The material/cases in this section were collected and organized by Dr. Guglielmo Pero. A neuroangio team effort!
Multiple Cone Beam Acquisitions and Fusions in a Complex AVM Treated by Targeted Embolization and Gamma Knife Radiosurgery
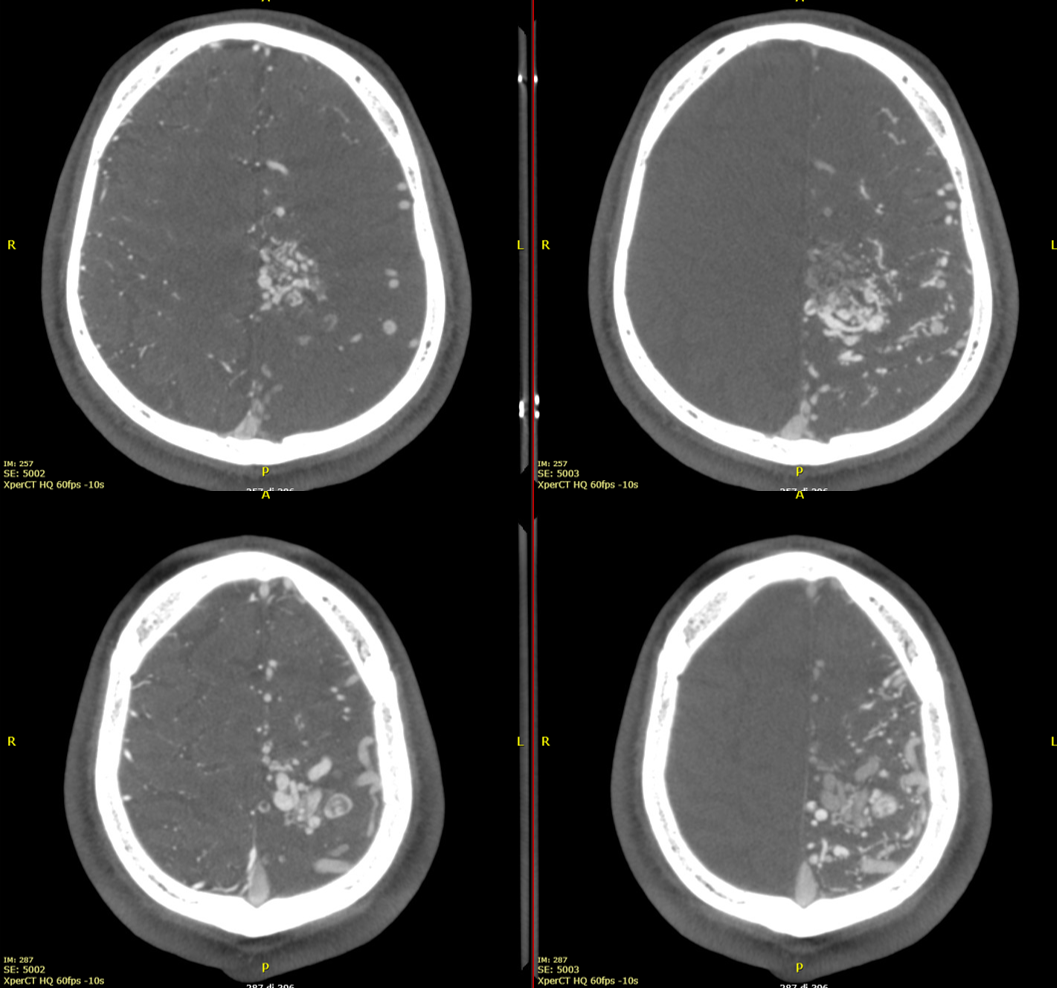
This is an Xper-CT acquisition done with the 48 cm FOV, HR 60 fps, 10-seconds protocol. We manually injected 30 ml of 50% contrast media (250 mg/ml), with a 30 ml syringe, beginning the injection 4-5 seconds before starting the acquisition.
The first pass to have good Xper-CT images for GammaKnife is a new reconstruction with 100% FOV, stent protocol, and 5123 resolution. The reconstruction must include the whole head.
Images will be sharper and with better contrast resolution.
