
SUMMARY
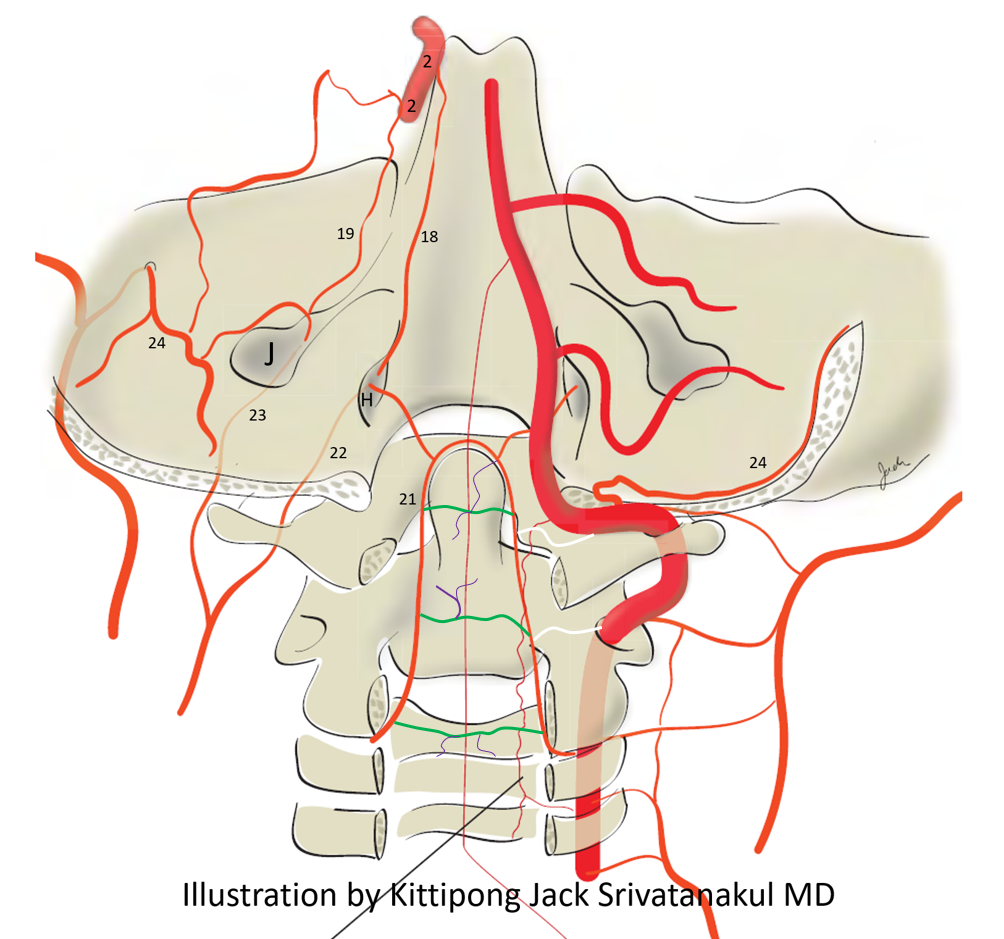
Although seen as a unique structure, the odontoid arcade (21) is homologous with the ventral epidural arcade of the rest of the spine. The reason it looks different is because C2 is different — incorporating the body of C1 into its own body as the “dens”. Like epidural arcade, it links bilateral vertebral arteries not just at C3, but at C2 and C1 levels as well (white above) as well as itself (green above), and participates in supply of the adjacent bone (purple above). Superiorly, it is unique in its connection with the hypoglossal division of the ascending pharyngeal artery, supplying associated dural fistulas and meningiomas. Higher still, it is homologous with the medial and lateral clival arcades, ultimately connecting to the ICAs via the meningohypophyseal trunk. The great thing about odontoid arcade is that it has no directly associated radicular or radiculopial/radiculomedullary arteries, this being a relatively good embolization position — relatively because potentially hazardous connections with the other vert, hypoglossal division, and radicular / medullary arteries still exist.
