
The fundamental distinction between brain parenchymal AVMs and dural-based AVFs is two separate disease entities is one of our firm beliefs. Of course, piodural anastomoses exist in various conditions — in steno-occlusive disease such as moya-moya dural support of the parenchyma is very common for example. The reverse — pial supply of dural hypervascular states such as dural fistula is also common. Up to 15% of AVMs have some dural supply — presumably because of AVM flow demand — not because they are intrinsically one and the same disease state.
However, there are exceptions to all rules, and these are extremely instructive. A small but well-recognized number of “shunts” seem to consist of distinct parenchymal AVM and dural AVF components. They are united by the common recepient vein — an extremely intriguing situation. It is also a way to see how important Cone Beam CT is to understanding these complex shunts
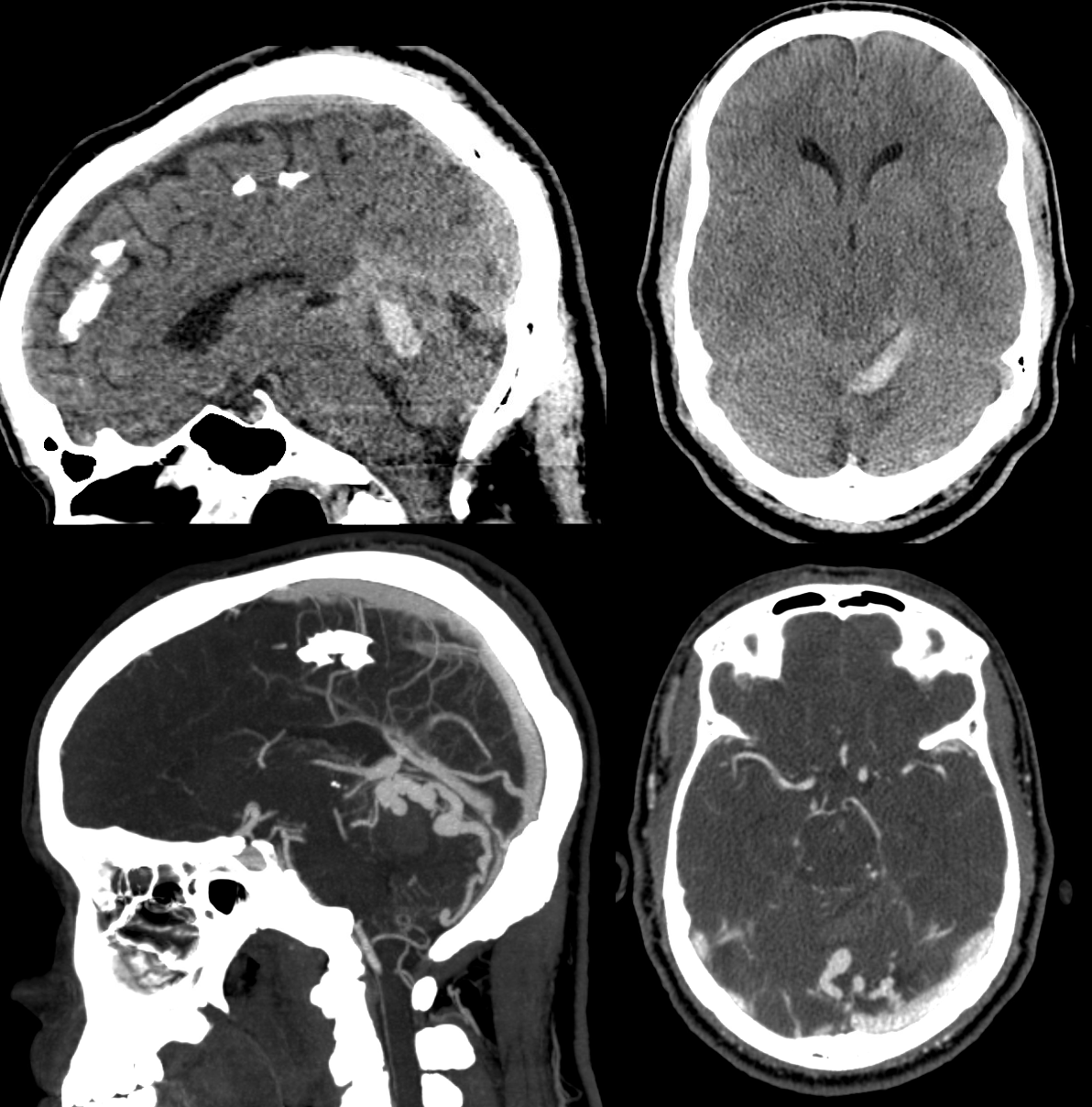
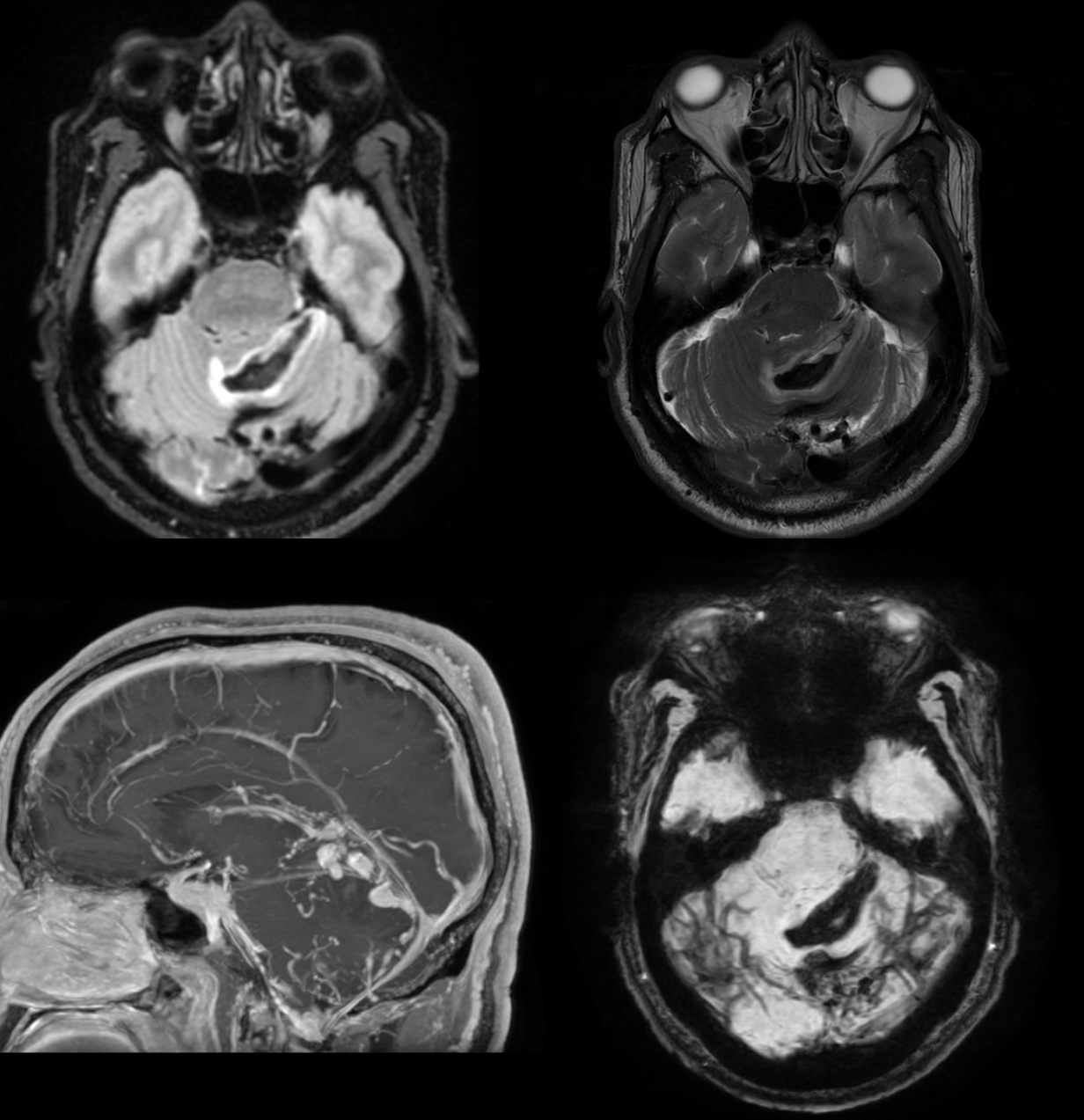
Presentation with gait ataxia
Dural components
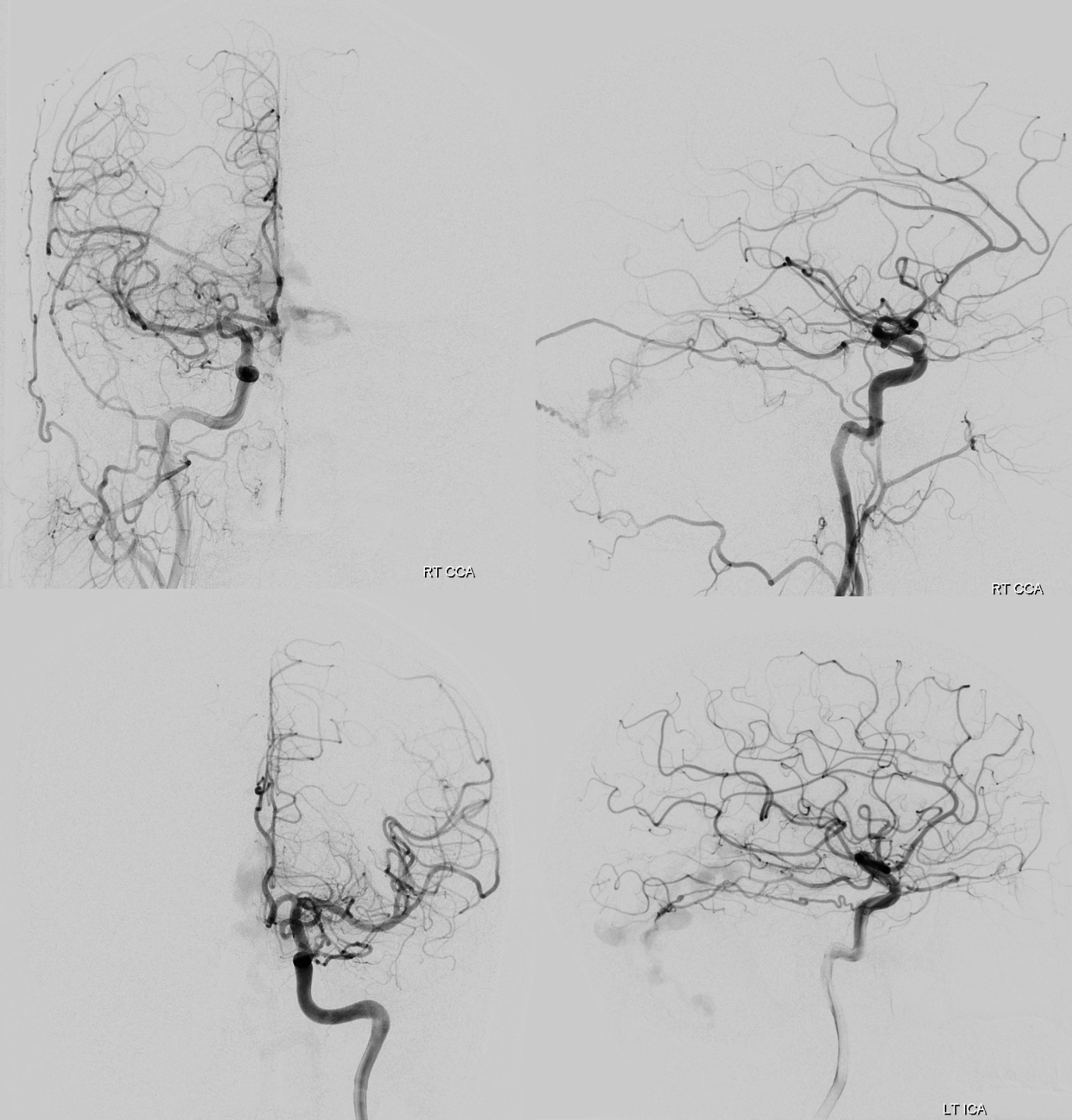
Looks like standard issue tentorial dural AVF
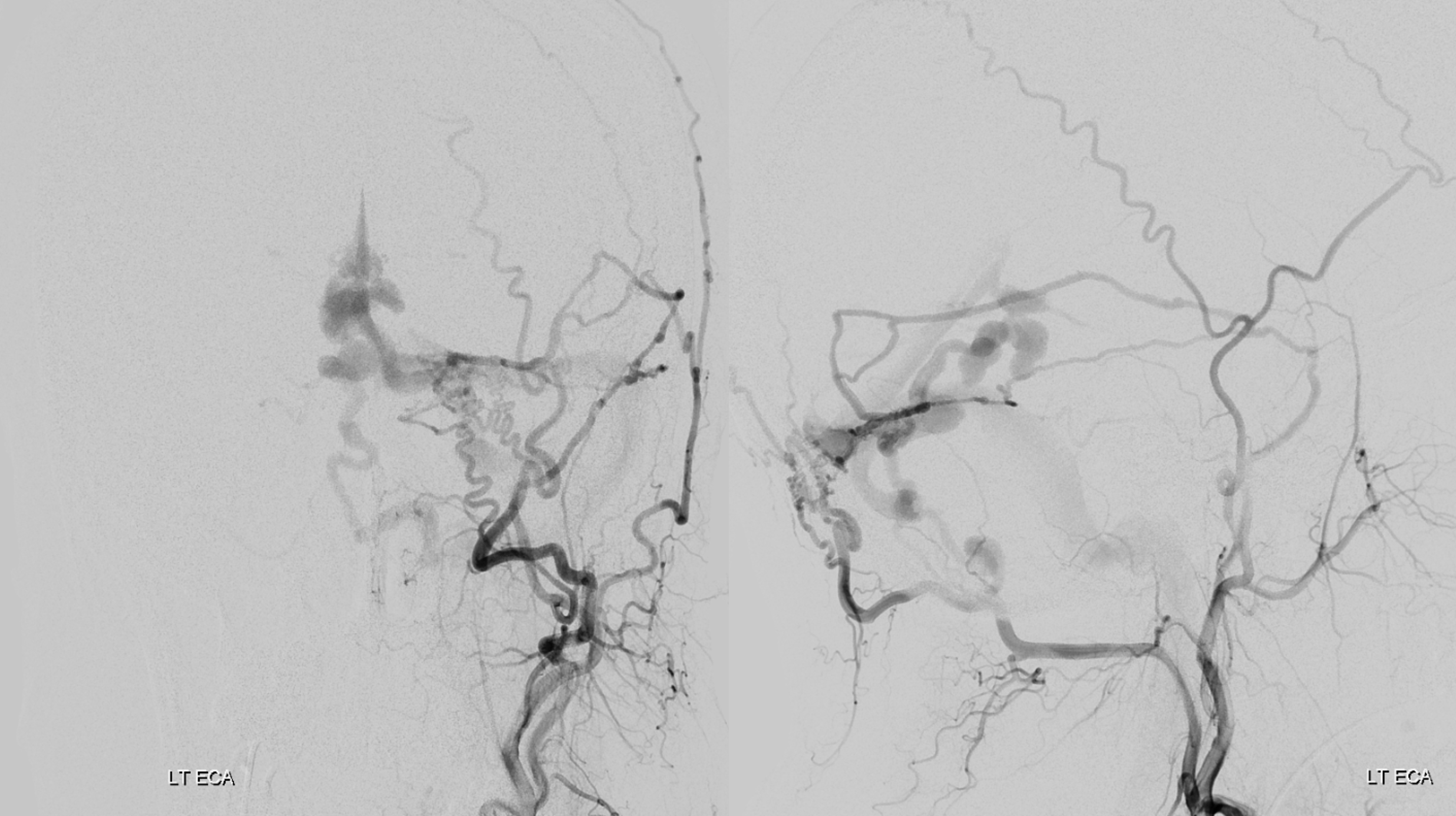
Except for this. In addition to dural supply via posterior meningeal and tentorium cerebelli arteries, there is what looks like a parenchymal paravermian nidus, supplied by SCA and PICA.
