
Referred by Dr. Kister
Knowledge of vascular neuroanatomy — the free, unrestricted dissemination of which is the primary mission of neuroangio.org — is key to planning and execution of a rational treatment strategy. This case of a middle-aged man with progressive back and lower extremity pain, foot dysesthesia, and recent onset of lower extremity weakness highlights many anatomical concepts and their clinical importance.
This man had a prior MRI study where dural fistula was not suspected, nor was it seen in retrospect
Here are standard T2 and post-contrast T1 images. There is diffuse cord edema but no obvious increased vascularity adjacent to the cord.
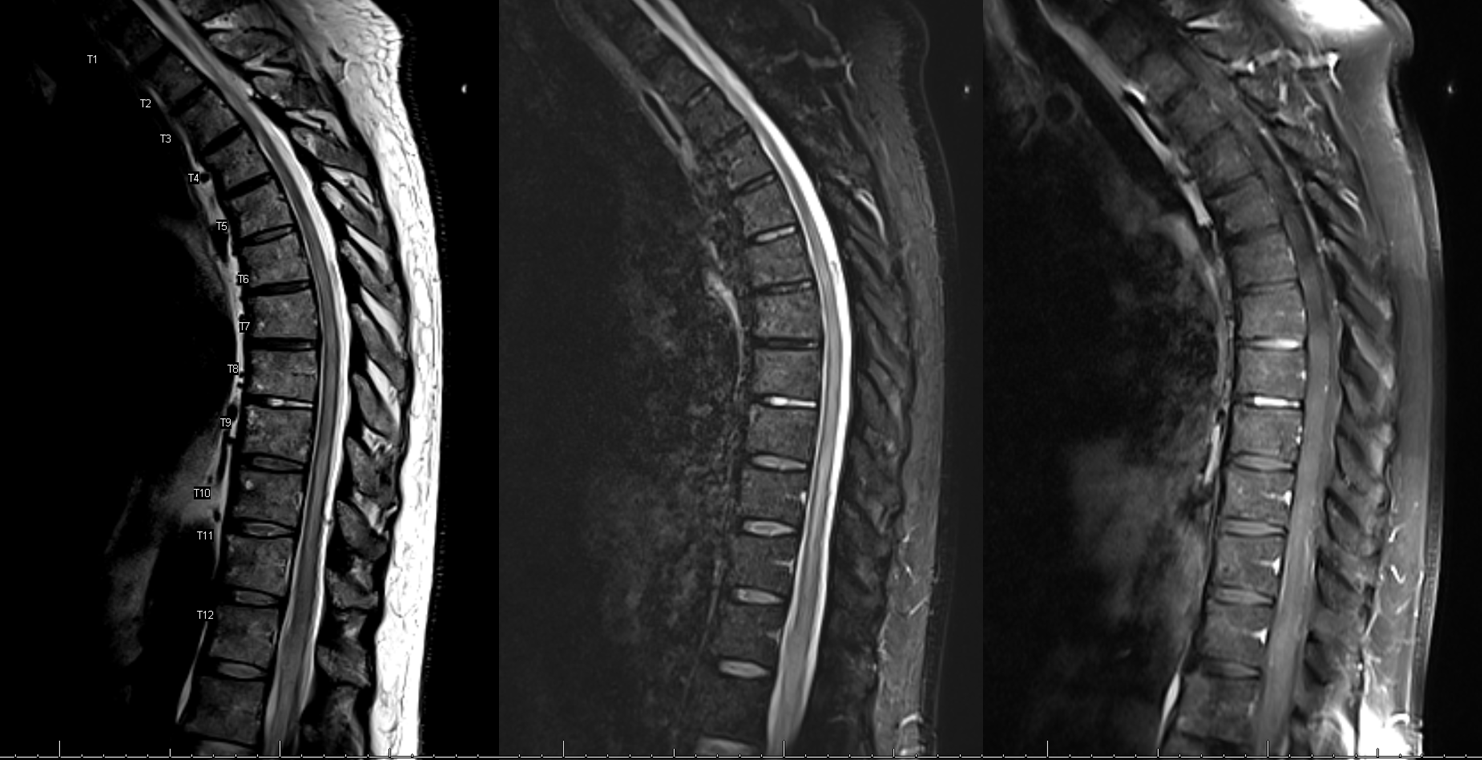
Our department selectively employs a T2 SPACE volumetric sequence. Here are two images, where there is suspicion of increased vascularity dorsal to the cord. Pretty big difference, right? The standard sequences are hampered by volume averaging and have thus missed the fistula

