
Fantastic case showing the value of advanced imaging for preoperative planning and effective and diligent embolization. It also shows that effective embolization can shrink meningiomas — something we should be doing much more of
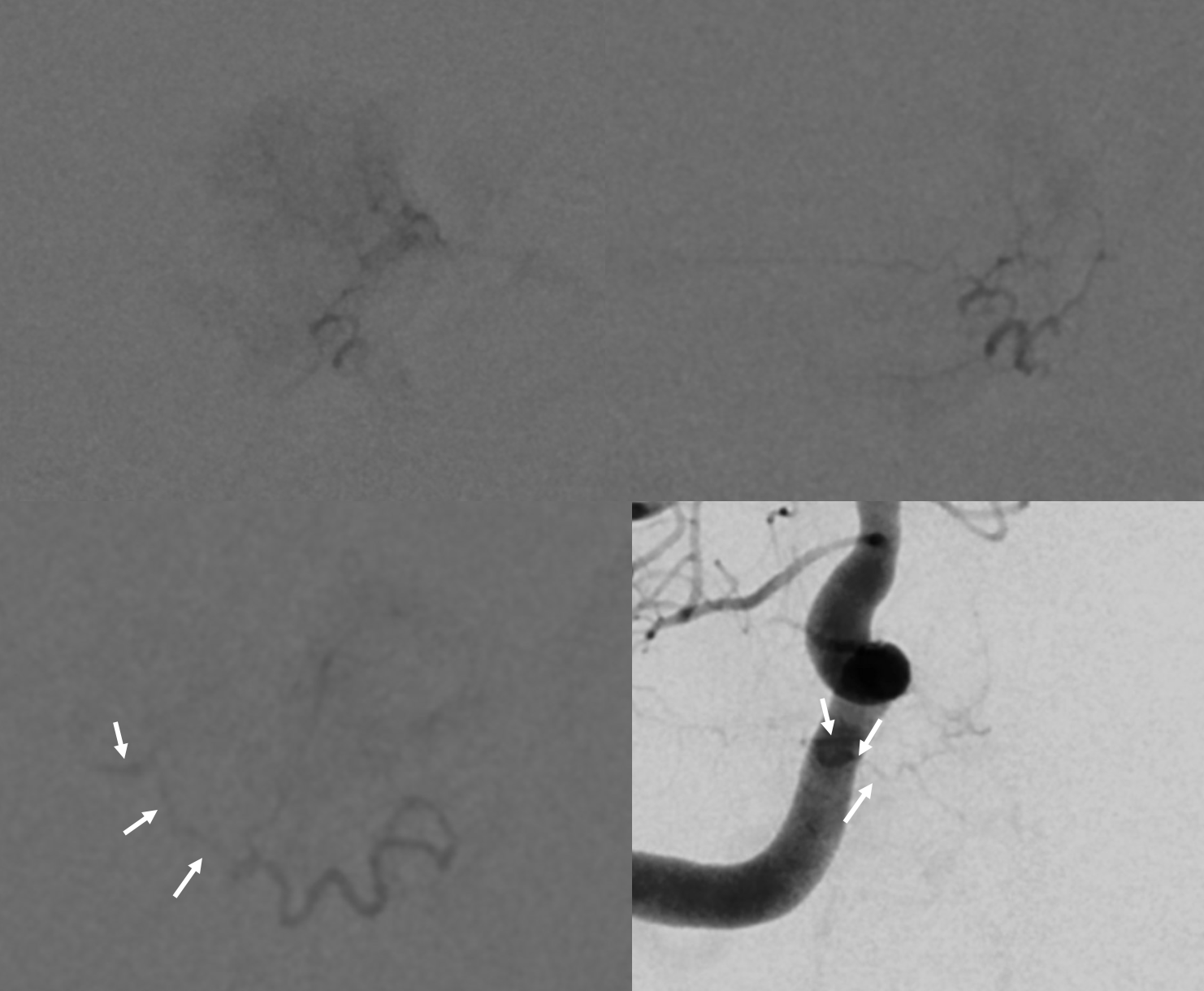
