
The good number 17 (white arrows) above — a.k.a. artery of Bernasconi and Cassinari — one of the few surviving eponymous vessels. Its an artery or network of arteries — if there is flow demand — along the tentorial edge. It is the most constant and probably the most important (by volume) artery in supply of the tentorium as well as the inferior falx cerebri. The artery starts at the anterior clivus — and so supply is from nearby vessels — MHT and ILT (see those pages for more). Since the ILT area for example is in balance and thus can be served by cavernous branch of MMA for example, or the accessory meningeal artery, or the artery of the sphenoid ridge — so can all of these also be participating in marginal tentorial arcade supply. The ideas of balance and spectrum are ever-present.
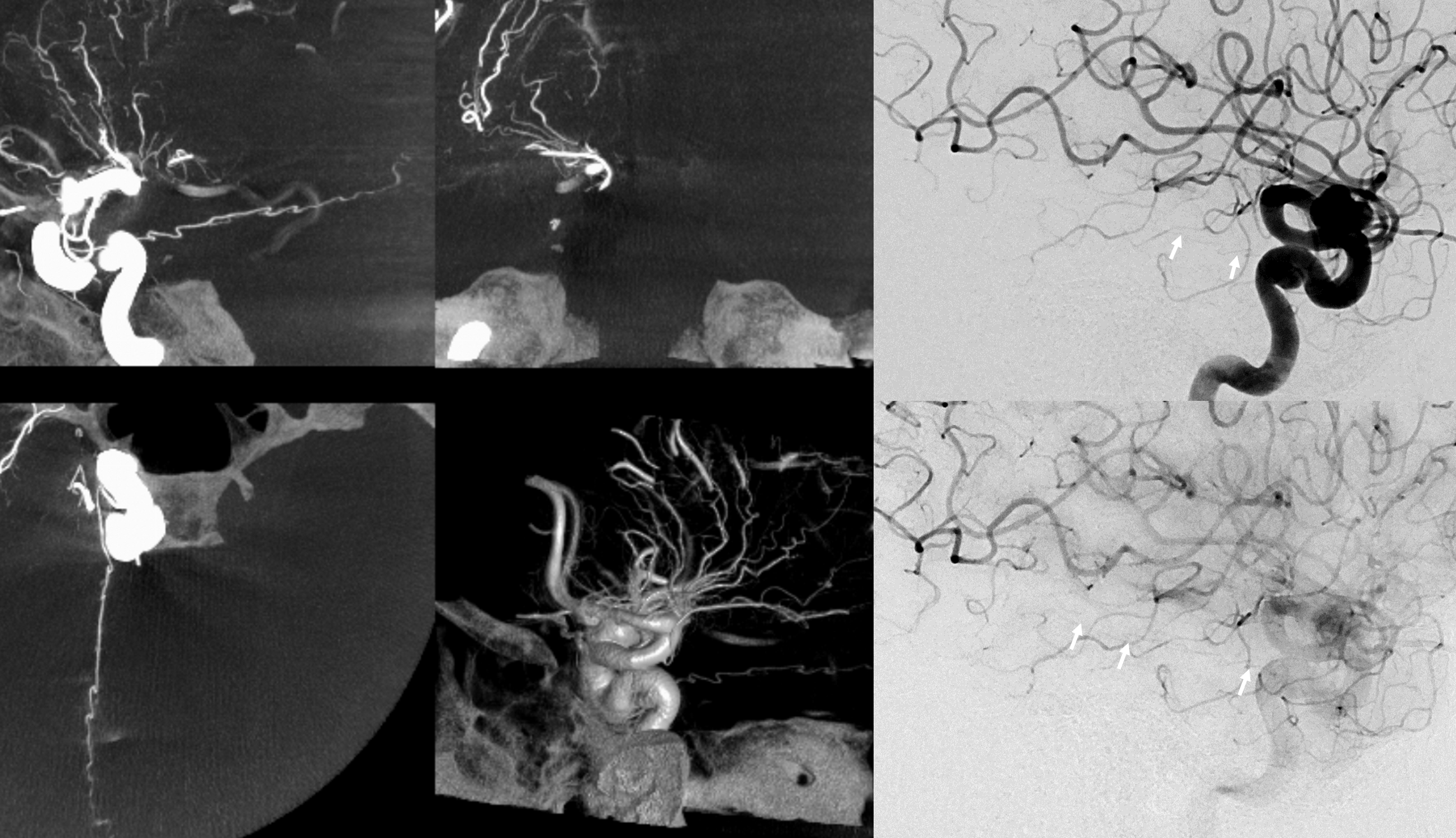
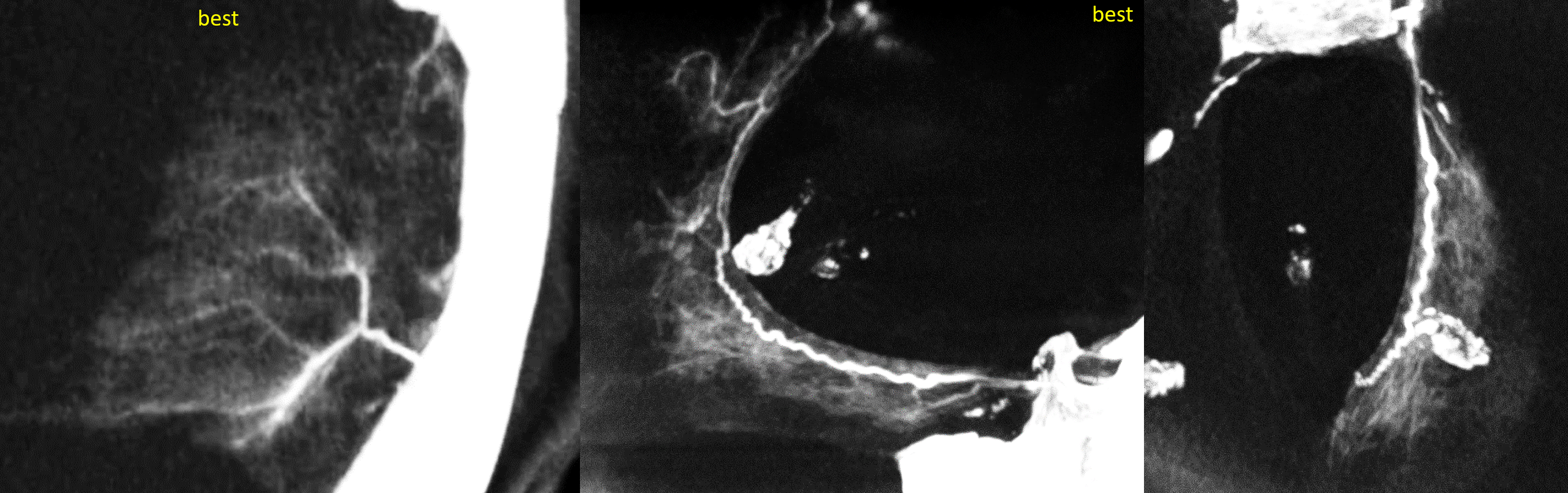
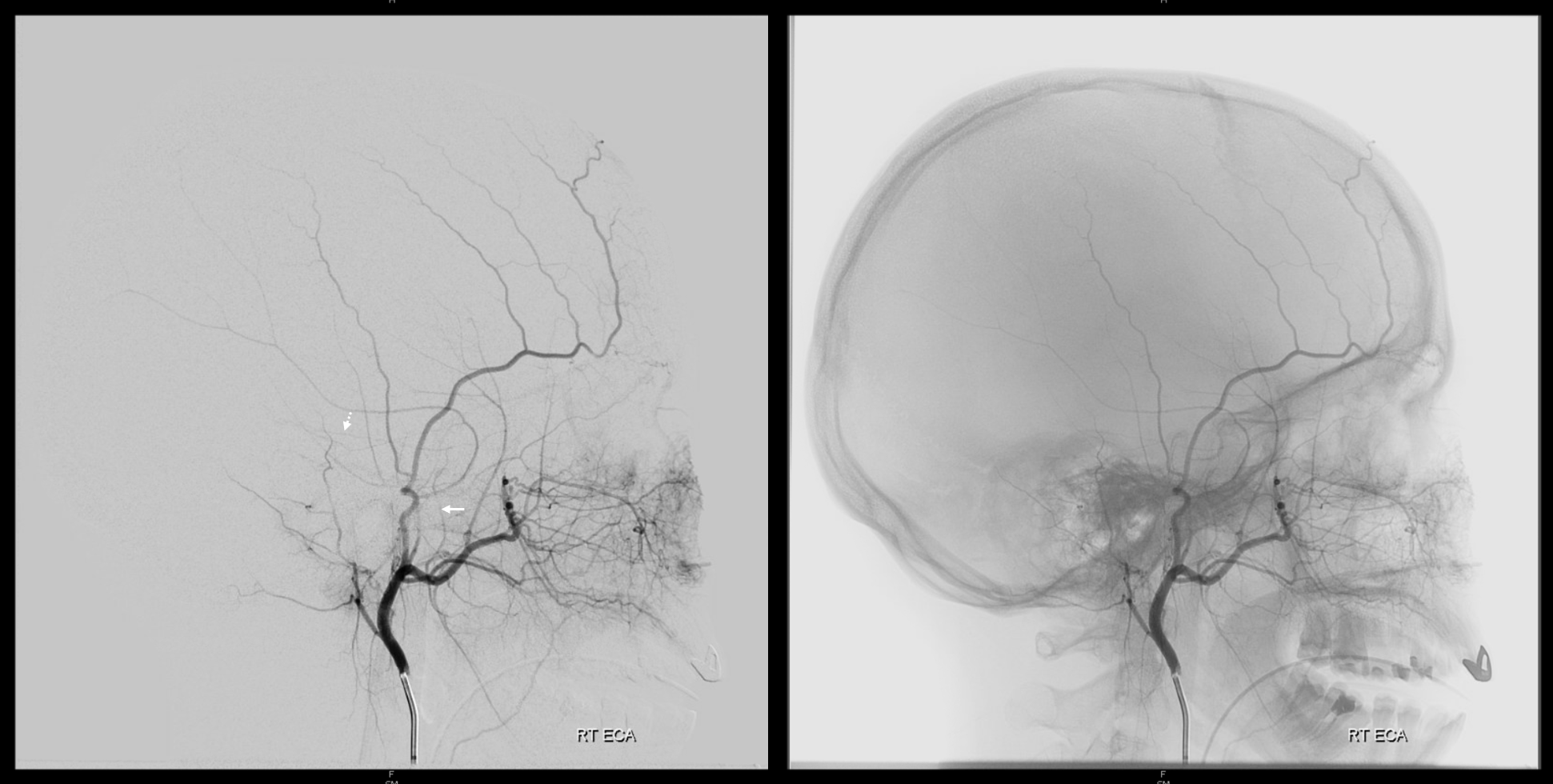
Although visualization is possible many times with 2D-DSA, to really see the artery well and undertand its balance with other vessels requries Cone Beam CT (DYNA, Vaso). See below the difference… ILT origin marginal tentorial.
