
Stab wound trauma with subsequent intermittent epistaxis over several weeks
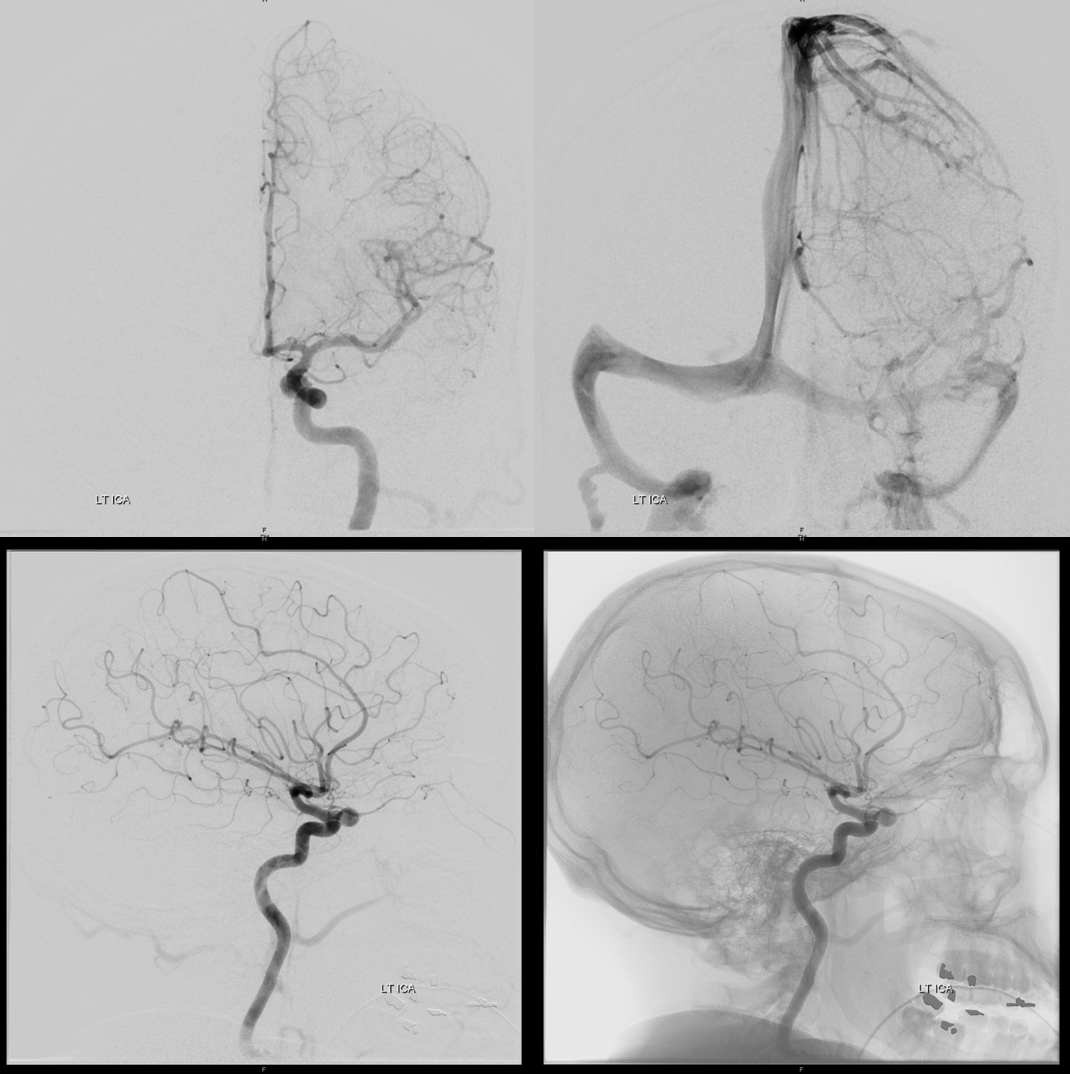
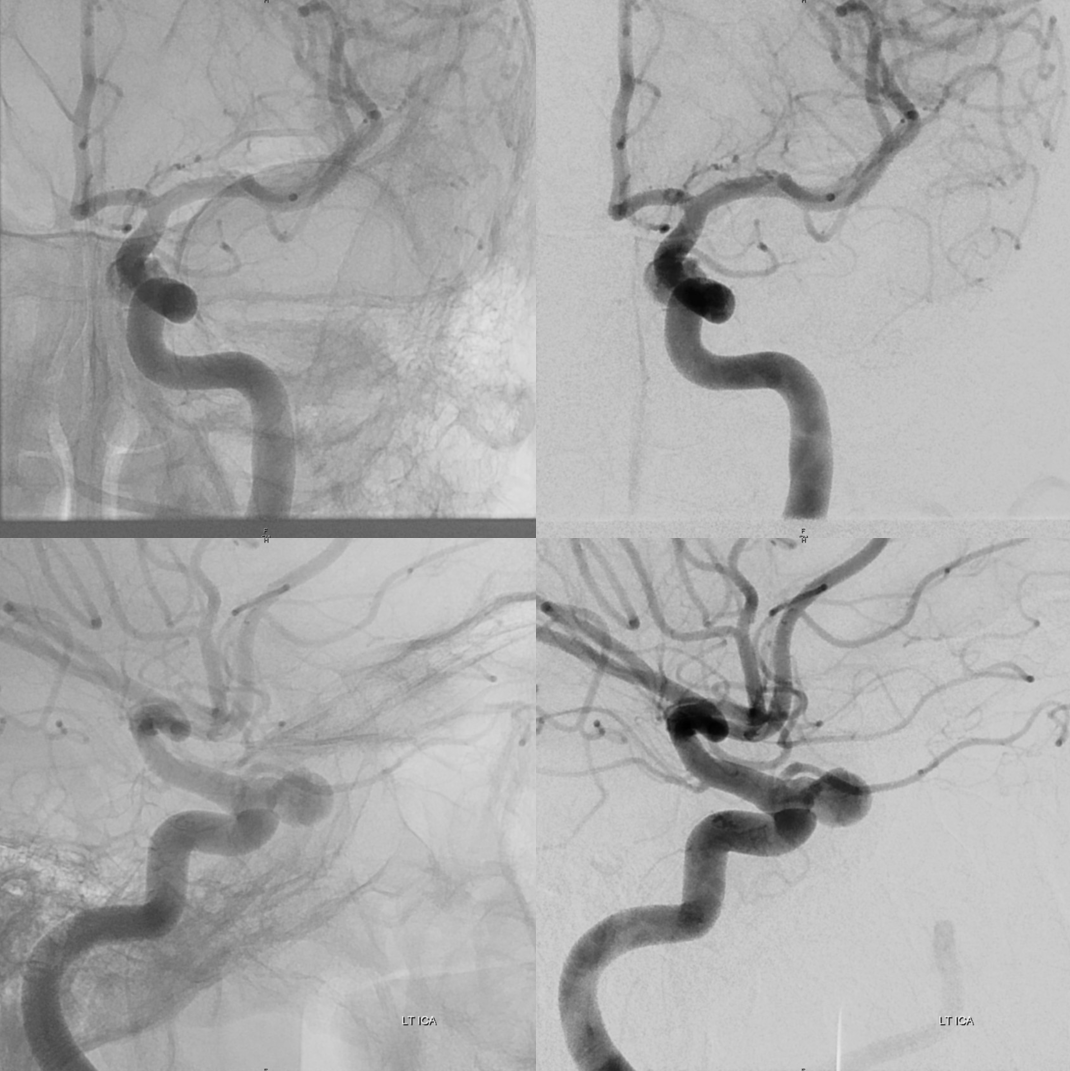