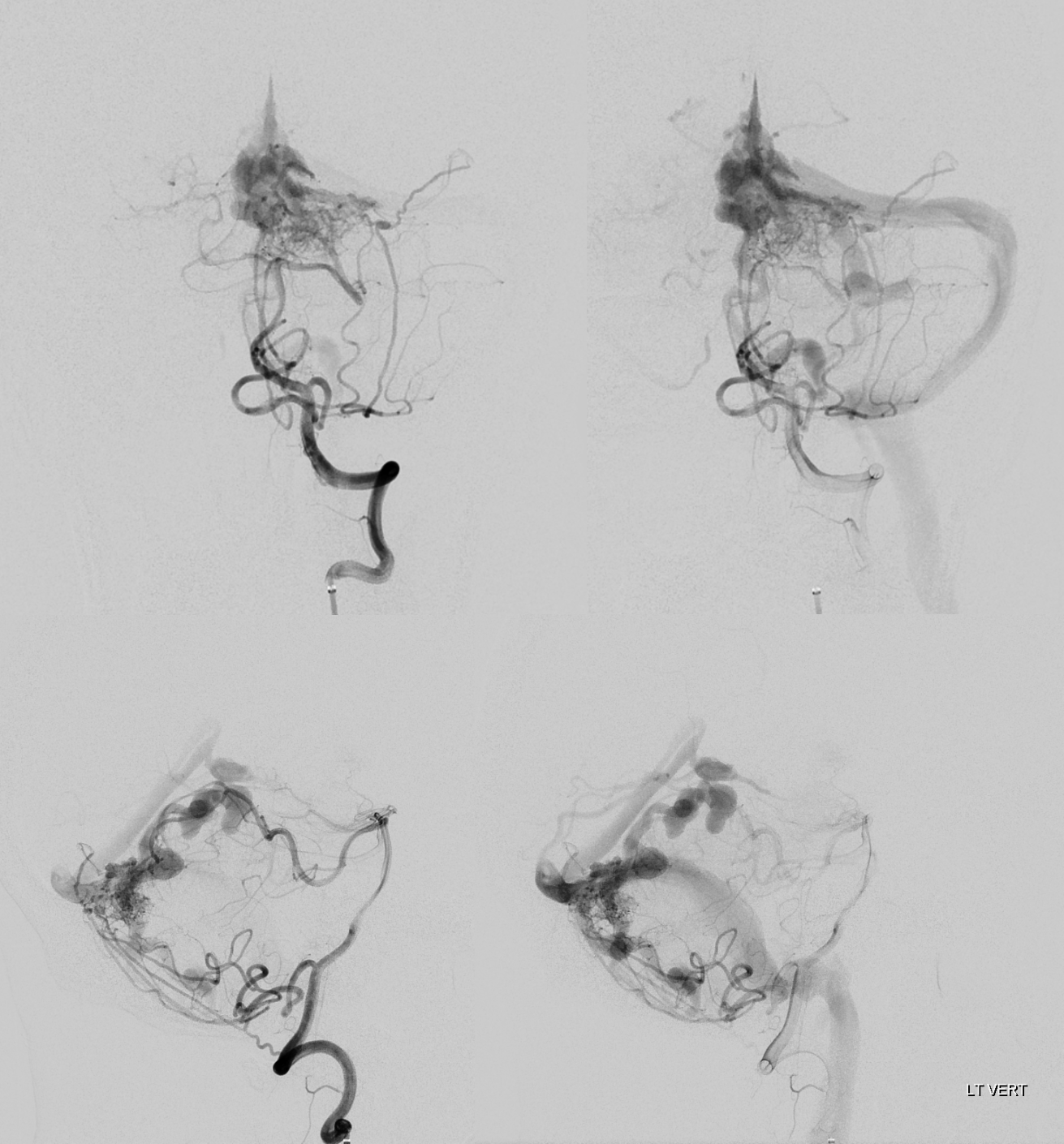
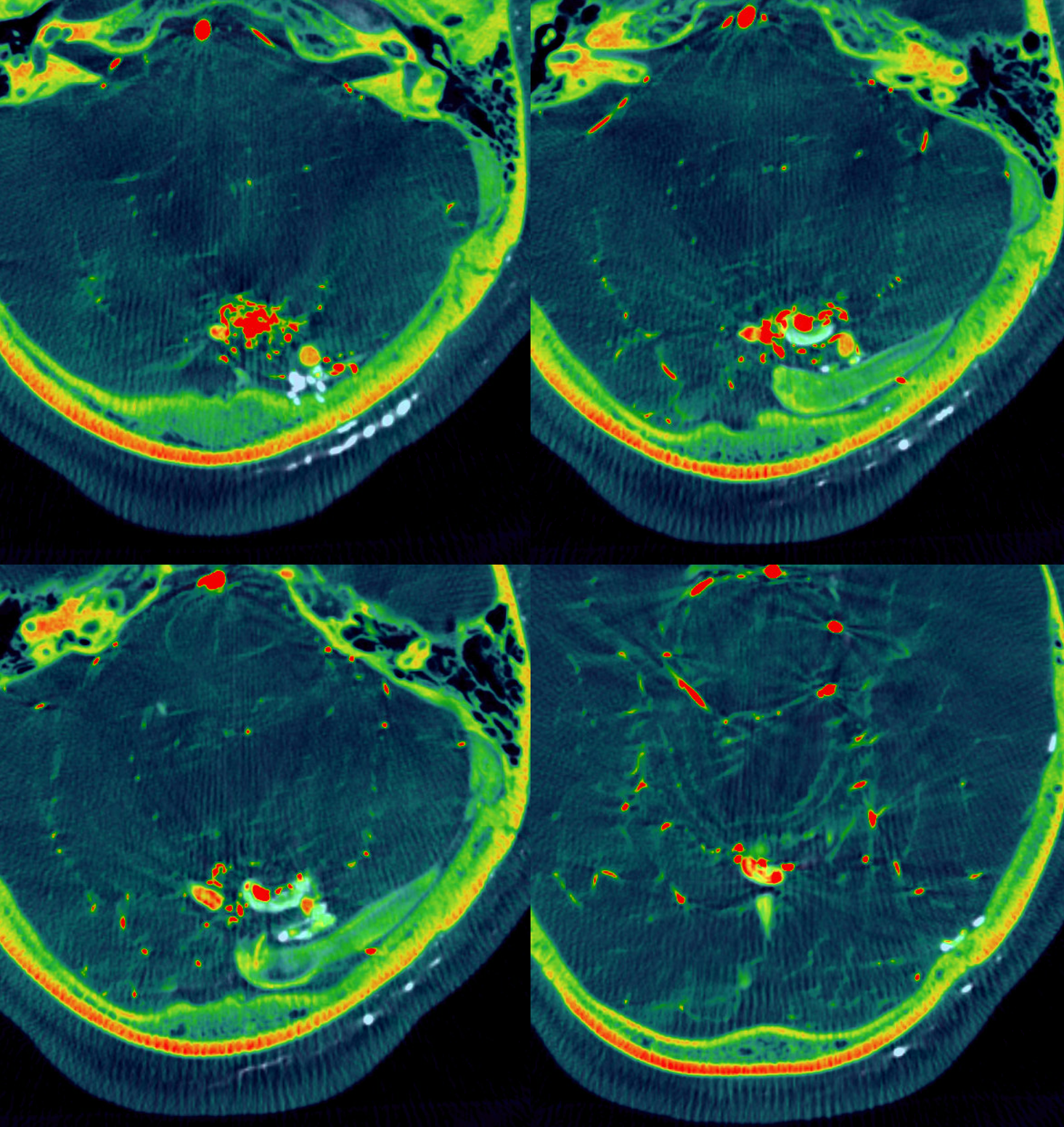
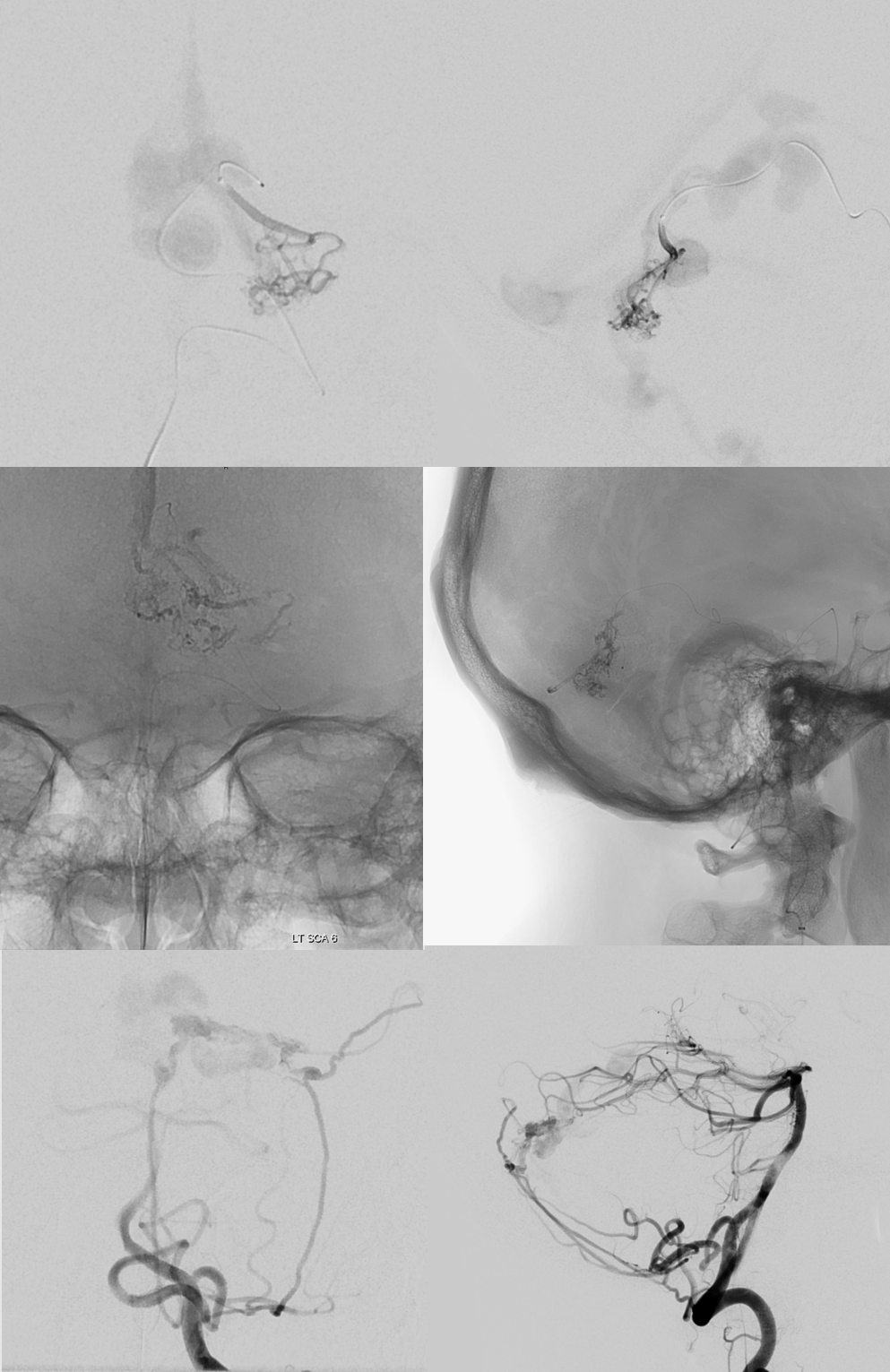
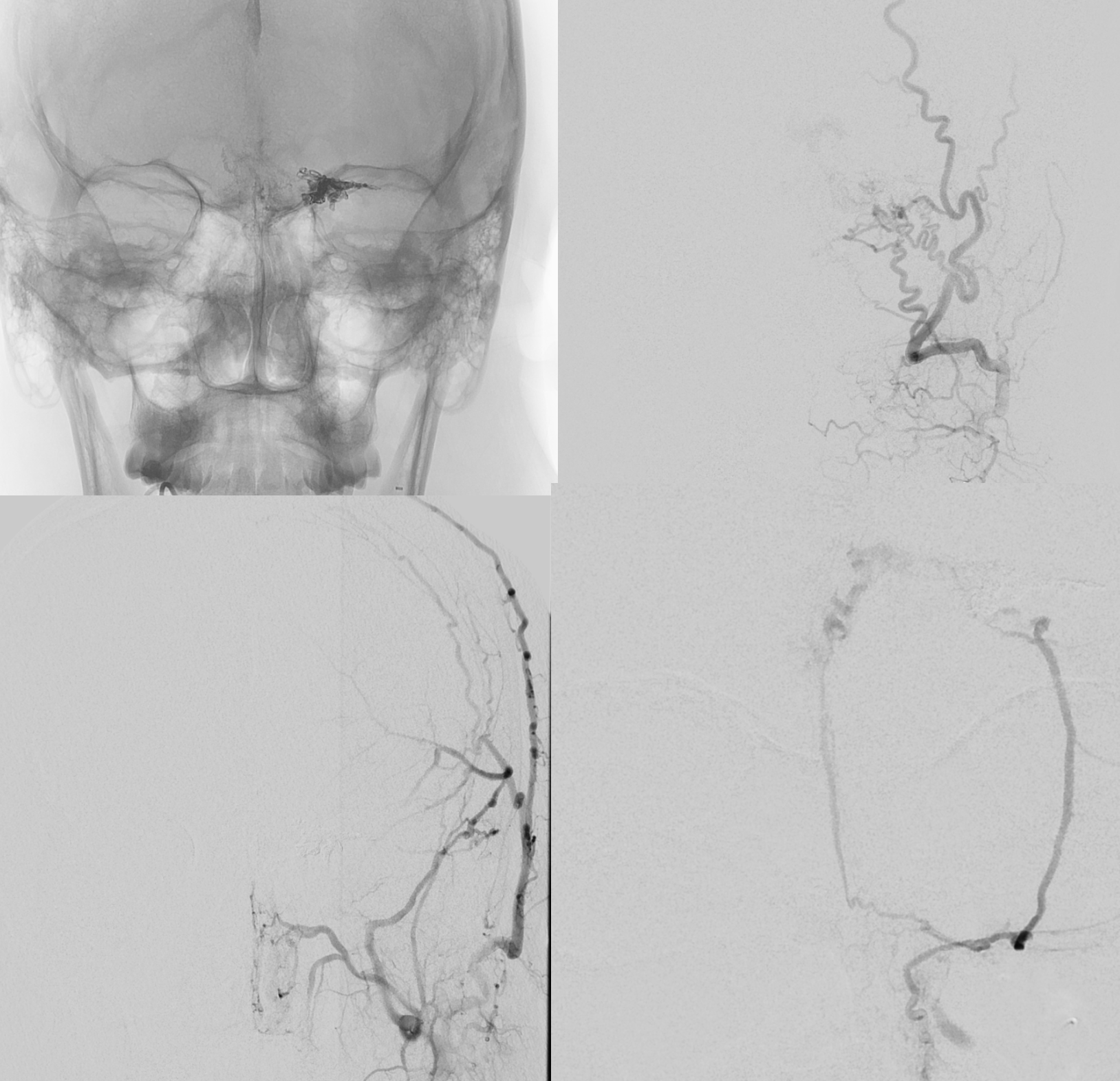
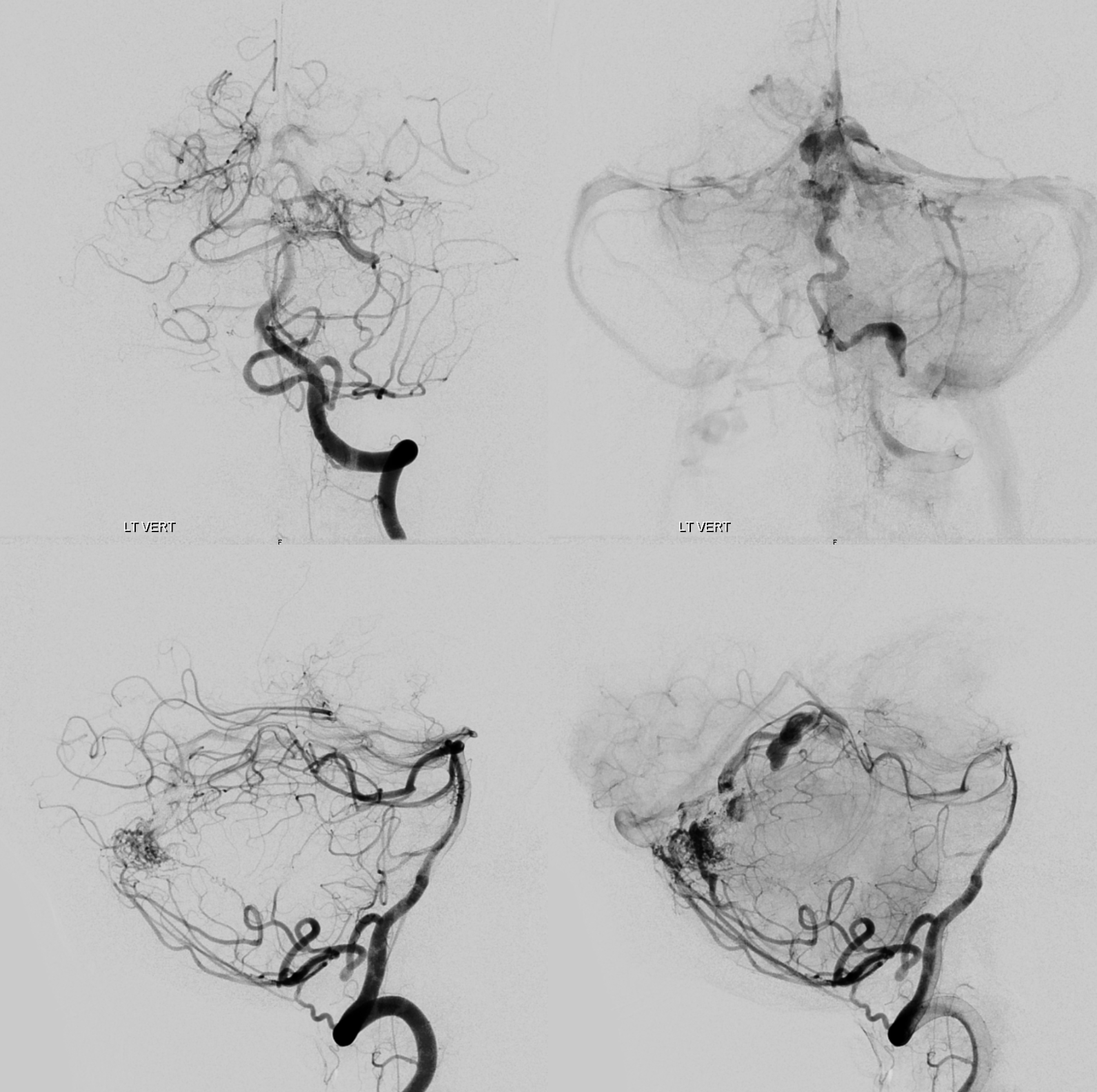
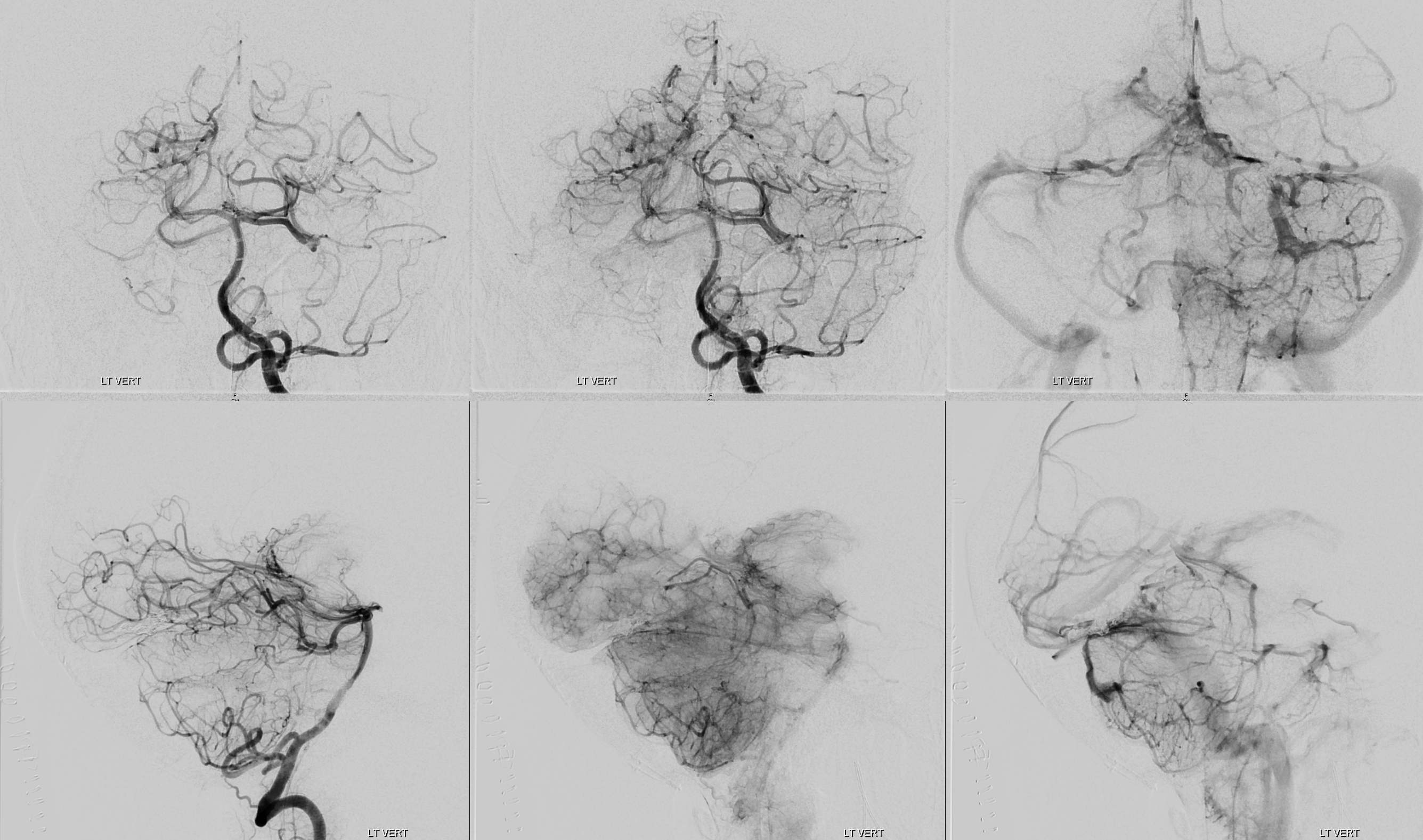
Cone Beam CT vert injection
Well, now lets analyze this in more detail. Cone beam CT is how to do it. Top row is CBCT of vert injection, bottom of left ECA.