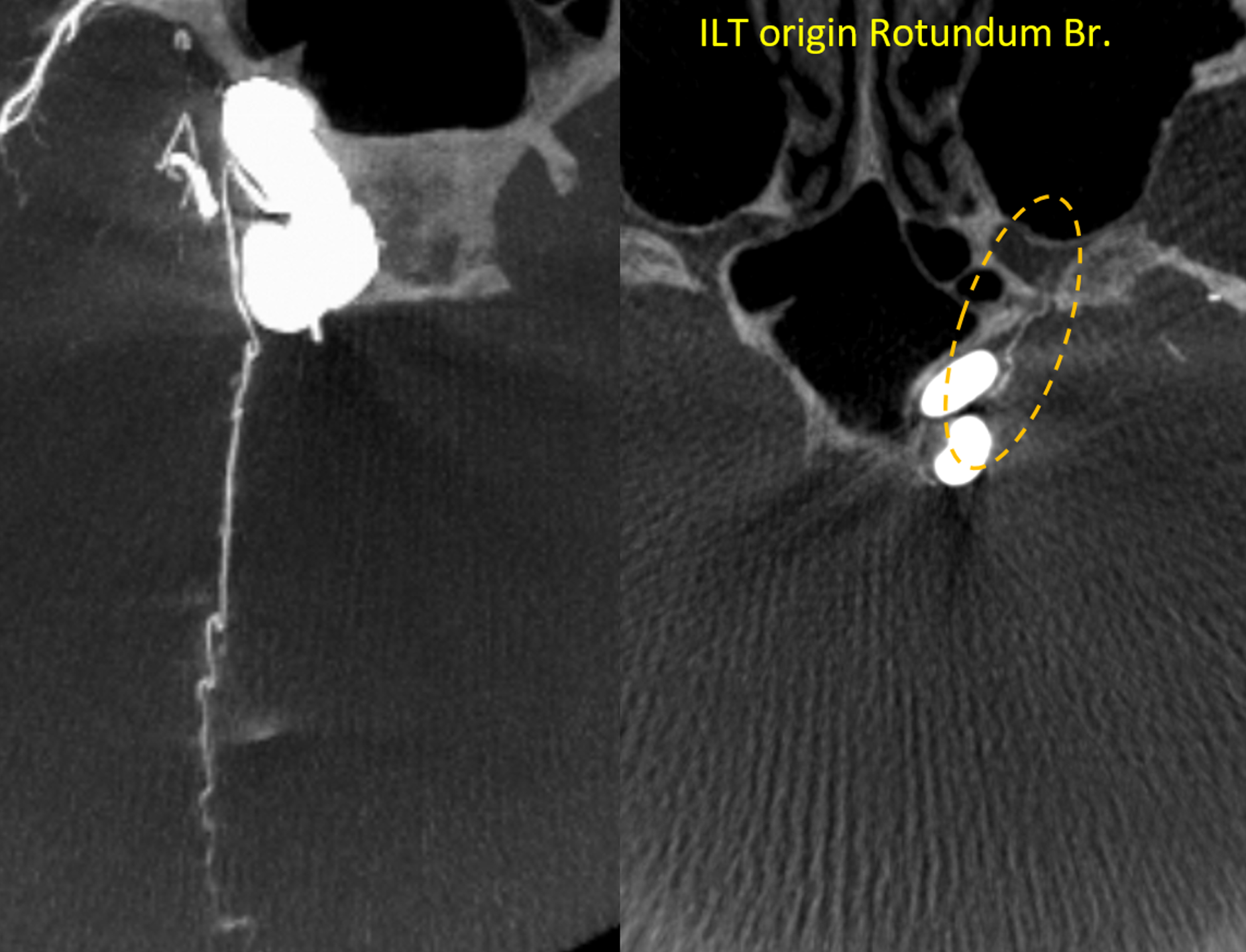
Balance is everpresent again. Usually one of the two marginal tentorials is larger than the other, and maybe enough to supply portions of the contralateral tentorium posterior to the incisura. See below case of right dominance. Incidental note of ILT origin foramen rotundum branch
Another example

Intrinsic Tentorial Vasculature
Unlike the convexity or the upper falx (see intrinsic dural vasculature page), the tentorial intrinsic vasculature is seldom seen. It is not because the tentorium is less vascular. The reason is likely that it represents a kind of dural watershed — along with the inferior falx, it is furthest away from the “main” sources of dural supply (anterior, middle, posterior meningeal arteries). This notion of dural watershed is important when we consider some dural fistuals and piodural anastomoses.
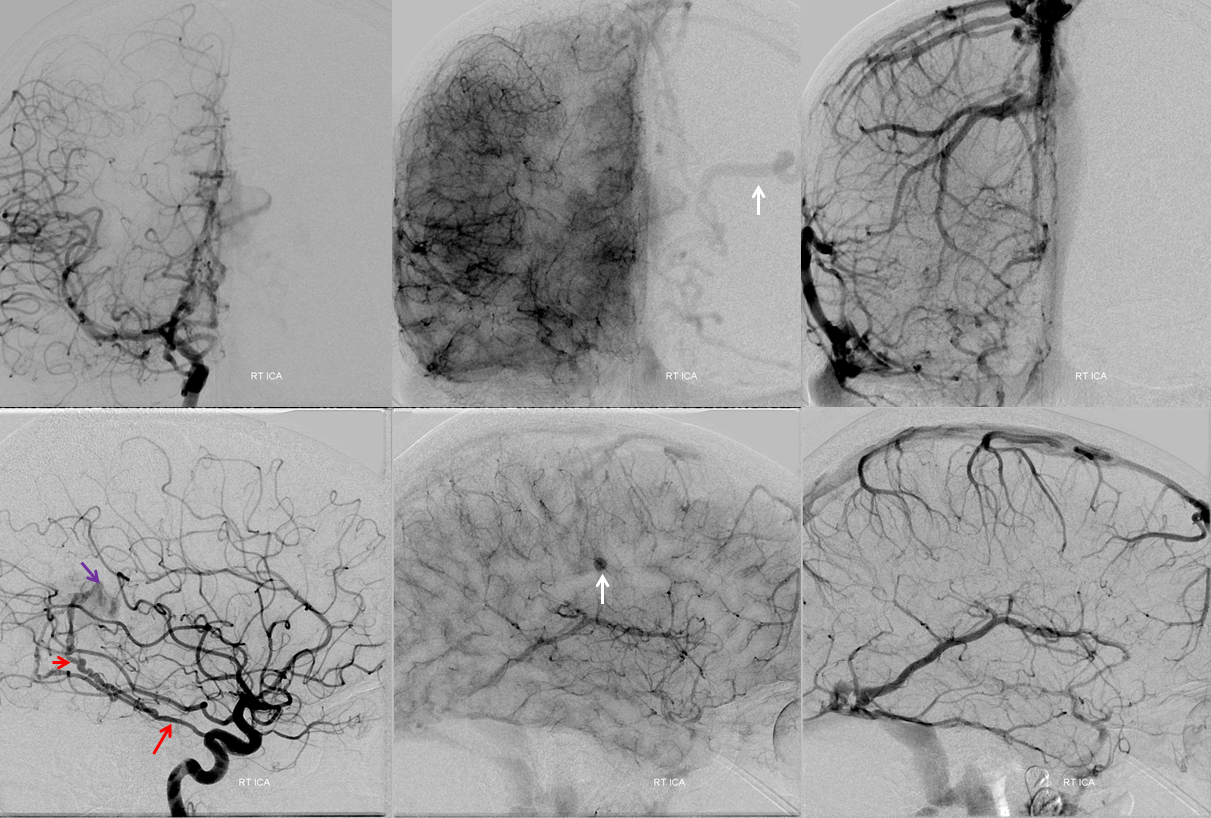
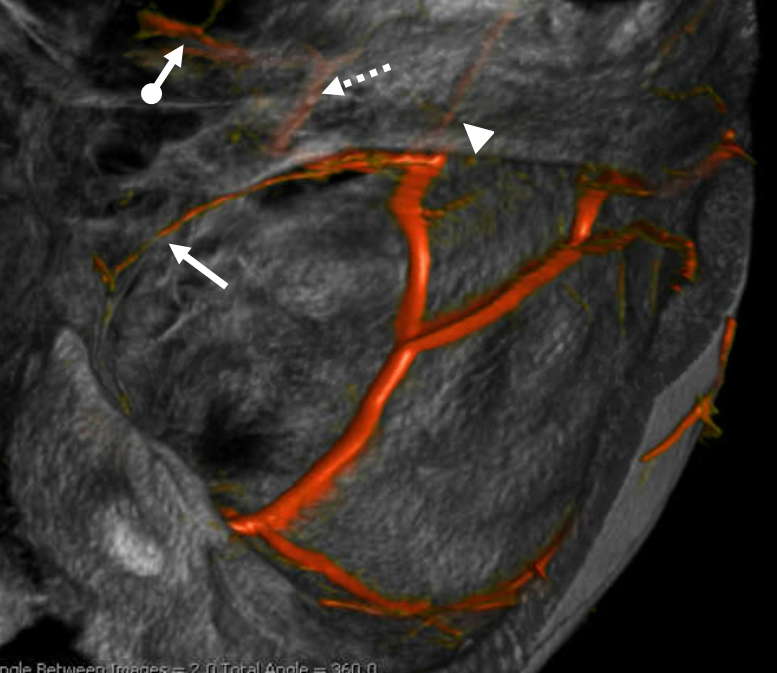
Below are examples of the unusually well seen dural tentorial vasculature.
