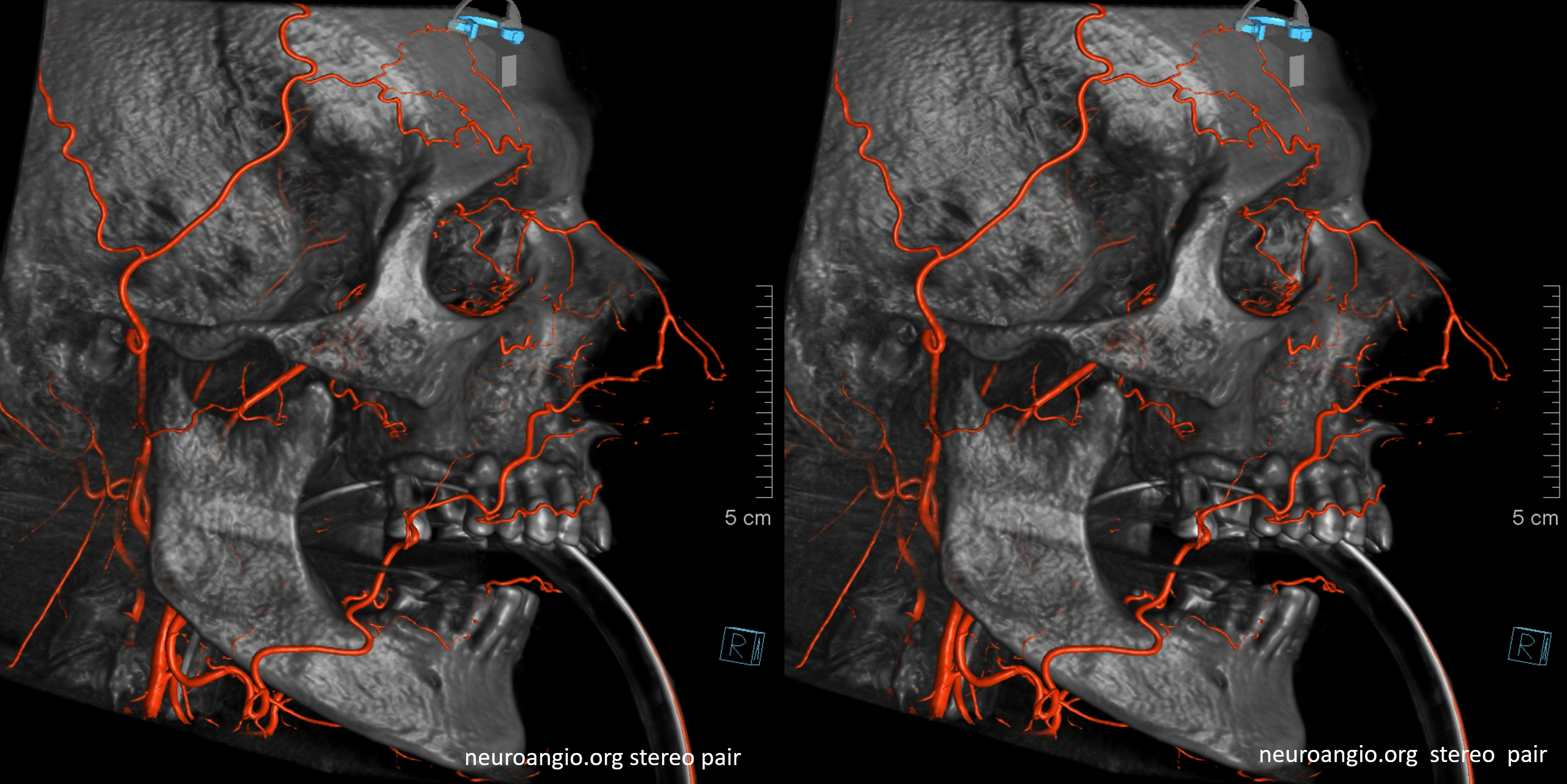
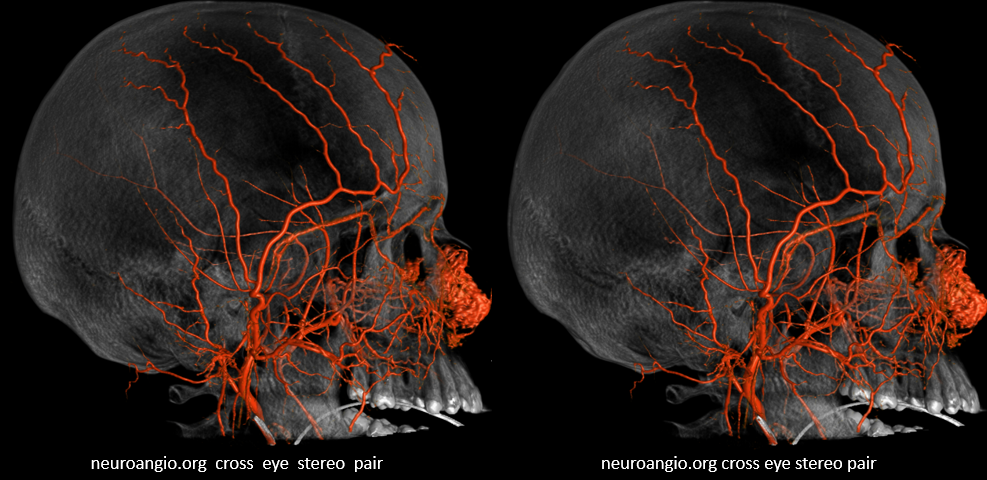
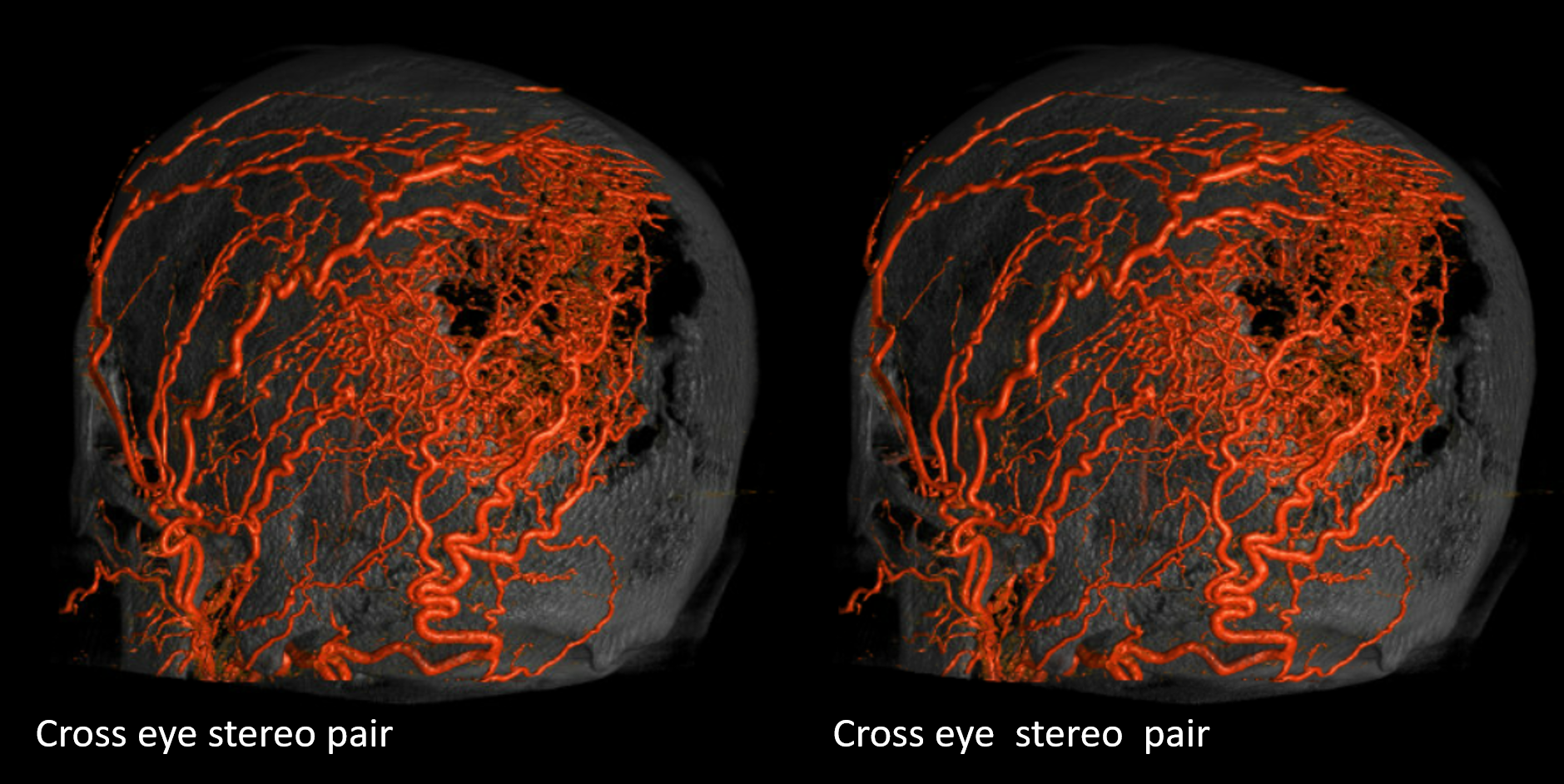
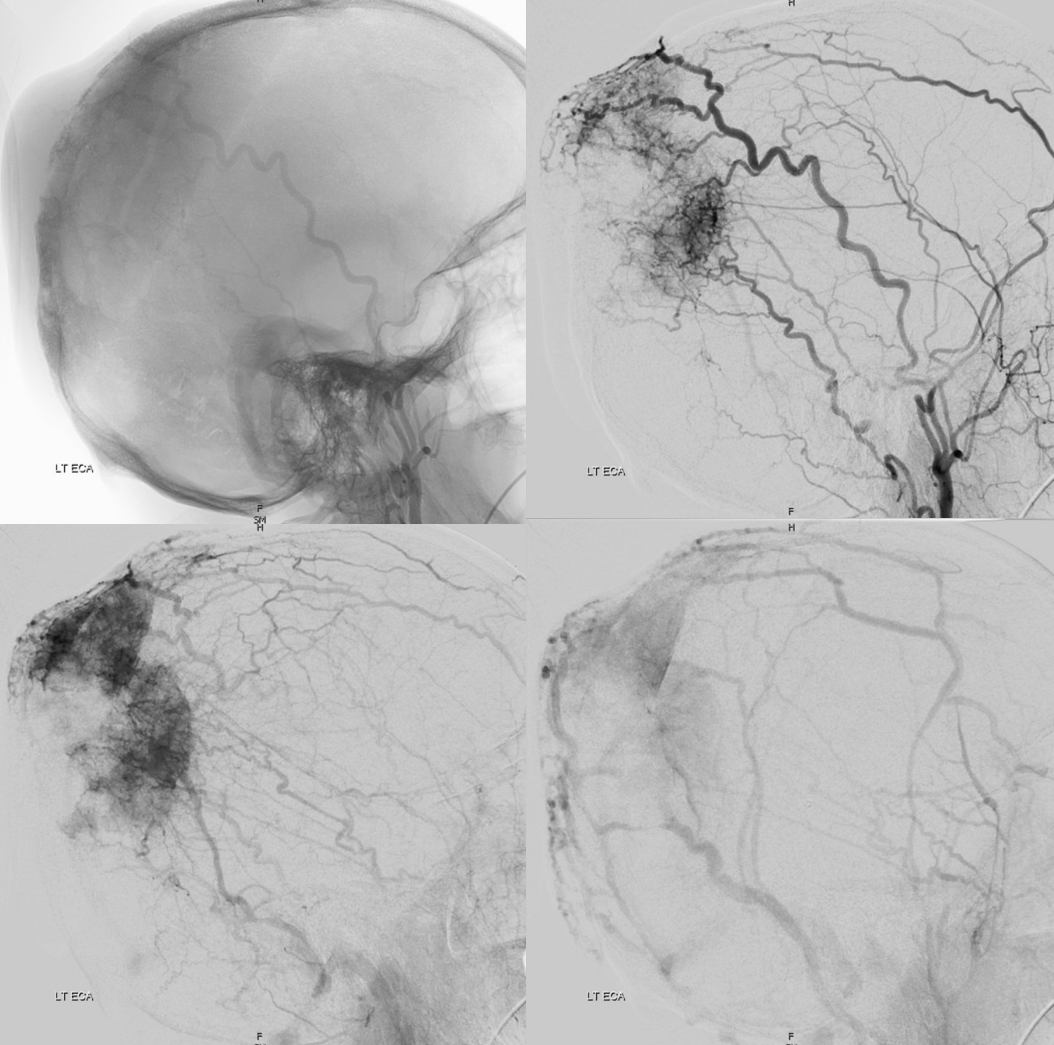
Cutaneous Artery of the scalp. Extensive collaterals with occipital, deep temporal, facial, and terminal branches of ophthalmic (supraorbital, supratrochlear). Important