
Though we will not take up the subject of whether or when one should do vertebral augmentation (I believe we should, and perhaps more often than we do generally), it is always important to make sure that a job is done well. Homeopathic cement injections are no different from sham procedures in randomized studies (same goes for undercoiled aneurysms, for example). Of course, better is the enemy of good — but only when “good” has been achieved.
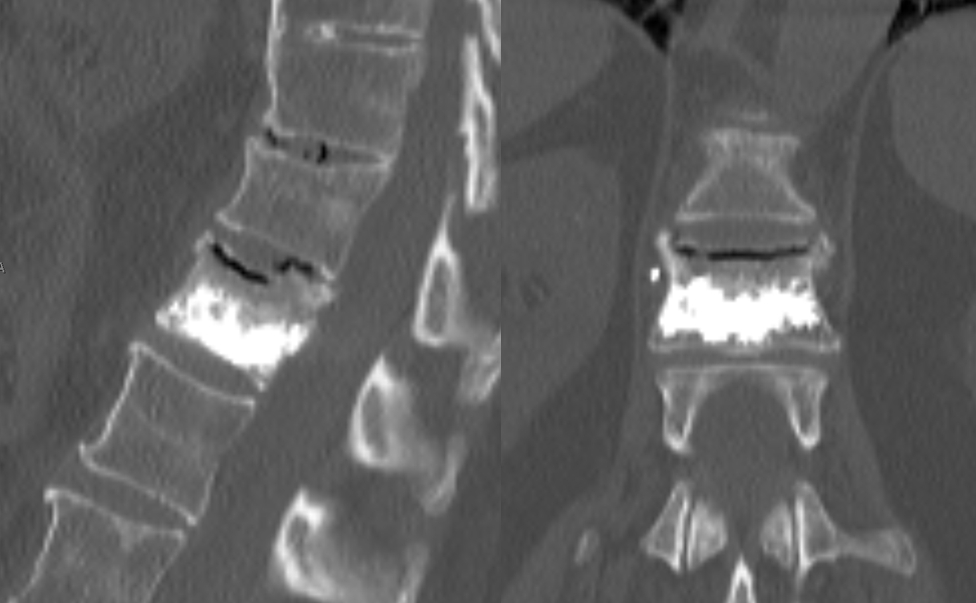
This ninety-plus patient, who bikes and swims daily at the gym, can not get out of bed for 3 days due to horrific pain. CT shows L2 inferior endplate fracture(white arrows). Notice typical expansion of disk space due to vertebral collapse, frequently to be filled with gas.

Not easy to appreciate this fracture on still shots

The cannulas are directed towards the middle of the body

Balloons inflate well enough to reach the inferior endplate

Seems like a decent enough cement fill, extending all the way posterior to the dorsal vertebral vein (not marked, see spinal venous anatomy)

Actually, leaving it like this accomplishes very little from the mechanistic standpoint, in my opinion. The fracture has not been filled. The solution is to re-access the inferior body, tapping in the cannula fully anterior (white), and injecting cement, which now nicely fills the fracture line on the left side (black arrows)

Still, not yet time to stop. The same is done on the right

In the end, the fracture line is well-filled, and we are confident that internal fixation has been achieved

The patient is doing very well. To the argument that re-access would increase the incidence of complication, I would answer that with it should be no different than primary access, while doing a suboptimal job is in fact harmful because it exposes the patient to procedural risks without real benefit. The purpose here is to show both approach and technique for the interested reader.
Case 2 — another illustration of same idea. Patient treated at outside institution with persistent pain. Fracture is not filled with cement. There is also a new superior endplate fracture of the upper level
re-treatment


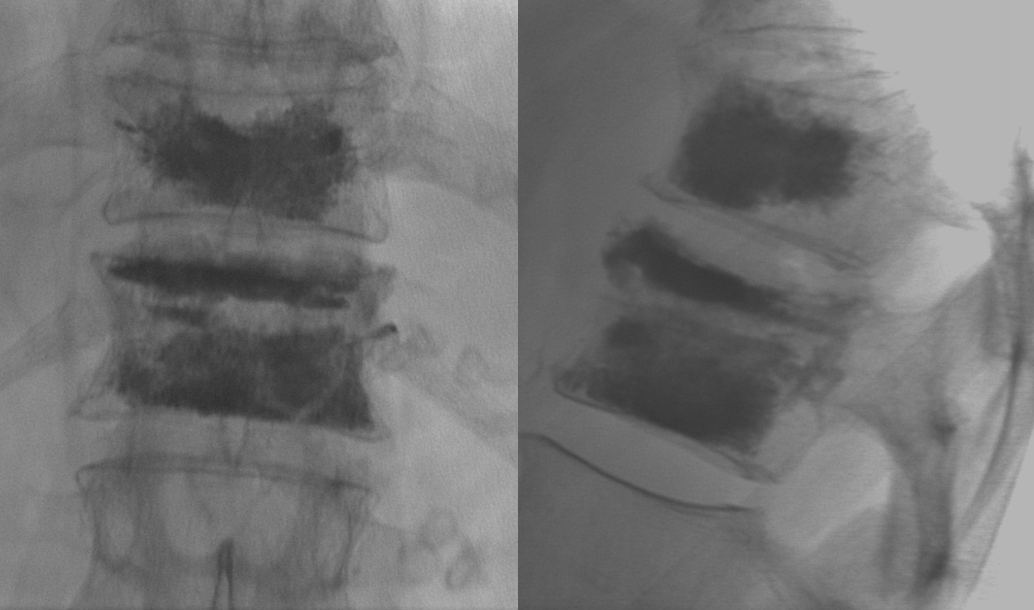
Same idea — pay attention to fracture lines