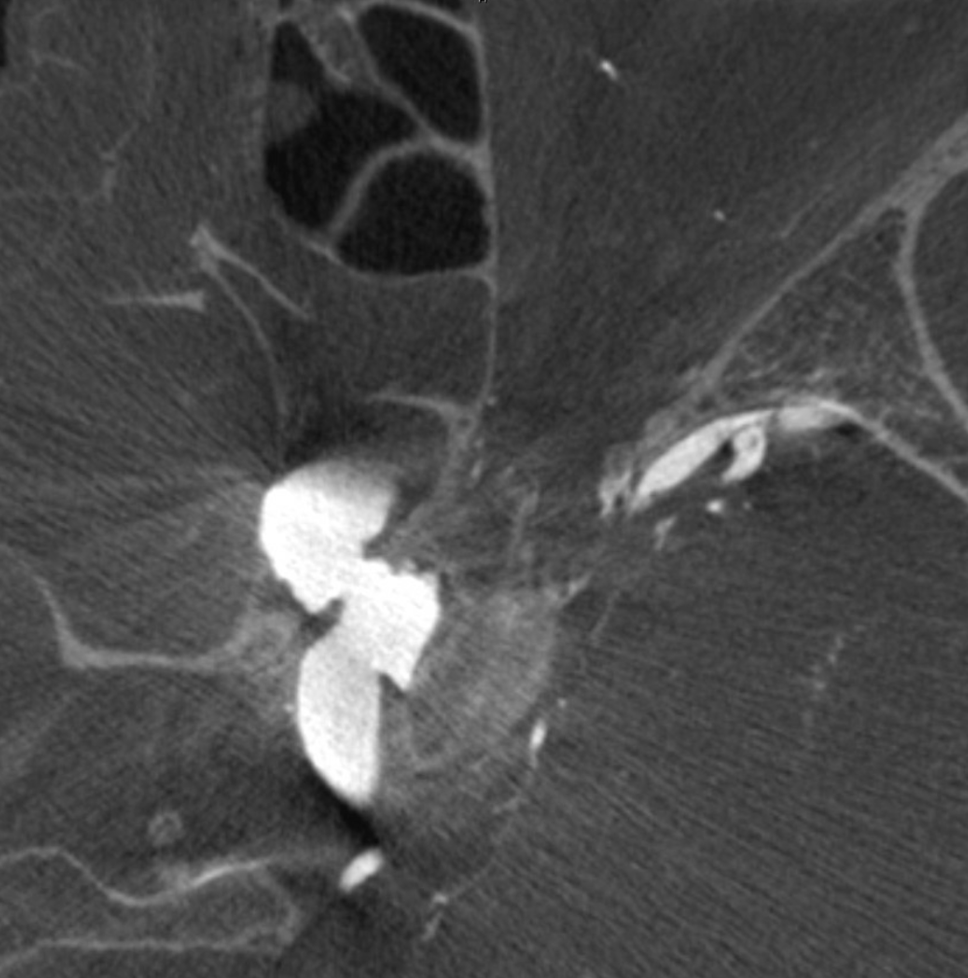
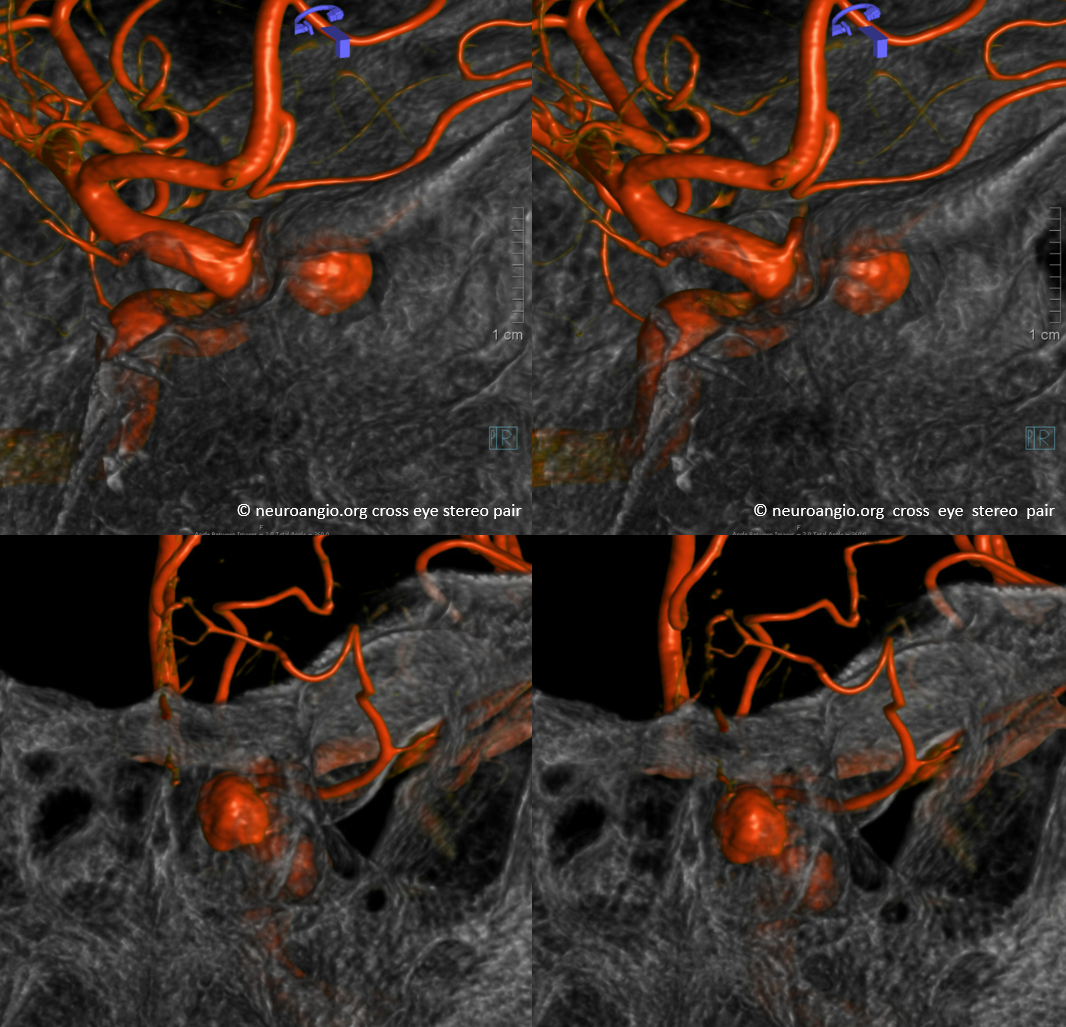
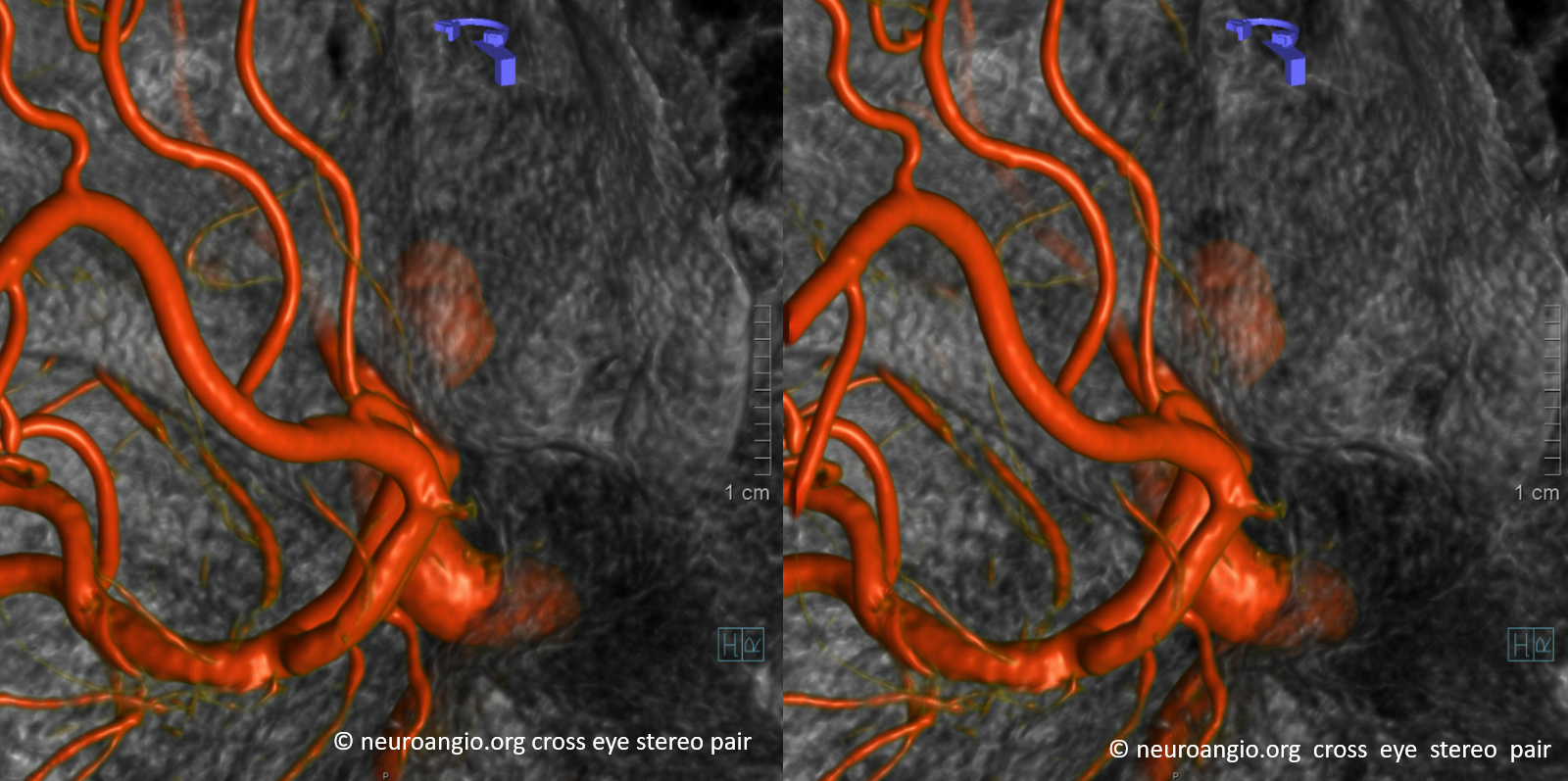
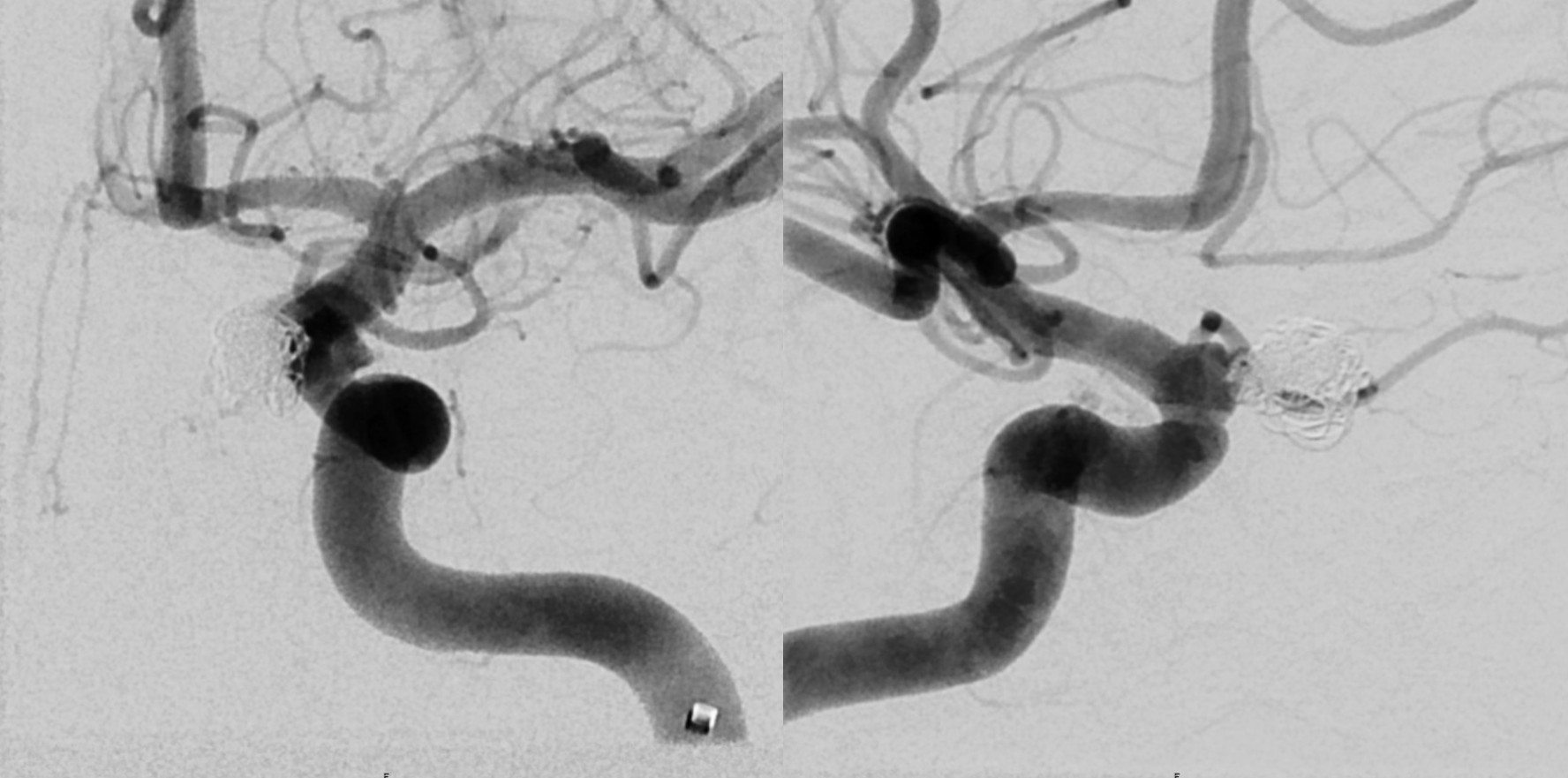
