Here is the party version — from terminal IMAX in pterygopalatine fossa, the descending palatine artery goes down in the greater palatine canal (with the greater palatine nerve), goes through the greater palatine foramen, after which it changes name to greater palatine artery and runs forward along the hard palate, supplying the nearby tissues (the lesser palatine artery goes back towards the soft palate, into a super collateralized area with ascending palatine and superior pharyngeal and vidian arteries). The terminal greater palatine artery anastomoses in the incisive canal region with the contralateral greater palatine artery and the terminal branches of the sphenopalatine artery. The incisive canal is in midline, so either midline septal branches or distal turbinate branches of the sphenopalatine can get there. In this area there is no shortage of anastomoses.
The real truth is that, like everything else, there is tremendous variability here also. For example, the descending and greater palatine might be one or several vessels, or a loose palatine network. It might supply the inferior turbinate — which is classically the territory of sphenopalatine artery. Or that it also supplies the teeth — not just the alveolar arteries. Its small stuff — there are much more important misconceptions out there where brain is concerned for example — but still, just remember that all those classic pictures are just that — nice pictures.
Here is definitely a truth — the descending palatine is a bit vulnerable to trauma in the greater palatine canal, were it can be injured during LeFort fractures, traumatic or iatrogenic as part of LeFort osteotomies. We are occasionally called upon to embolize a pseudoaneurysm of either the descending or sphenopalatine arteries injured in this manner. See case here.
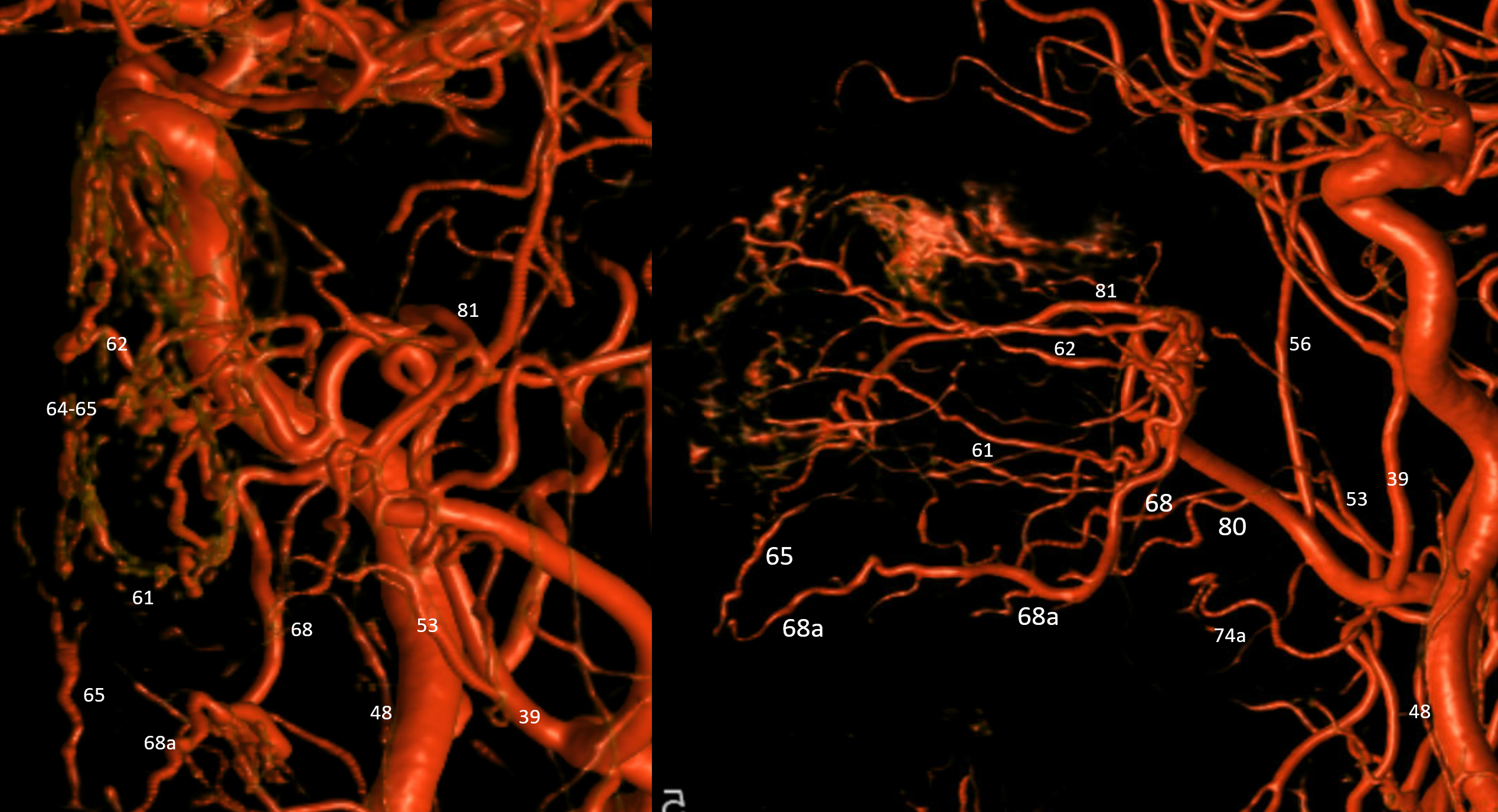
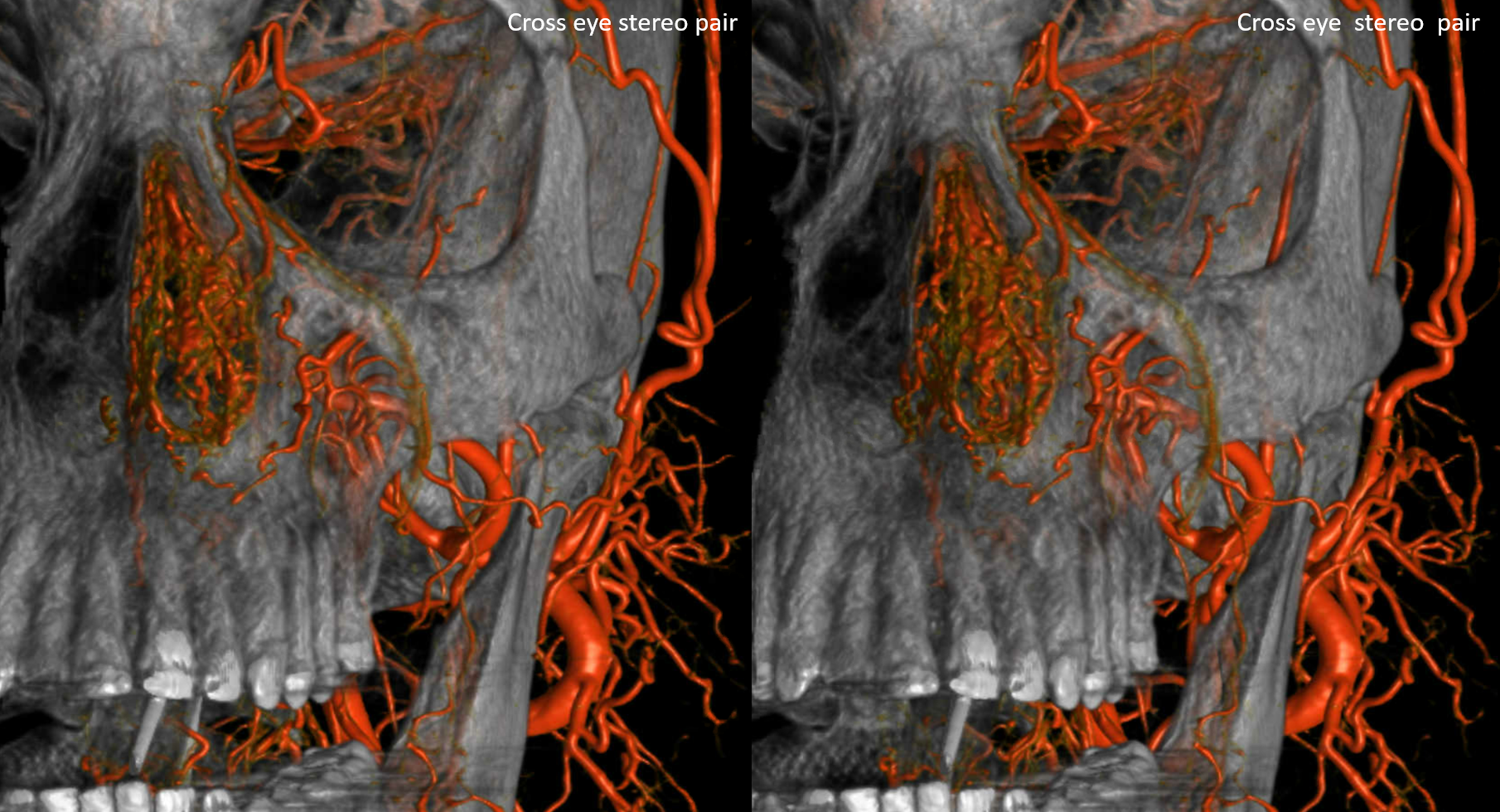
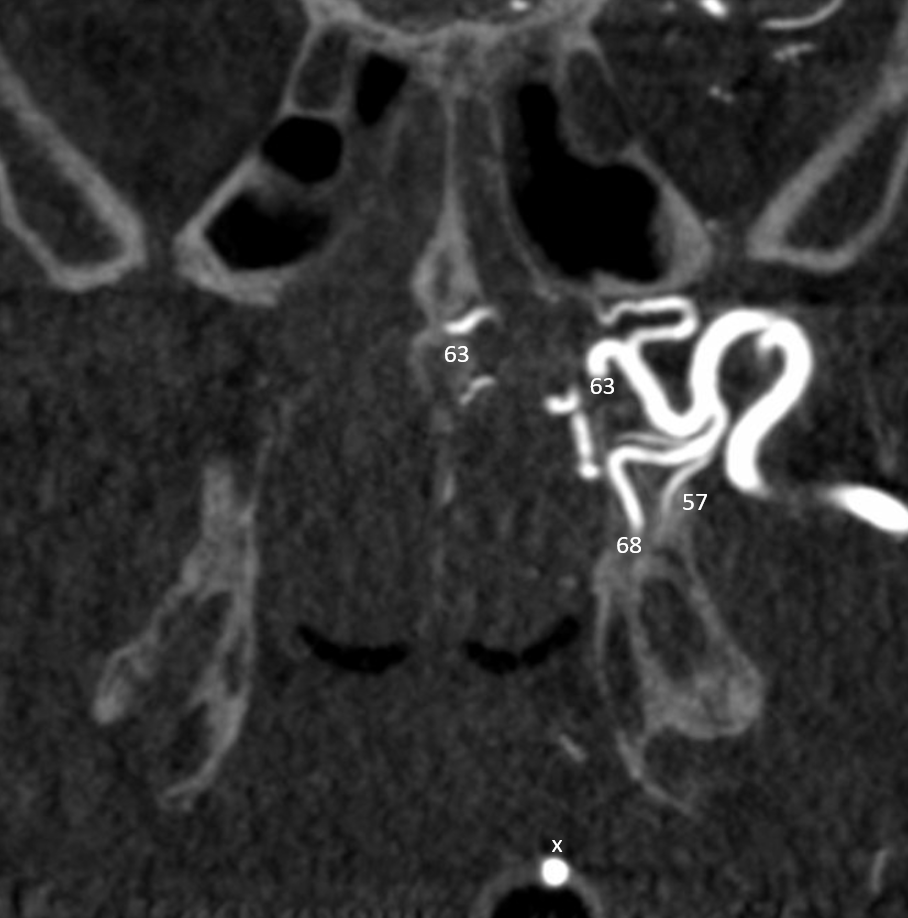
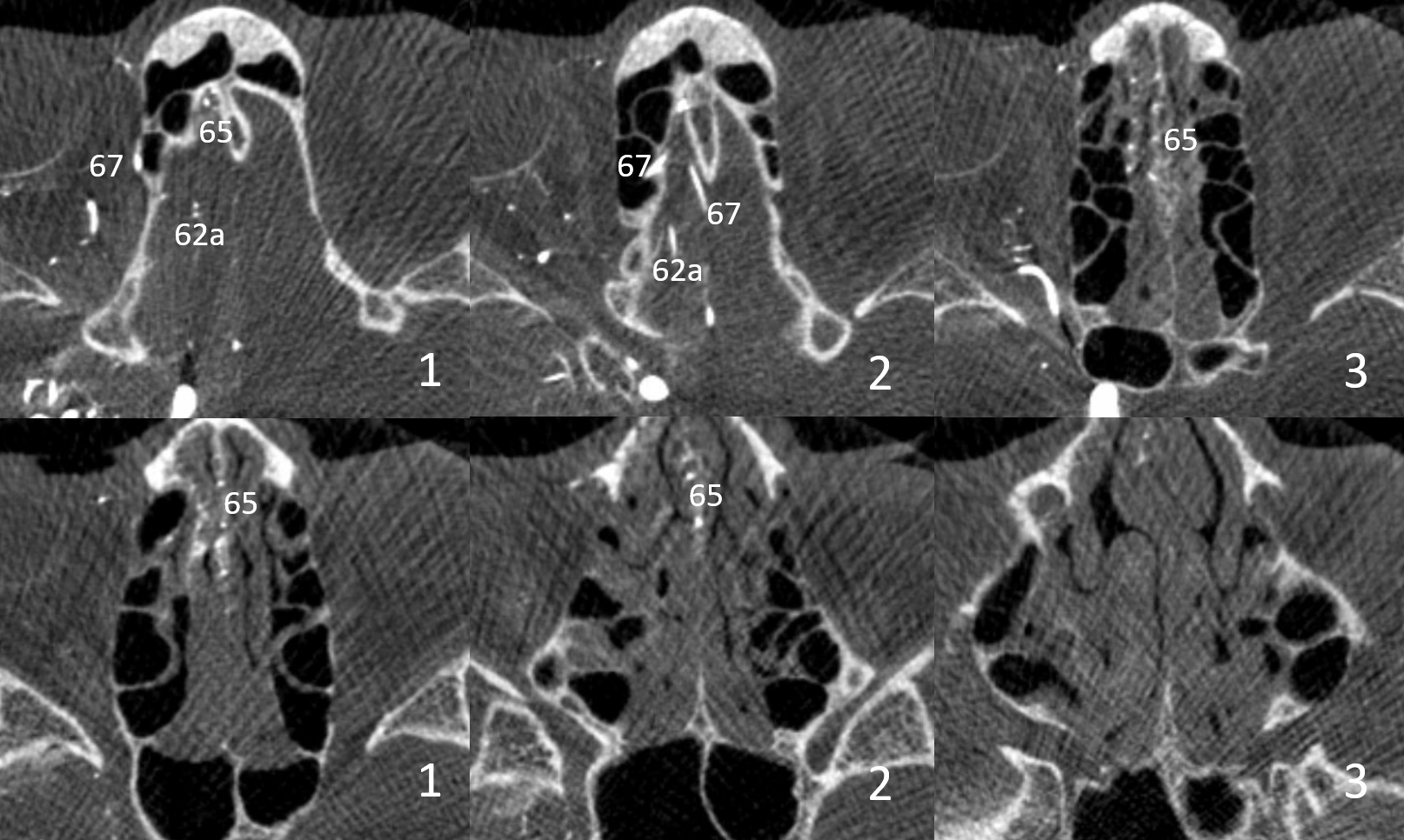
