
Venous sinus stenosis is the most under-recognized cause of pulsatile tinnitus. Venous sinus stenosis, particularly of the sigmoid sinus, is common and, in vast majority of cases, asymptomatic. Which is why it is usually overlooked on imaging studies. Many patients ultimately proven to have venous stenosis as a cause of PT have had their studies interpreted as normal. How to avoid this problem? You need history and physical exam info.
- Is the sound unilateral? In the vast majority of times, the sound is on the side of the dominant sinus.
- Can the sound be abolished by ipsilateral jugular compression? Jugular compression is an extremely sensitive and specific maneuver in diagnosis of venous pulsatile tinnitus. Compression of the jugular vein stops or markedly reduces flow in the entire ipsilateral transverse/sigmoid/jugular conduit. It is a simple and under-utilized test.
So, if a patient has PT on the side of a dominant transverse/sigmoid sinus stenosis that they can suppress by jugular compression, it is extremely likely that stenosis is the cause.
Other causes of venous PT also respond to jugular compression — for example, jugular plate dehiscence or sigmoid diverticulum. It should be noted that diverticula and high-riding bulbs are frequently sited as causes of PT. It is difficult to prove however that they are, unless the diverticulum can be selectively occluded. In many instances there is an associated stenosis which is the primary cause an the diverticulum is part of post-stenotic dilatation.
Below is a range of imaging findings in venous stenosis.
You don’t need an MRV or a CTV to diagnose venous sinus stenosis. A contrast MRI will do just fine. All but the worst quality contrast MRs will show it. A modern, volumetric post-contrast T1 makes MRV pretty much obsolete.
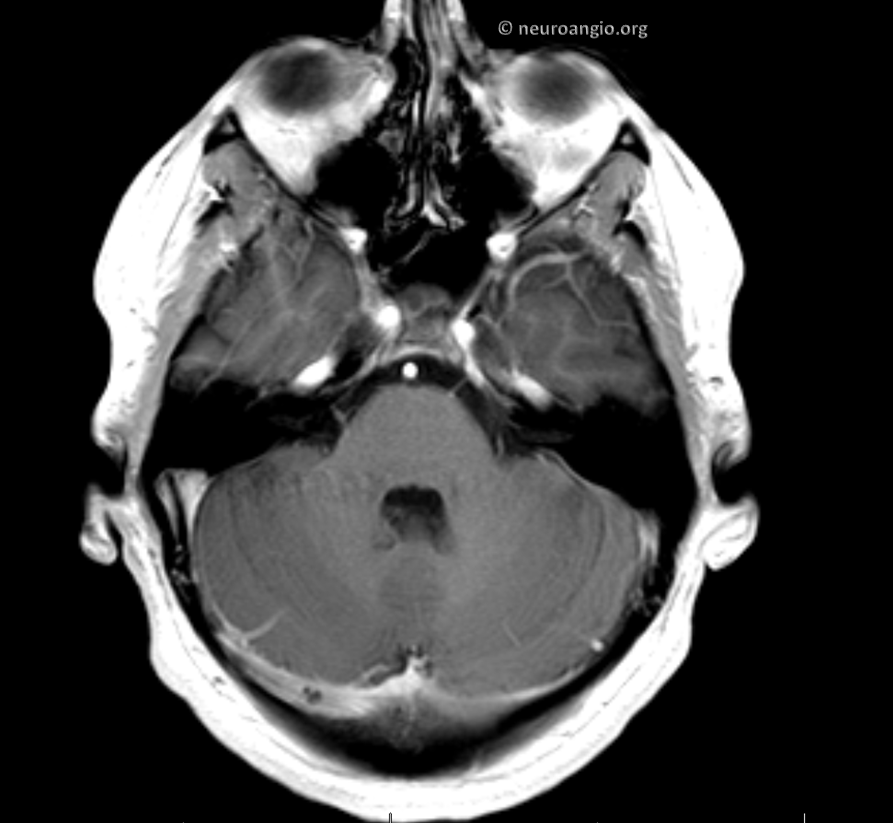
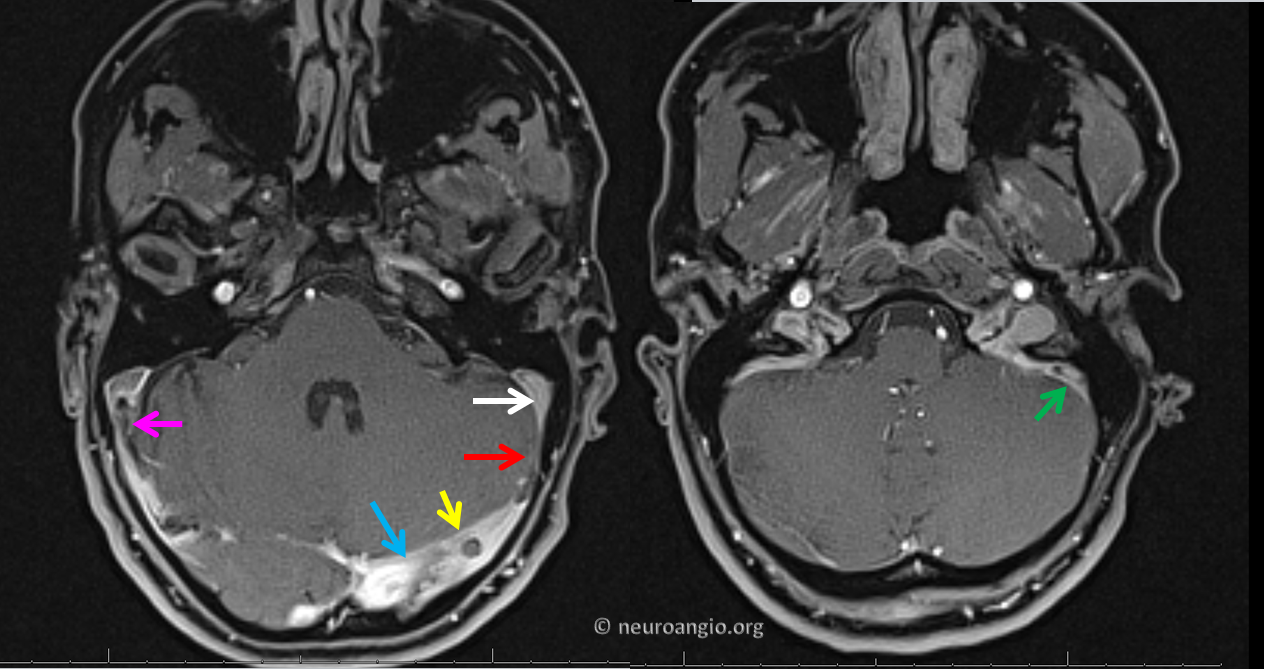
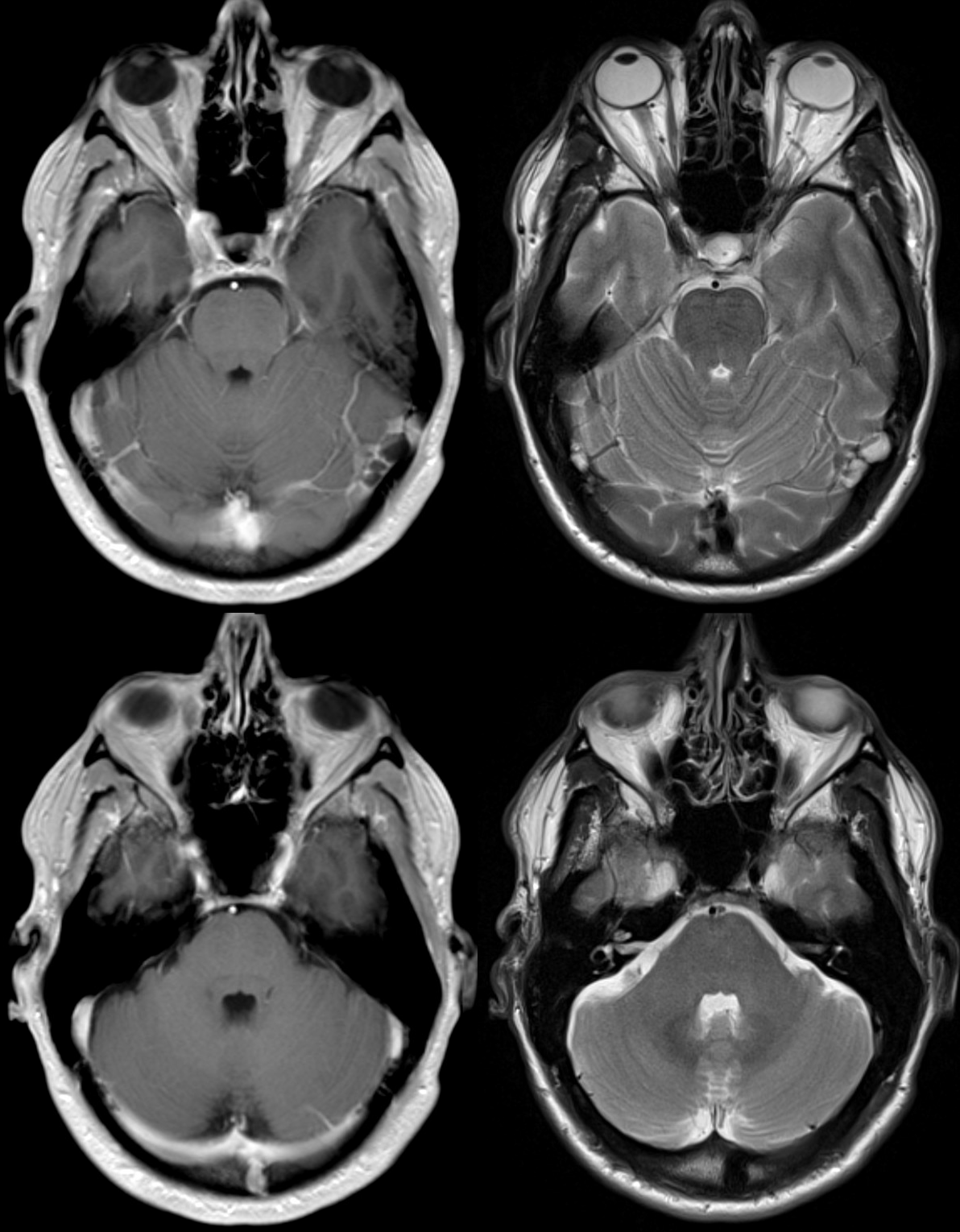
Here is a typical postcontrast axial MRI. Its a Siemens volumetric “MP-RAGE”. Usual right sinus dominance. The transverse (blue) and sigmoid (white) sinuses are normal. There is a severe proximal sigmoid sinus stenosis present (red). A flow jet atrifact at location of stenosis (green) is an inconstant and unpredictable finding, varying widely based MR equipment manufacturer, sequence parameters, etc. Nevertheless, it is an intriguing and helpful finding that makes intuitive sense for patients with pulsatile tinnitus.
