
Giant basilar presents with perforator occlusion:

Angio — left ICA. It takes about 2 seconds to fill this aneurysm completely from start of injection (not shown)
Angio dominant left vert frontal. This injection does not completely fill the aneurysm, and does not visualize the right vert. therefore, these settings would not be good for a “spin” — no 3D or DYNA or Vaso or whatever. The injection needs to be stronger or should be done bilaterally.
Lateral view
Hypoplastic (or smaller) right vert injection. Must be done to understand PICA and perforators between PICA and the VB junction. You can see there are many even on 2D – -because the AICA is dominant and there is a small PICA, so expect intradural perforators.
Now, notice that there is a PCOM on left ICA injection. Thats unusual for this aneurysm. There is also a small one on the right. So, we will do DYNA and then Balloon Test Occlusion of both verts.
Below are videos of the dynas — they are all together here in 1 video — just a pain to separate them, that’s how they now come to our PACs..
First spin is of the hypoplastic right vert. There is no expectation to fill the aneurysm well, so we are doing it for right vert perforators.
Protocol — Siemens ICONO 7 second DCT (single spin) 22 cm FOV “micro” unbinned. Rate = 2 cc/second, 2 second delay, undiluted contrast (total =2×9 = 27 cc contrast)
Second spin is the left ICA. Protocol — Siemens ICONO 7 second DCT (single spin) 22 cm FOV “micro” unbinned. Rate = 3 cc/second, 3 second delay, undiluted contrast. (So total of 3 cc/sec x 10 sec = 30 cc contrast)
