
Number 13 below. We dont skip numbers…
The classic definition is an artery to the lacrimal gland. As in anything else vascular, this is an oversimplification. Its a lacrimal network — supplying the lateral aspect of the orbit. In addition to the lacrimal gland, there are other structures there — lateral and superior rectus muscles, fat, bone of the lateral orbital wall…
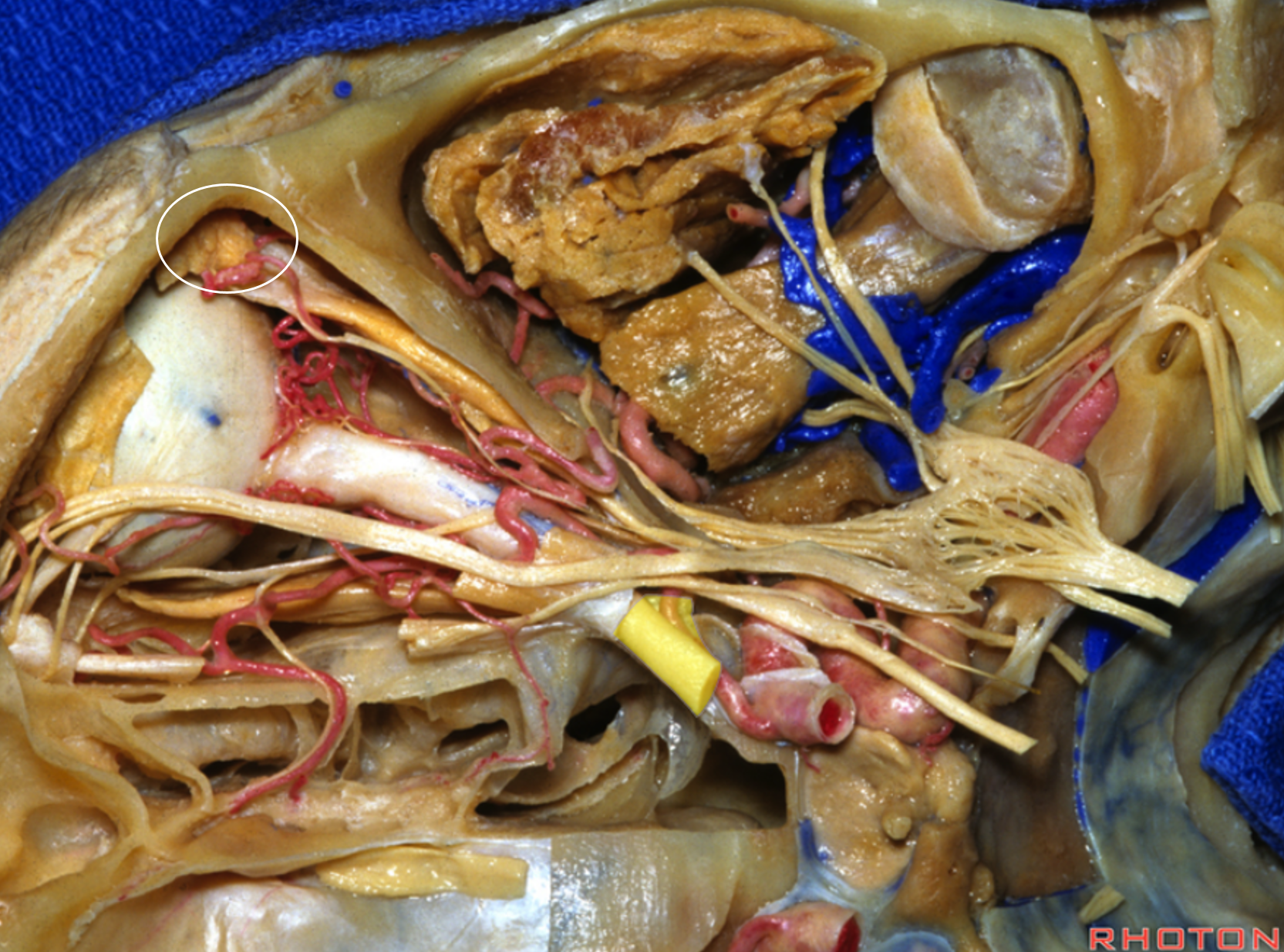
Below is an image of a beautiful Rhoton dissection (used with permission). The upper aspect of the lacrimal gland is in white oval.
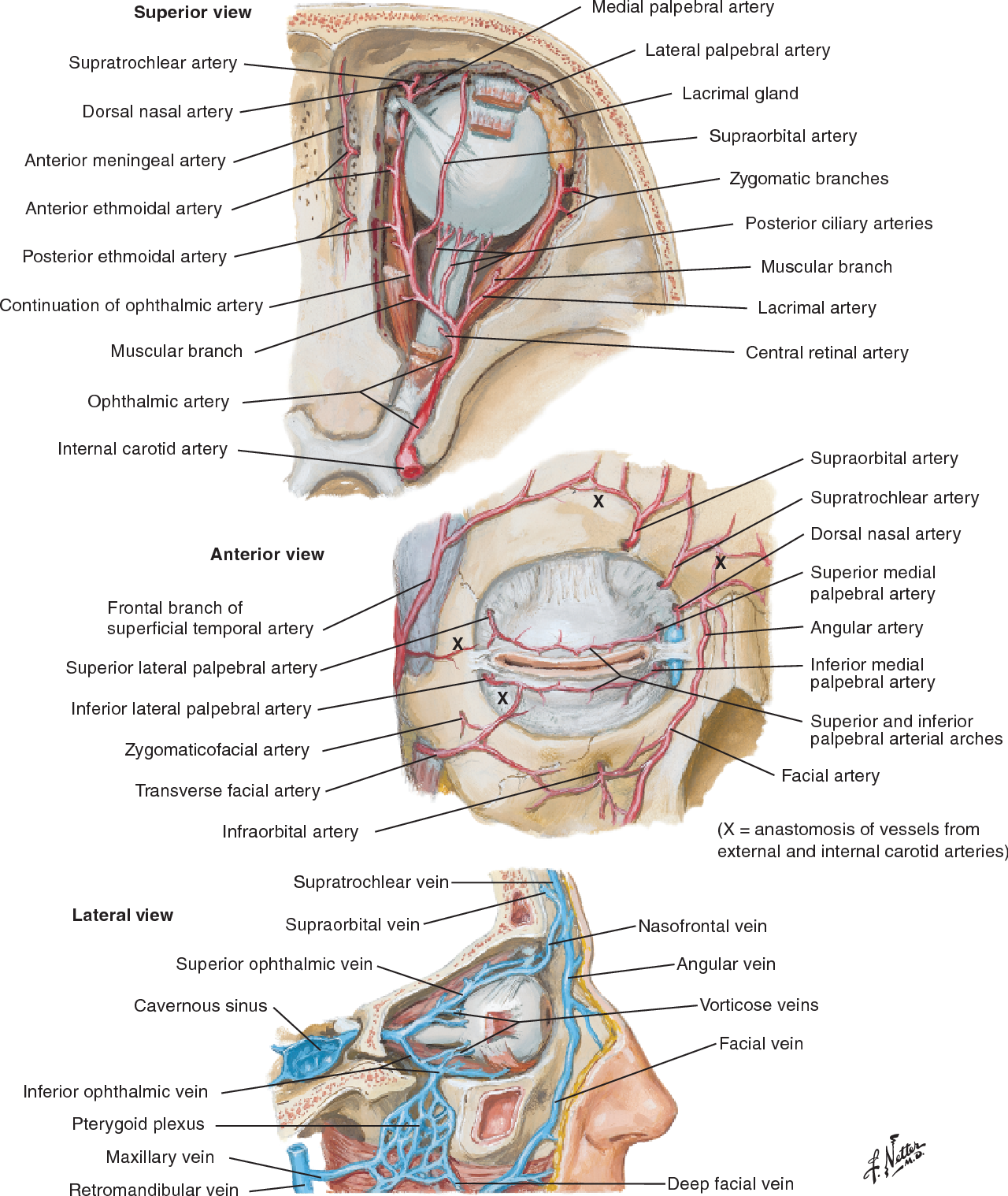
The immortal Netter images below
The lacrimal region lies at the “watershed” between the oththalmic and middle meningeal arterial territories. Classic supply is from the ophthalmic (4), however there is a balance. The “meningolacrimal” variant is when the MMA (39) “takes over” the lacrimal territory. In rarer cases, the MMA takes over even more ophthalmic territory. The reverse — ophthalmic “takeover” of the MMA territory follows the same rules — progressively more territorial takeover the correspondingly less common. This is illustrated in diagram below:
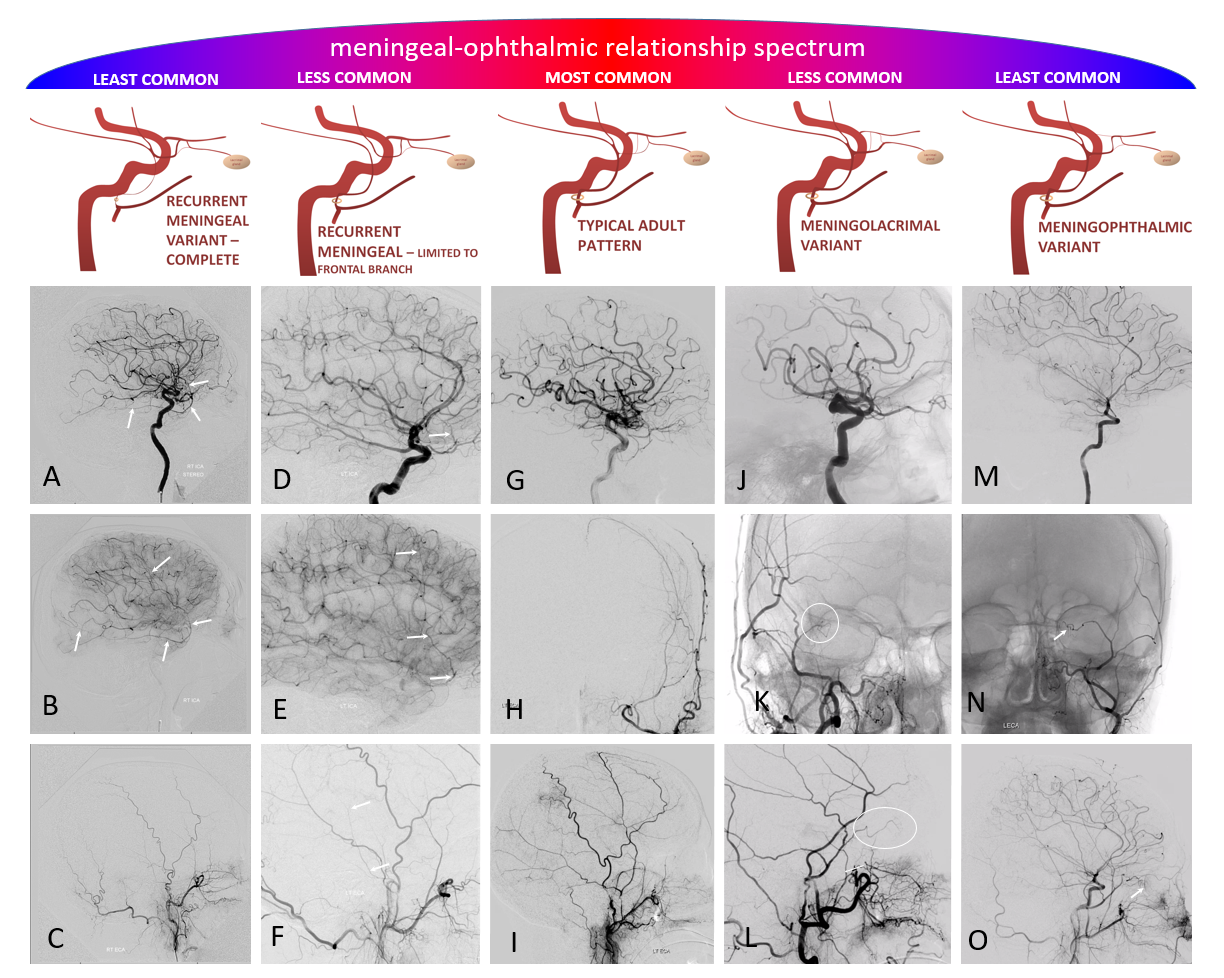
There are no discrete states. Anastomoses / connections between lacrimal, middle meningeal (via artery of the sphenoid ridge — 40), and ophthalmic systems are pretty much always there, even when not angiographically apparent. For example, if “only” meningolacrimal is seen on the injection of the MMA — and not the globe — it is still not wise to embolize the MMA.
