The petrous branch (33), together with the styloid / stylomastoid branch (32) of the occipital or posterior auricular arteries makes up the “facial arcade” — supplying the facial nerve, gasserian ganglion, the greater petrosal nerve, and other structures of lesser importance (bone, dura) in the area. It is usually very small, originates from the very proximal intracranial MMA (as soon as it emerges from spinosum) and projects posterior and somewhat medial. As always, there are many tiny branches in the area that might go to the petrous apex region and nearby dura, but not exactly into the facial canal. The point is that proximal MMA embo is a treacherous idea — besides the petrous branch, there is also the cavernous branch going towards the Meckel cave/cavernous sinus region, and more distal potential orbital anastomoses. See MMA page for complementrary info.
Usually, the petrous branch is tiny. It is hard to see on DSA, especially in lateral view, where it may be obscured by dense temporal bone.
Below is a figure from our JNIS publication on MMA anatomy (different subjects). The petrous branch is labeled with arrowheads. Cavernous with arrows. The very rare recurrent tentorial branch (ball arrow) is opacified via the sphenoid ridge branch (dashed arrows). Notice how small the petrous and cavernous branches are (angio example)
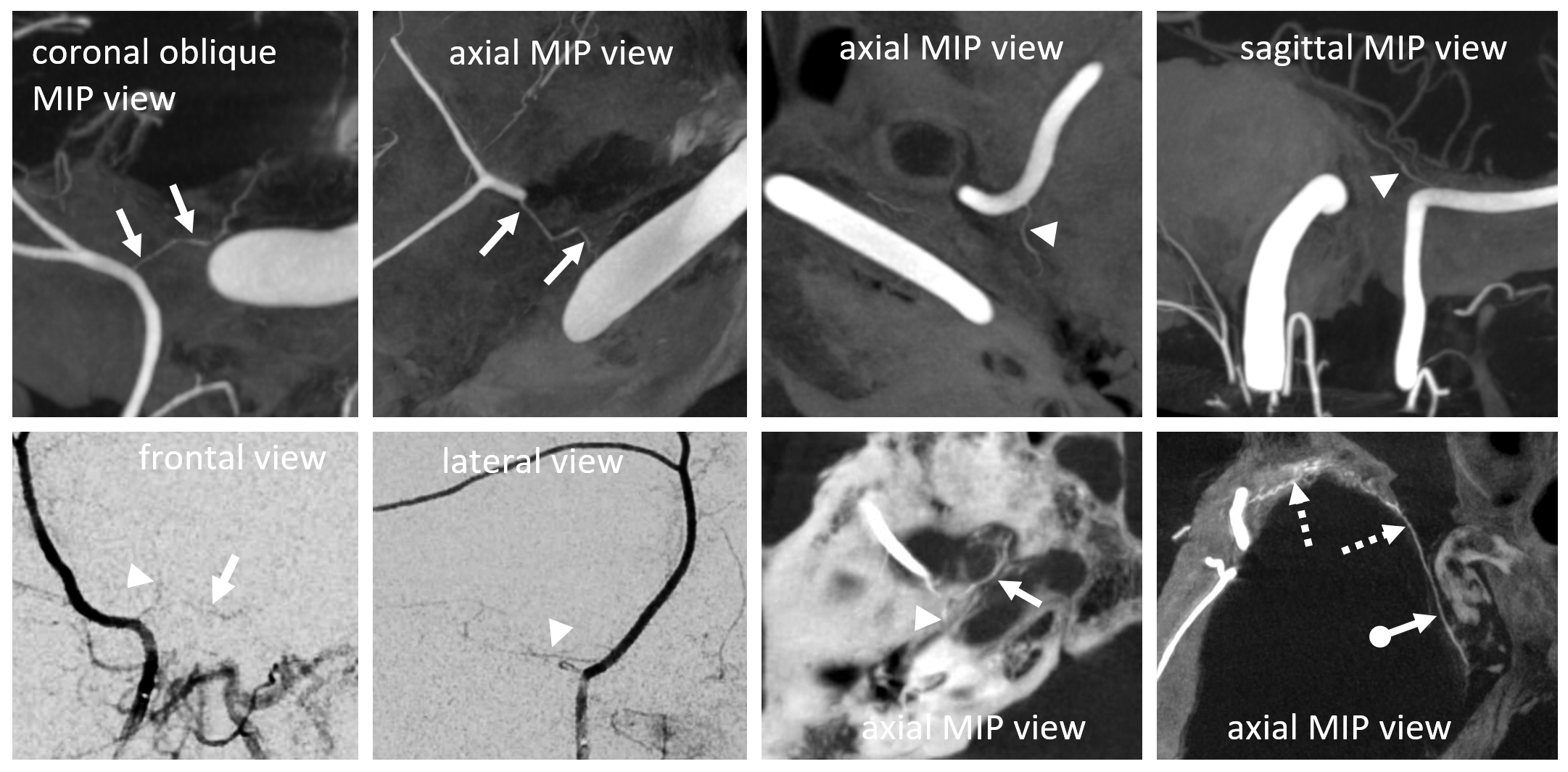
Another angio image — petrous branch (arrowhead) is superimposed in lateral view on the much larger petrosquamosal branch (arrows) — and is frequently confused with it — don’t make this mistake. The petrosquamosal branch, despite tremendous variation in its presence, always projects laterally on frontal views. Petrous branch of course does not. Open arrows point to skull enhancement, which should not be confused for the “cotton wool” appearance of a subdural — there is none in this case.