Right more than left MHT supply, plus something even more challenging…
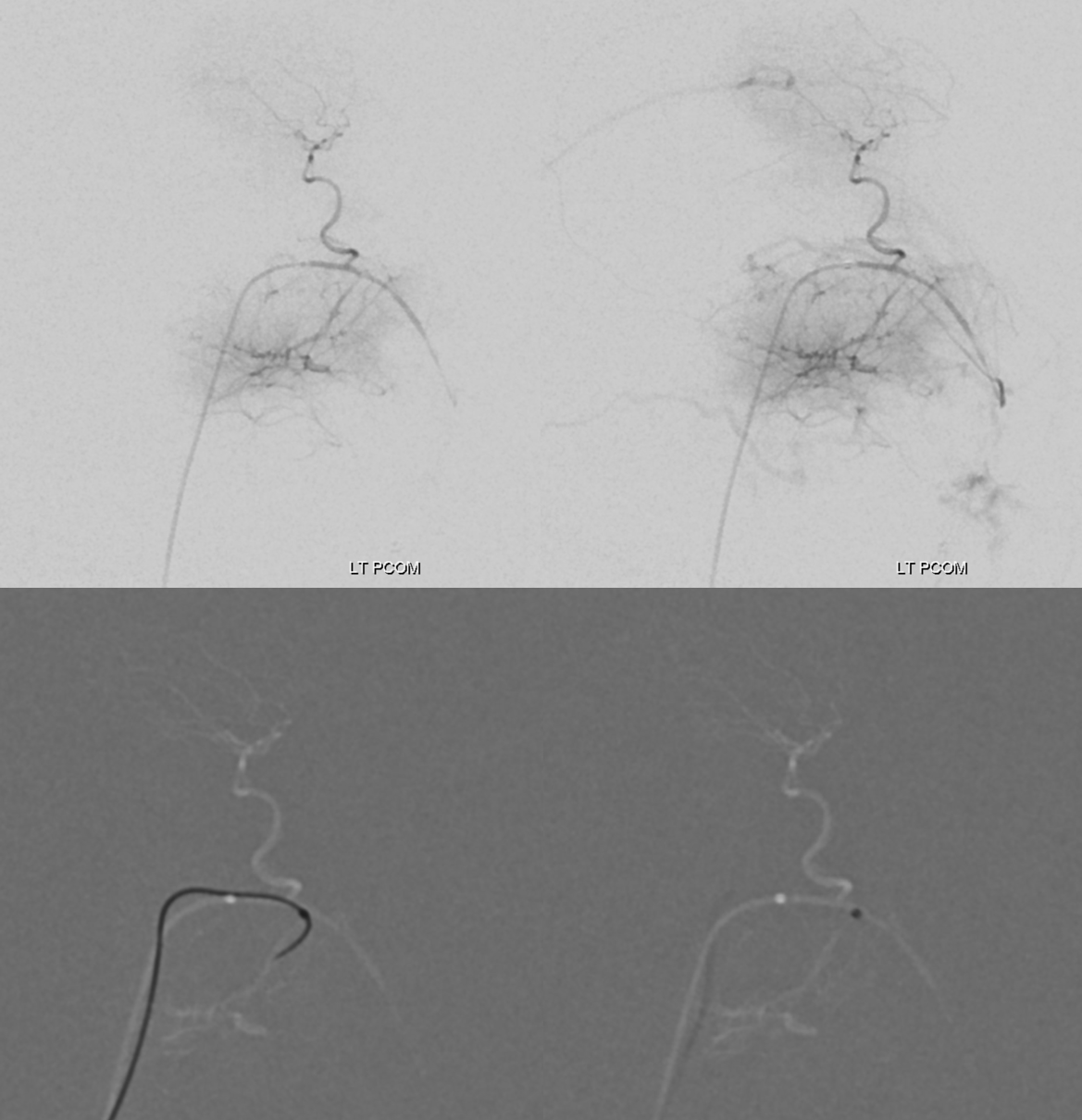
A small piodural anastomosis (dashed arrows) between the PCOM (arrows) and the tumor. Anything is possible…
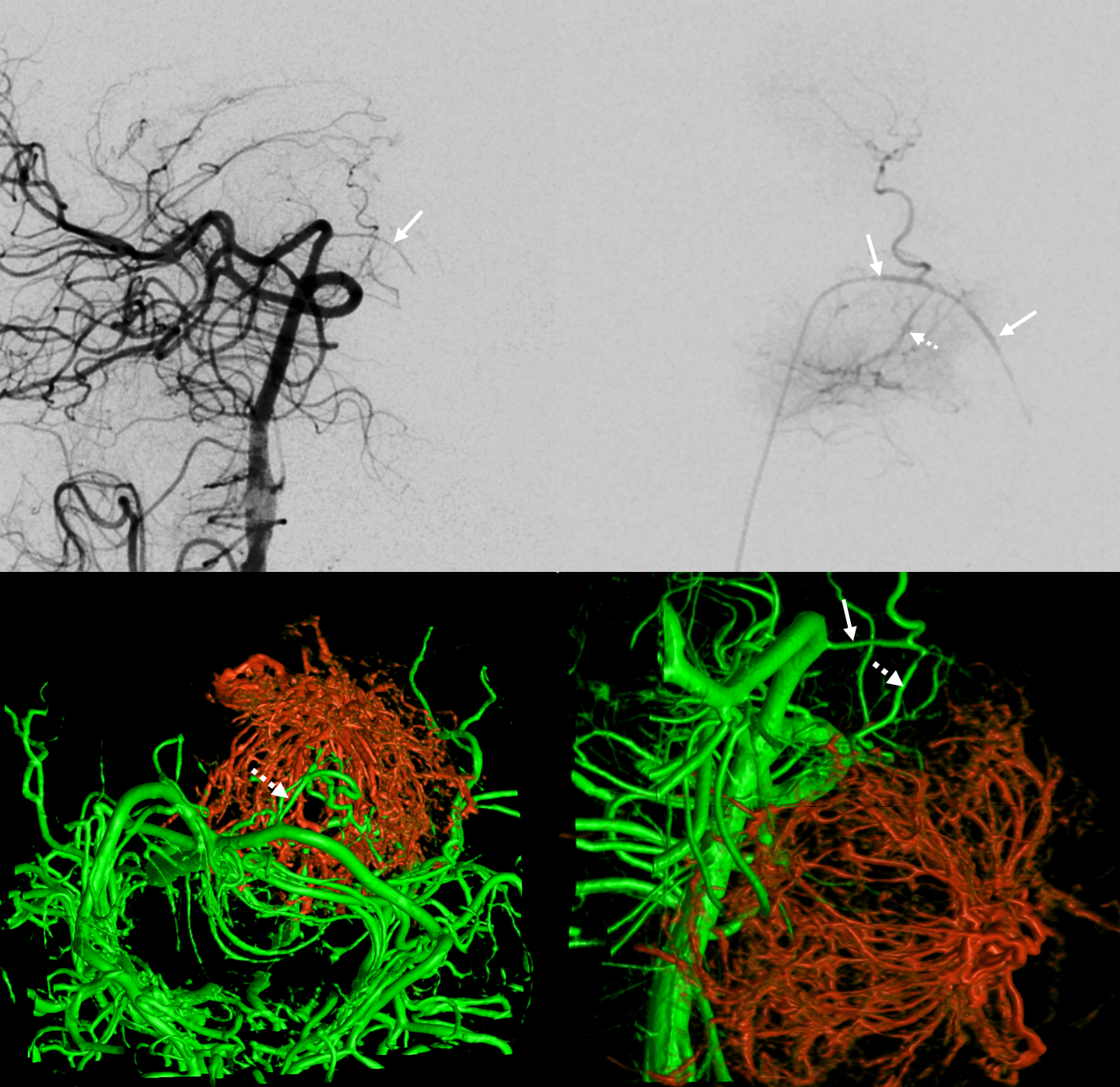