Opthalmic Supply to Lacrimal Gland
CTA and MRA do not currently have enough resolution to visualize the lacrimal artery, except when enlarged by hypervascular diseases. Angiography is the mainstay
Seeing the lacrimal territory is easier from MMA injections of meningo-lacrimal variant, since the area is not superimposed upon by other structures (see below). For ophthalmic injections, the key is to have a frontal view. Lateral view will superimpose lacrimal branches upon ethmoidal and other arteries.
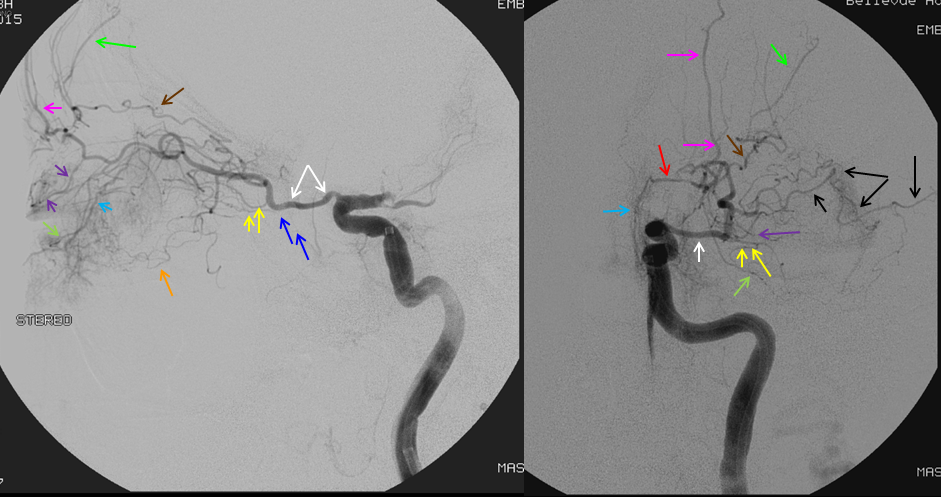
Below is an old image of this, from early thrombectomy days. The lacrimal branches are marked with black arrows in frontal view. It is very hard to differentiate them from other branches on the lateral view. The central retinal artery (one of the yellow branches — can’t tell which one — most are ciliary and only one is retinal) nearly always arises from the second portion of the vessel (the angle) — or the first bend of the vessel. Other vessels