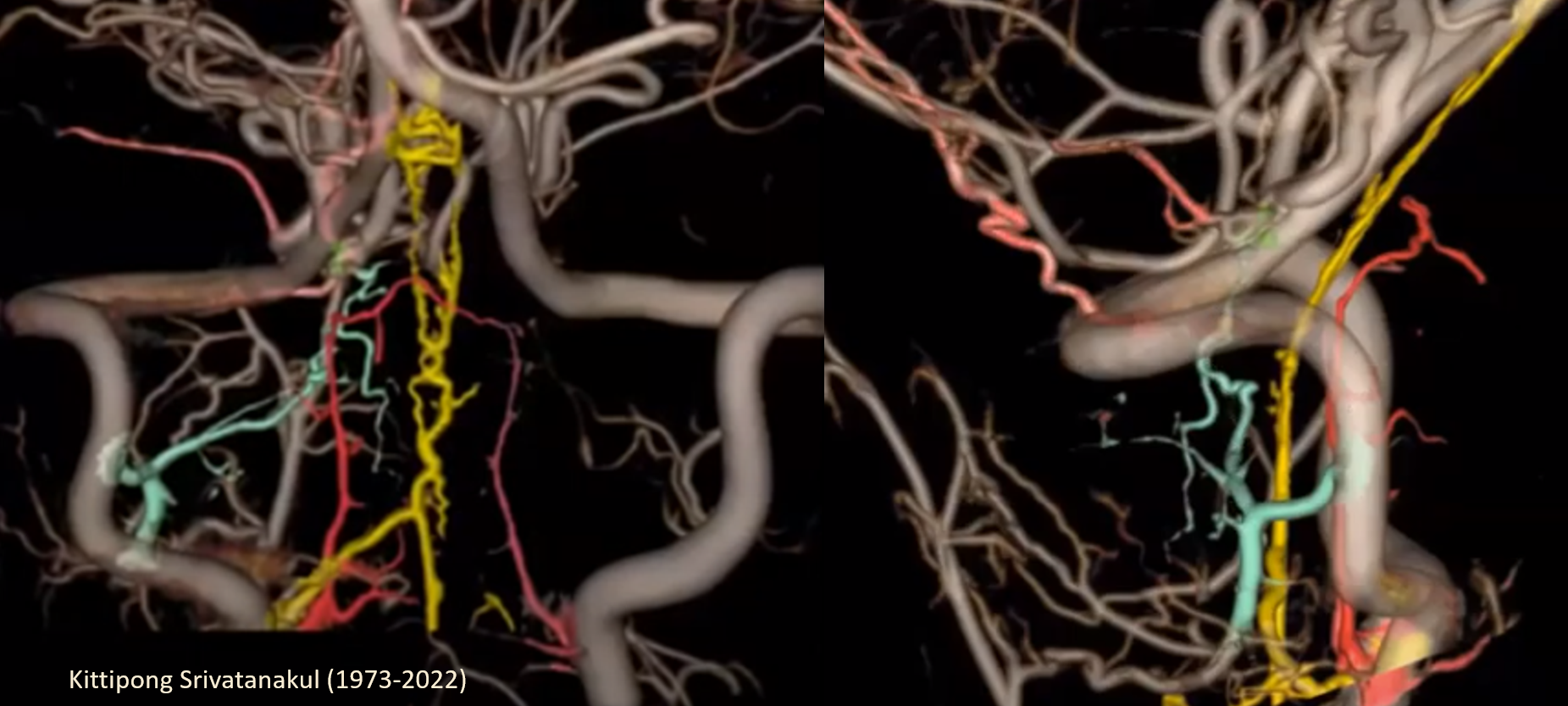
A nice segmentation by Kittipong. Note C3 (yellow) and C2 (turquoise) and C1 (rose-colored, frontal image) contributions to the anterior and posterior/lateral spinal systems. These are typically separate from the odontoid arcade, the latter being a relatively safe embolization position.
BALANCE / ADJACENT TERRITORIES
- Vertebral artery — the odontoid arcade connects both verts. Injection of one side should be monitored for potential spillage into the other
- Hypoglossal division of the ascending pharyngeal artery. This division traverses the hypoglossal canal and thus supplies the XIIth nerve. The odontoid arcade connects with the continuation of the hypoglossal division intracranially. Liquid embolic use in this area risks CN XII palsy, which is problematic unilaterally and devastating bilaterally.