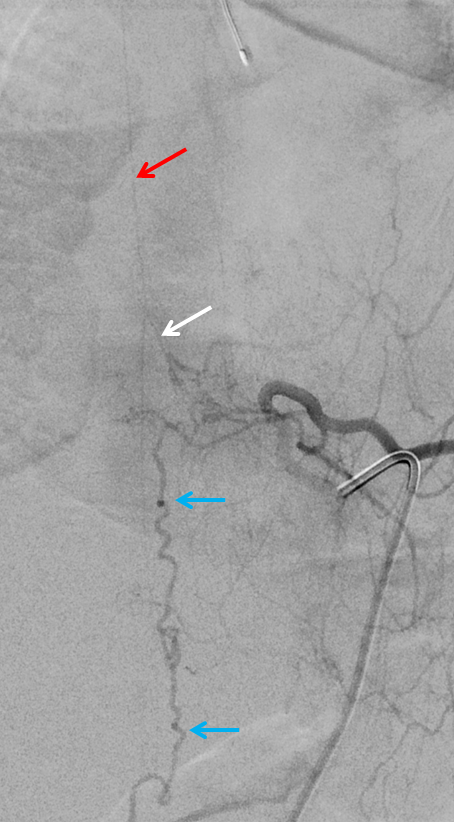
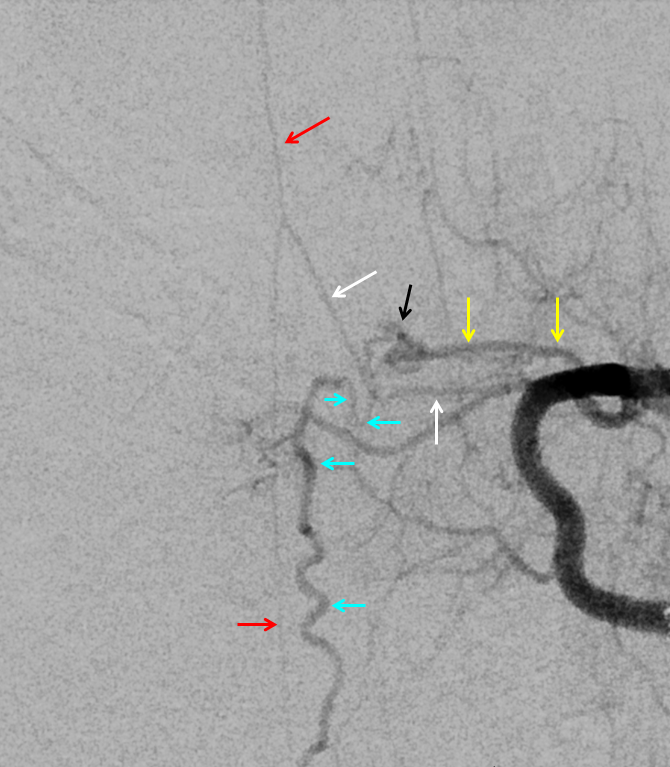
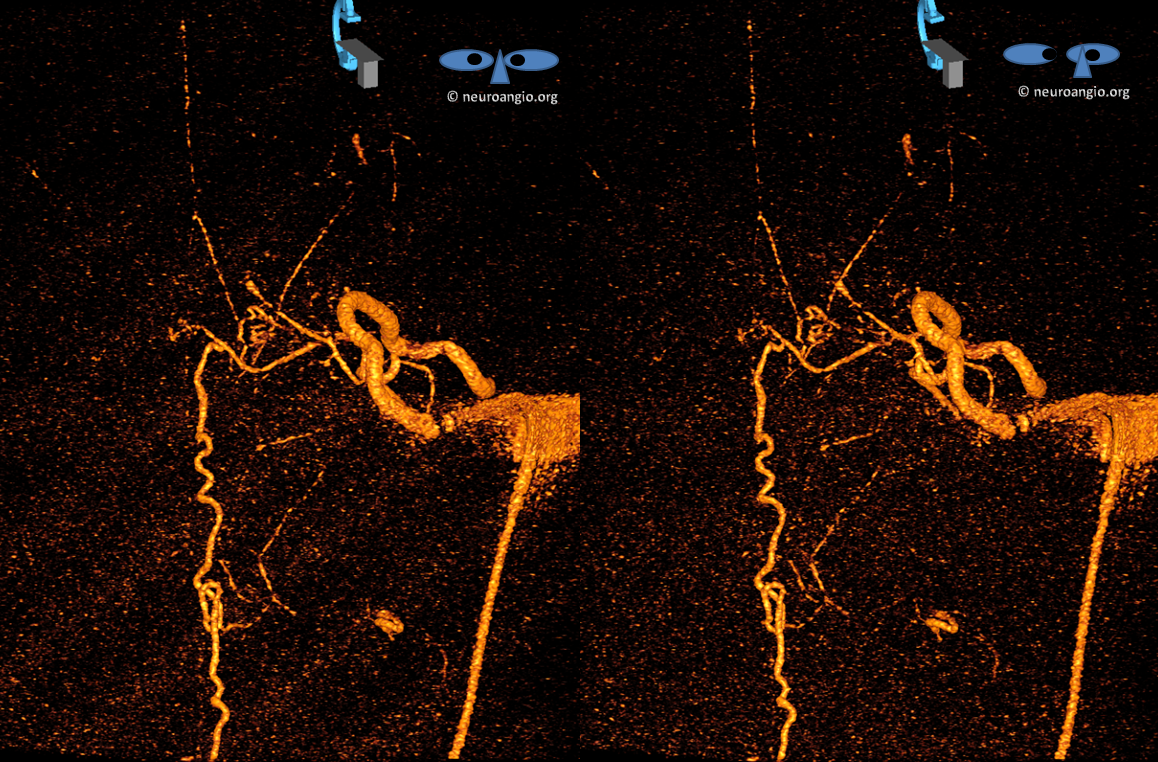
Angiography identifies dural fistula (blue) at left T8 segmental artery level. The radiculomedullary artery (white) supplying the anterior spinal artery (red) happens to arise from the same level
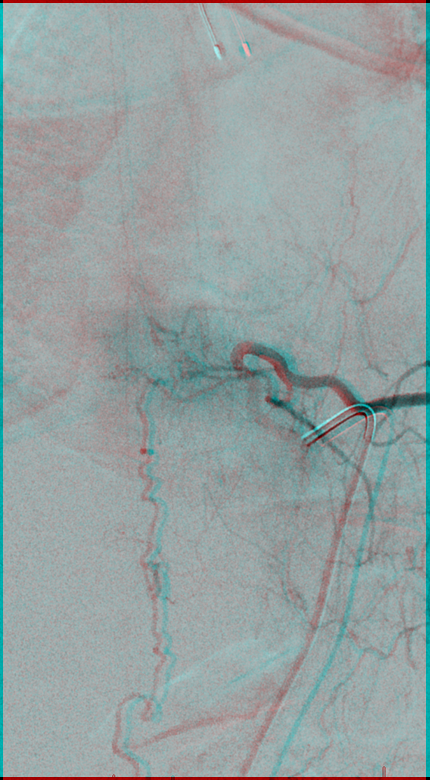
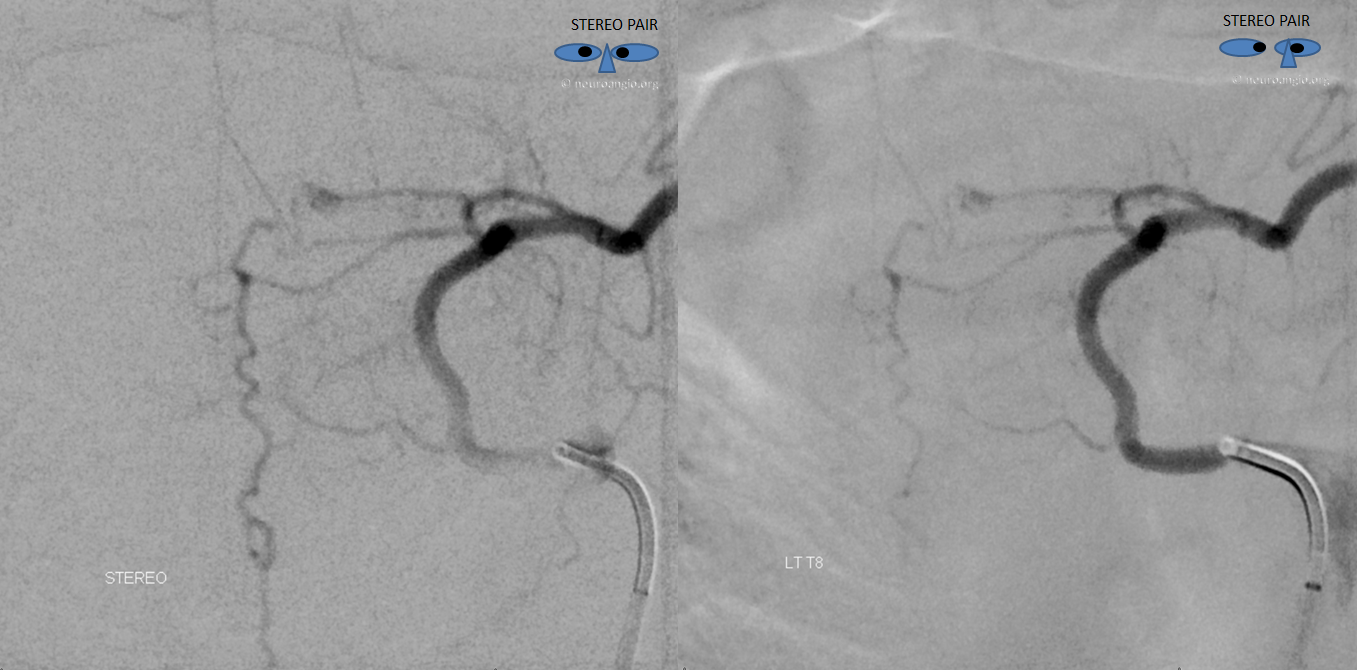
Stereo pair

