
History is progressive cord compression symptoms

Supply from right T7 only. Some vascularity. Notice venous drainage — along spinal cord surface vein superiorly, draining via right T3 and left T2 radicular veins — similar to what a spinal dural fistula might do
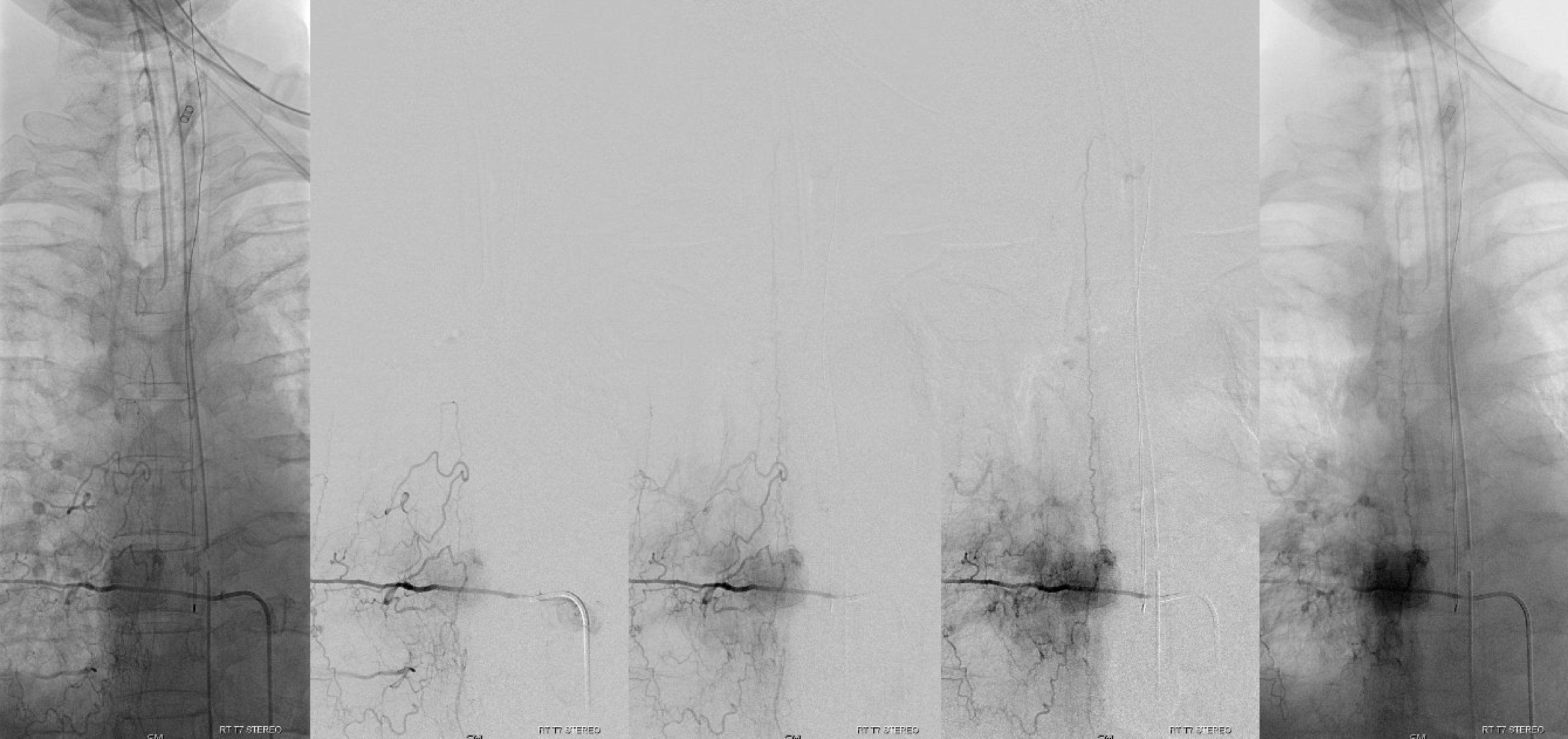
Adamkiewicz from right T9 — thats the main reason to angio — make sure there is no major spinal supply from right T7 pedicle
DYNA — see that venous drainage?