More typical meager if any visualization is seen below

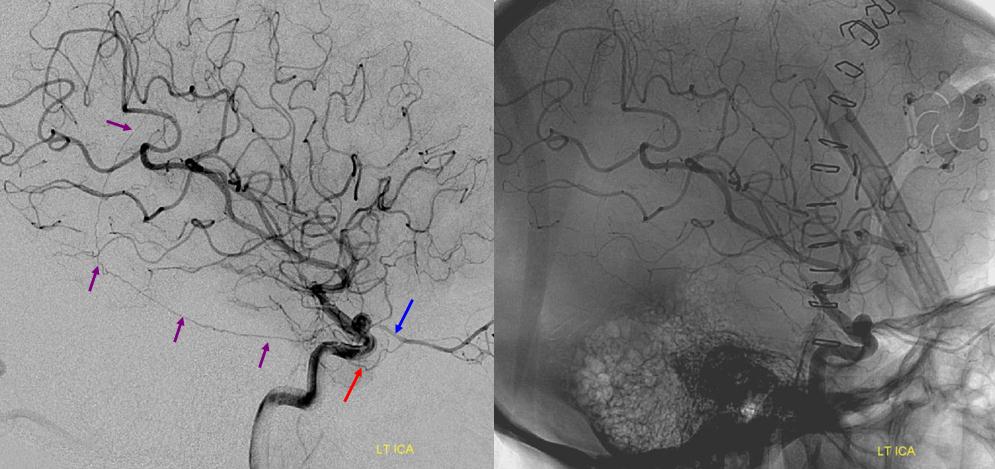
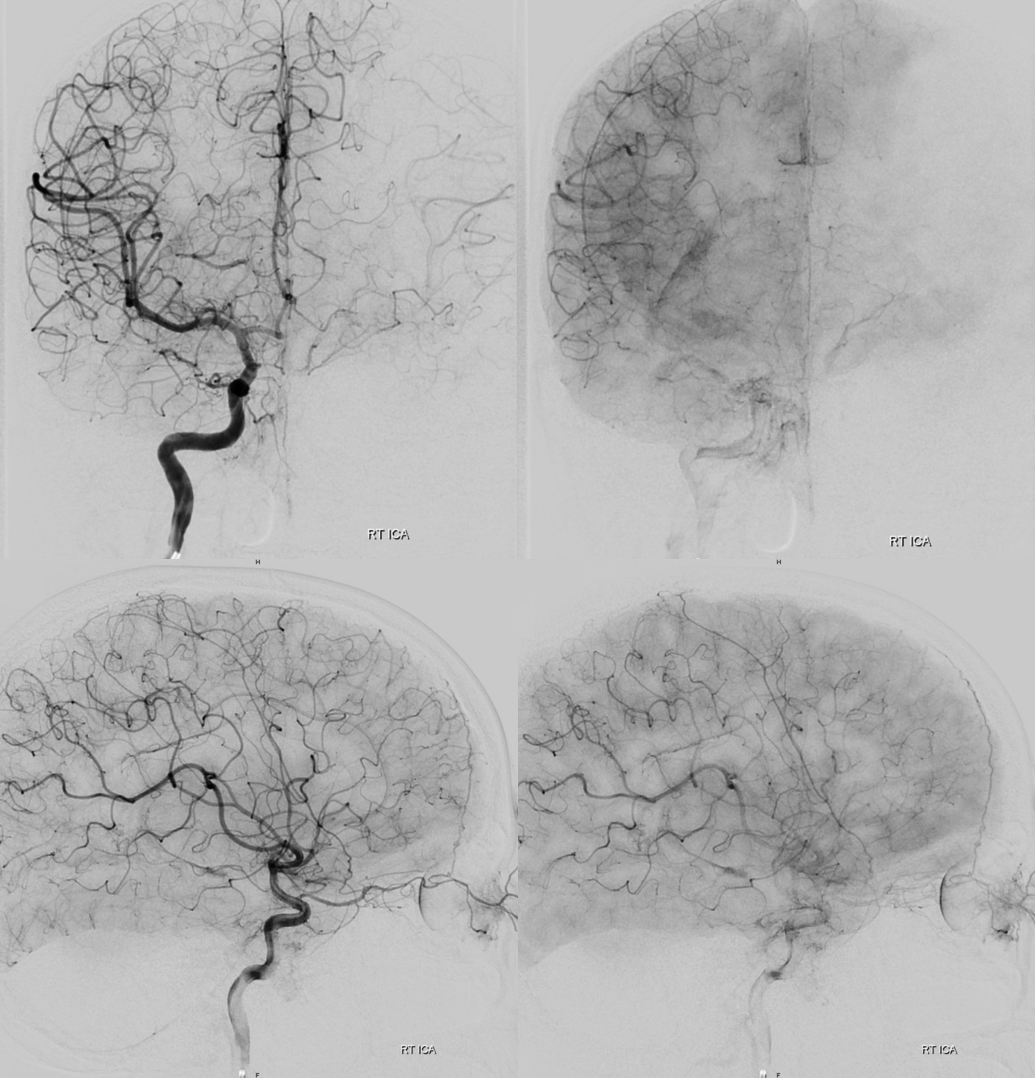
Lest you think you cant see it ever with angio, here is an example
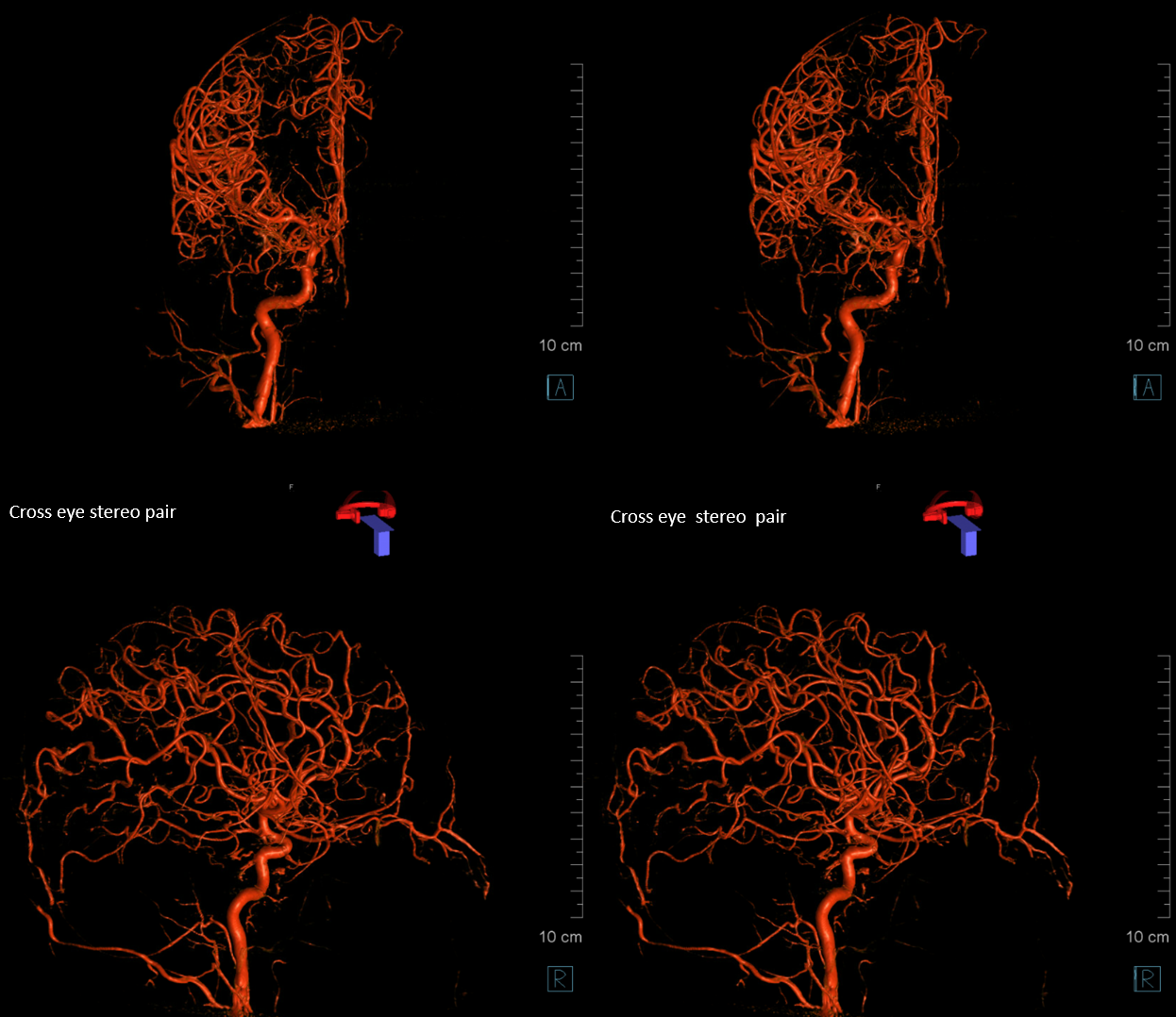
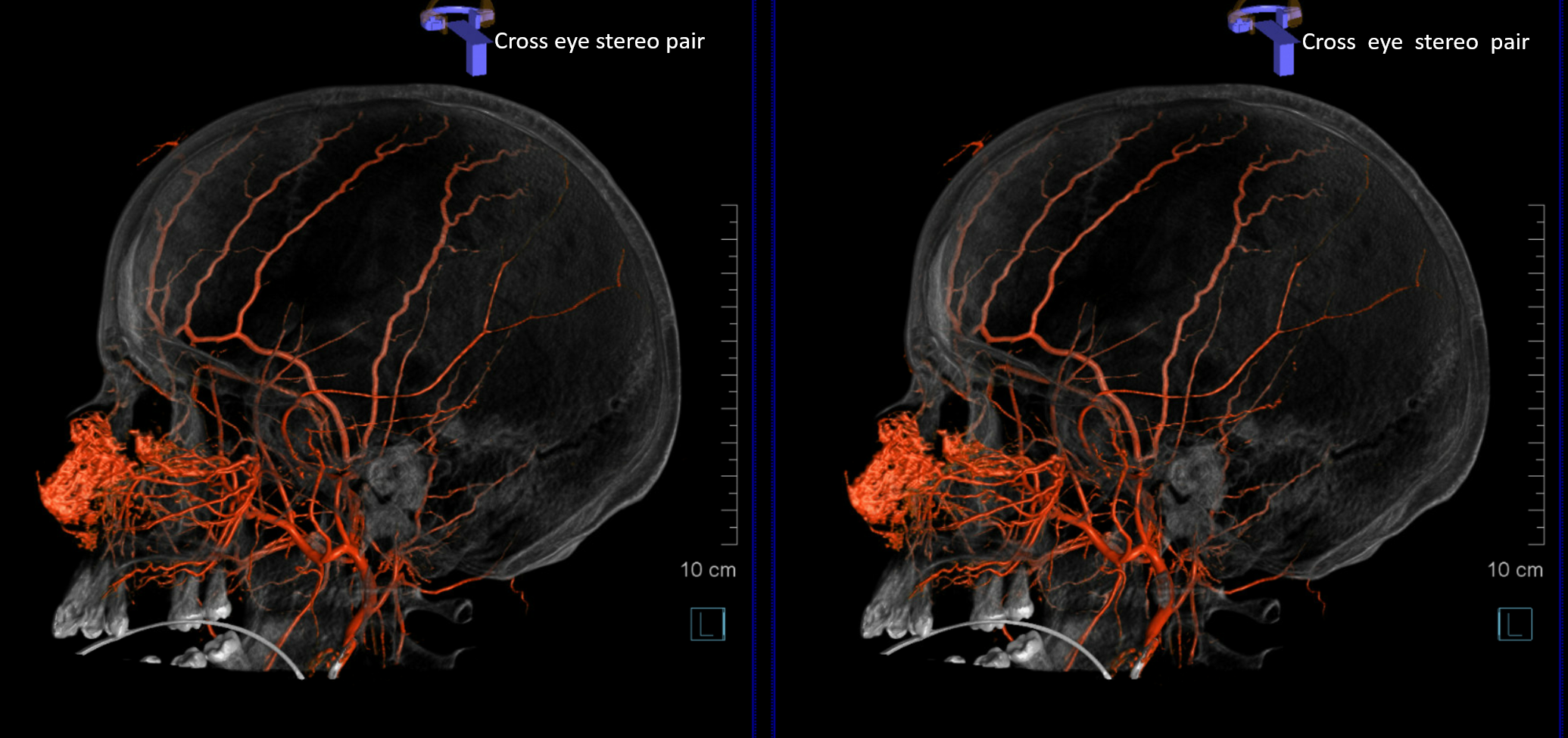
A bigger one (purple) — why? Again, think network — of the MMA is taken down by surgery — so other meningeal vessels pick up the slack
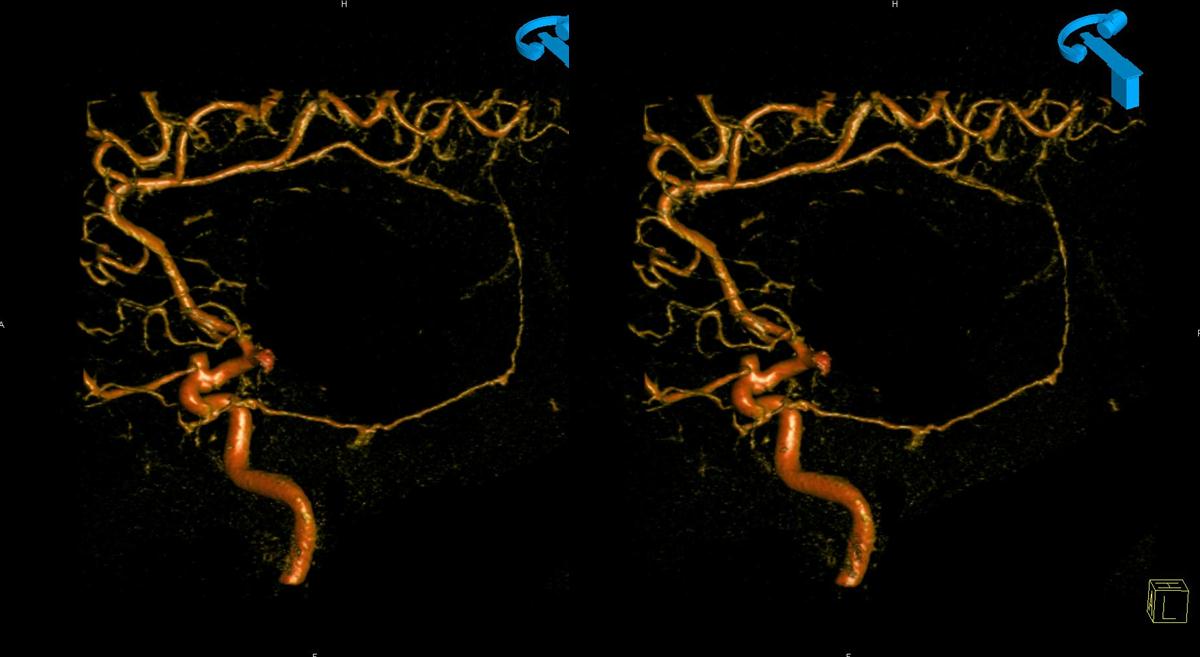
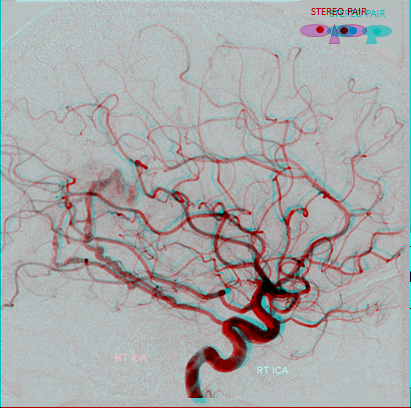