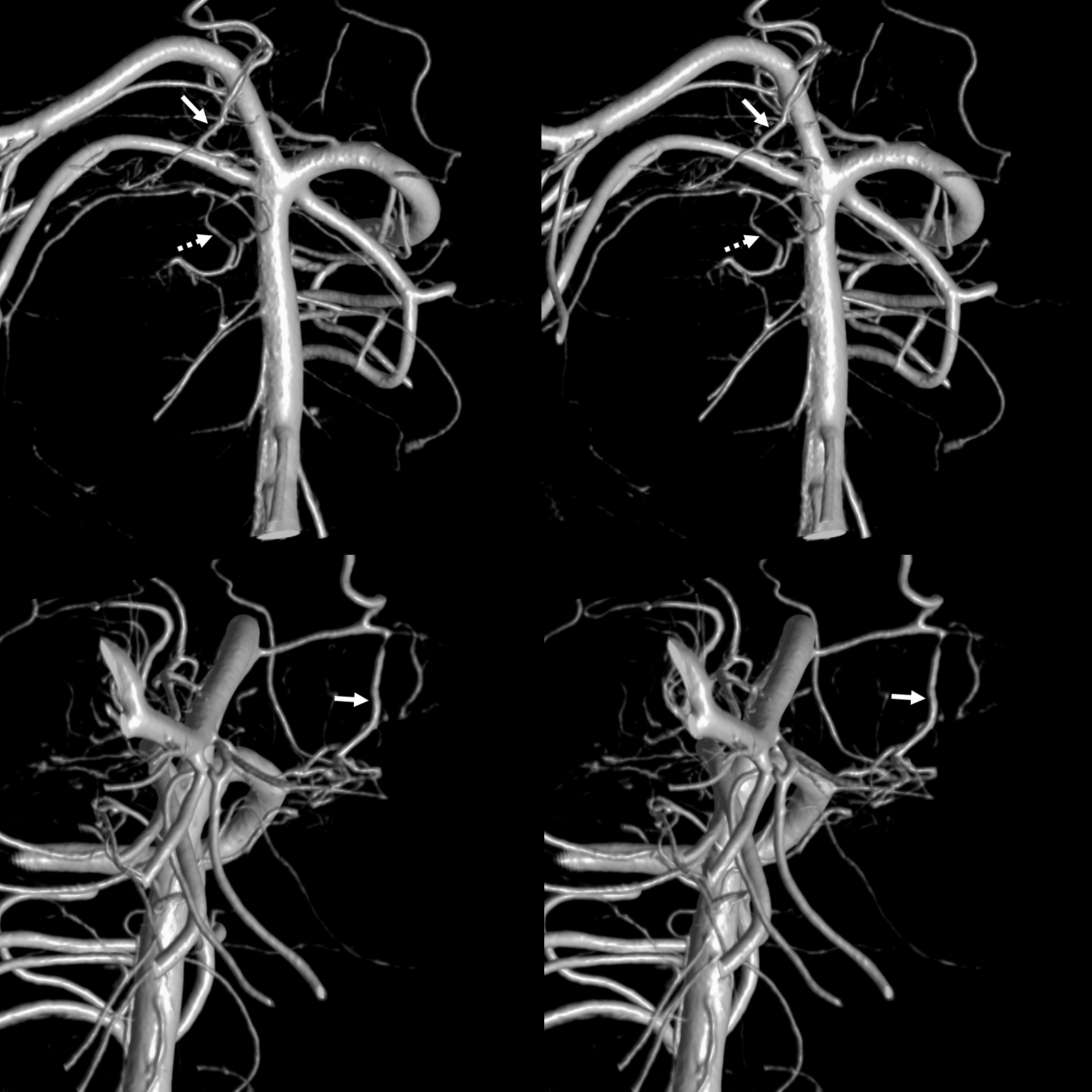
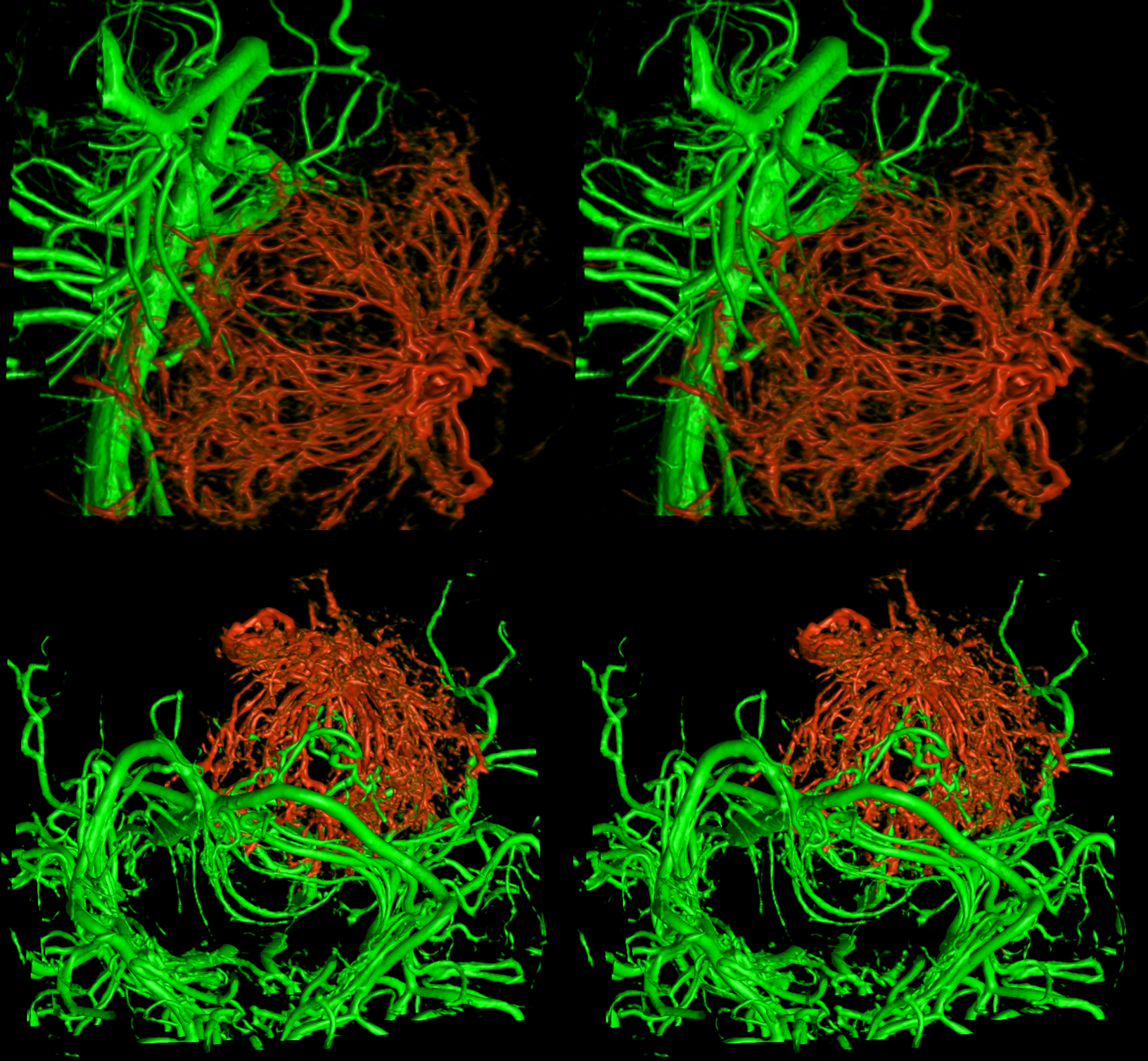
Fusion of DYNA CTs from left PCOM (green) and right MHT top set — stereos. Bottom set are carotid fusions
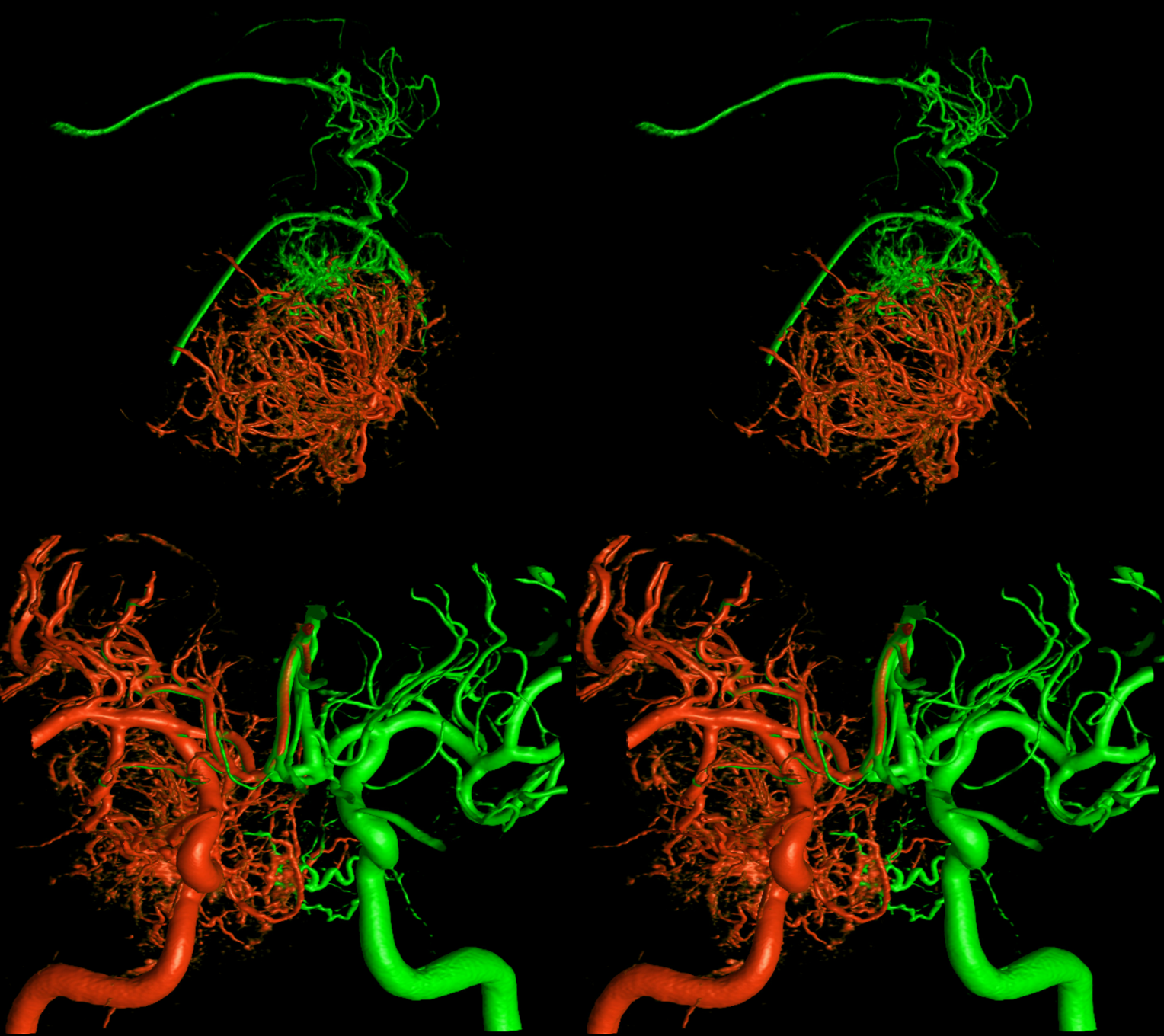
Fusion stereos