deep collaterals include under some unique and important circumstances the meningeal arteries such as the MMA
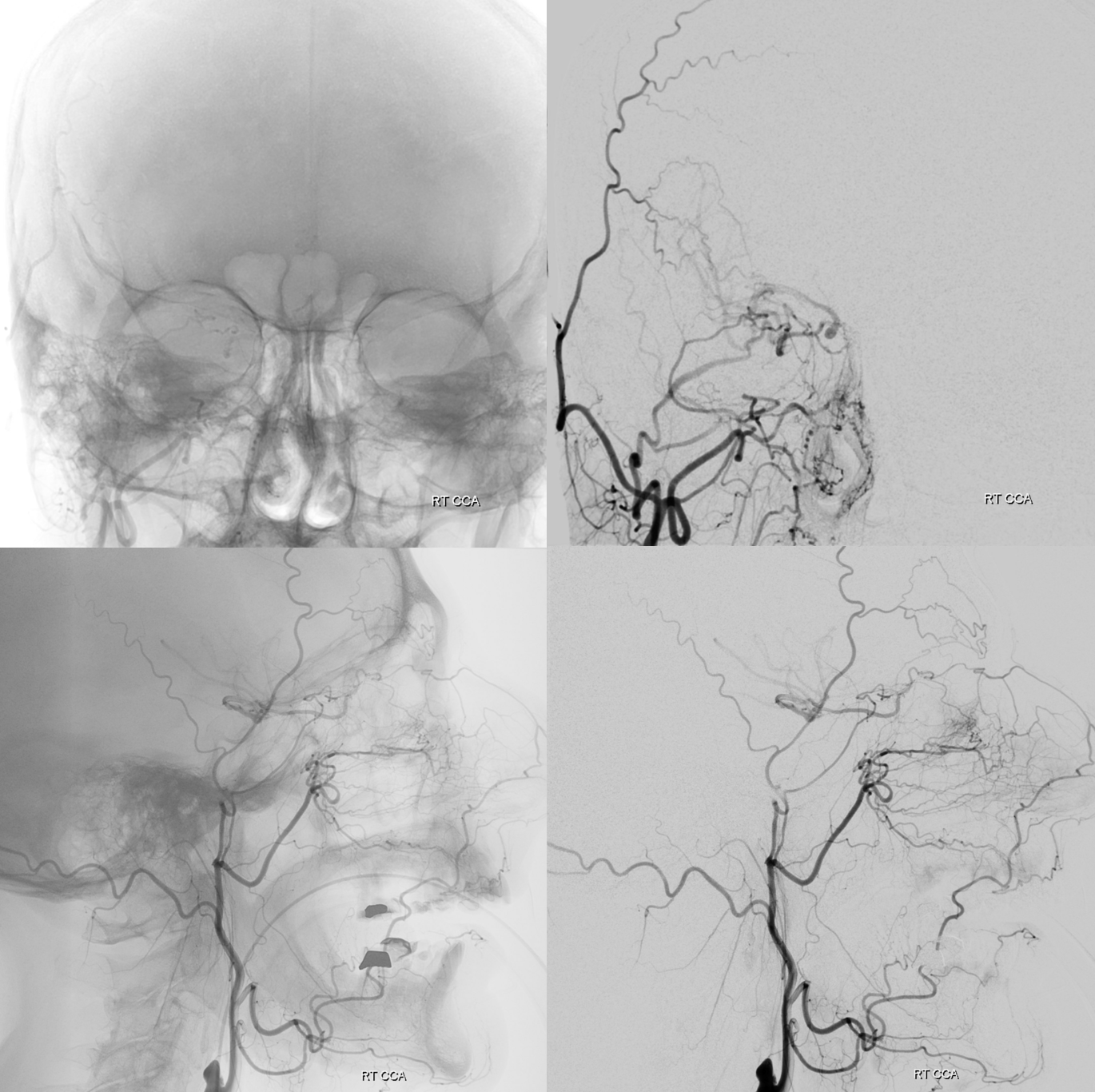
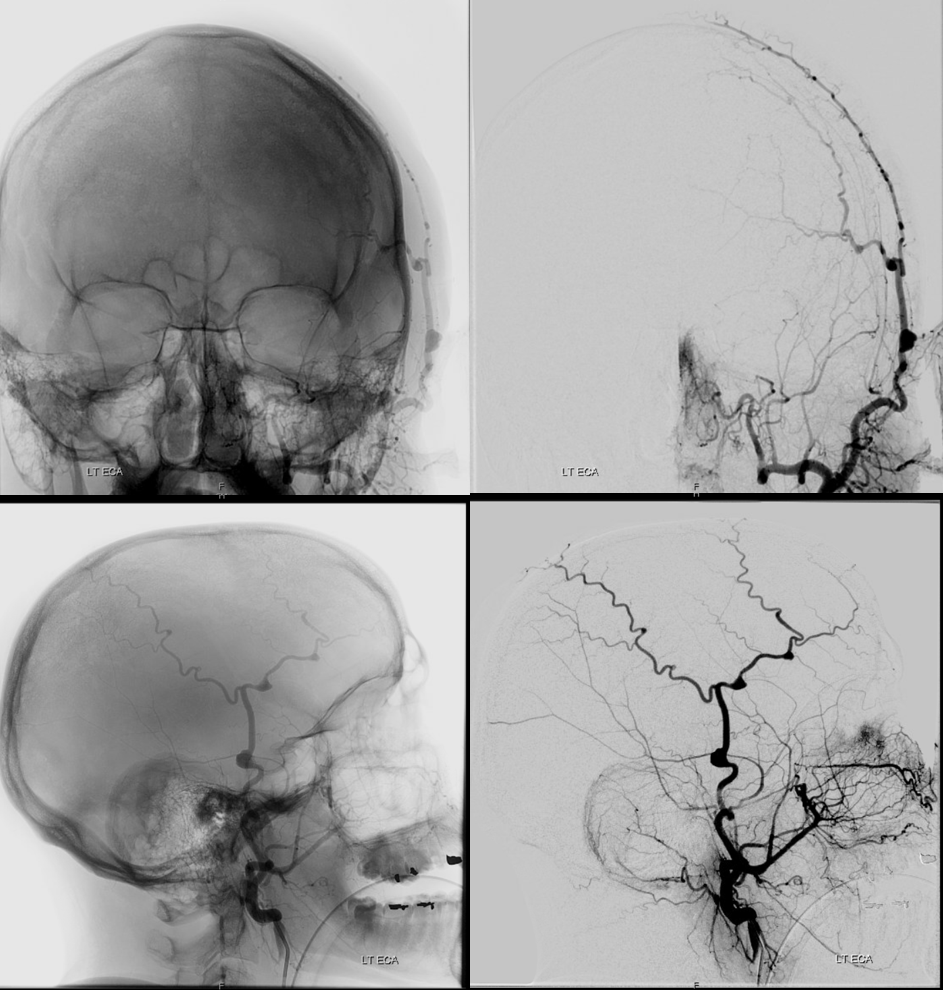
Here is a very dominant frontal branch — not so good for bypass huh… Even better seen when the troublesome MMA has been embolized (bottom row)
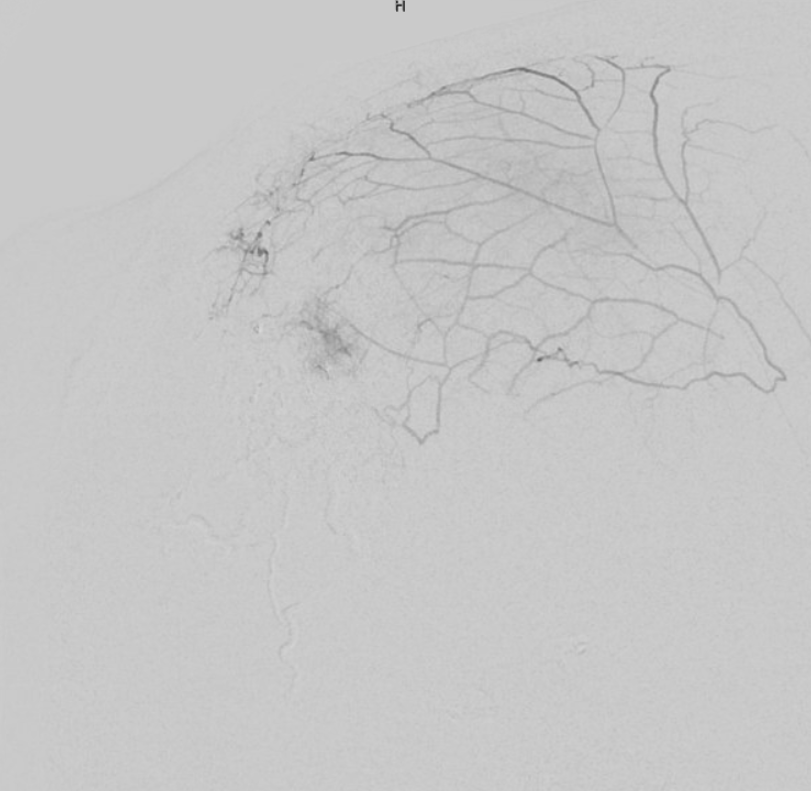
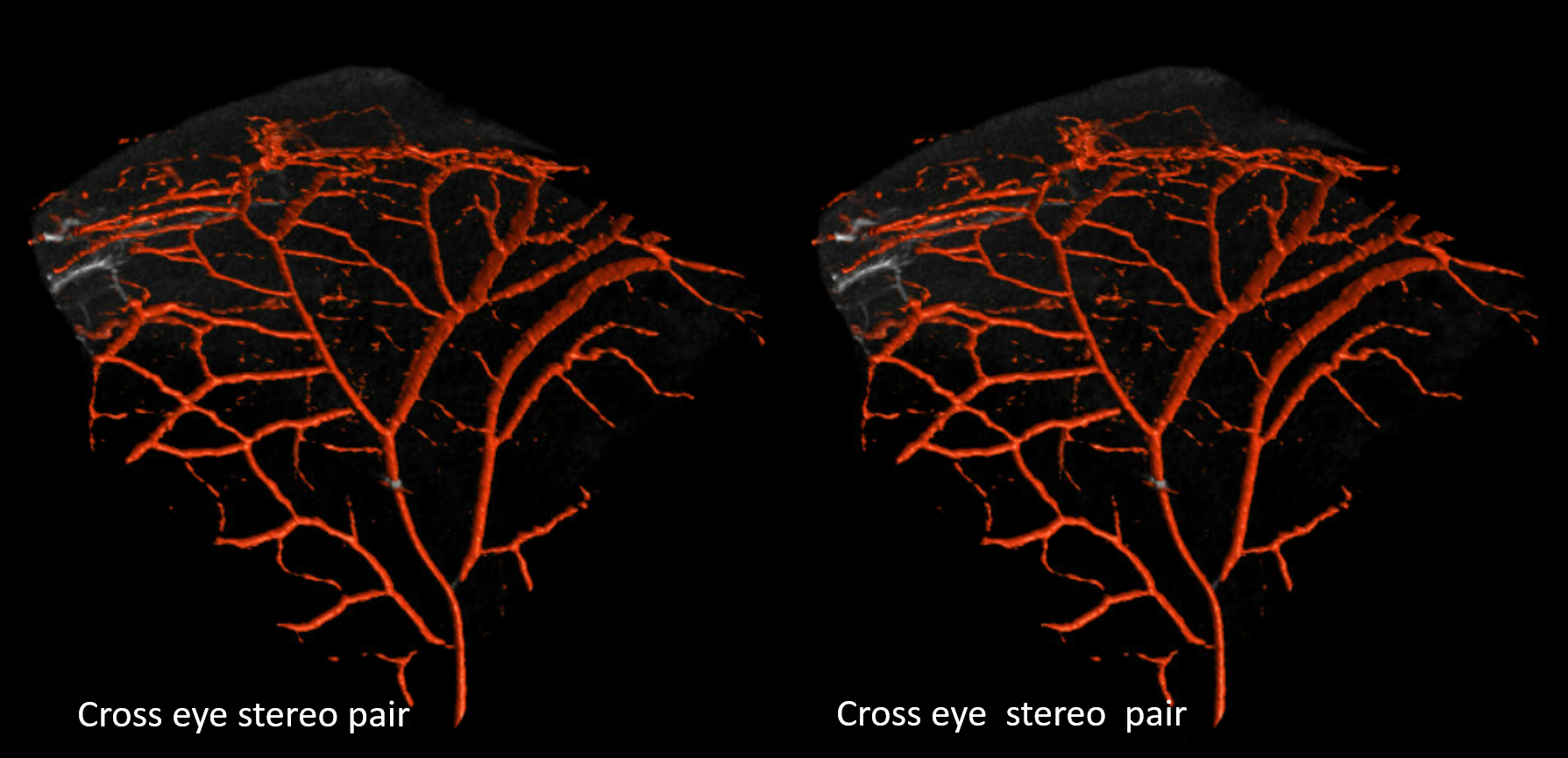
Another bunch of dominant frontal branches — anything is possible basically, and nobody is surprised when it’s the STA. Why then treat the endless MCA or any other vessel variations differently?
STA Aneurysm
Pretty easy to mangle the STA if skull keeps taking hits. STA dissections especially in blunt side of head trauma are not so rare. Of course, hardly anyone looks for them, and clinical significance is minimal (big ones can be felt, like the ones below). Its just like any vessel, and given the hopefully hard surface underneath, traumatic injury happens. No good for no bypass neither.
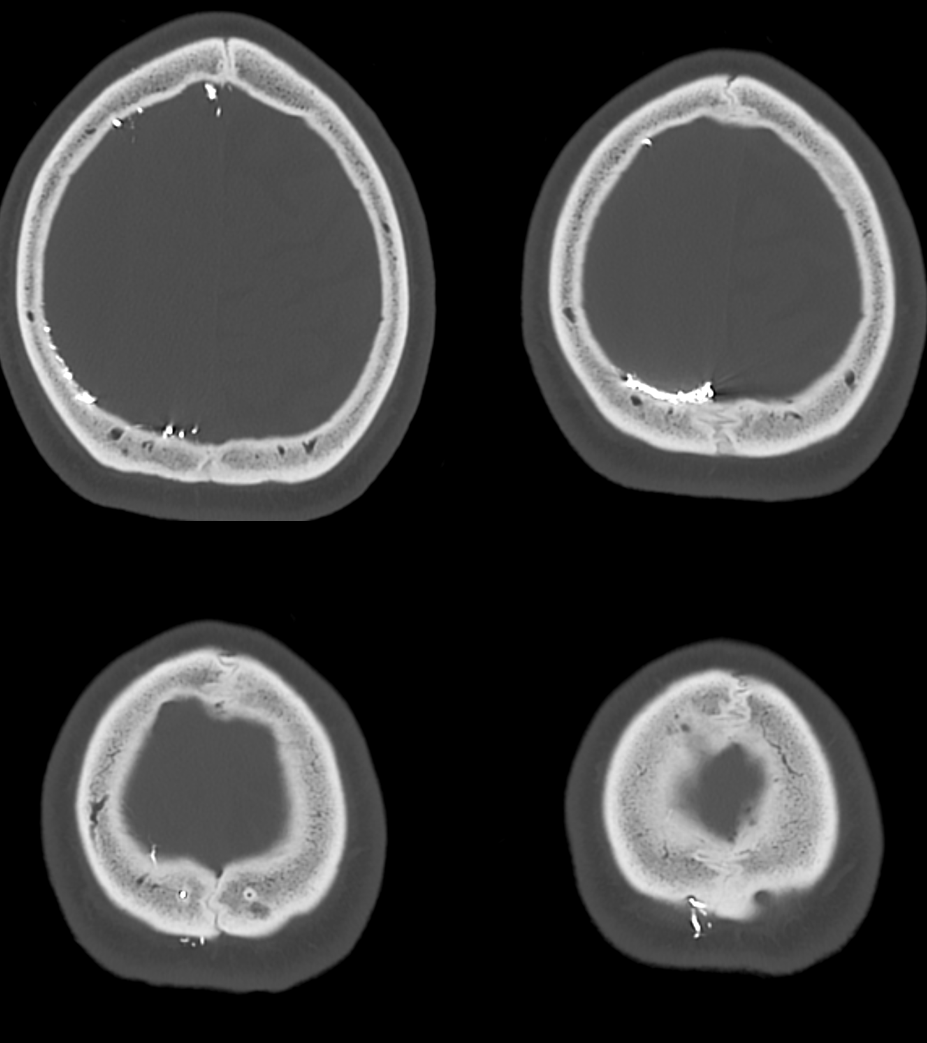
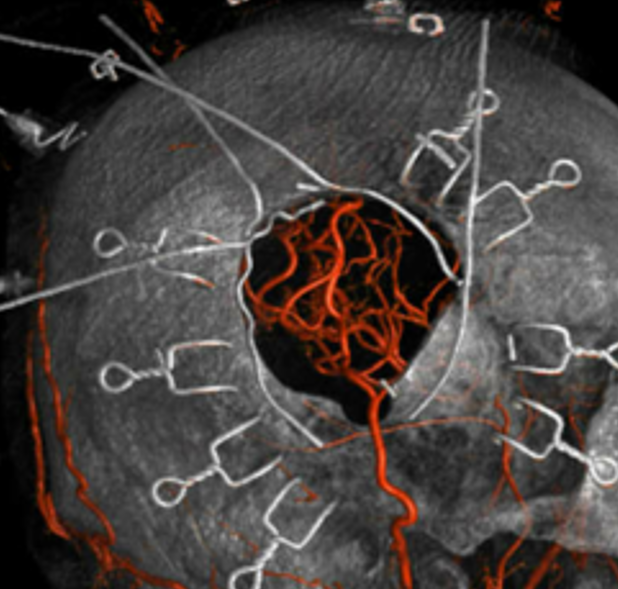
Supply of the skull
What vessels feed the skull? The ones next to it — meningeal ones below, and superficial ones (occipital, STA, supraorbital, supratrochlear, deep temporal). Its a balance of course. Frequently the STA can be involved when mets or other lesions destroy the skull. Here is a particularly exetnsive example of a renal cell metastasis
Meningeal supply is minor here
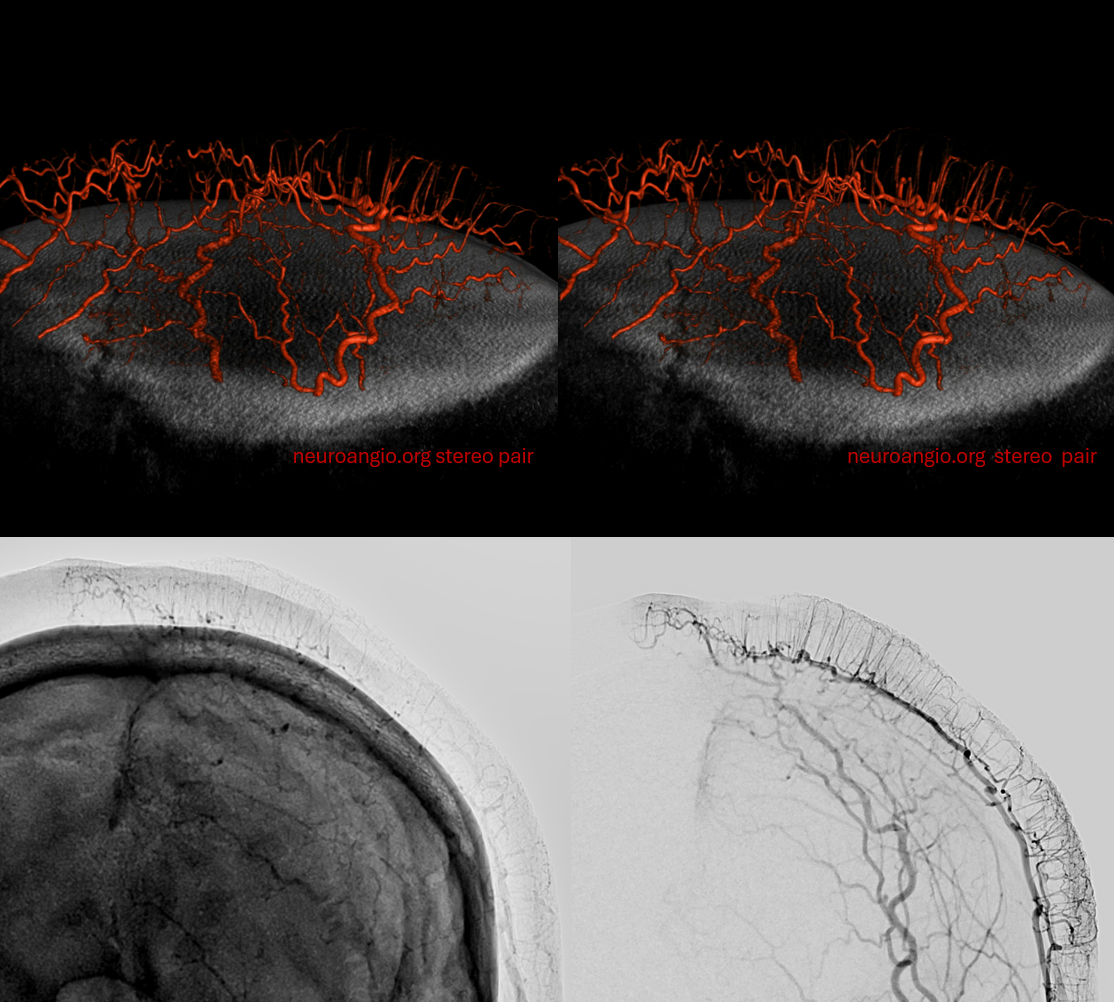
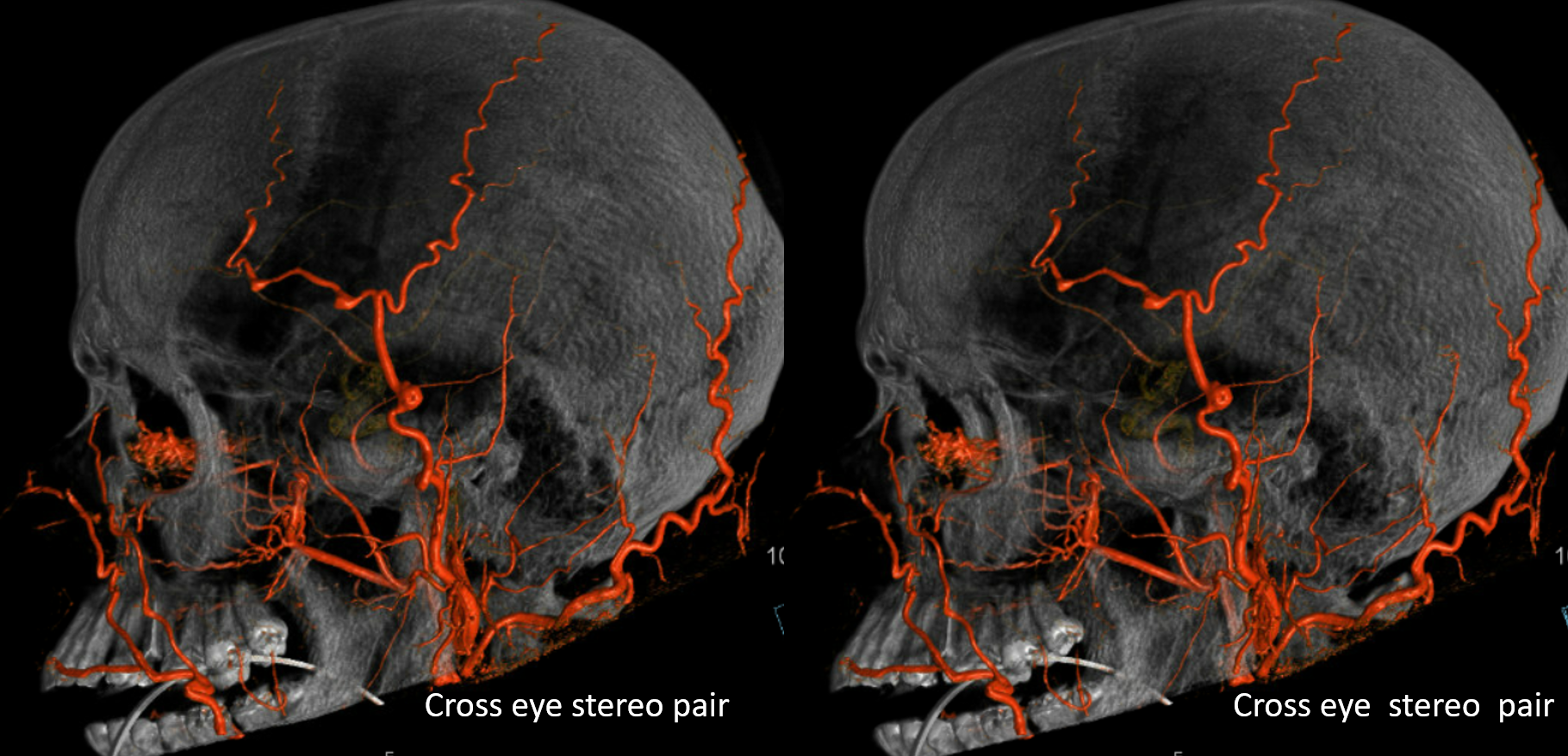
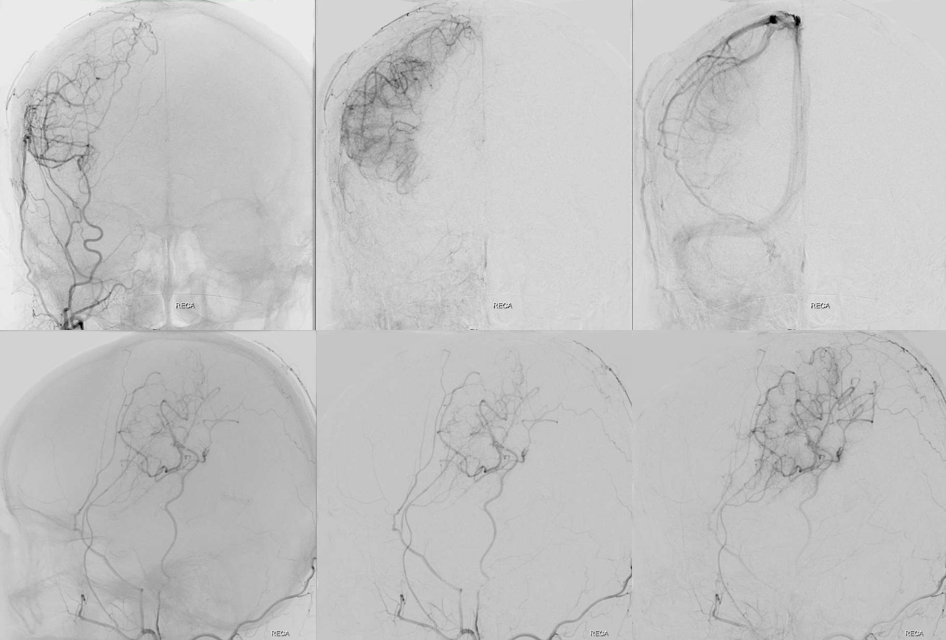
STA-Occipital-Meningeal Anastomoses
Same idea as skull supply — these are all connected. Often there is one hole in the parietal skull in particular where MMA connects to either STA or occipital. Clinical significance is that STA and occipital can reconstitute the MMA and perhaps make MMA embo for example less effective. See example here of significant occipital supply of meninges during MMA embo.
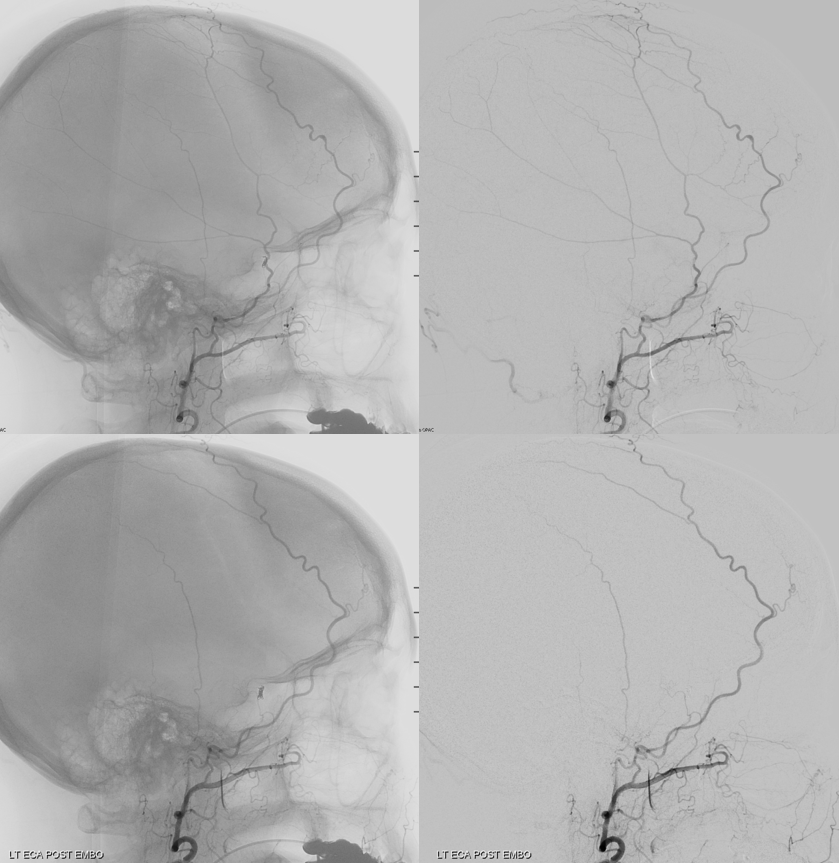
Below is an example of a permanent record of such connection, as shown by Onyx cast injected into MMA, extending through this particular parietal hole into the subcutaneous STA. The mirror image hole on the left remains functional. Notice that some Onyx also spilled into meningeal veins (upper right image) as it tends to do, more often than is acknowledged.
EC-IC Bypass
One of our areas of excellence (cranial bypass program) under leadership of Dr. Erez Nossek. Lots to talk about. Basically, the usual scenario is an STA to MCA bypass. Needs a “good” STA — best one that overlies area of targeted anastomosis. Can be done with expert hands down to something like 0.8 mm STA diameter.
Some examples — intraoperative angiogram successful anastomosis
A “good” STA — needs unsubtracted and common images though 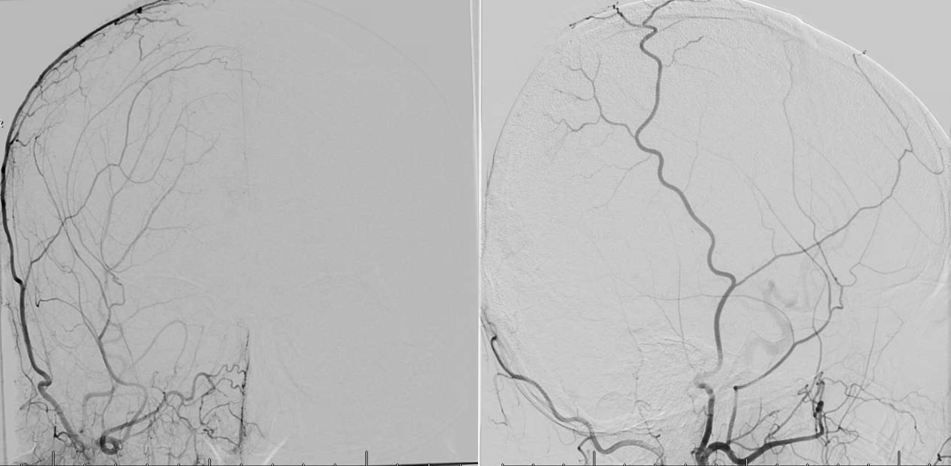
Delayed post successful STA To MCA bypass angio
Failure of “indirect” bypass — the STA is tunneled under the scalp flap. In many adults, indirect bypass is, well…
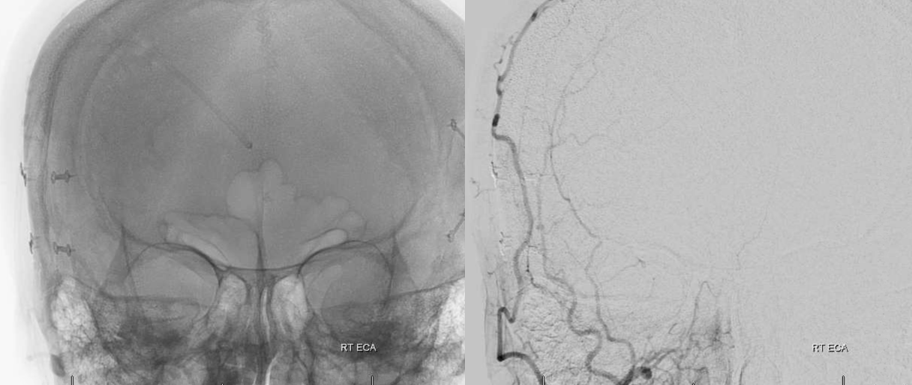
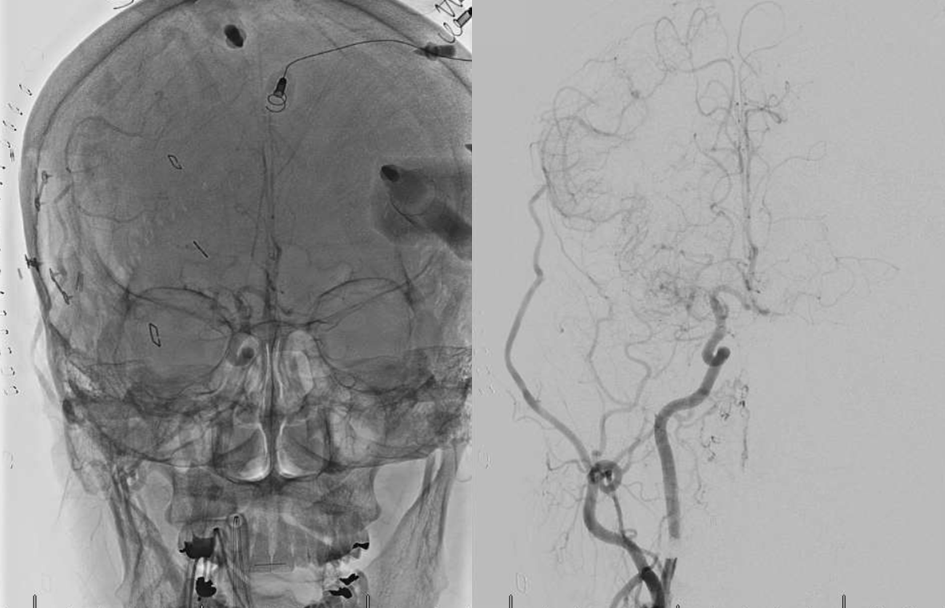
ICA reconstitution via Ophthalmic Artery
The most efficient by far ECA to ICA cervical carotid reconstitution is via the Ophthalmic Artery. Tons of possibilities — via MHT, anterior deep temporal, facial, ethmoid/anterior falcine, etc. Here, in case of proximal right ICA dissection, there is a really nicely seen STA to supraorbital anastomosis, and an anterior deep temporal to lacrimal branch also.