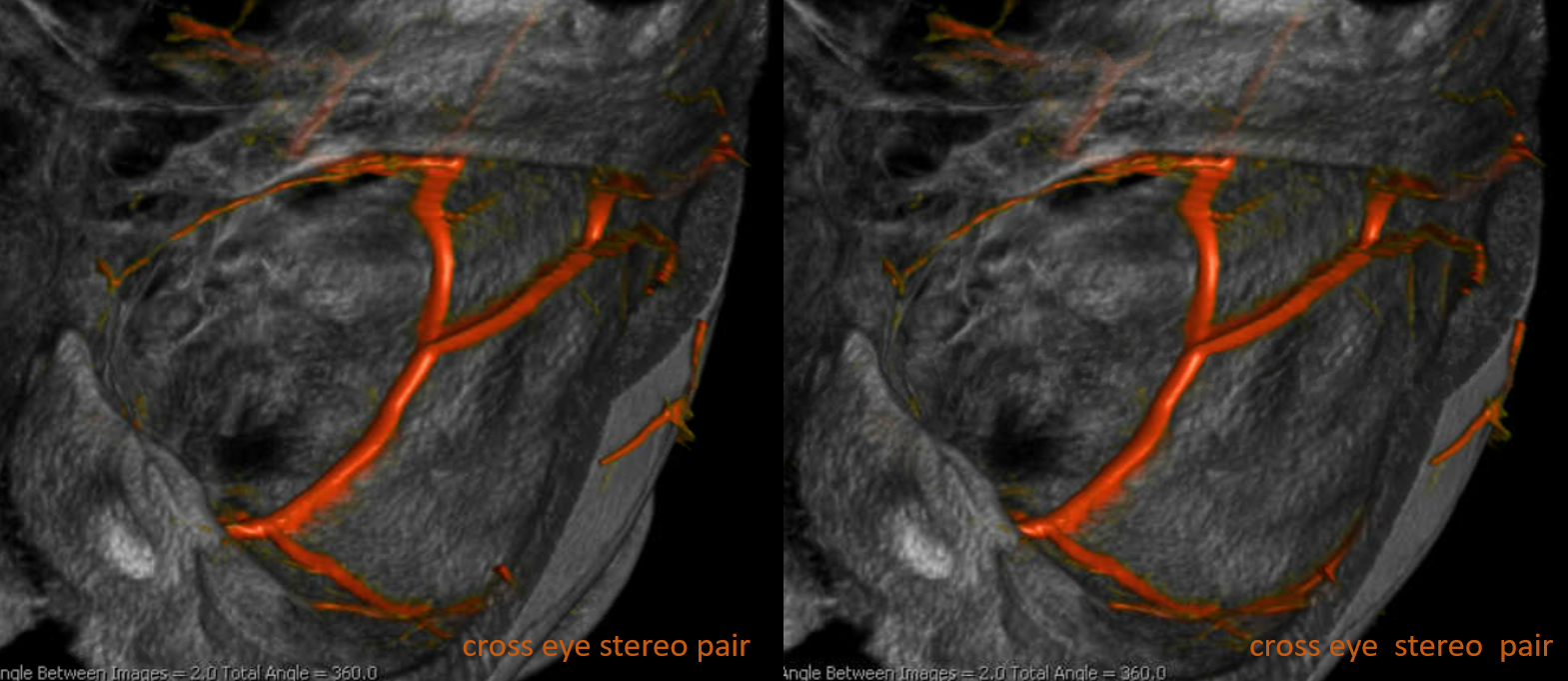
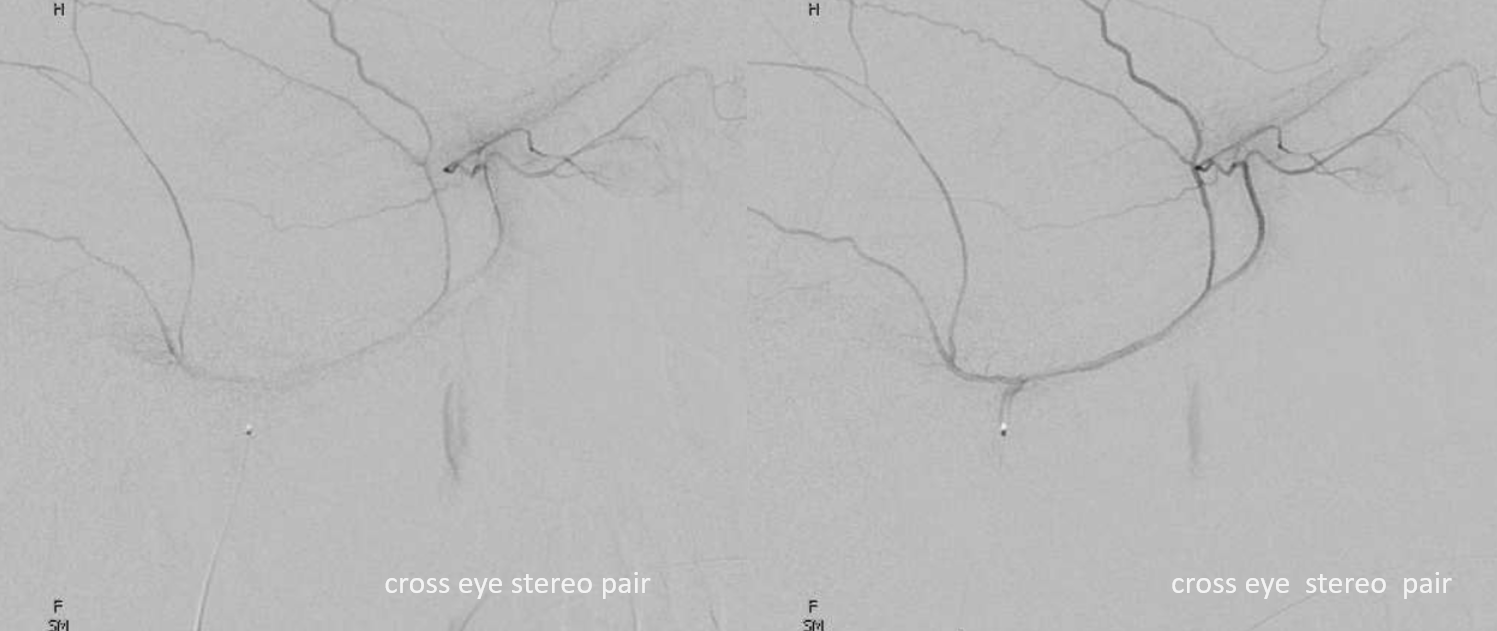
Same in a vintage volume-rendered stereo view (circa 2010)
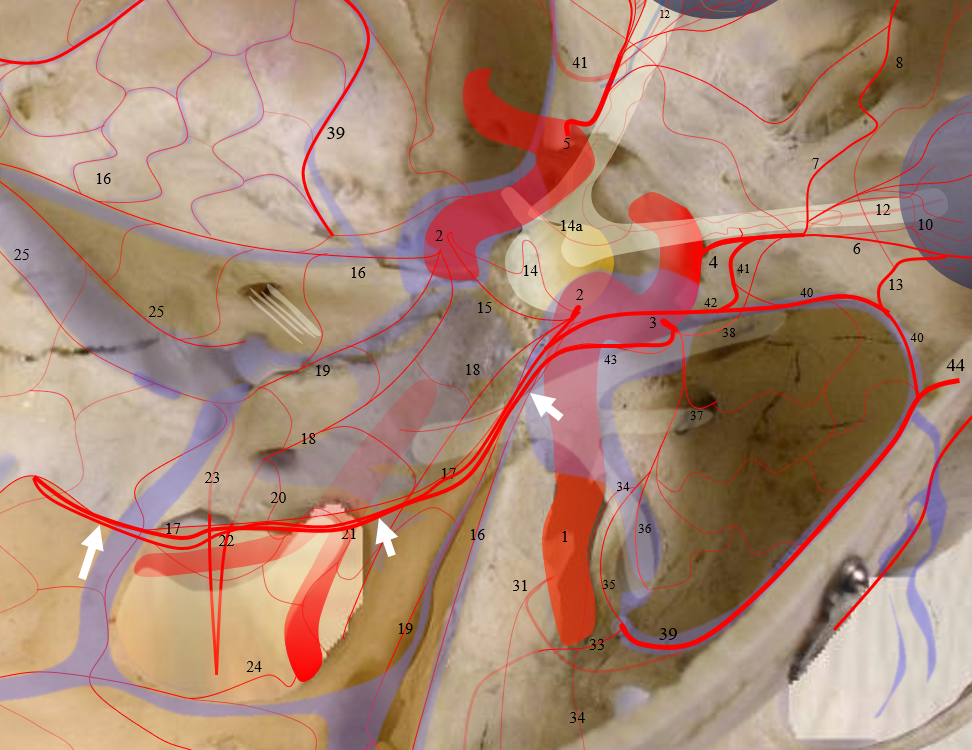
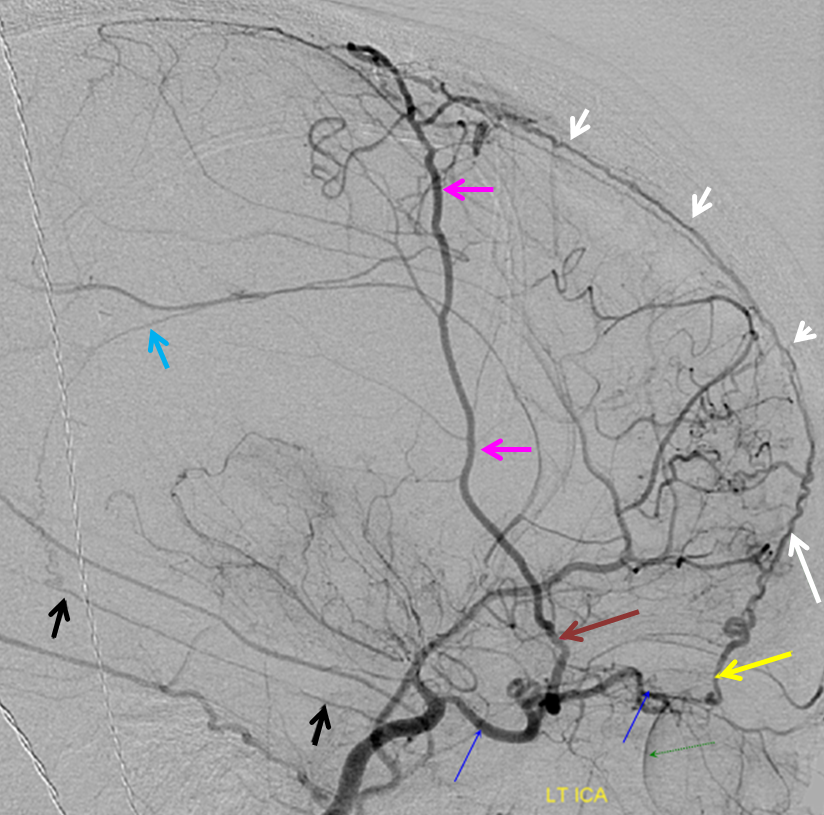
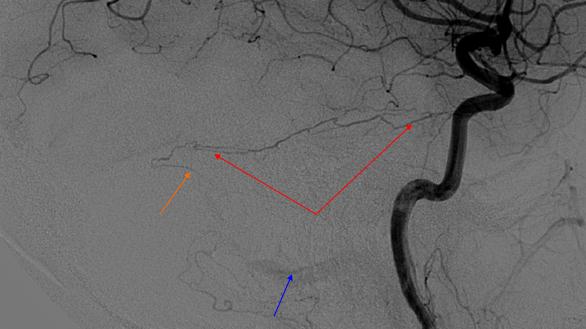
Everything is a spectrum. The dura is a “tabula rasa” for vessels — arteries an veins. Given enough demand, there will be rivers of blood running through the dural sheet — like a flash flood in a desert plain. Here is a falcotentorial dural fistula — look at all of those marginal tentorial vessels (red) off the MHT — just give them more demand and there will be tons more. Look at the rest — several MMA branches (black) and STA (orange) converge upon a sheet of arterial flow (green) within the falx, all heading towards the fistula (blue). Notice also innumerable “Davidoff-Schechter” arteries — that ball of arterial vessels anterior to the fistula venous pouch are all pial-dural Davidoff-Schechter anastomoses (there is a fetal PCOM here).