here are: blue = nasal septal via anterior ethmoids; bright green and pink = supraorbital and supratrochlear; purple = upper eyelid; light green = lower eyelid
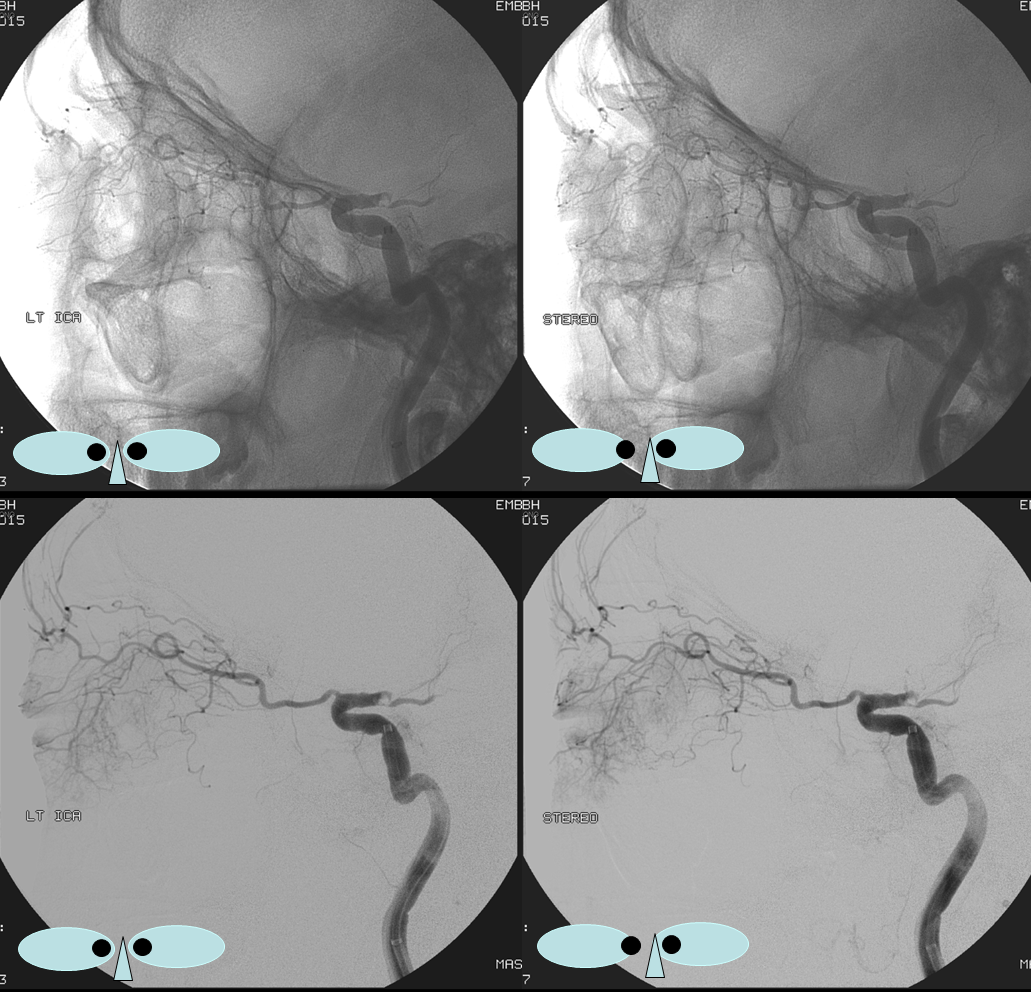
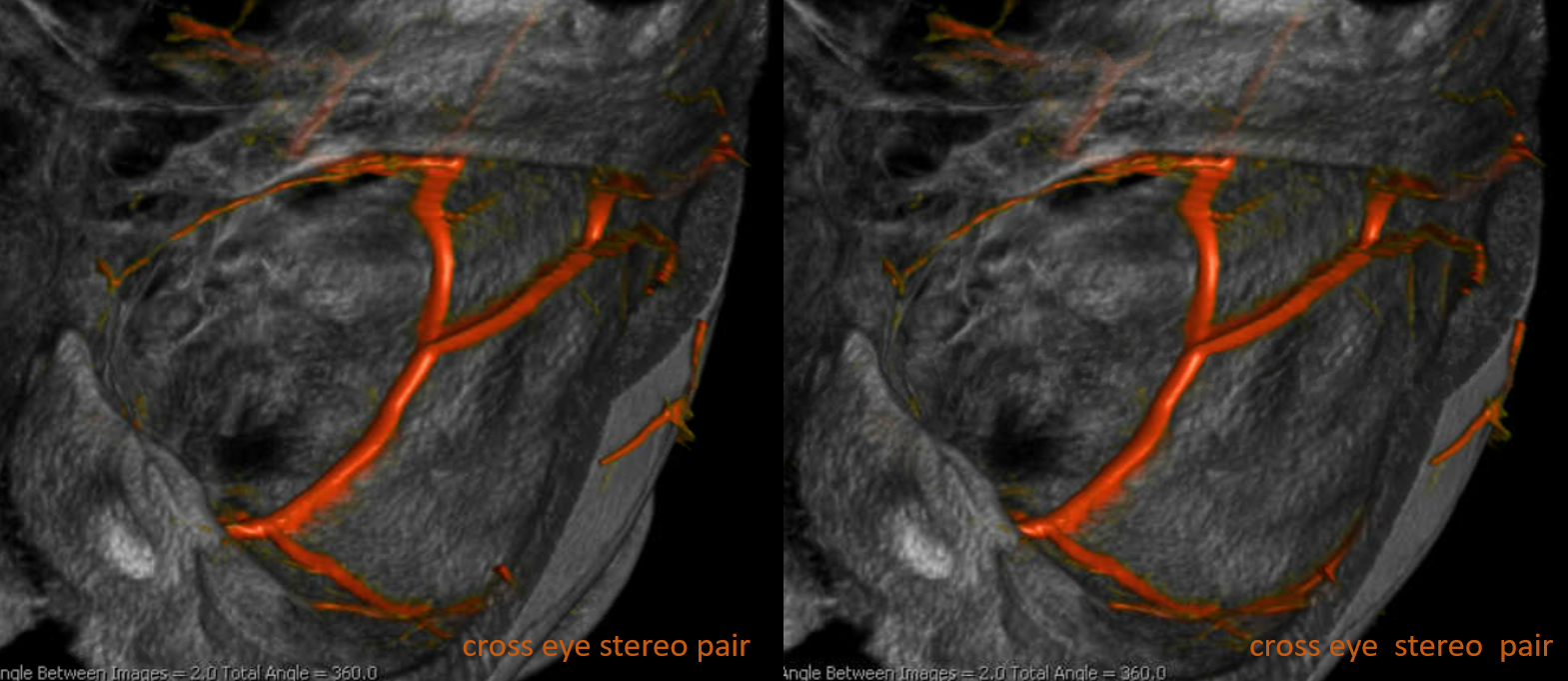
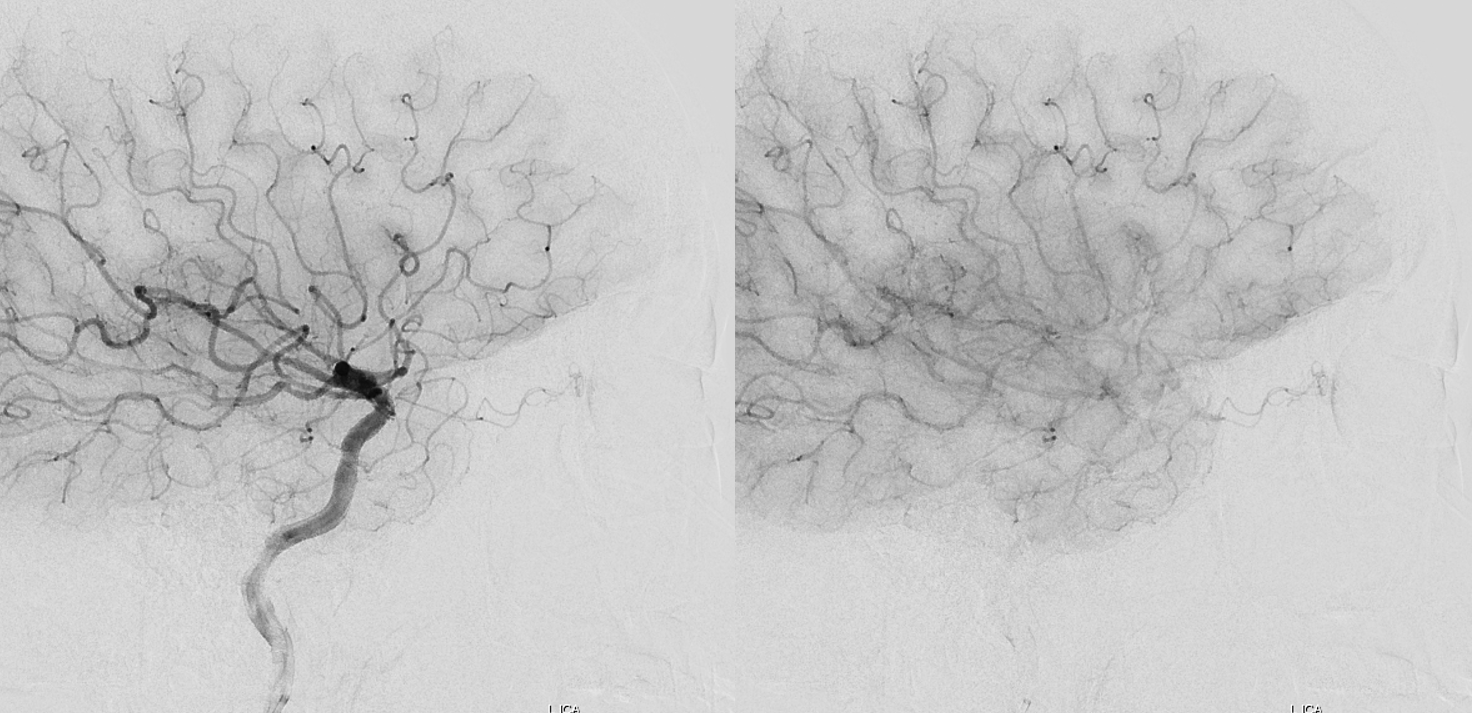
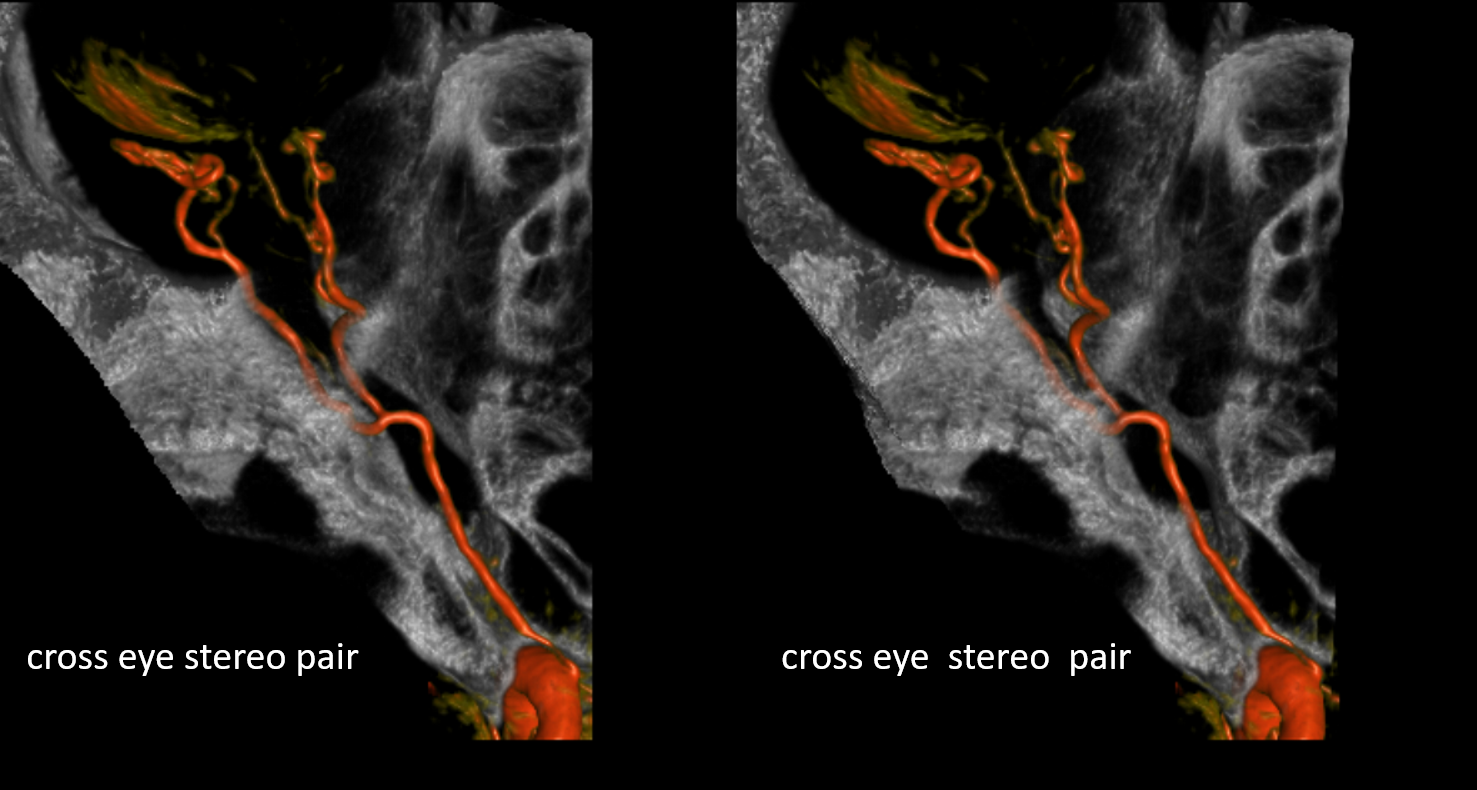
How did we ever figure out all those branches on an analog machine, without functional rotational capabilities? Stereo imaging. Check it out here. Cross-eye stereo images below
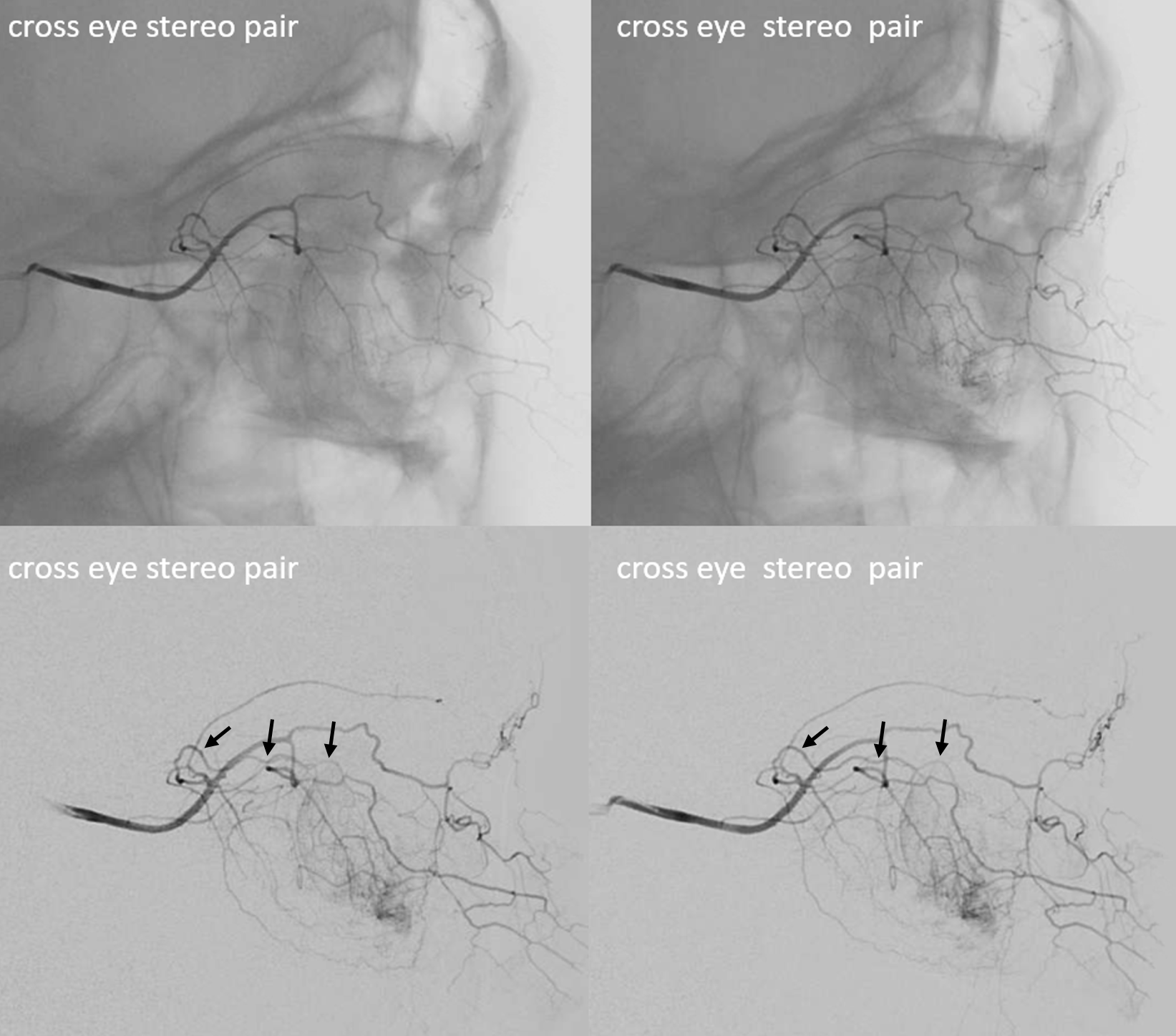
With aid of the stereo, the lacrimal branches can be seen as closest to the viewer (stereo is from lateral to medial). See black arrows below

Here be another example below — only with aid of stereo can you tell which one it is for sure. Generally speaking, the lateral orbital / lacrimal branches are a lot smaller than the medial orbital ones that supply the ethmoid arteries — these have a lot more territory as a rule and so are a lot bigger.