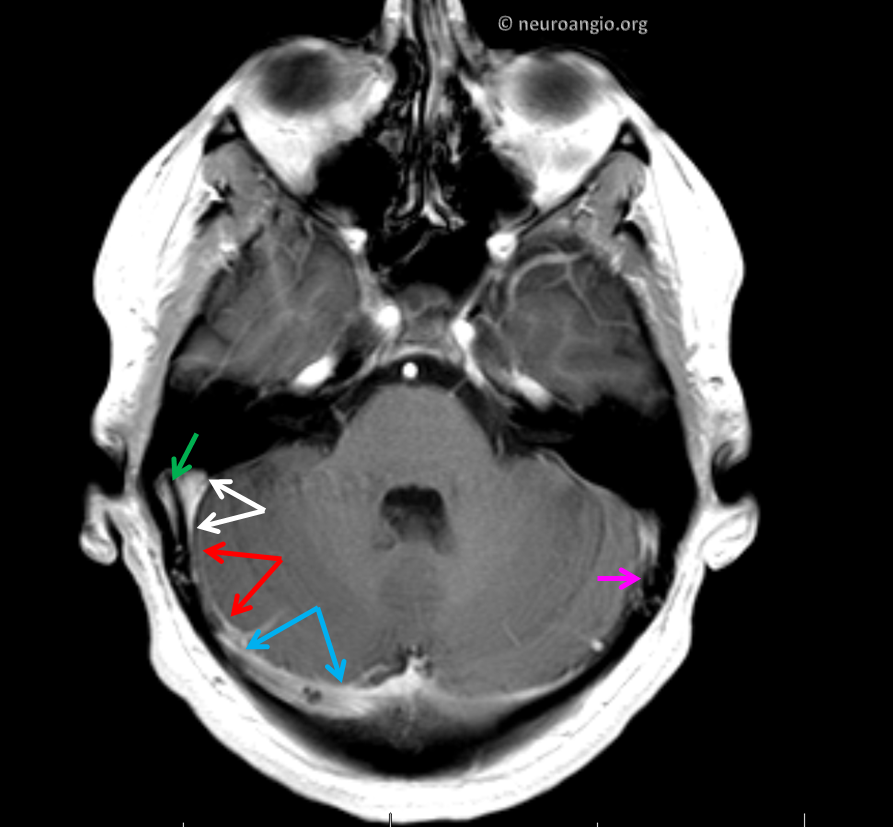
Here is a thick section T1. Classic findings of severe distal sigmoid sinus stenosis (red) with normal cailber sigmoid (white) and transverse (blue) sinuses. There is as good a flow jet artifact as you can get (green). Notice also mirror image flow jet on the left (purple). As usual, the pulsatile tinnitus is on the side of the larger sinus
A CT of the same patient is shown on the left, next to the MRI. We all know that water shapes stone. Certainly, blood flow shapes bone. Years of jet flow have remodelled the temporal bone to produce a diverticulum (blue). In fact, if you pay attention you will notice that lots of diverticula have an associated stenosis just upstream.
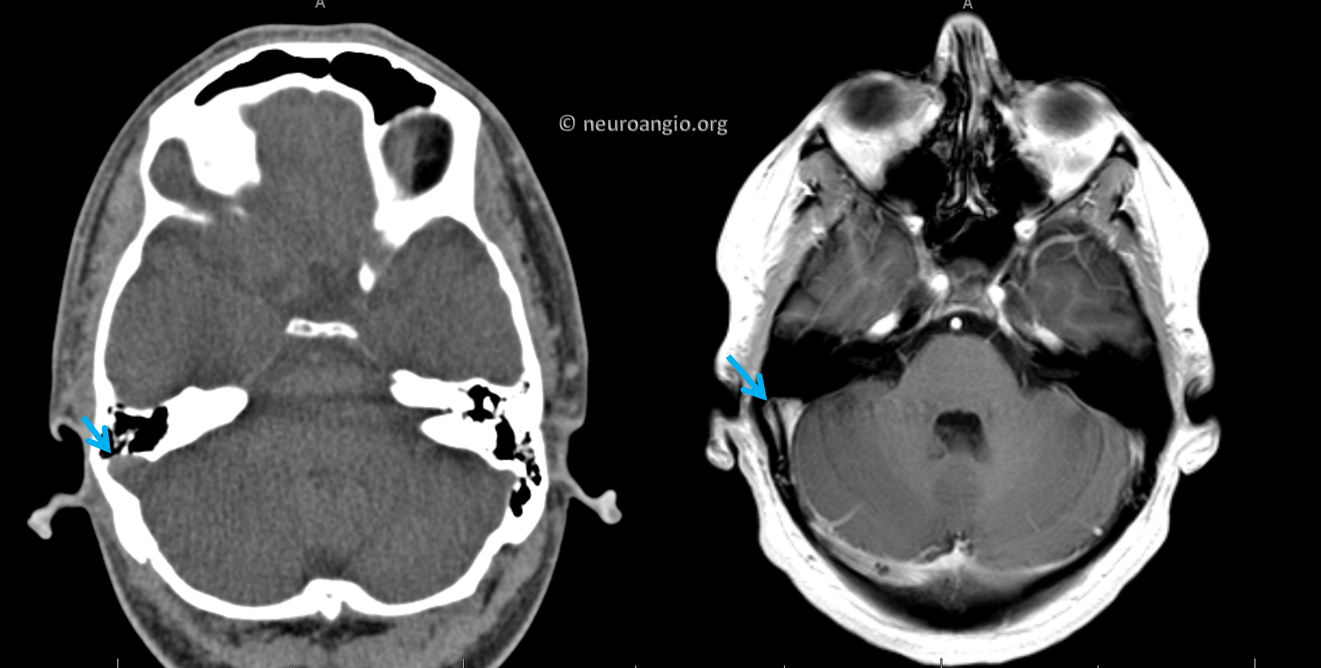
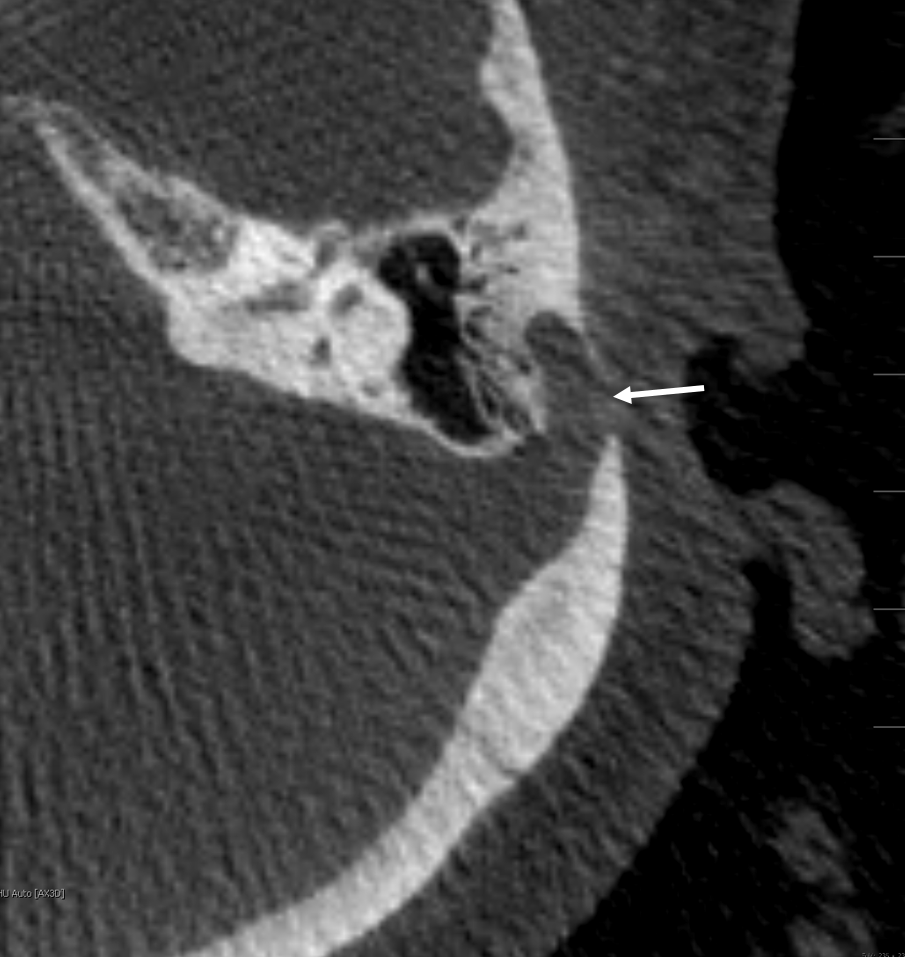
Thin section temporal bone CT shows some pretty impressive thinning of the mastoid petrous bone lateral to the sinus.