Another falcotentorial junction fistula — giant marginal tentorial (red arrows)
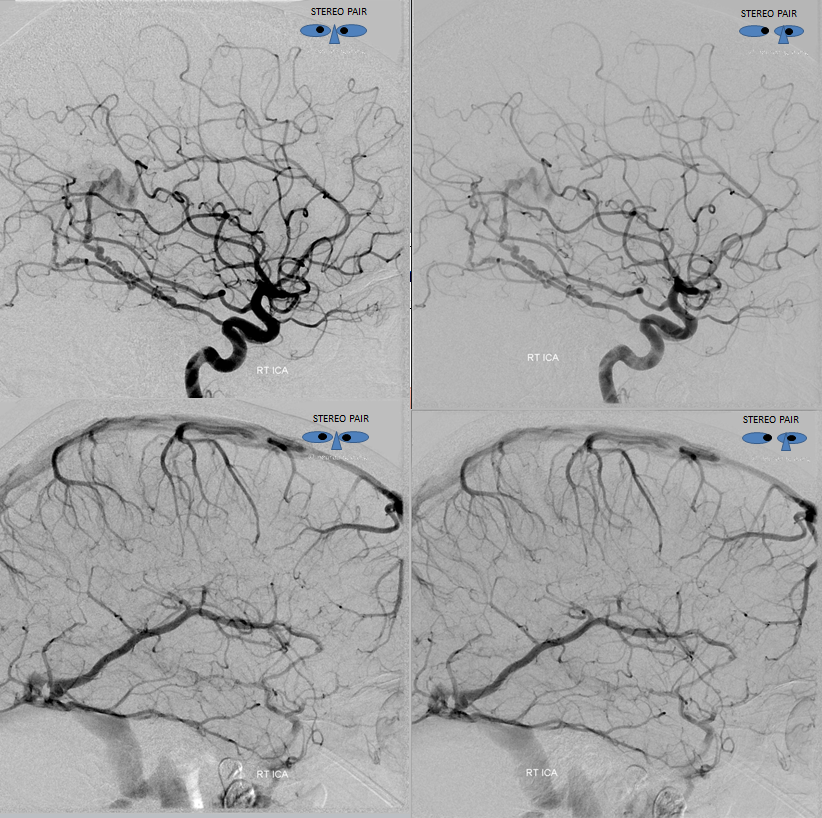
Anaglyphs
Stereos
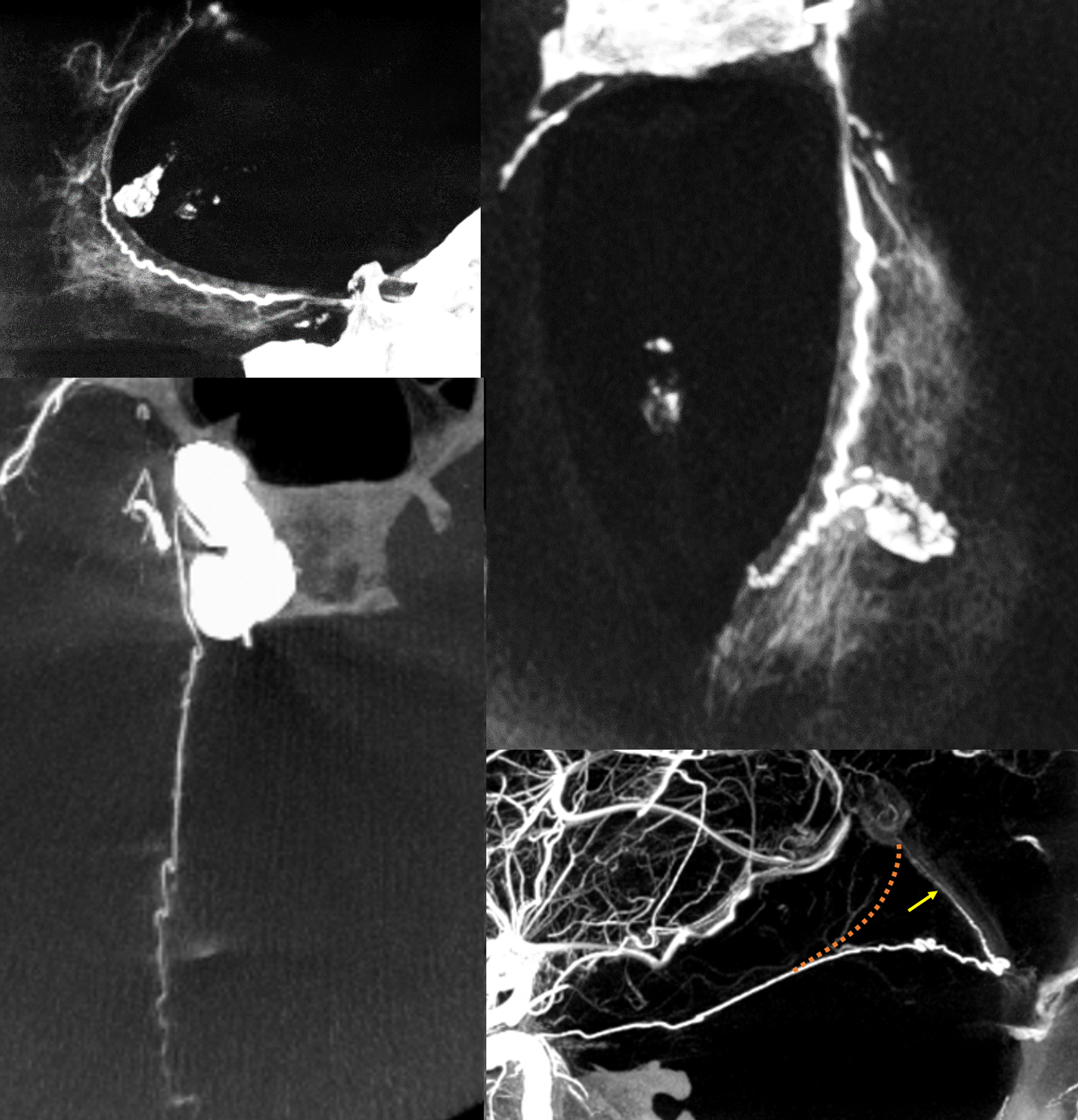
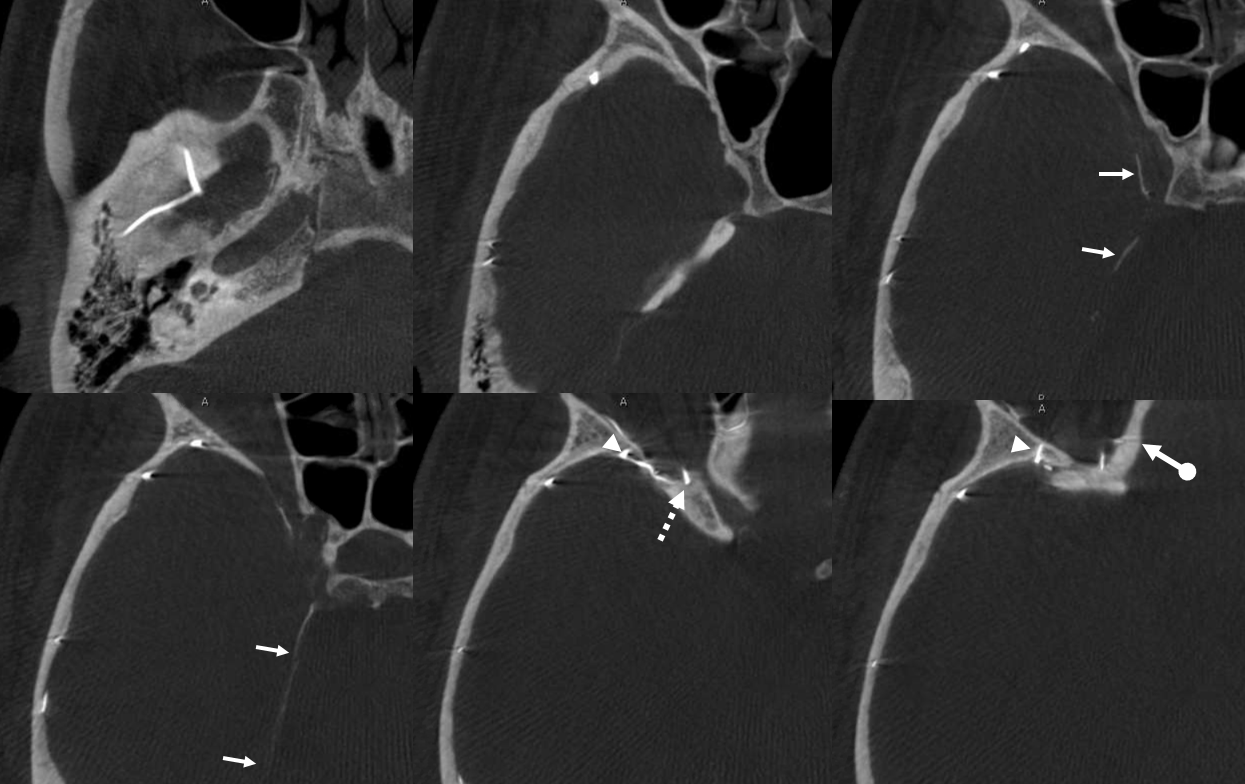
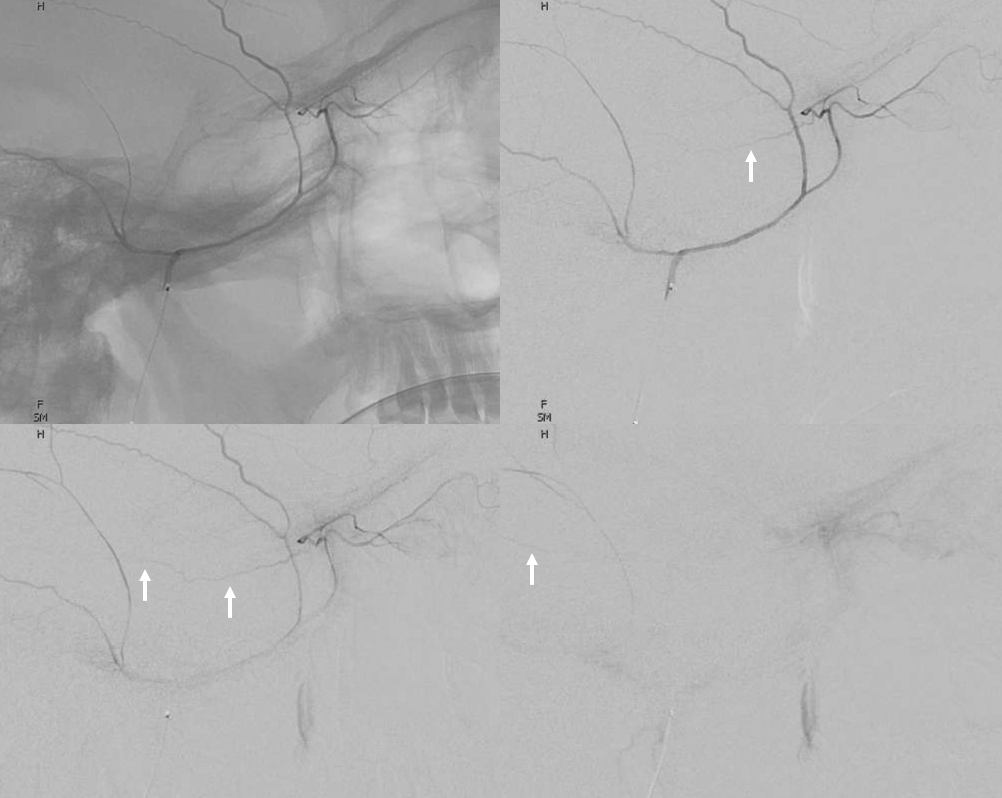
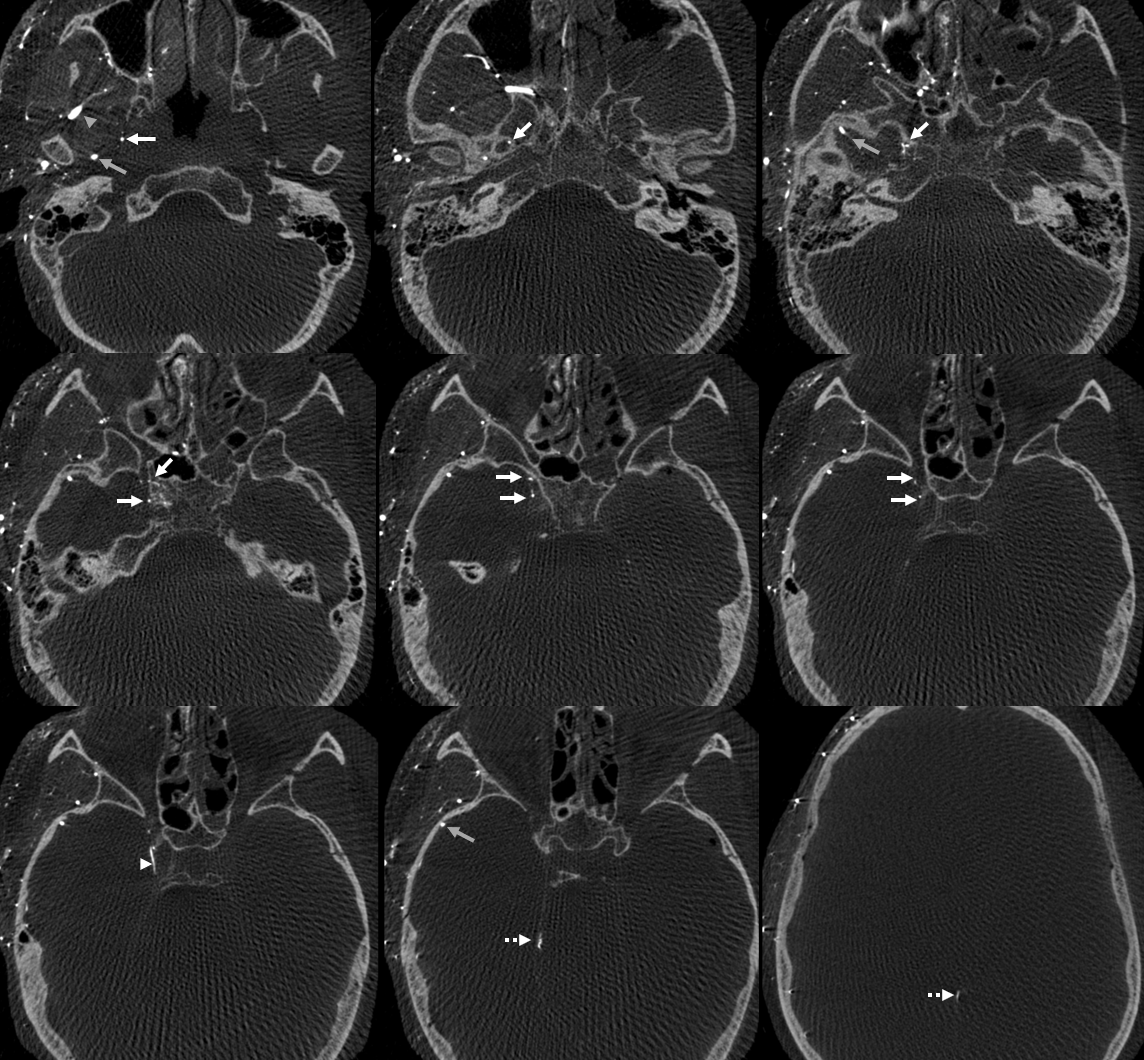
Bodies don’t read books. In example below, the meningeal contribution to the orbit includes both classic “meningolacrimal” artery via foramen of Hyrtl (arrowheads), and a superior orbital fissure contribution (dashed arrow) that mainly goes to the posterior ethmoidal foramen (ball arrow). Neither directly supplies the orbit. Also present is a rare but important connection to the tentorial arcade (arrow) going backwards — usually supplied by ILT .