Palpebral Branch
That one runs across the eyelid (arrows). Usually its a bridge-like connection between the distal ophthalmic proper medially (dashed arrow) and the distal lacrimal laterally (dashed oval). Below is an example. Other arrows point to the ethmoidal arteries and septal branches — figure it out 🙂
Meningeal Supply of the Orbit
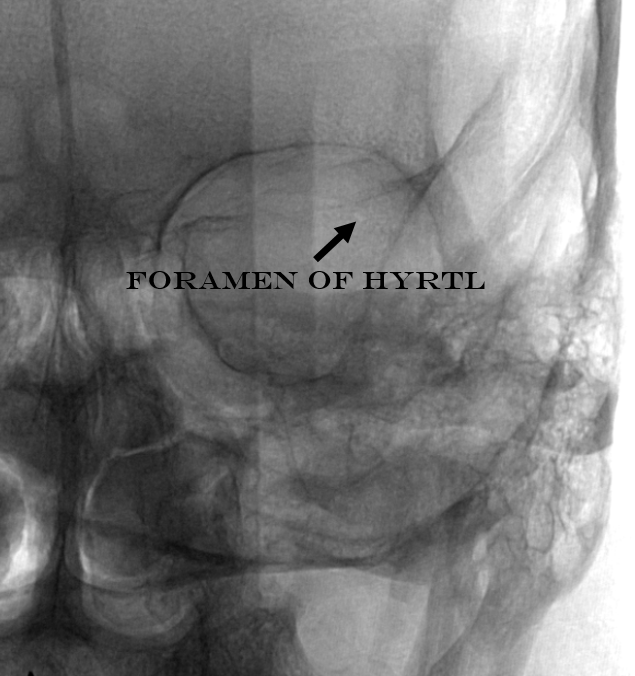
The classic meningolactrimal variant is MMA supply of lacrimal territory. The “lacrimal branch” enters the orbit via its own foramen of Hyrtl
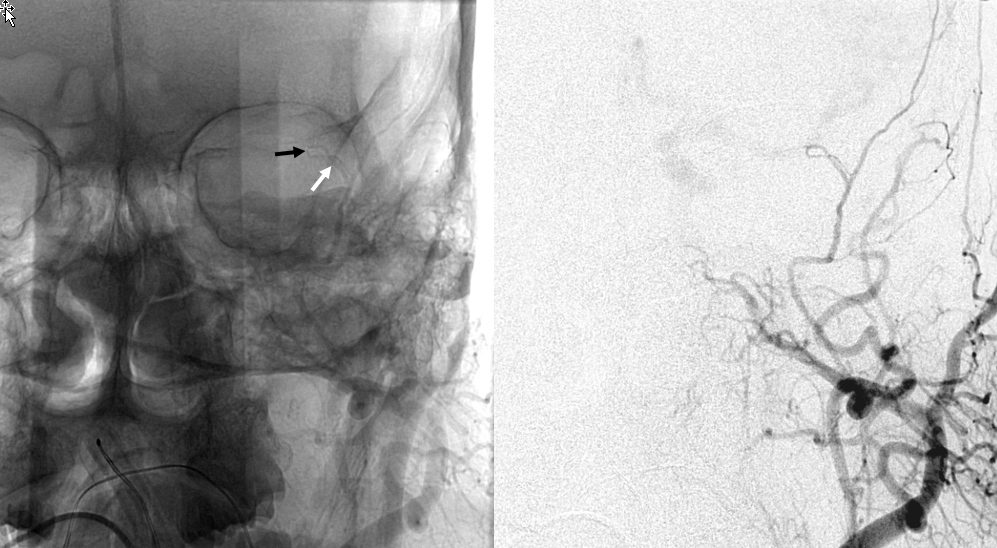
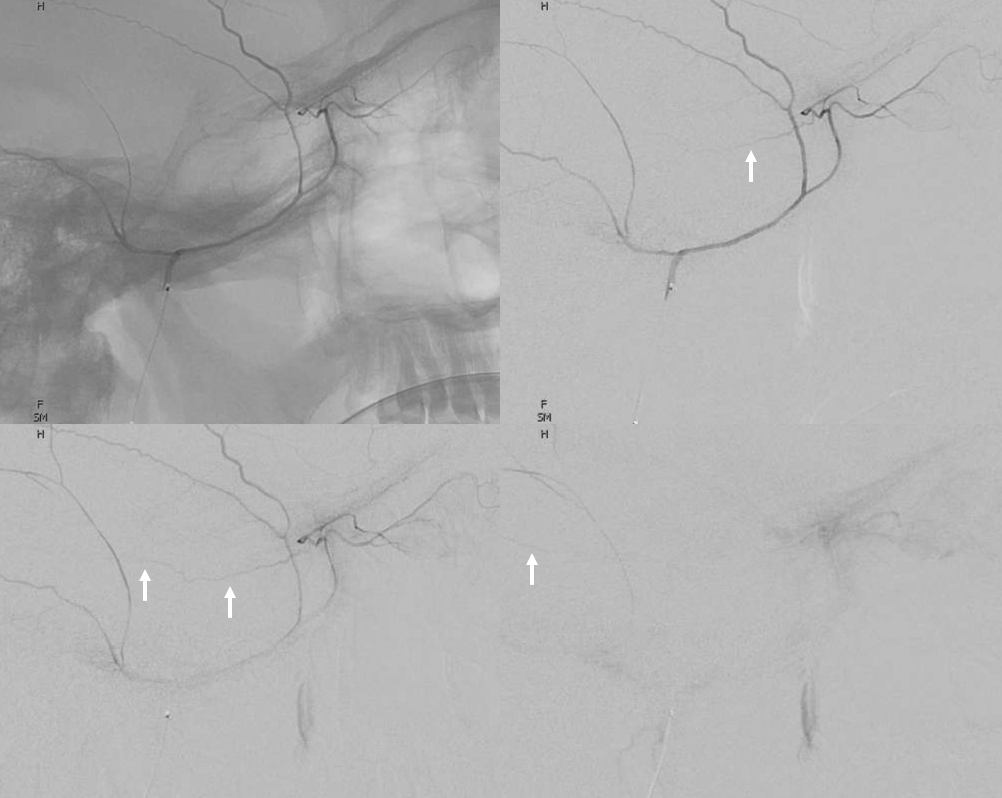
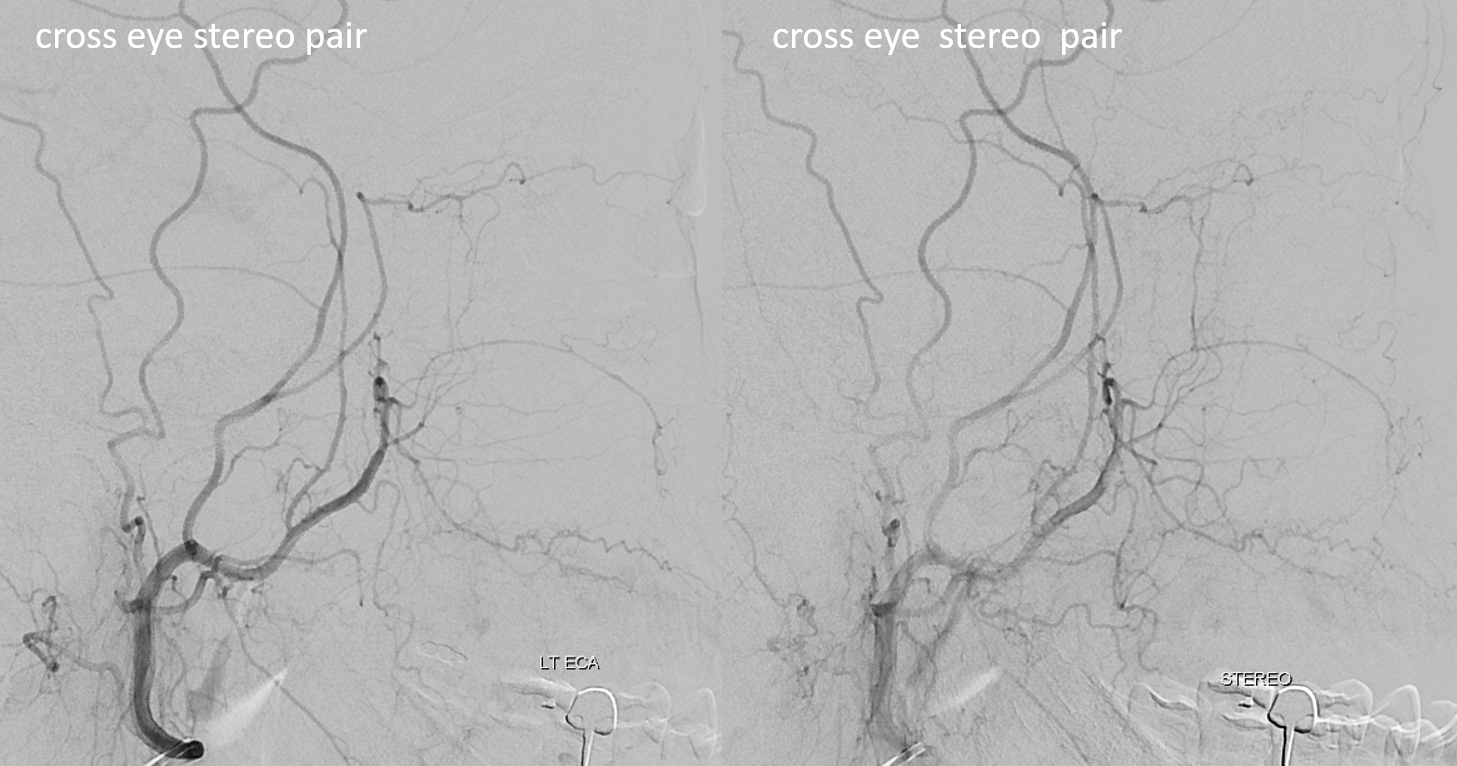
Frontal views of the ECA are key. Anything projecting over the orbit is either in the orbit, or is the occipital artery all the way in the back. If the ECA distal to occipital origin is injected, anything over the orbit is IN the orbit. Below is an ECA injection, with meningolacrimal branch (white) entering the lateral orbit via the foramen of Hyrtl (black)
Another example below — note blush of the lacrimal gland (beige) in parenchymal phase. The sphenoid branch — a key MMA branch that runs along the sphenoid ridge, like a railroad, connecting the various ophthalmic variants, is shown by white arrow. Lacrimal branch is brown. Faint visualization of the more distal sphenoid branch, where it will connect, to your peril, with the more proximal ophthalmic artery, is shown in red.