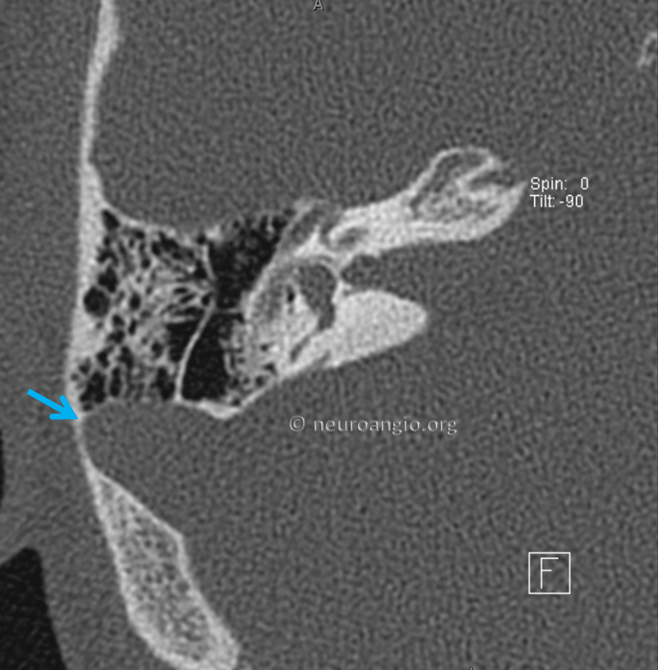
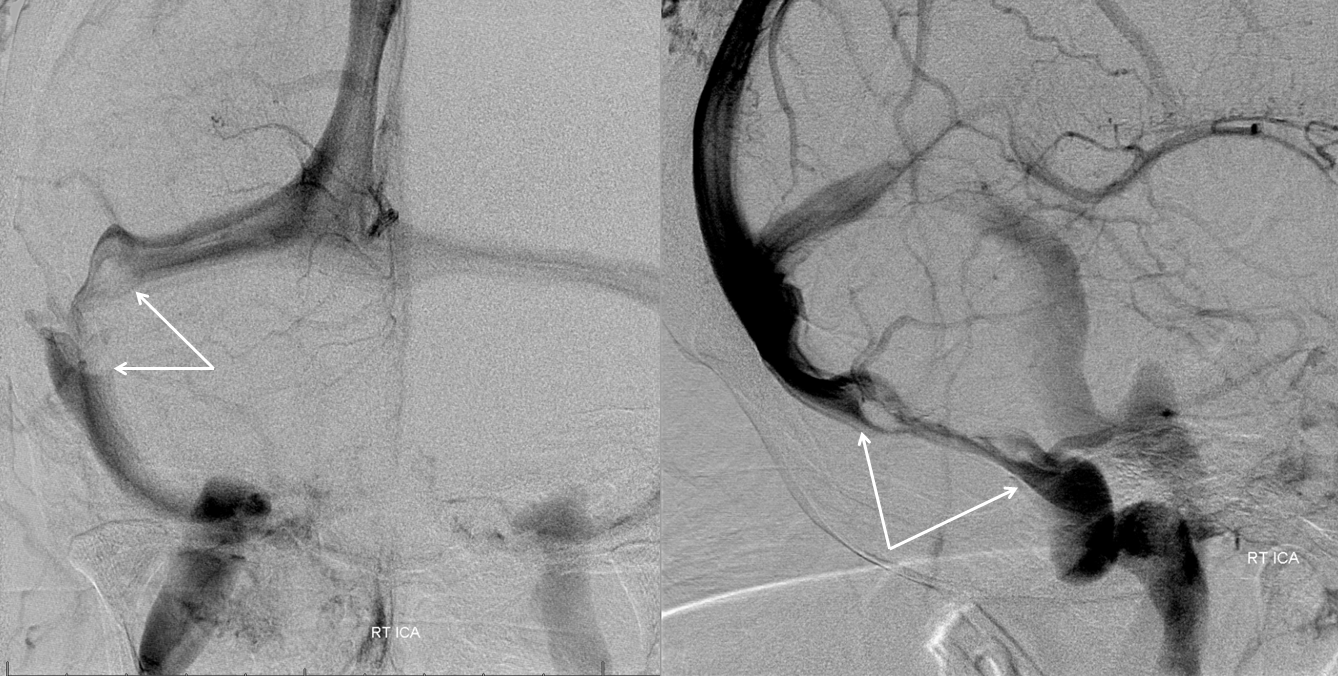
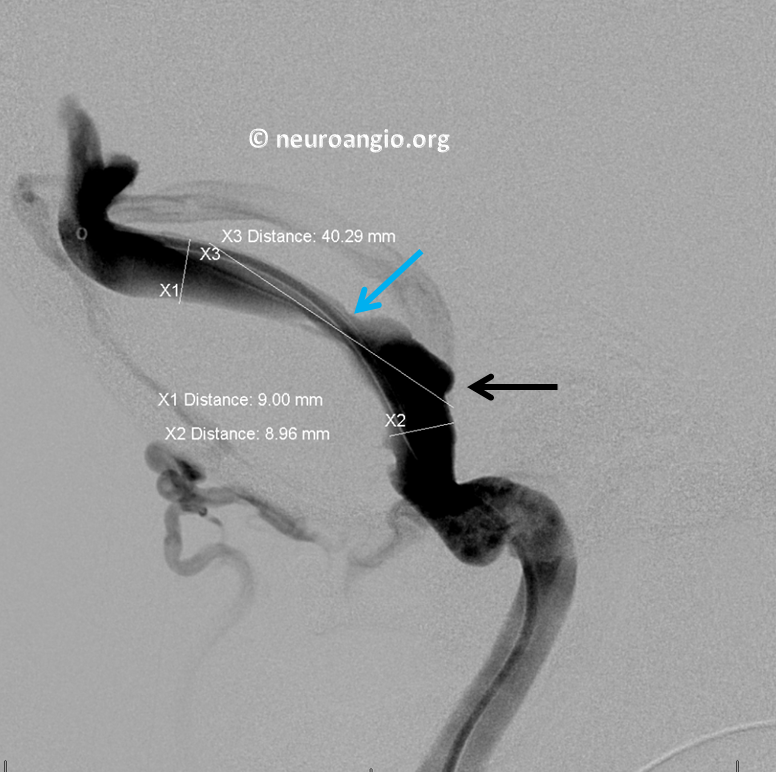
Below is an example of a really large diverticulum, remodeling the temporal bone, on a “DYNA CT” — modern angiographic version of temporal bone CT
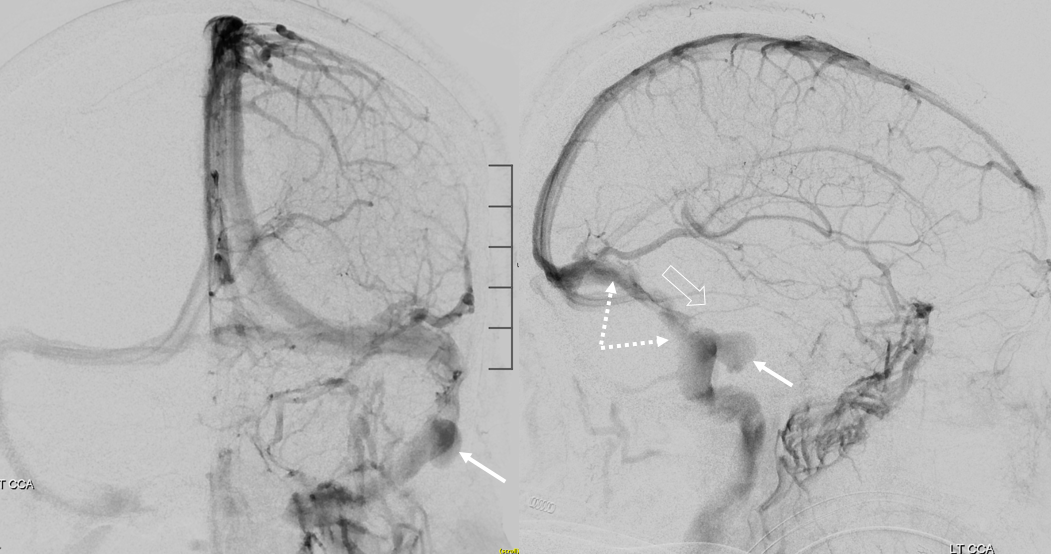
The angiogram shows the diverticulum (arrows). However, the primary problem is the stenosis (dashed arrows). The direction of blood flow, impacting temporal bone and sculping out the diverticulum, is shown by open arrow
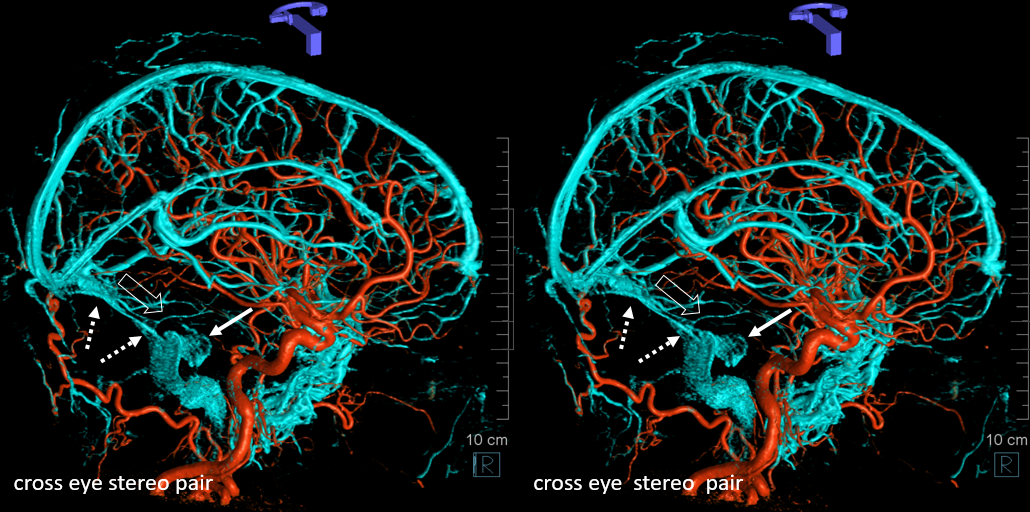
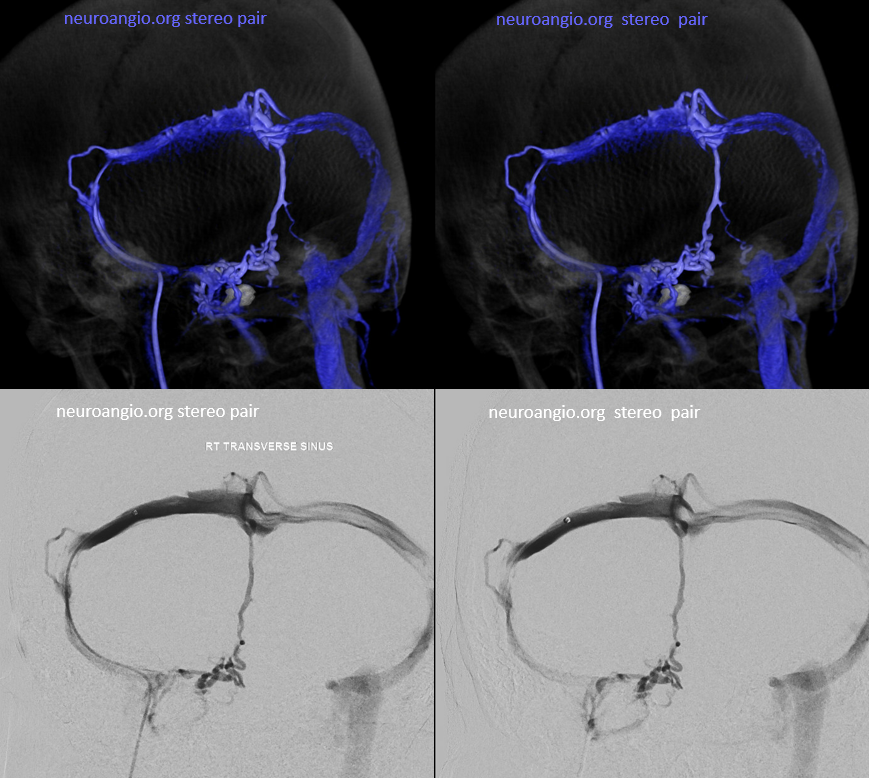
Cross eye stereo pair images of the same patient
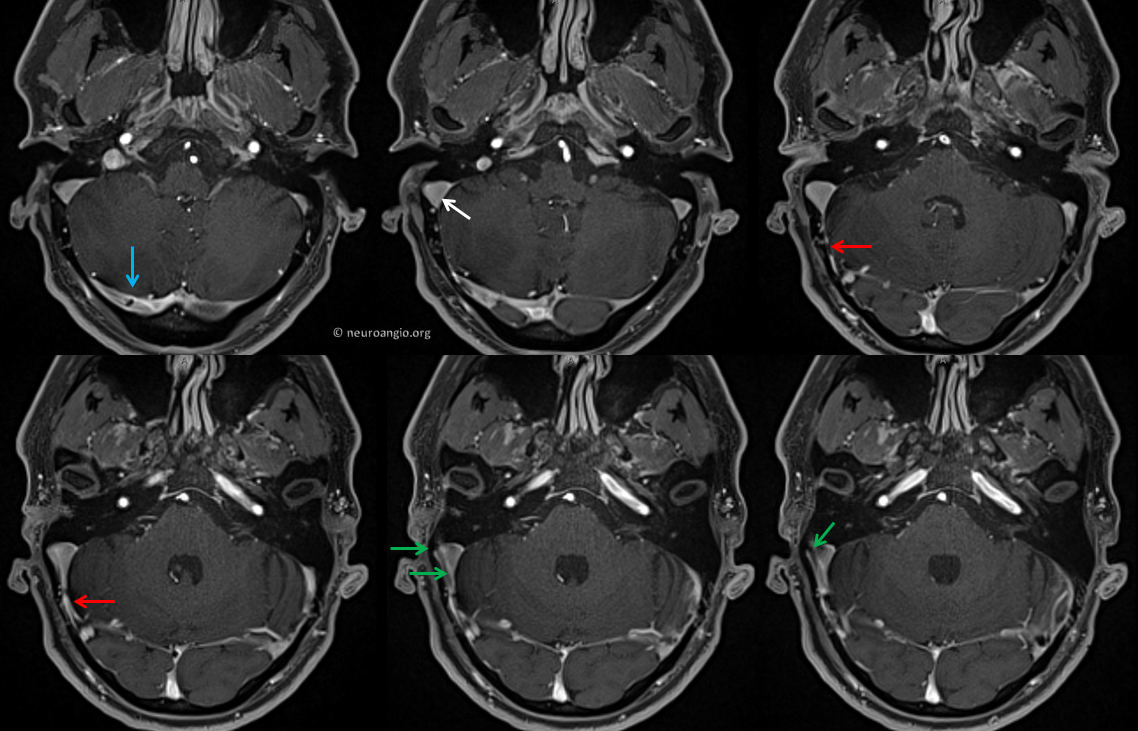
Below are some variations. In this case, the dominant sinus and PT are both on the left. Again, compression of left jugular vein stops the sound. The same color arrows apply, including flow jets (green, purple). A small arachnoid granulation (yellow) is present. Its size and position make it an unlikely cause of PT However, in a few causes they see to be the culprit.