A very interesting connection to ventral cord venous system via transmedullary veins (veins running through the substance of cord — image 3 and level 3 — see Spinal Arterial Anatomy page for details

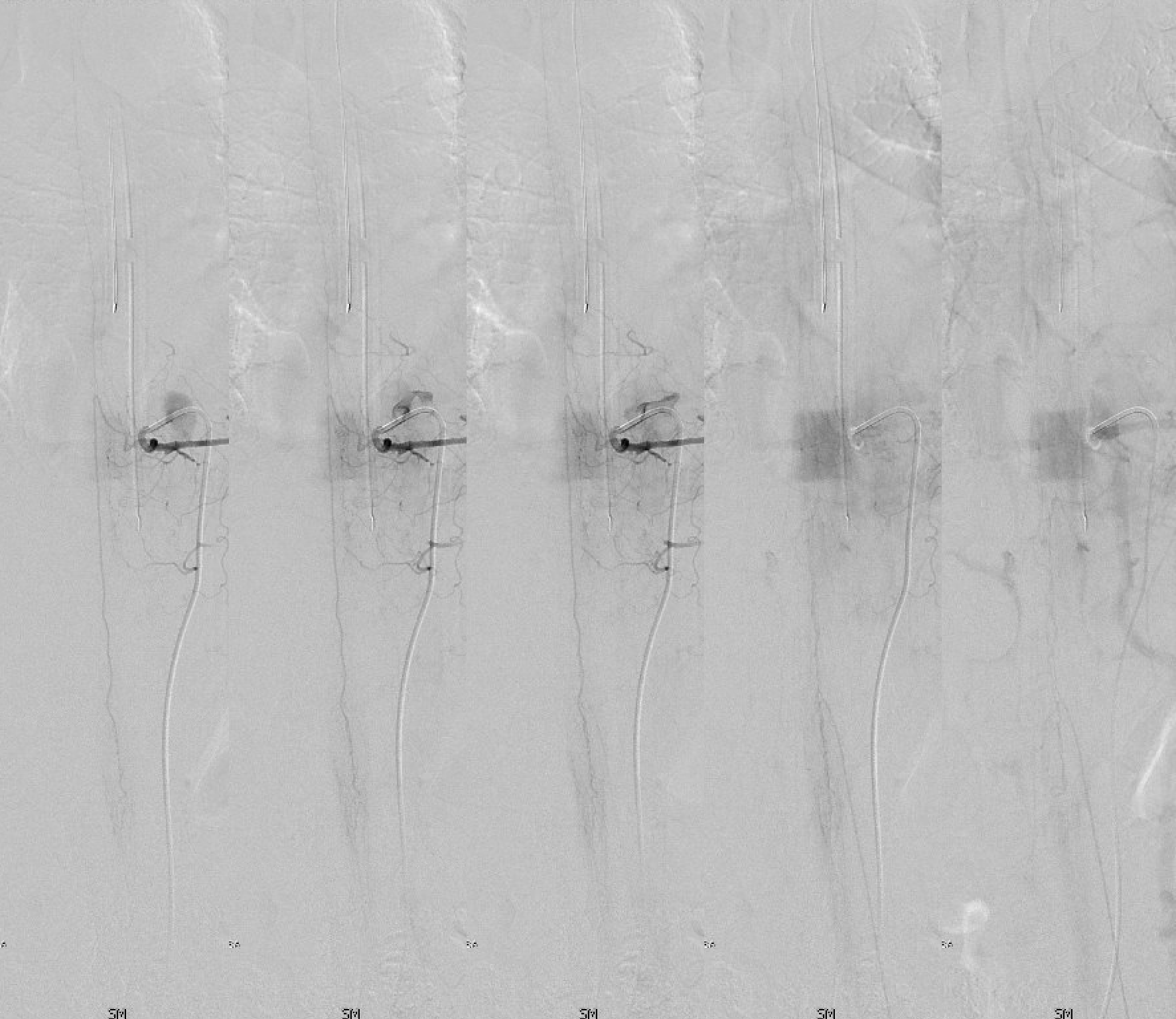
ASA — lower aspect. Notice single major draining vein — variants in drainage are important. The nerve roots are well seen also