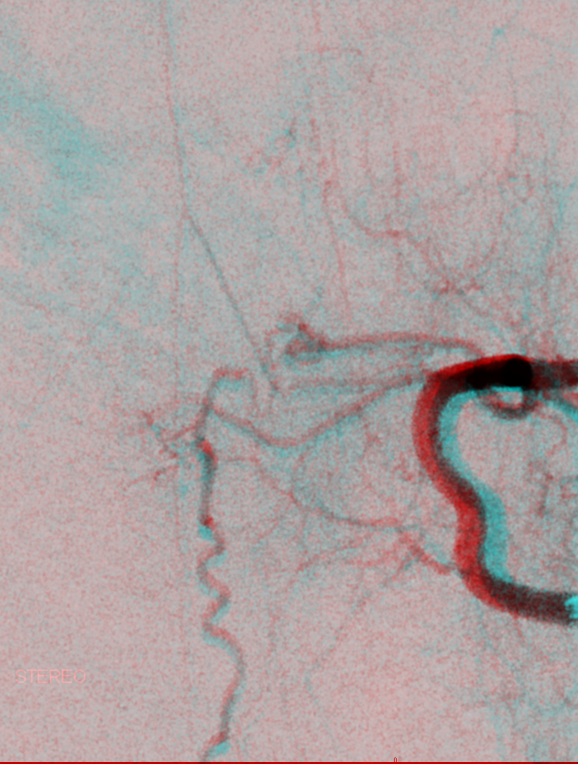
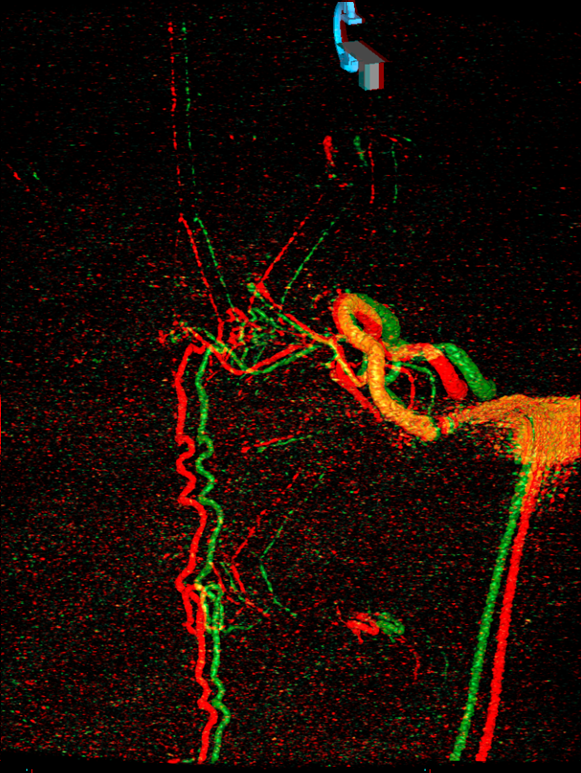
Anaglyph stereo
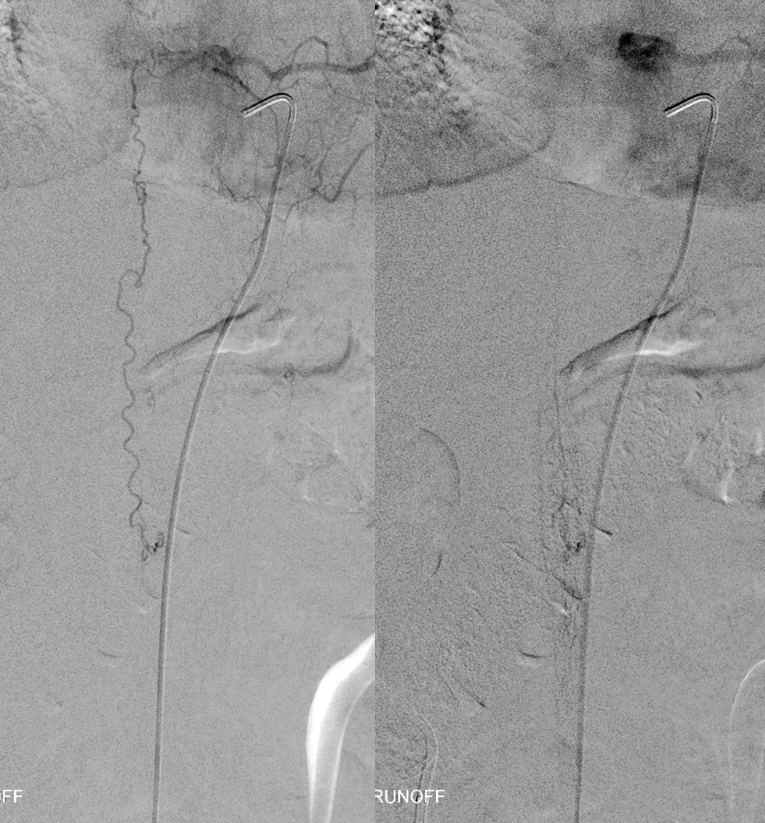
Delayed images of fistula runoff show the same vein that was seen on the MRI. Despite a relatively small burden of venous opacification, this vein has absolutely no radicular outflow. Delayed image (right) shows marked venous congestion. This explains how such an inconspicuous fistula is capable of creating so much cord congestion and deficit.