Of course, if MRV is available, it works just fine. Here is one of the more severe cases we’ve seen
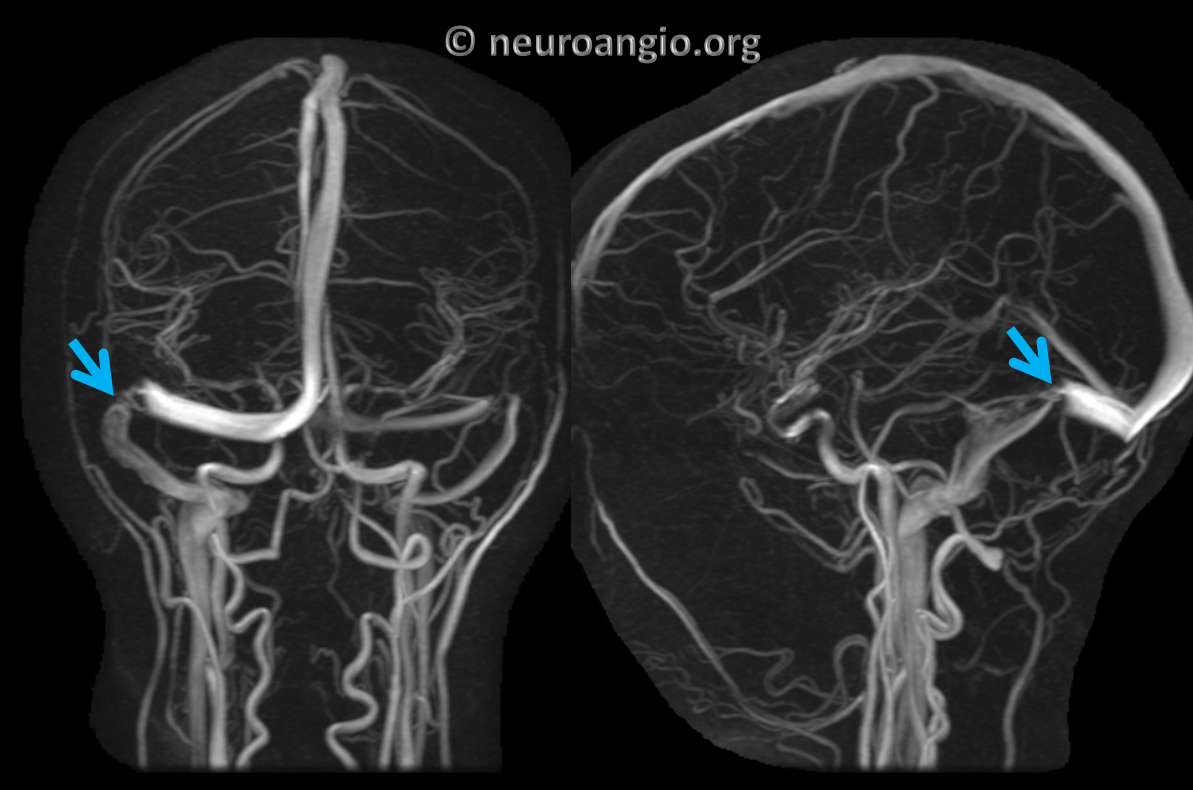
What is unique about this case is that this patient has been previously treated for intracranial hypertension, which is well-known to be associated with venous sinus stenosis, by placement of a programmable ventriculoperitoneal shunt (white arrow). The above stenosis persisted after shunt placement and further confirmation of shunt function by resolution of most intracranial hypertension symptoms and with valve knowledge of shunt pressure. This patient was treated by venous sinus stenting, with full resolution of symptoms

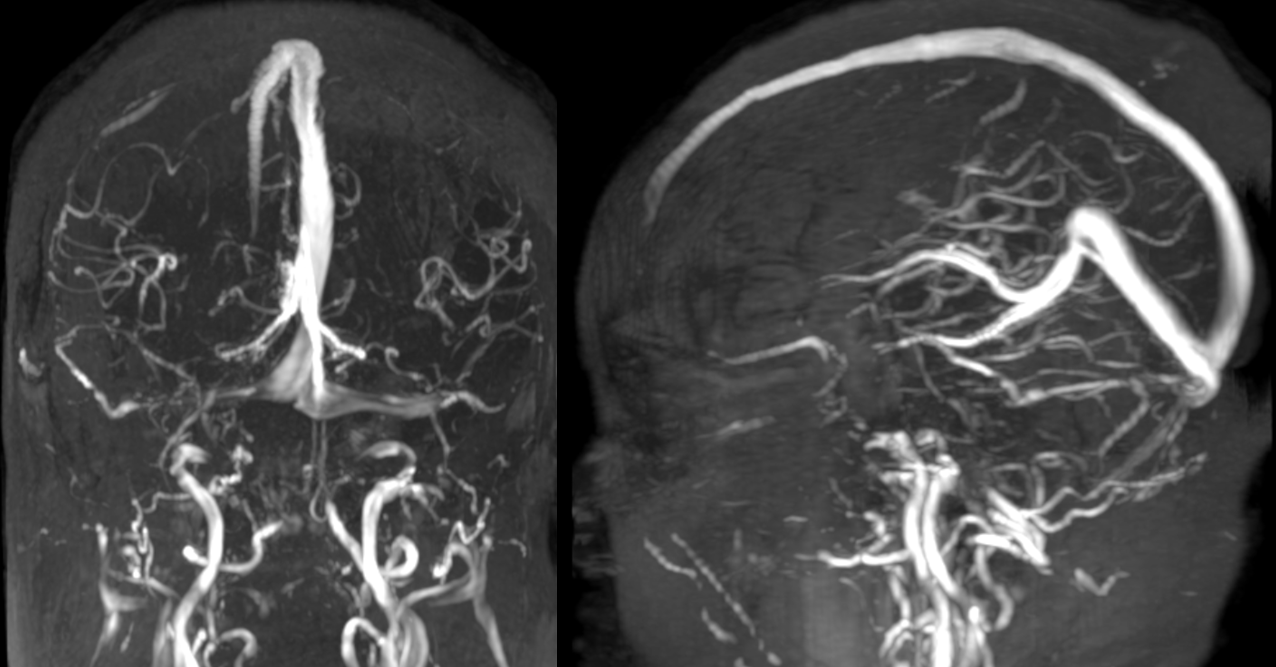
Below is another case, in this instance of a patient with co-existing intracranial hypertension. The association between sinus stenosis and IH is well-known. What continues to be debated is which is the cause and which is the effect. Does stenosis cause elevated intracranial pressure? Does elevated pressure result in collapse of the sinus? I think the answer is yes and yes. The above case clearly shows that venous sinus stenosis can persist after shunt correction of intracranial pressure. However, there are clear instances of sinus stenosis resolution following stenting or immeidately after lumbar puncture. It is likely that IH is a heterogeneous condition with both possibilities. Anyway, below is a typical IH-related venous sinus stenosis as seen on a contrast MRV
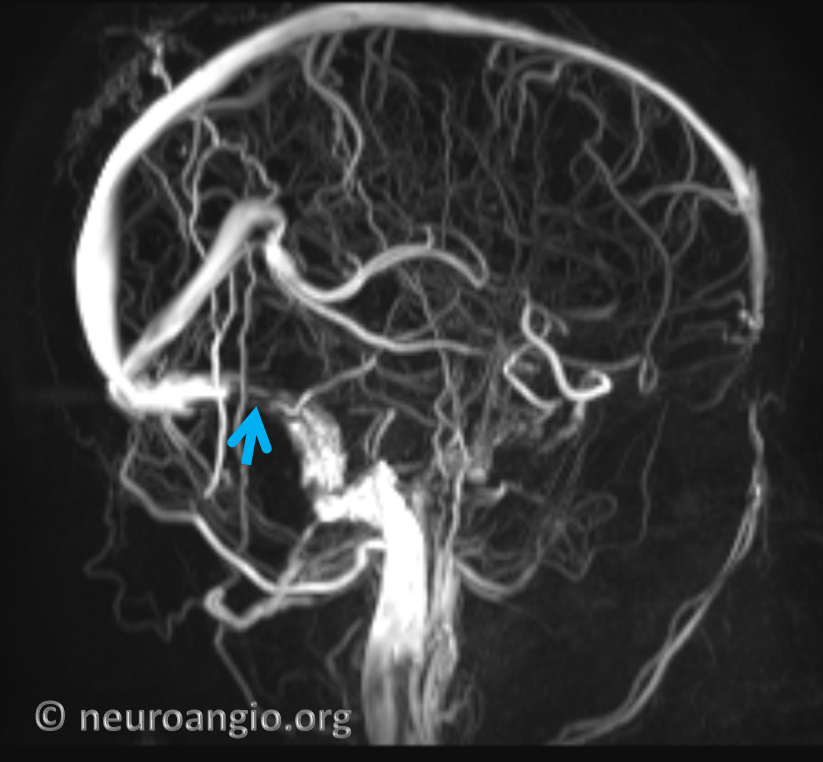
TOF MRV of the same patient. Notice how much worse the quality is. Usually, contrast is better.
Angiogram of the same patient. A flattened appearance of the sinus is typical
Catheter venogram of the same case
Another patient with IH — same flattened appearance of the sinus
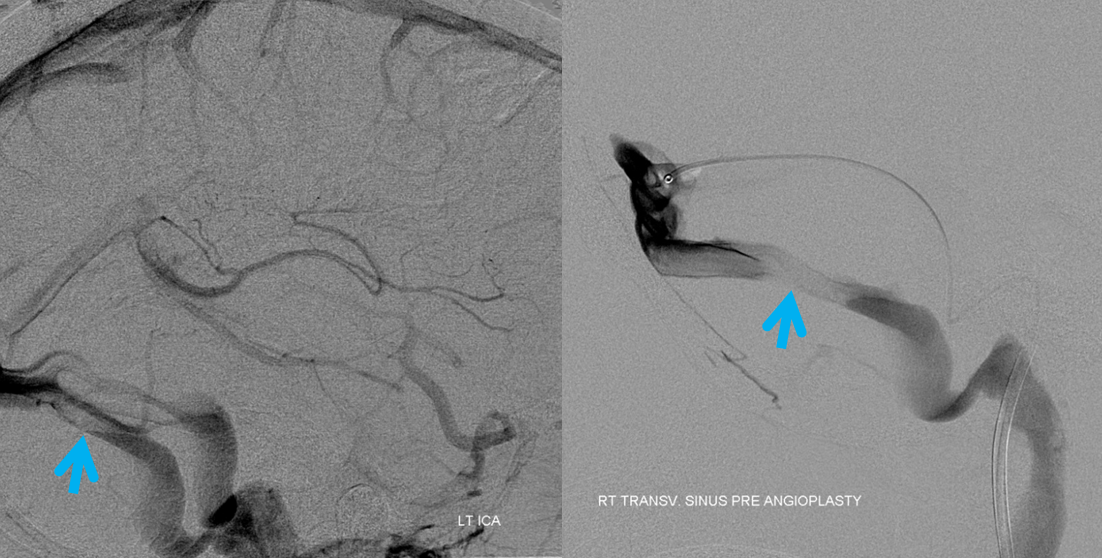
Here is an unusual cause of pulsatile tinnitus on a non-dominant sinus side — a sigmoid fenestration (arrow). The sound was completely abolished by neck compression.