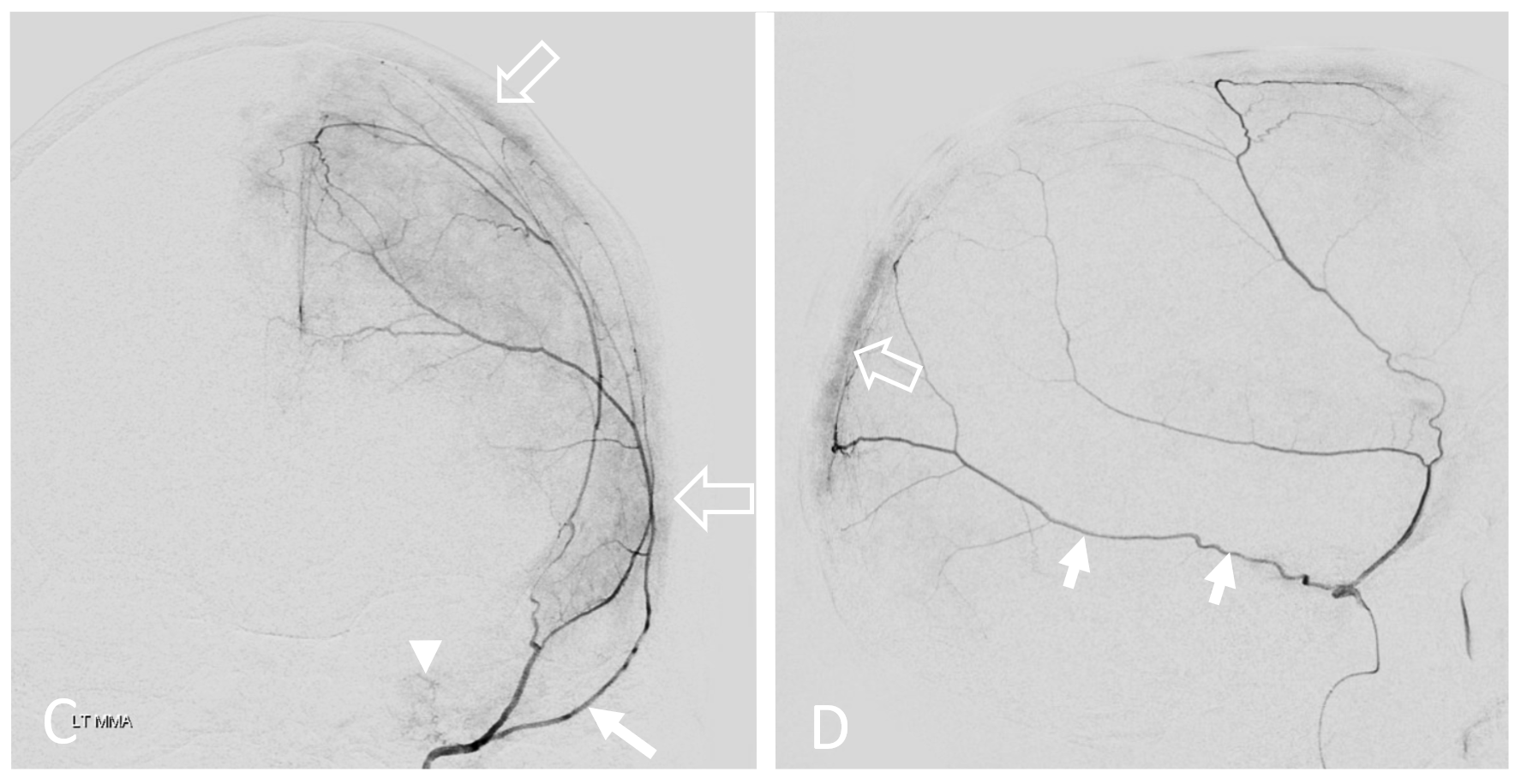
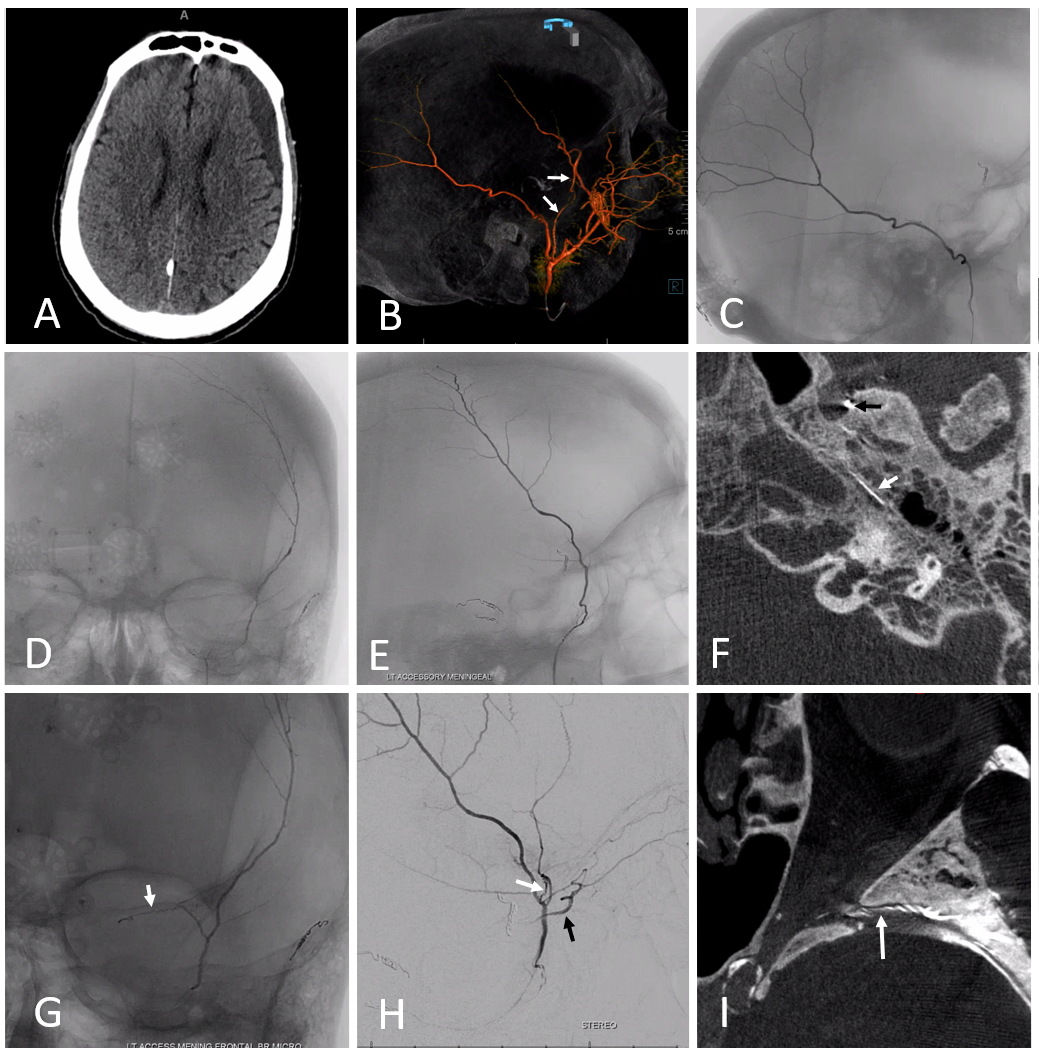
In the case below, a variation is present with frontal MMA branch (B, white arrows) supply from the accessory meningeal artery, which also supplies the petrous branch (F, white arrows. Black arrow is on catheter tip in foramen ovale). Images G, H, and I show sphenoid ridge branch (white arrows) opacifying the ophthalmic artery (black arrow) during superselective catheterization of the frontal branch (in this case of AMA origin) — this connection was not visible on a nonselective injection (B) So, be careful…
