
Number 116b

A classic “piodural” vessel — like the Davidoff-Schechter or the Wolfschlaegger and Wolfschlaegger. Origin is from the AICA, nearly always at the “loop”, and close to or together with the Labyrinthine artery. Supplies the dura and osseous elements of petrous bone. From the “spectrum” perspective, it is in balance with the petrosal branch (MMA origin) and occipital transmastoid meningeal branches. Runs in the subarcuate canal or canaliculus (aka the petromastoid canal, aka the antrocerebellar canal of Chatellier). The more obscure the structure the more names it has from mutually unaware literature descriptions. It is truly an osteodural branch (dura and bone supply). Clinically significant as participating in virtually all petrous alex dural fistulas.
Normal subarcuate artery is impossible to see on 2D-DSA. Visualization is inconstant by High Resolution Cone Beam CT (HR-CBCT) — see additional images here. It is not clear if visualization is limited by resolution since the artery is not always seen surgically or post-mortem — where it seems to be present in about 1/3 of cases according to Salgado-Lopez, Leonel, Aydin and Peris-Celda and in all cases by Tekdemir Aslan and Elhan. More research is nonurgently needed.
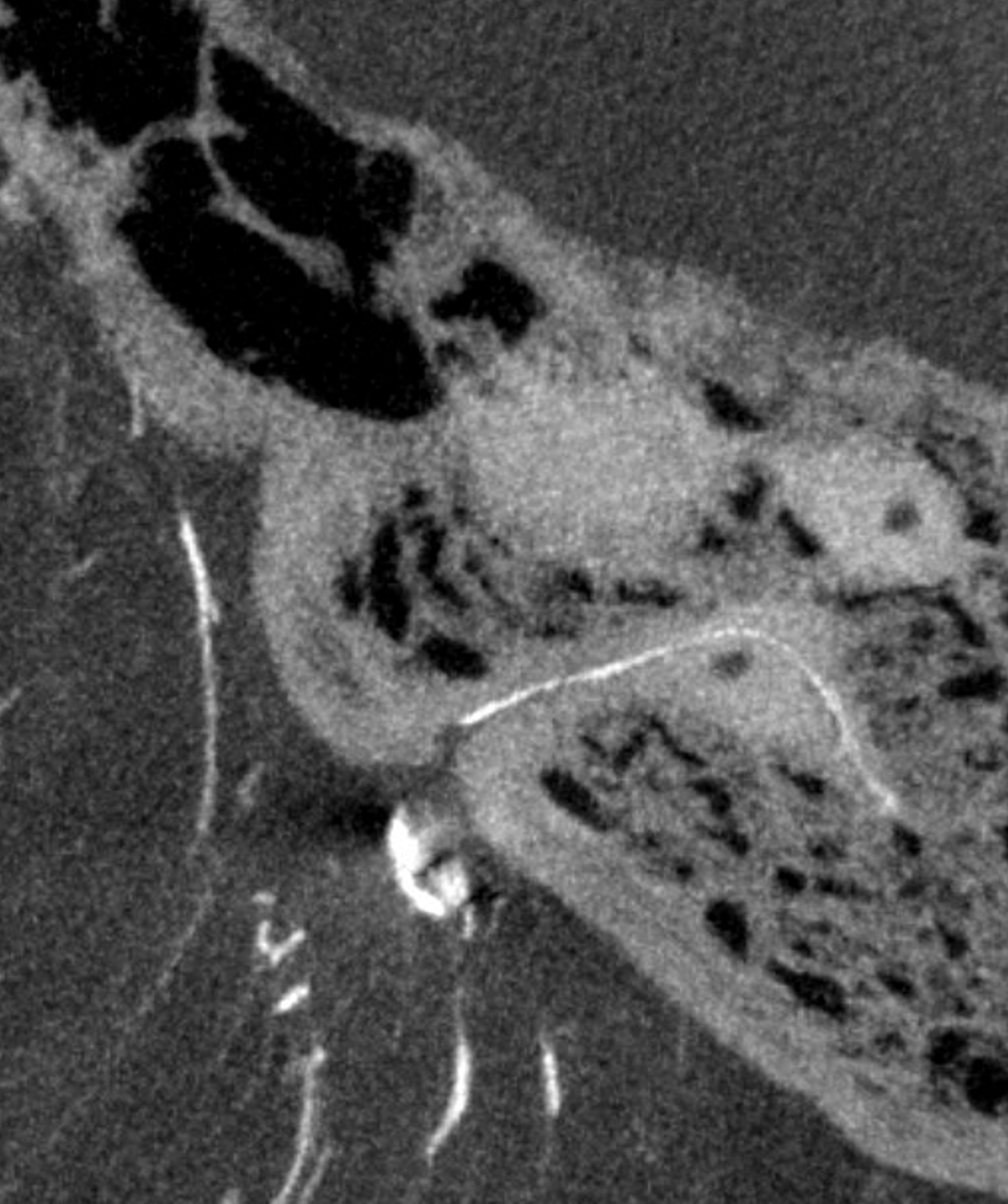
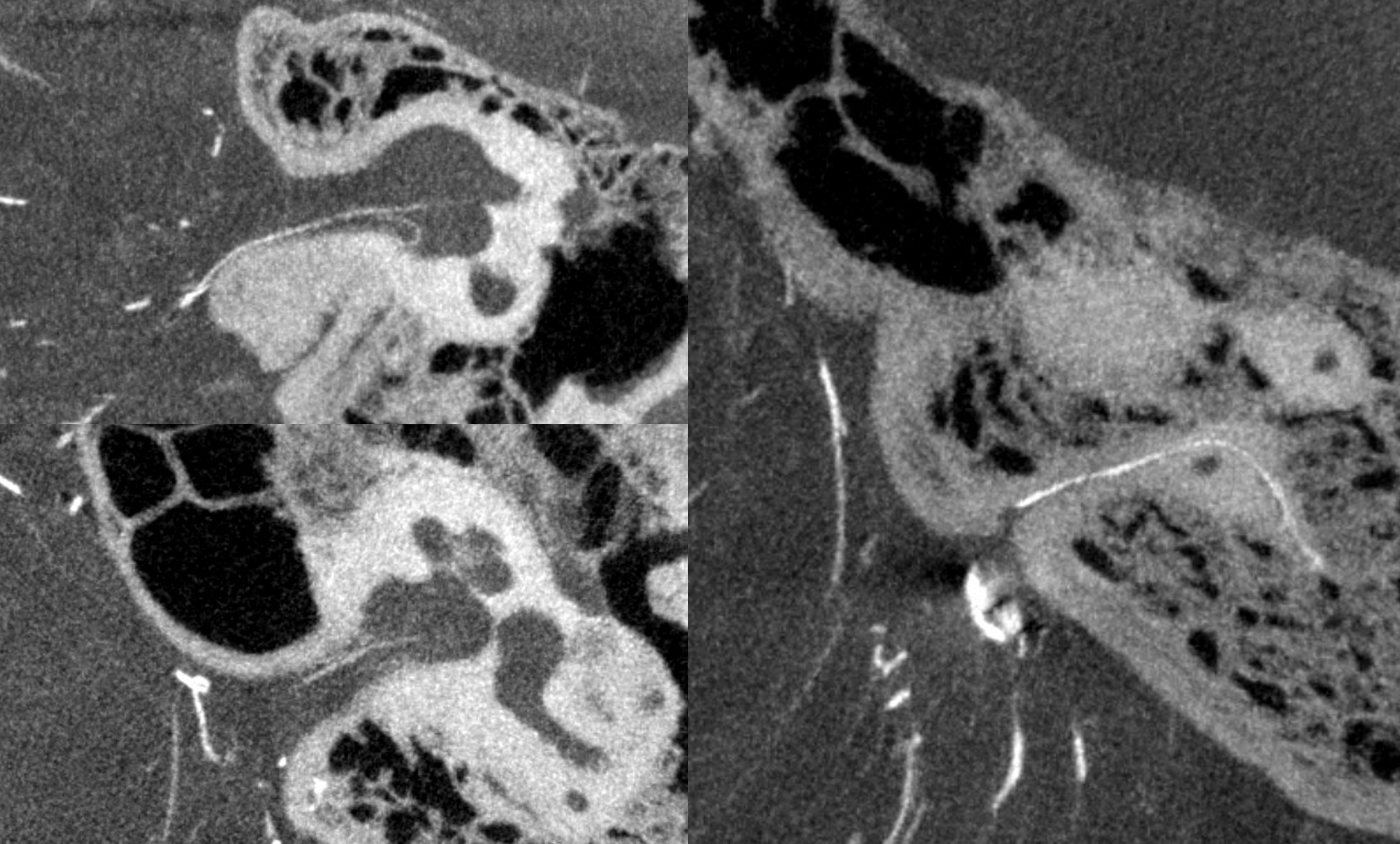
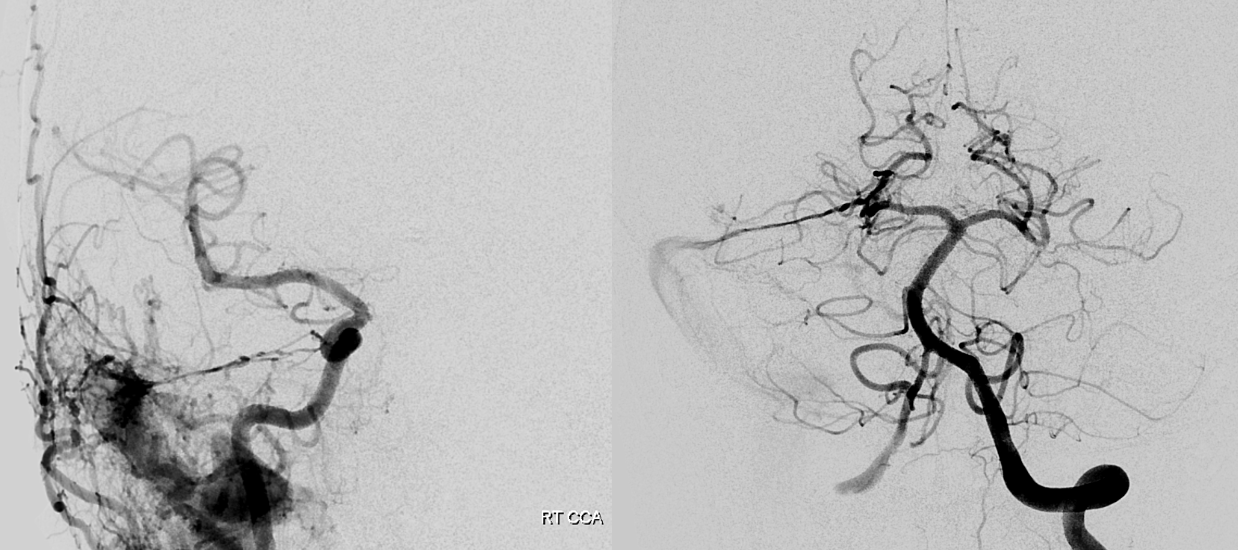
Below are some examples — biggest one we’ve ever seen — image on right. Also see the Labyrinthine artery in same collage — 2 images on left.
