

If you eat cheese first, and bread later, is it still a sandwich?
The answer is no, it is not. Especially when its a s..t sandwich…
History is trauma
What about the left side?
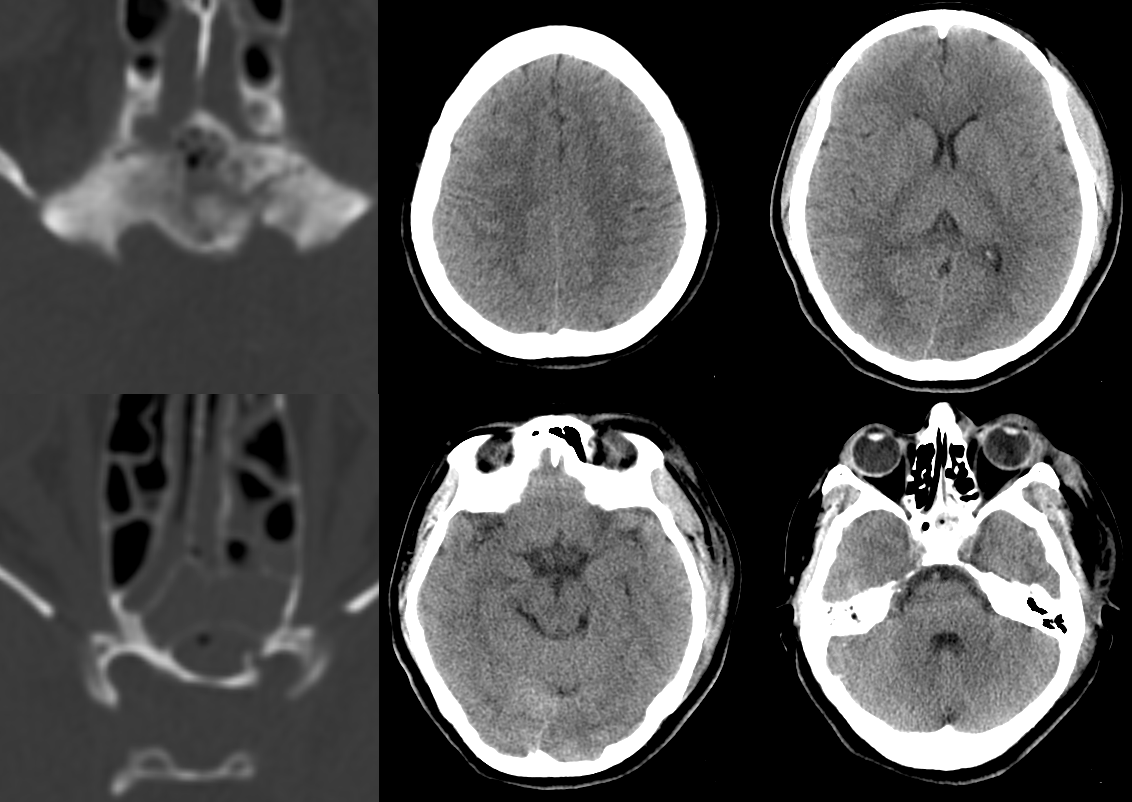
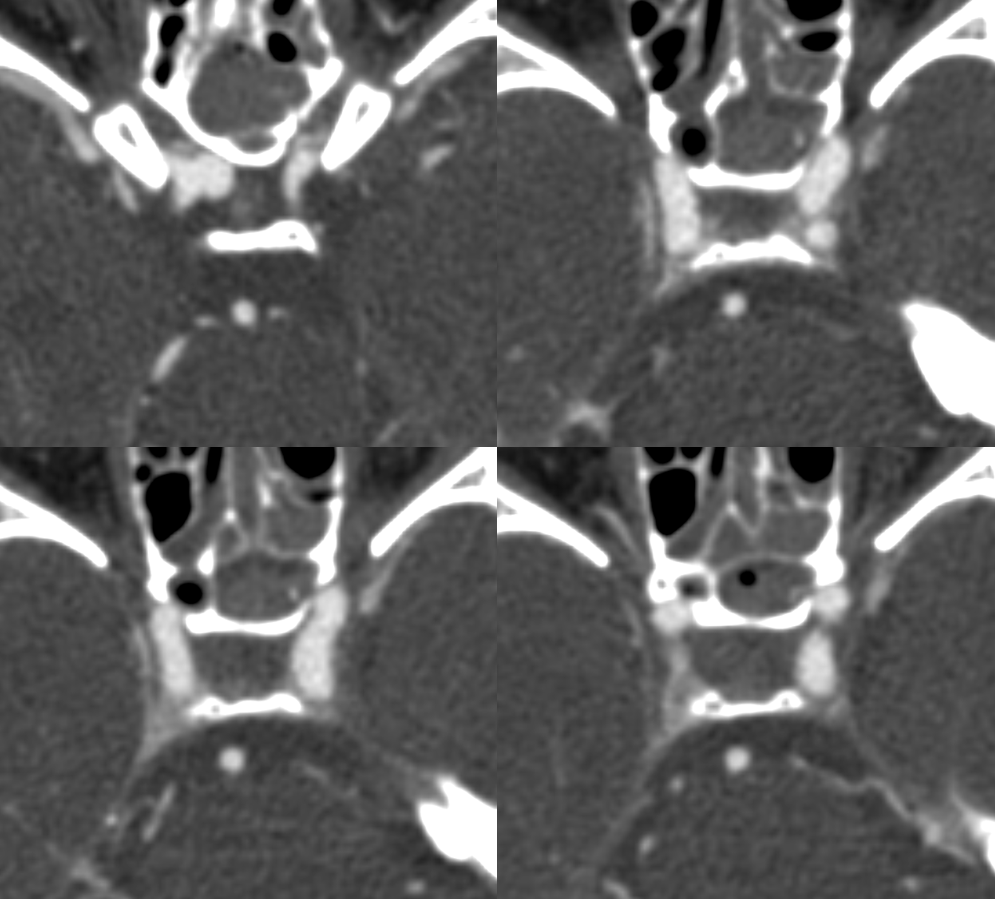
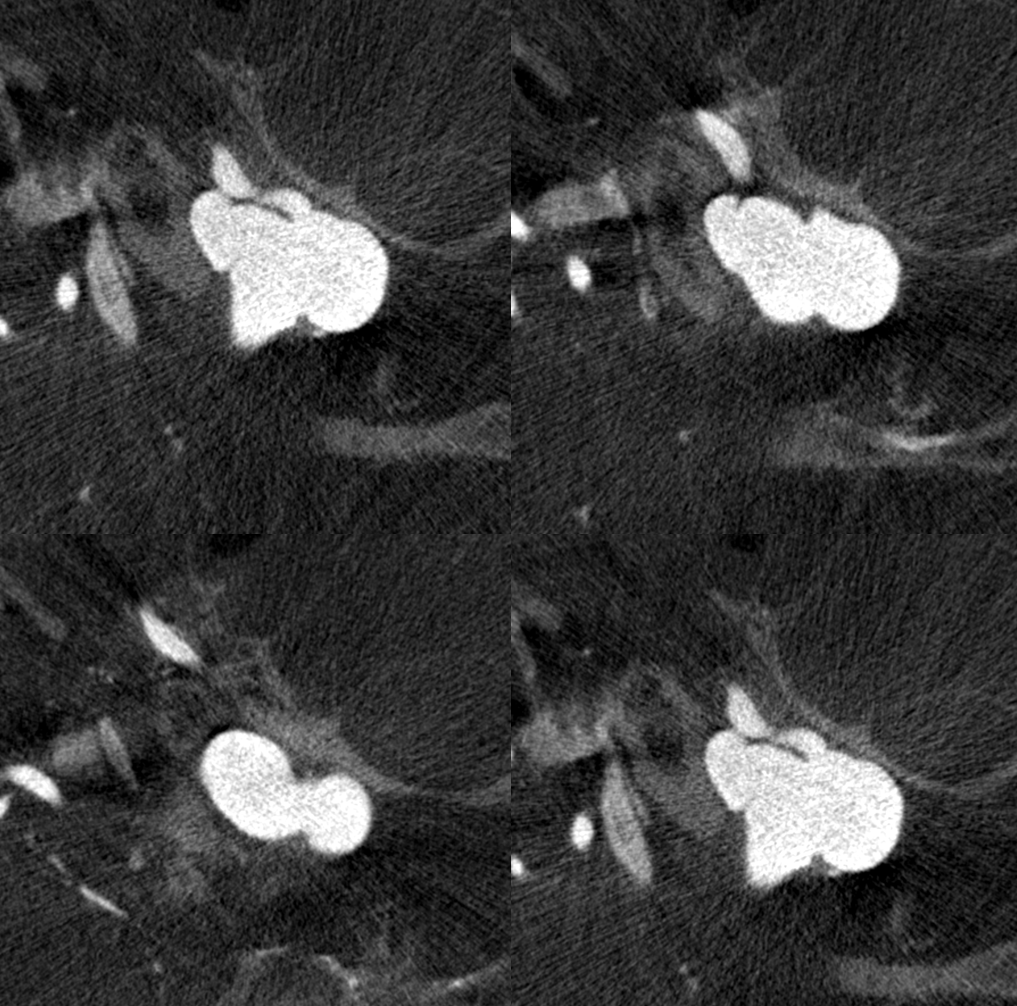
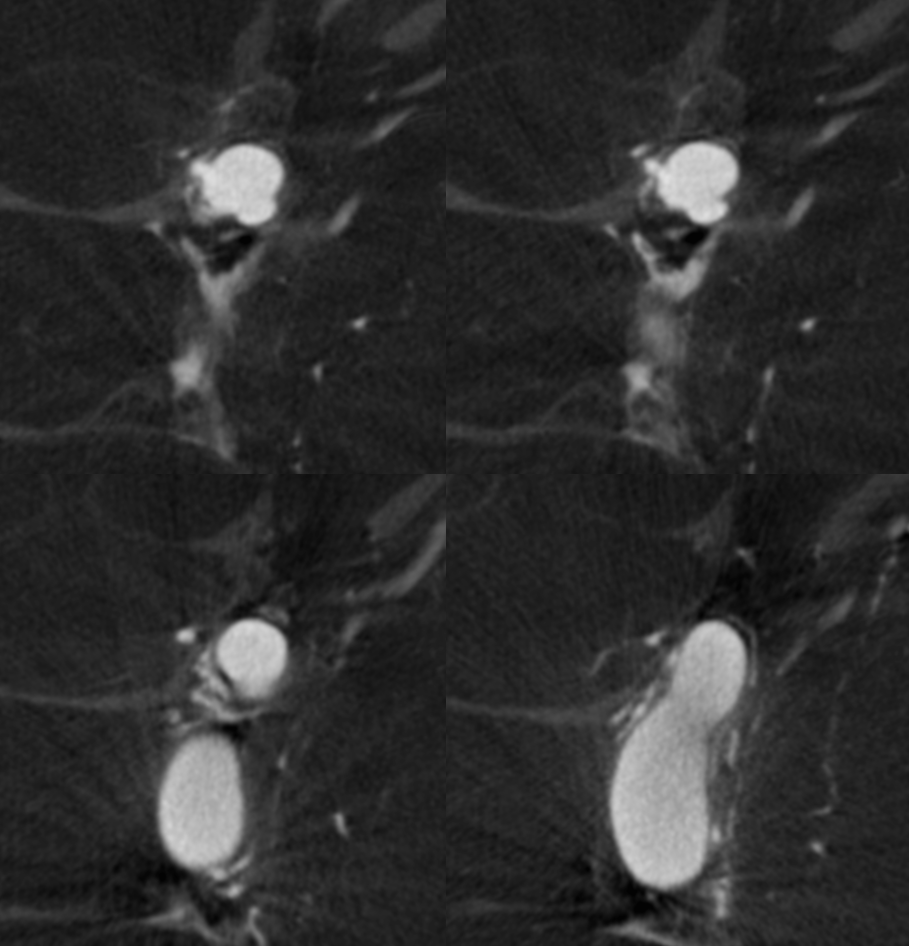