Axial images

CT angiography is not our first choice for evaluation of PT — poor timing is common, leading to venous contamination. However, while identification of dural fistula is hampered by venous contamination, venous sinus stenosis becomes easier to see. Here is stenosis (blue arrow) on a badly timed CT angiogram
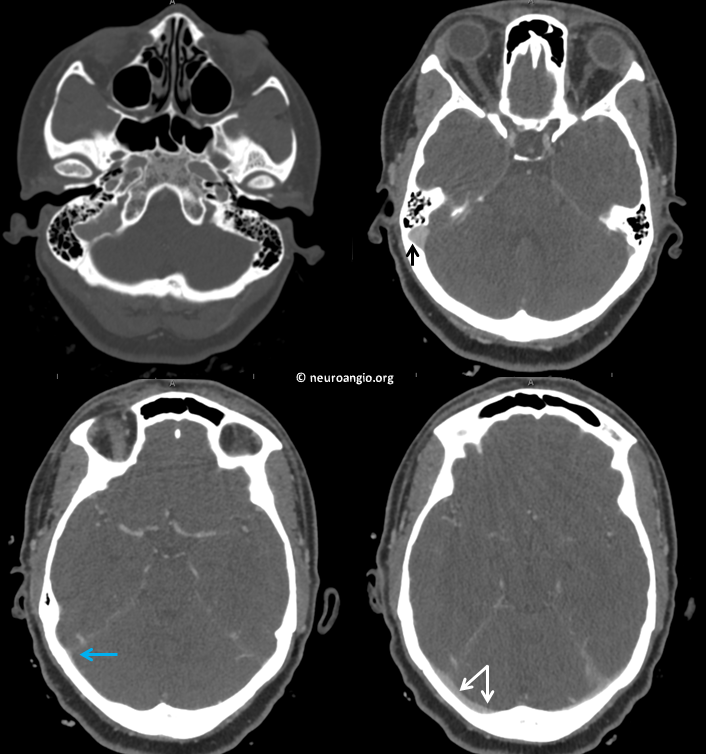
Coronal reconstructions are even better
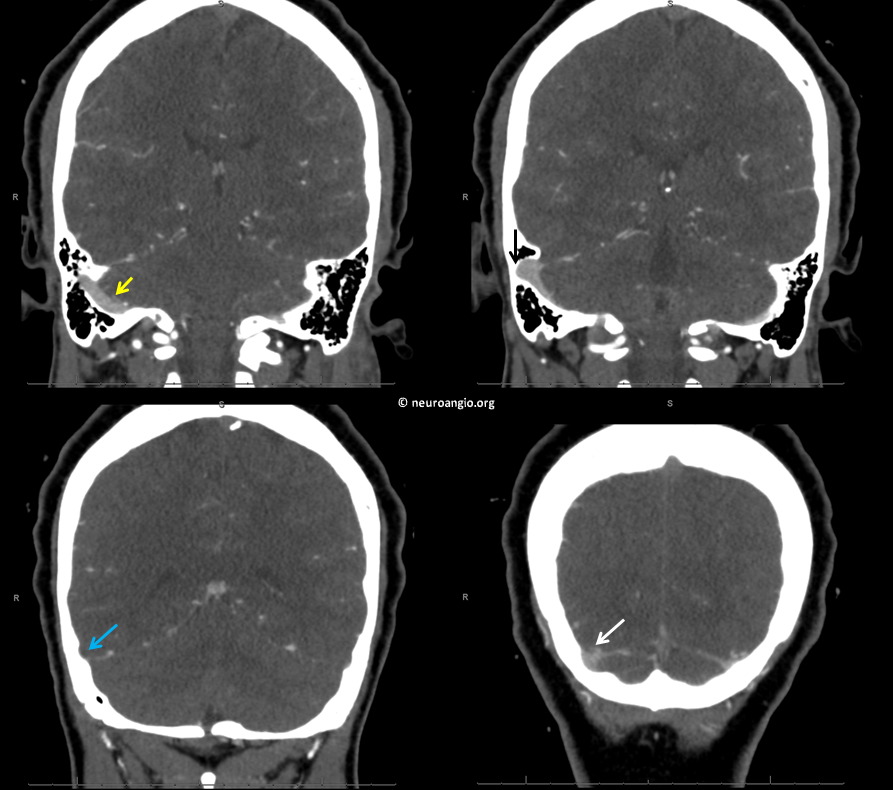
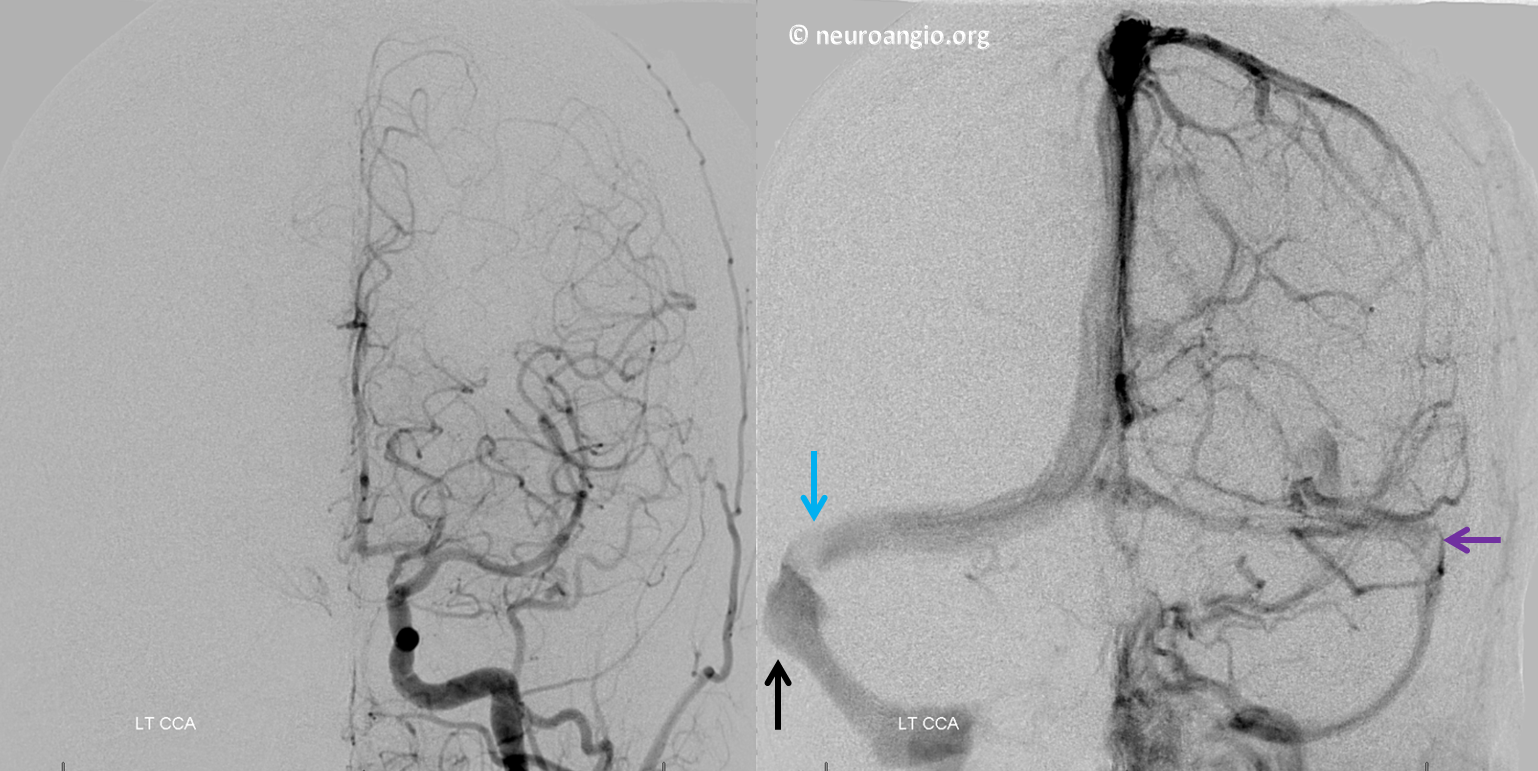
Angiographic image of the same patient, with stenosis and associated post-stenotic diverticulum (black). Mirror image hypoplastic sinus stenosis (purple) on left
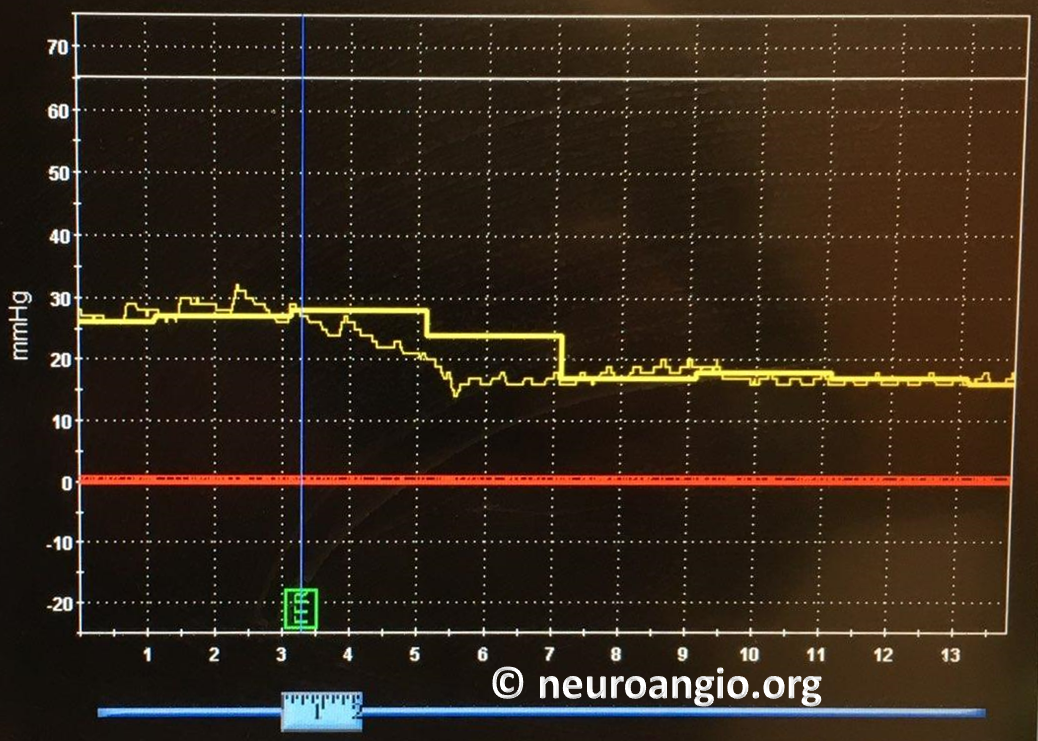
Pressure gradient across the stenosis, as measured by Volcano 014 pressure wire