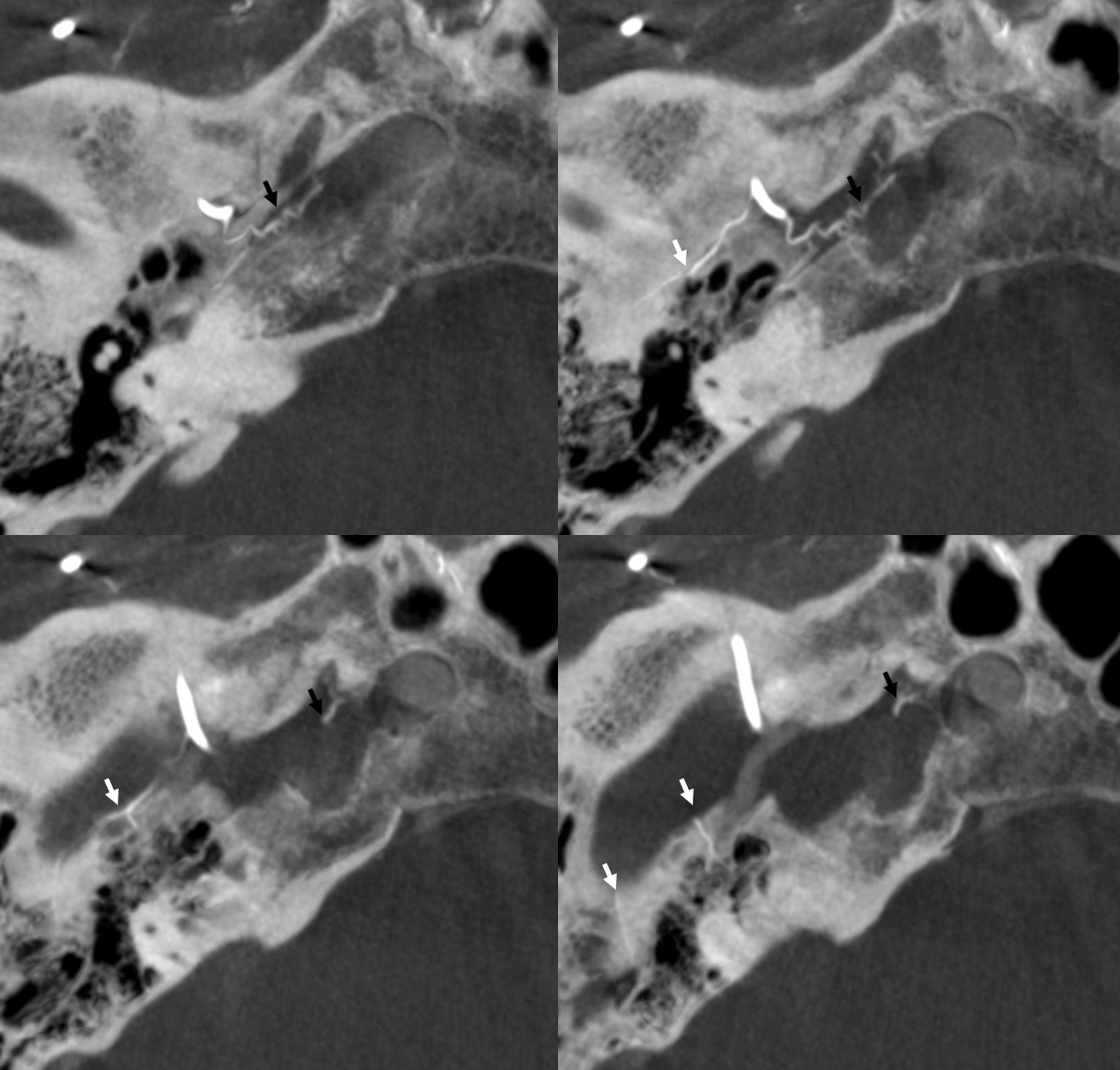
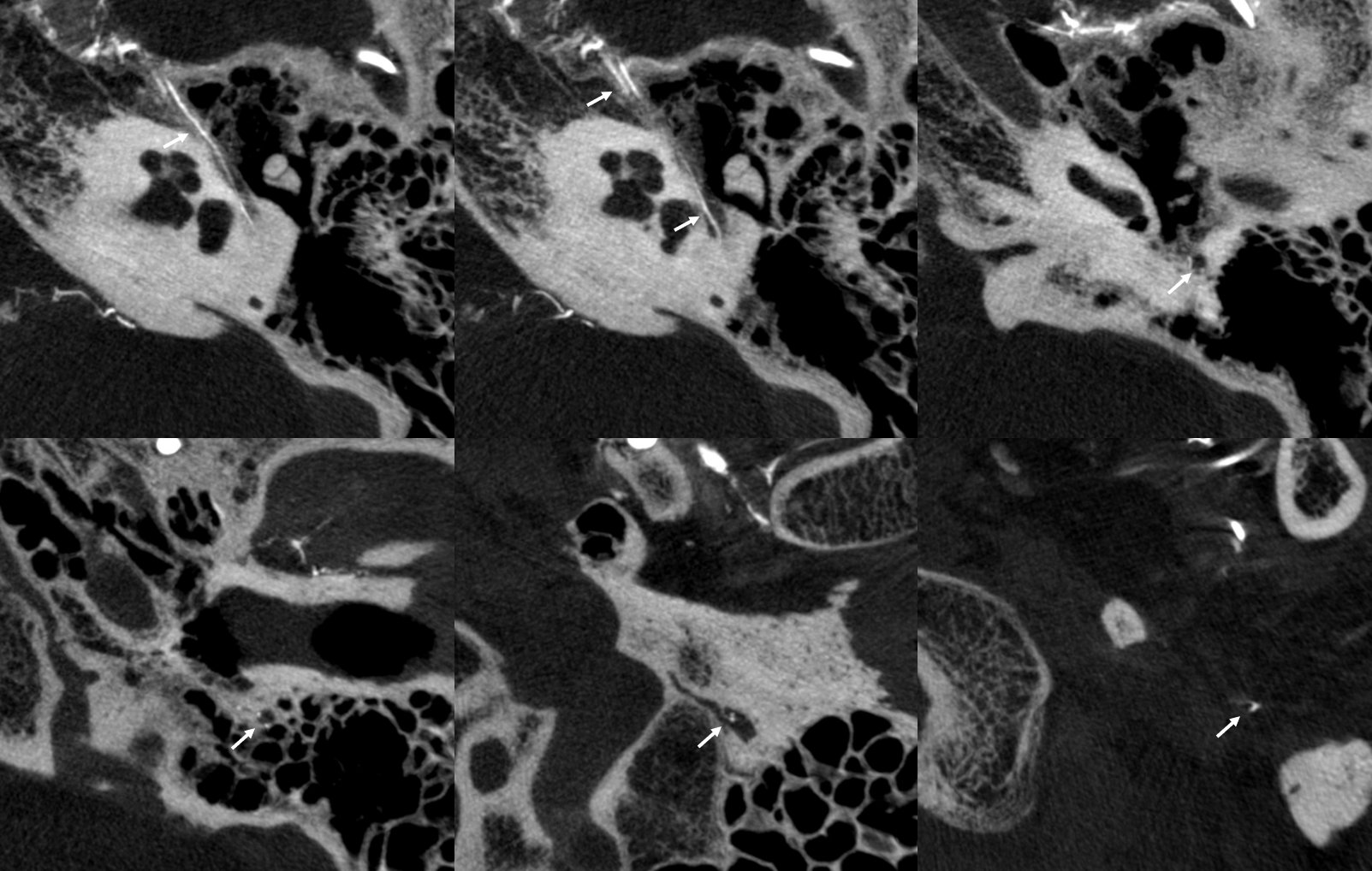
Facial Nerve Supply — Beautiful DYNA CT demonstration
Very prominent facial arcade — so much so there are two branches in the facial canal…
Axials
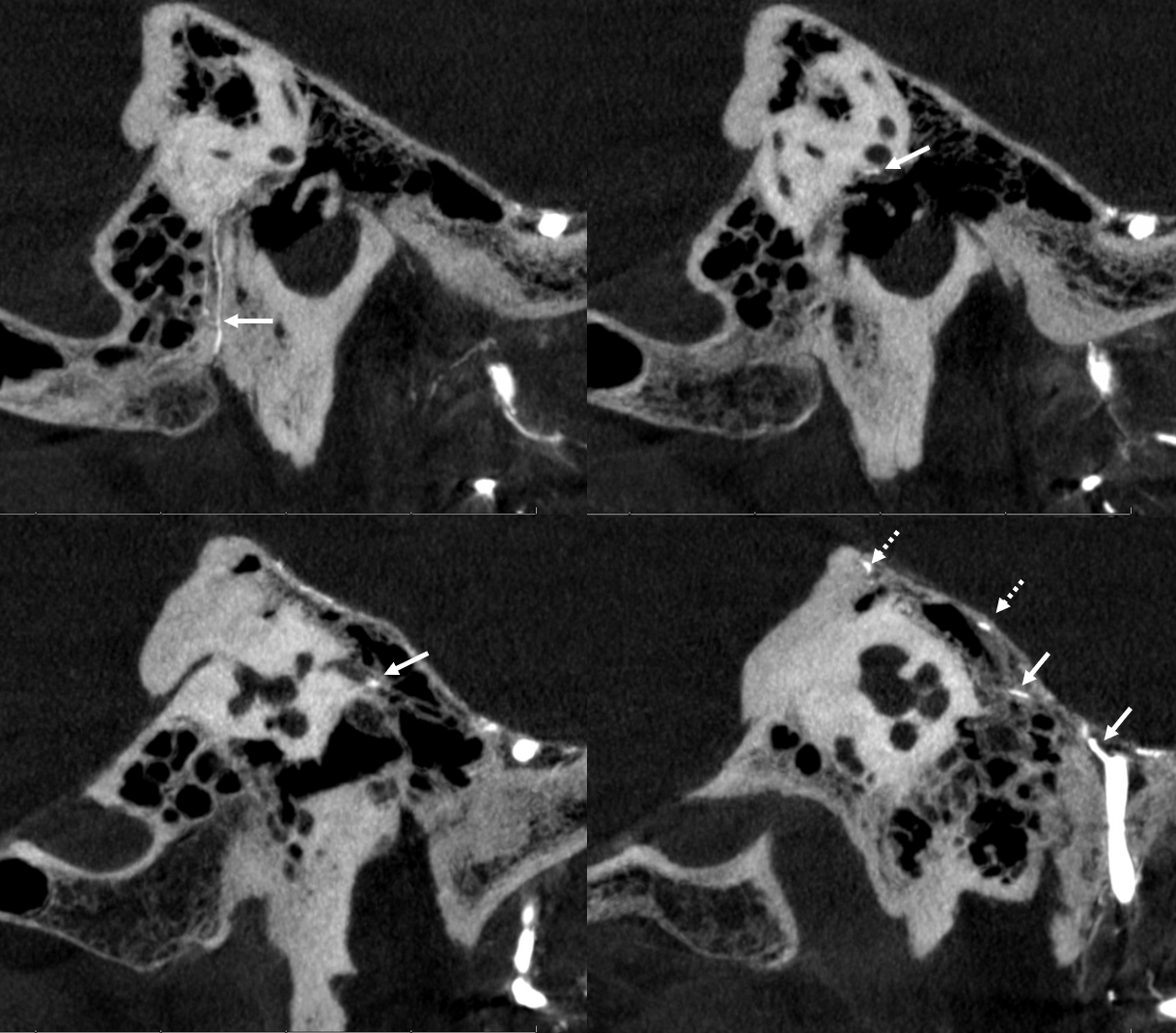
Sagittals
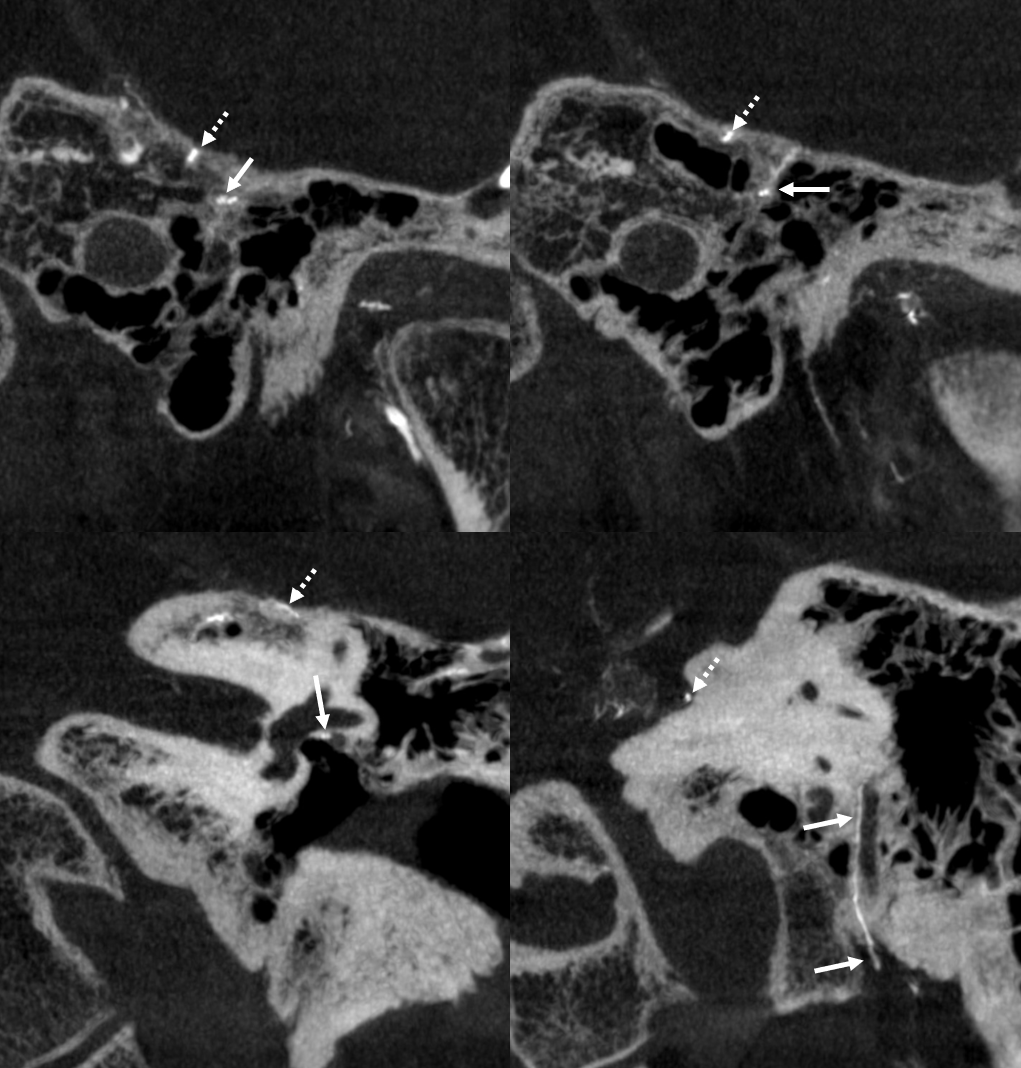
Coronals
Petrous Branch — facial and petrosal nerve supply. Be careful.
It is simple — proximal MMA embo, especially with liquid embolics, risks facial/greater petrosal nerve injury. Embryology tells you that there is always going to be