In essentially all cases, fistulas arising from same level as the ASA go to surgery as embolization of fistula carries substantial risk of anterior spinal artery injury, and therefore these cases are referred to surgery (see one such case here). However, a closer look in this case shows something important. The radiculomedullary artery (white) supplying the ASA (red) originates as a separate branch from the radicular artery (yellow) which supplies the fistula (fistula point black arrow, fistula venous drainage blue arrows)
Why two separate vessels? Because there are typically two radicular arteries — dorsal and ventral, each supplying its respective nerve root — there is after all a dorsal and a ventral root at each level, and each one has to have blood supply. Sometimes, there is one common branch entering the neural foramen which divides inside foramen into dorsal and ventral branches. Sometimes, these come off separately. Note — a better name for radicular branch is “radiculo-dural” because it also typically supplies the dura and the epidural space. See Spinal Arterial Anatomy page for all kinds of details. Here, the ventral nerve root branch also supplies the ASA (therefore it is called radiculomedullary). Bottom line is that in this case the fistula is supplied by a different branch — close to but not the same — than the ASA. Here is a cool stereo, which shows that the radiculomedullary branch and the anterior spinal artery is indeed anterior (ventral) to the more posterior (dorsal) spinal vein draining the fistula
Anaglyph stereo, for those that don’t use the cross-eye option
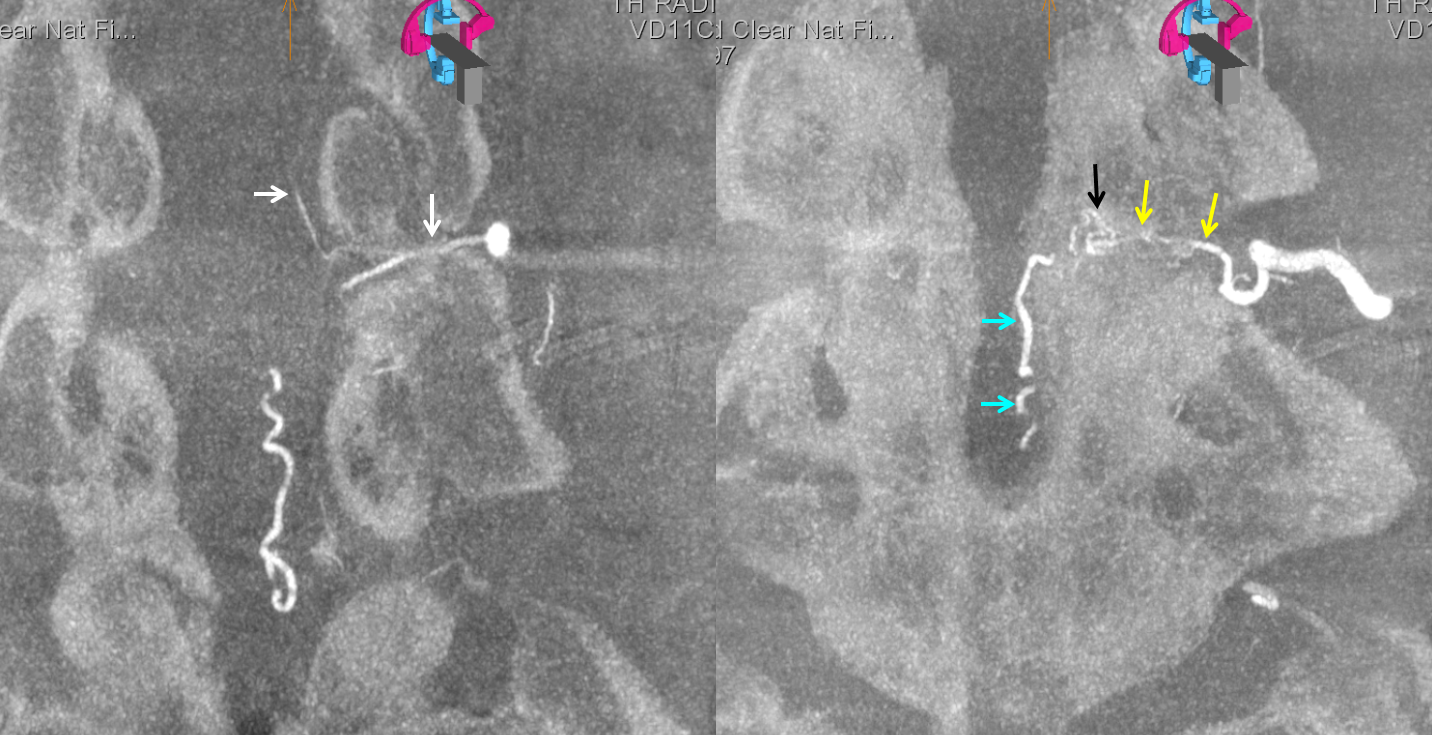
Now, we can get even fancier with advanced imaging technology. Here is a Dyna CT showing beautifully two separate radicular vessels inside the foramen. Arrow colors same as above
We can get even super-fancier with this Volume Rendered reconstruction (in stereo)
Anaglyph
Another anaglyph

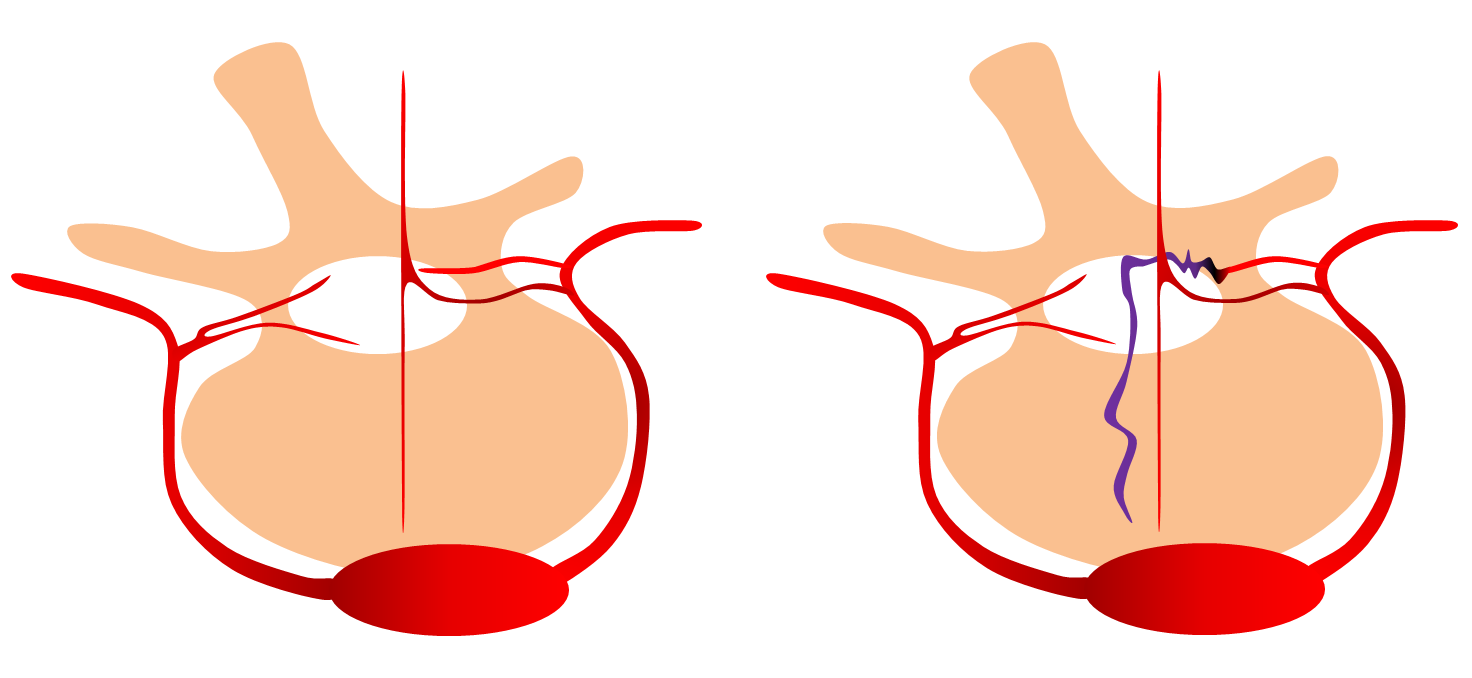
Finally, a drawing. Disposition on left shows variants of single and separate pedicle dorsal and ventral radiculo-dural artery supply (ventral on left is a radiculomedullary artery). Disposition on right shows how the dorsal pedicle supplies fistula while ventral supplies anterior spinal artery