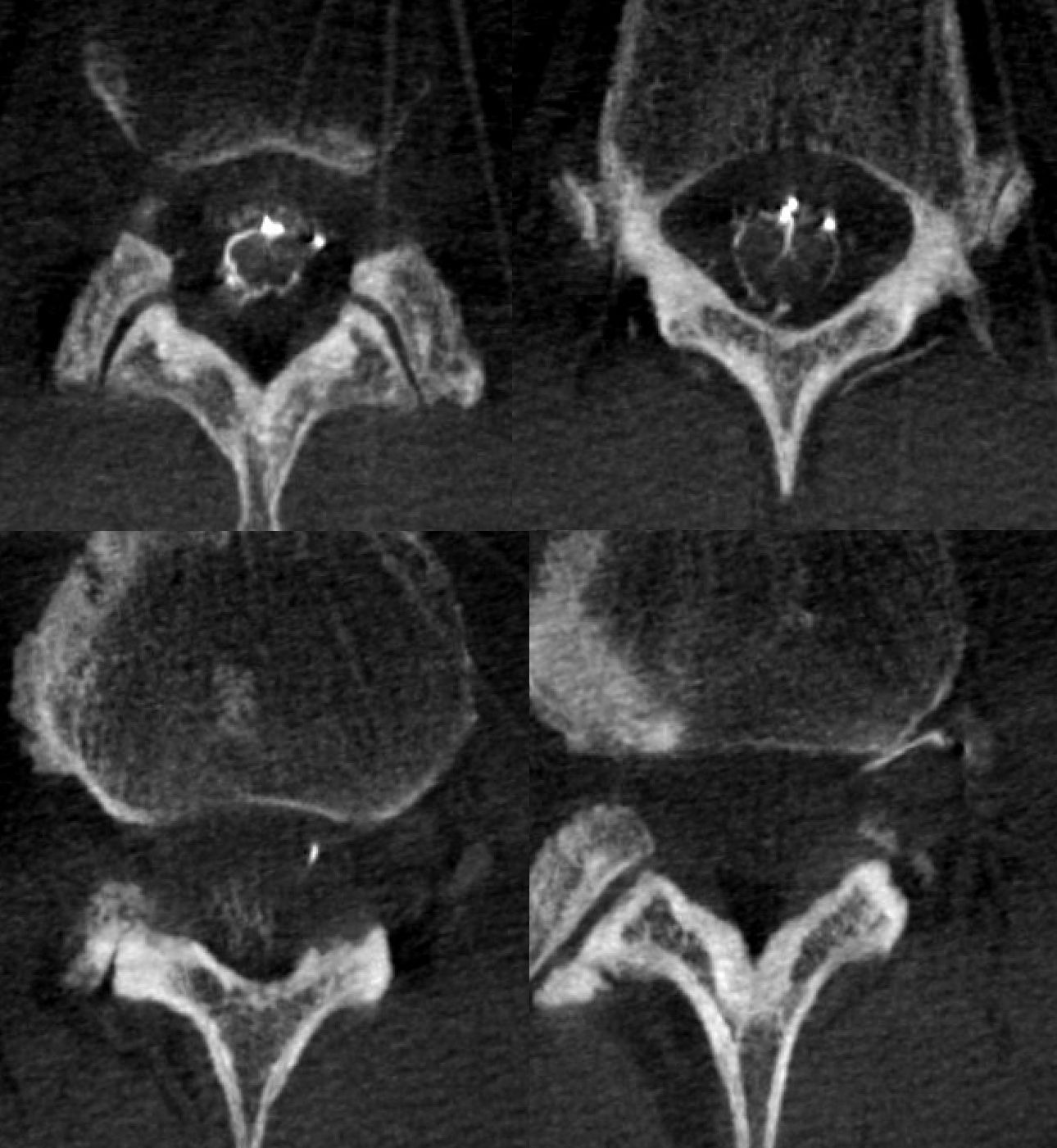
Sagittals – note preponderance of sulco-commissural vessels at the conus

Axials lower cord
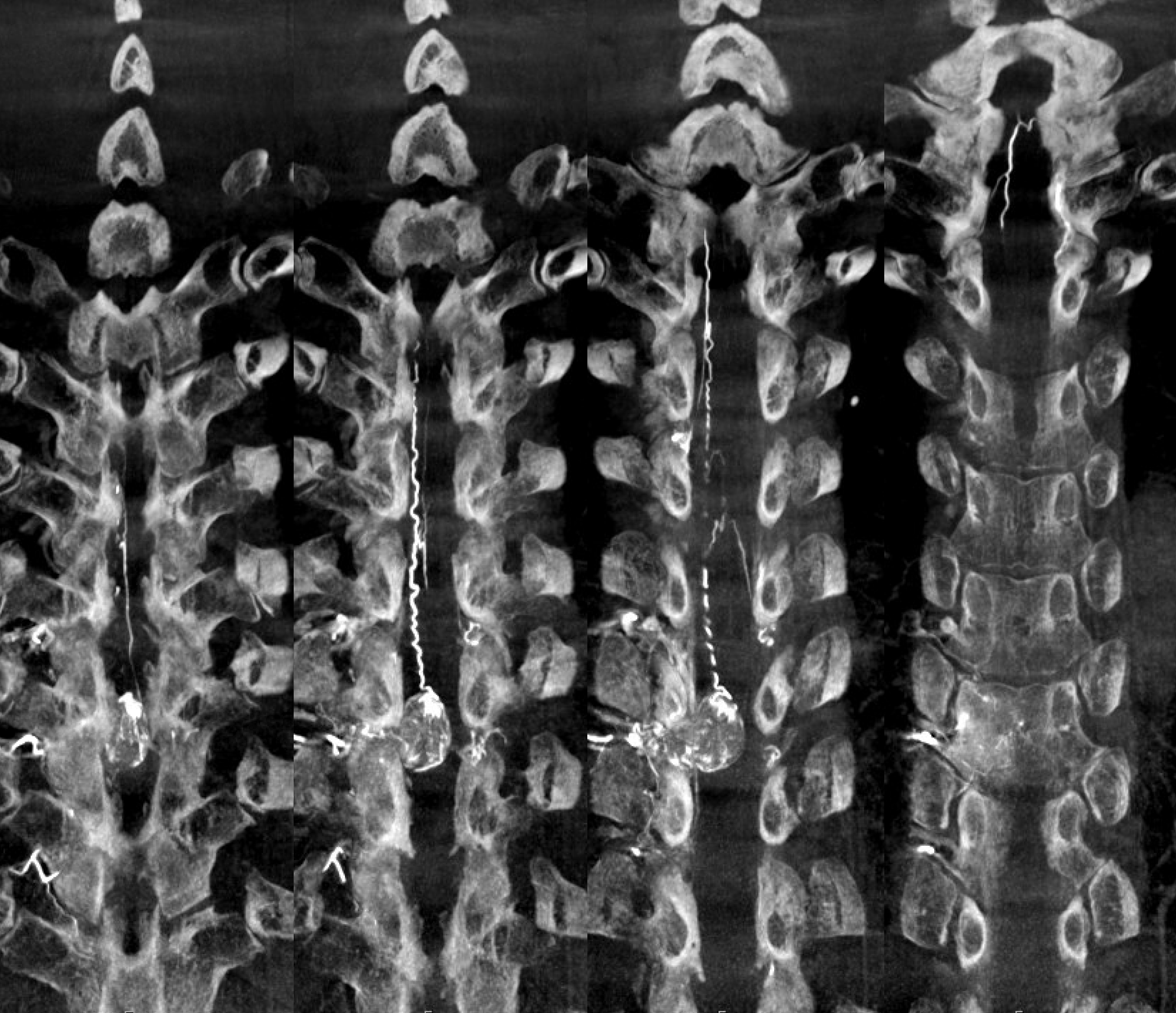
Rotational MIP
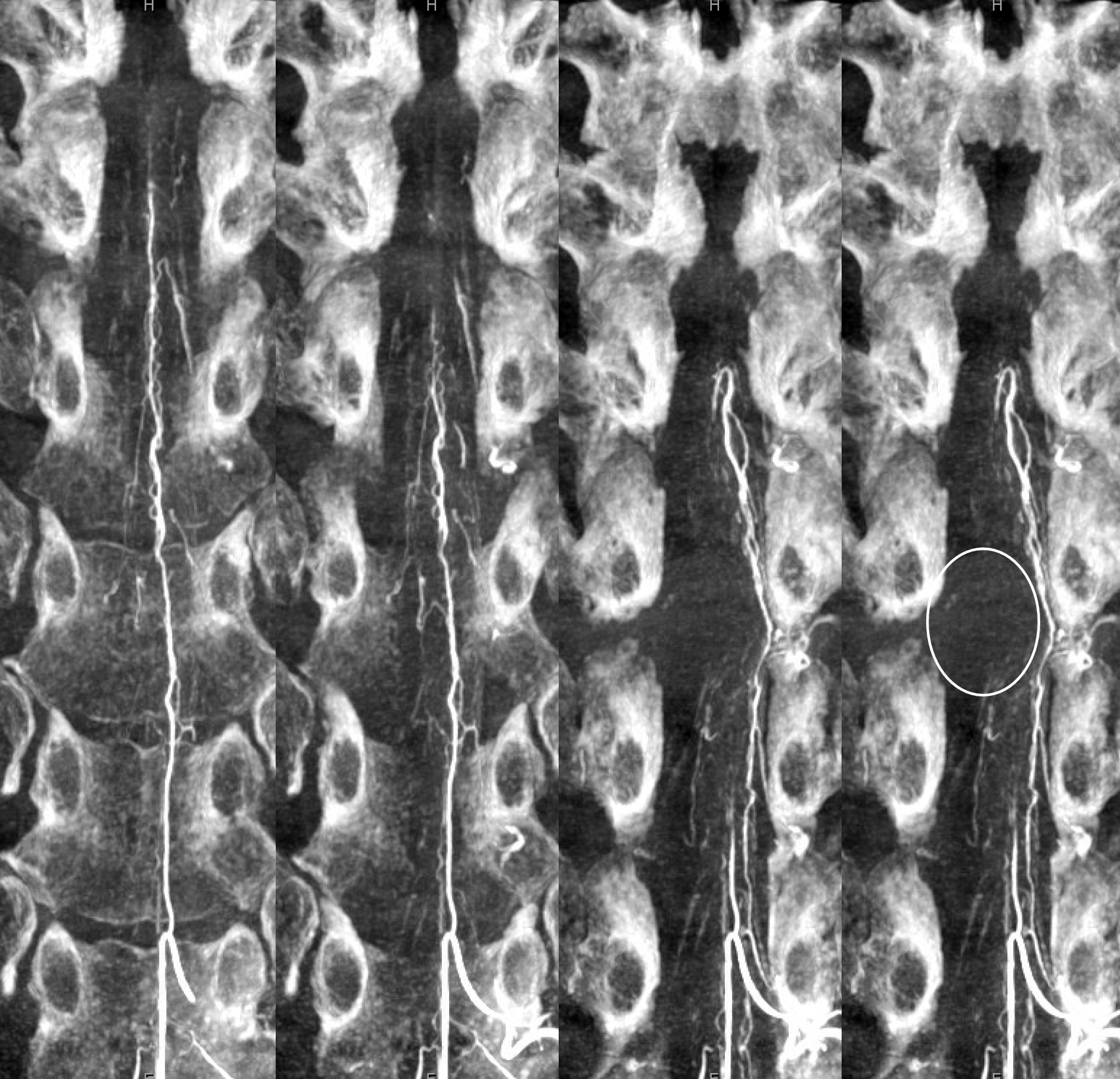
Upper coronal MIPs of the ASA — see mass effect from the tumor
The presumed diagnosis was meningioma. The final diagnosis however is Schwannoma.
What lessons can be gained from this? See the angiographic venous drainage pattern — it is very similar to what a spinal dural fistula may look like. Why? I think the reason has to do with the “seat of disease” — the anatomical location of the disease. The dural fistula is located in the nerve root sleeve, and is a pathologic connection between radicular artery and radicular vein. A Schwannoma is also centered on the nerve root — therefore its arterial supply and venous drainage will likely be those of the root involved. Which is precisely what we see here — radicular artery and radicular vein. A meningioma might be more likely to drain into meningeal vessels. We don’t really understand this well enough yet, as there are not enough modern angiographic images of these. But we are getting there.