a petrous branch of the MMA . It is a remnant of the ultra-early hyostapedial system. Petrosal branch is part of the “facial nerve arcade” (together with the occipital or posterior auricular artery), and supplies not only facial but also (more proximally) the greater superficial petrosal nerve. Don’t mess with them. Because of petrosal branch, embolization from proximal middle meningeal position carries risk of aforementioned nerve injury. Particles are unlikely to penetrate and disable the nerves if petrosal branch is very small (and usually it has anastomoses). But liquid embolics will penetrate… Like this:
Patient presents with posterior cavernous dural fistula. Supply is from left ascending pharyngeal and left MHT
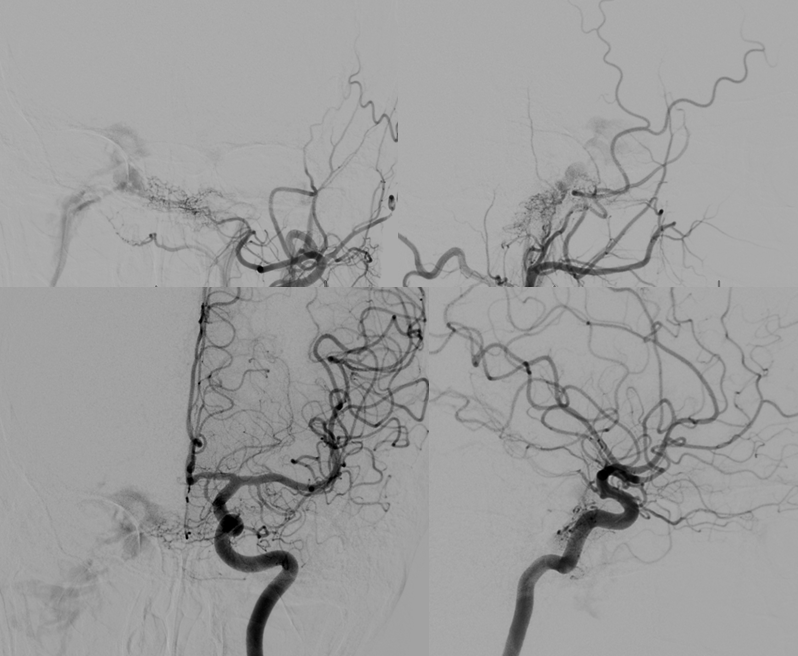
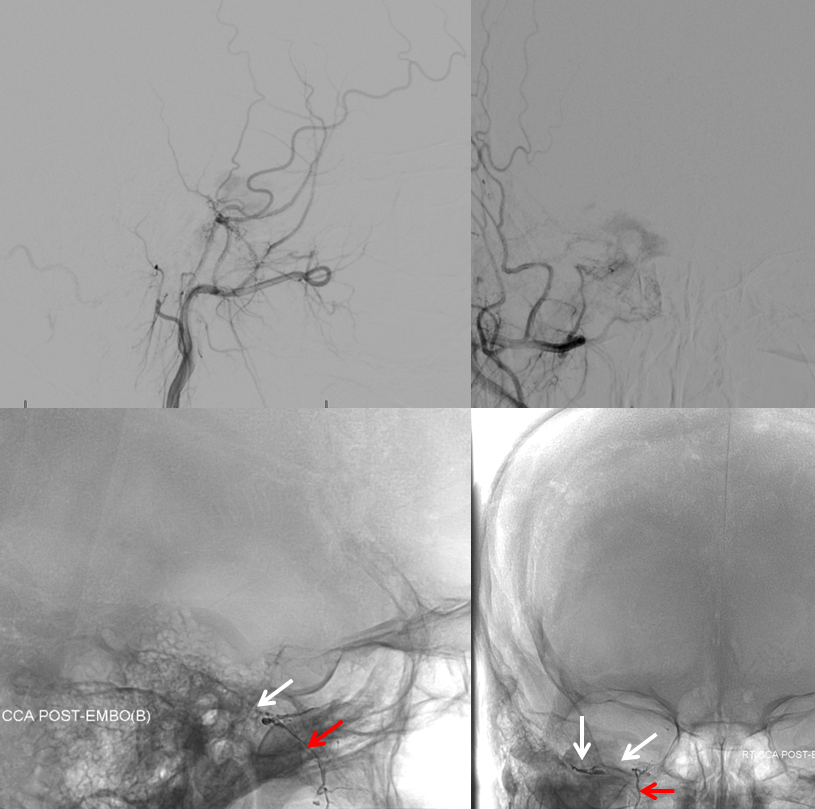
For some reason, embolization from right proximal MMA is attempted using Onyx. Top row is pre-embo. Bottom row shows Onyx in the proximal MMA, refluxing into the accessory meningeal artery (red) and petrosal branch (white). The patient developed an isolated greater petrosal nerve syndrome (taste aberration, lack of tears, and lack of nasal