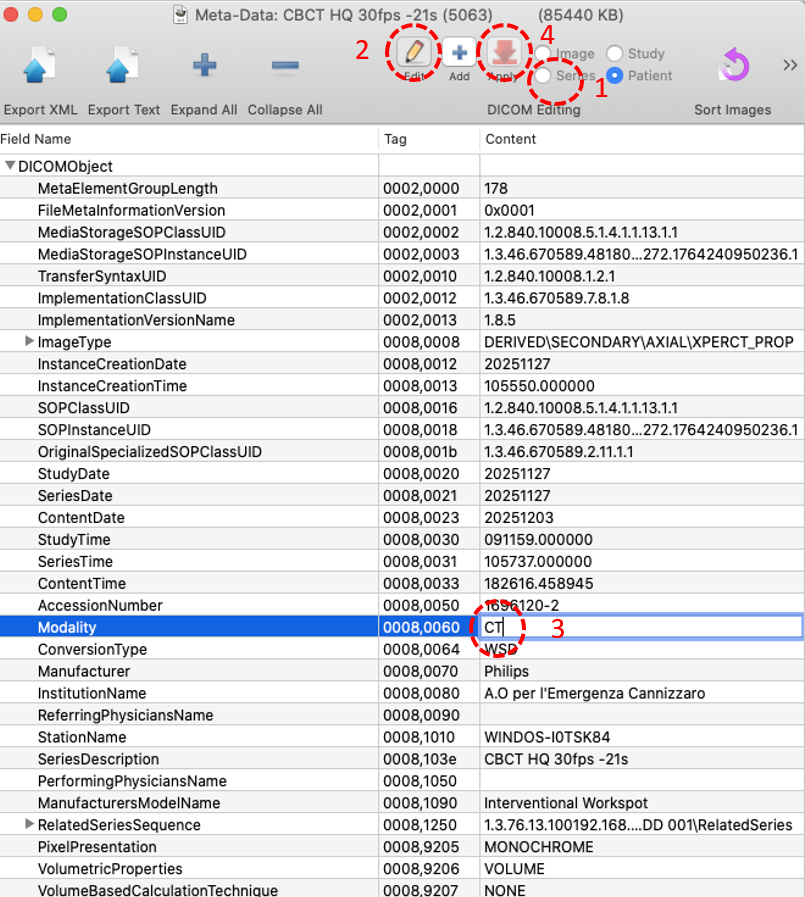
To import the Xper-CT images in the GammaPlan software, we have to change the image modality in the DICOM tags from XA to CT. I do it with Horos.
Open the Xper-CT acquisition and then its metadata window.
- Select the series level option.
2) Activate the editing mode of the metadata pressing the “edit” button.
3)Find the modality line, double click on it, and change from XA to CT modality.
4)Press the ”apply” button to make the change stable.
Now you can send the series to the GammaPlan.
Right and left ICA injections