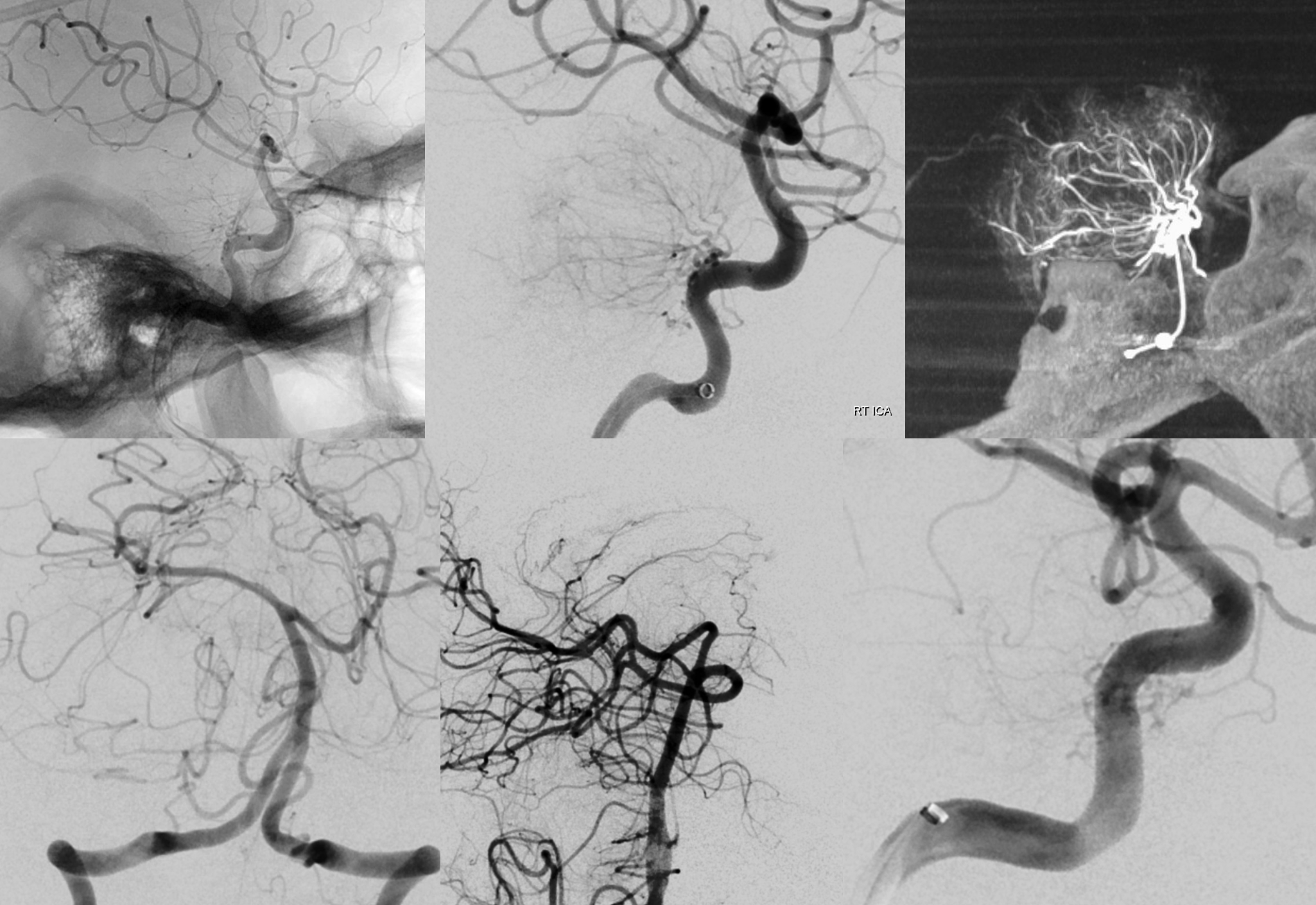
RT MHT
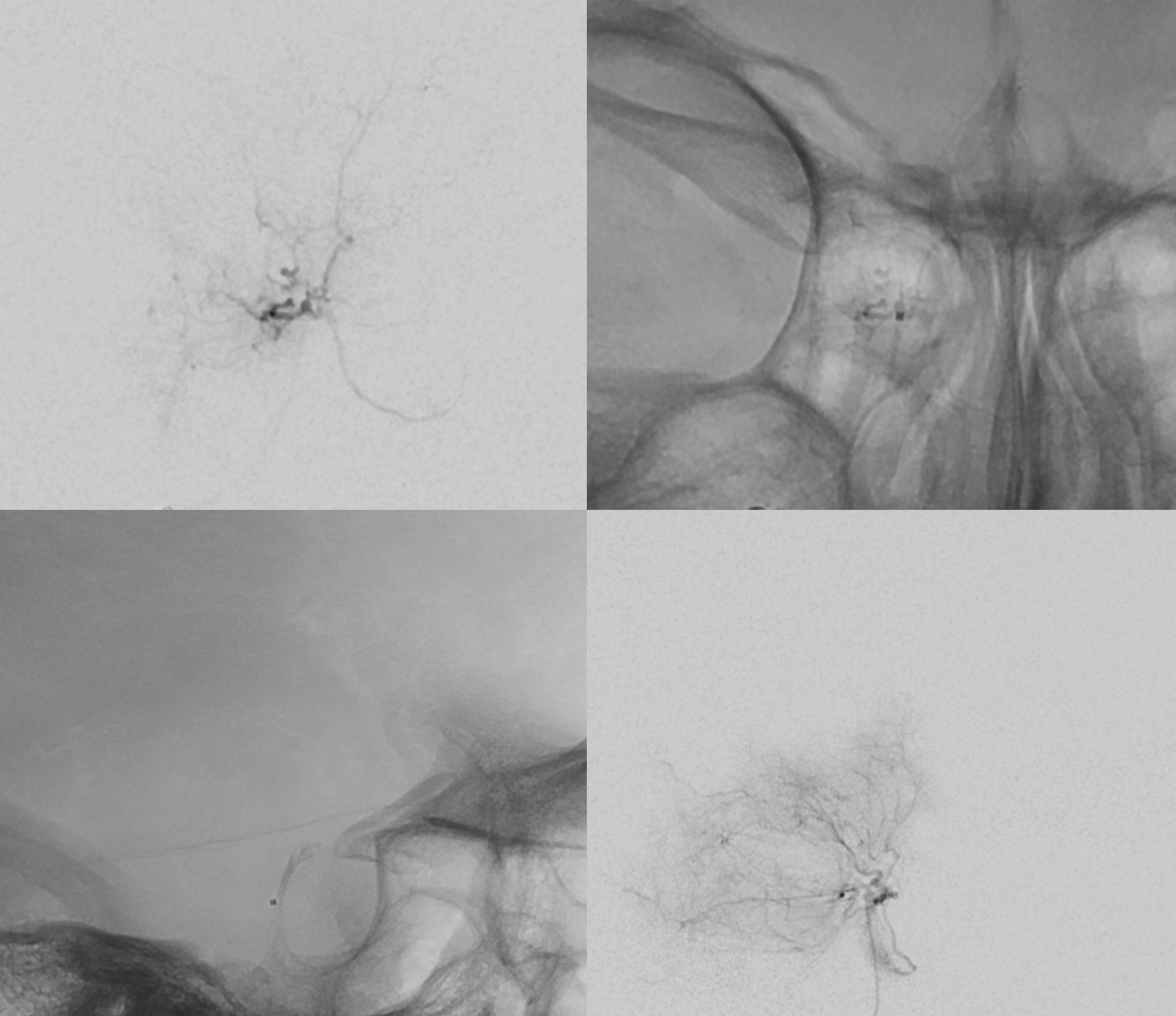
Contour 45-150 right MHT embolization followed by a coil
Left MHT cath and micro DSA — marginal tentorial here also
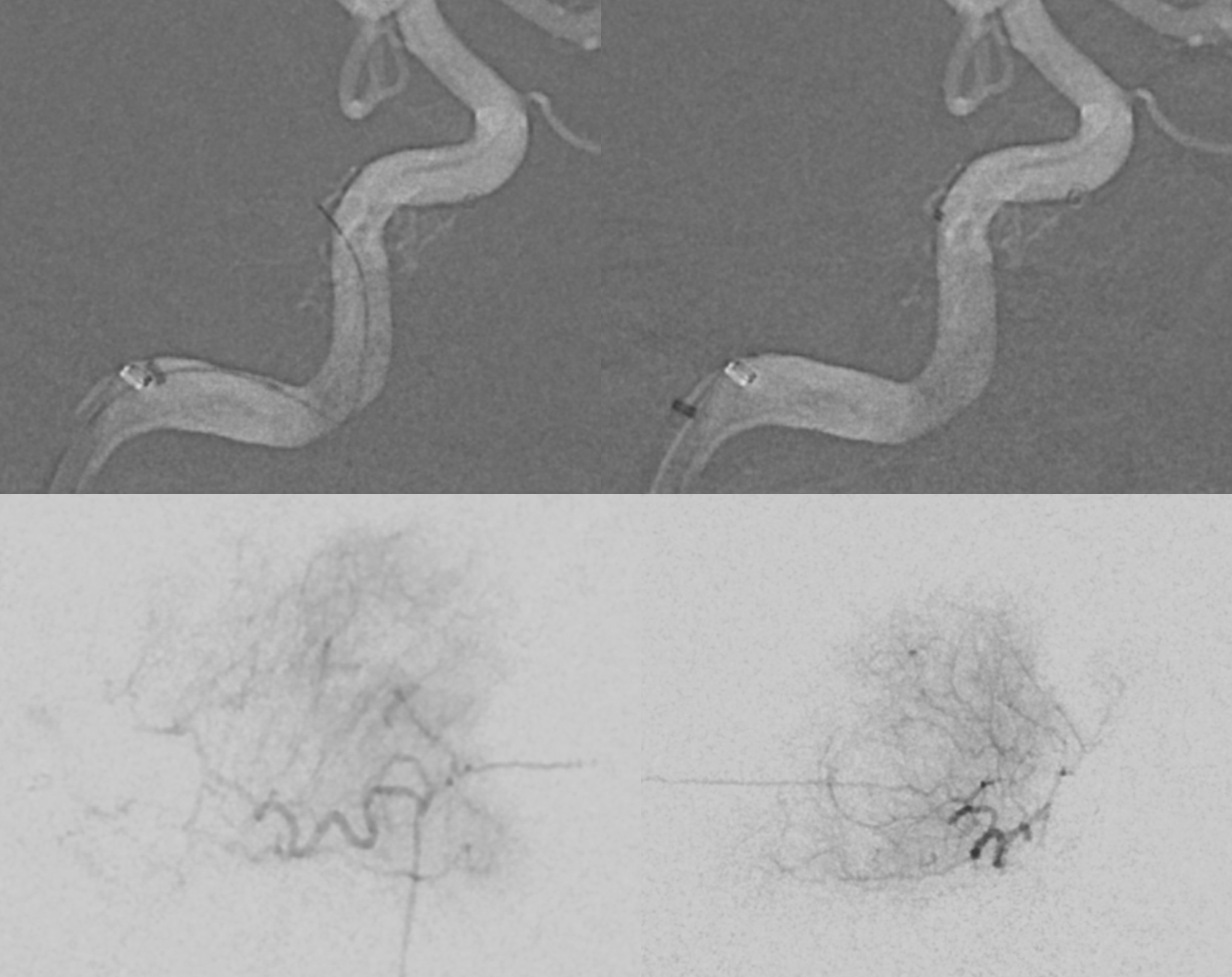
Embo