Big mistake avoided with high resolution cone beam CT

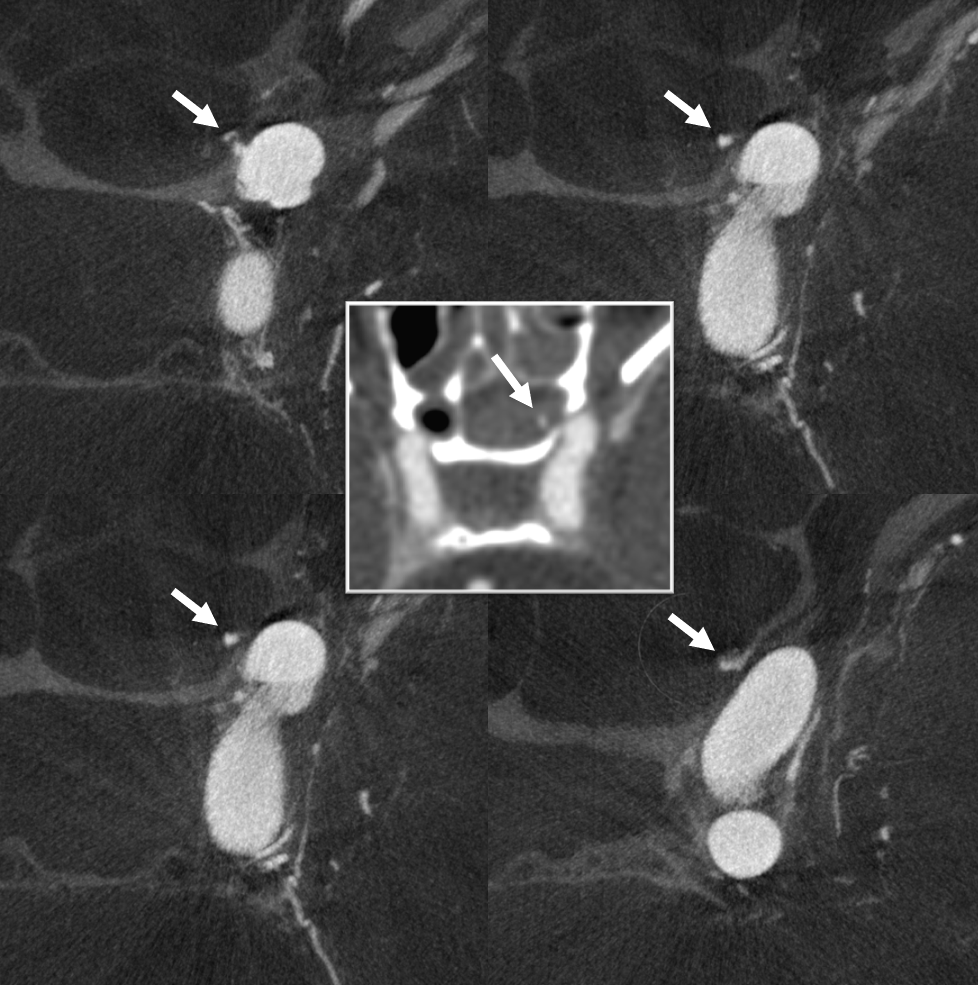
Looking at cross-sectional data is key. In retrospect, the injury is visible on CTA also (center inset)
Working left anterior oblique angle
Just before starting treatment, repeat imaging… Let’s say the situation is not exactly stable.