Same patient — left side
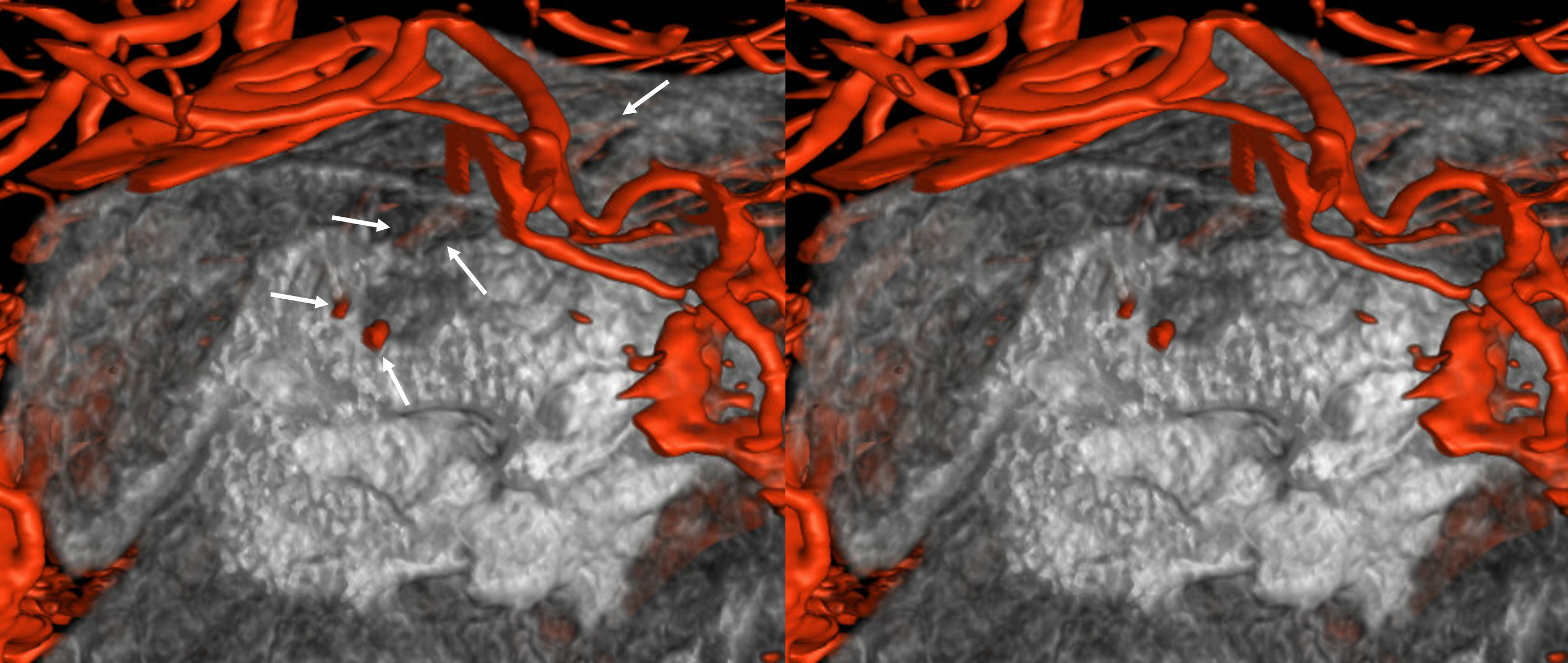
With arrows

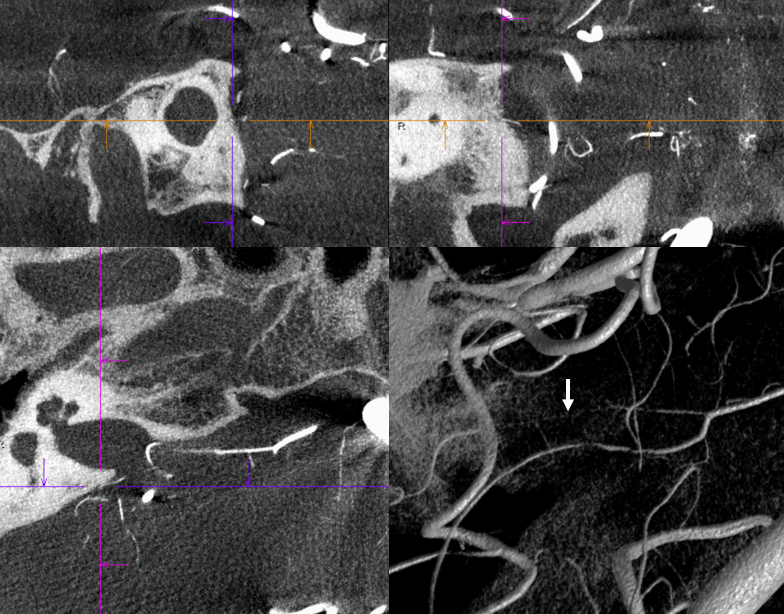
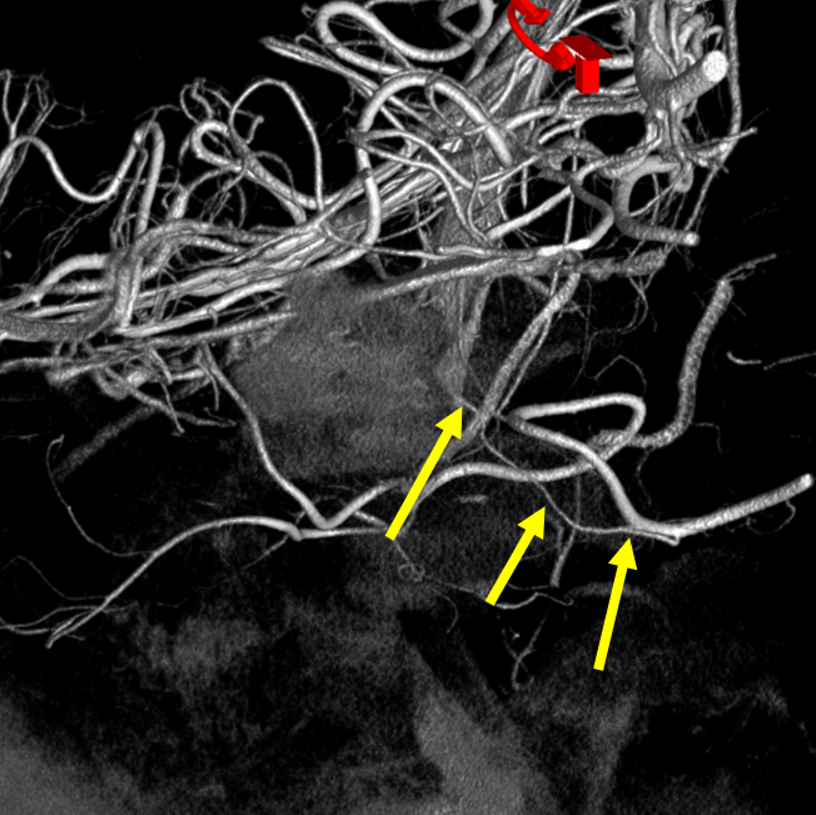
VR image of the same case as above. See the subarcuate artery (arrows) inside the petrous bone, below the arcuate eminence