Above is left vert injection. There is a C2 level spontaneous dissection, which together with the hypoplastic baseline nature of the vert with wedge position of the 4F vert catheter allows one to see so much more. The odontoid arcade (white arrows) and the dorsal epidural arcades of C3 and C4 opacify the normal right vert. C1 level transverse anastomoses (typically with the vert) are present as well. Above the dens, the odontoid arcade anastomoses with the hypoglossal division of the ascending pharyngeal artery (black and dashed black arrows)
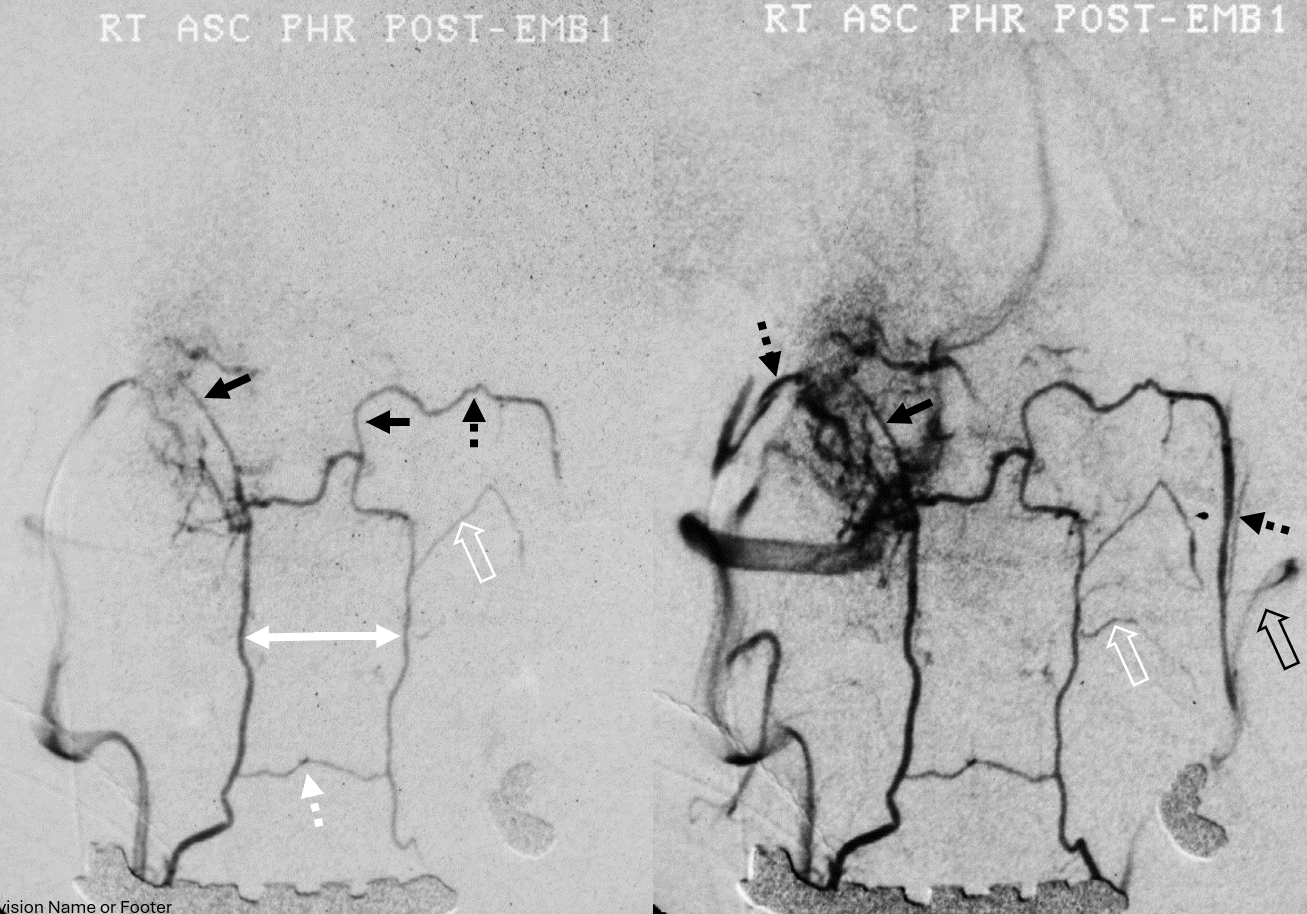
Vintage analog subtraction angio of the same. Microcatheter in the right proximal odontoid arcade, refluxing into right vert in earlier phase