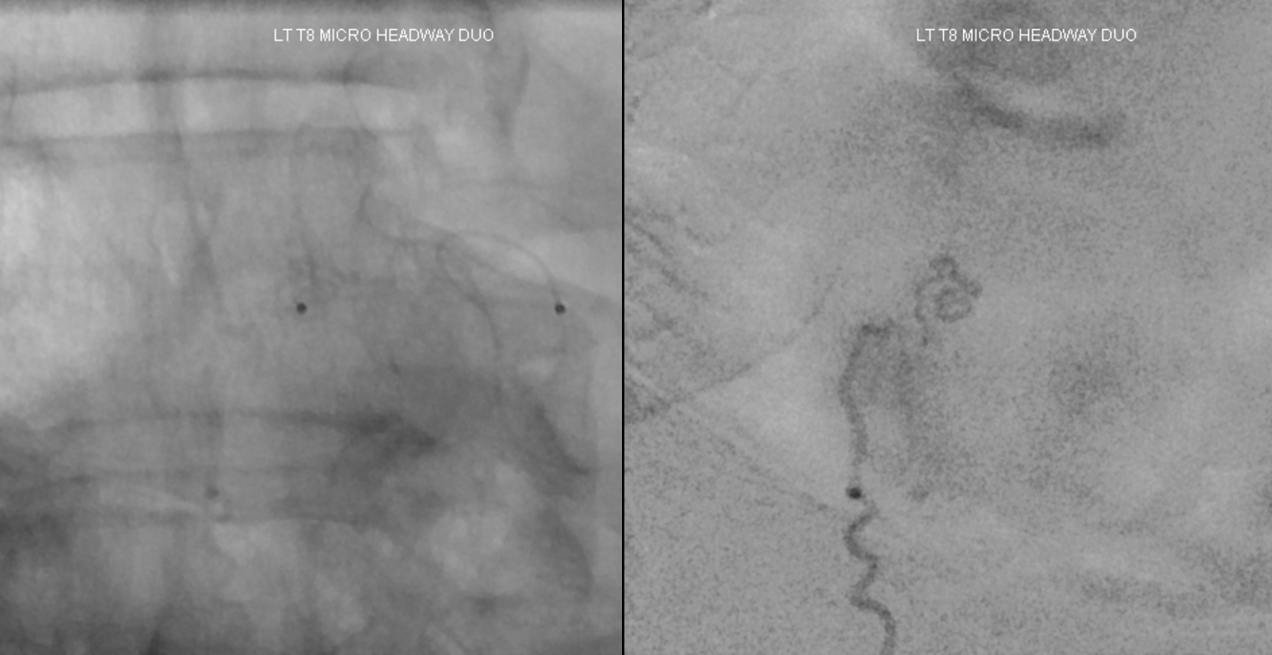
OK, that’s been a good dose of anatomy. Now we move on to treatment. Here is a microcatheter position immediately proximal to the fistula point. It is very good anatomical position however there is some reflux as seen on the DSA image, so there is no flow control

We get a slightly smaller profile microcatheter and get into a better situation. No reflux at this point. We especially did not want to have reflux because of ASA proximity. The good news is that fistula anatomy here is pretty simple
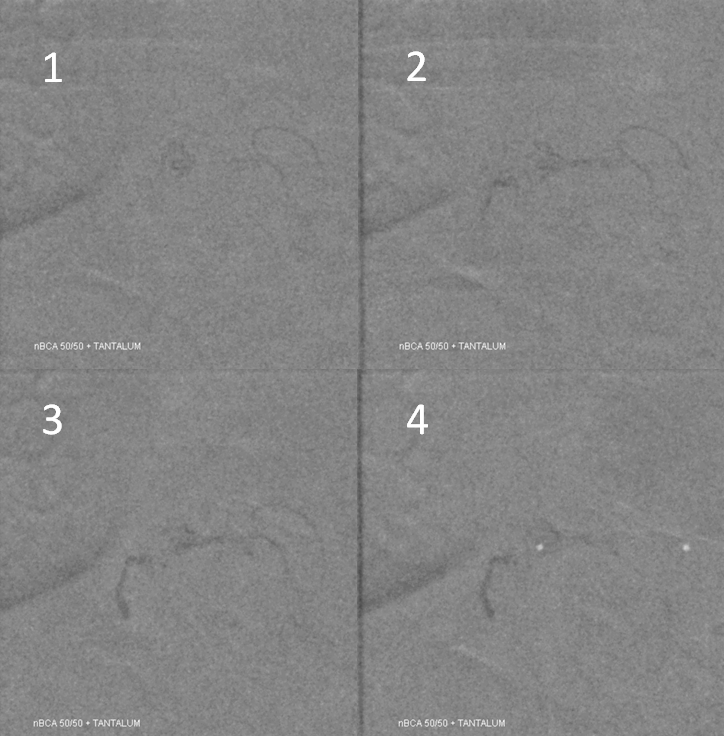
nBCA injection (50:50 with lipidol and a pinch of Tantalum) shows what happens. Still some nBCA refluxed but well within safety. The glue does not enter the main vertical segment of the spinal vein which is ideal as this vein can now be used fully by the cord again. Unfortunately there is no outflow for it anyway so probably it will not be too useful. However, this shows what an optimal glue injection for fistula should be like — and a decent amount of luck always goes into it.