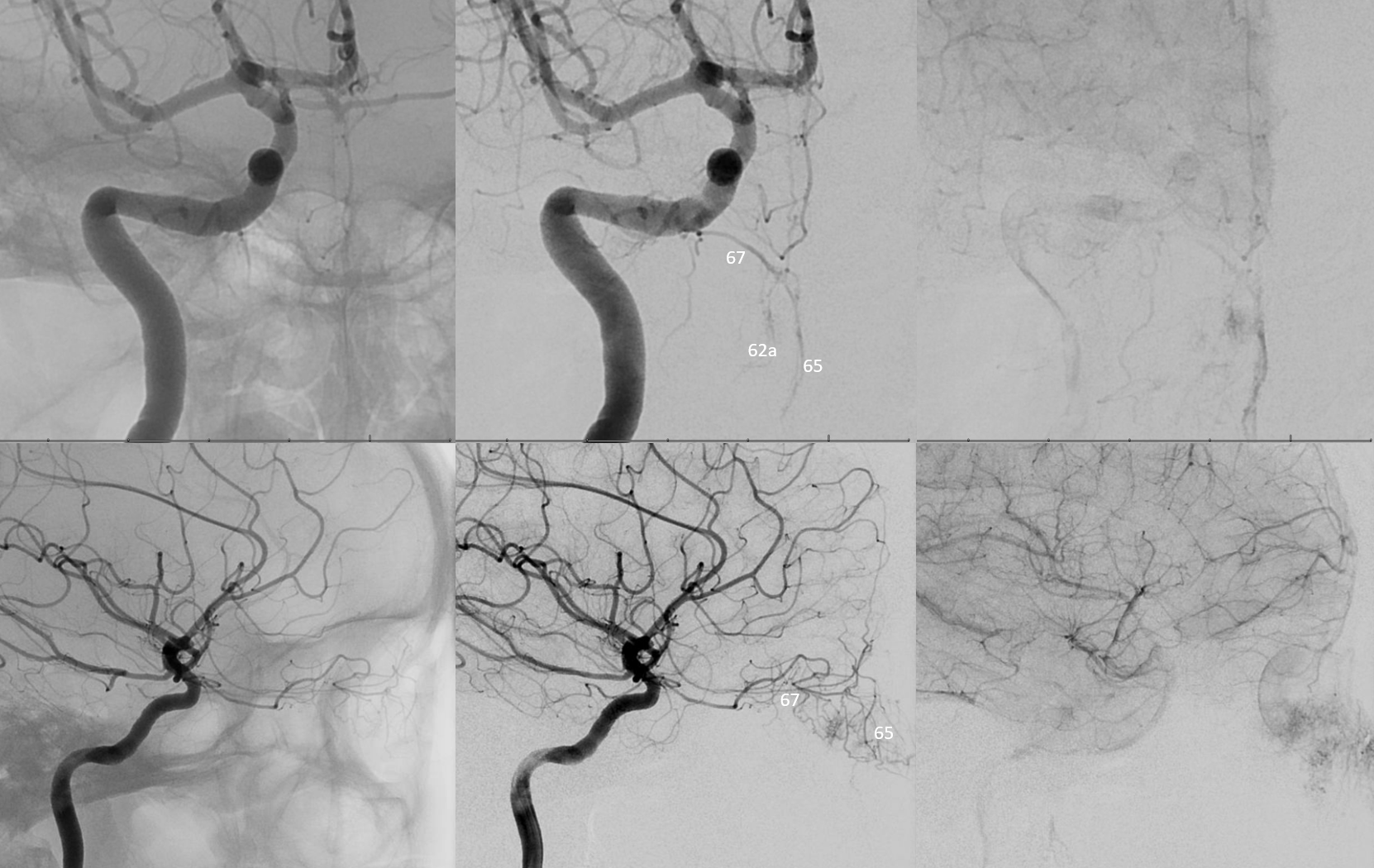
Here is a classic — see “Diagrams and Drawings” for number keys
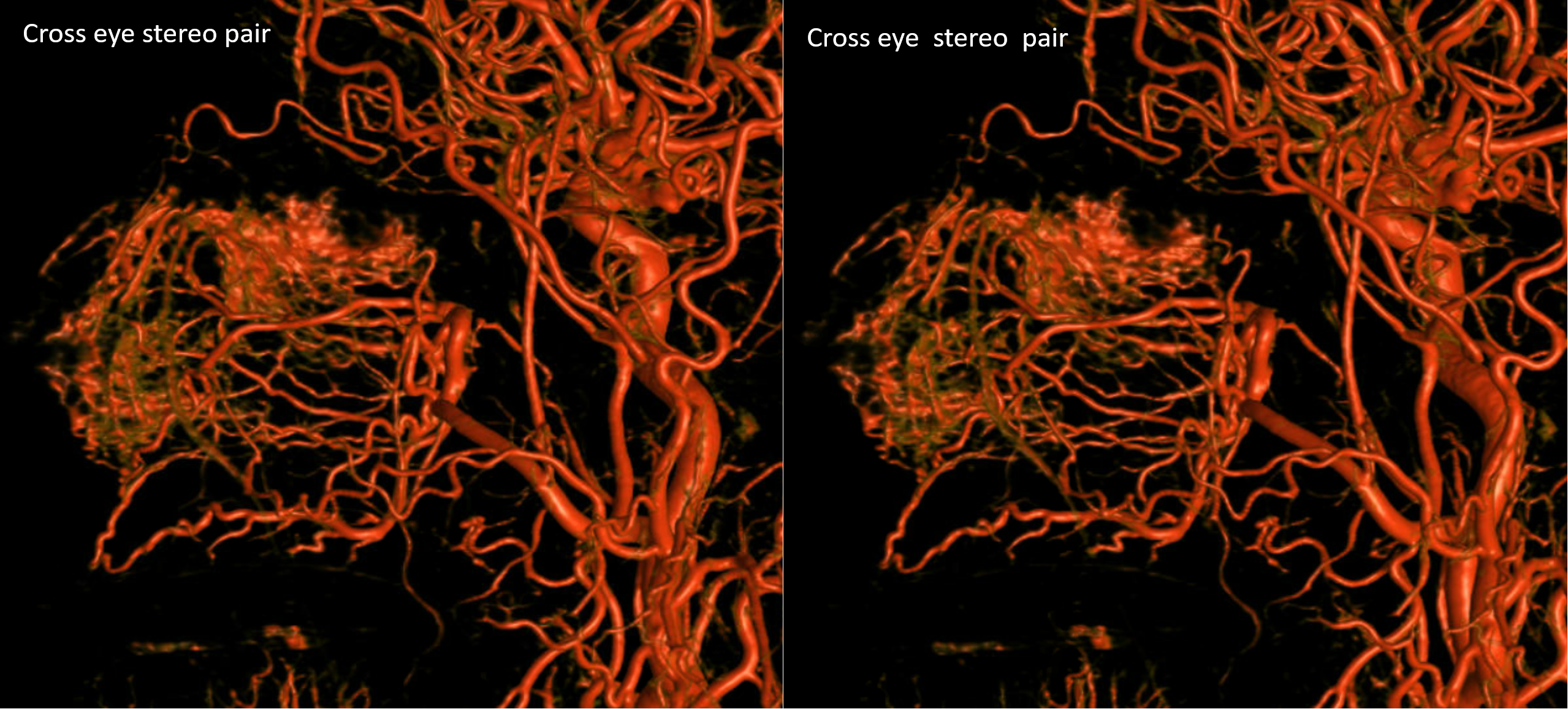

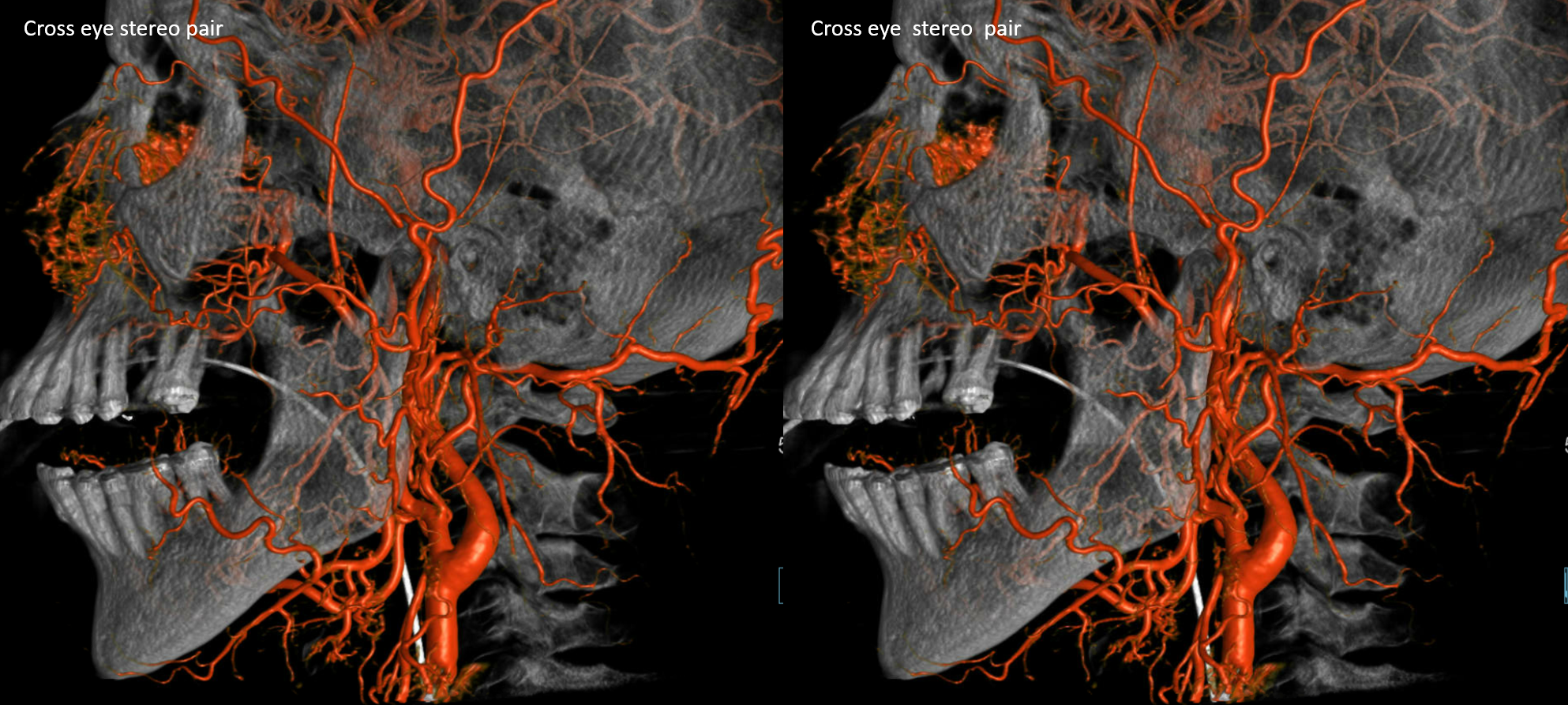
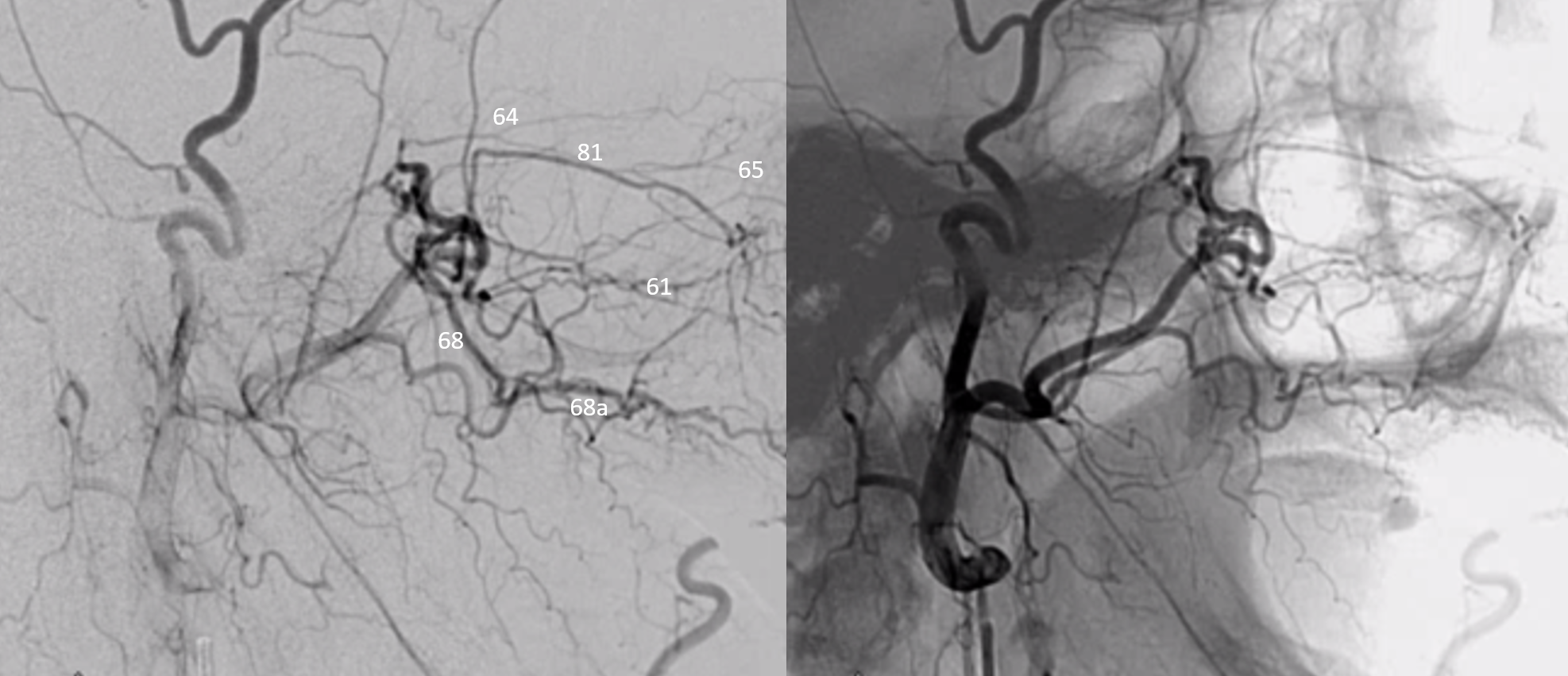
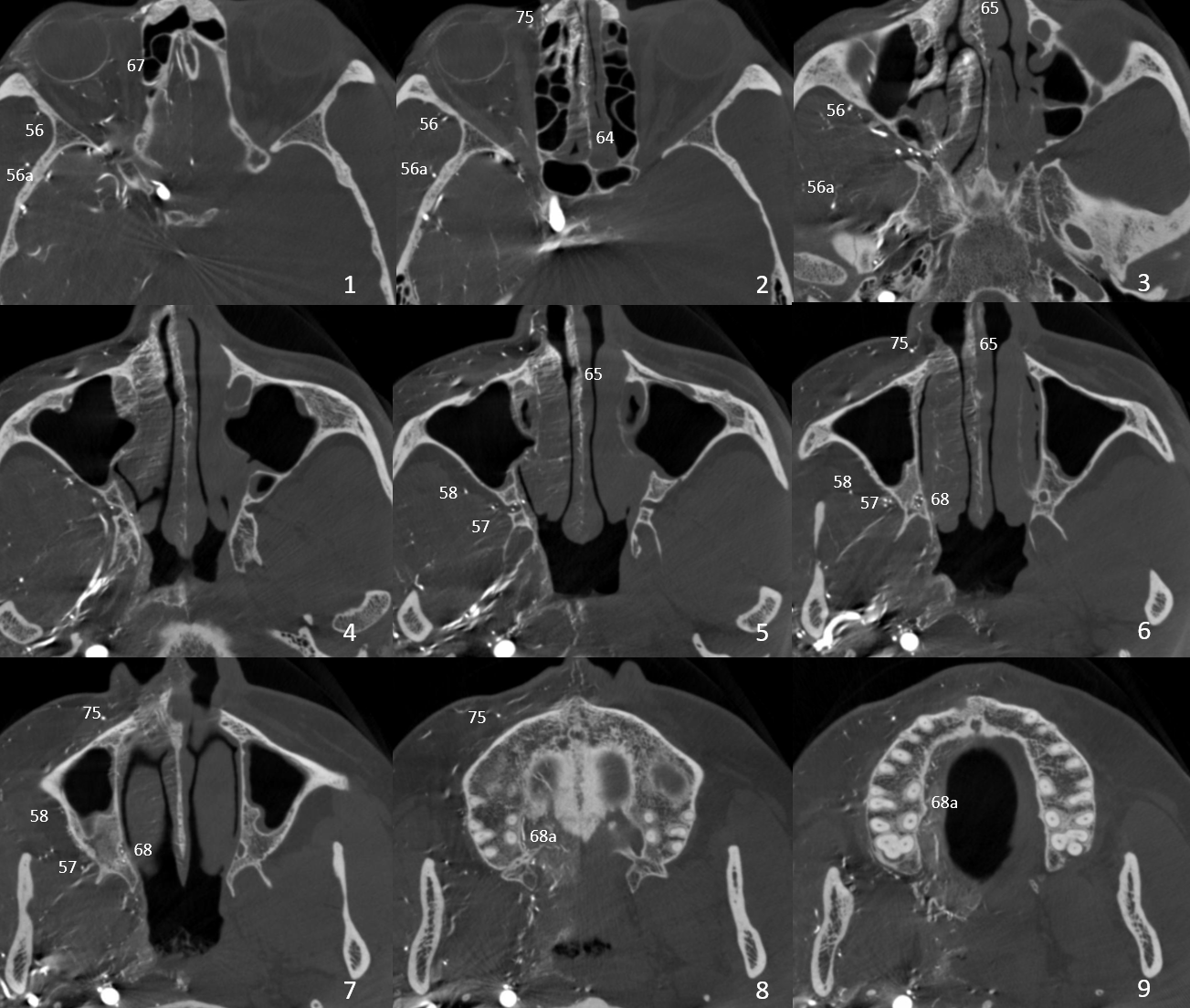
Below is another case — relatively hypoplastic descending palatine — 3 separate vessels in the canal — and a