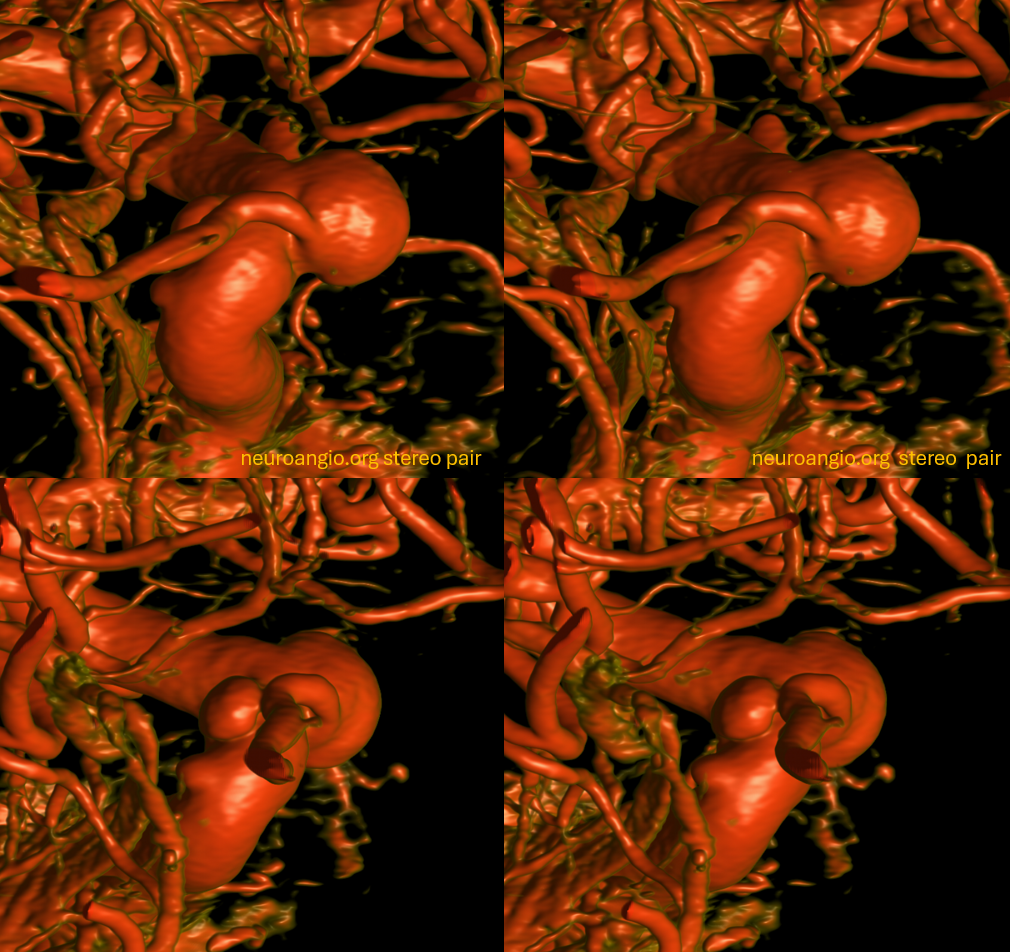
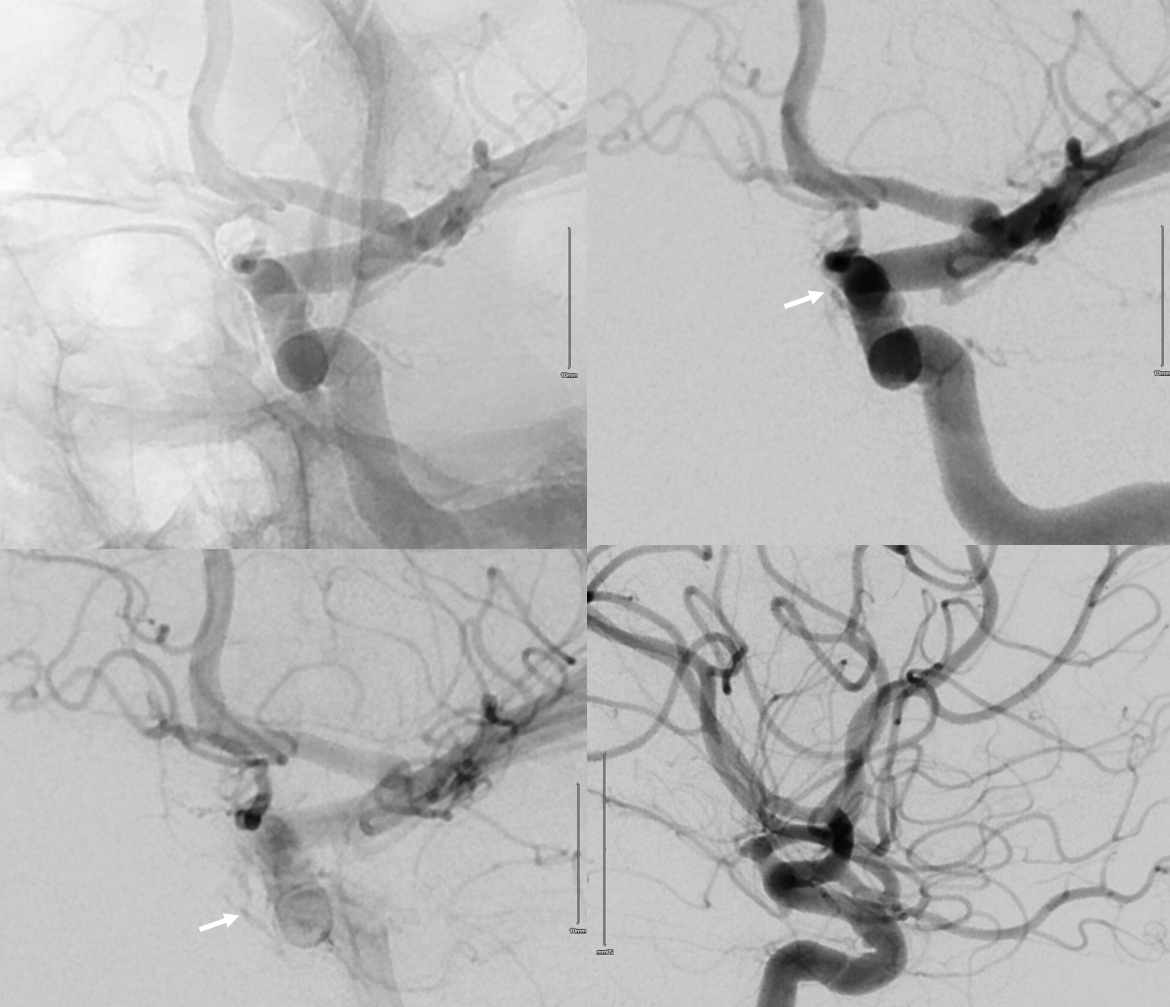
