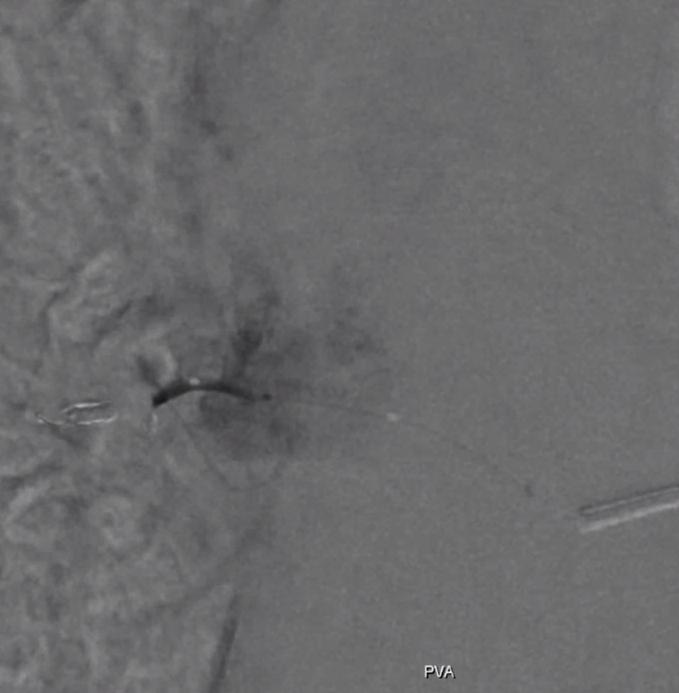
Two coils are placed distal to the radiculodural branch — in the intercostal artery and in the dorsal ramus distal to radiculodural origin — to block particle flow into unwanted territories. This leaves pretty much only the radiculodural artery open for PVA Contour 45-150 micron particle embolization (rightmost image)
PVA embo
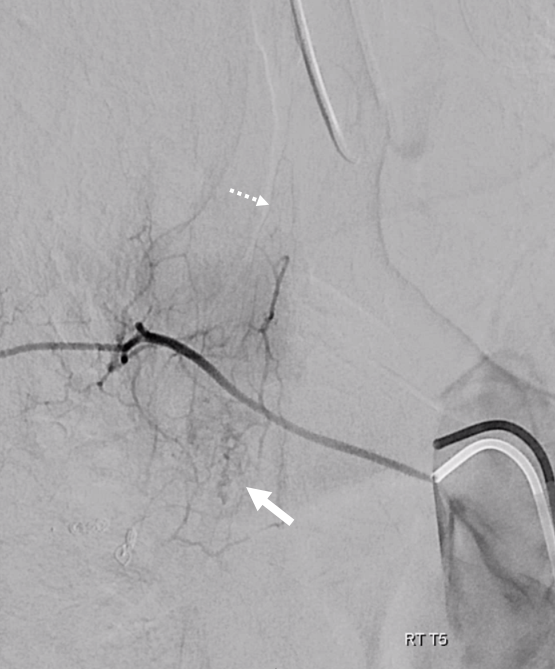
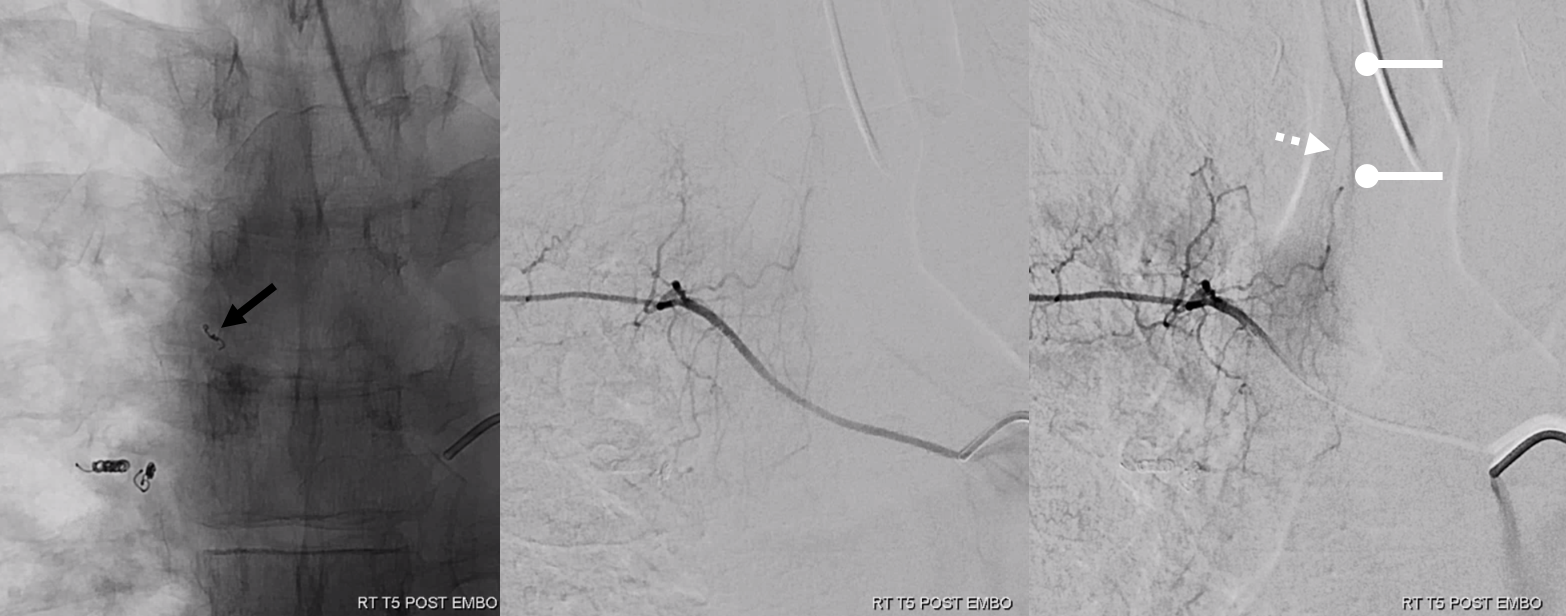
Post embolization control angiogram of right T5 — reconstitution of the upper portion of the hemangioma via the lateral dural