network of greater palatine area vessels instead of single trunk. There is also a larger anterior ethmoidal branch contributing to supply of nasal tissues

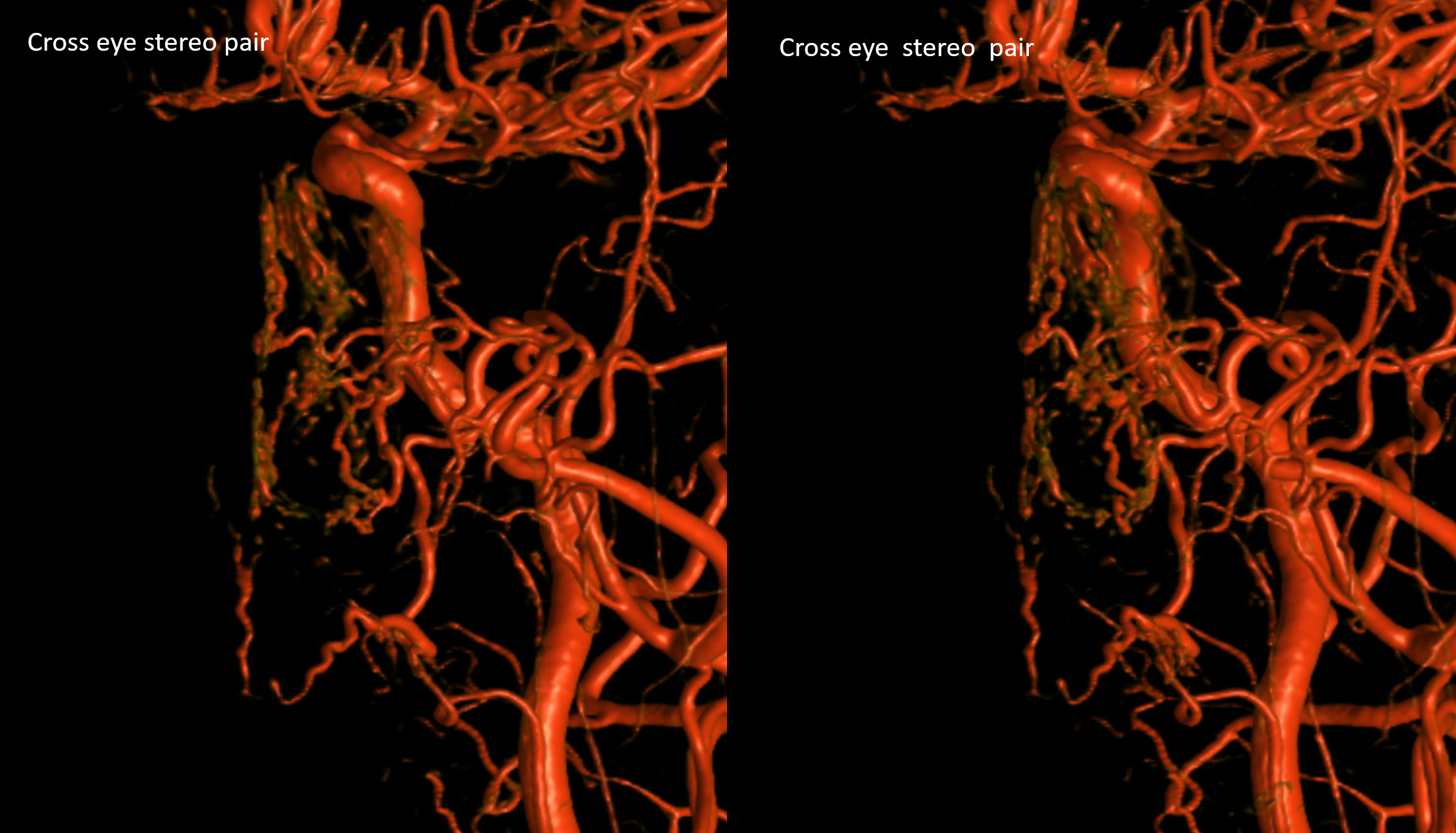
A DYNA of the internal can show the ethmoidal contribution in isolation
Corresponding ICA injection
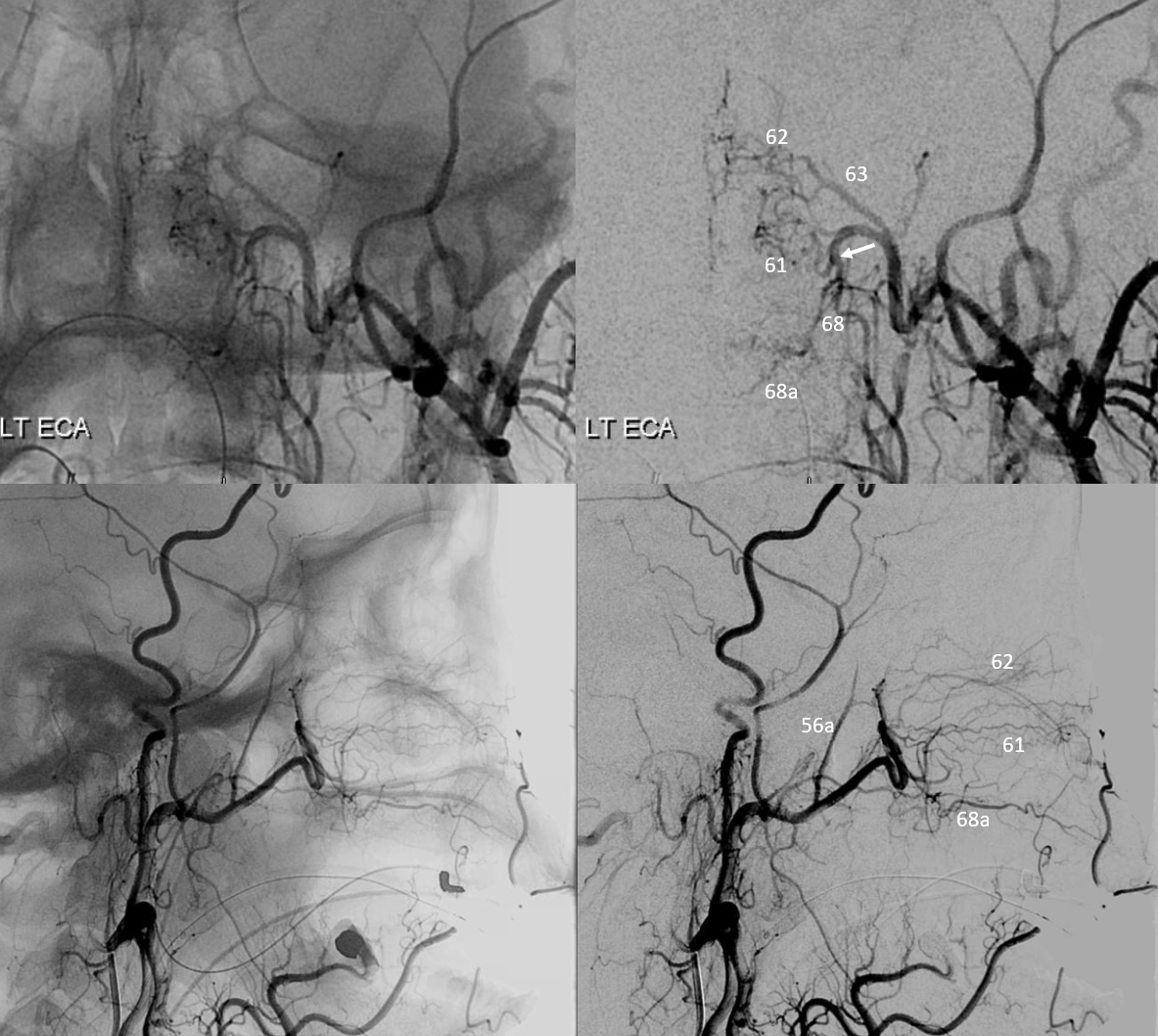
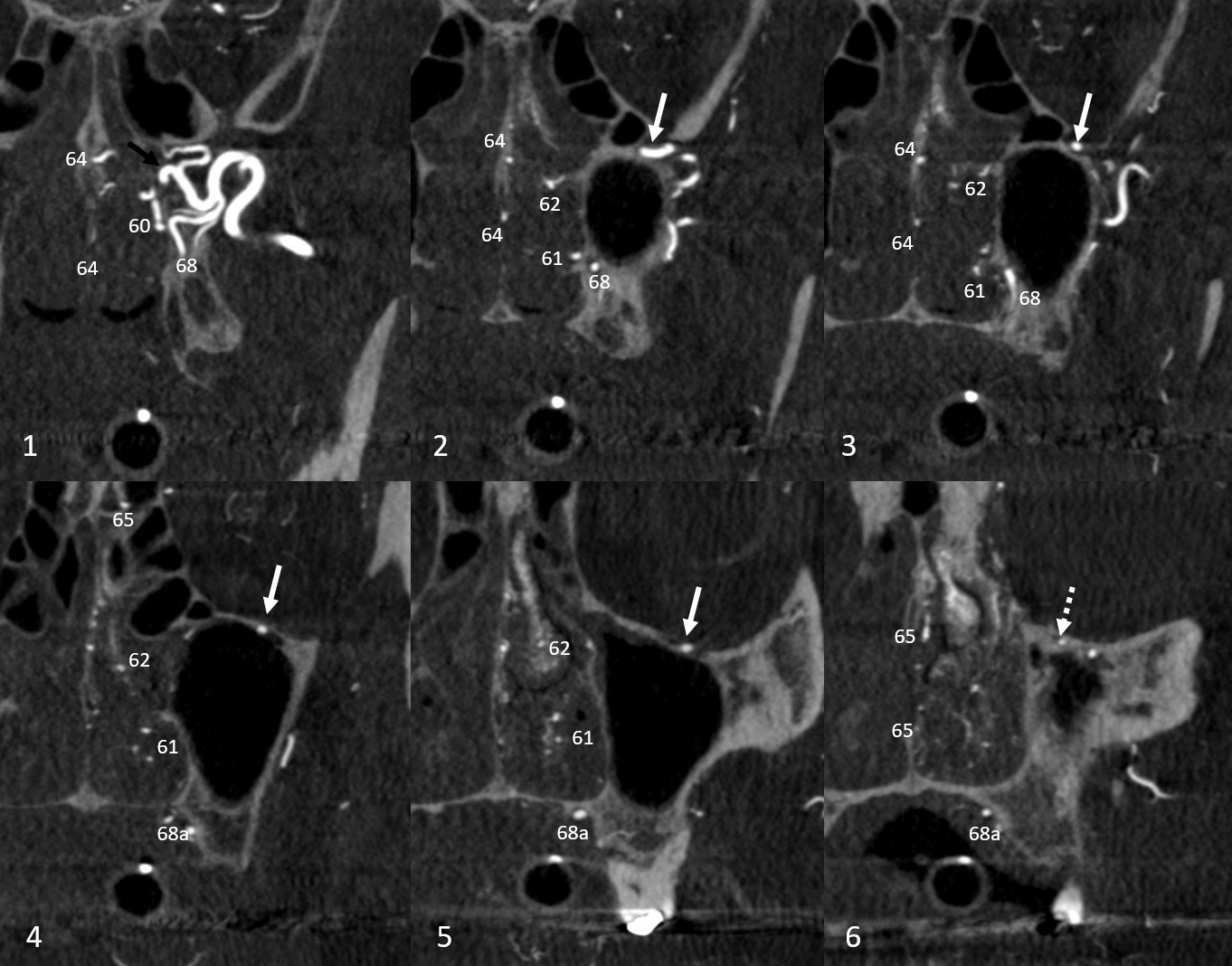