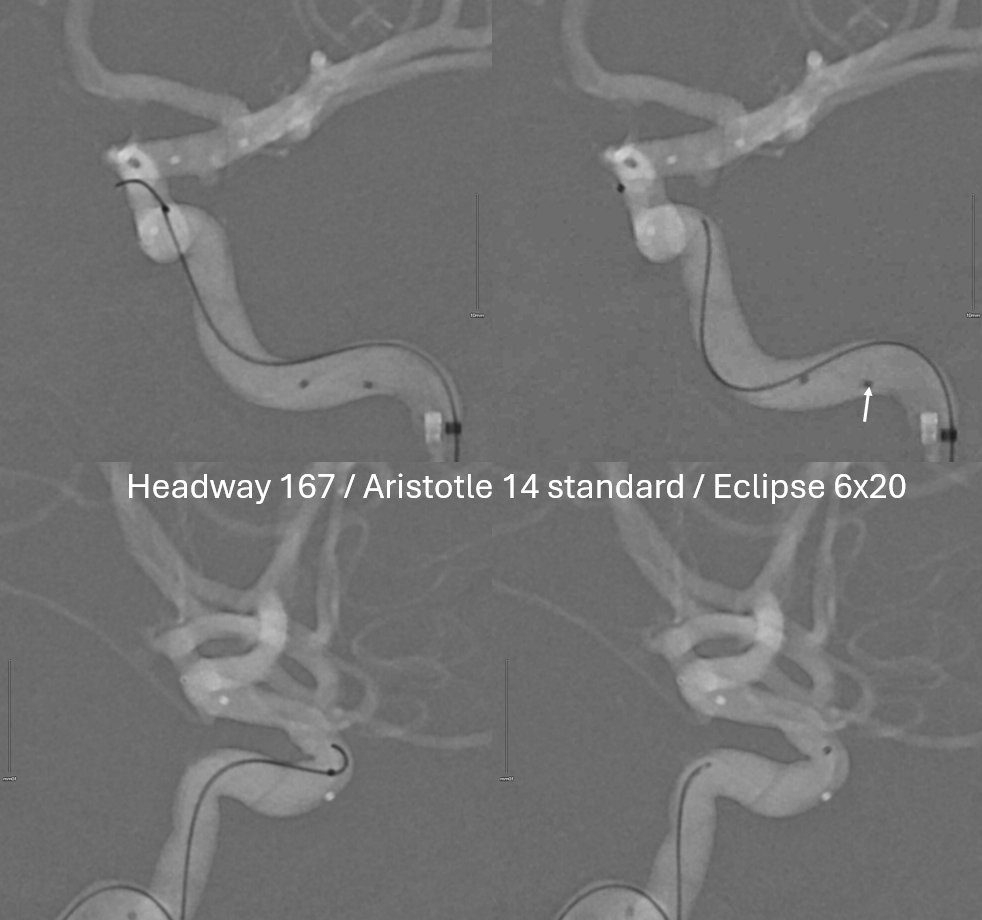
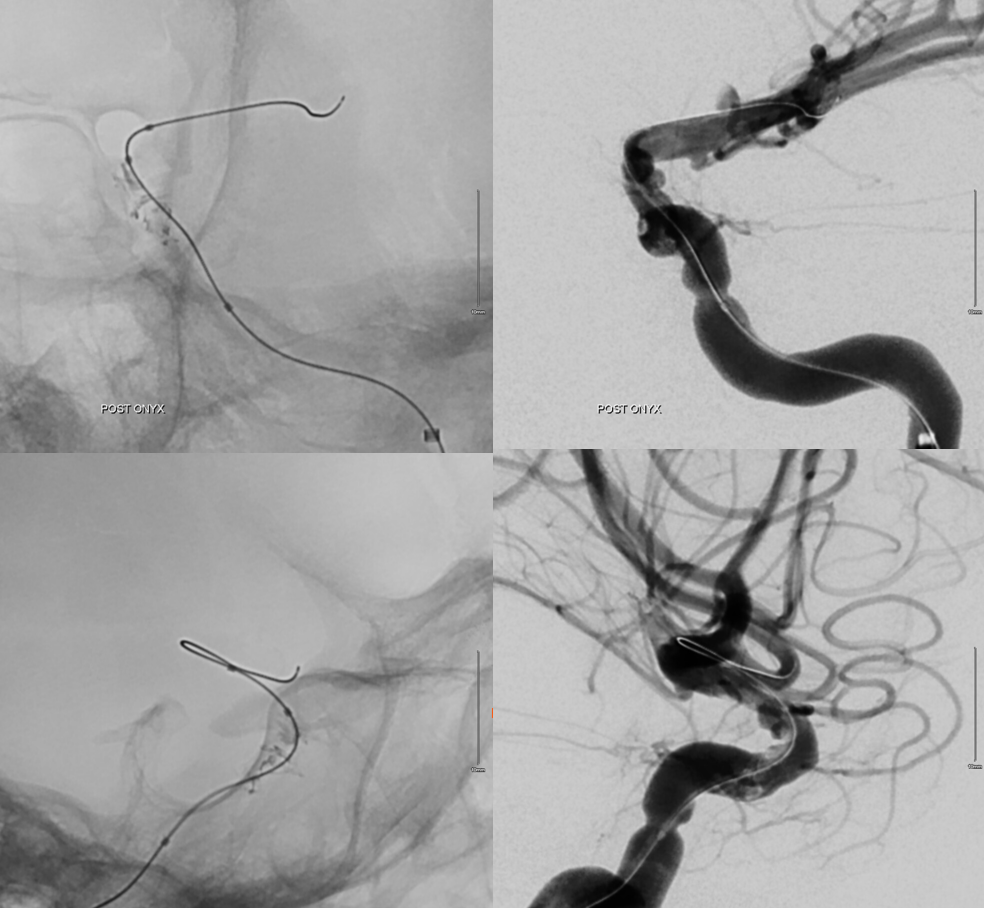
Now there is a hole into the sphenoid sinus (arrows) and a carotid cavernous fistula (dashed arrows). Repeated DYNA below.