Vert Injection
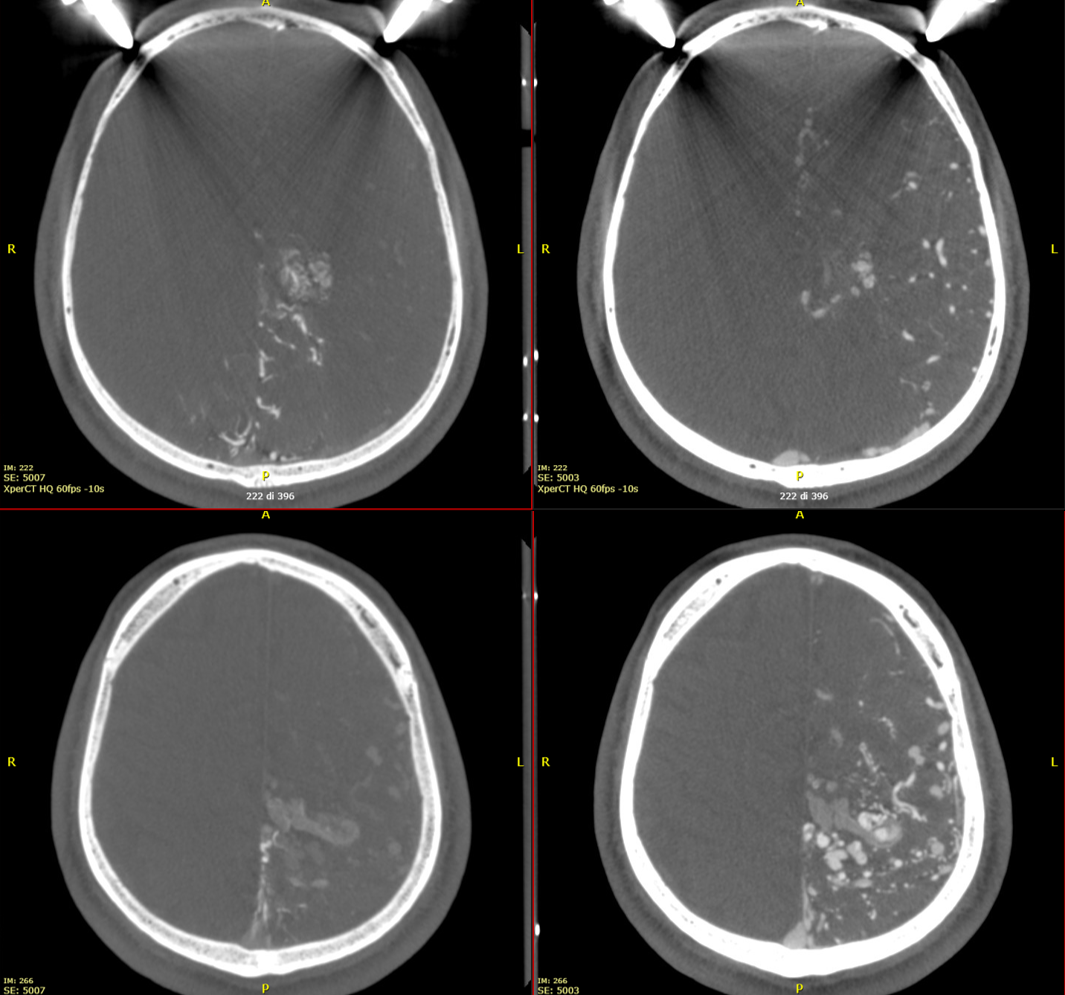
Fusion!
Another suer useful tool is the fusion of two different datasets (one for each AVM feeder).
First of all, open one of the two (or three, or more) datasets; then activate the fusion option and the select the dataset you want to fuse.
Viva Philips for language support! Imparare e vivere!
Then coregister the datasets; if the results are not optimal, you can manually improve the correspondence of the two datasets.
Result
These are examples of a complex AVM. Unfortunately, we cannot save the fused datasets as a new dataset to be imported in the GammaPlan software, but just as videos.