secretion production on the right. CNVII remained intact likely because of Onyx did not go posterior enough. All symptoms resolved in 3 months)
Another example — cavernous dural fistula (purple) presenting with vision loss in left eye. Even though fistula is small, both superior and inferior ophthalmic veins have thrombosed, leading to marked ocular venous hypertension. Full case is here. Supply is primarily via right MHT
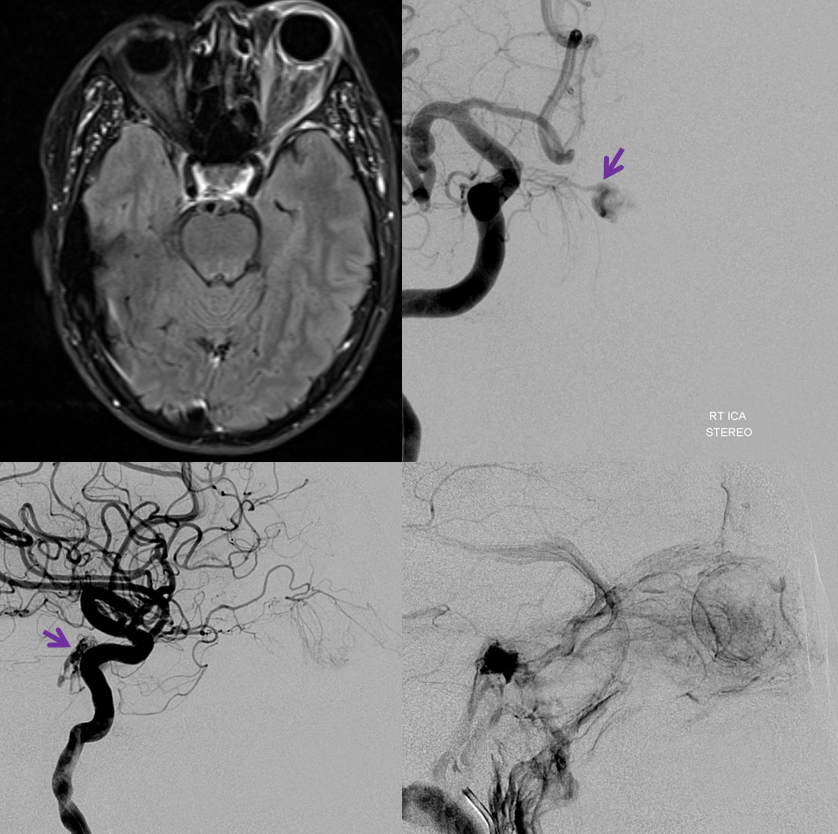
There is suggestion of supply from right ECA (below)

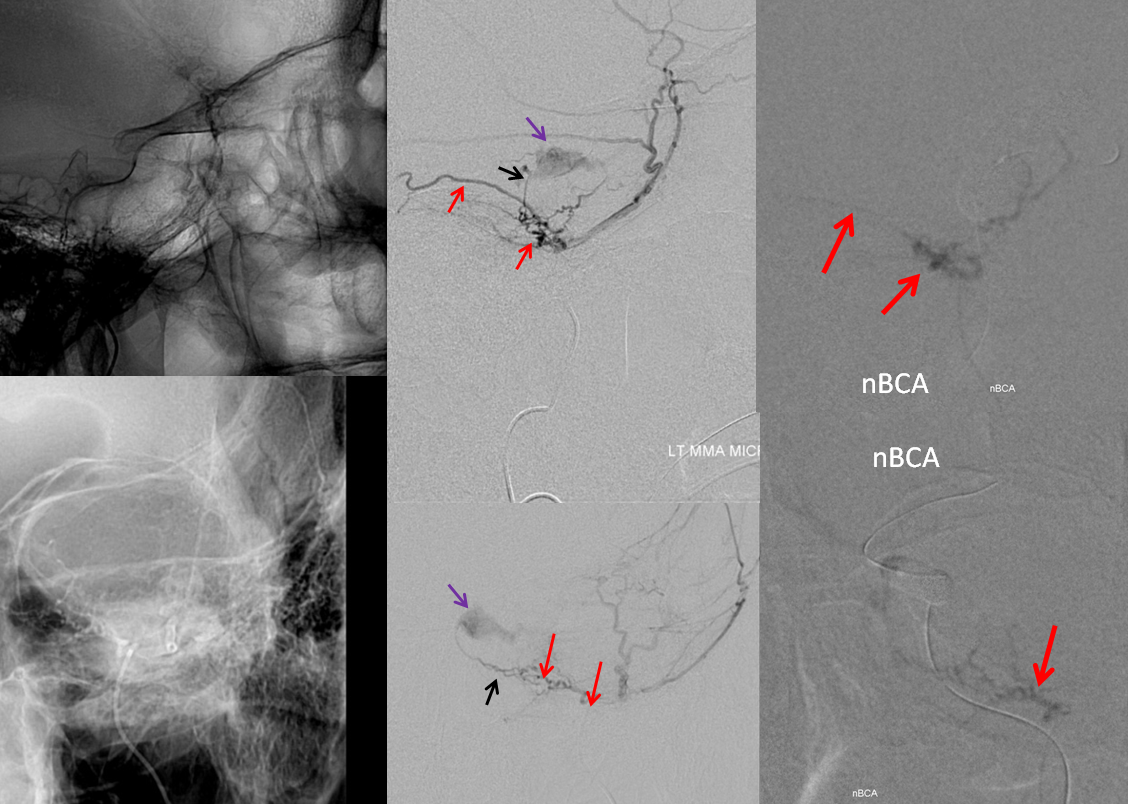