left image, and in later phase via retrograde opacification of the left odontoid arcade spilling contrast into the left vert (open black arrow). Both C1 epidural connections (black arrows) to the hypoglossal divisions (dashed black arrows), and in later phase further retrograde opacification of bilateral pharyngeal trunks — no arrows, figure it out yourself. There are ventral epidural anastomoses at C2 body (dashed white arrow) and C2 longitudinal segmental dural / radiculodural arteries (open white arrows). In the later
Osseous Suppy
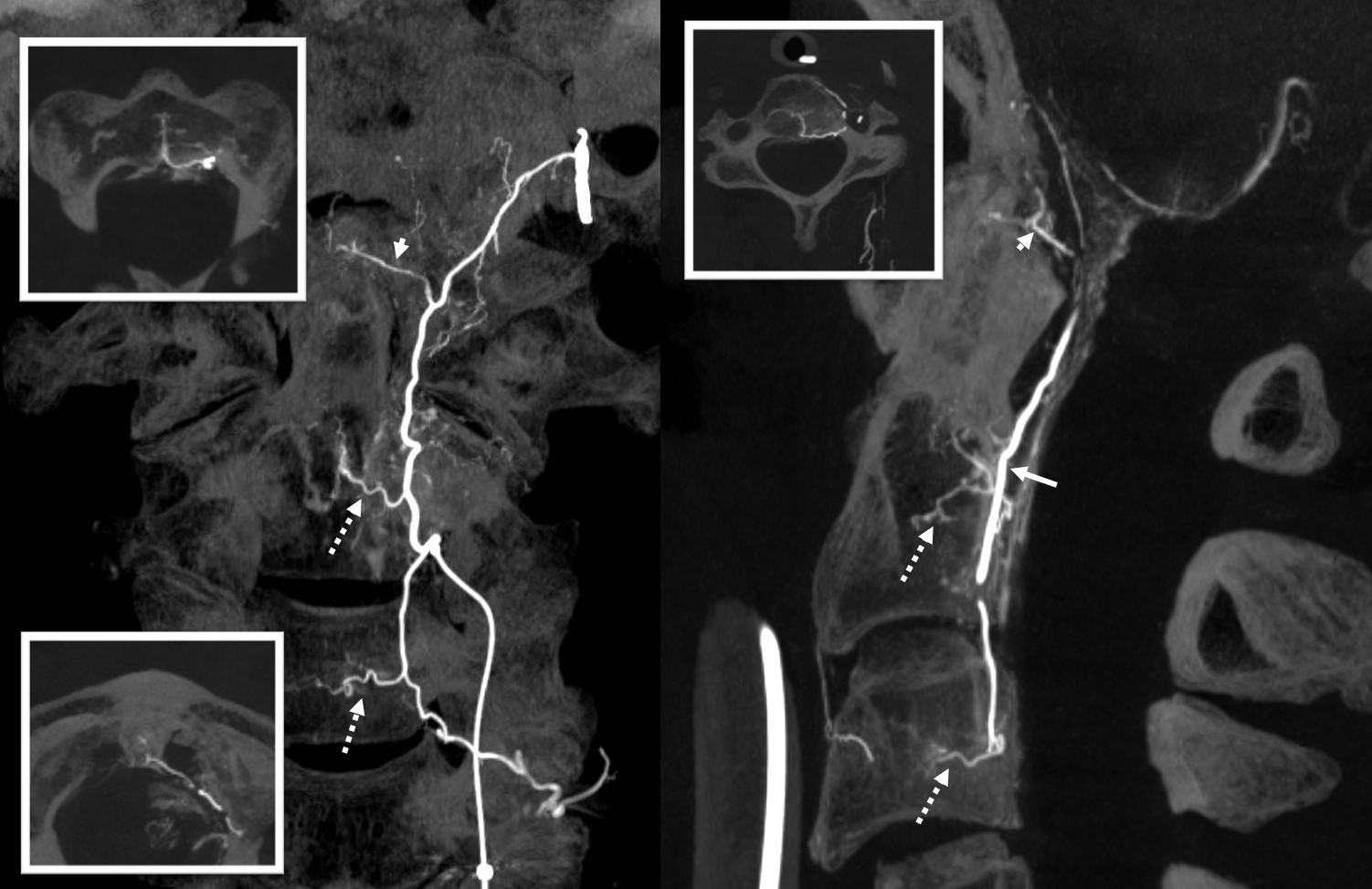
Often overlooked, and just like elsewhere in spine, the odontoid/epidural arcades supply adjacent nonneural structures — dura and bone — C3 C2 and C1 in