Both sphenoid sinus cells (larger right and smaller left) are damaged with multiple wall fractures. Miraculously, the pseudoaneurysm remains tamponaded and, after initial fairly large epistaxis, only intermittent bleeding was present.
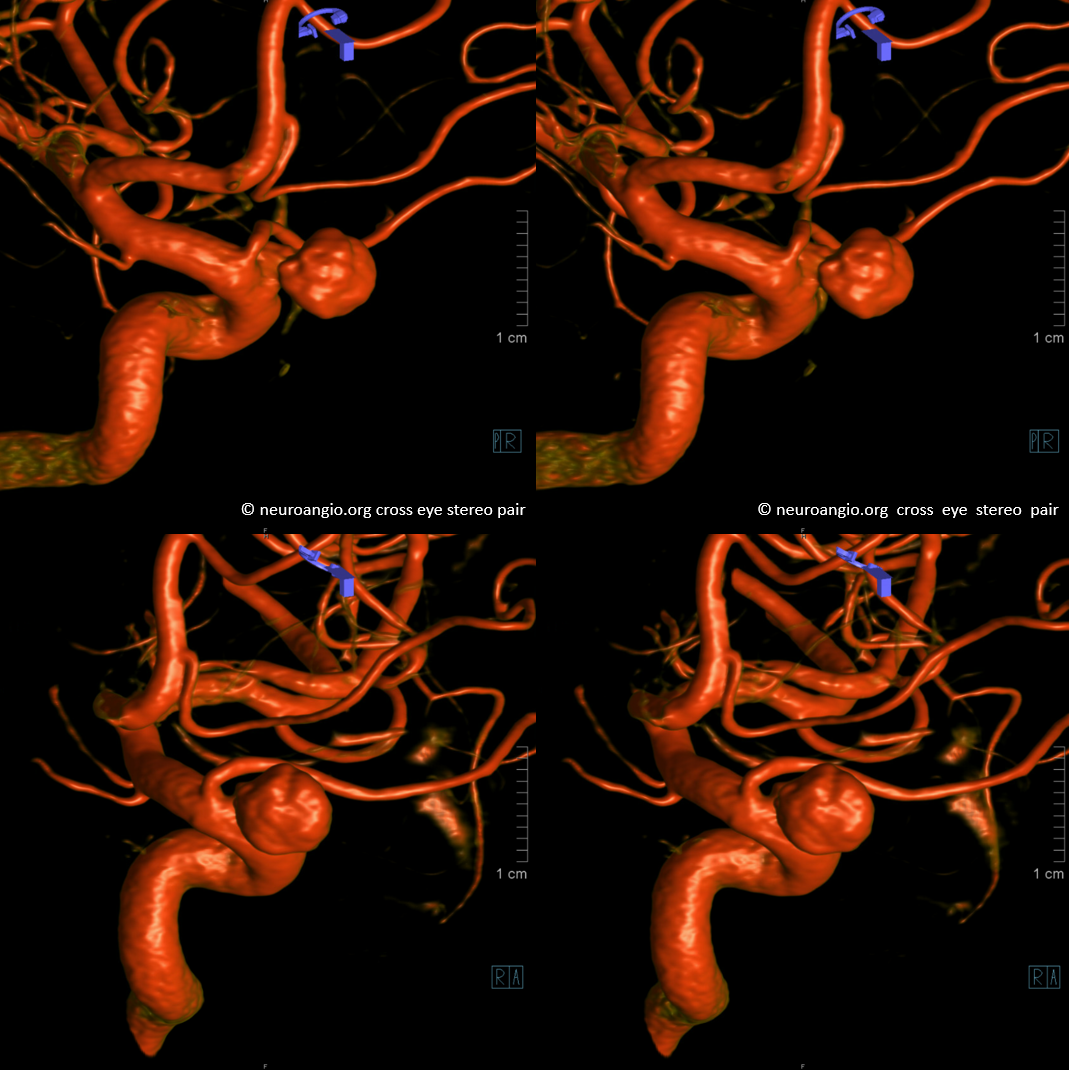
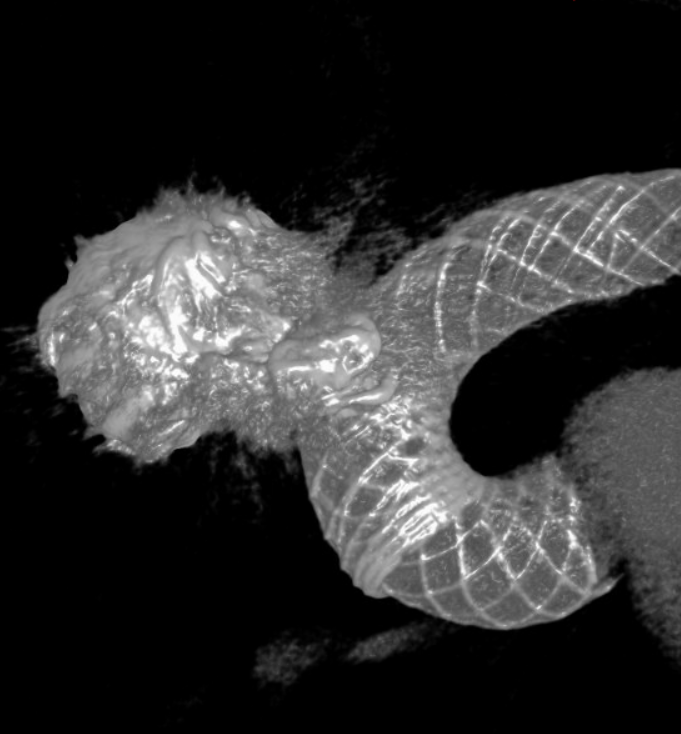