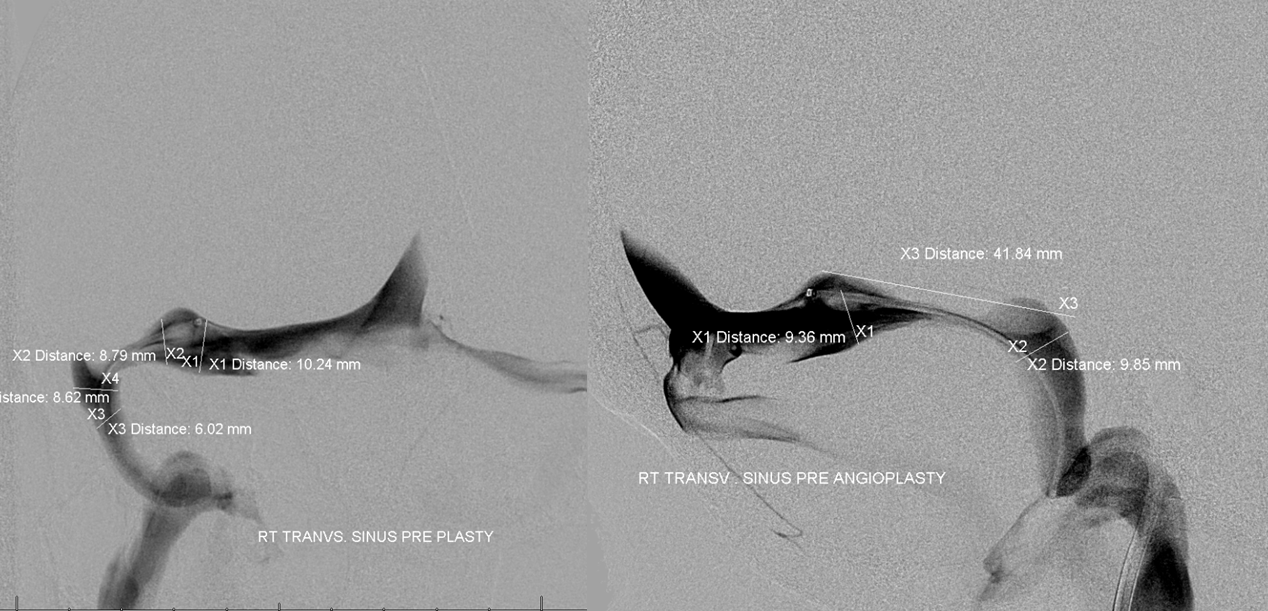
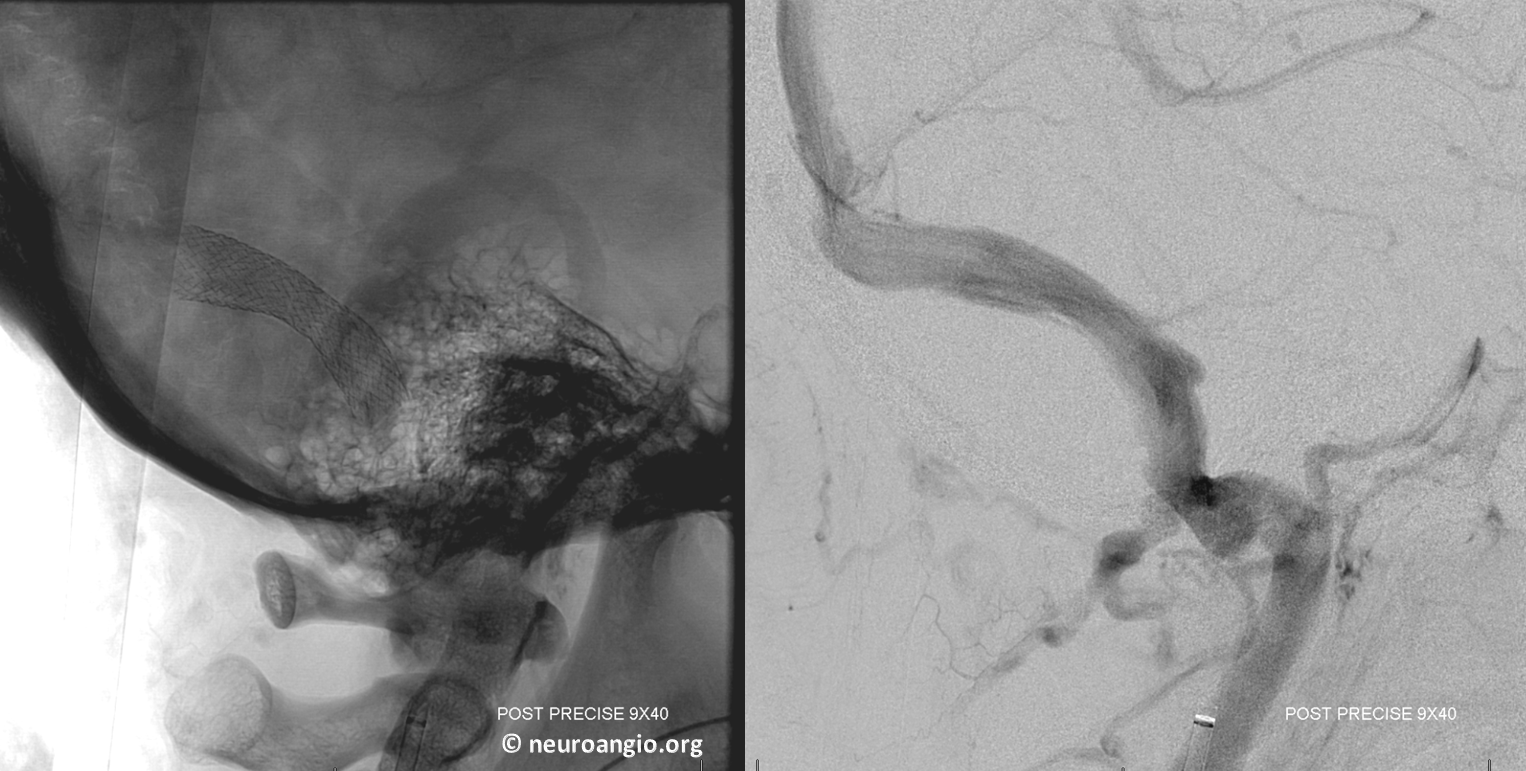
Sinus venogram before stenting
Post-stenting of the sinus
See full case here
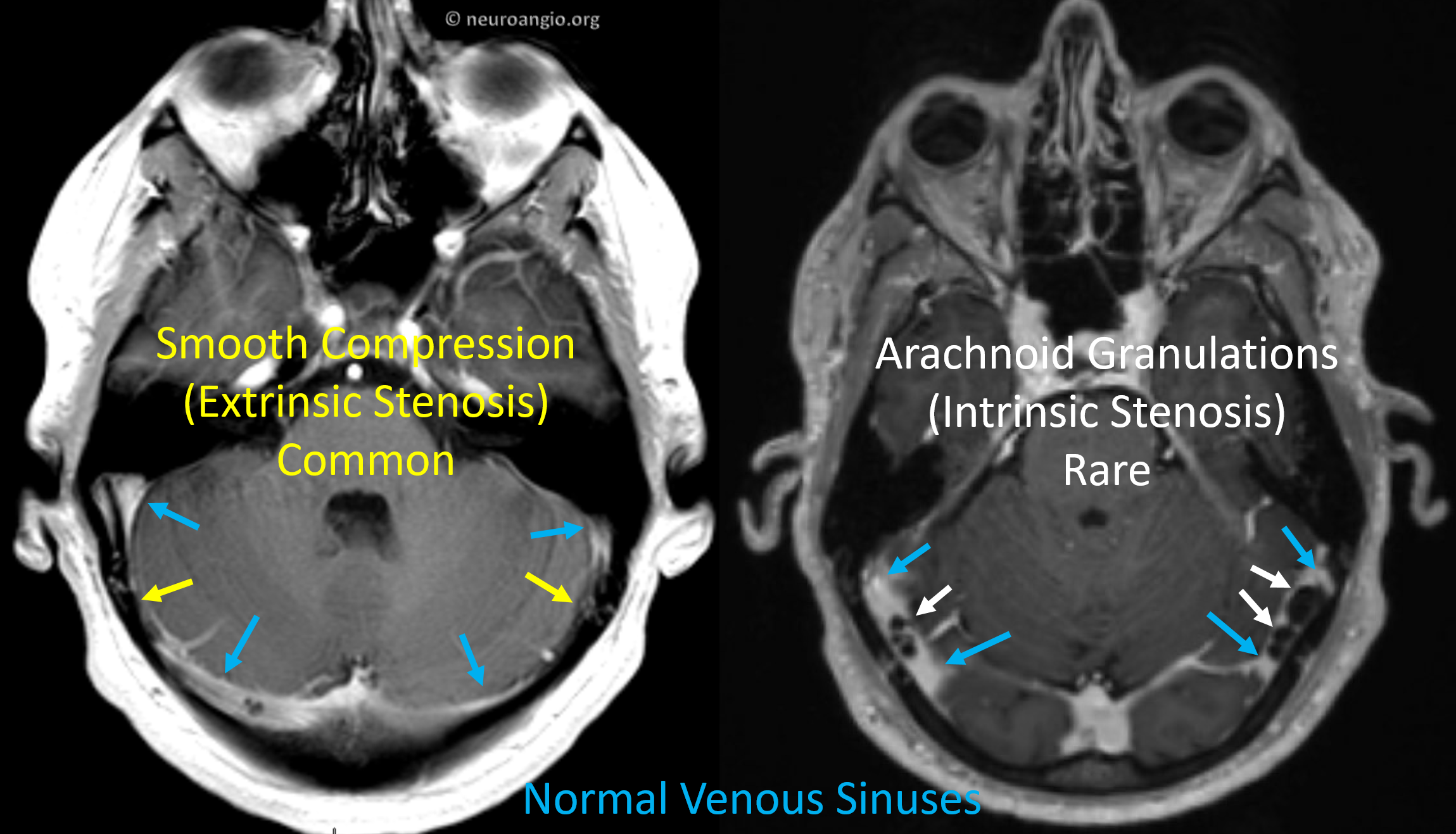
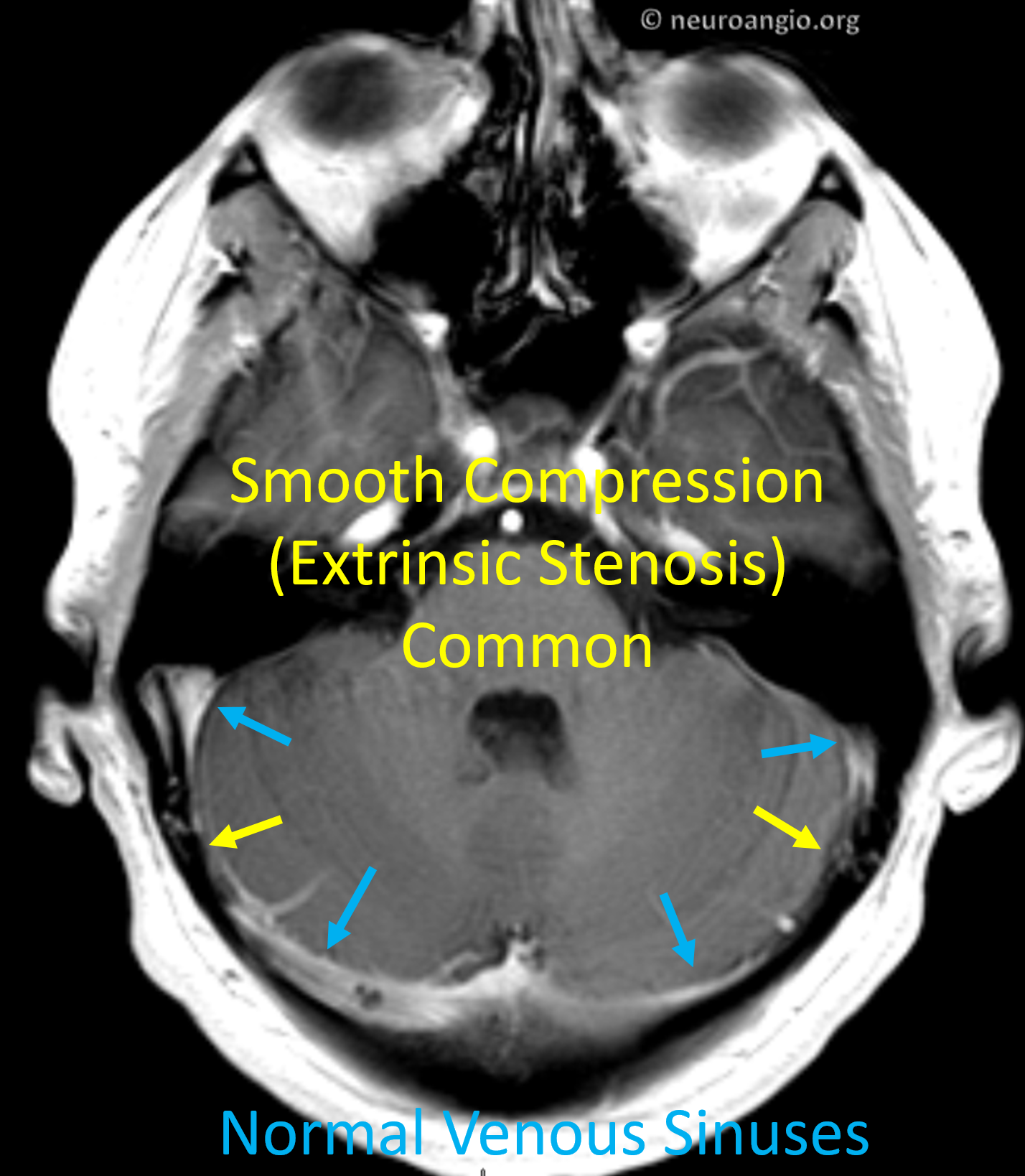
Extrinsic vs. Intrinsic Stenosis
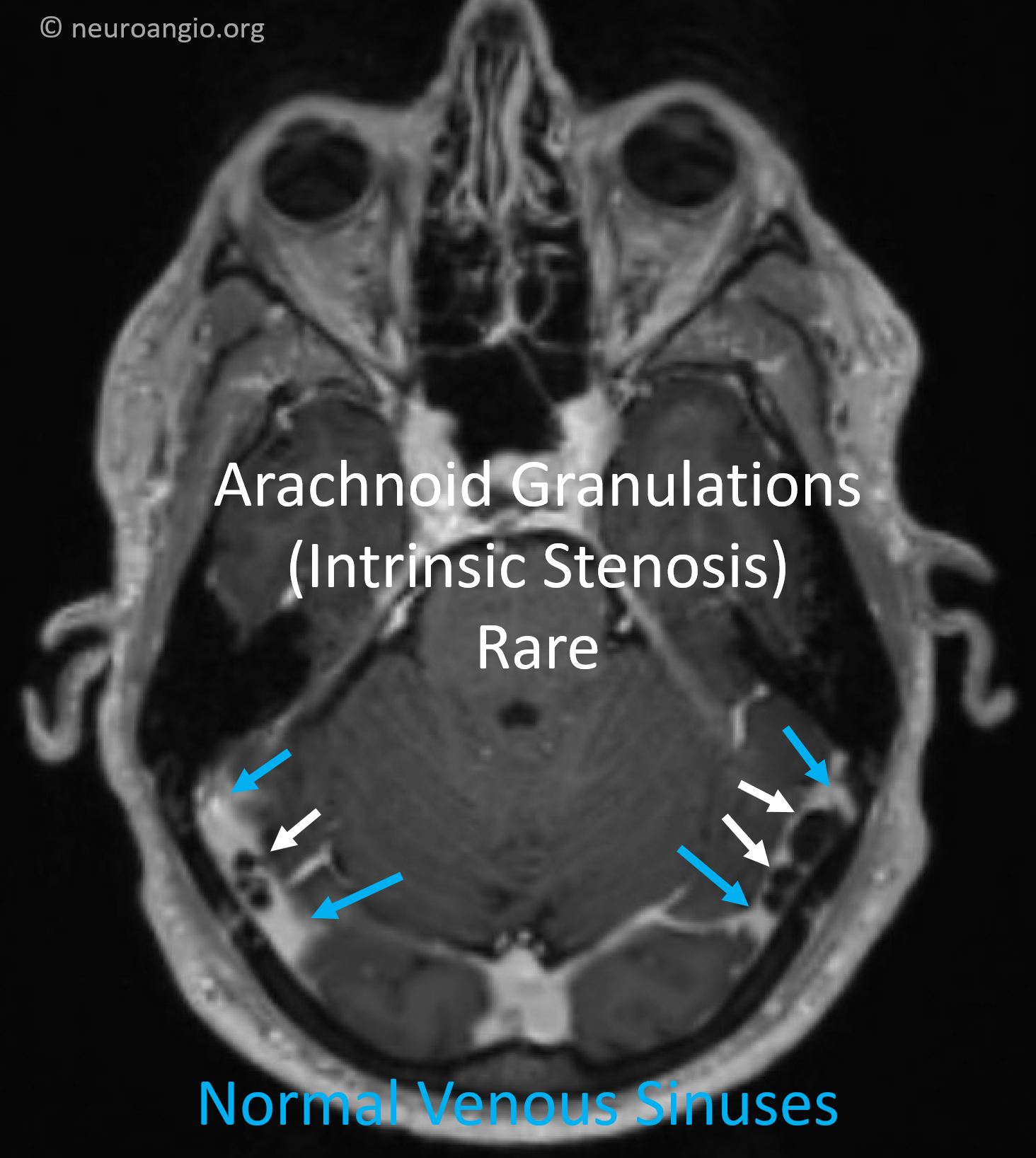
We come now to the last important point. The question as to whether intracranial hypertension causes venous sinus stenosis or the other way around remains unanswered. There are experienced people on both sides of the debate. I happen to believe that stenosis is not the cause, but consequence of intracranial hypertension. This is an “extrinsic” type — compression from outside. It is by far the most common. Much rarer, but very real, is an “intrinsic stenosis” — caused by something that sits inside the venous sinus and makes it narrow. Usually, the thing that sits inside is arachnoid granulations. These are normal structures that we all have, and they live inside the sinuses, like outcroppings or peninsulas. Their function is to help absorb cerebrospinal fluid which surrounds the brain and spinal cord. They are normally scattered throughout the sinuses and other dural structures. Rarely, instead of being spread around, they are bunched up together, narrowing the sinuses a lot. When this happens, the pressure upstream of narrowing can become quite high. MRI imaging shows it best. Another clue is that patients with this problem are often not the typical demographics of intracranial hypertension.