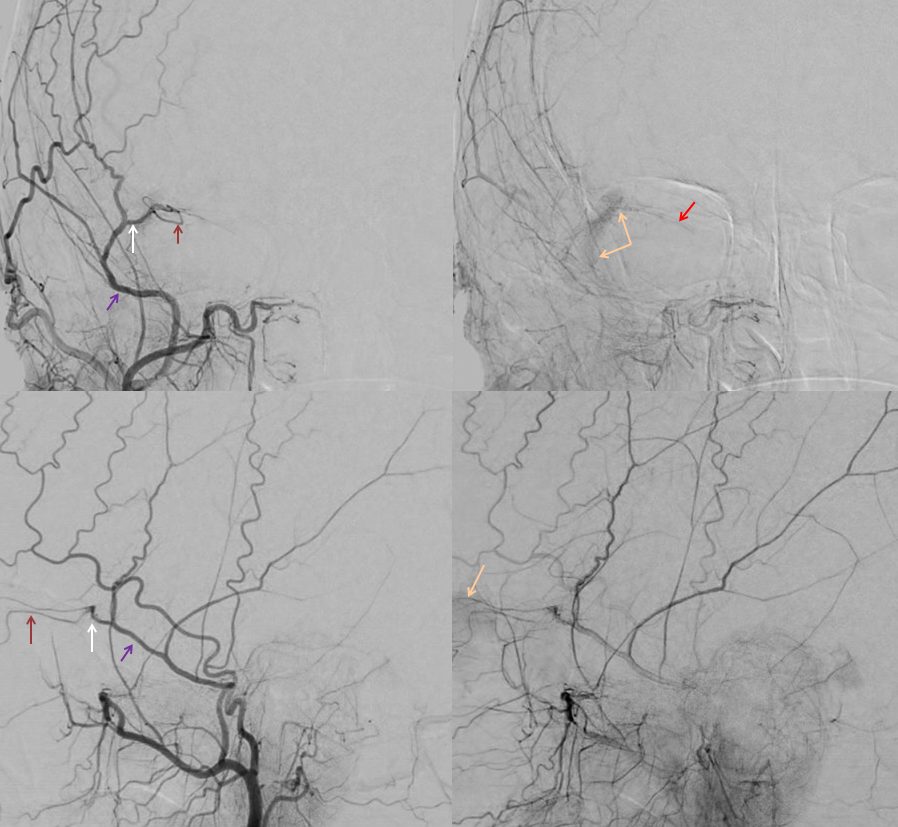
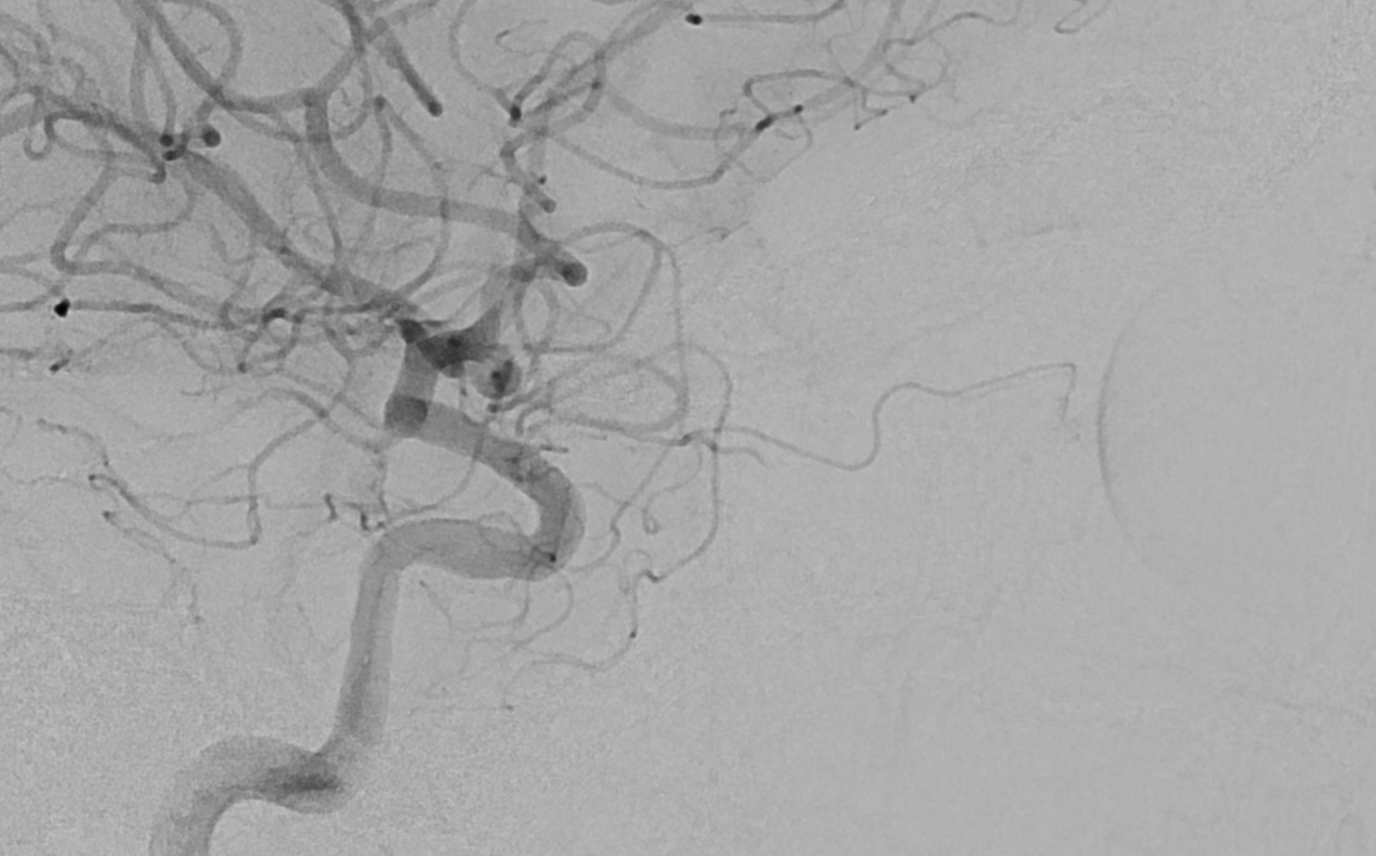
ICA injection of same patient shows globe (ciliary) supply via classic ophthalmic. The artery is slightly smaller than in its full expression, owing to its less than complete orbital supply
Greater MMA supply of orbit
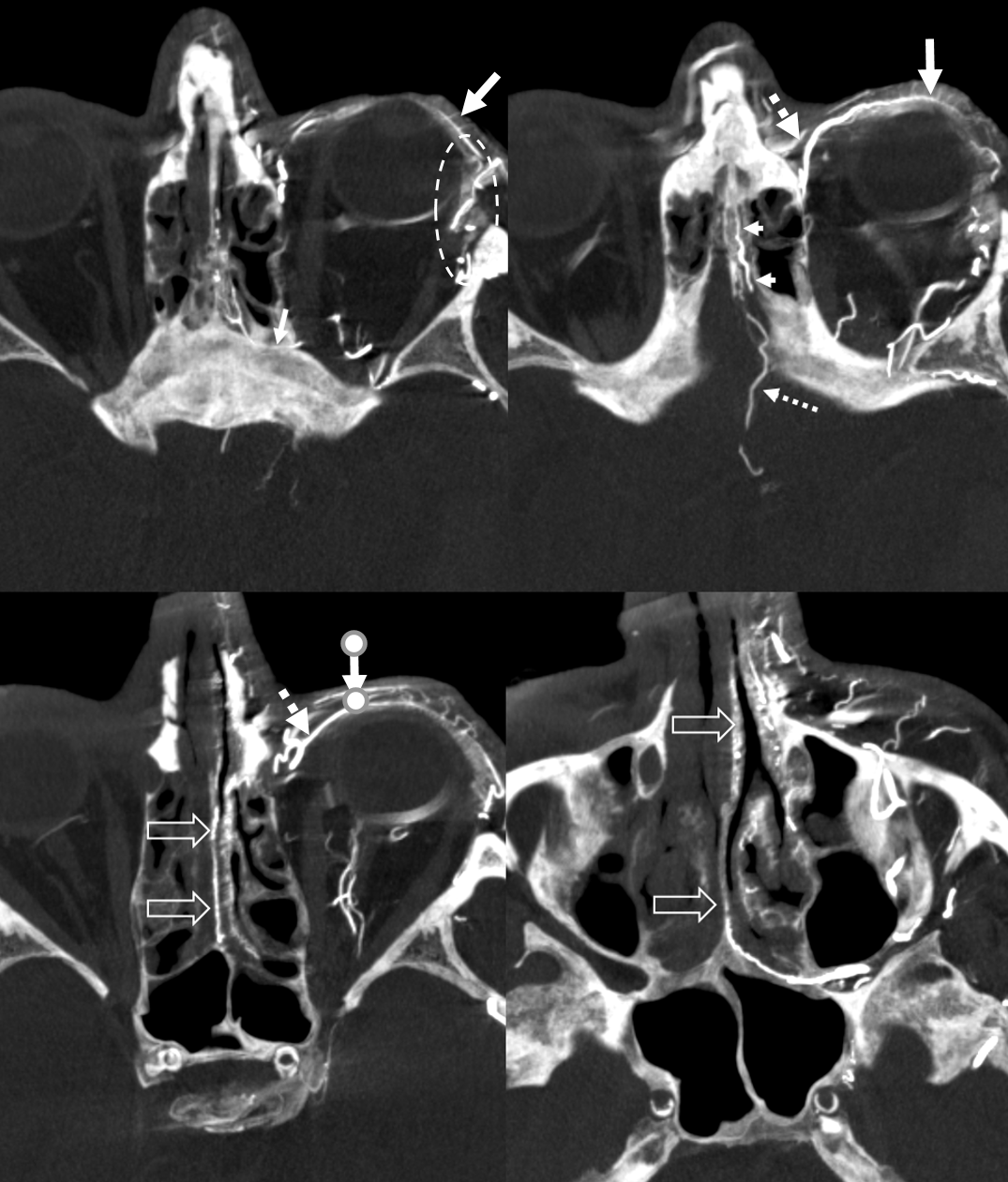
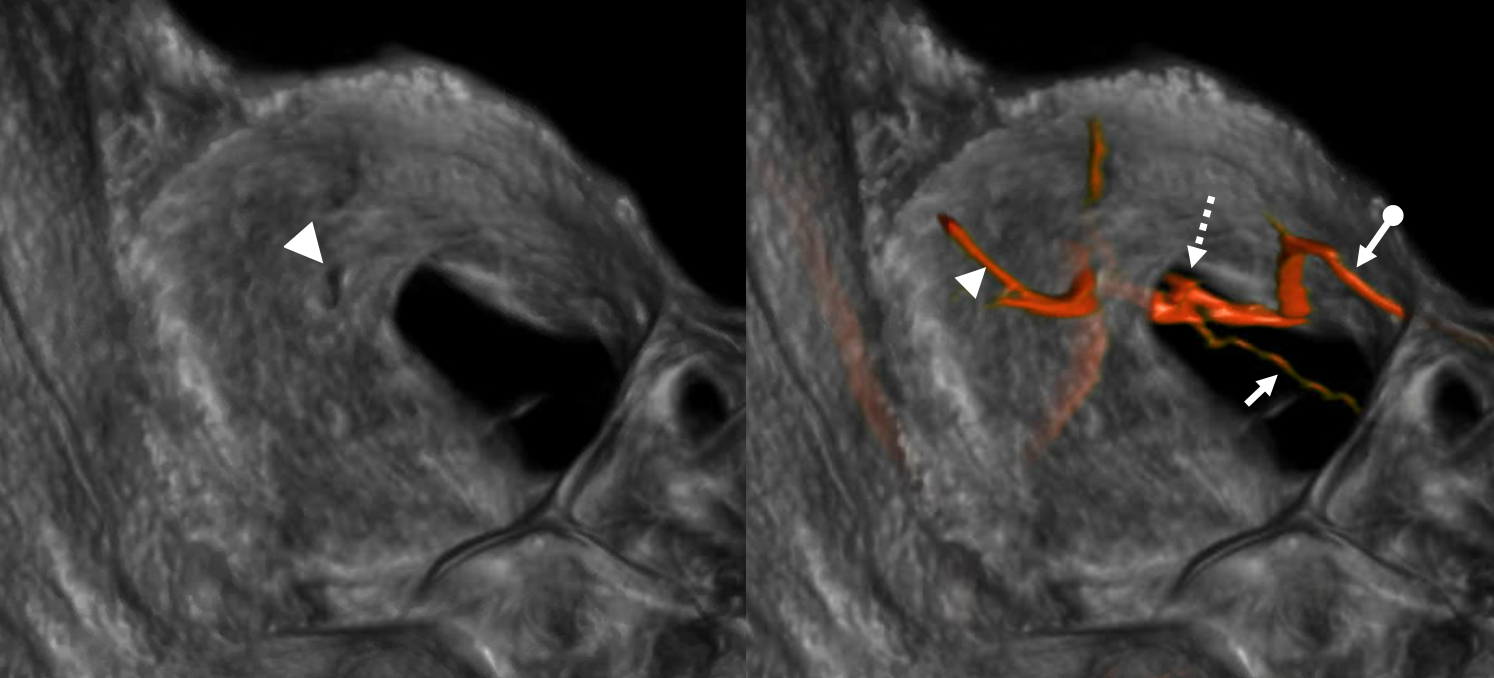
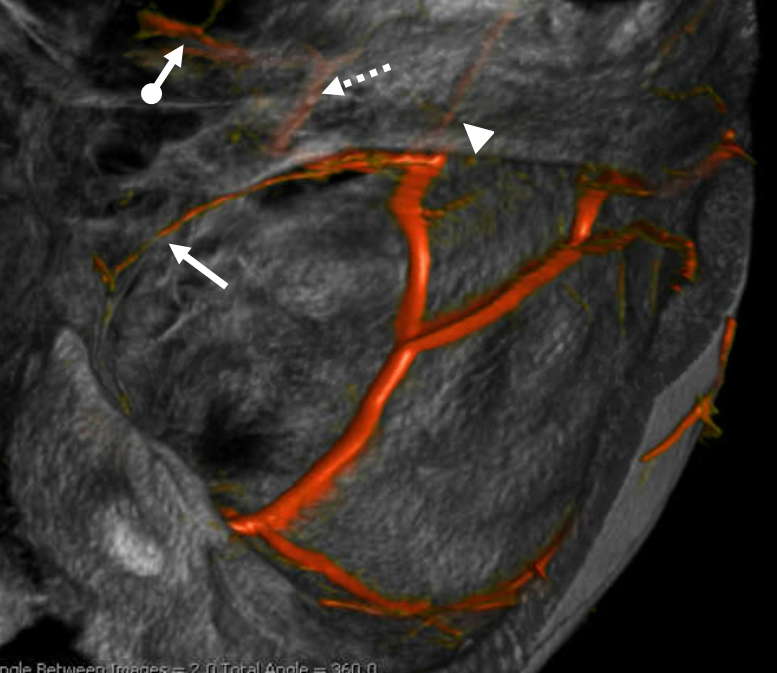
Again, the spectrum. The continuum is shown below, meningeal contribution to the orbit inclues both the classic “meningolacrimal” artery via foramen of Hyrtl (arrowheads) and superior orbital fissure supply (dashed arrows) that manly goes to the posterior ethmoidal foramen (ball arrow). Also present is a rare but important deep recurrent meningeal branch (arrow) supplying area of ILT and going as far back along the tentorial arcade as tentorial incisura…
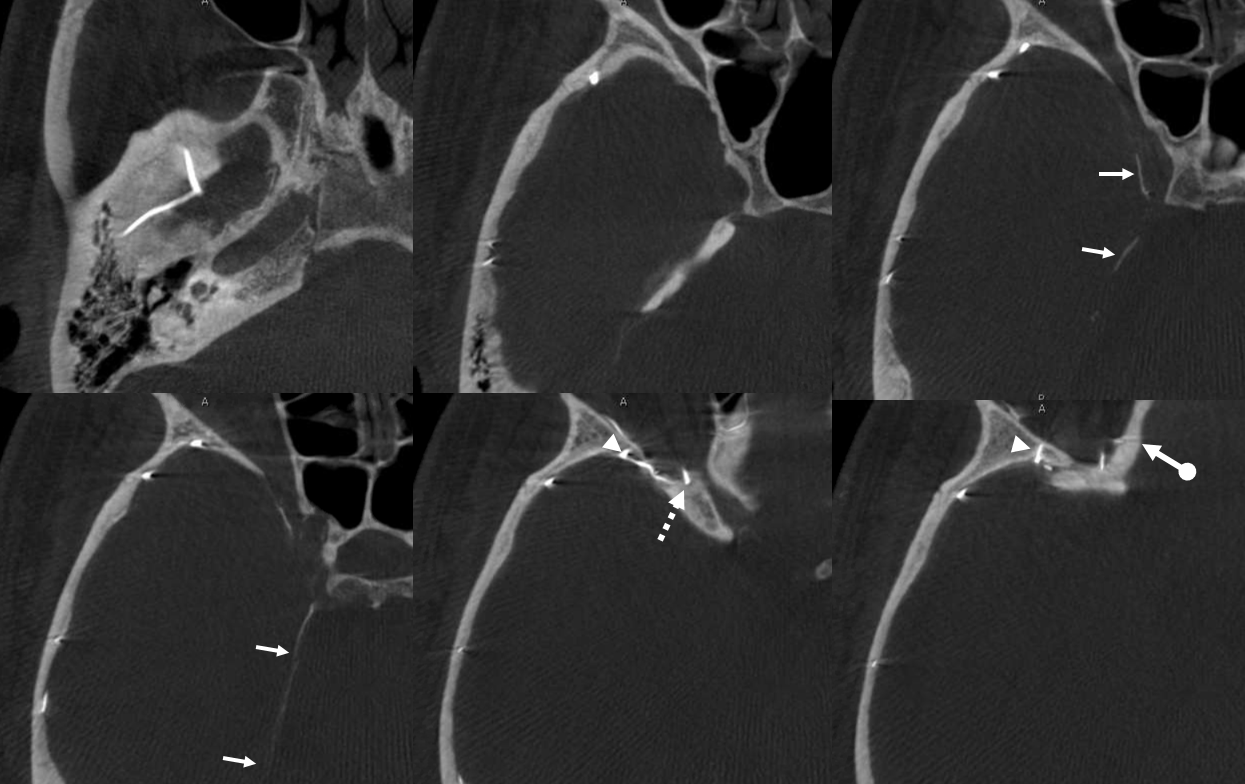

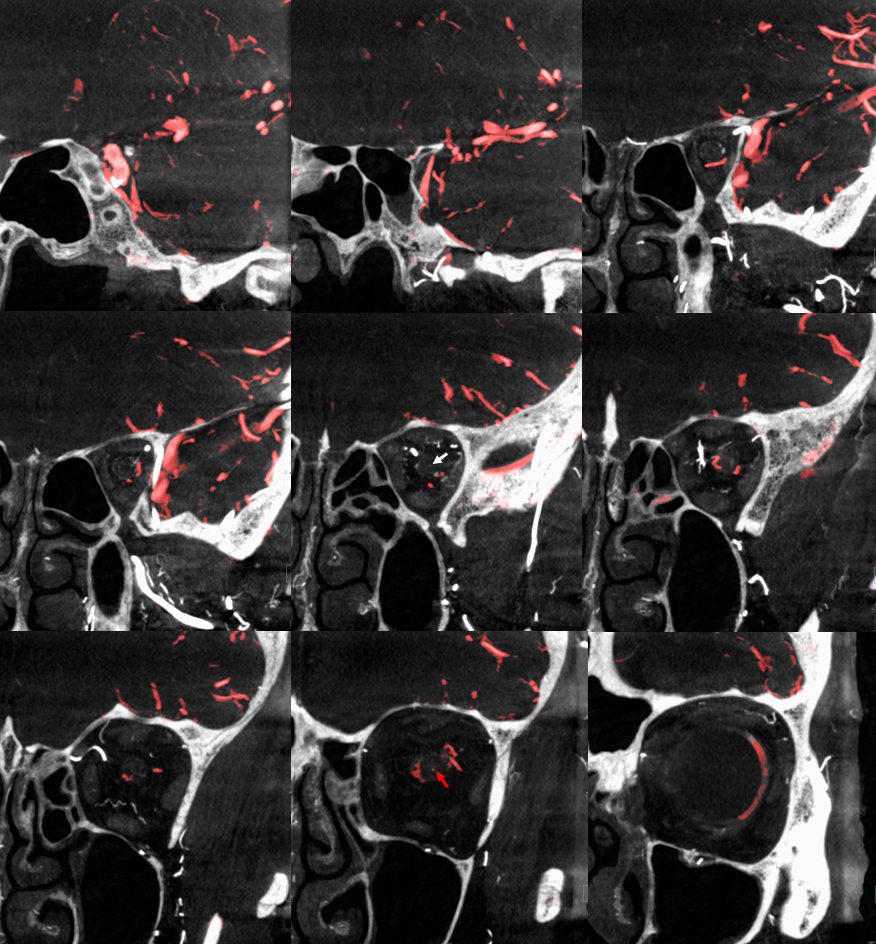
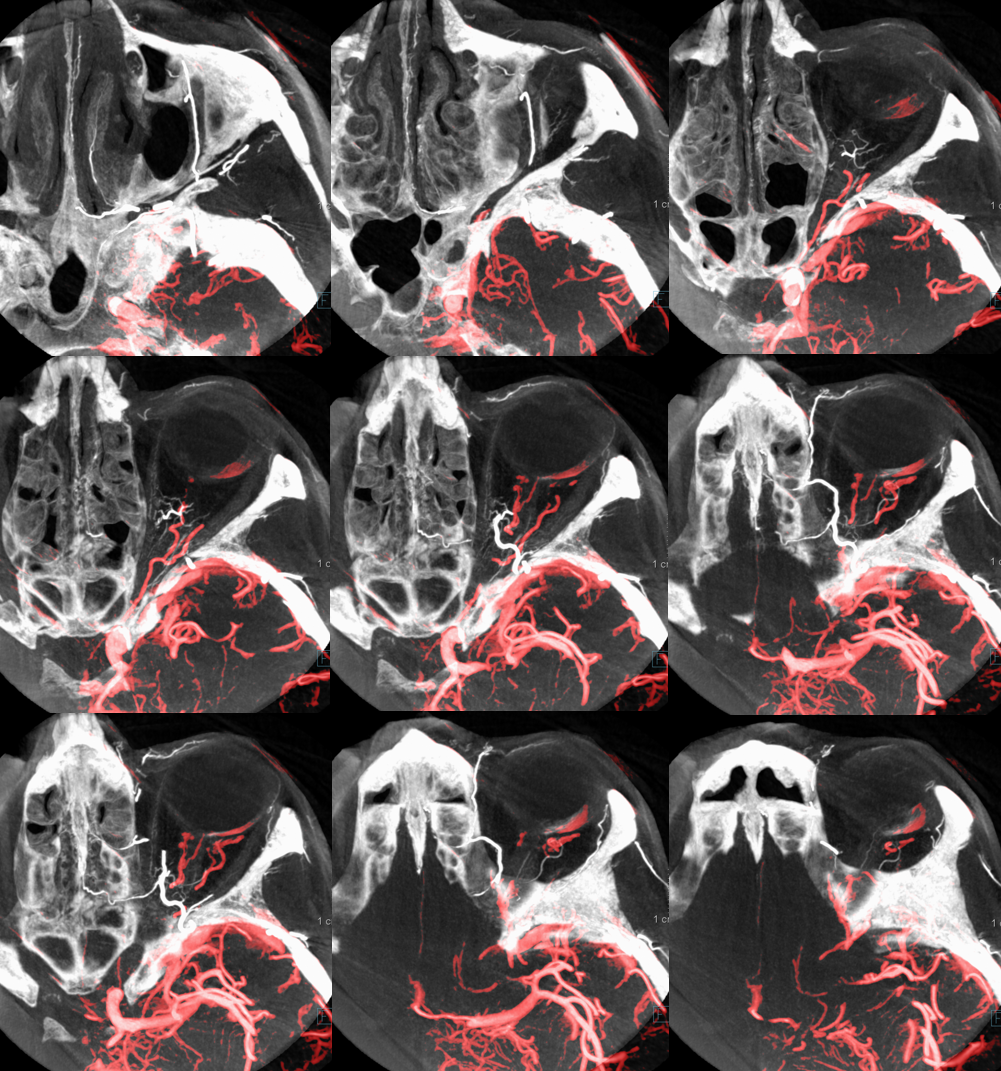
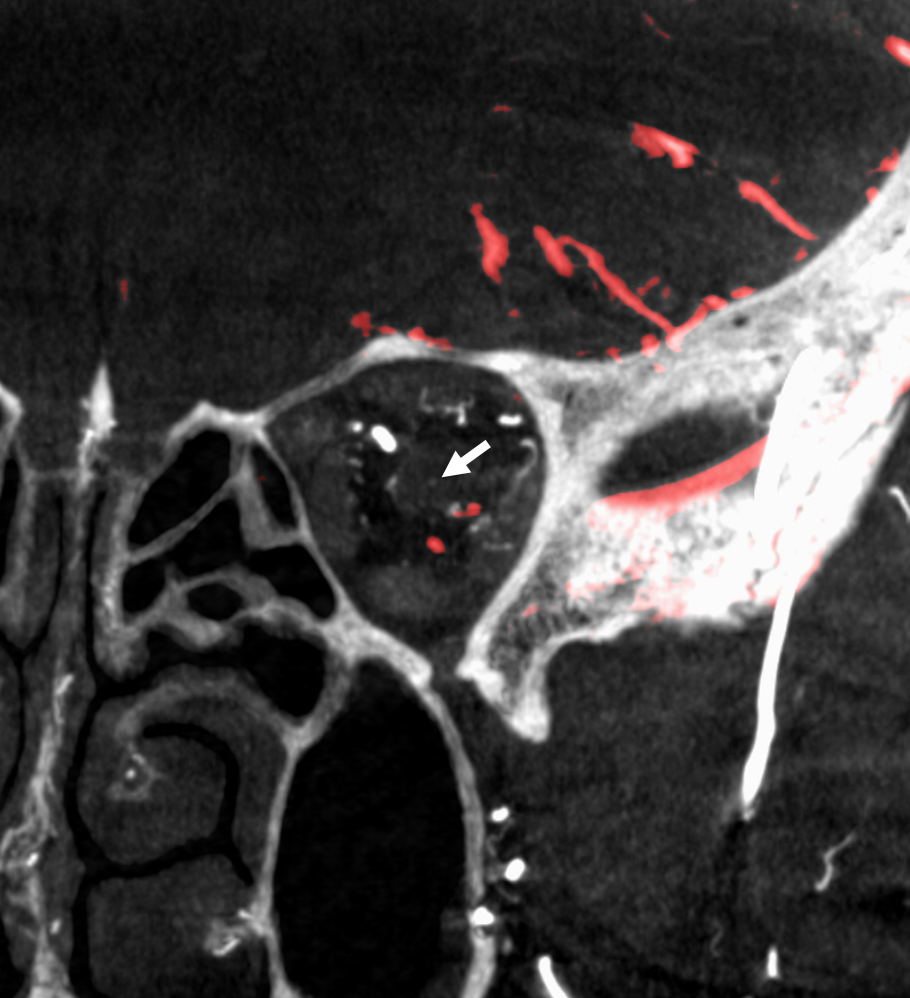
Movie of DYNA axial data — pause and scroll thru images
Nearly complete MMA supply of orbit — the meningo-orbital variant.