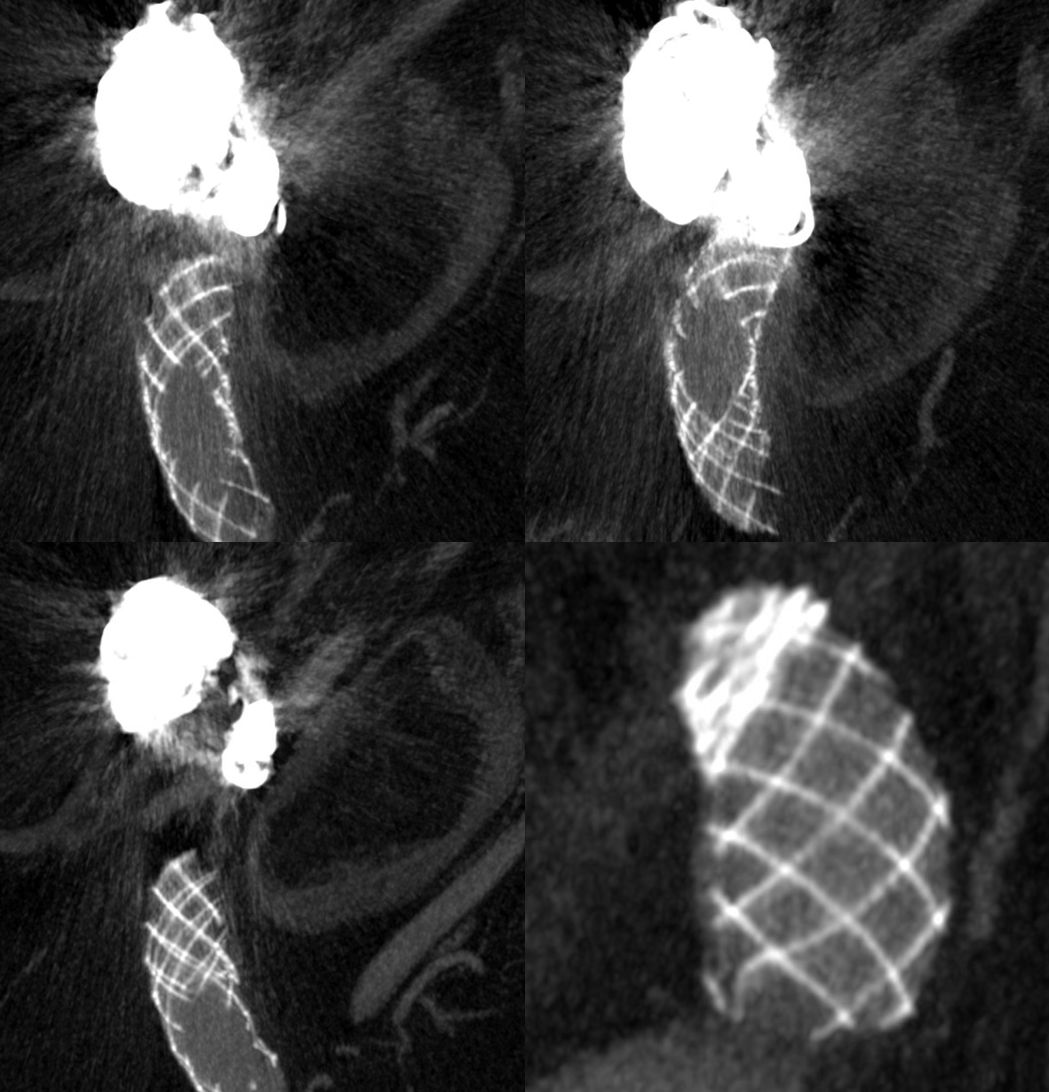
Look at the perfect online of the dural rings — wedge shaped — open anteriorly. The space between the rings is the “carotid cave“.