Movies of the same
What we can see is that both AVM and dAVF share the same veins
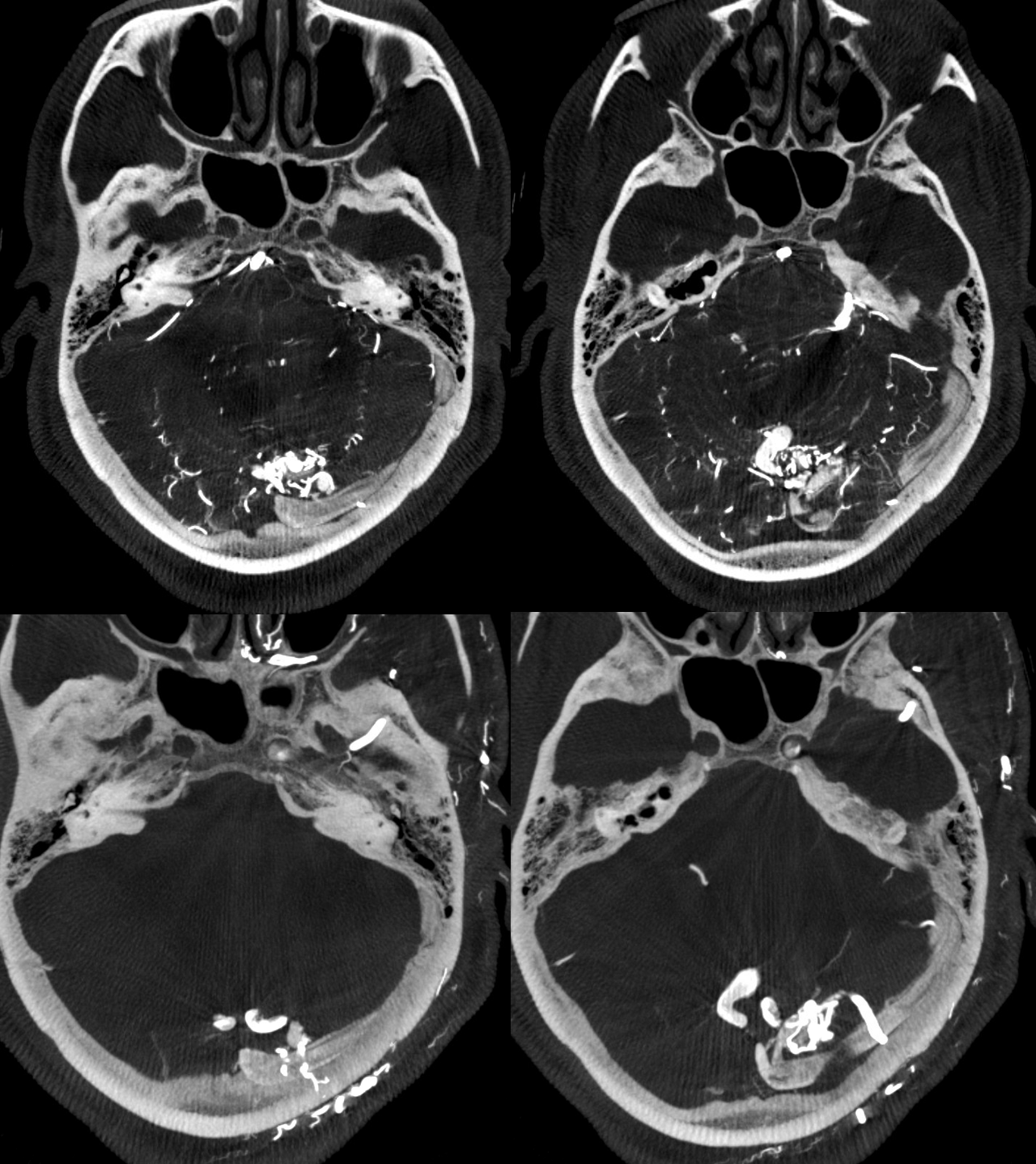
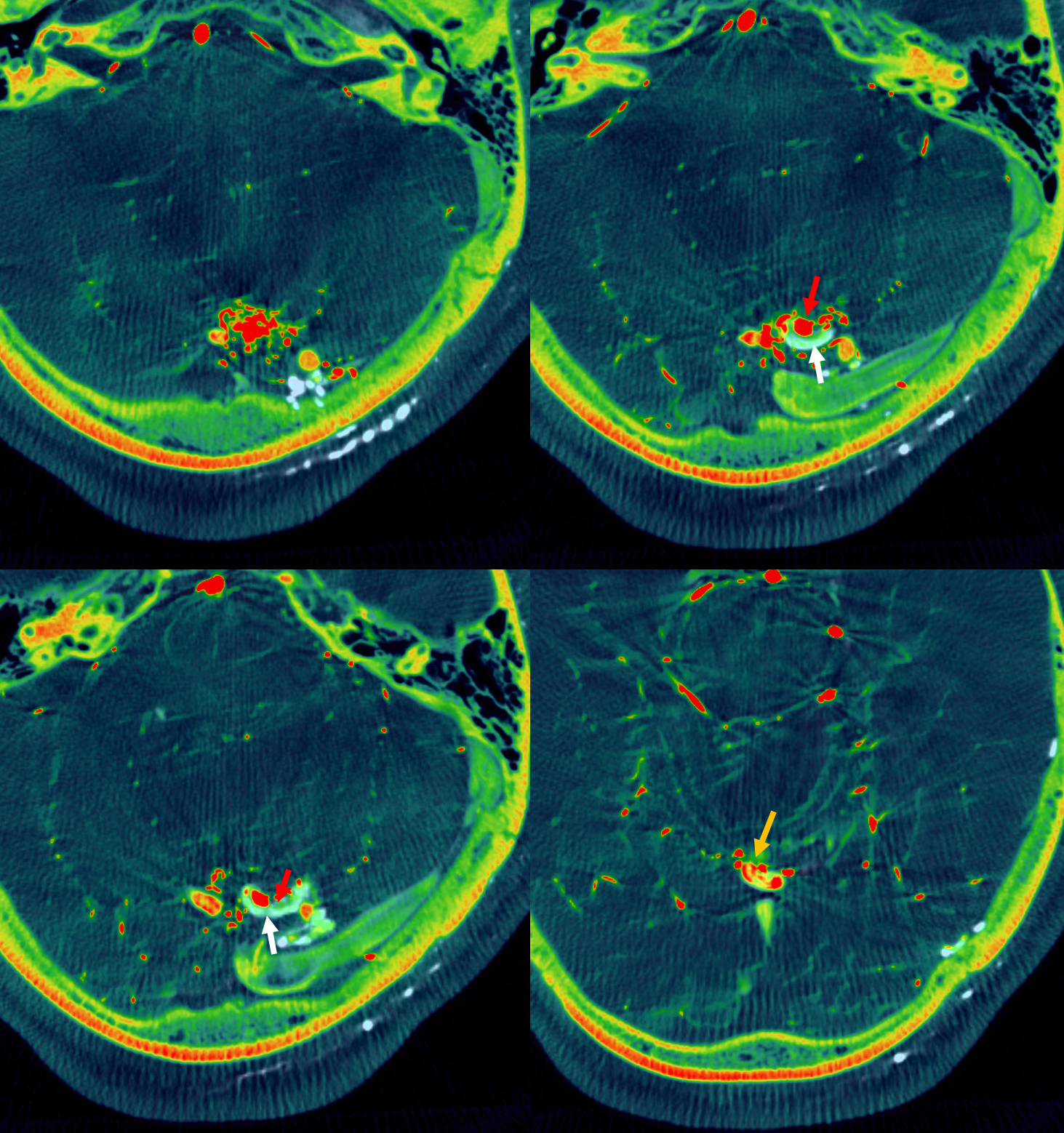
Lets take it one step further — by analyizing exactly how the shunts are related to the principal draining vein. Careful exam shows that the dAVF drains somwhat more distally into the common vein than the AVM. This can be shown in several ways. One is to co-register the datasets with individual color coding. The dAVF is white. AVM is red. Axial images
Arrows — the more distal vein draining the dAVF is white arrows. The inflow from AVM is red arrows. The downstream admixture of both is orange arrow