Third spin is the most important one — left vert. With longer delay and stronger injection we can hope to fill the aneurysm completely and reflux (retrogradely opacify) the right vert. Some are nervous about this in terms of aneurysm pressurization. If you are nervous, do bilateral vert injections — one injector, one manual.
Protocol — Siemens ICONO 7 second DCT (single spin) 22 cm FOV “micro” unbinned. Rate = 3.5 cc/second, 3 second delay, undiluted contrast — therefore total contrast dose is 3.5cc/sec x 10 sec = 35 ccs.
Note excellent reflux into the right vert throughout the entire injection — that’s important. Visualizing the structure half the time is not good — will be a ton of streak artifact. So longer delay is better as in here.
Below are reconstructions
Left ICA
Left vert
Secondary reconstruction of the left vert injection in “sharp” mode and smaller FOV
Right vert DYNA reconstruction. Notice how many perforators there are from the distal intradural vert. Sacrifice here would be a big mistake
Although there is excellent reflux into the right vert, we can still do a fusion like this of the two verts — for kicks
Fusion MIPs axial
Coronal fusion MIPs
Fusion left ICA and left vert
Now for the BTO — need 3 access points — two femoral one radial. Block 2 verts (essential) and inject ICAs sequentially

BTO
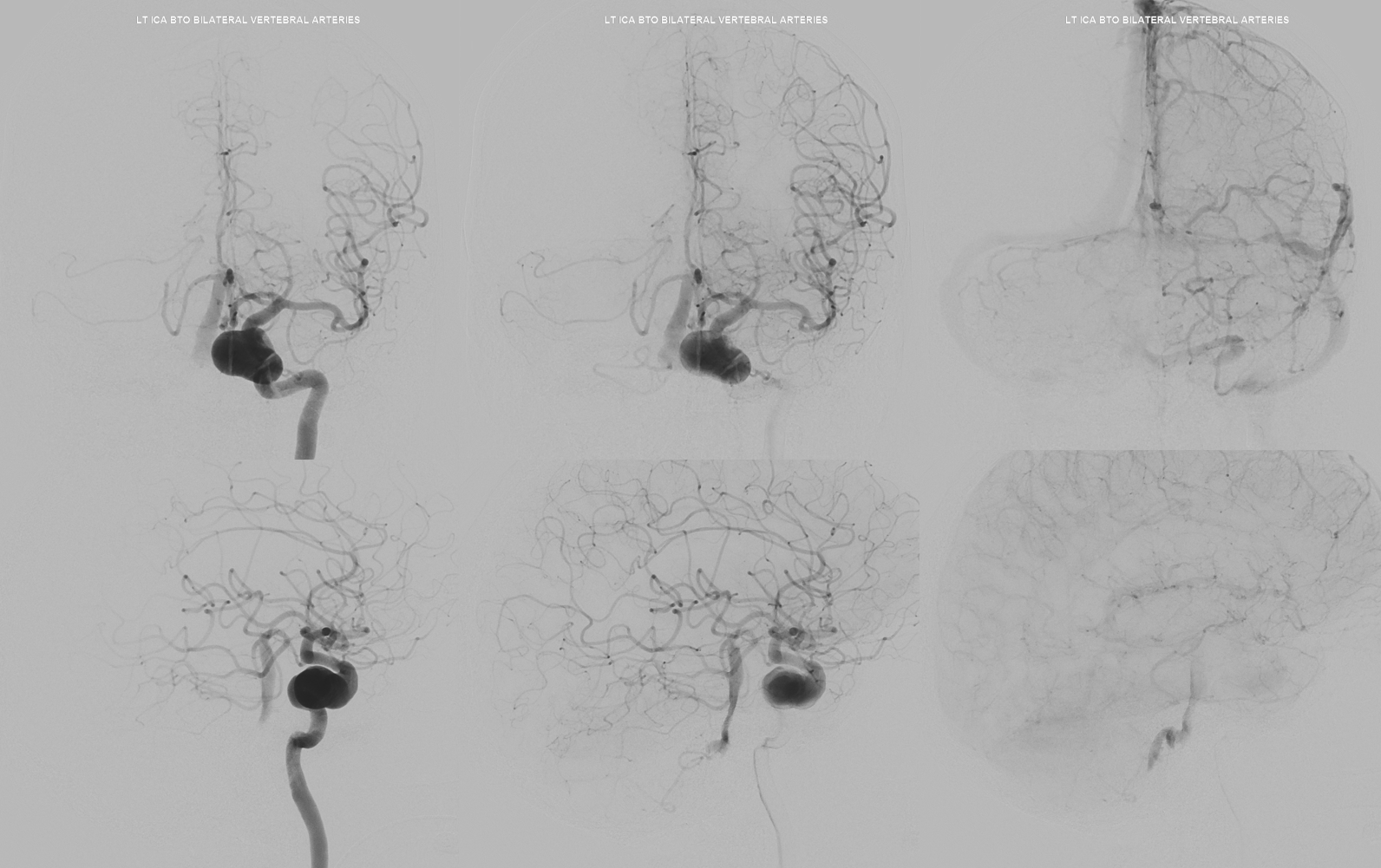
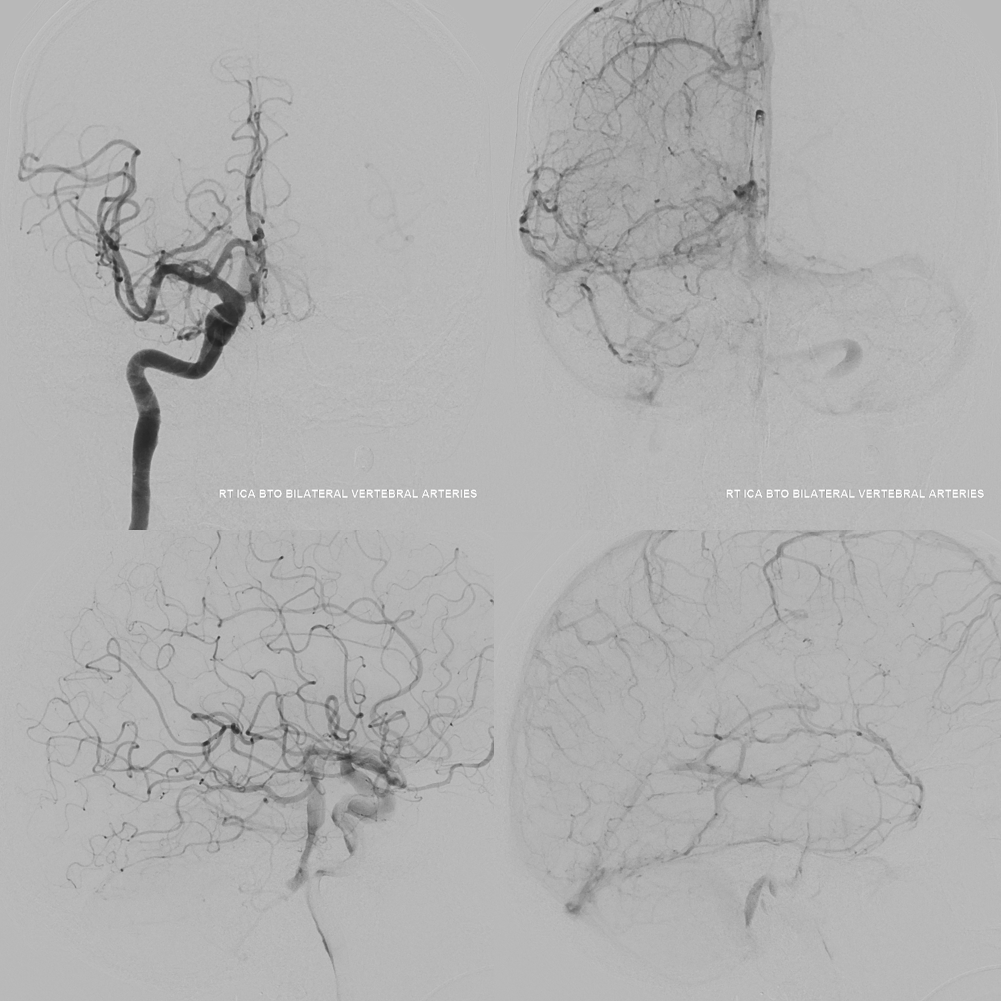
Treatment – not for show… This is about diagnosis and workup. Without a good angio and BTO like this, the angio is worthless and CTA or MRA are in fact of better value…