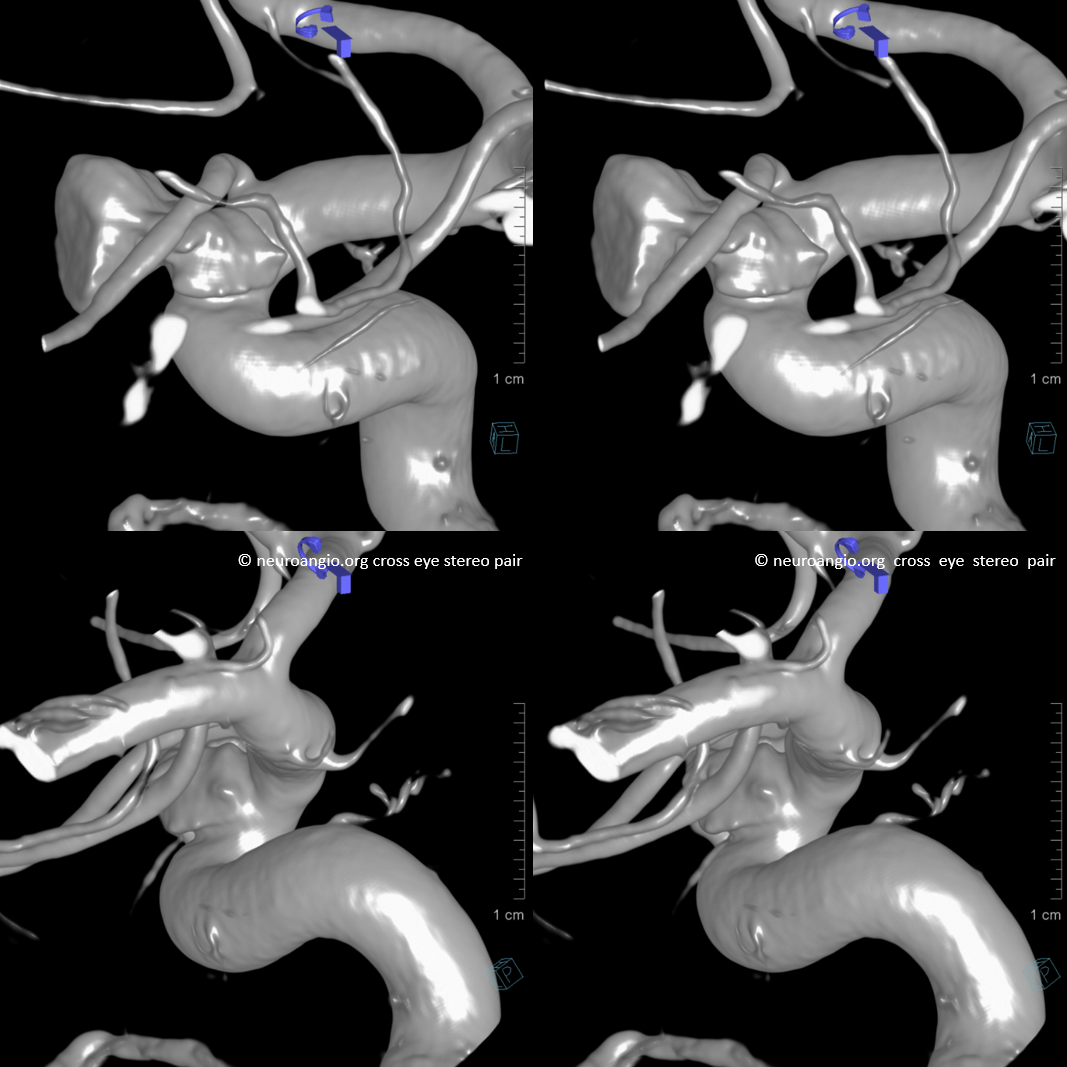
Solid and dashed arrows mark proximal and distal rings. Although the cave is a potentially intradural space, this case is one way to show that intrinsically it is not. A “true” saccular aneurysm may eventually erode the distal ring and extend into the intradural space, however most remain small.

Anaglyphs


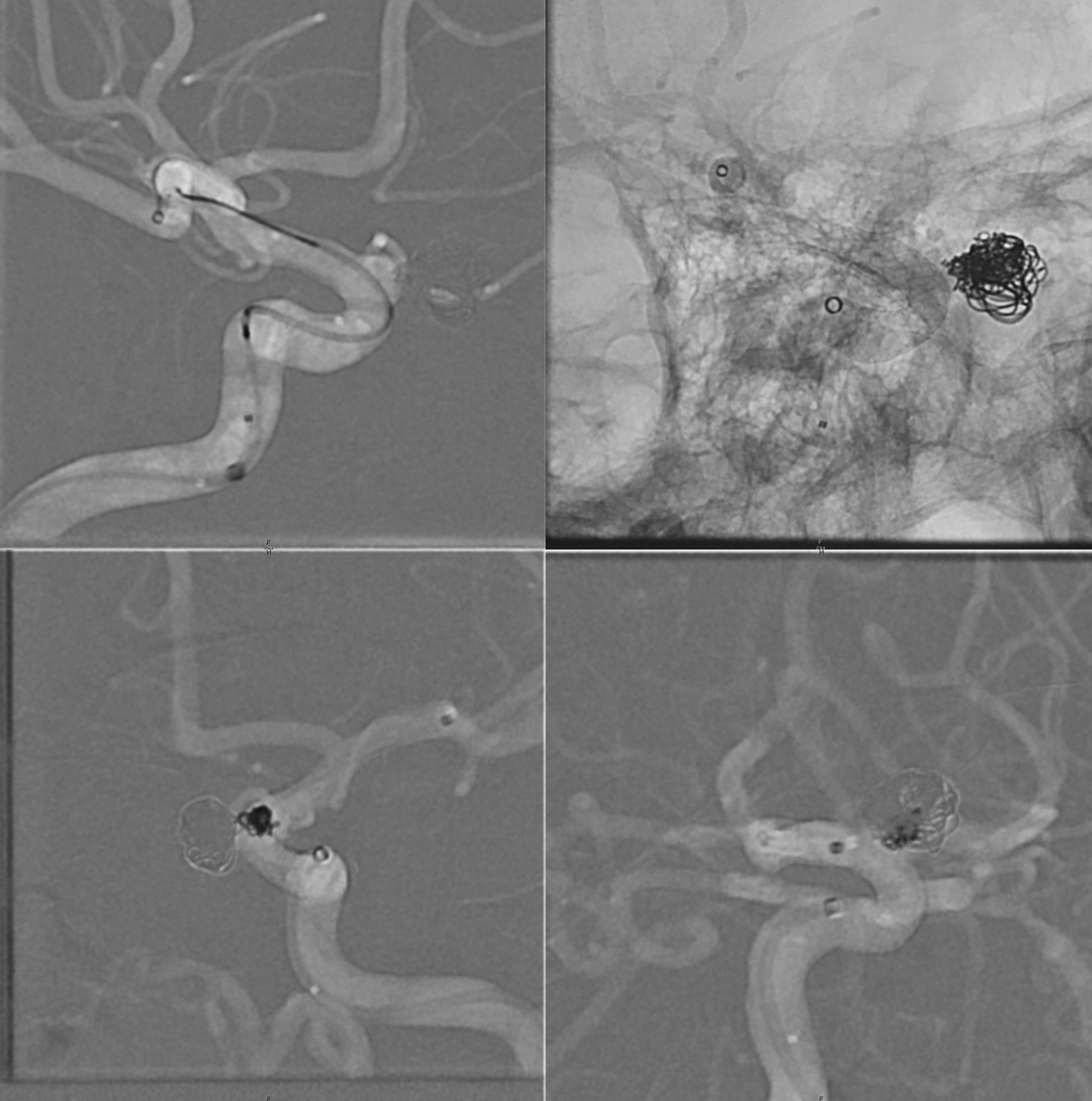
Treatment — BMX, Sofia 6F, Scepter 4×10 for protection in case it ruptures, SL-10 for coiling
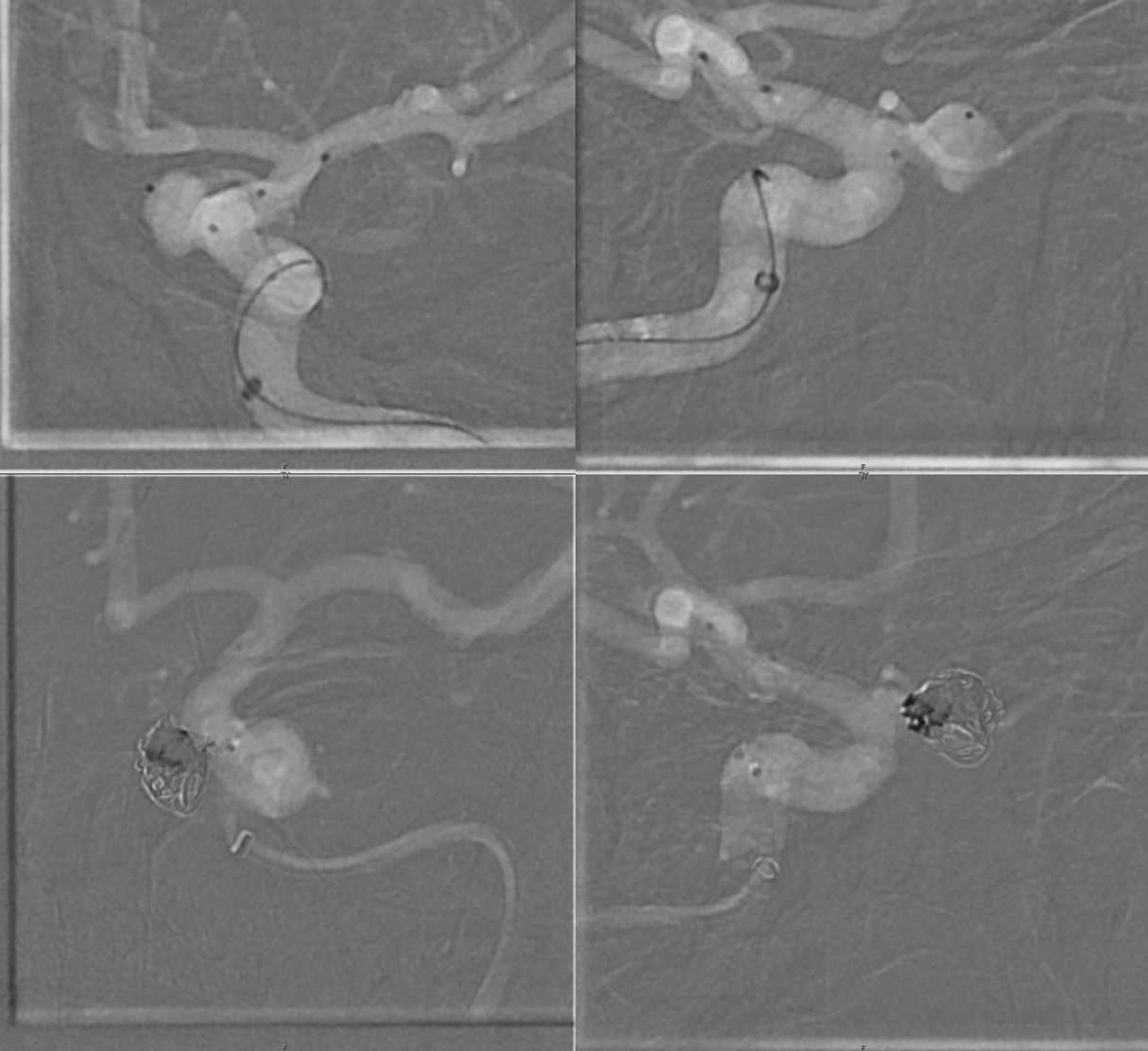