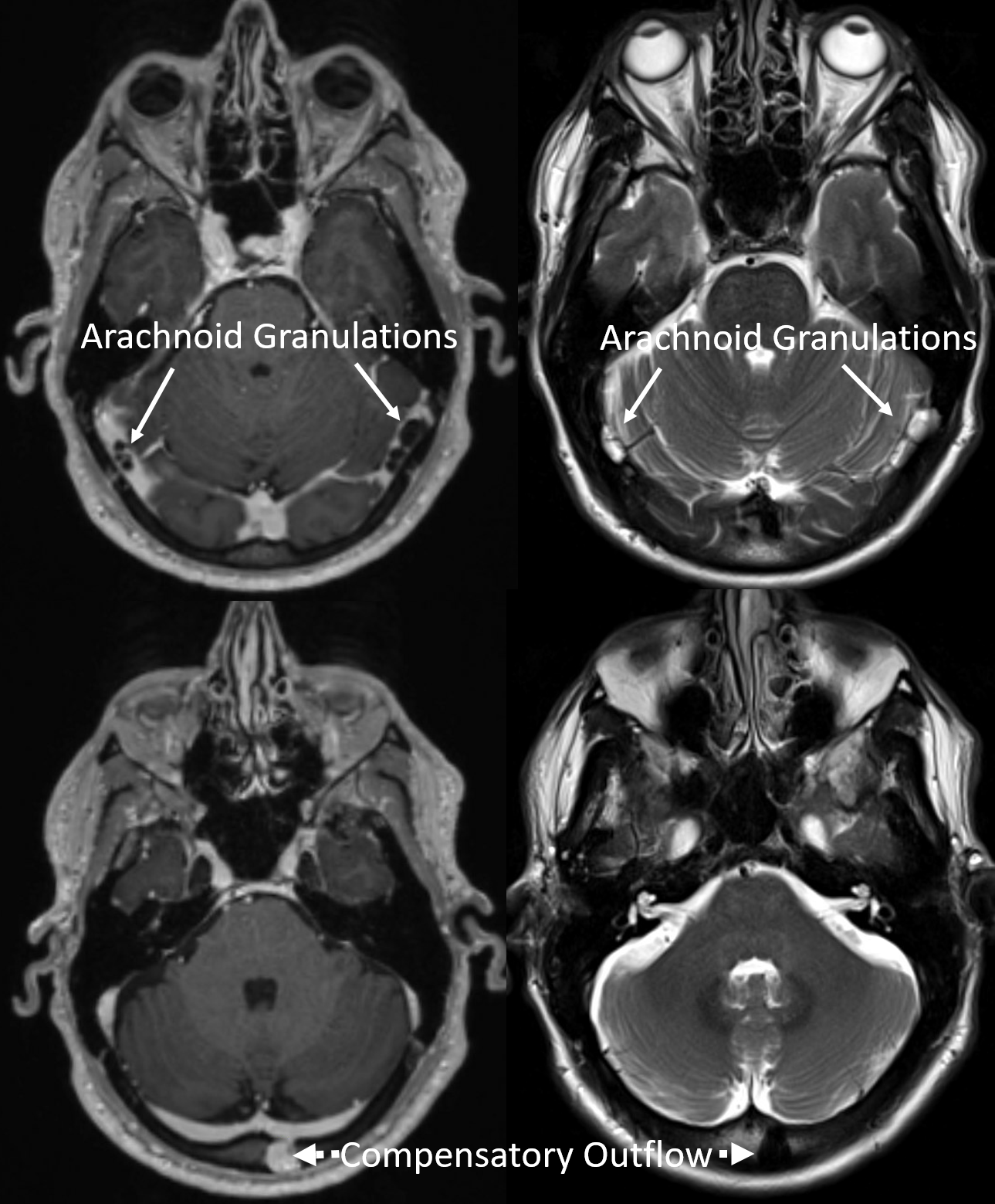
Below are examples — arrows and colors speak for themselves
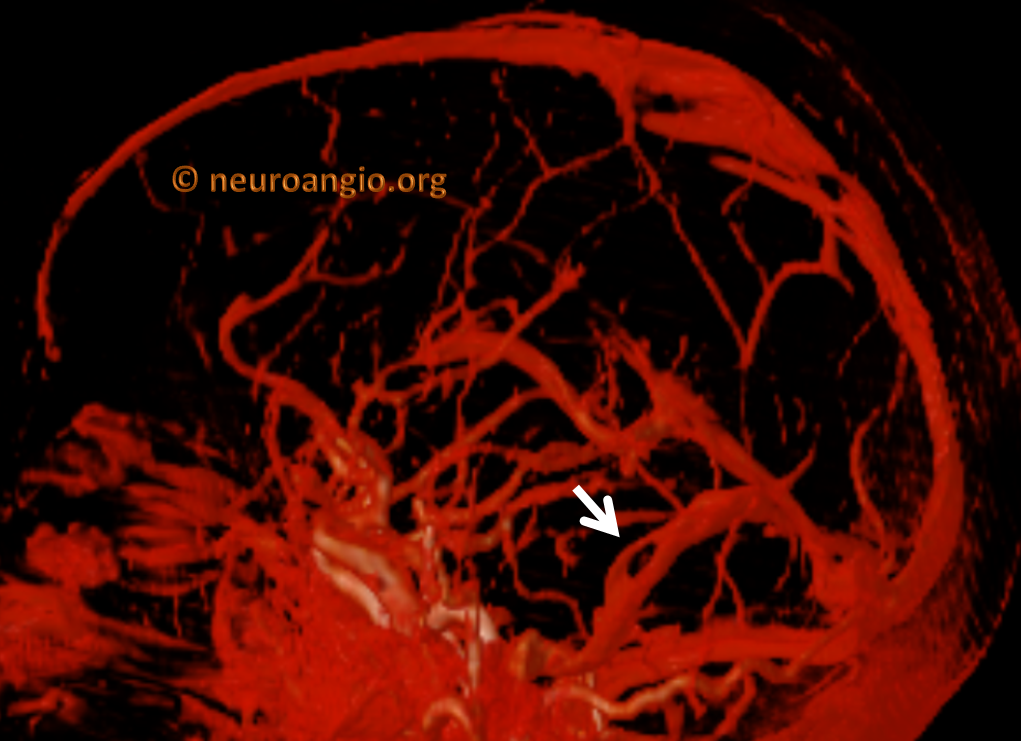
More detailed views — in addition to narrowing the sinuses, the long-standing stenoses also led to some adaptions — in this case another route for blood to leave the head — via an opening (foramen) in the back of the head — its a type of “emissary vein” — labeled “Compensatory Outflow”
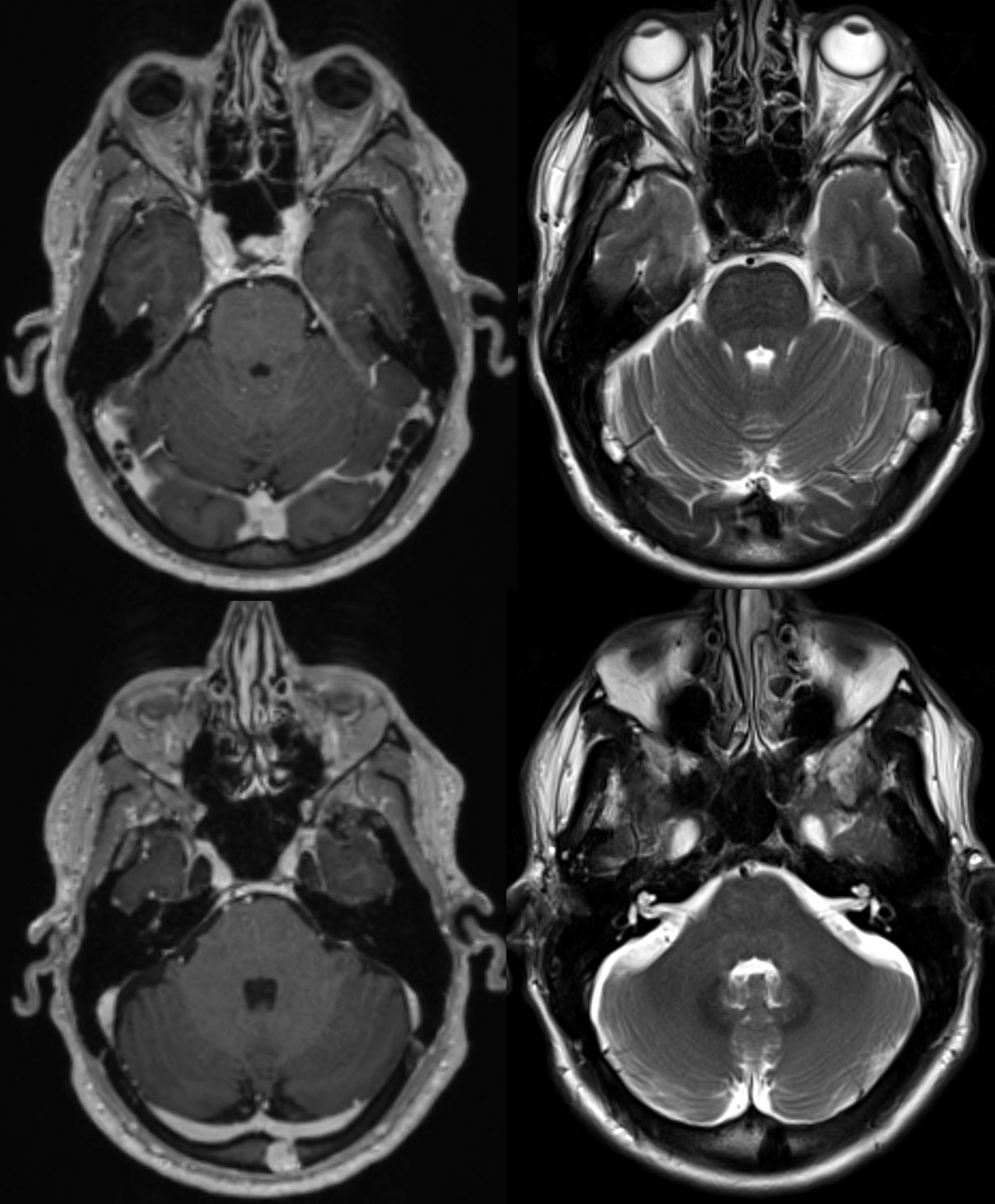
Without Labels
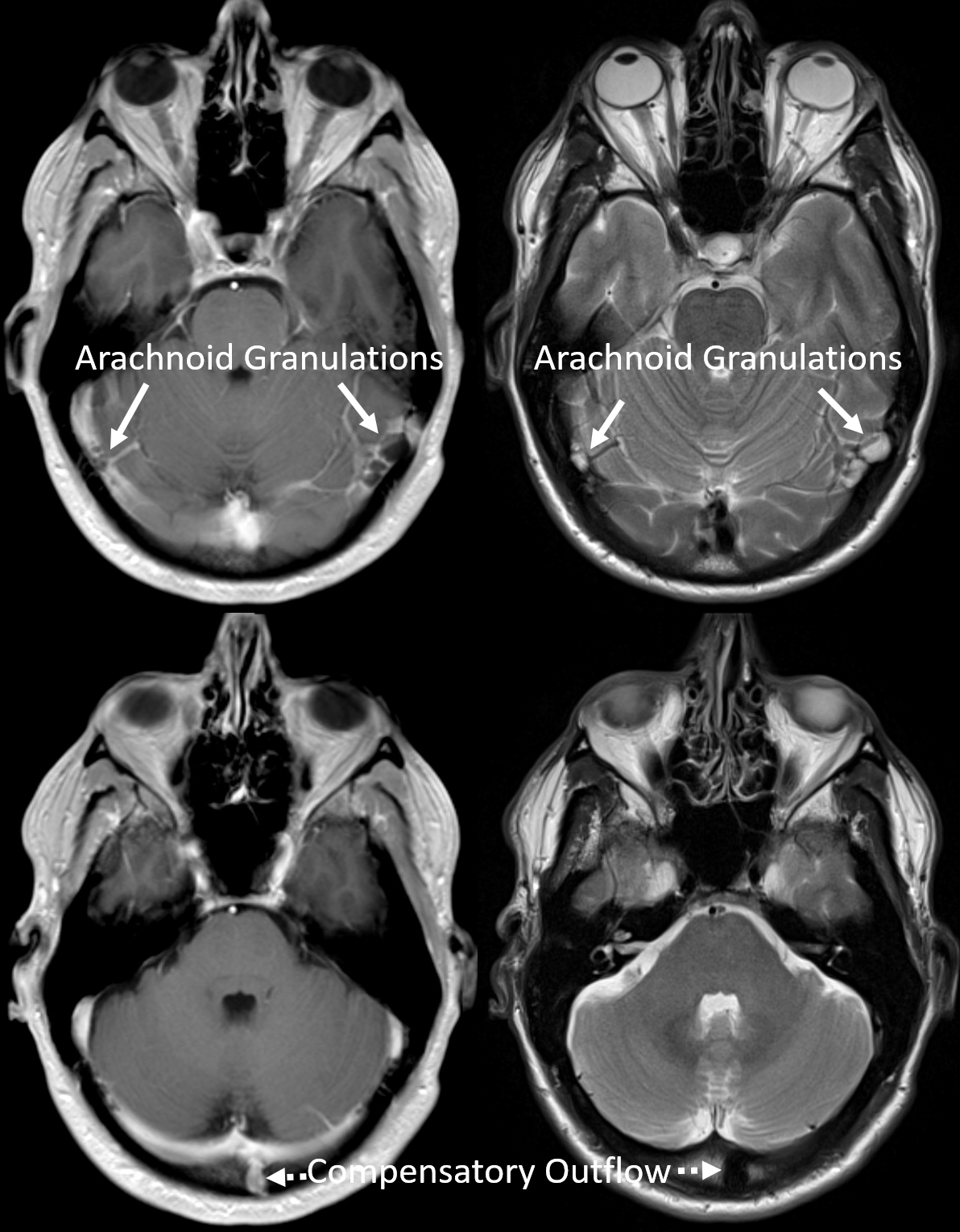
This person had intracranial hypertension for over 10 years. The findings were always there (below is the same person in 2015) however they were unrecognized. Thanks to more education, now they are often correctly picked up and reported. But not always.
Occasonal venous “detour” or bypass venous channels develop to circumvent the long-standing stenosis. Here these are diploic veins. A nice example of how important it is to sent the right channel…

See
Back to Diagnosis and Treatment of Pulsatile Tinnitus