
A well-known association between pulsatile tinnitus and intracranial hypertension is now established. Most patients with significant IH have at least sigmoid sinus stenosis. The chicken/egg question of what begets what remains unsolved. Does high CSF pressure collapse the sinus? Or does venous outflow obstruction due to sinus stenosis lead to increased CSF pressure? Those who believe stenosis to be a secondary phenomenon point to well-documented cases where previously narrowed sinus becomes fully patent after lumbar puncture or ventricular shunting. They also argue that recurrence of IH after venous sinus stenting, which is usually associated with narrowing of the sinus just outside the stent, speaks to continued external pressure. On the other hand, believers in venous stenosis being the primary pathology argue that other conditions which lead to increased intracranial pressure (mass lesions, subarachnoid hemorrhage, trauma, etc) do not lead to venous sinus stenosis. They are undeterred by observation that there are many other ways for venous blood to leave the head — cavernous sinus and emissary skull foramena, for example.
Who is right? I believe both points of view are valid. This case shows persistence of severe venous sinus stenosis despite prior placement of a programmable ventriculoperitoneal shunt. The shunt works — headaches and papilledema resolve and shunt pressure is, if anything, on the low side. However, severe and disabling pulsatile tinnitus persists on the right side, with severe sigmoid stenosis. So, clearly in this case the stenosis was not a result of IH, since intracranial pressure is now normal or even low. However, a companion case (click here) shows a situation where IH symptoms of headache and vision issues recurred about 18 months after stenting of venous sinus stenosis. The only symptom that never recurred was pulsatile tinnitus. It is one thing we have learned from experience — IH may come back after stenting, but PT does not.
I believe that the etiology of iH is not understood, and that subtypes of IH patholgenesis may exist — in some venous stenosis is primary, and in others secondary phenomenon.
Here is the case. Programmable shunt is in place

Severe persistent venous sinus stenosis
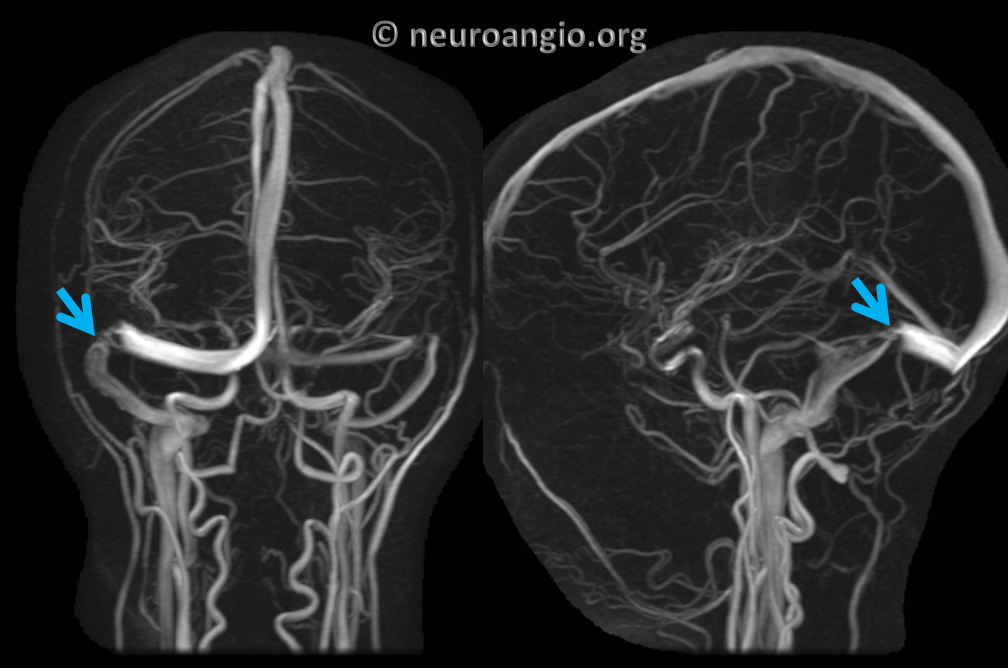
Angio
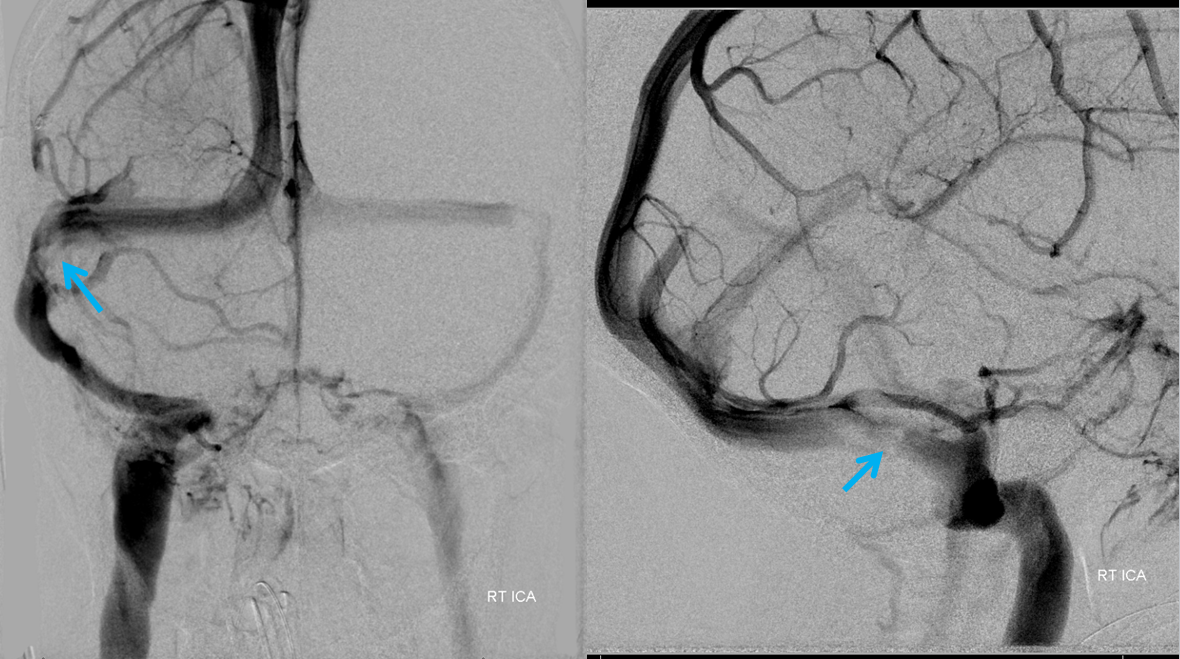
Vert injection