Post coil. The coiling is to temporize. It never worse as a long-term solution for pseudoaneursyms
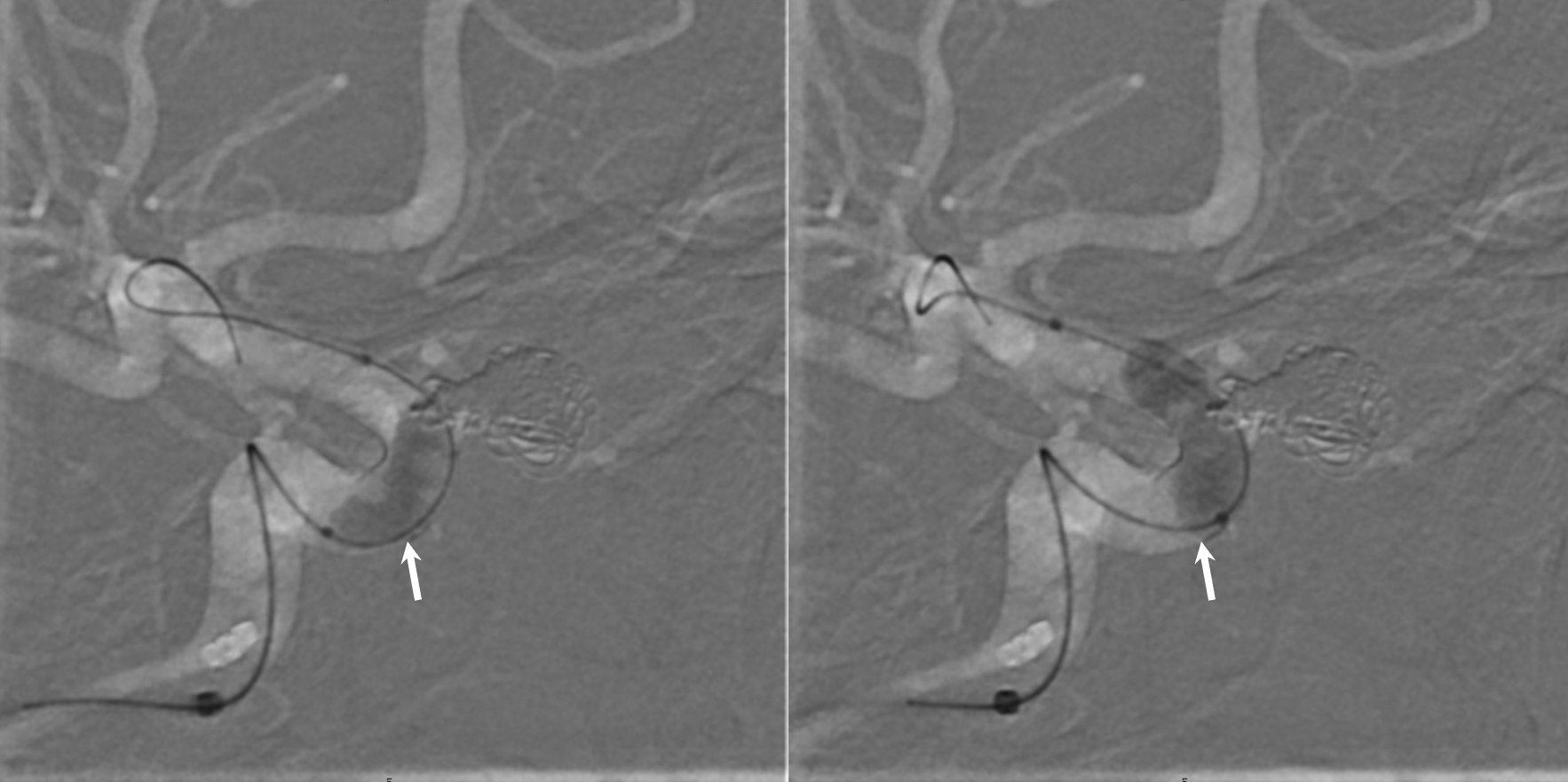
Step 2 — Remove Sofia, Scepter, and SL-10. Place a Phenom Plus, and Phenom 27 into M1. Place an SL-10 back into aneurysm from BMX — it fits alongside Phenom Plus. Deploy Pipe Shield 4.75×12 in this case (Give integrilin just before deployment). Coil whatever more pseudoaneurysm can be coiled (small nanos).