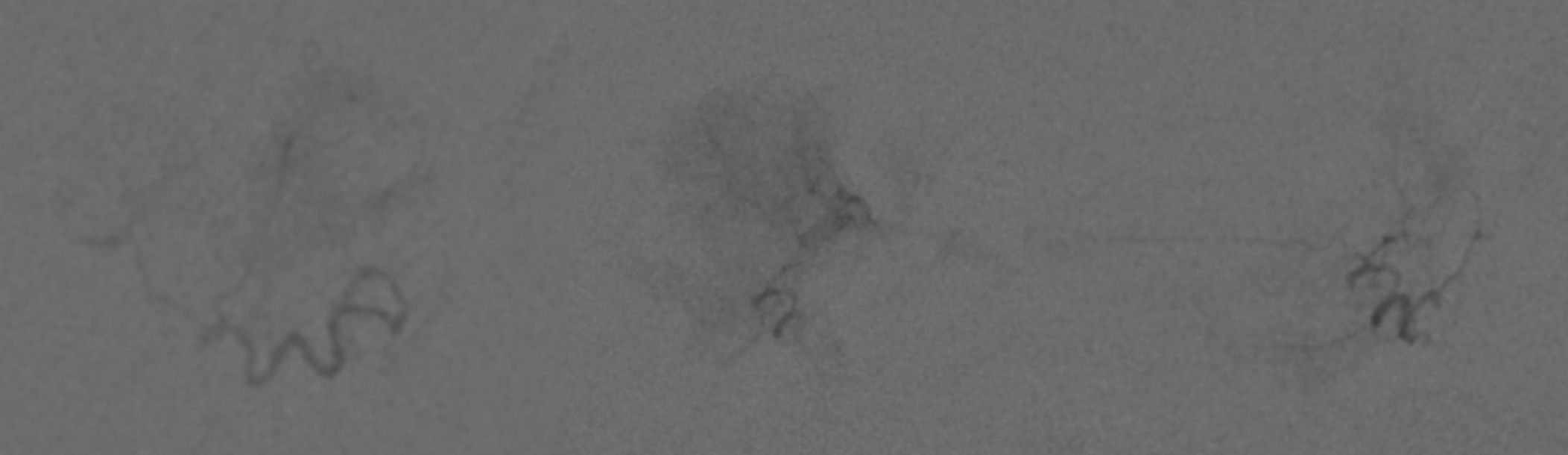
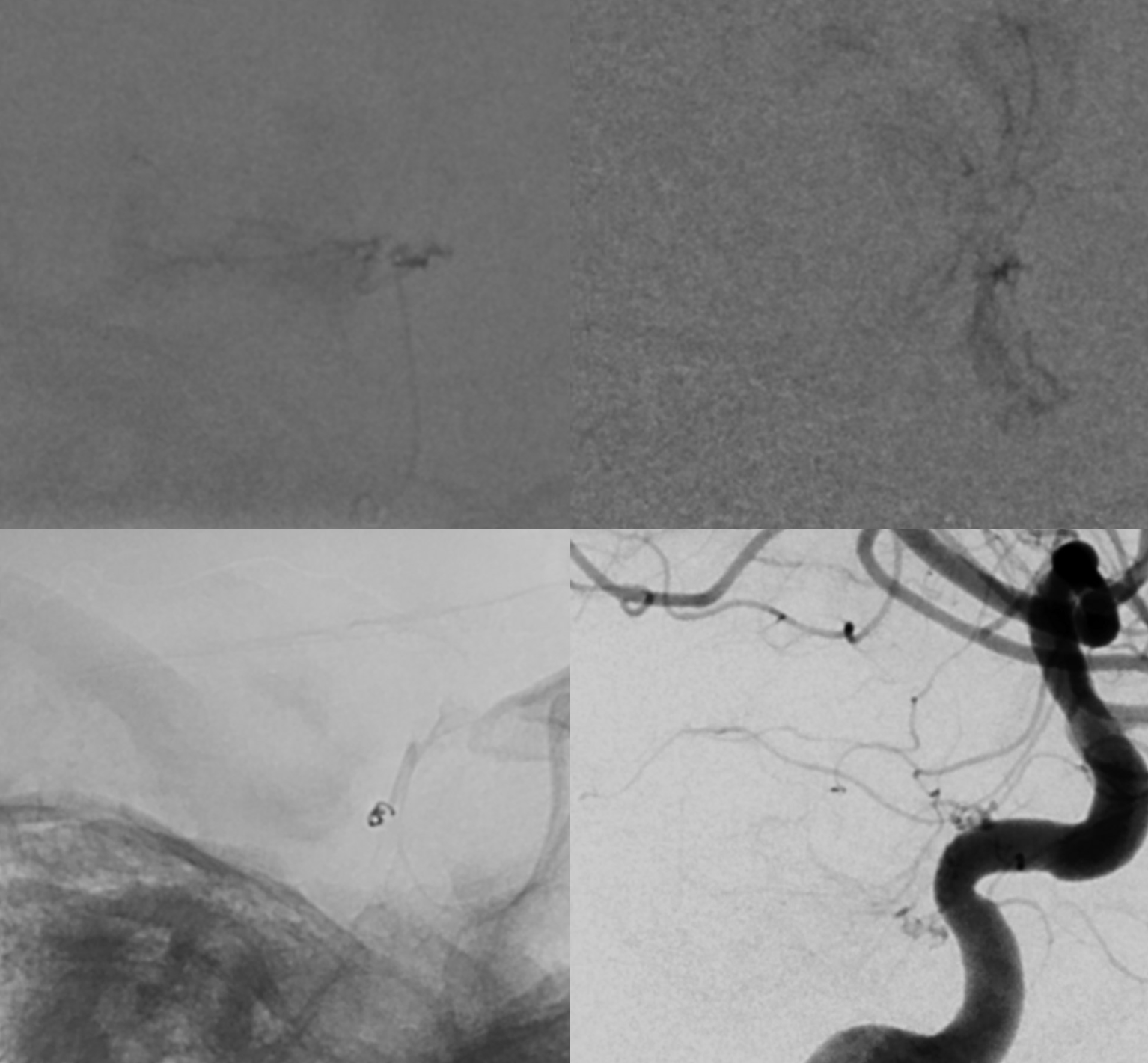
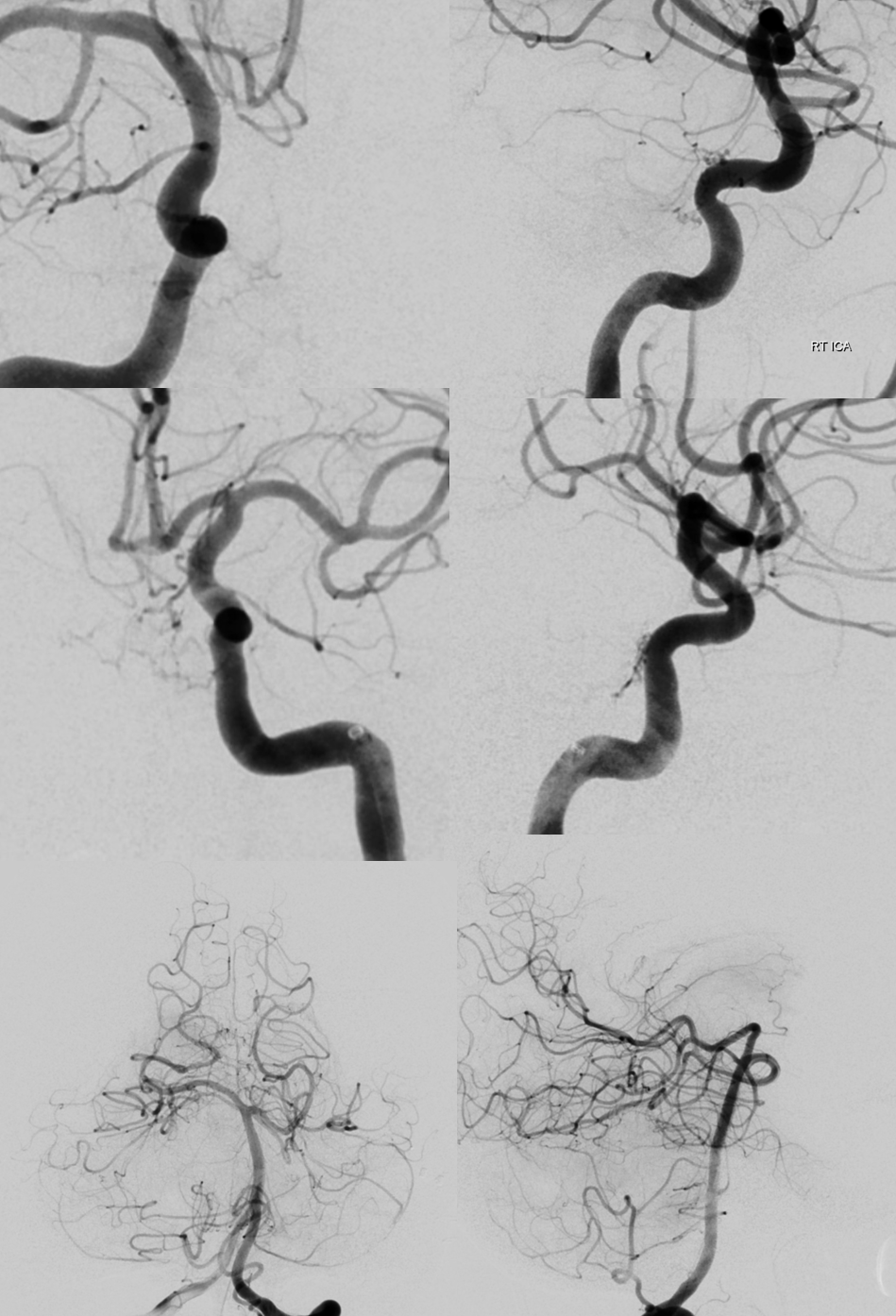
Posterior clival anastomoses MHT-MHT — almost seeing the right ICA — almost…
Smaller one of the two MHT pedicles is too small
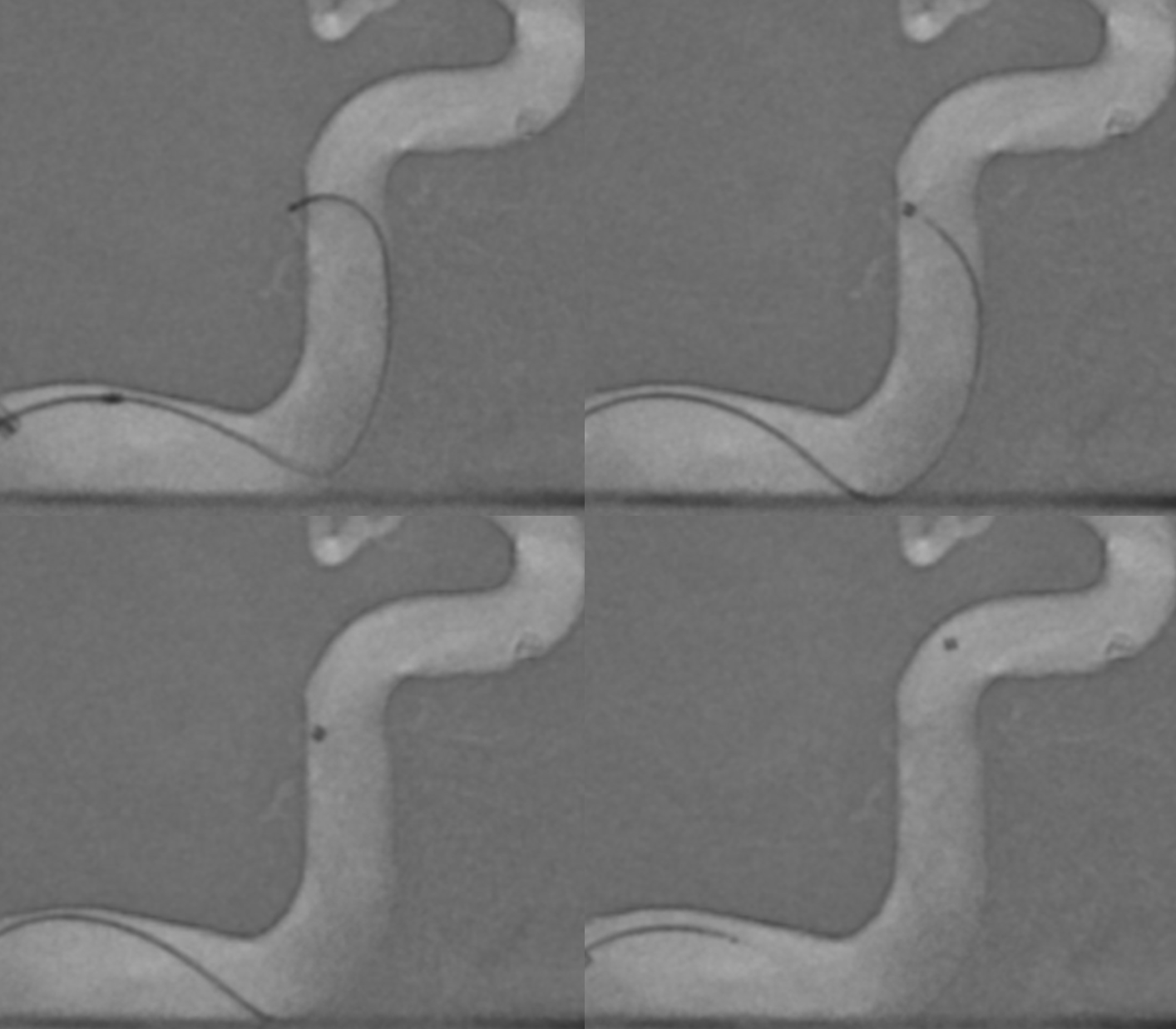