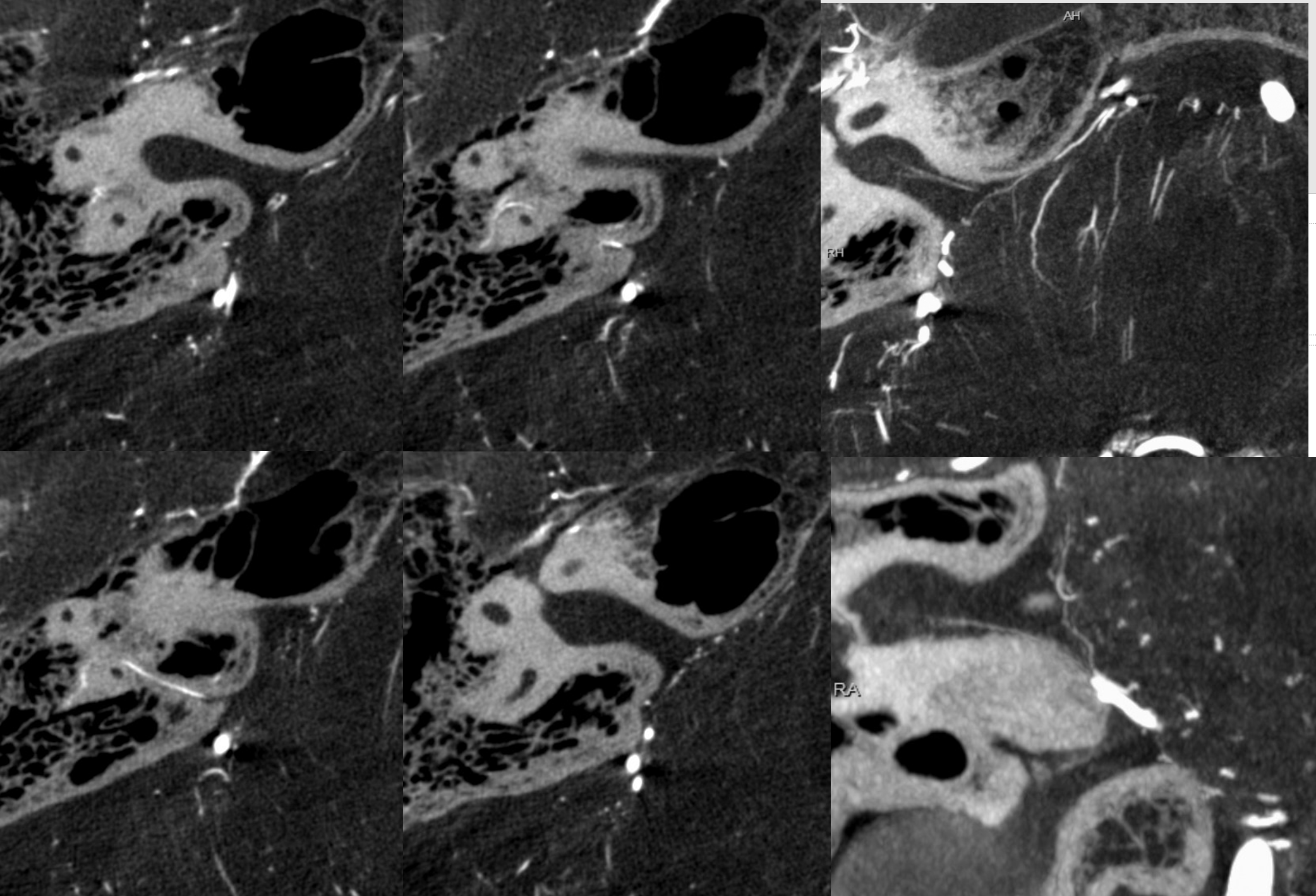
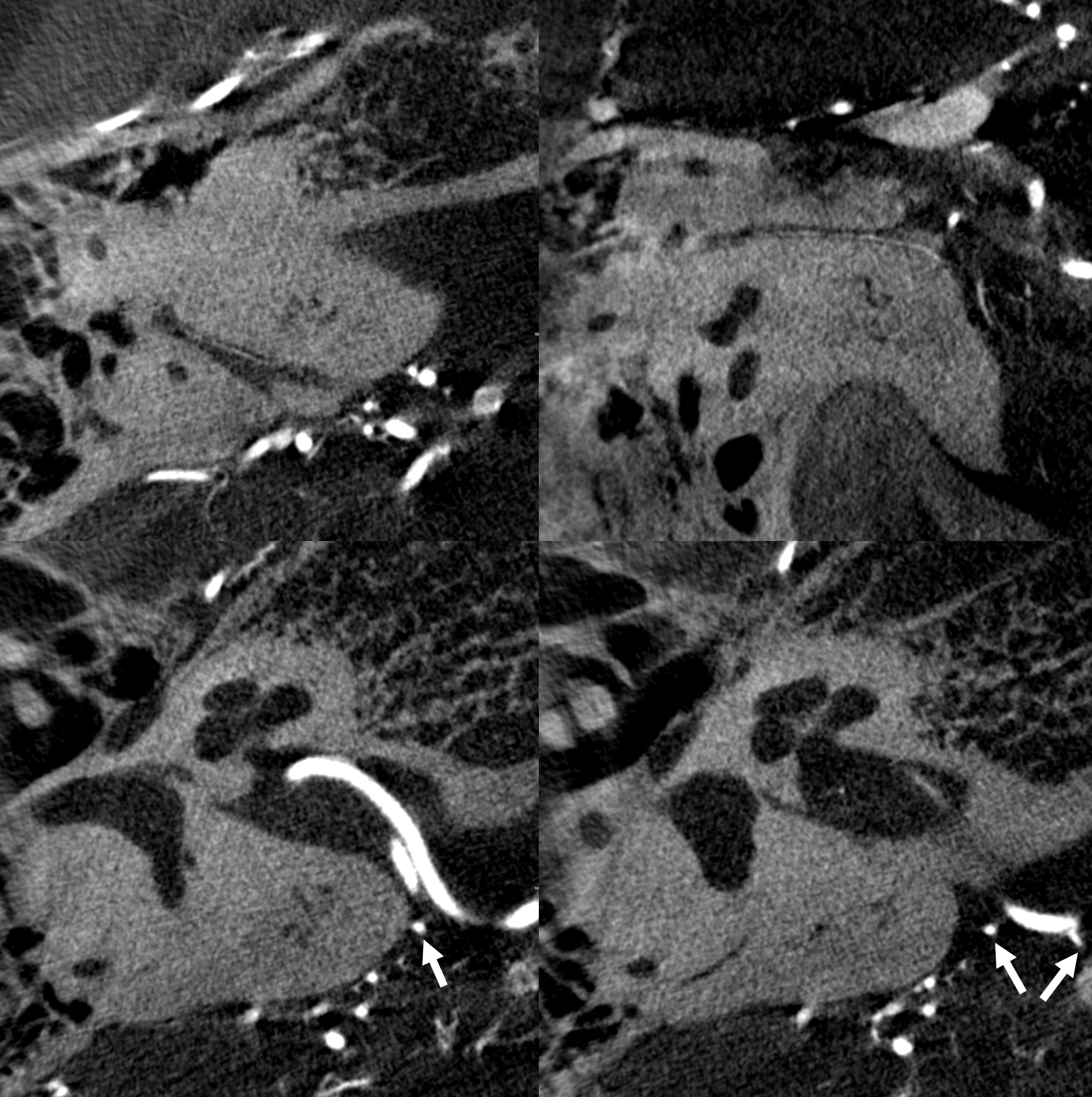
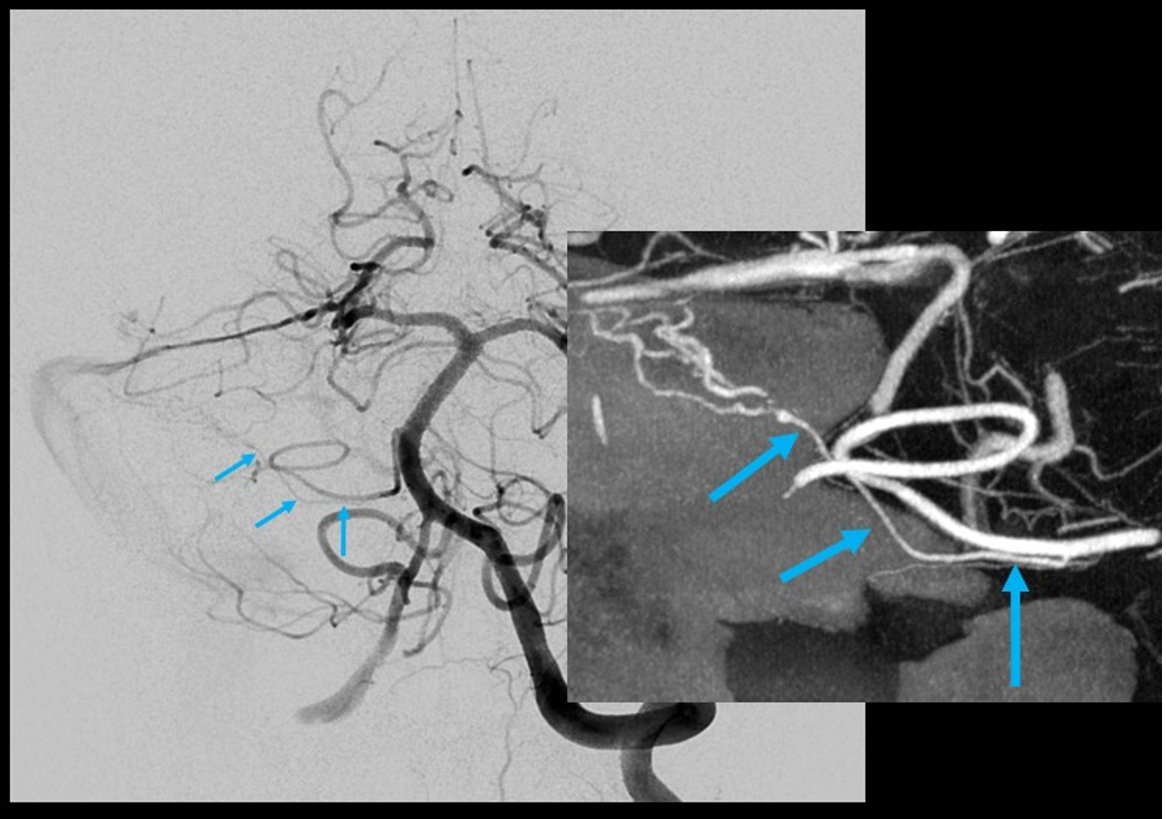
Below another example of normal appearance (dashed arrows) in the petromastoid canal. Solid arrows point to an AICA branch from which it arises. Arrowhead points to the labyrinthine artery