Take out SL-10. Balloon Shield — it needs to appose vessel nicely after SL-10 is out — and did, but we ballooned anyway to be sure. See how distal end is now in a much better spot — more distal, better apposed than before? Can also be seen as increased coverage of the proximal portion.
Place another Pipe shield for double coverage. 5×10 would have been ideal — but thats history now. So we did a 5×14
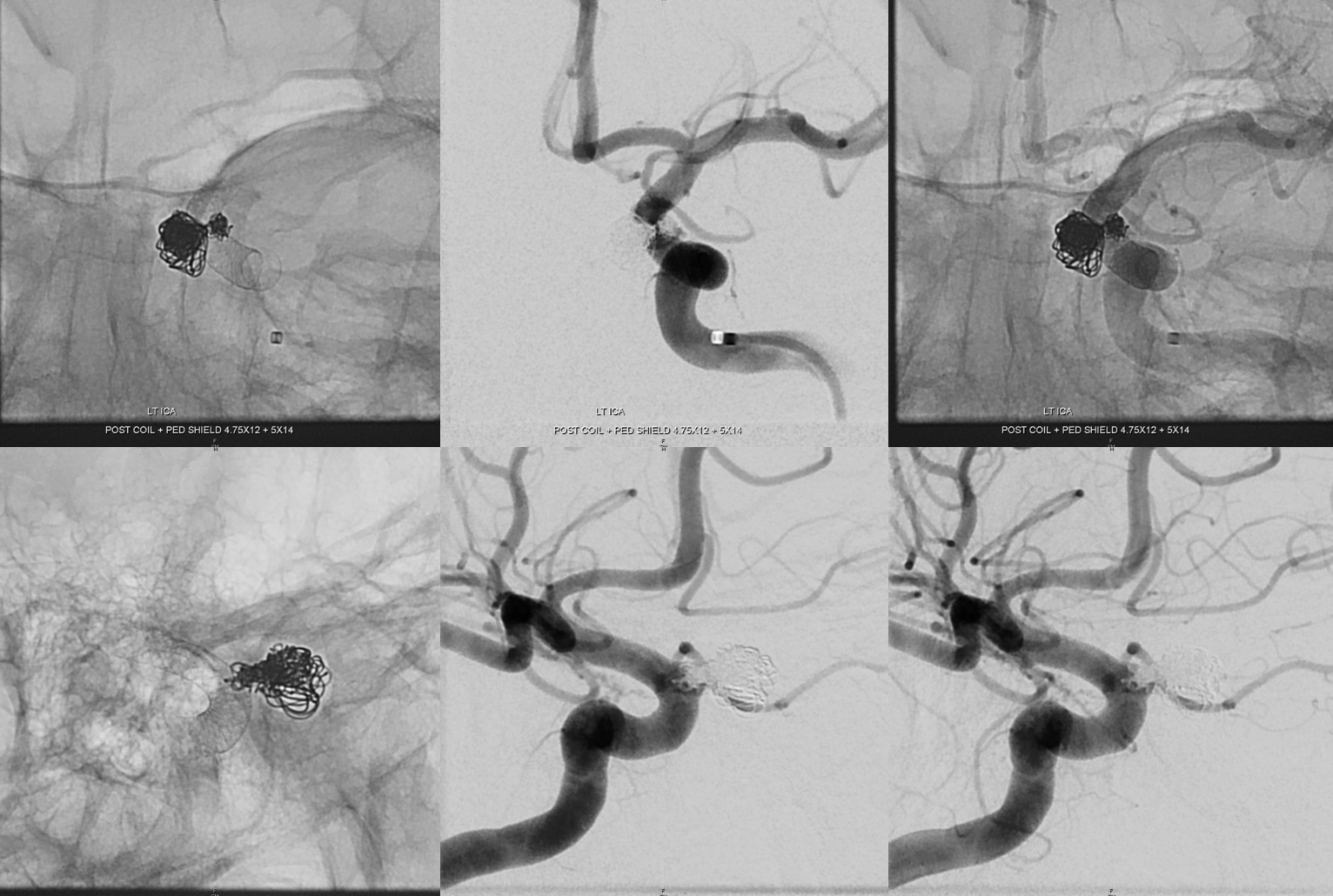
A lot of very interesting information is in these post DYNAS
For more info on carotid cave, see ICA and its aneurysms page