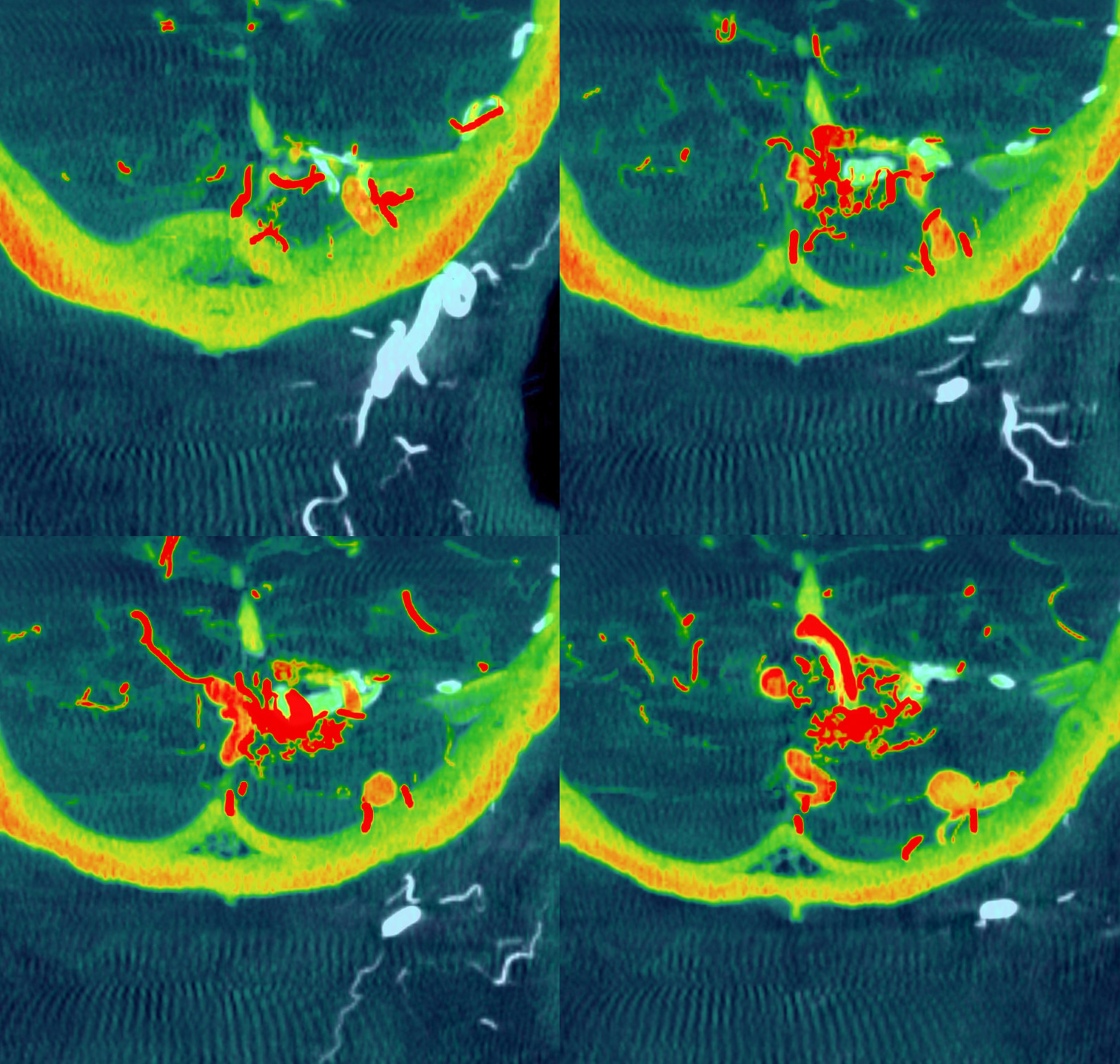
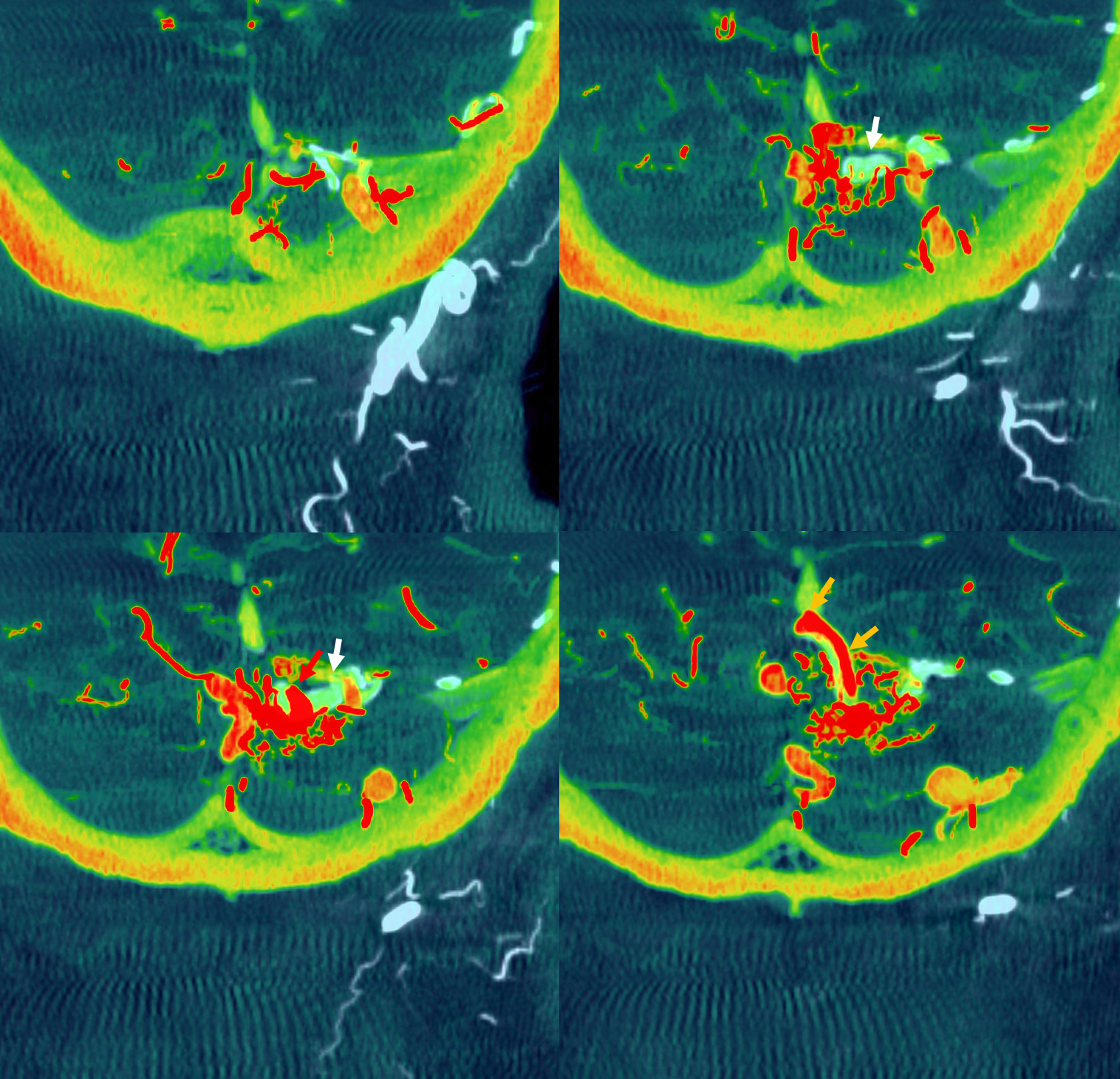
coronals
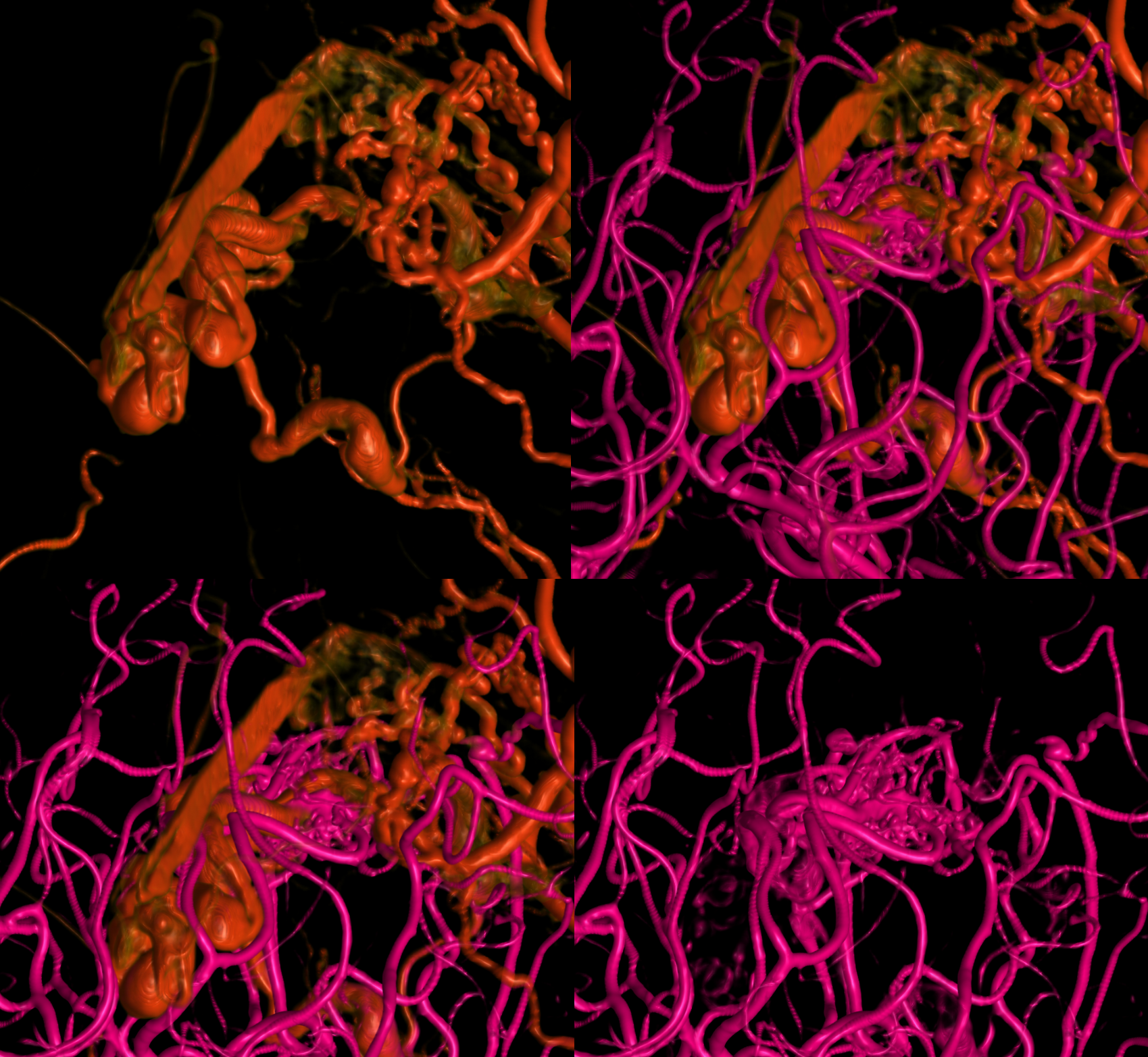
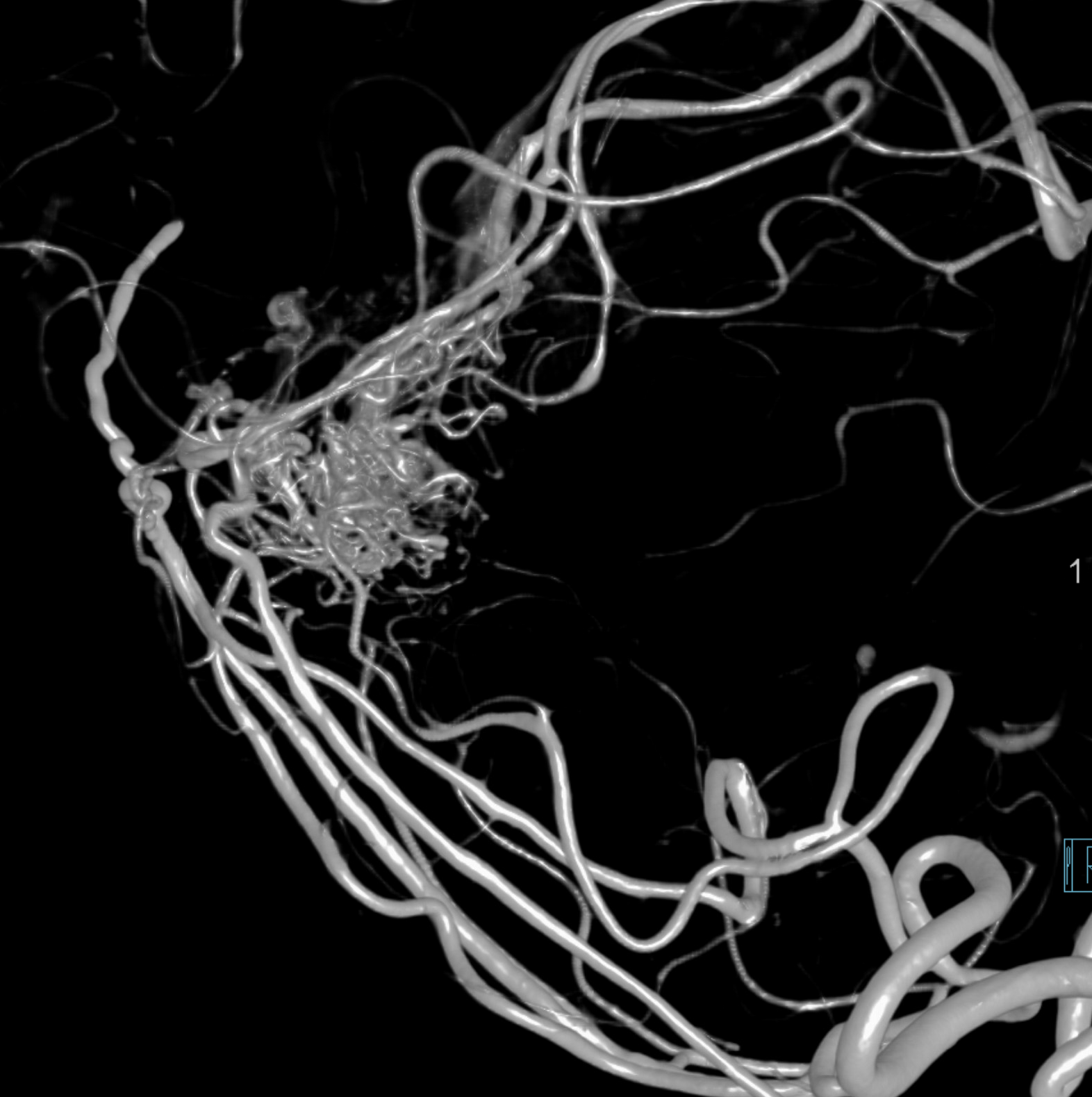
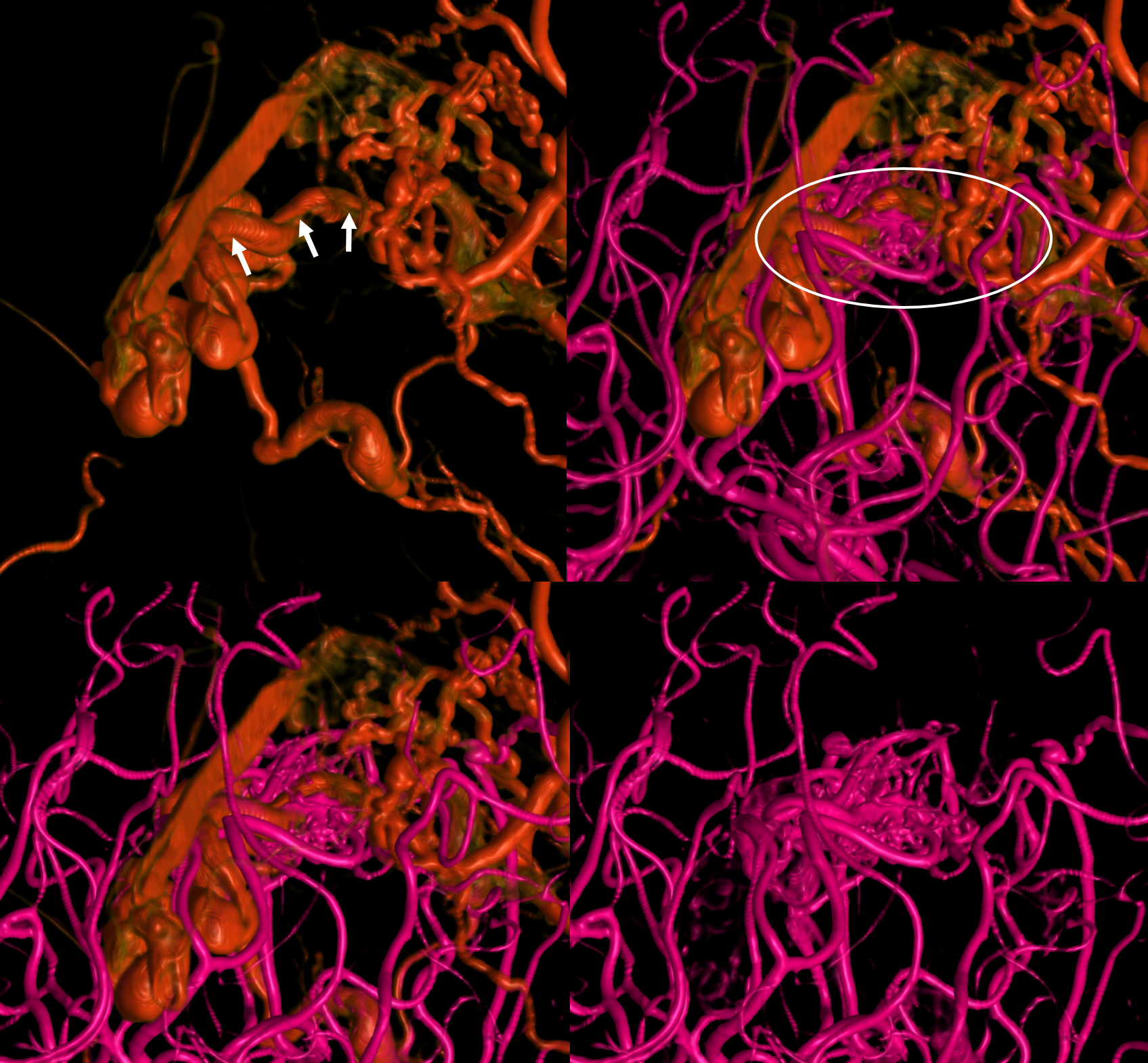
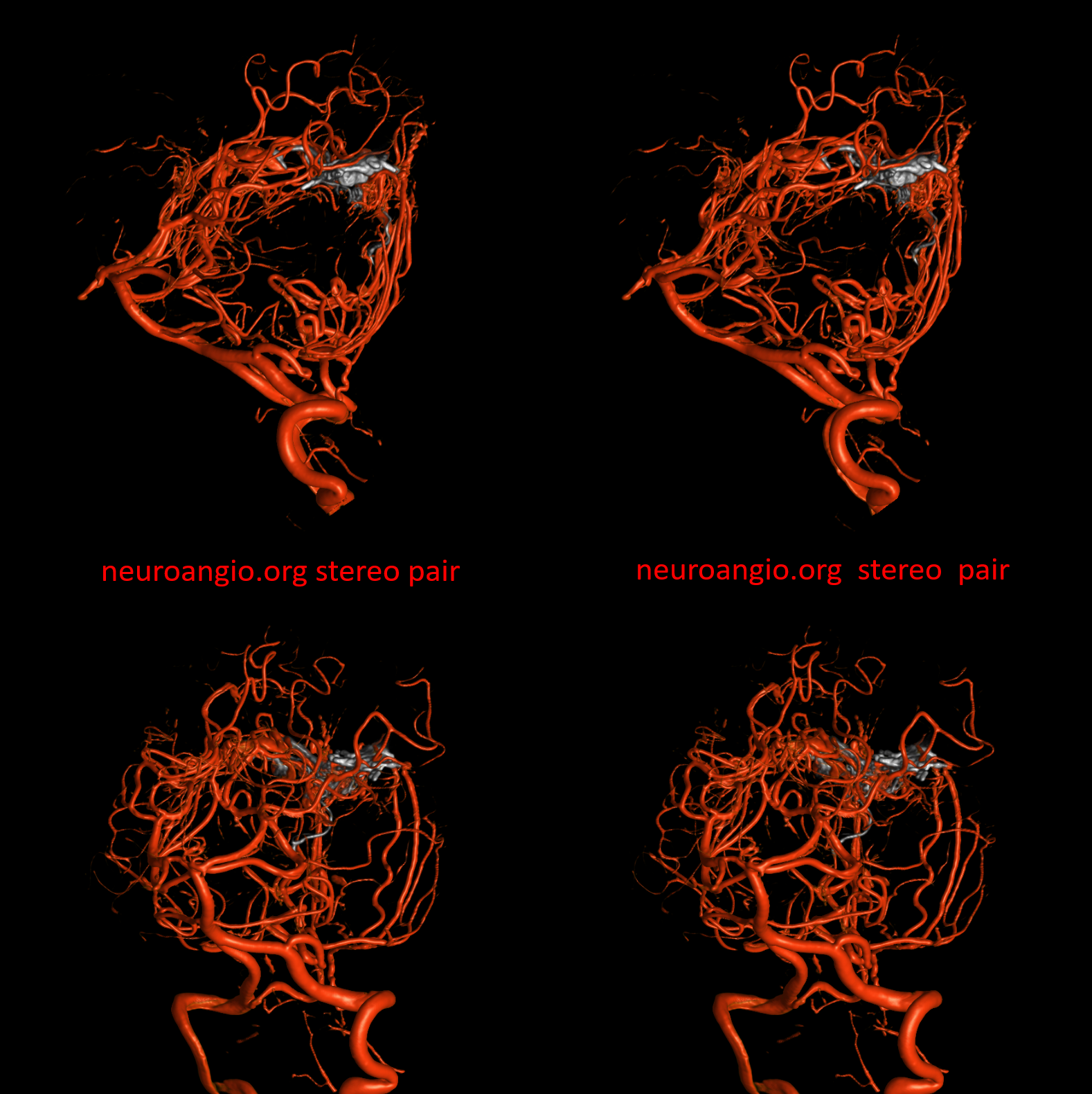
Volume-rendered views — ECA is red, vert is pink
Note common vein (white oval) with inflow artifact from AVM into the common vein shown by arrows
Movie
This is important in itself, and always this kind of understanding has therapeutic benefits. Now we can have a rational treatment strategy — not a mindless injection from some pedicle into something else we dont know what.
The strategy is preoperative-type AVM component embolization, followed by occlusion of the dAVF. The above analysis permits us to understand how far the we should allow the embolic material to permeate the vein, to shut down the dAVF without compromizing outflow of the AVM. The goal here is not tranvenous AVM embo, but rather a preoperative embolization. The difference in strategy is important — the goal of embo is to take down arterial pedicles with maybe some nidal penetration, but without occluding the part of the vein draining the AVM.