Rarer, of course, since it represents a more complete takeover by MMA of the orbit — but not as rare as one might believe, since it is not discussed as frequently as the “meningolacrimal” variant. That’s another error we want to correct. In this kind of spectrum, we see MMA primarily supplying most of the orbit — except that there is no choroid blush. That comes from a gracile ophthalmic artery, which seems to be limited to supply of the nerve and ciliary vessels. Since it does not have a name, we hereby name it the meningo-orbital variant. Well, why not? Again, there is nothing new under the sun. In words of the great Hayreh (based on his observations and the literature he studied extensively): “It is very rare for the entire orbit, including the central retinal artery, to be supplied from the middle meningeal artery. The central artery of the retina usually preserves its connexion with the cerebral circulation by arising from the internal carotid even though other branches in the orbit may arise from other sources such as the middle meningeal“
In this example, courtesy Dr. Daniel Sahlein — ophthalmic supply limited to nerve and globe — notice also the relatively distal origin of the ophthalmic — the classic hypophyseal segment — see spectrum above
DSA of MMA injection
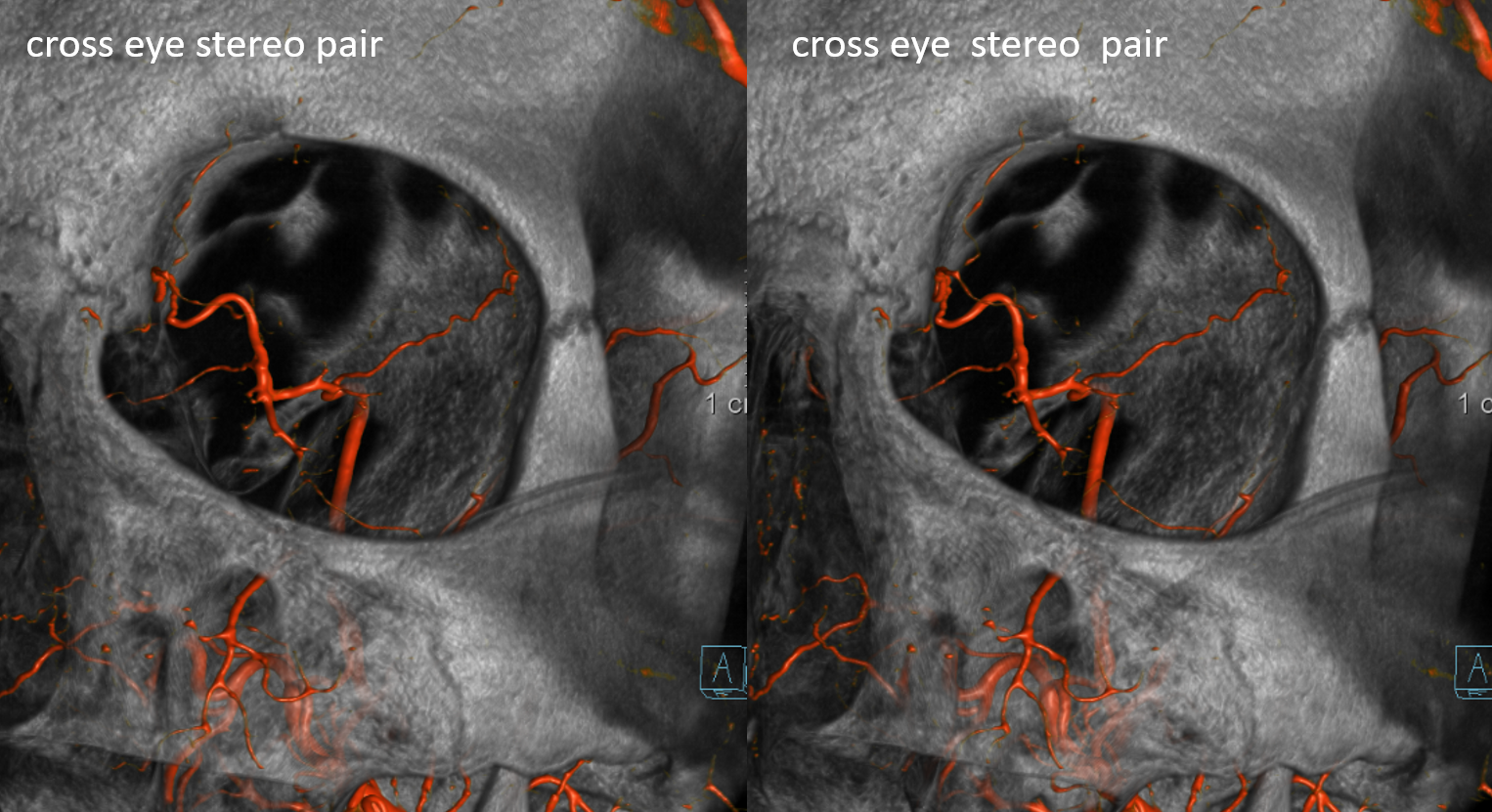