Post-embo DSA shows patency of the ASA and no more fistula

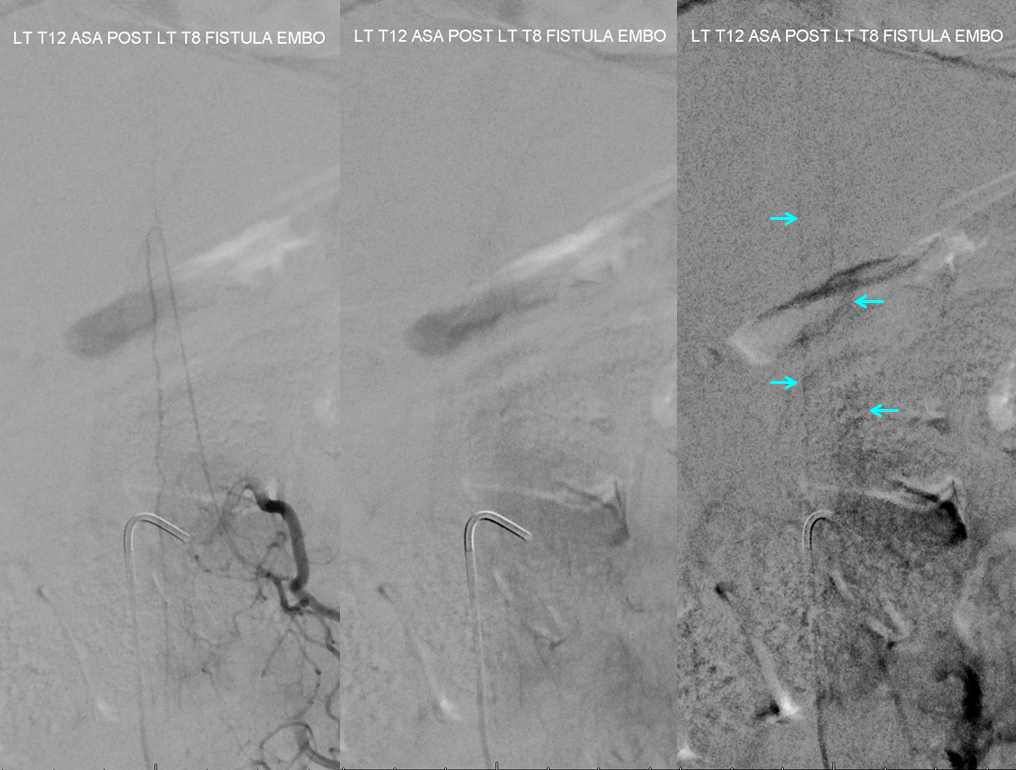
Can we tell how spinal cord congestion is doing? Of course. In order to do that, we have to look at venous drainage of cord before and after fistula embolization (just like brain dural fistulas). Here is injection of left T12 segmental artery (a different vessel from left T8 fistula and ASA) which supplies the Adamkiewicz. Look at image on the right — it is a delayed image where we should be seeing raducular veins draining the cord or at least a cord blush. We see nothing due to congestion of the cord (this is before fistula embo)

Here is the same injection after fistula embo. Now cord and radicular veins are clearly seen (blue arrows) showing immediate congestion relief
Great case to show many important points
- Great MRI sequences are better than less great MRI sequences. Seriously, though, this shows that reliance on prominent spinal veins on MRI alone to decide if there is a fistula or not can be misleading. In this case, clinical judgement played key role
- Cord congestion is better correlated to paucity of fistulous venous outflow than to prominence of spinal veins. Many spinal veins with preserved radicular outflow is better than one with none at all.
- Anatomy explains why in this case embolization with preservation of the ASA supply was possible
See Spinal Dural Fistula page for more cases
Also: