With Erez Nossek, MD
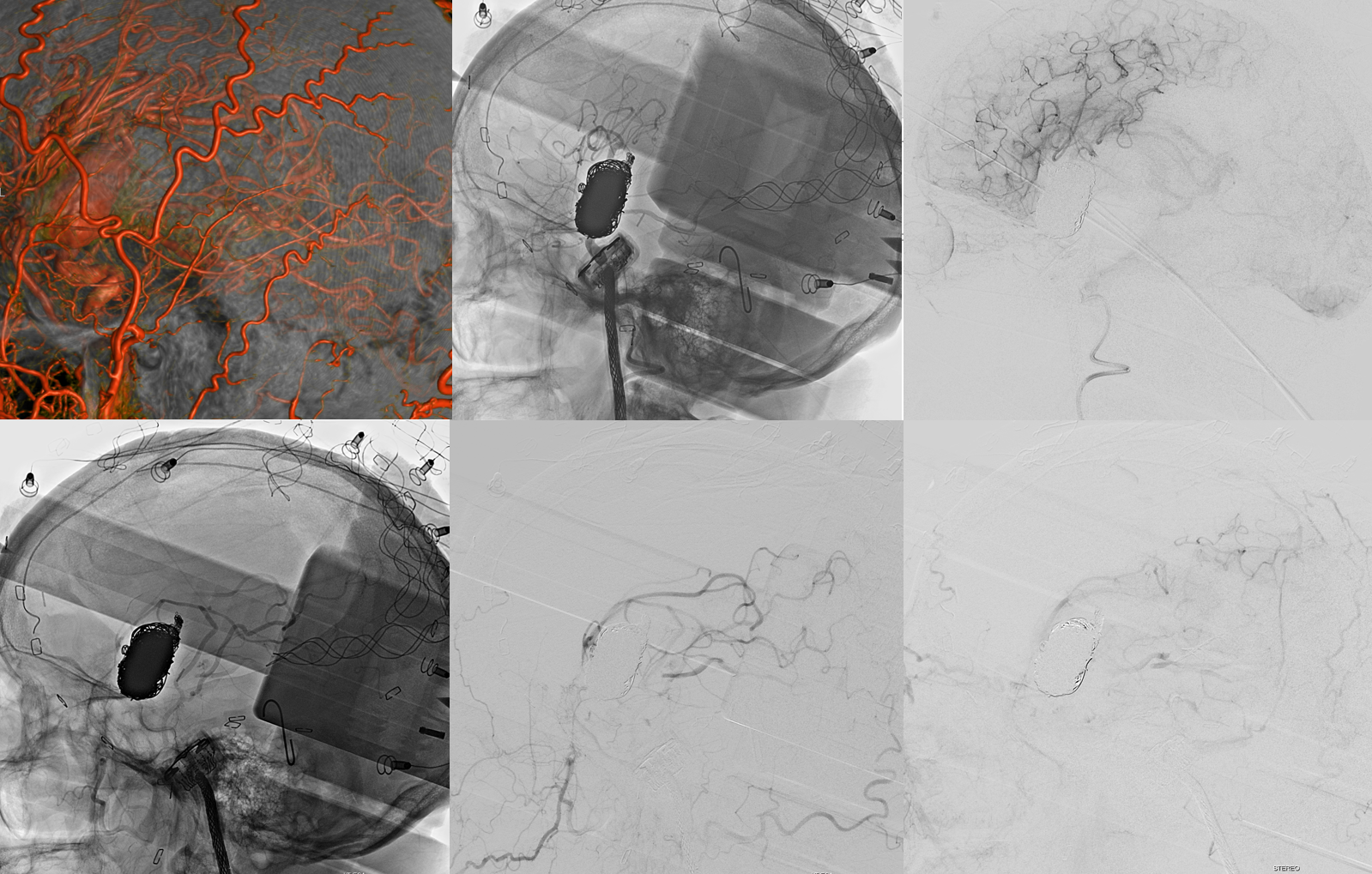
Presentation with SAH. NCHCT. CTA. “Cinematic Rendering”. FLAIR. SWI. T1 Post

DYNA — HR-CBCT. 8 sec DCT “micro DYNA” nonbinning. Injection 100% contrast 3cc/sec for 39 cc; 5 sec delay — to allow for filling and outflow. Extremely important — a too short delay will not allow one to see the outflow.
Secondary Reconstruction in “normal” mode. Note vessels apparently stretched over the aneurysm dome (arrows). These are vasa vasorum — vessels feeding the aneurysm wall. The wall of aneurysms such as this one has a life of its own. It is impossible to get rid of an aneurysm like this without closing these vasa vasorum.

DYNA movie secondary reconstruction
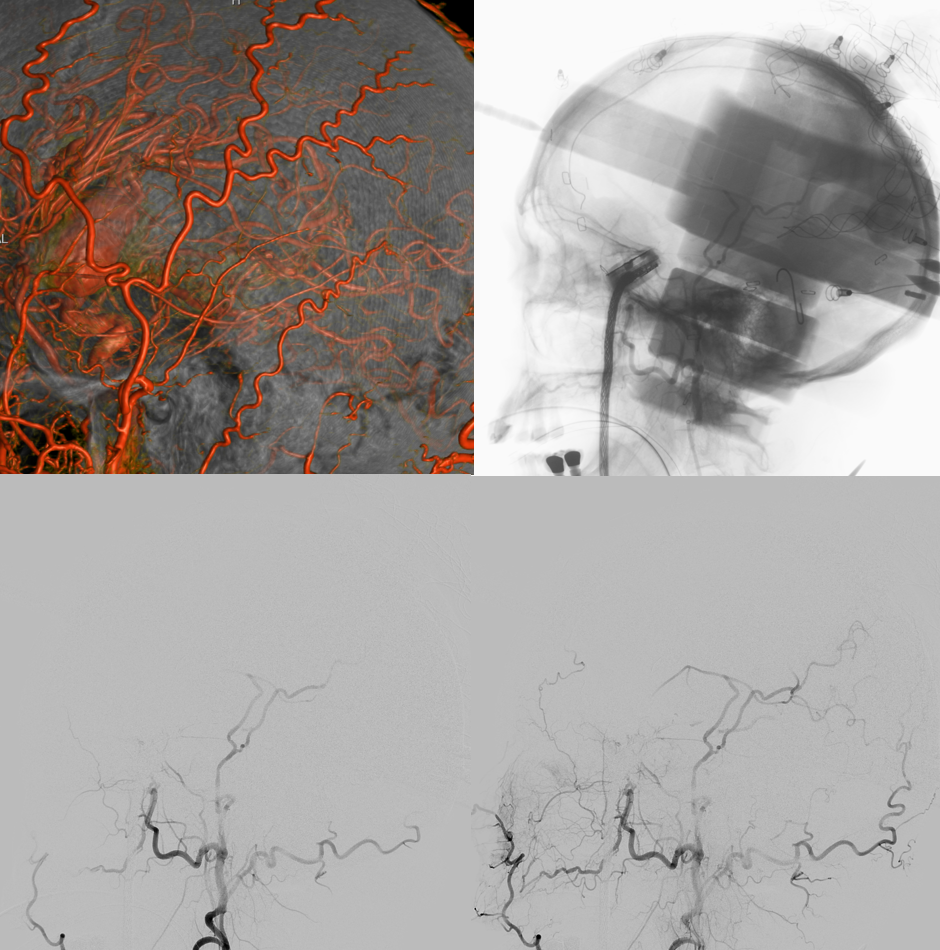
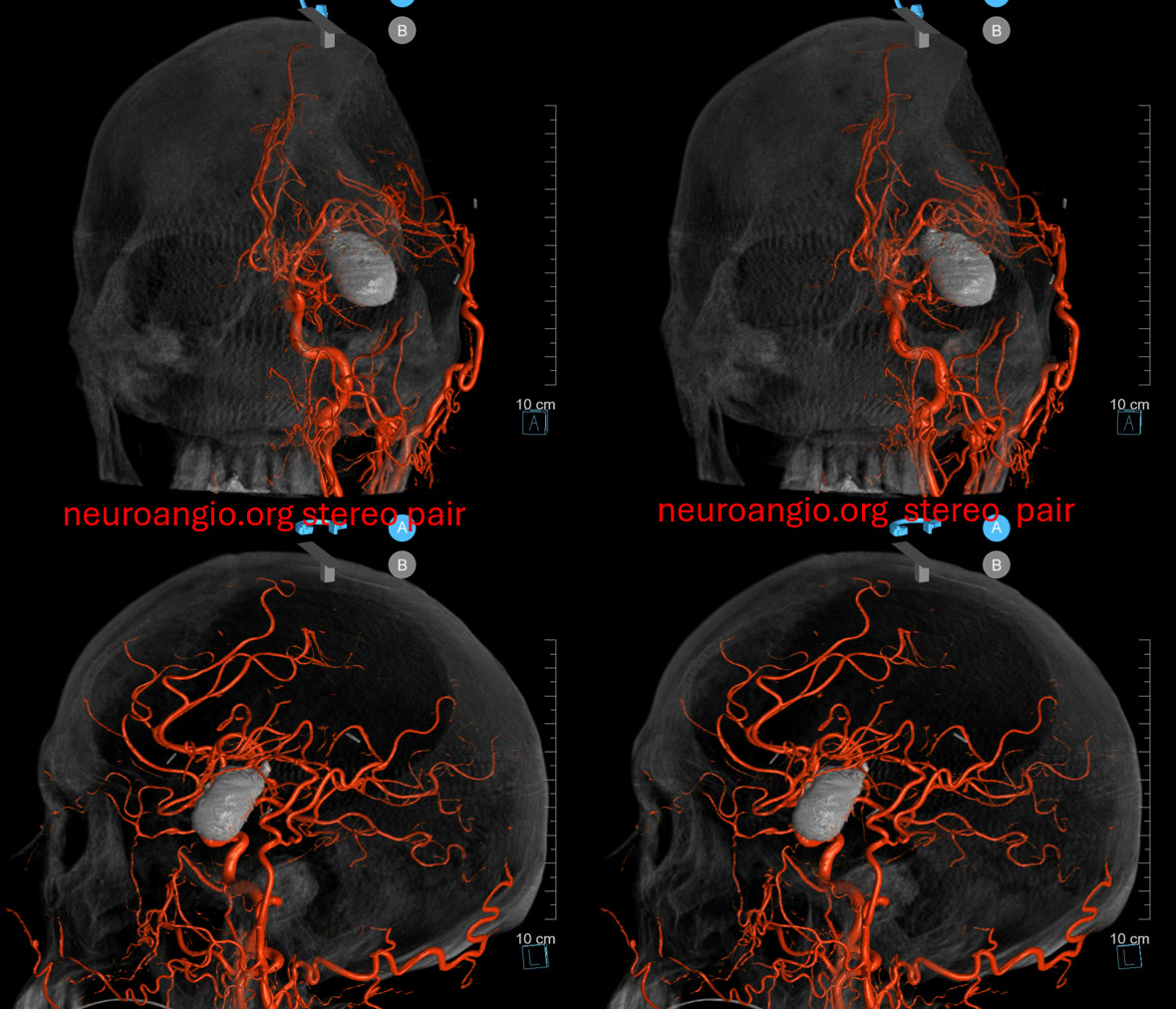
Volume rendered movie of the vasa vasorum
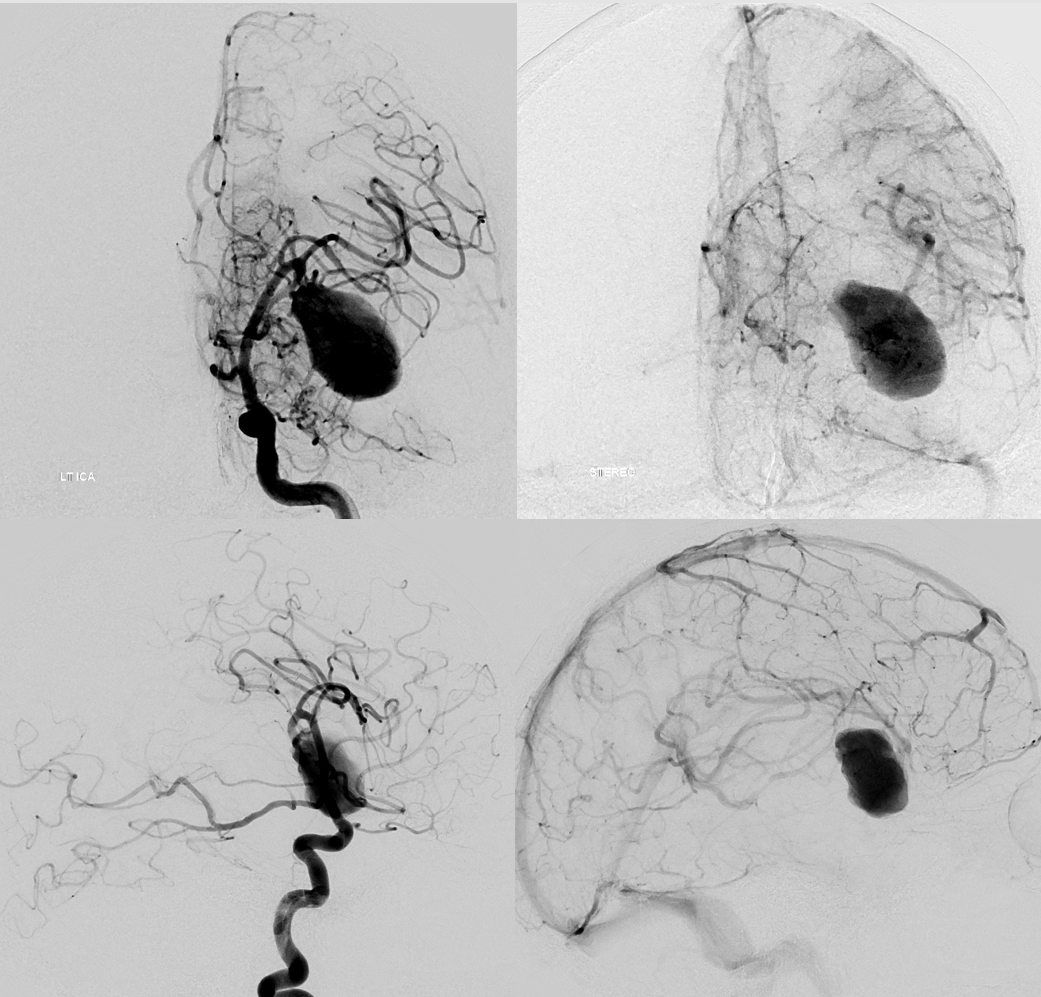
This is not an aneurysm likely to do well with flow diversion. Deconstructive if possible is best. It is often feasible just to close the aneurysm and the collaterals will be fine. We test with BTO of the inferior division. It is a failure in our opinion. We could chance it on the right, but too much to risk on the left.

The BTO is carried out with the Scepter C. You can inject the scepter to see if there is backflow from collaterals. Here, the injection allows one to definitively separate the vasa vasorum (arrow) from lenticulostriates — in case anyone doubts what they are

Planning for bypass. This is a 4 second DSA DCT “3D-DSA”. Injection 4 cc/sec for 36 ccs, 5 sec delay. The point is to see the STA and the overlying MCA target M4 vessels.
Its a double barrel bypass — two STA limbs, two recipient M4s
The open portion of the aneurysm is then coiled — taking care to extend coils proximal enough to cover the vasa vasorum
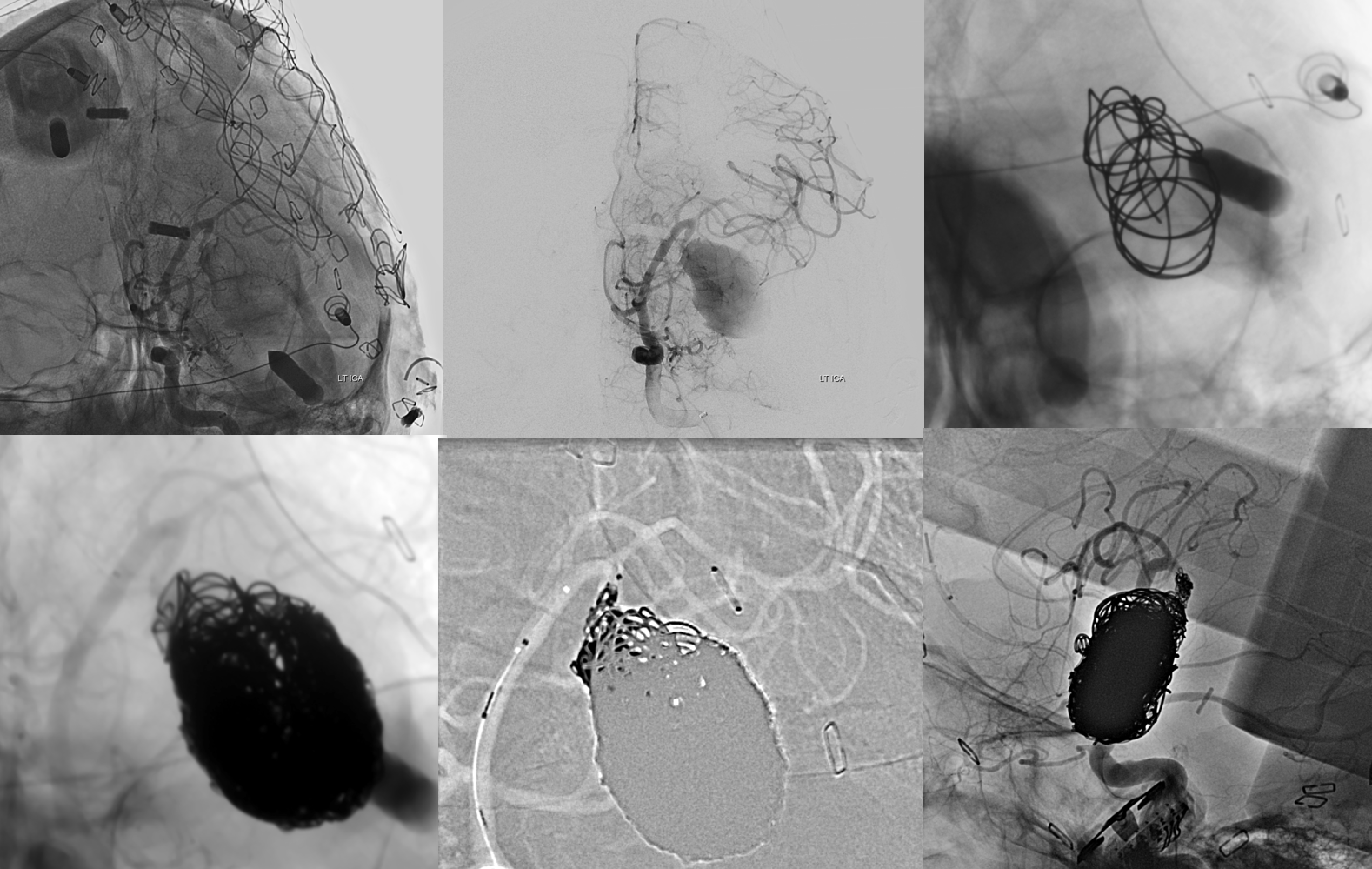
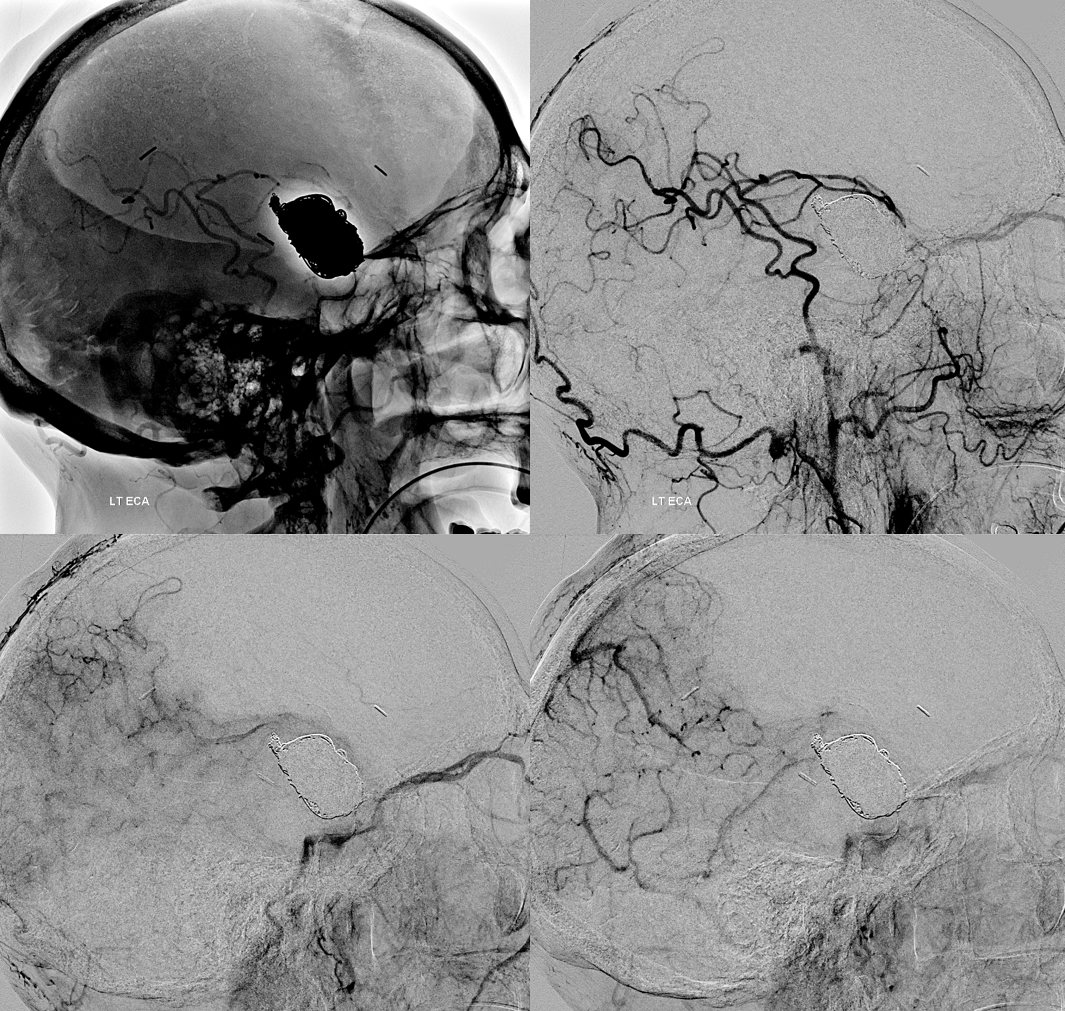
CCA pre-op (top left). Post bypass and coil ICA injection (tol mid and right). Post bypass and coil ECA injection (bottom row).
Coiling was followed by aneurysmorrhaphy — surgical opening of the aneurysm and debulking of the thrombosed portion until coils were encountered in several places. No bleeding.
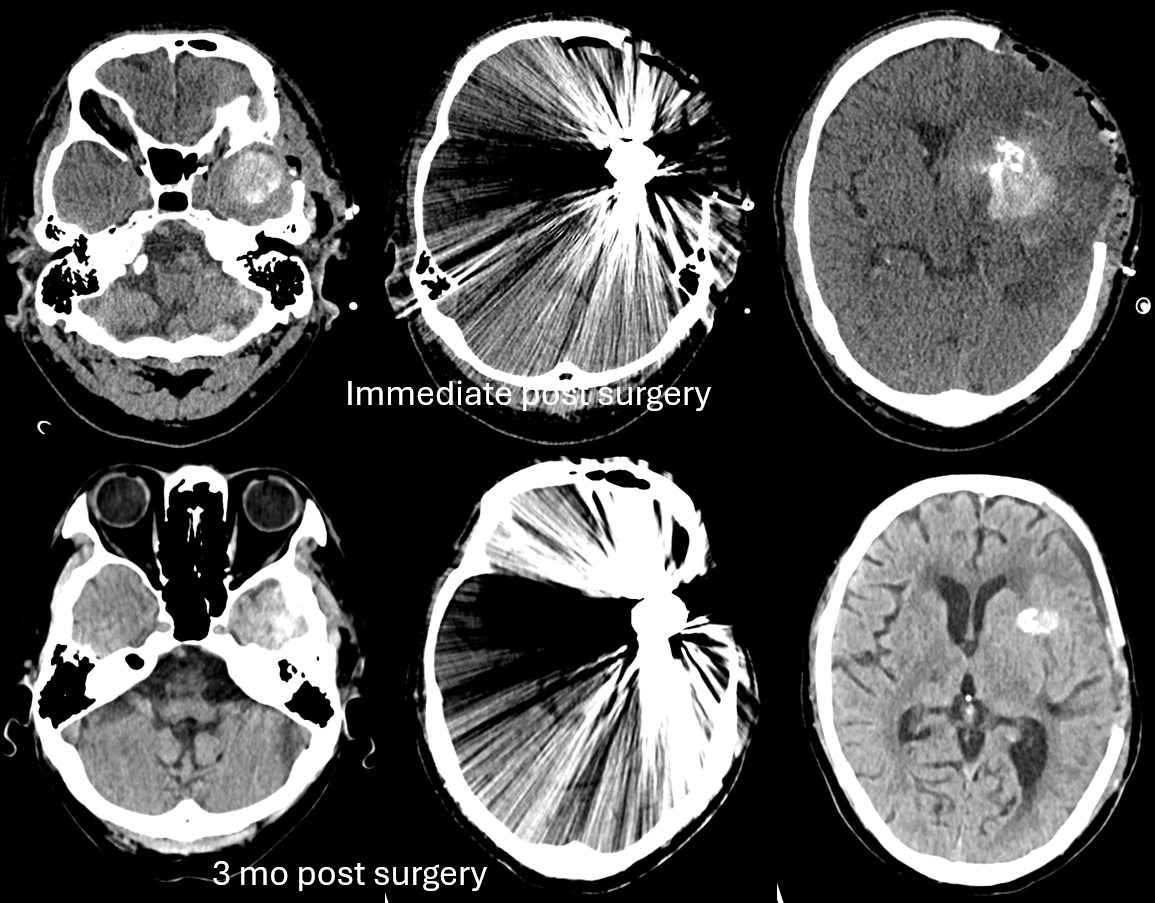
Two months later, before reconstructing craniectomy defect. Clinically doing excellent
ECA injection shows huge amount of brain supplied by the bypass
ICA
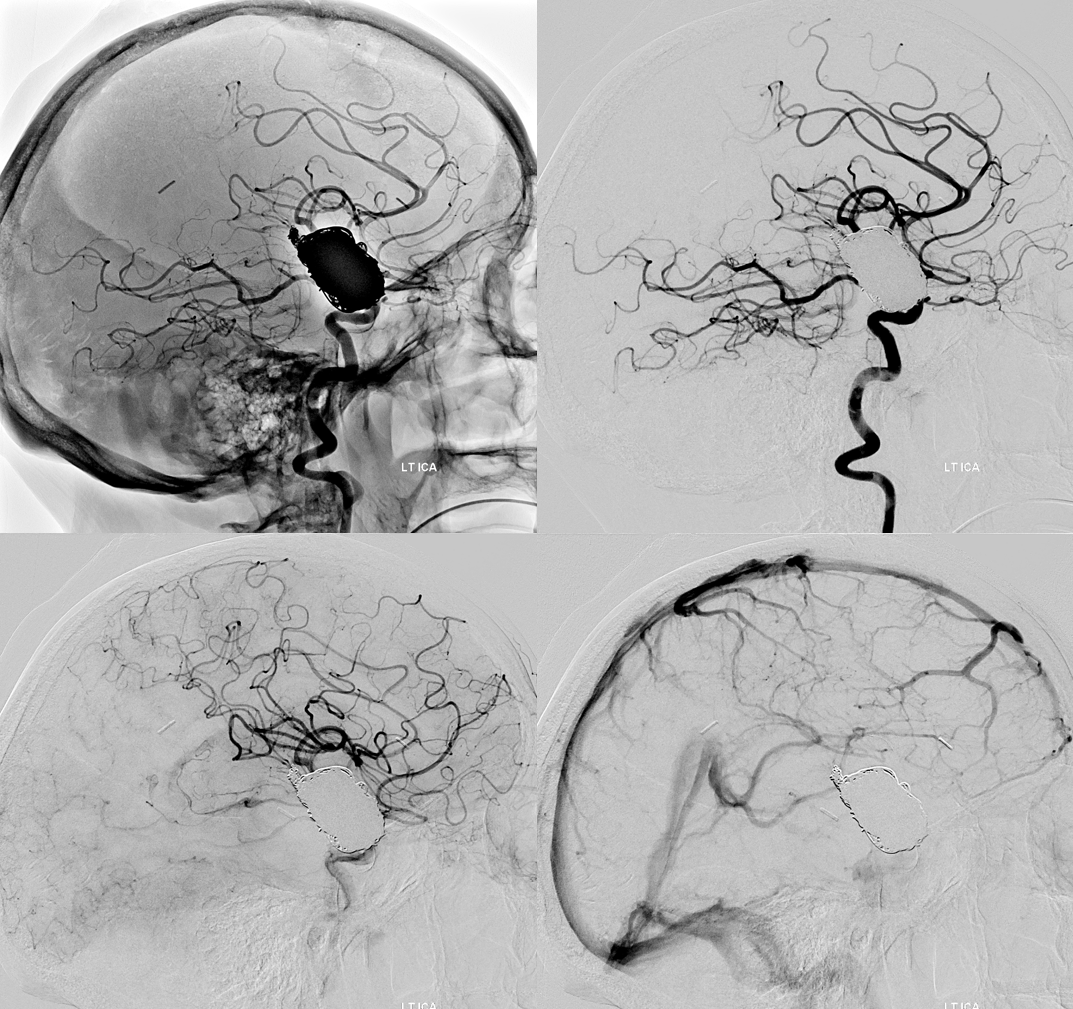
4sec DSA DCT
Movie
Post CTs