branch (white arrow points to the stump of this branch post immediately preceeding right T6 embo). The radiculomedullary artery is shown by dashed arrow.
No more embo? Or is there a way?
Coronal Dyna CT images. The radiculomedullary artery is again shown by dashed white arrow, anterior spinal by ball arrow. The lateral dural artery reconstituting the residual hemangioma is shown by white arrow. Open arrow points to the same lateral dural artery stump that was embolized from below. Also present is a third branch (black arrow) — part of the epidural arcade supplying the posterior central portion of the vertebral body

Now we have a rational strategy — microcatheterization of the lateral dural branch
VR stereo pair — the three branches inside the canal are clearly visible

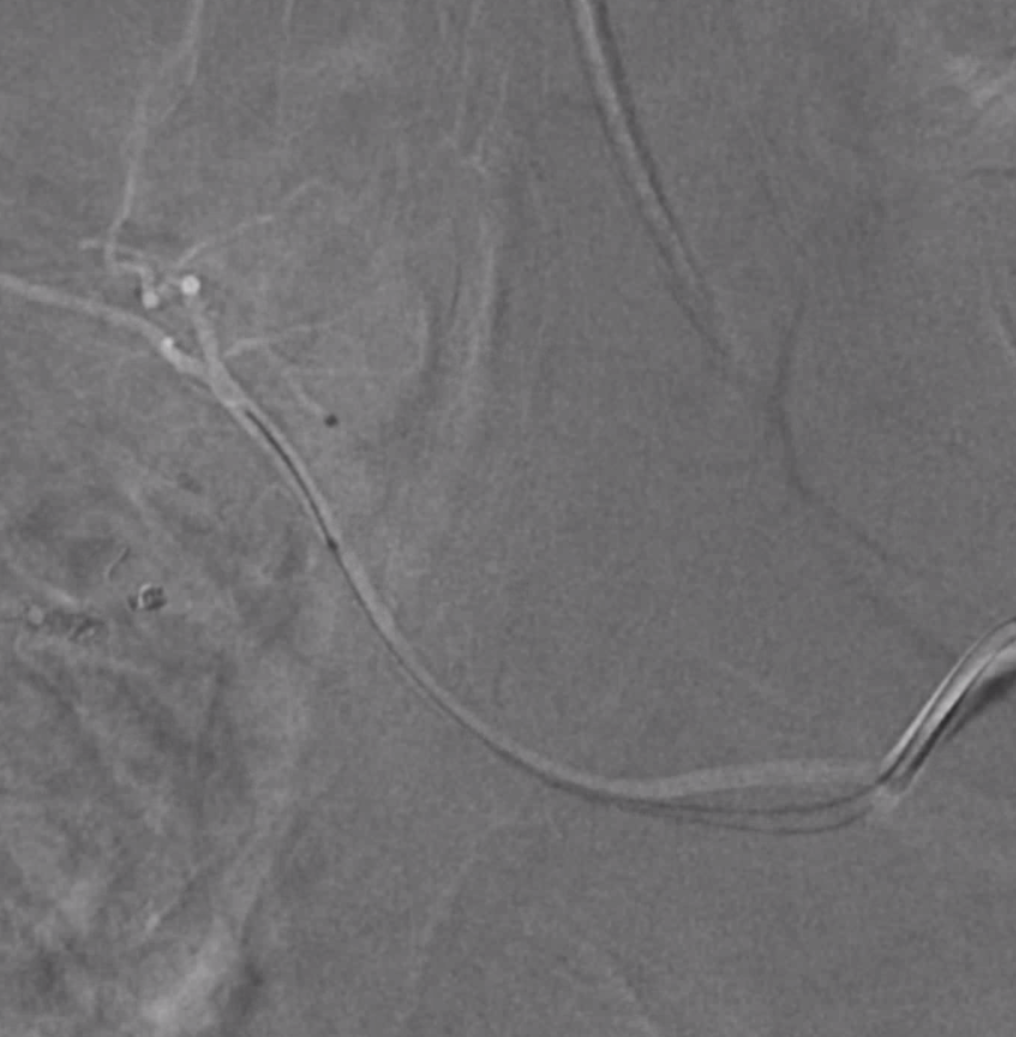
Proximal microcatheter (headway duo) injection — the three branches — radiculomedullary, epidural arcade, and lateral dural — are well seen, as well as some hemangioma blush
Lateral dural branch microcatheterization
Embolization position
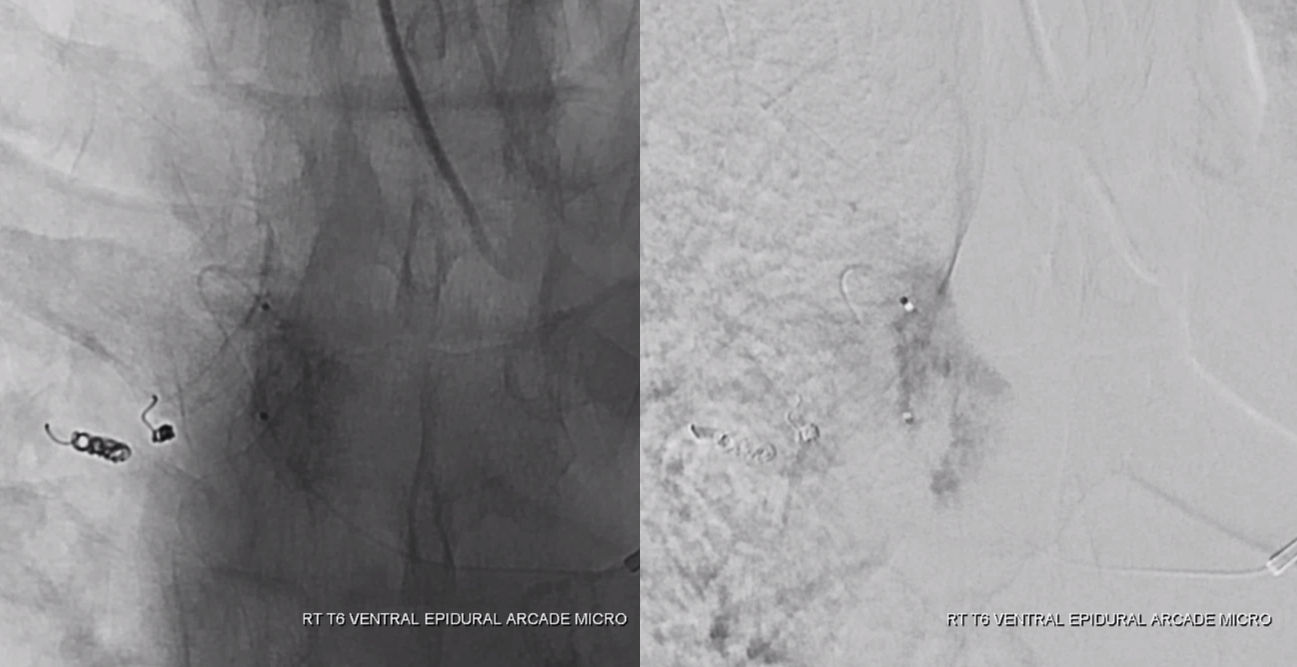
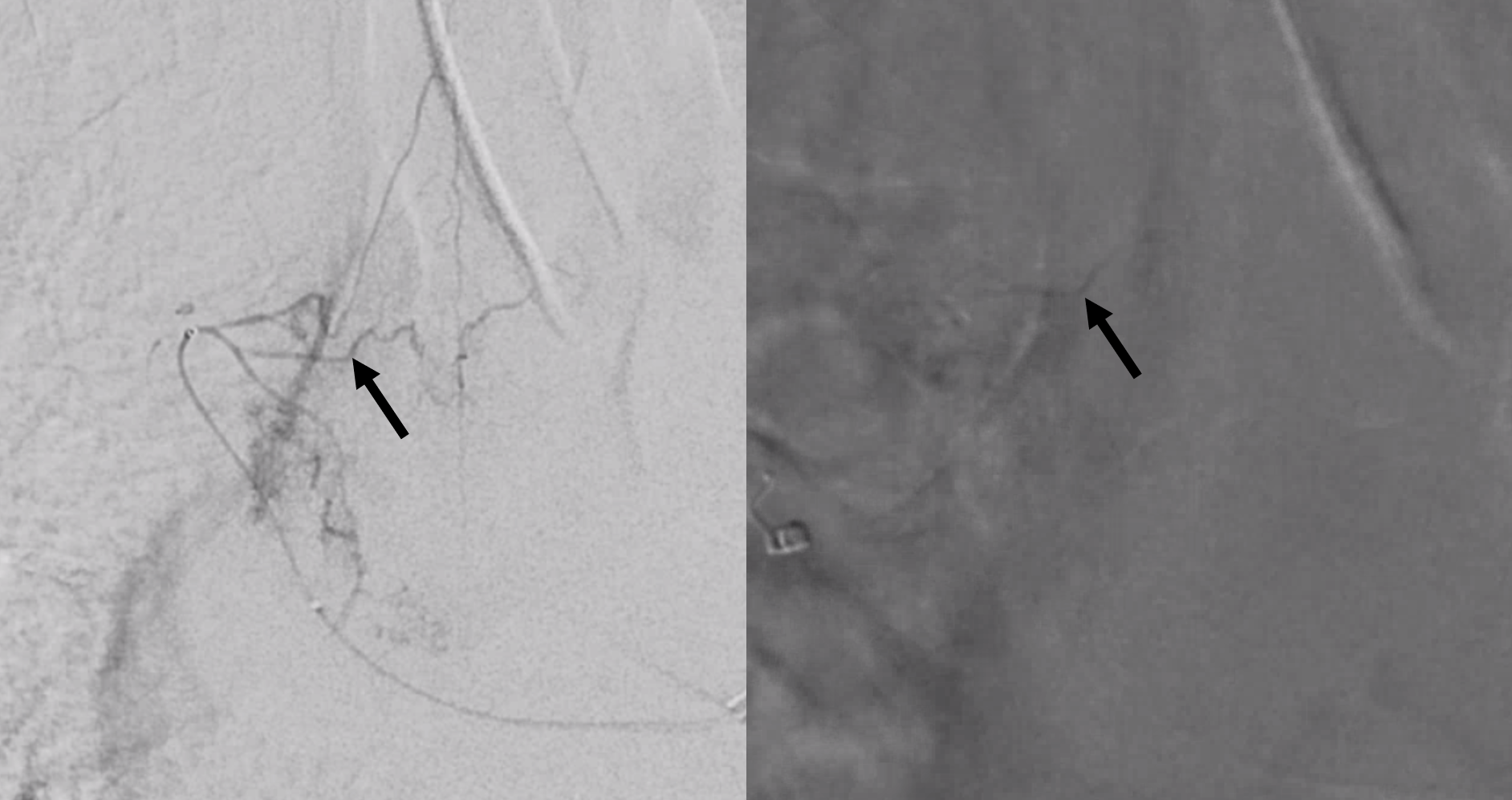
Image on right shows transient reflux of contrast/particles into the ventral epidural branch (black arrow) after filling the hemangioma – our safety margin. Any more reflux would then end up in the radiculomedullary artery, so no good. Image on left is for reference
A small coil (black arrow) is placed into the lateral dural branch. Post-embo control injection shows preservation of anterior spinal supply (white arrows)
For more cases of how to rationally embolize next to the anterior spinal artery, see:
https://neuroangio.org/parkes-weber-embolization-of-paraspinal-arteriovenous-fistula/