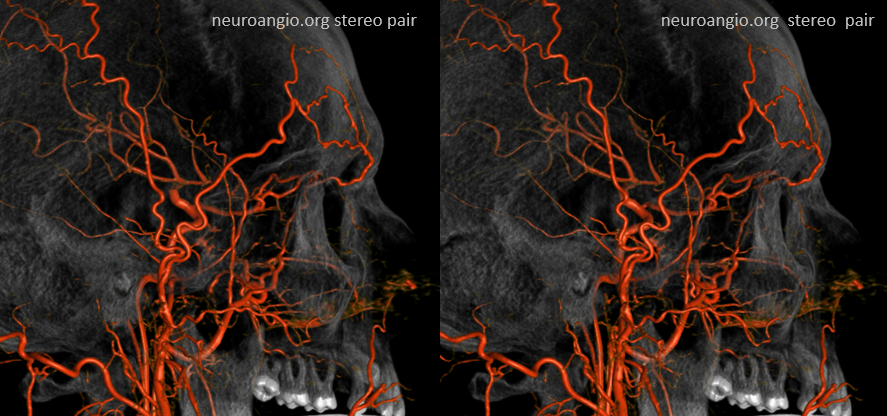
Can you see a myriad others on this MIP image?
Another example — multiple routes of ophthalmic artery reconstitution: superficial temporal via supraorbital artery (arrows), MMA (dashed arrows), infraorbital (open arrows), and facial/angular (ball arrows)
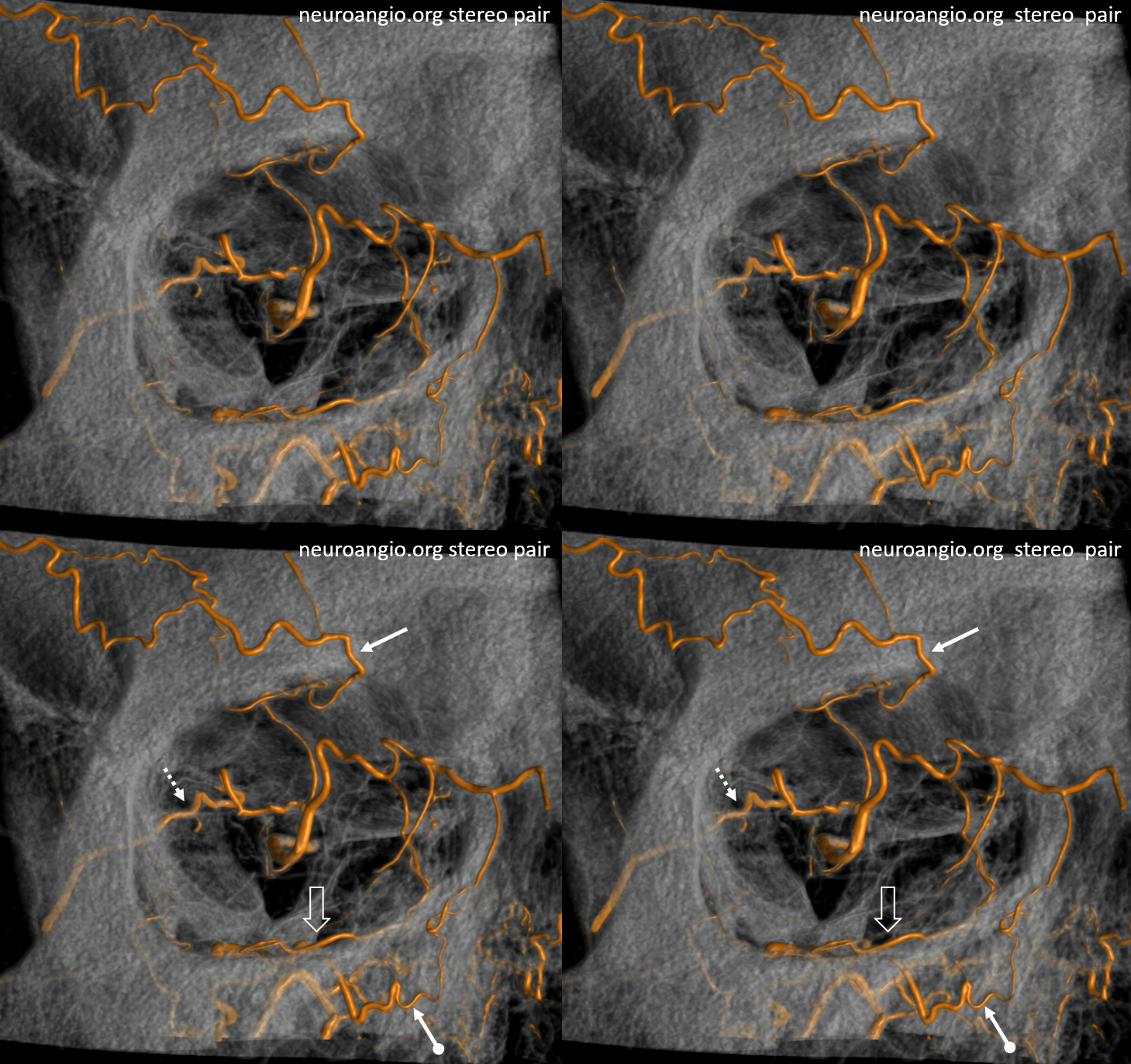
Especially well seen are superficial temporal and angular / nasal anastomoses.