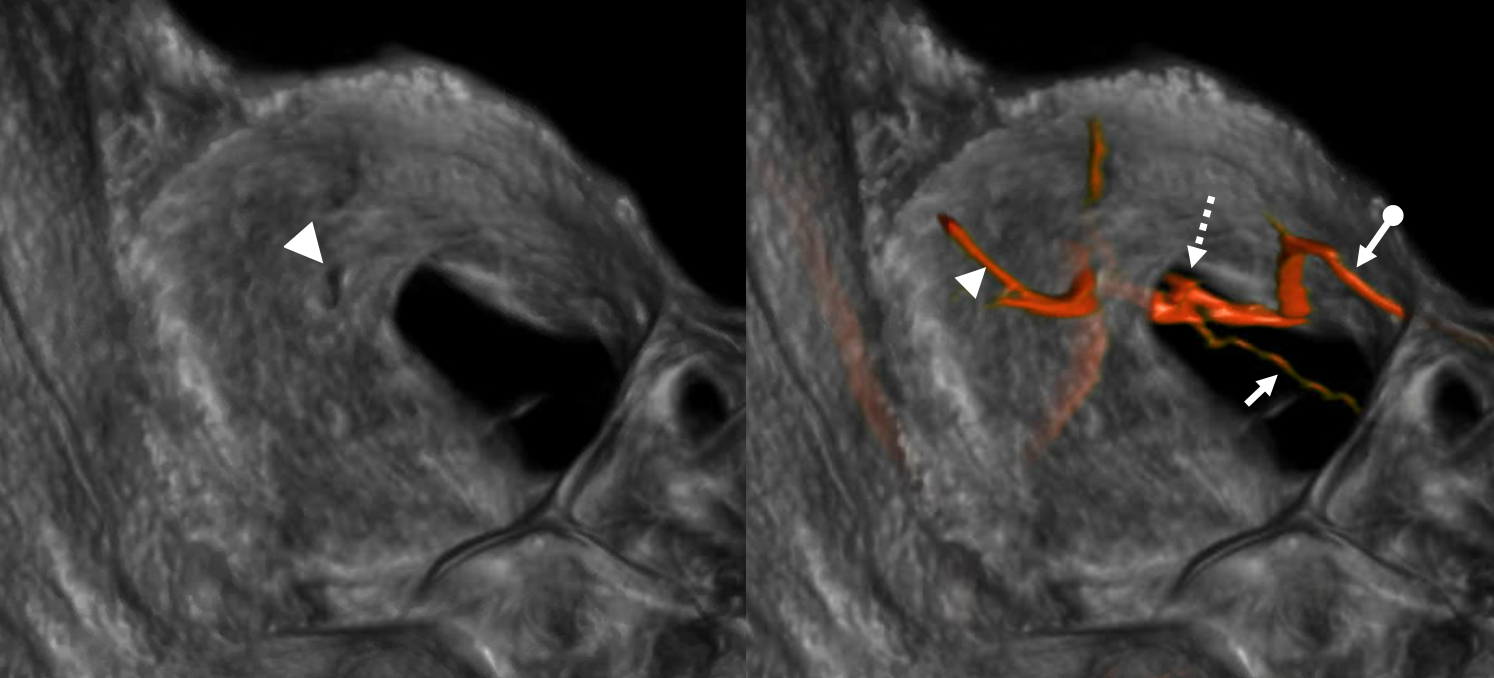
The recurrent tentorial branch (arrows) heads far posterior to become the free margin artery (Bernasconi-Cassinari)

Movie — pause and scroll thru images
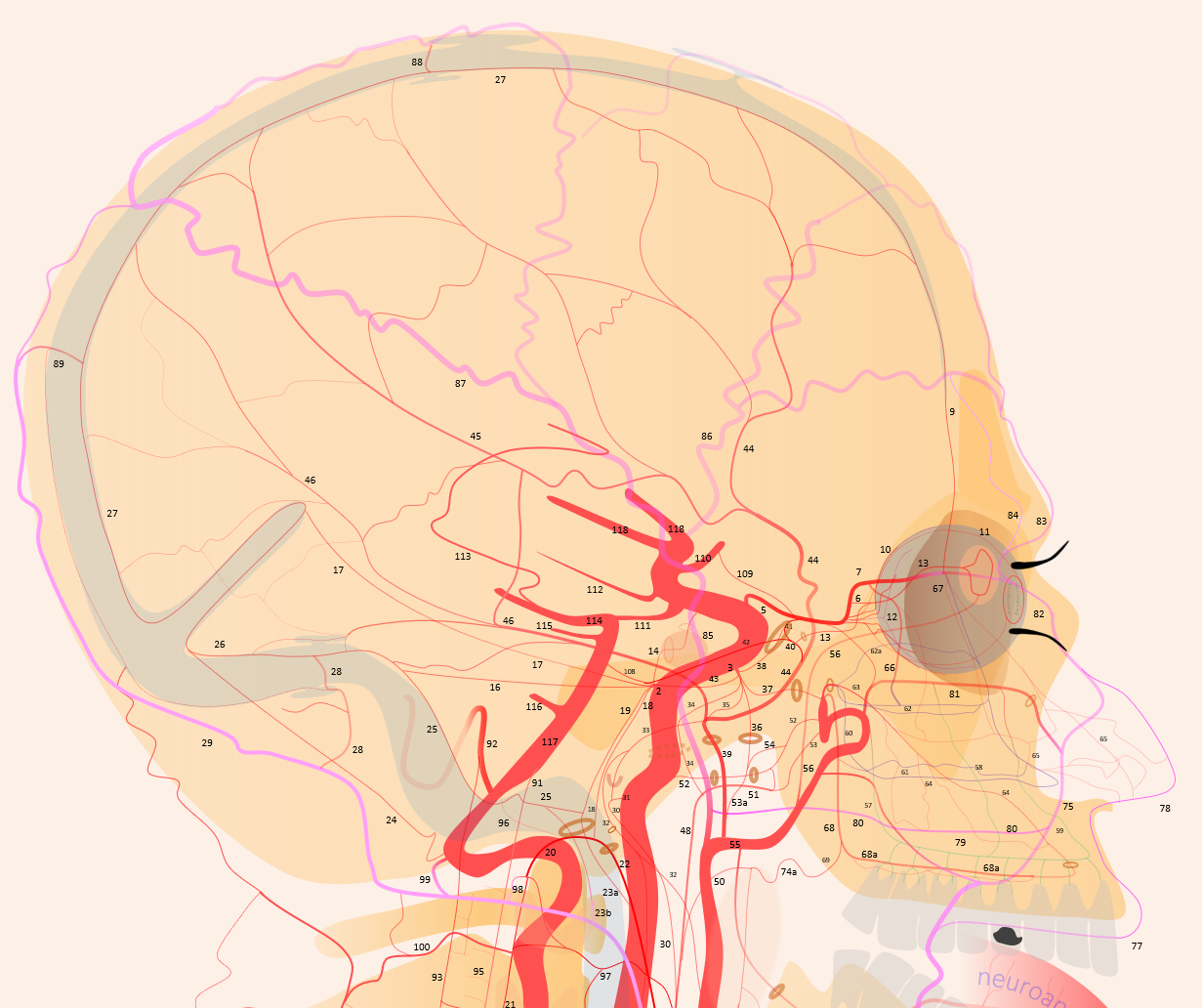
Post-radiation vasculopathy — a sad case of total brain irradiation in a child, treated abroad for a presumed malignancy. Years later there is extensive Moya-Moya like change. There are multiple meningeal autosynangioses, with a prominent anterior meningeal artery (the anterior part of Superior Sagittal Sinus artery — white arrows) forming a network with frontal branch (pink) of MMA (recurrent meningeal variant, sphenoid branch = brown arrow). Also notice medial tentorial (Bernasconi-Cassinari) branch (black arrows) of MHT supplying dural branch in the wall of inferior sagittal sinus (light blue arrow). The separate pericalossal arteries are faintly seen slightly higher
Accessory Meningeal Supply of Cavernous Sinus and Marginal Tentorial Arcade (Bernasconi-Cassinari) via the deep recurrent meningeal artery
Variations are endless — here is one where recurrent meningeal from ophthalmic supplies frontal MMA territory (below)
Posterior MMA territory is via classic MMA . However, a very large accessory meningeal (solid arrow) directly supplies the cavernous / ILT region (the ILT is thus hypoplastic) and, via large deep recurrent meningeal artery along the free edge, continues as prominent marginal tentorial arcade (dashed arrow) way above the falcotentorial junction — to the inferior sagittal sinus region
Note how separate origin of MMA (grey arrow) and Accessory Meningeal Artery (white arrows) is associated with the superficial course of the IMAX (grey arrowhead). The marginal tentorial is dashed arrows
Movie — everything is there — stop and scroll thru individual images
How do u tell on a lateral view the medial vs lateral tentorial arcades? The former has a gentle upward swing towards the falcotentorial junction. Latter (red) dips down towards the sigmoid sinus — in this fistula case. See lateral tentorial arcade page here
Frontal view of course is clear