Catheter in proximal MMA position shows supply to fistula via small cavernous sinus branch of the MMA (black arrow). The Petrosal Branch is marked with red arrows. Images on right show nBCA in the petrosal branch. The patient awoke with complete facial nerve paralysis, and made only partial recovery. The fistula was closed by nBCA embolization via the right MHT. See full case here
Conclusion — proximal MMA embolization, especially with liquids, is a treacherous undertaking
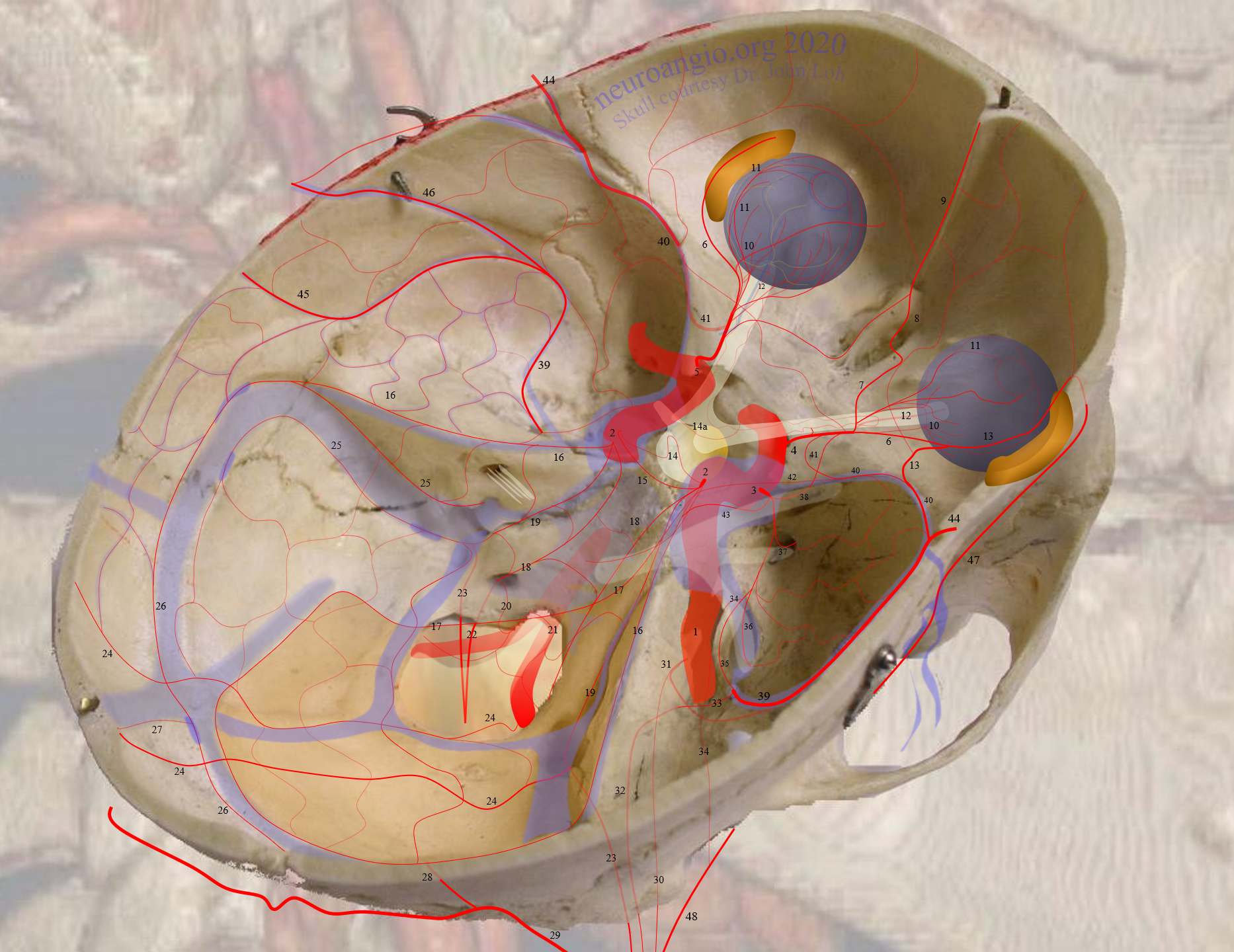
Meningioma Petrous Branch Supply
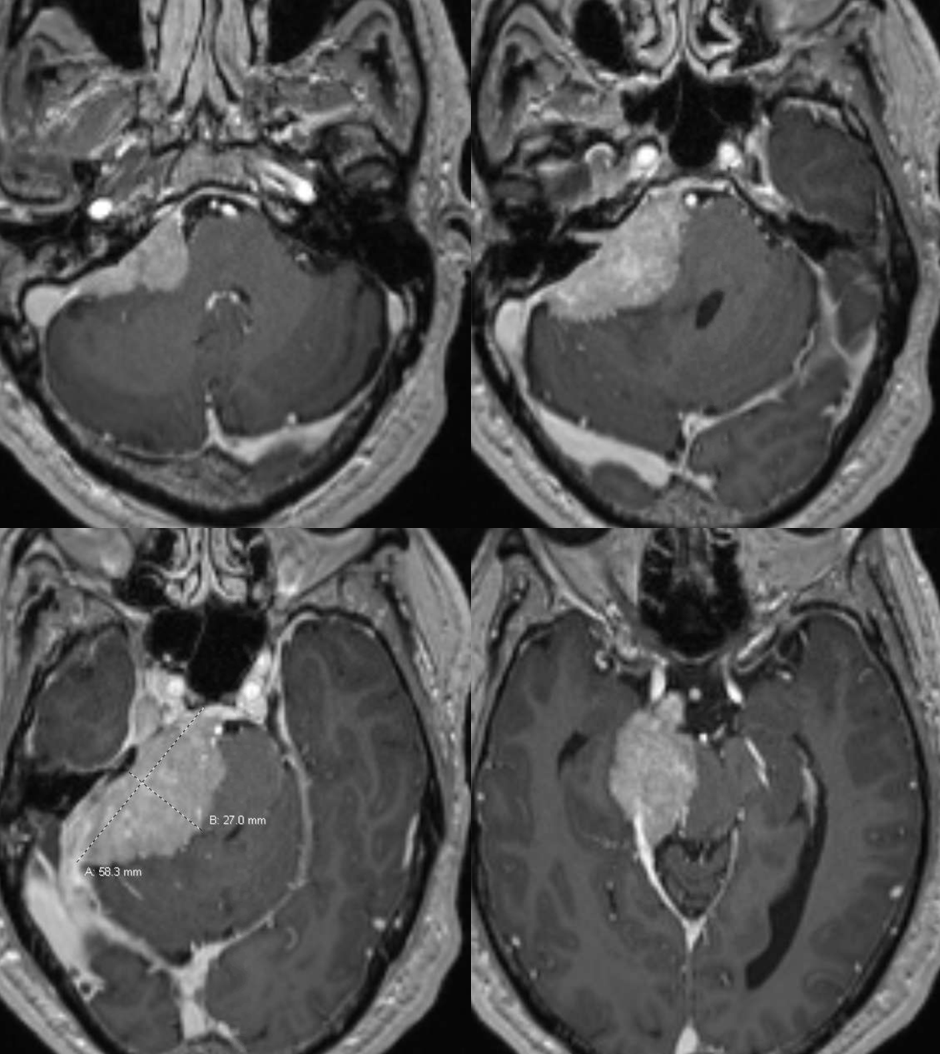