this case. Odontoid arcade (open arrows), transversely oriented epidural branches (dashed white arrows), intraosseous branches (solid white arrows), and ventral bone supply from C2/C3 segmental branches (dashed black arrows)
Without annotations below
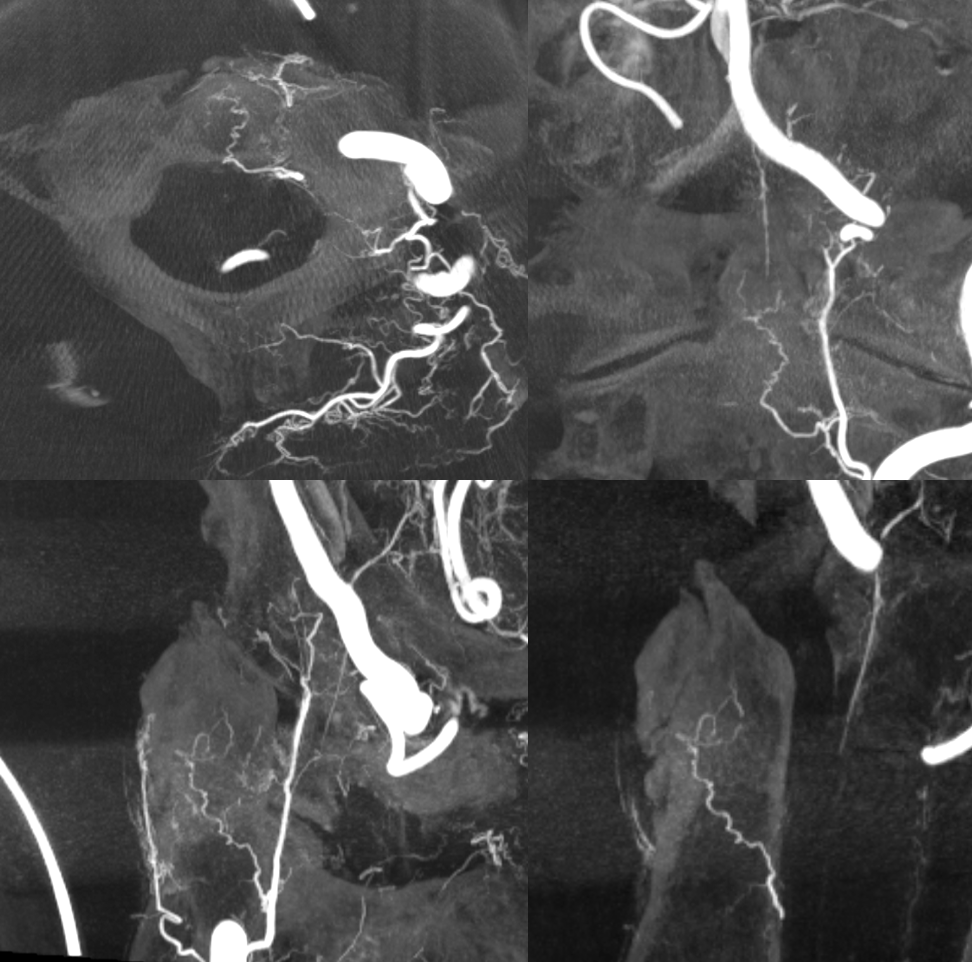
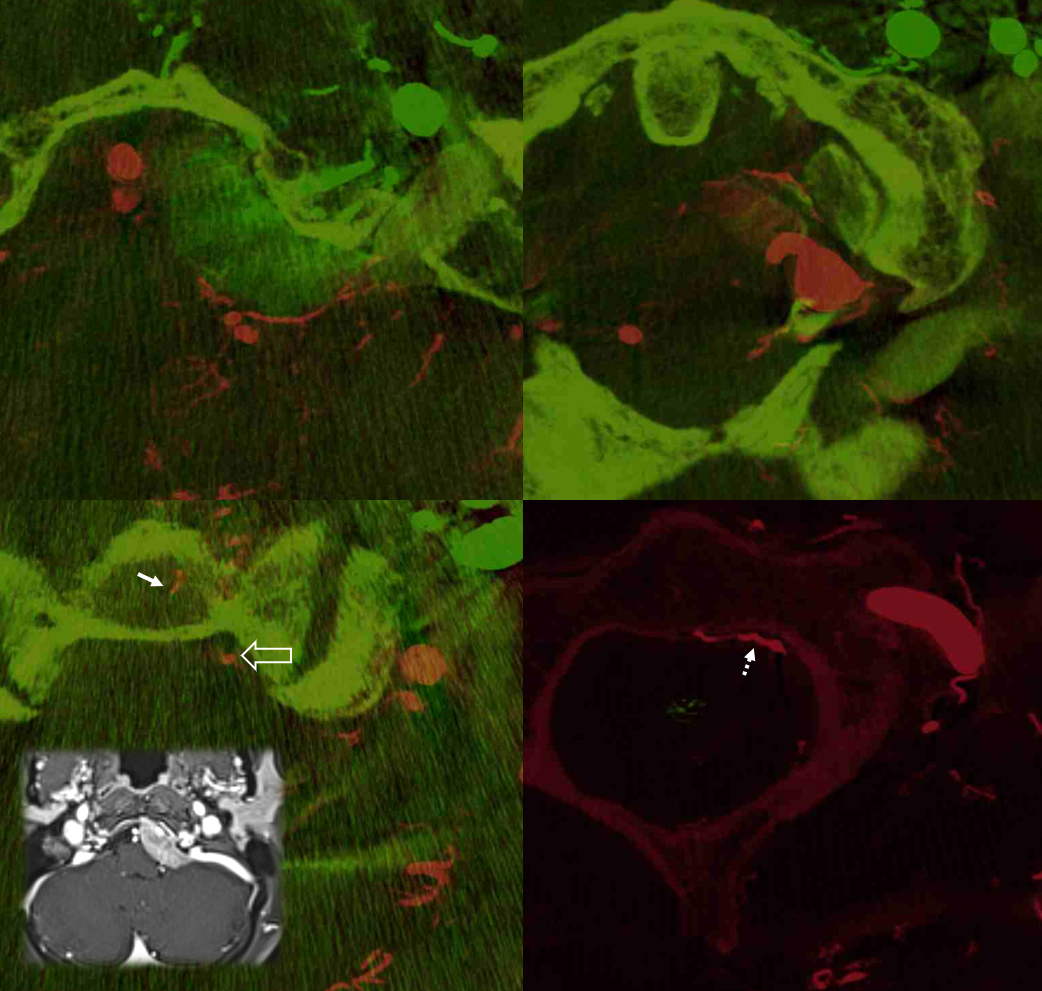
Many cases, like the one above, are derived from embolization of meningiomas, allowing for subselective odontoid catheterizations. Below are fusion DYNA CT images of this case, showing the target lesion. Most of the supply is derived from hypoglossal division, seen via the green-colored left ECA injection. The vert injection is in red, opacifying the arcade among everything else vertebrobasilar.