Amazing DYNA MMA images, best of what’s available in 2021. Lets see what happens 10 years from now — the original ophthalmic artery page was made 10 years ago — see how much things have improved…
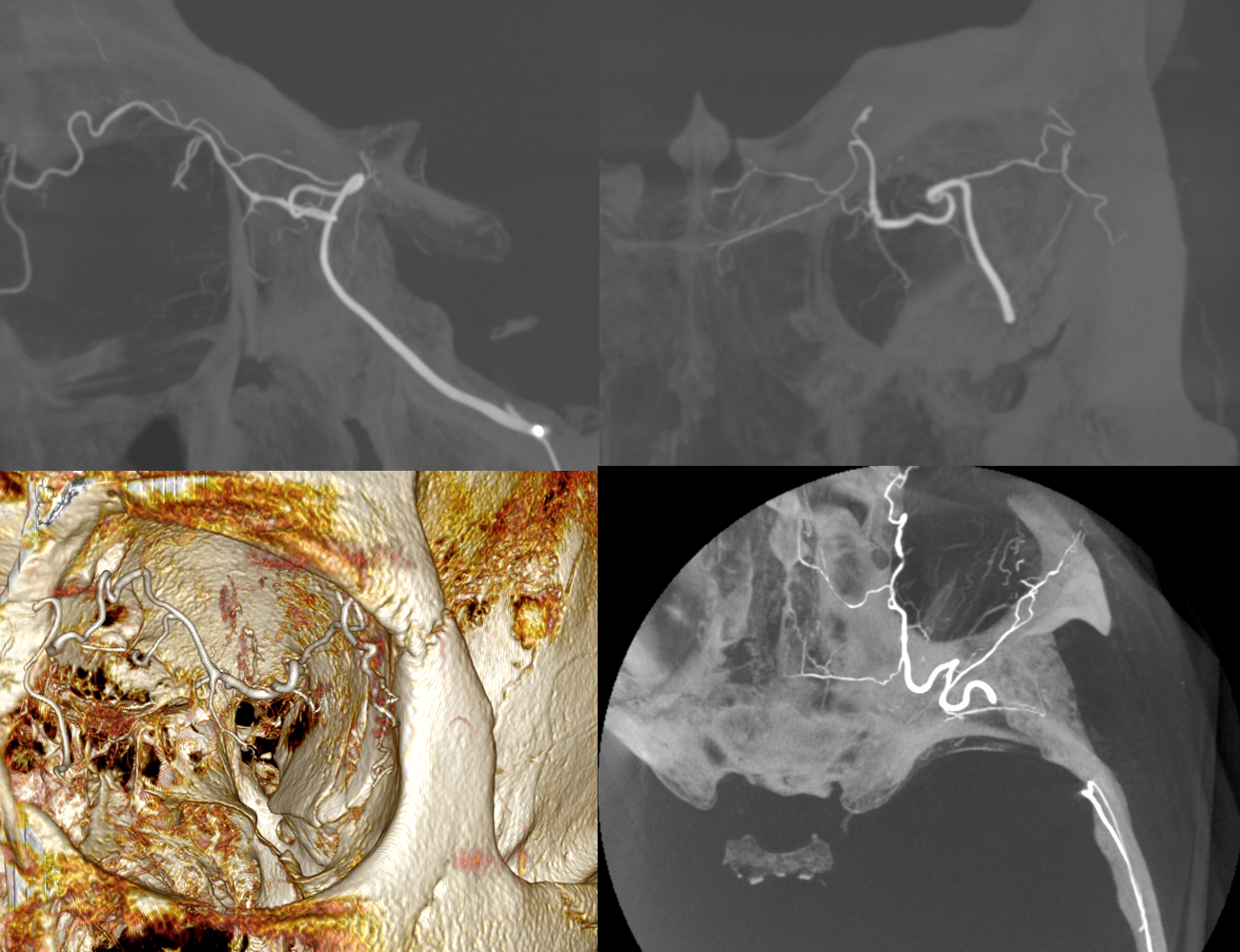
Another example below — there are extensive images here, with DYNA movies and a wealth of information related to supply of nerve, orbit, globe, etc. Bottom line is that ophthalmic supply is mainly to nerve and globe, via the long and short ciliary arteries (more on that below). The CRA is beautifully seen. The MMA supplies nearly all of the rest of orbit — except for probably one short ciliary branch — see that part of choroid blush? Its all a spectrum…
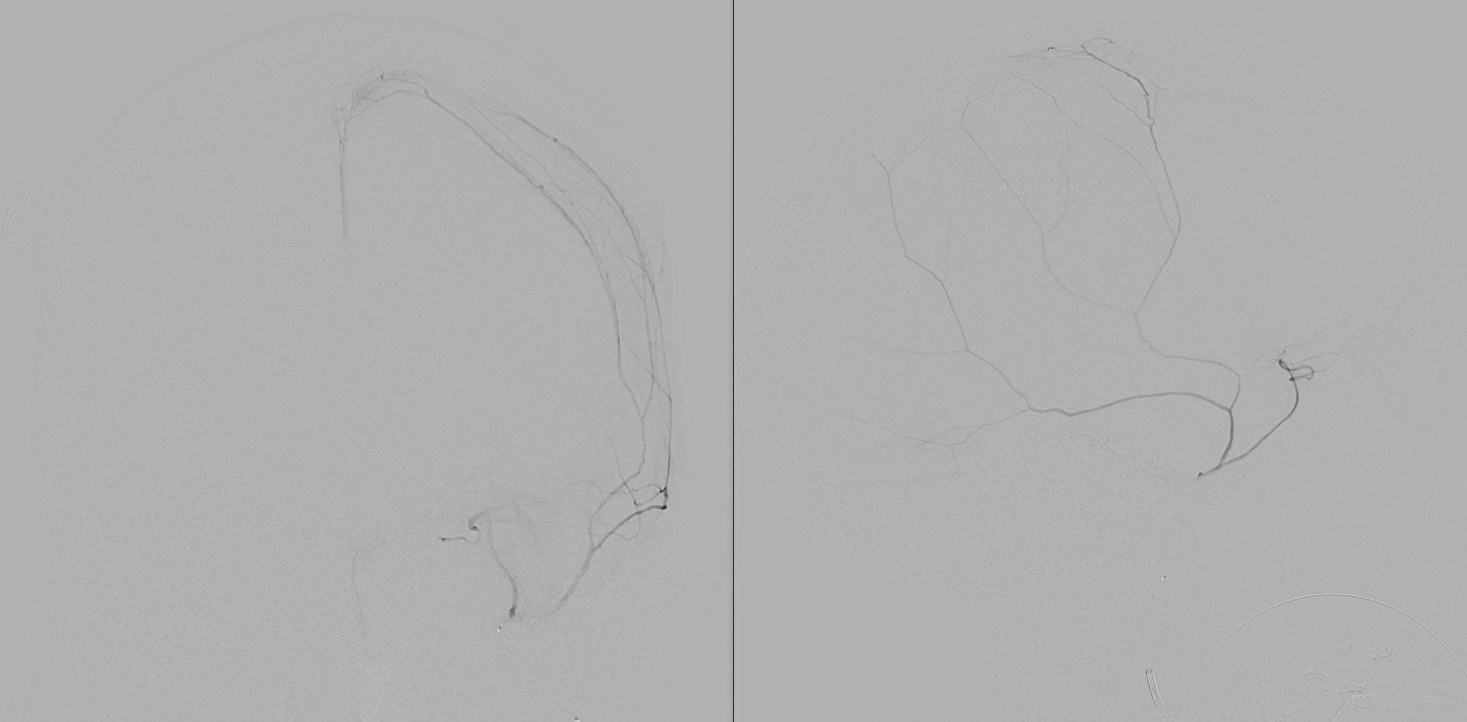
ICA
ECA
MIP DYNA ICA
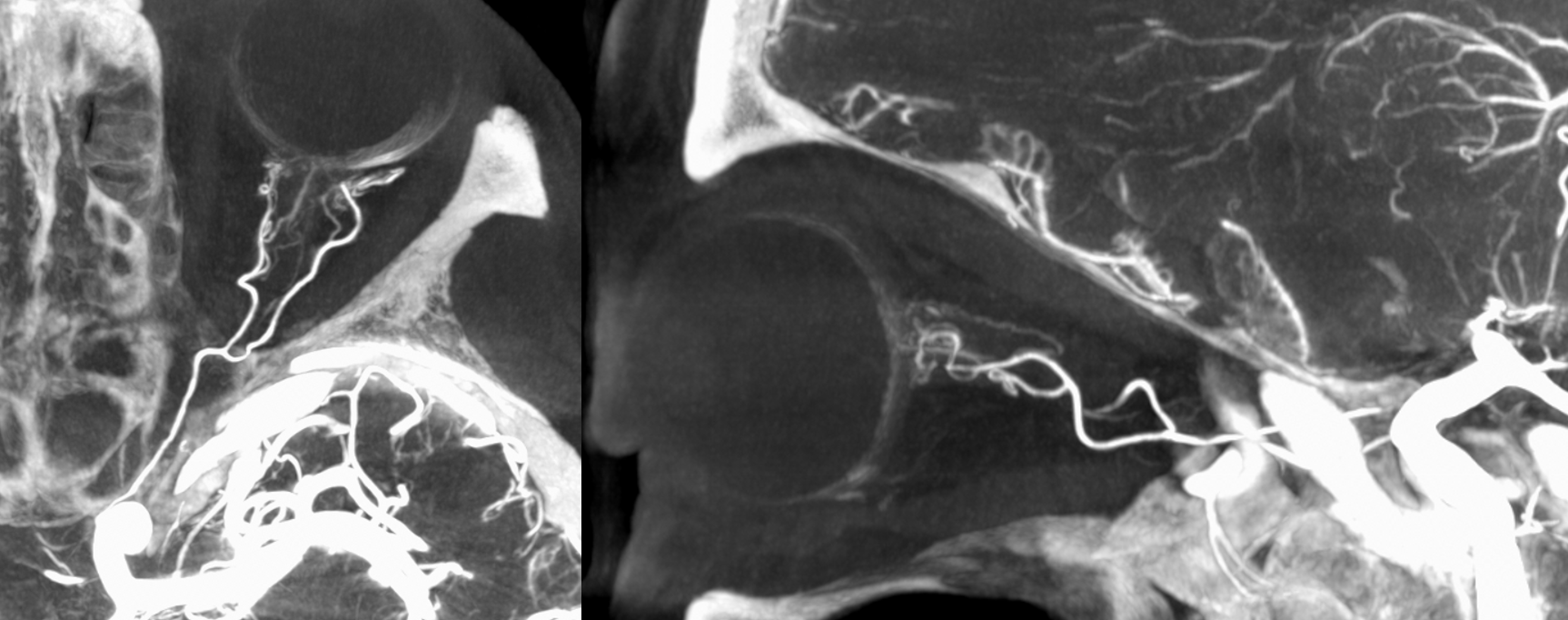
MIP DYNA ECA
Stereos ECA
Stereos ICA
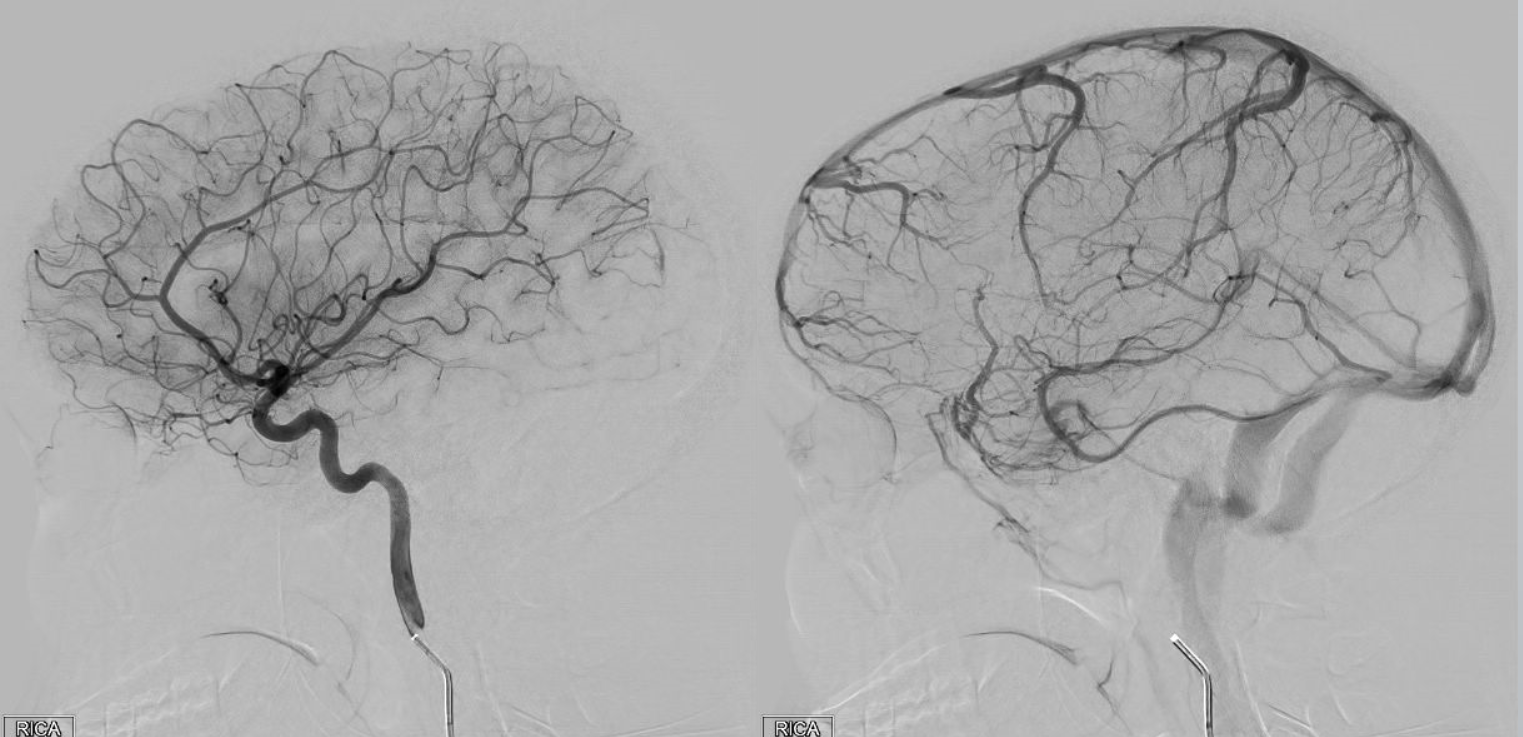
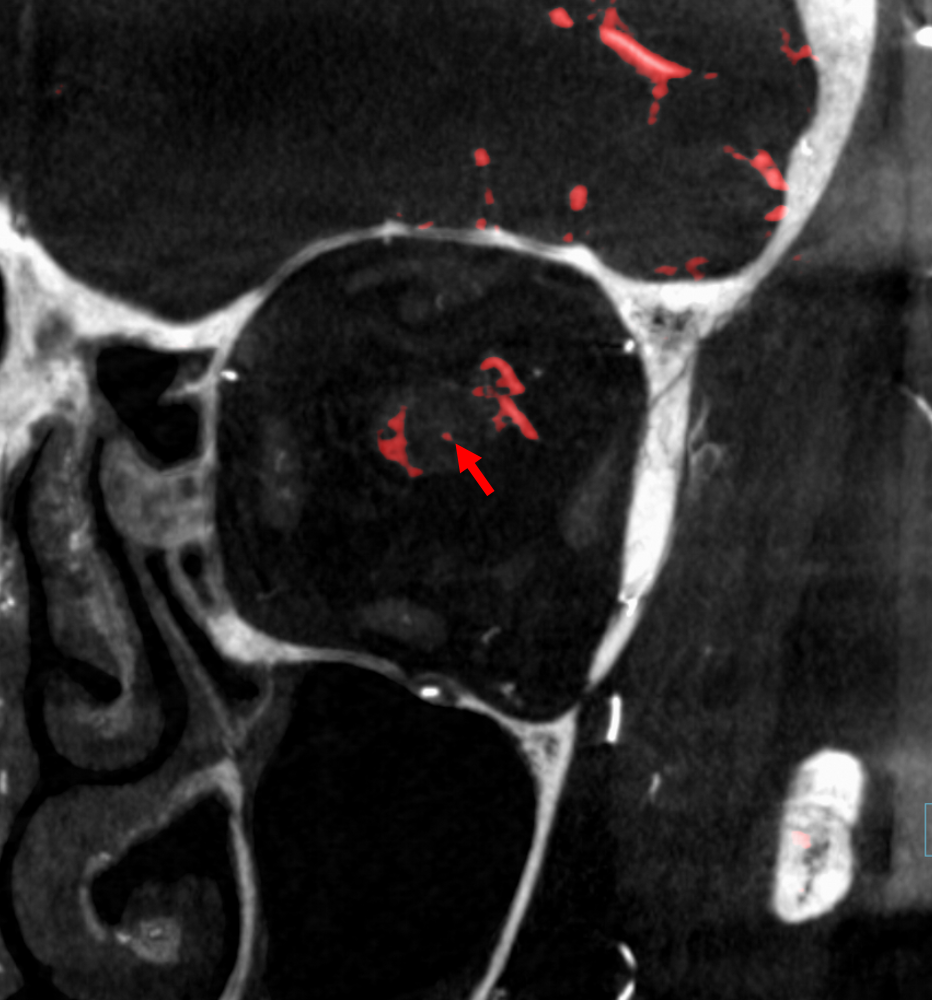
Beautiful co-registered ICA and ECA injection DYNAs — there is dual supply to the optic nerve — proximally its from MMA (white arrow), more distally / CRA is from ophthalmic (red arrow)
Movie
Cases involing the Lacrimal Artery? Click on link to see more
Orbital Lacrimal AVM — preoperative embolization
Orbital AVM — direct puncture and trans-ophthalmic embolization
Orbital metastasis preoperative embolization