Petrous branch (33) supply – the branch is enlarged because of additional mening supply. Typical course.
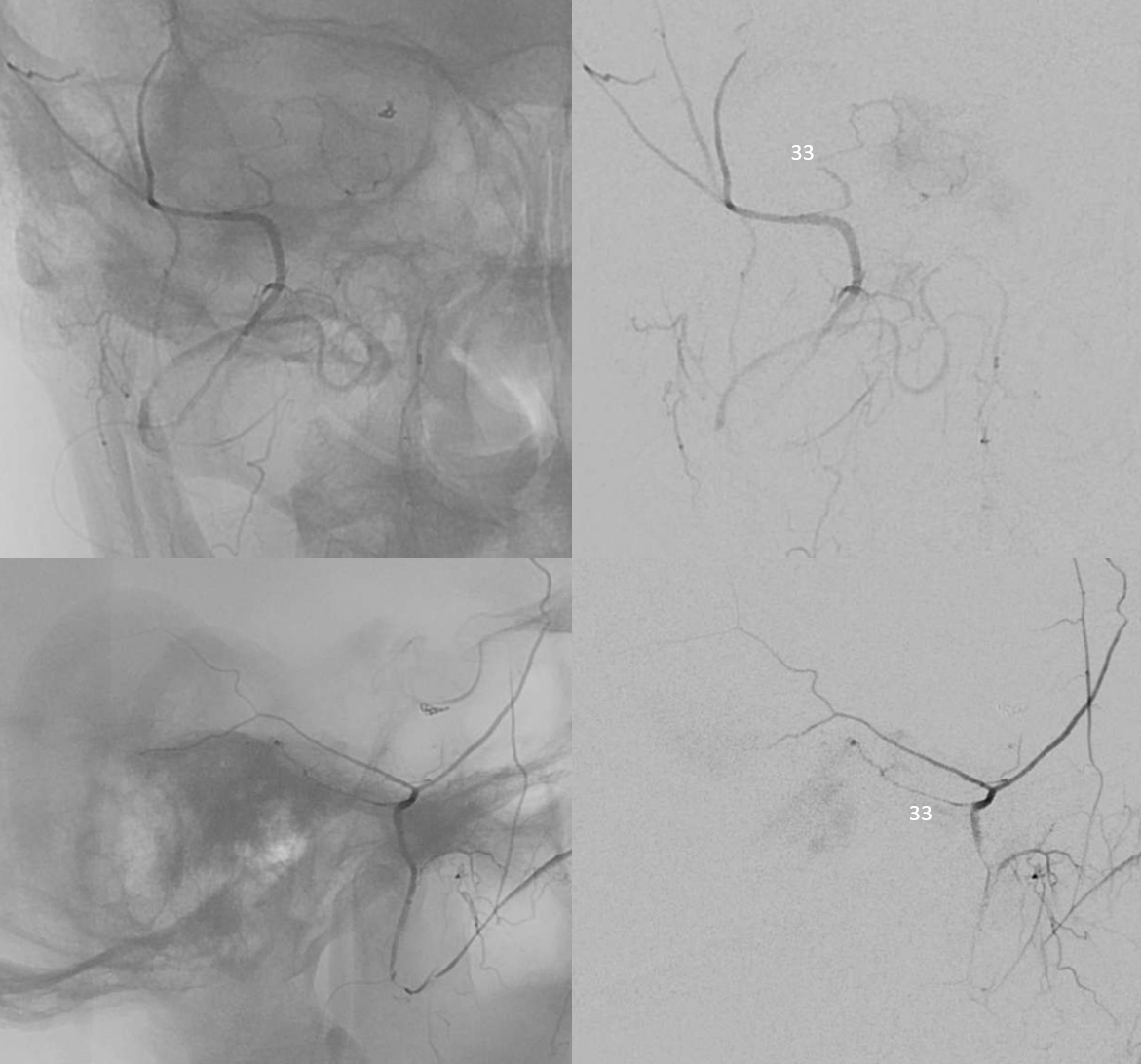
Additional supply from MHT, ILT, and jugular division arising from occipital artery
Cavernous Branch
Much less often discussed than petrous branch. Connects MMA with ILT— it is the same branch as the posterolateral branch of ILT. Can supply nerves of the Meckel cave and cavernous sinus. Another reason not to embolize from a proximal MMA position. Here both cavernous (black arrows) and petrous (white arrow) branches are shown well