Another case study of odontoid arcade from another meningioma
The microcatheter (its relatively easy to catheterize the arcade given it favorable angle of origin from the vert) is in the arcade (solid white arrow, retrogradely visualizing the left portion of the arcade (black arrow) the left vert (black arrowhead). C2 and C1 epidural connections are present. The hypoglossal division (dashed white arrow and arrowhead) retrogradely opacify the ascending pharyngeal artery and the external carotid (open white arrow).

Another case — cone beam CT is great of course for odontoid arcade and most everything else. Left vert injection opacifies the odontoid arcade (arrows) and its supply to C2 bone (dashed arrows). Note also excellent visualization of both anterior spinal artery territory (white oval) and very prominent posterior / lateral spinal region (dashed white oval)
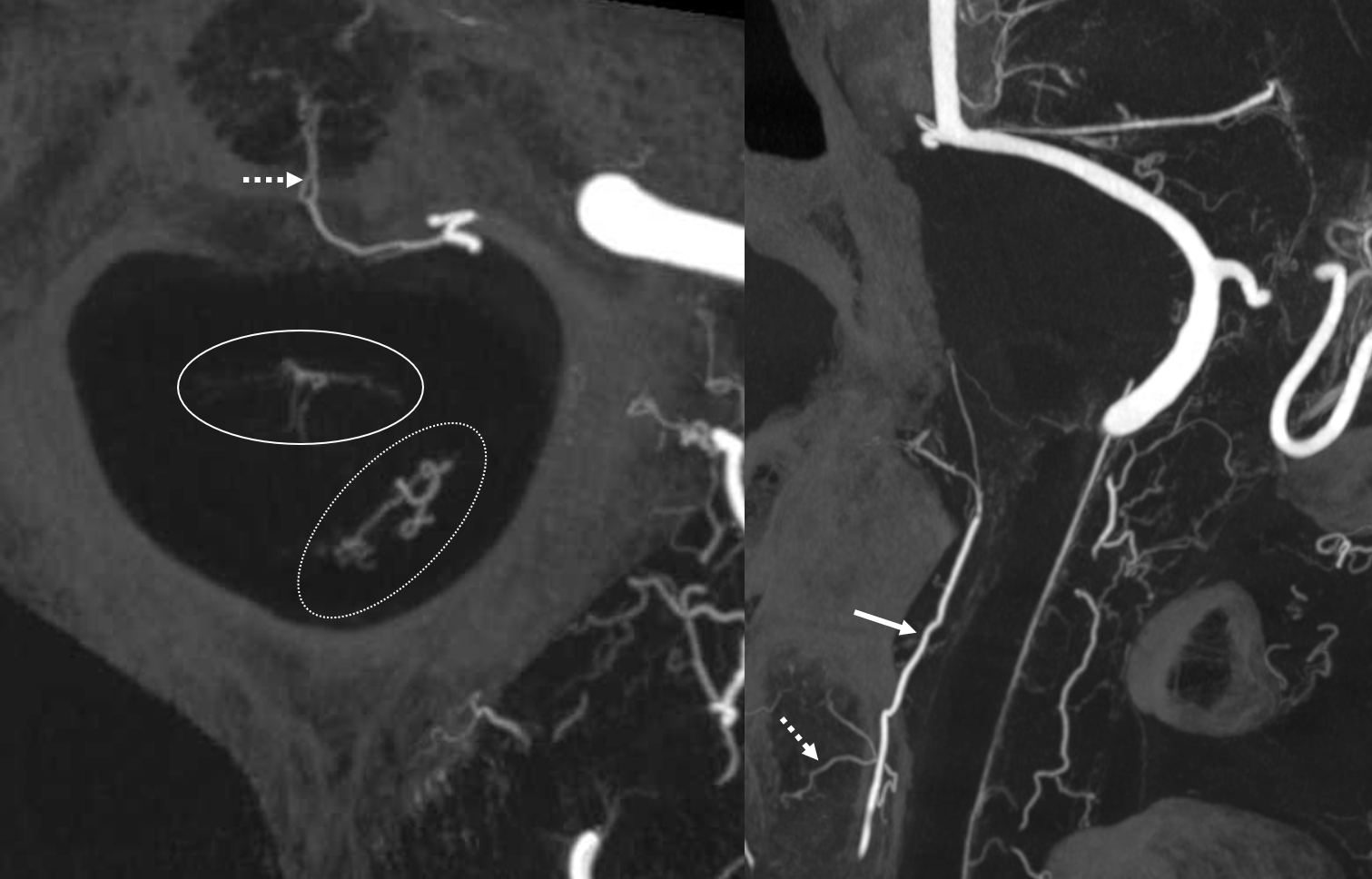
The same case, now with microcatheter position in the odontoid arcade. The same supply to the bone is noted, however note complete lack of spinal cord or radicular artery visualization. Direct spinal cord supply from the odontoid arcade is exceptionally rare, making it a relatively good embolization position in what is still a very treacherous area.