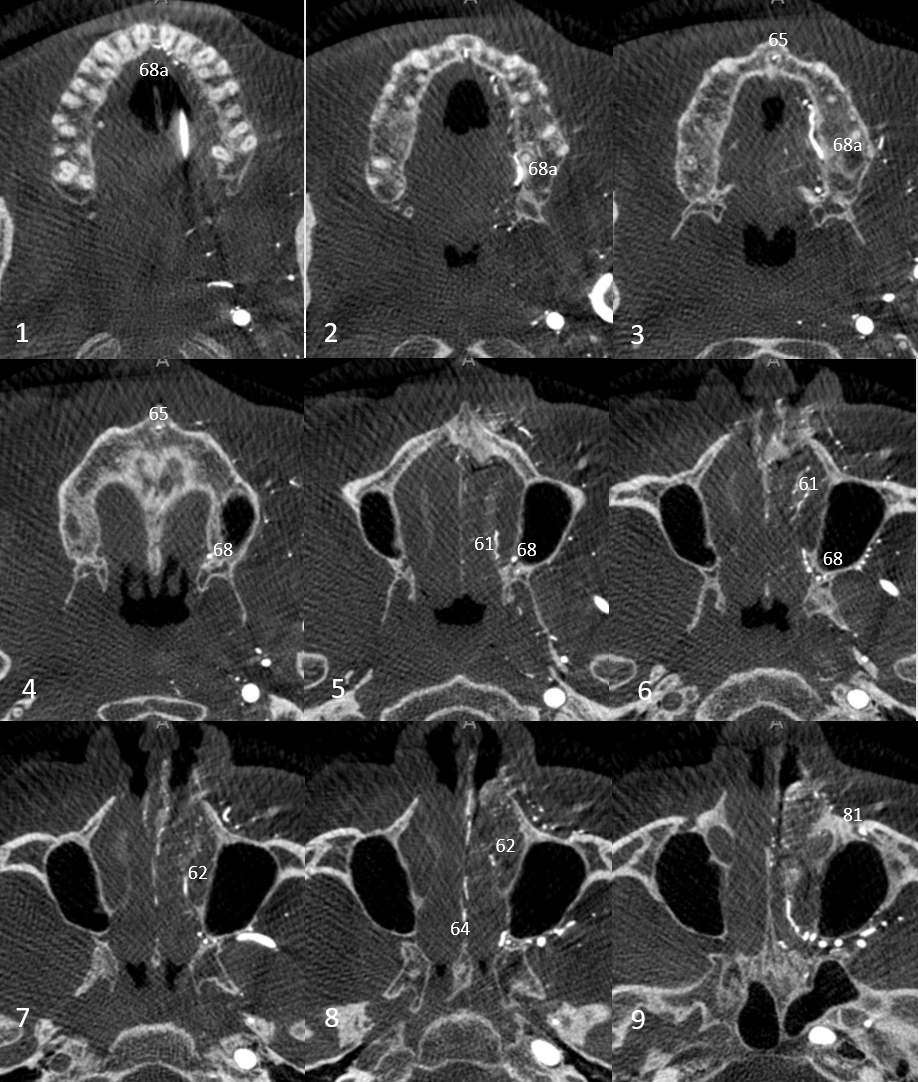
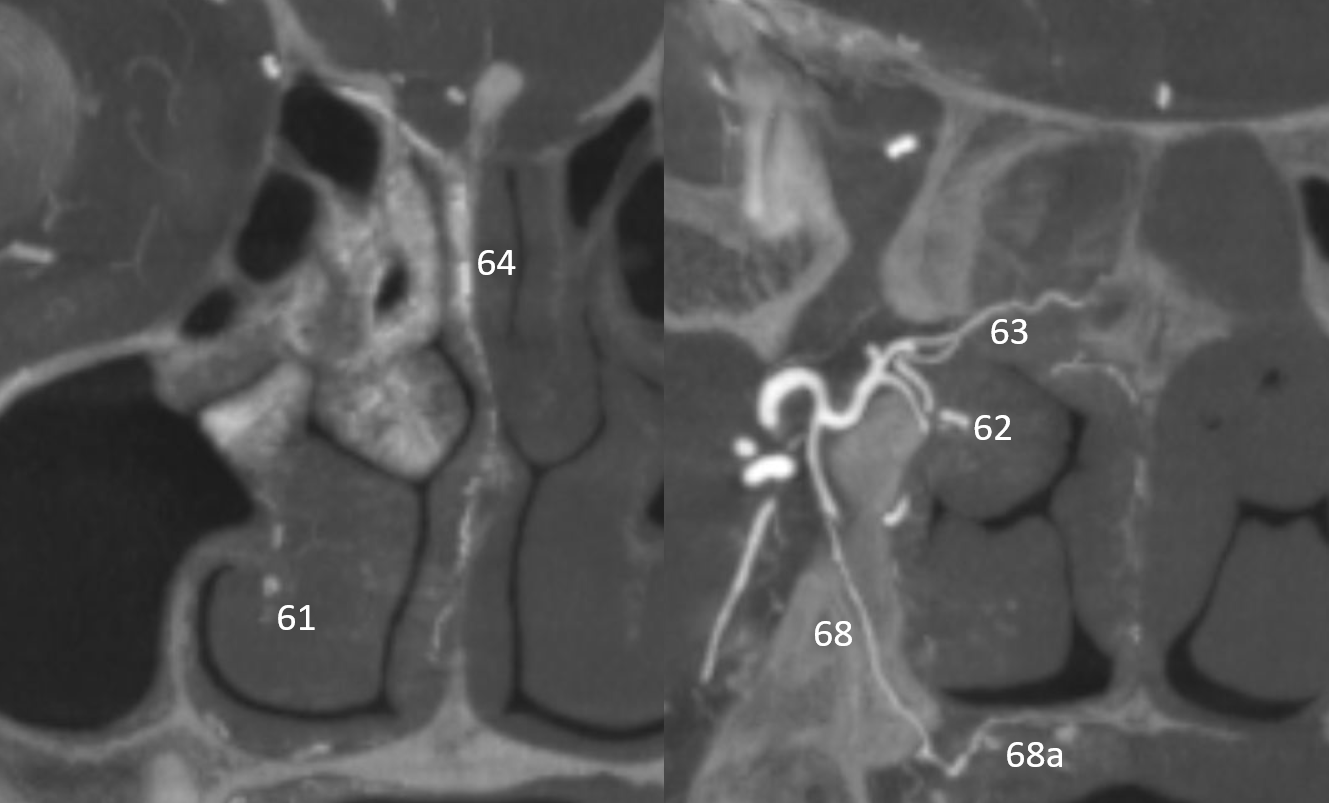
Here is an example of descending palatine supplying the inferior turbinate (usually sphenopalatine territory) (through a hole in the greater palatine canal)
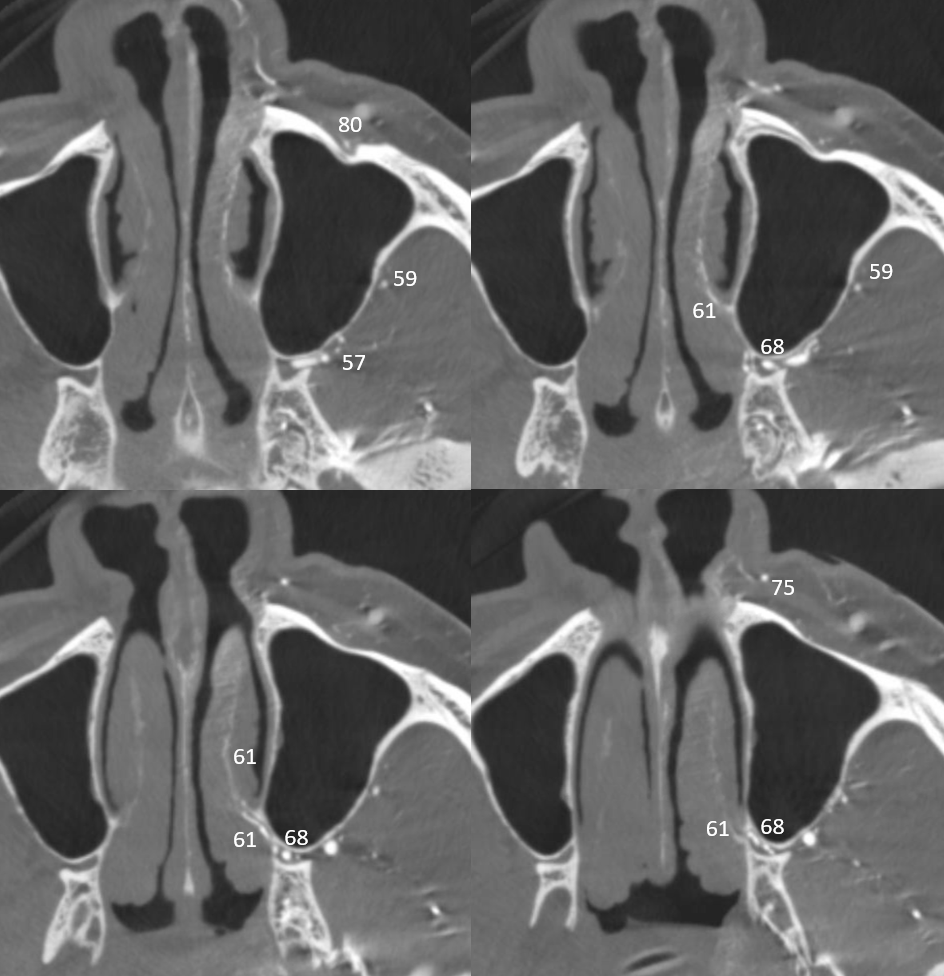
The frontal views are much more helpful on a DSA for all this — arrow points to origin of branch to the inferior turbinate (62)