PCOM catheterization from P1 — wire goes in, but 1.2F catheter does not… there is a stenosis of the piodural branch at the proximal aspect (upper set of images). Closing the PCOM at the origin of the piodural branch is felt to be unworthy of the risk should the large thalamoperforator also go down…
Post embo
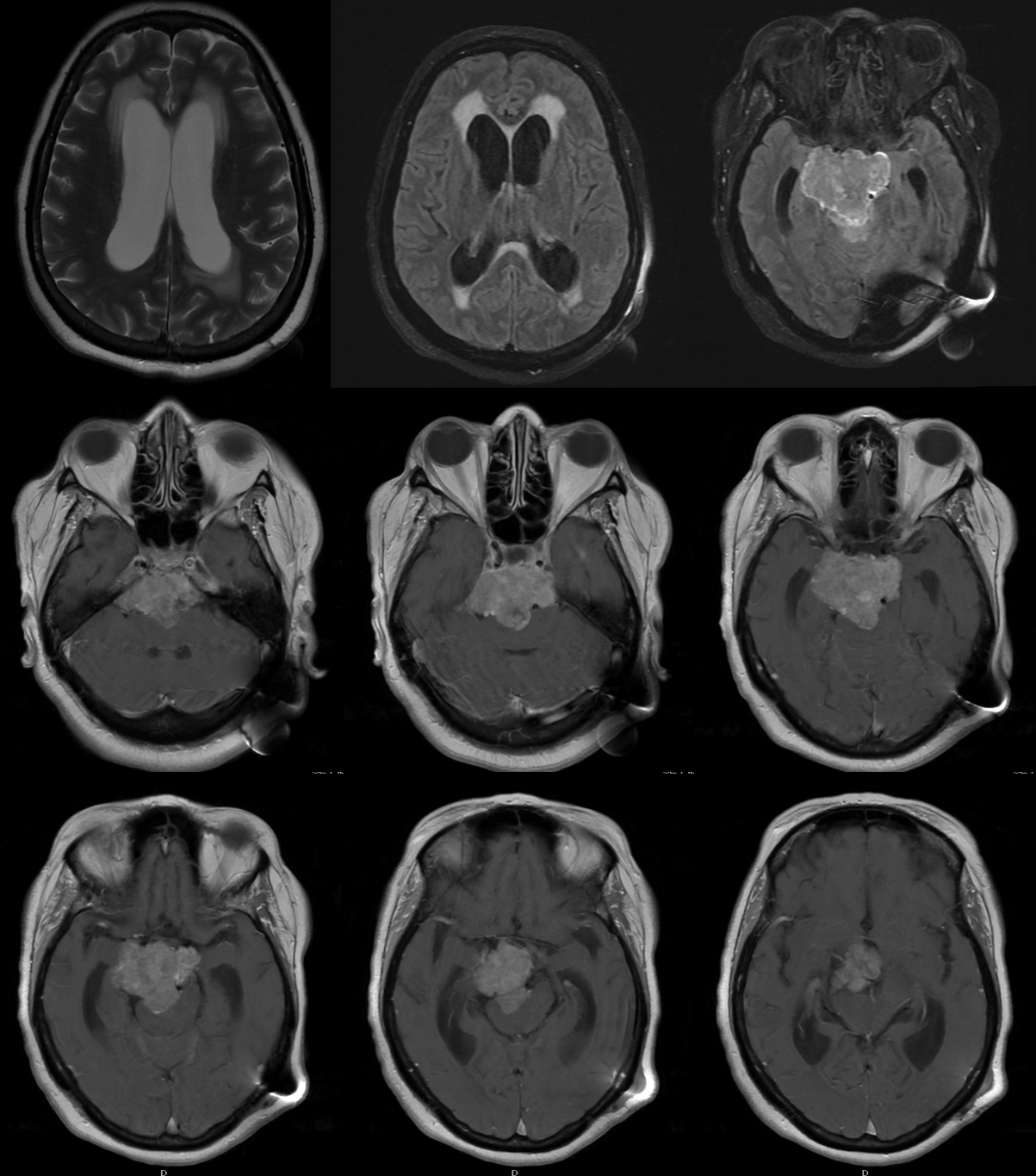
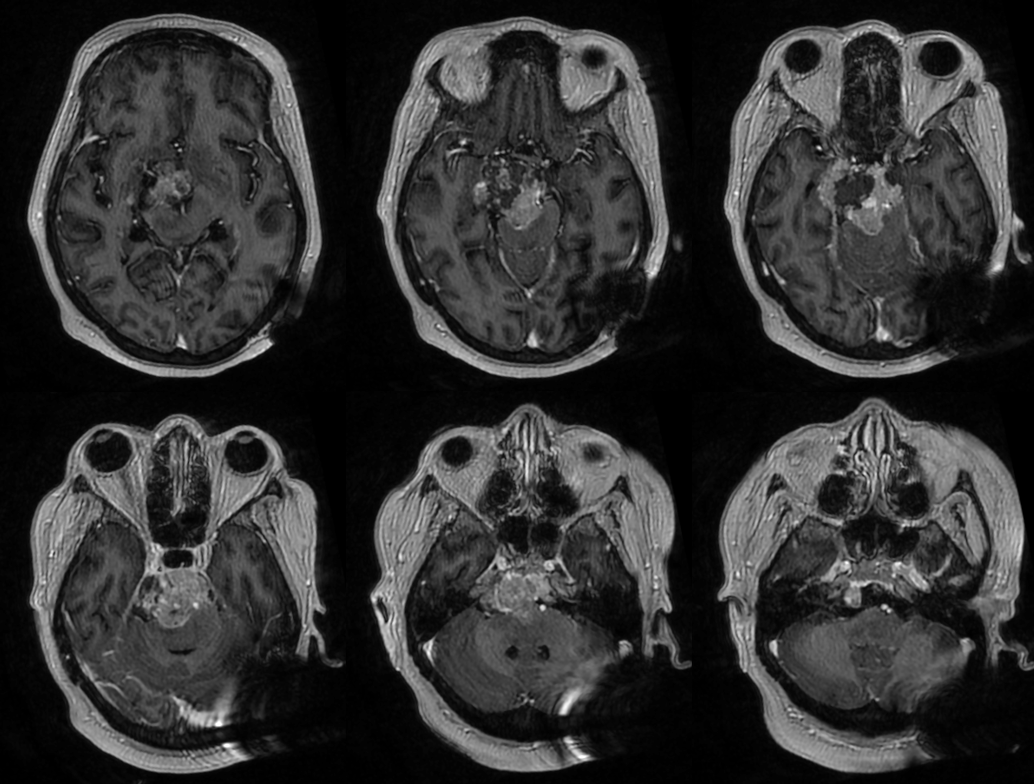
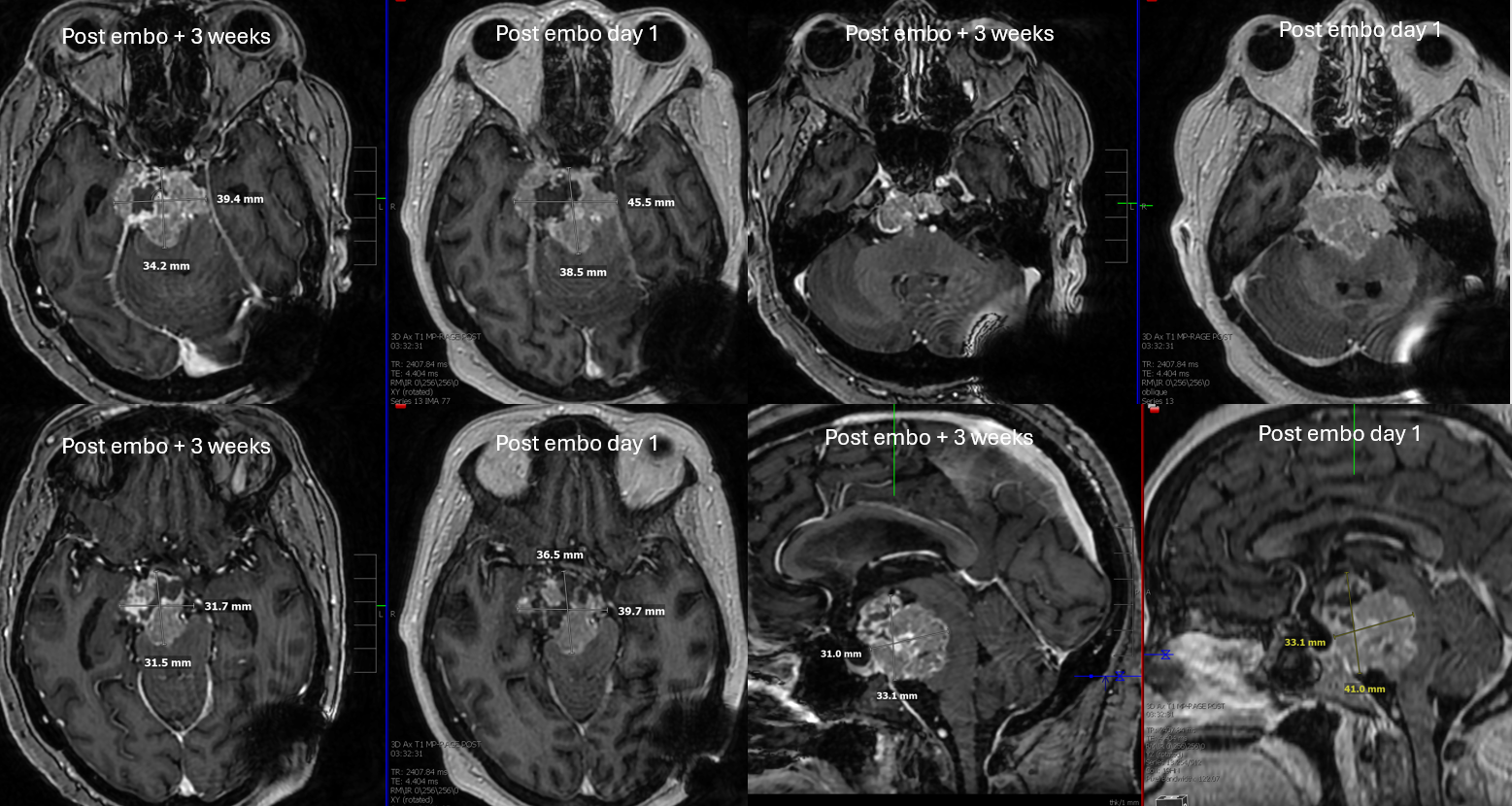
Post embo MRI — day 1. Central hypodensity due to post-embo necrosis.