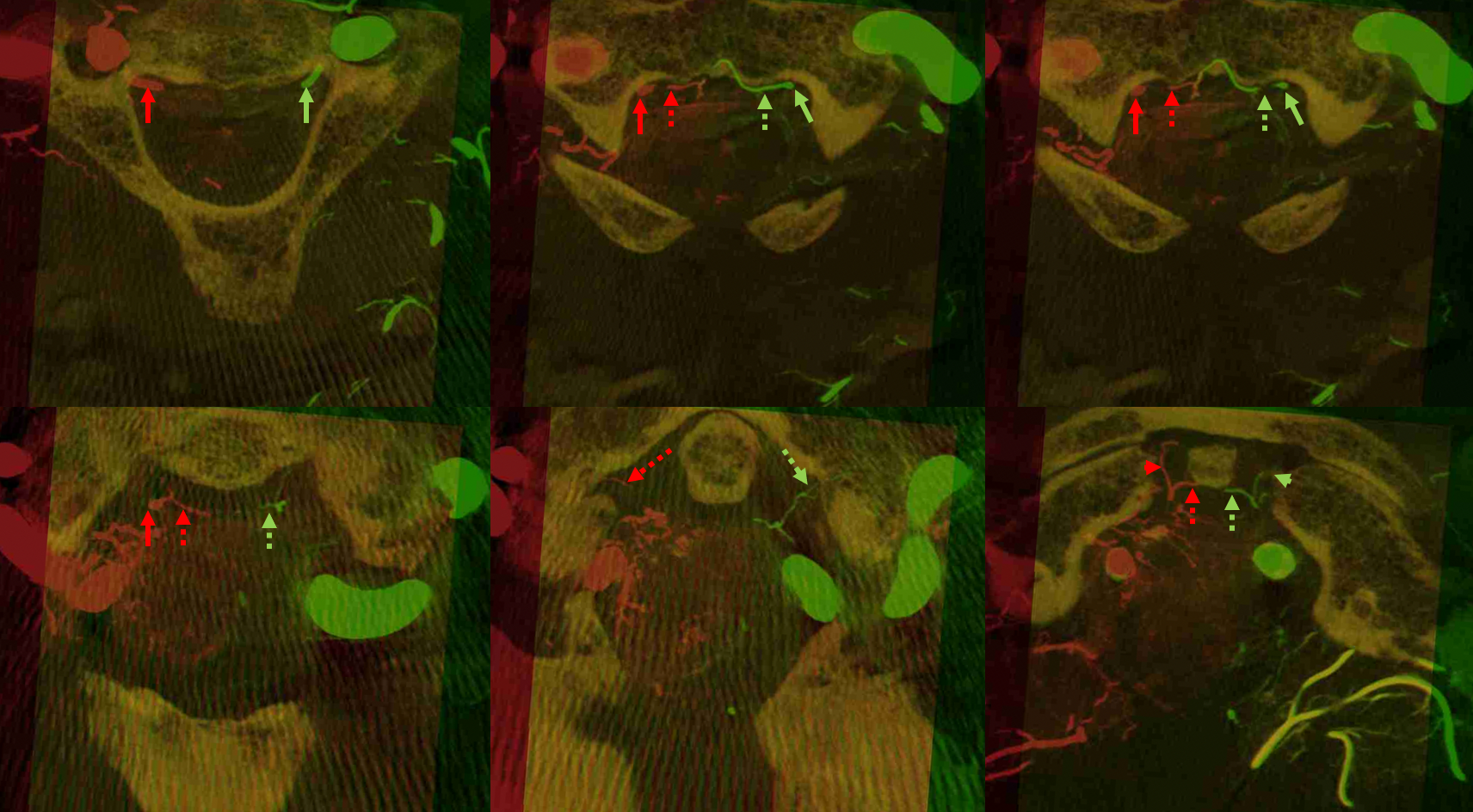
Fusion of two vertebral artery Cone Beam CT injections demonstrating both odontoid arcades (solid green and red arrows), and the intersegmental epidural connections between them (dashed arrows). At the apex of the arcade, supply to the ligamentous / adipose tissues around the dens is also present (arrowheads)
Radicular / Cord Connections
Of course, they do exist – in this relatively safer territory there will always be things to watch out for. In the same case, we see below the left odontoid arcade (arrow) connecting via epidural branch (dashed arrow) to a likely dural branch in the C3 nerve root sleeve (arrowhead). It is a thinner branch and separate from the more prominent beautifully seen ventral (solid open arrow) and dorsal (dashed open arrow) radicular branches which supply the C3 nerve and lateral cord. Both the nerve root sleeve (arrowhead) and radicular branches arise from the common C3 segmental artery (ball arrow). Therefore, injection of embolic material (liquid embolic especially) should be done with care.