Same problem in Siemens — the fusion datasets are not DICOMs. Work on it, you both…

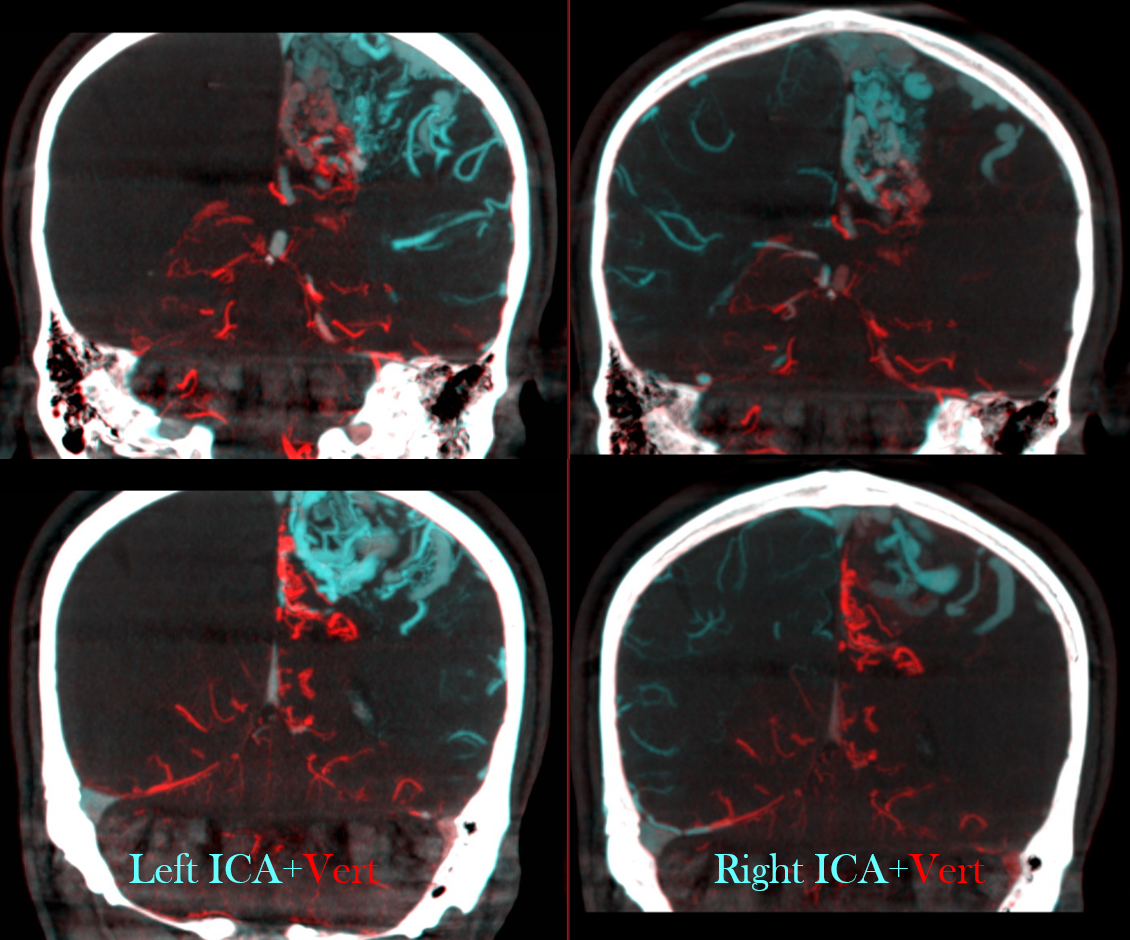
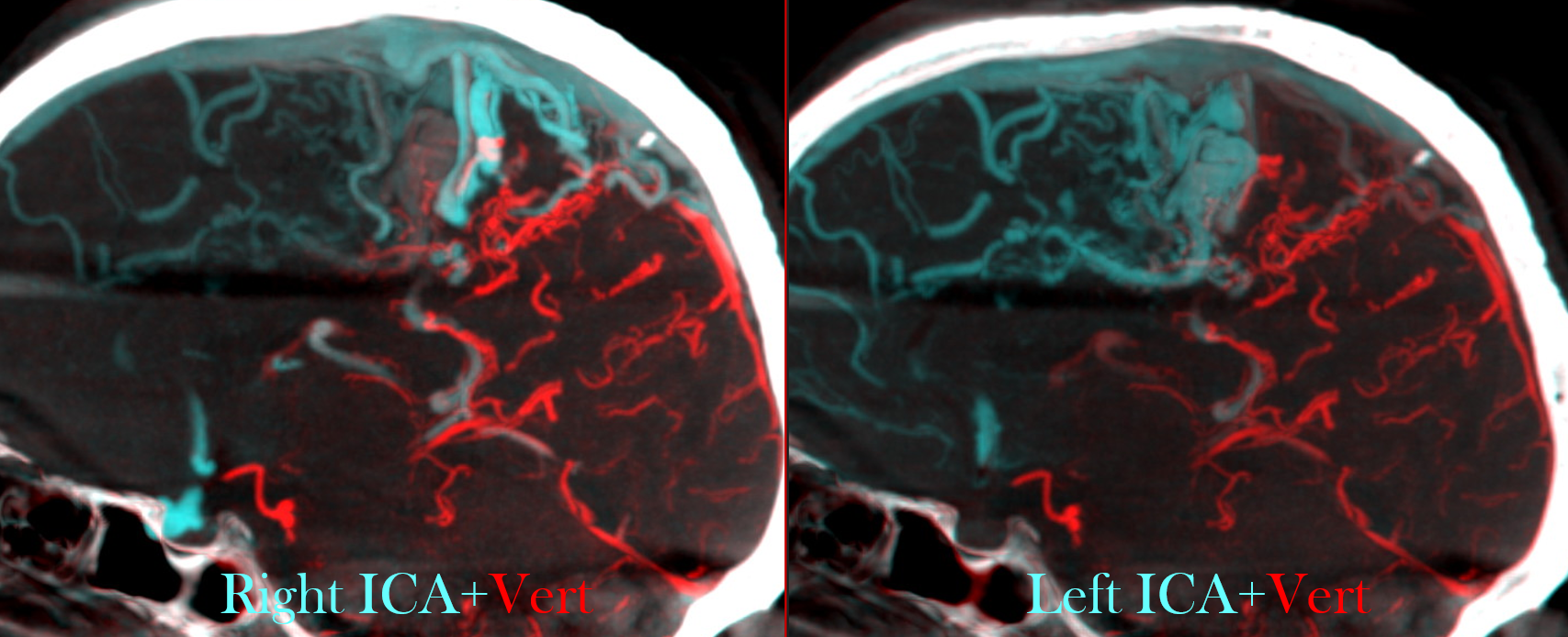
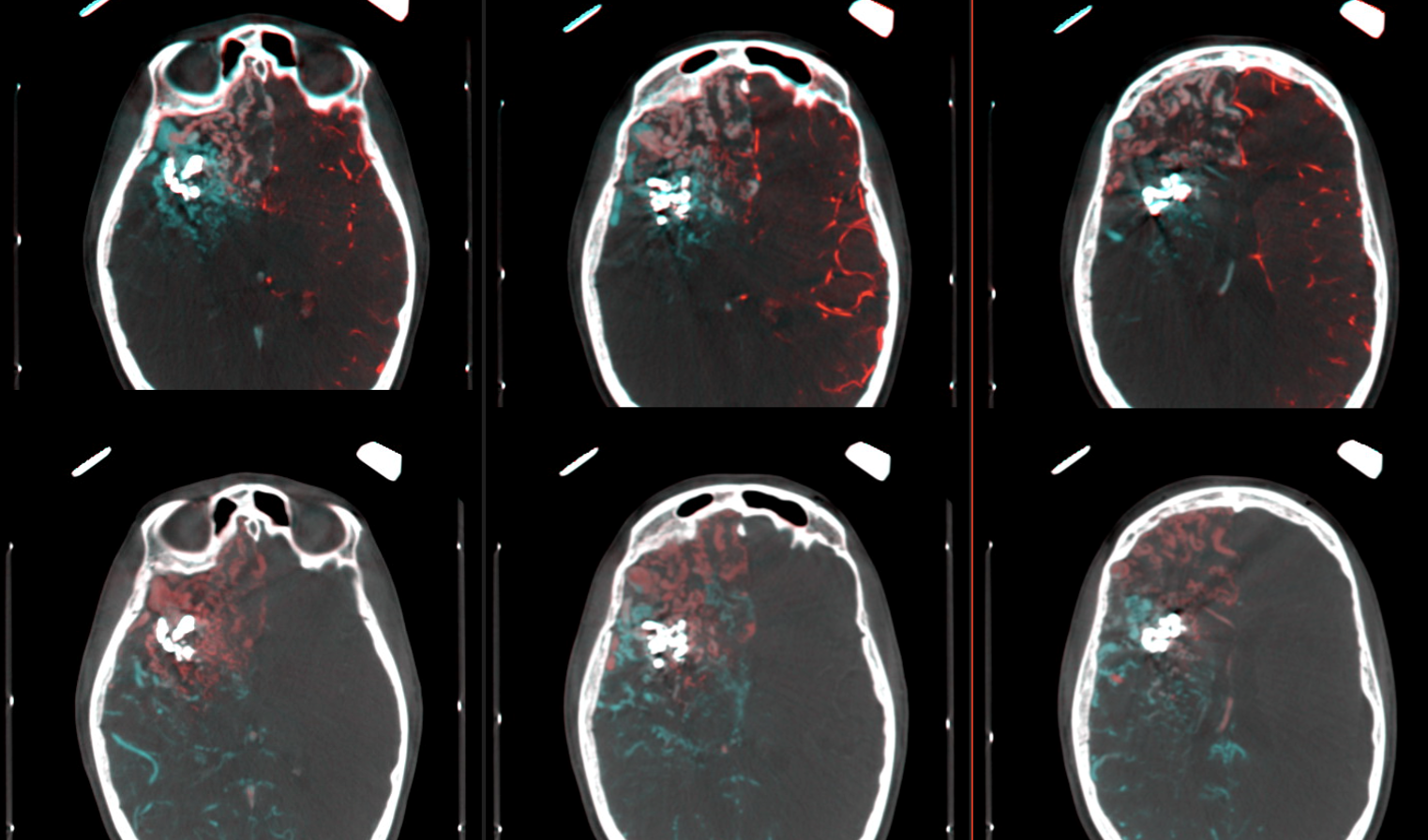
Here we see fusion of right (blue) and left (red) ICAs in the upper line and right ICA (red) and posterior circulation (blue) in the lower line. In white you see the cast of glue injected into some large AV shunts before GK.
Although this page is not about embo technique, or outcome, or whatever multiple clinical itch questions or comments you might have, the point to be made is that gamma knife does a terrible job with macro / large intranidal shunts. If there is any chance for it to work at all, close the big shunts sub selectively and maybe some of the vein (just not the whole vein…) and gamma knife the smaller vessels which are probably not even part of the nidus to begin with… It does work better.
Note that a cyanoacrylate was used here, not EvOH. That’s why anyone who wants to attack an AVM should know how to use glue. This job is for glue.