Venogram

Post-stent

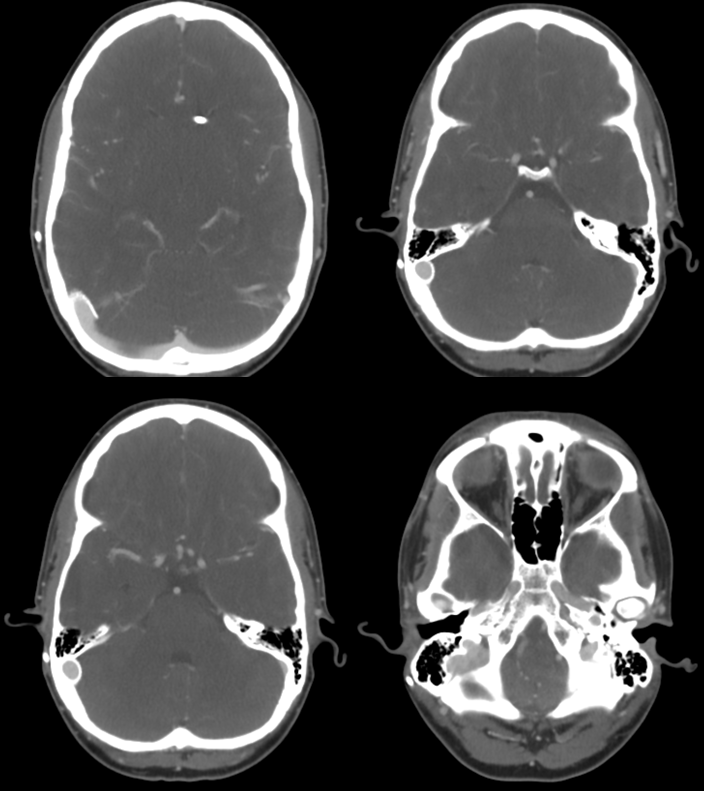
CTA follow up 1 year later. Full stent patency. No more PT
Back to Diagnosis and Treatment of Pulsatile Tinnitus