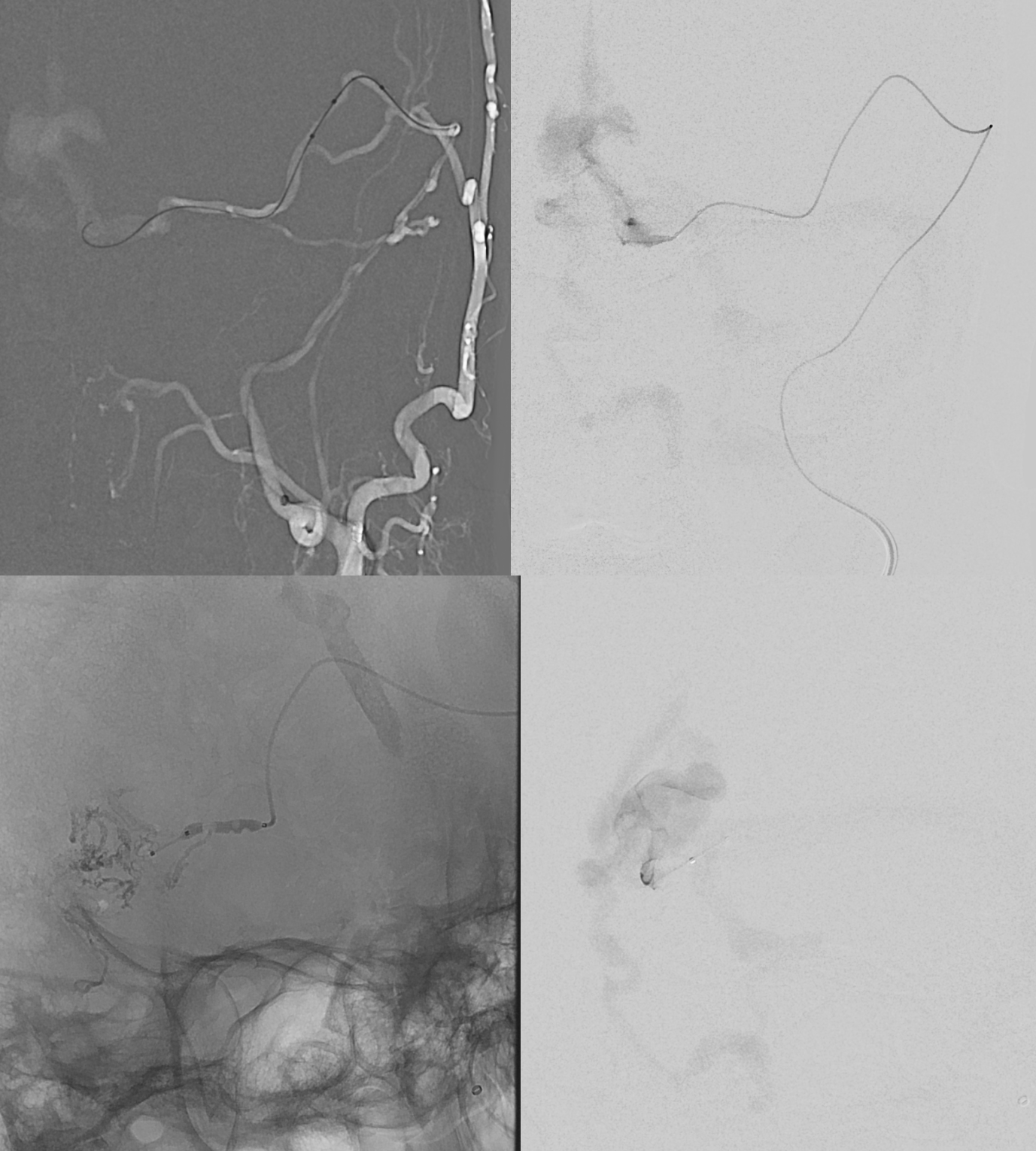
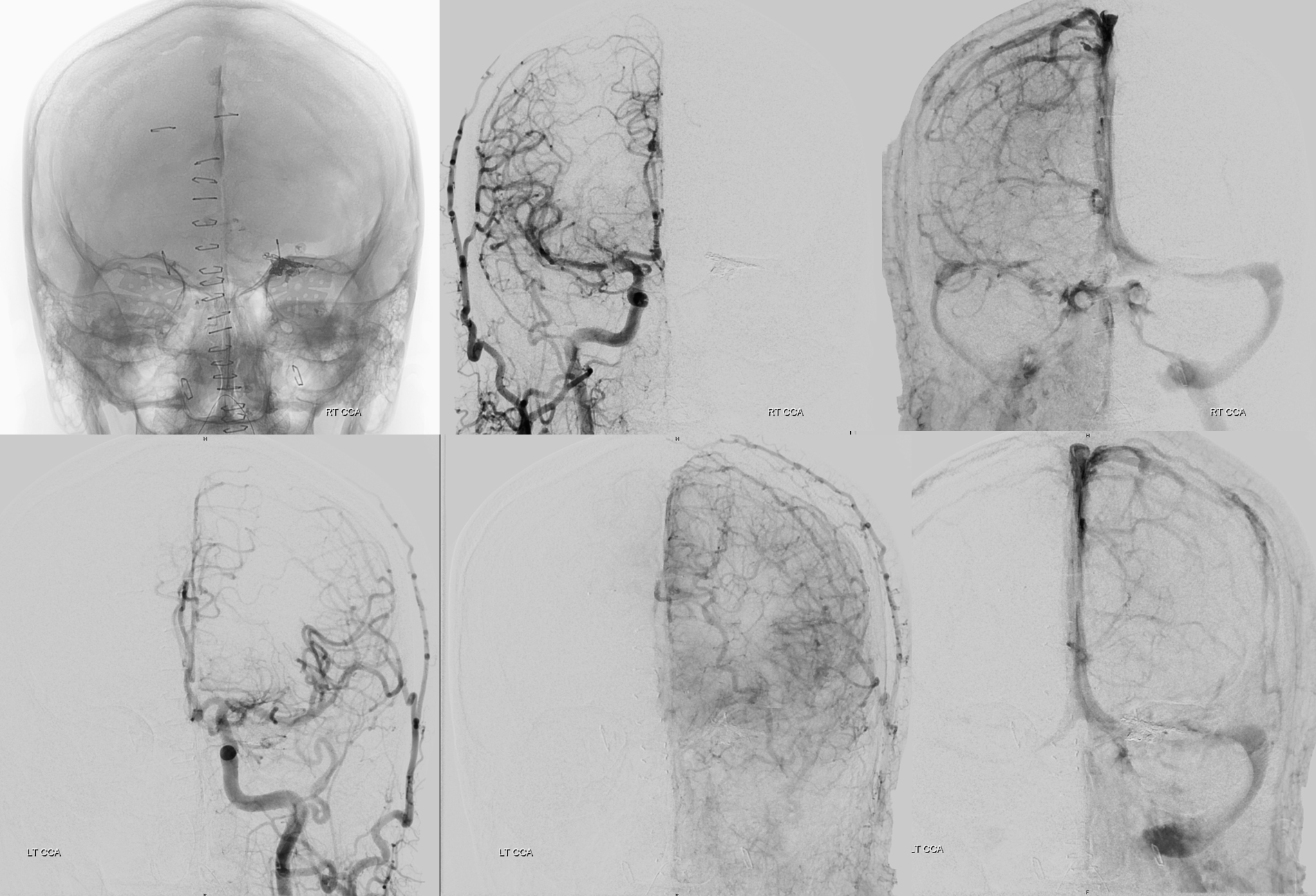
Below are subselective SCA injections (followed by preoperative style arterial nBCA embolization). Bottom rows shows post-embo images with intended leftover of PICA supply and patent vein
Next comes dAVF treatment. Our choice is usually a dual lumen balloon when possible. In this case Scepter C goes directly from the petrosquamosal branch of the MMA into the vein.
At this point transvenous embo of the AVM is possible as well. We decided to stick to the preop plan and not take the AVM.
Controlled occlusion of dAVF portion of the vein is facilitated by coil placement, followed by Onyx injection.
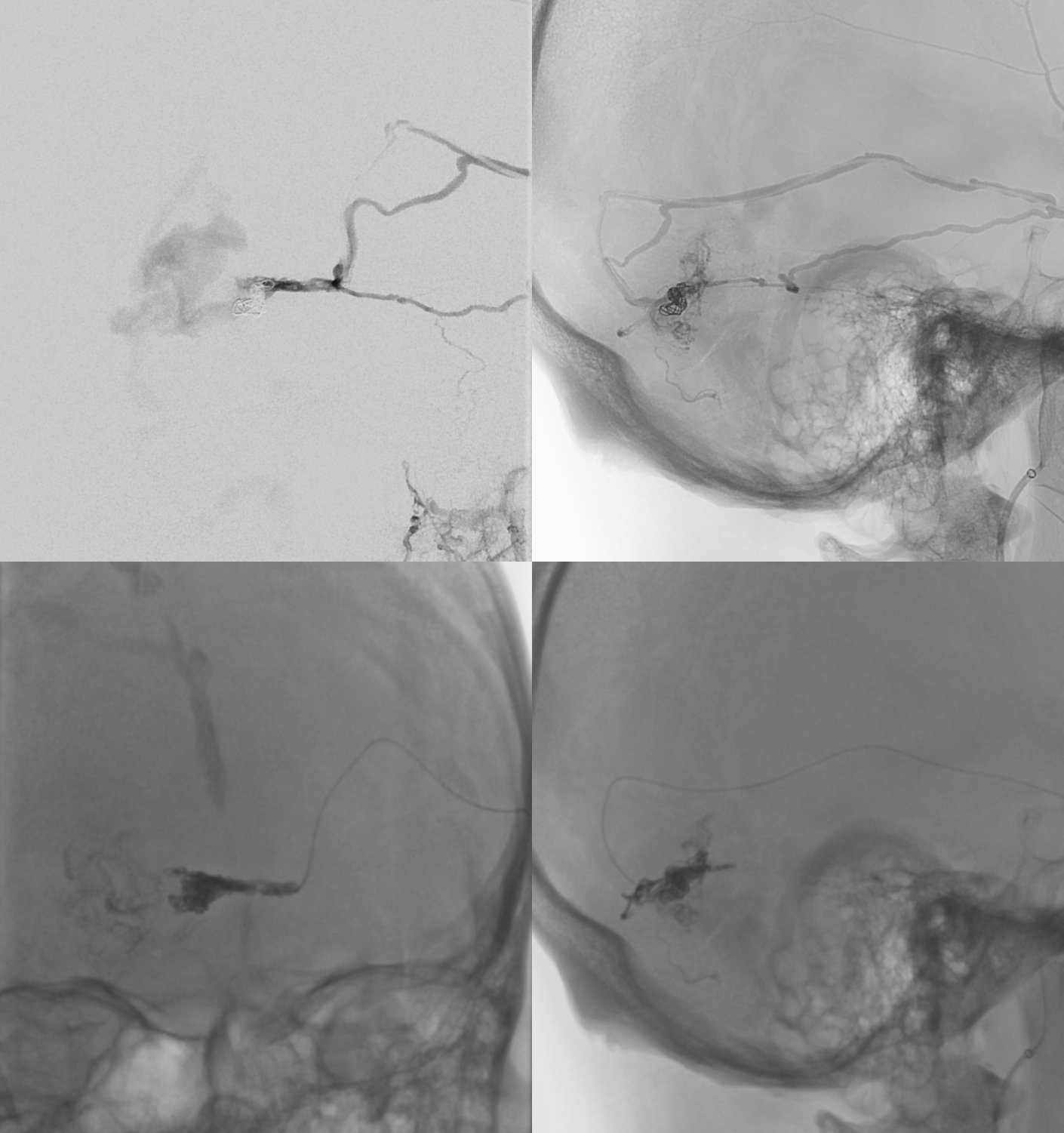
Post-dAVF embo
Dural dAVF supply is gone. Residual AVM is supplied by the vermian PICA
Post resection
Complex case, lots to appreciate