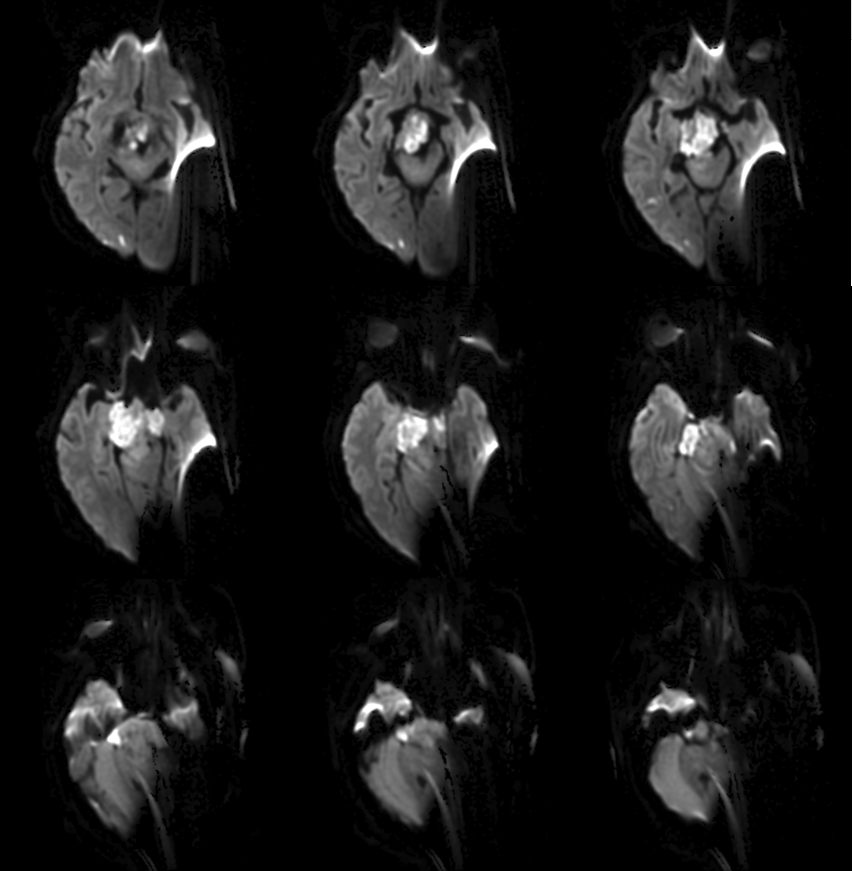
Diffusion restriction in the hopefully dead tumor
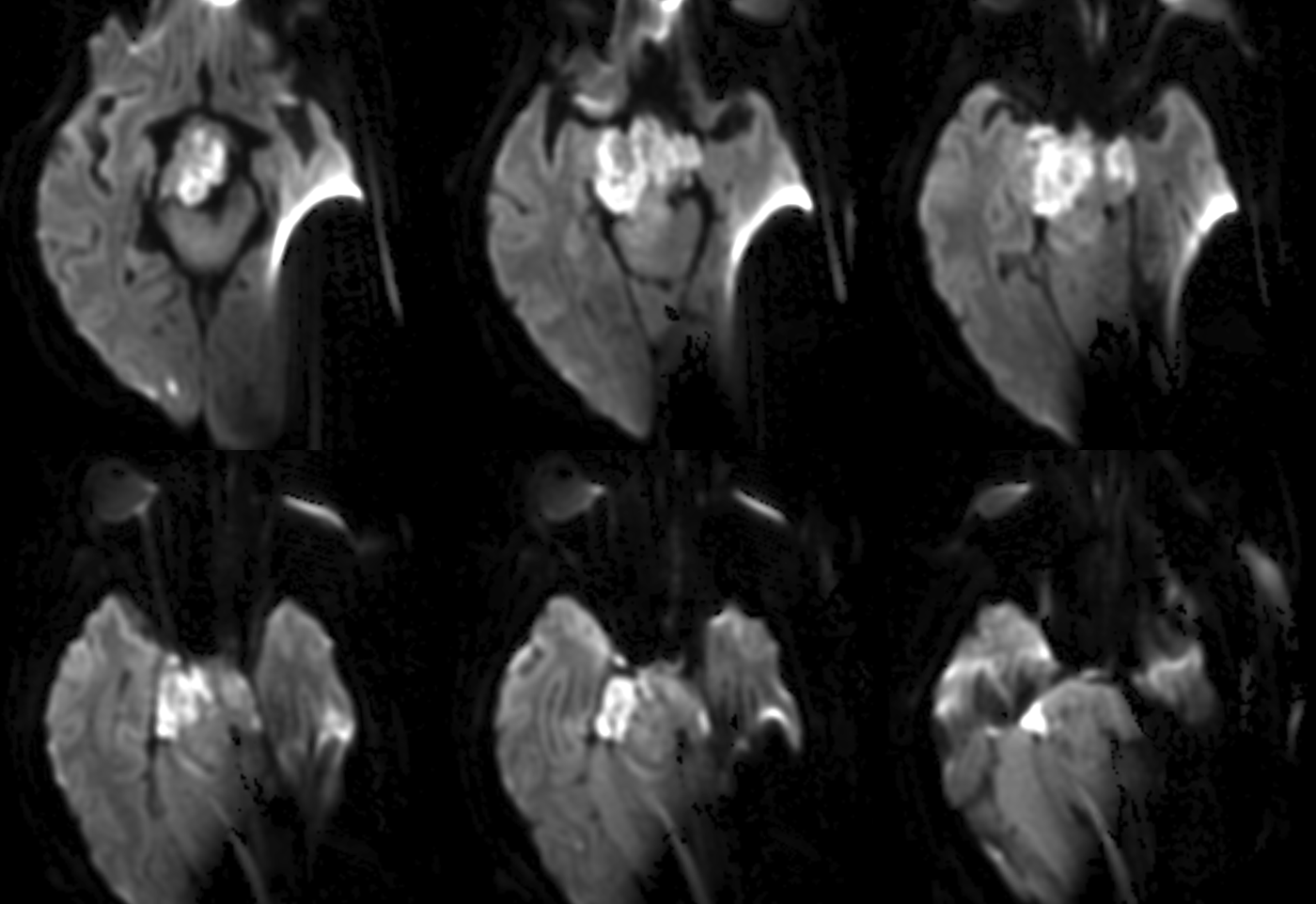
Surgery is delayed by 3 weeks. Fortunately another MRI is obtained just before resection. Still restricting diffusion
Interesting is post T1s. Note that the tumor has shrunk by a good amount
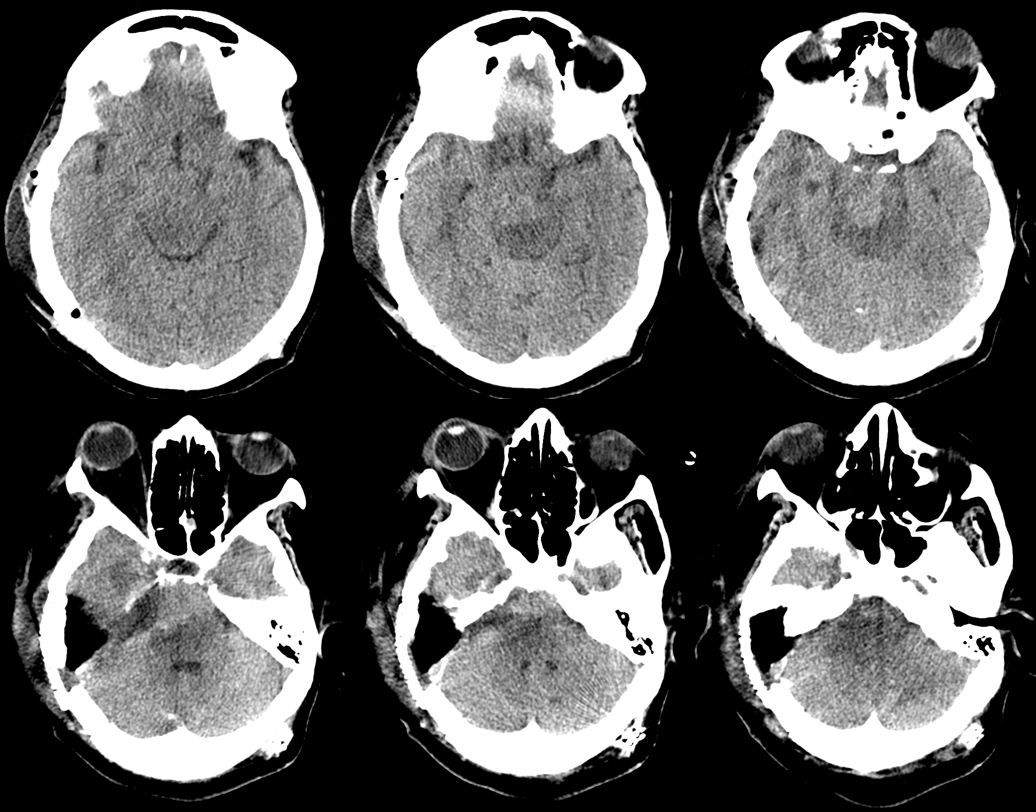
Post resection have a CT… but no matter — one can see there is a lot left behind
What happens later?