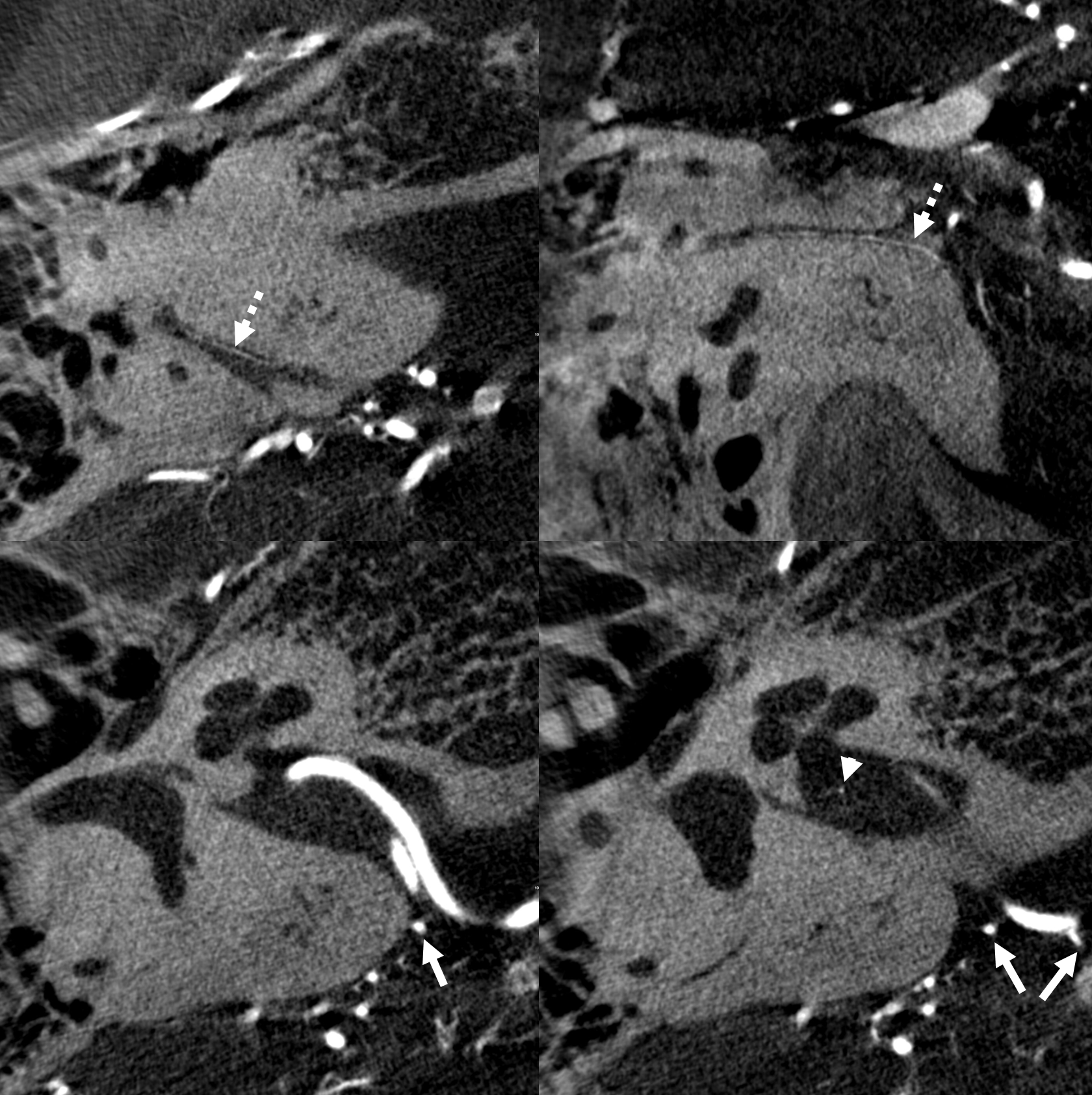
Sin Labels
Uno mas
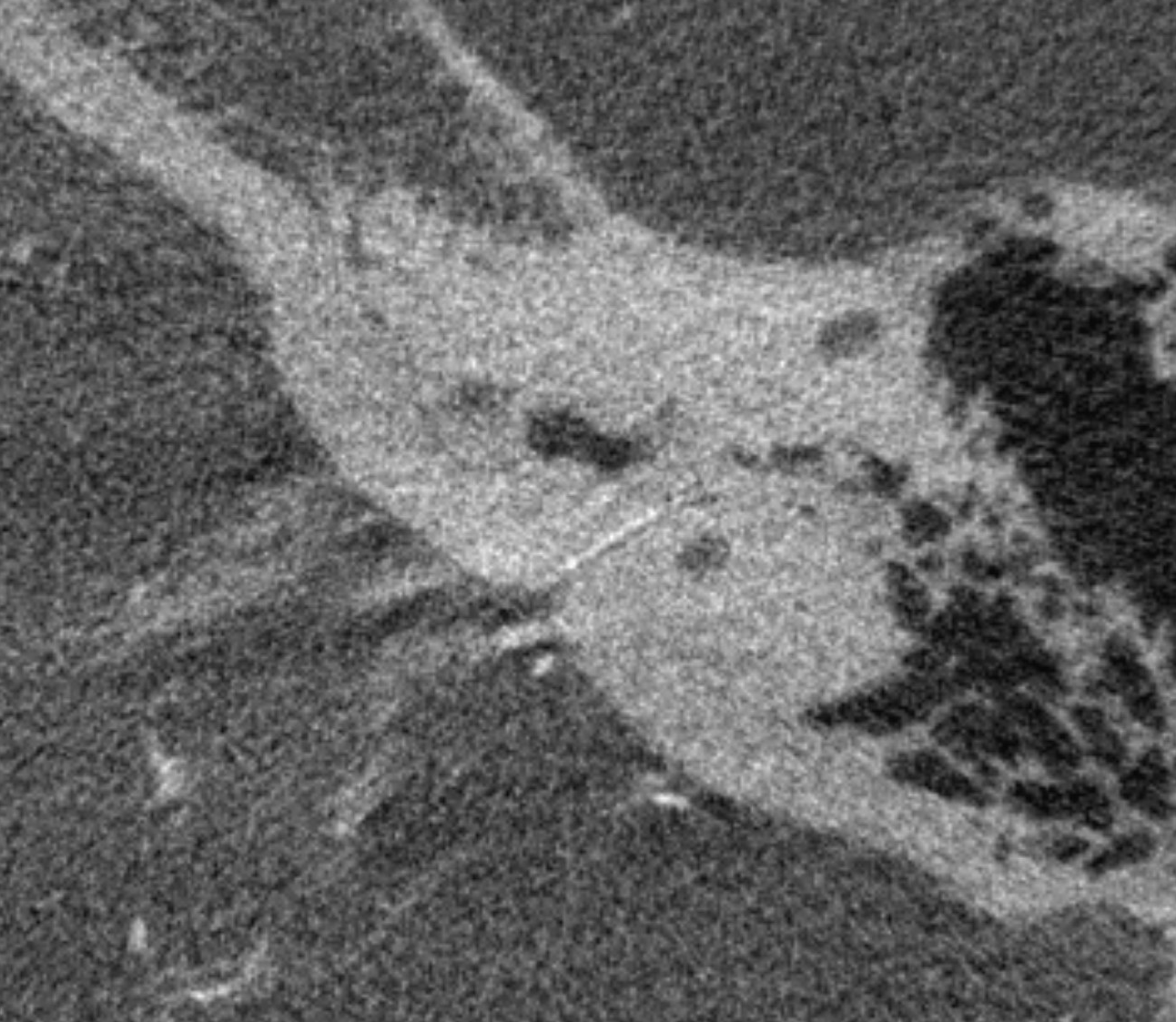
Another one — barely to be seen in the canal. The smaller it is, the less bone and dura it supplies
Subarcuate Artery and Dural Fistulas
One time we can see this artery a bit more consistently is high flow shunt states — dural fistulas specifically. Here is a sigmoid sinus one, courtesy Dr. Eytan Raz, with pial contribution mainly from the SCA. A very small amount of AICA supply is present also, but impossible to say more without DYNA
DYNA CT MIP images show the arcuate artery supplying fistula. The cochlear branch is too small to see (might be the very small lower one)
It is not a good idea to use AICA as embolization route — too small and too eloquent. Below different case example shows why not.