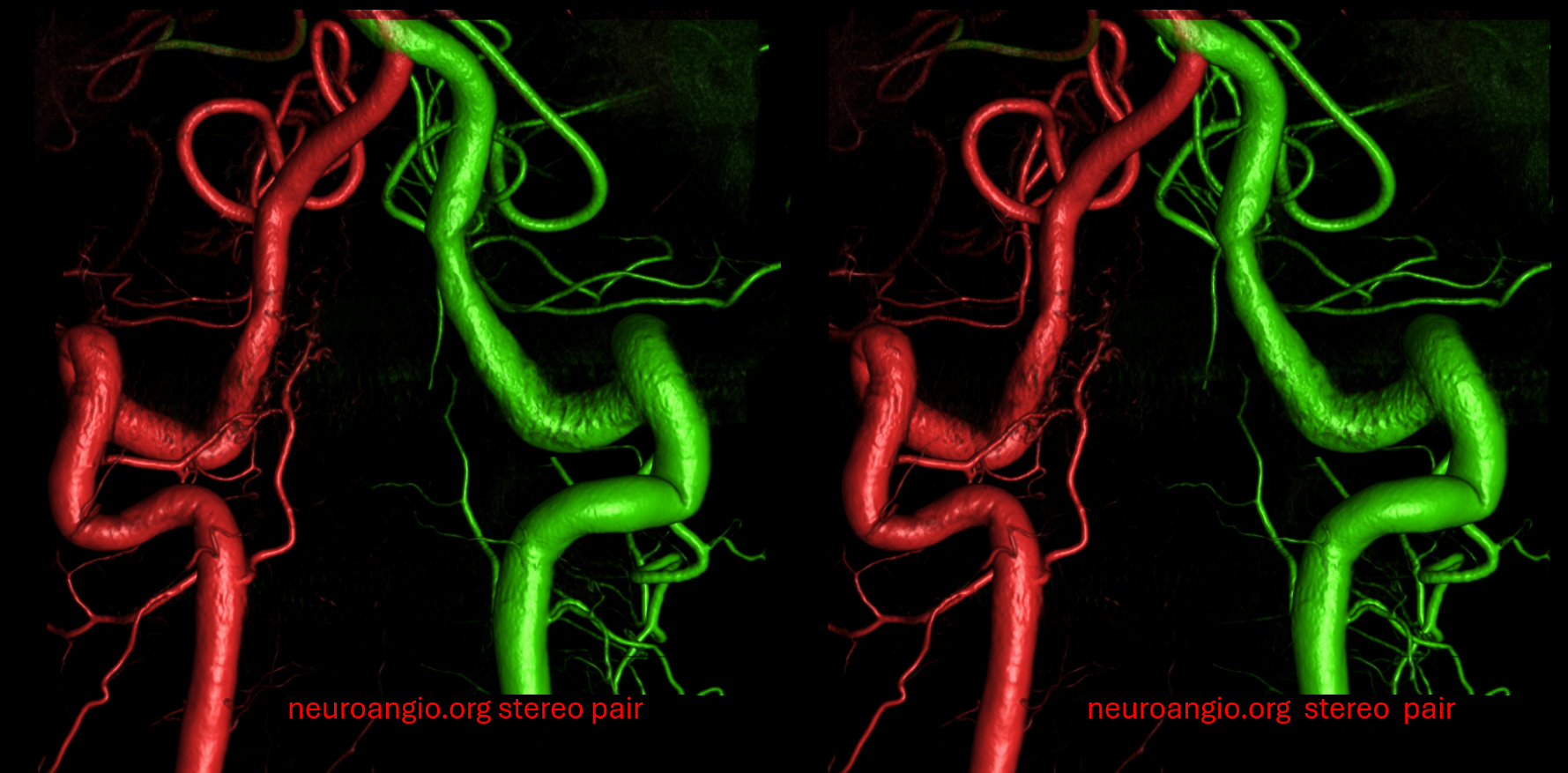
Stereo VR view
Summary
The odontoid arcade is a homolog of the ventral epidural arcade, its unique morphology parallelling the unique anatomy of C2. Lack of direct contribution to the spinal cord is a plus when it comes to embolization in this highly treacherous region, however various eloquent connections exist, especially to both verts and hypoglossal divisions. The arcade is usually involved in craniocervical junction meningiomas and upper cervical pial / dural fistulas.