Here, a petrous apex fistula is supplied by SCA, AICA (arrow), and MMA (not shown)

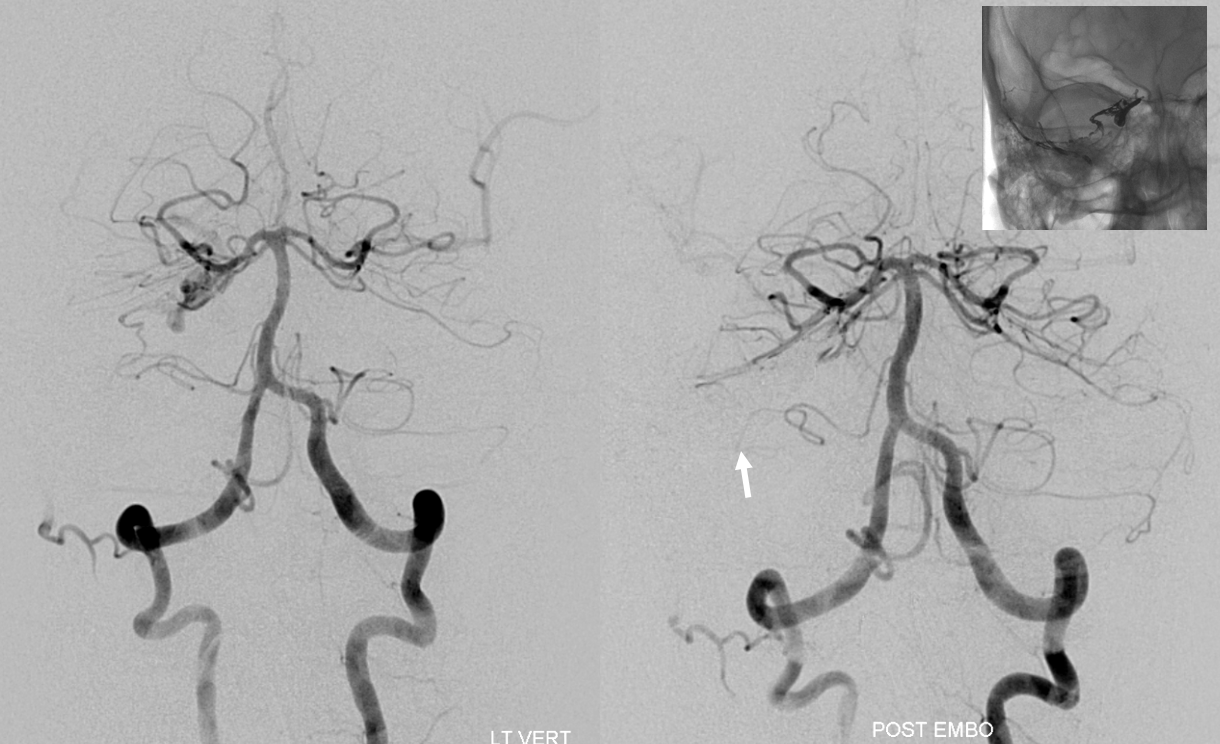
An ill-advised catheterization of the AICA (left image) results in a perforation sustained during attempted navigation of the AICA loop (right image arrow), which spontaneously seals after minimal bleeding. The catheter was wedged in the AICA, and perforation was not the problem…
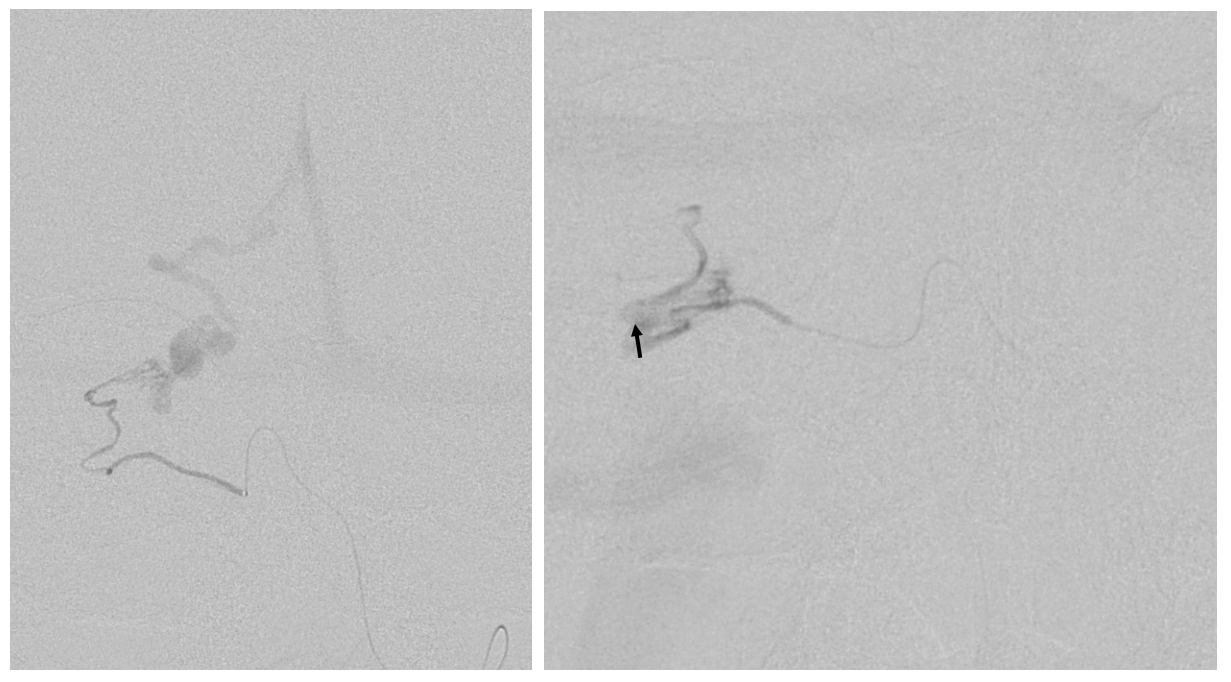
The fistula is cured via MMA onyx injection. However, at end the distal AICA has gone down by thrombosis after perforation (compare pre-embo left and post-embo right images). The patient lost hearing about 12 hours after procedure despite permissive hypertension — probably because collaterals to inner ear went down.
Let this page end with a warning — getting beyond the AICA loop is technically challenging, and deafness is bad enough — but the often-associated tinnitus can be even worse. Be careful