The sphenoid sinus hole is more important. Eclipse balloon (arrow) interfered with catheterization and had to be moved below
Micro injection
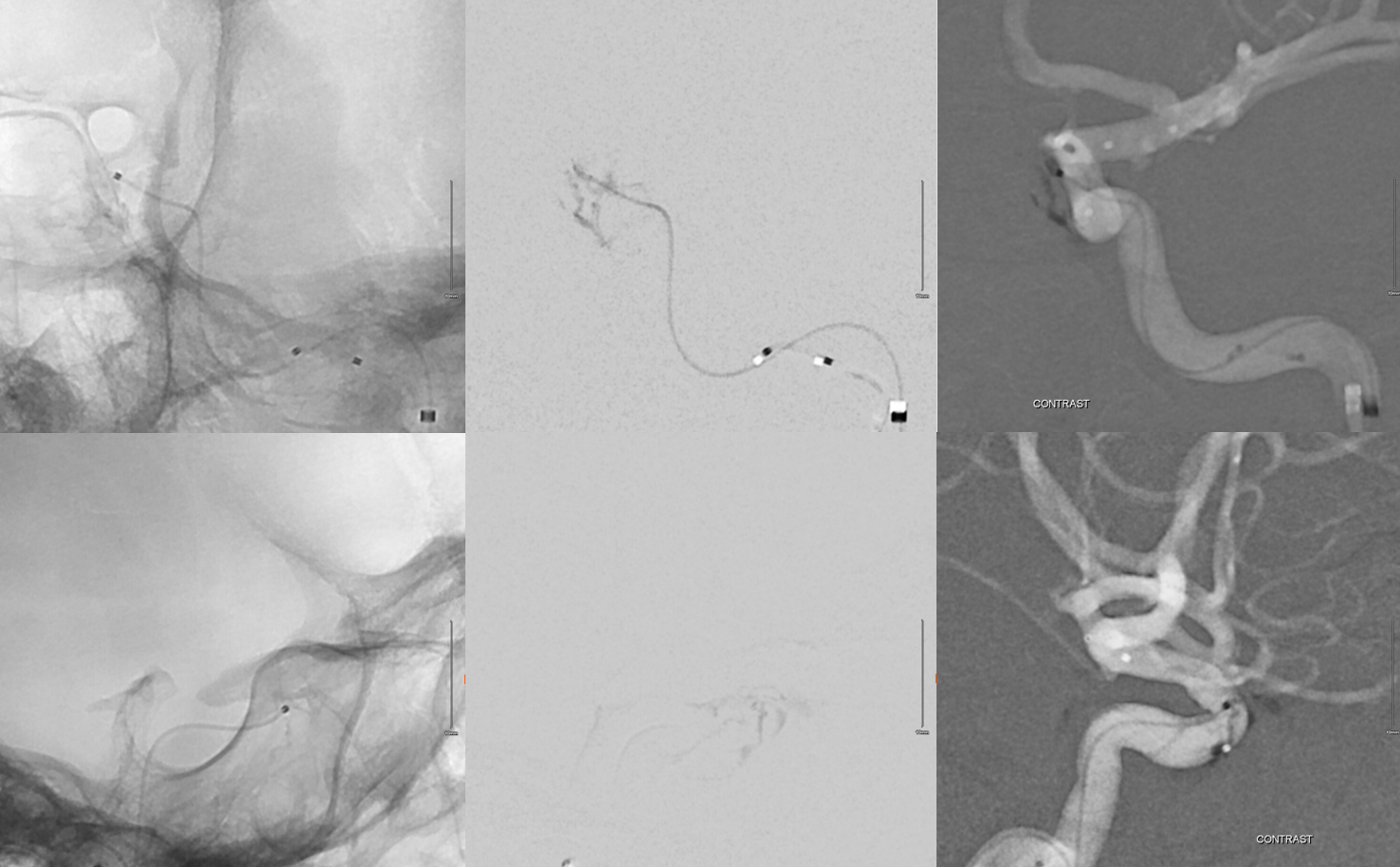
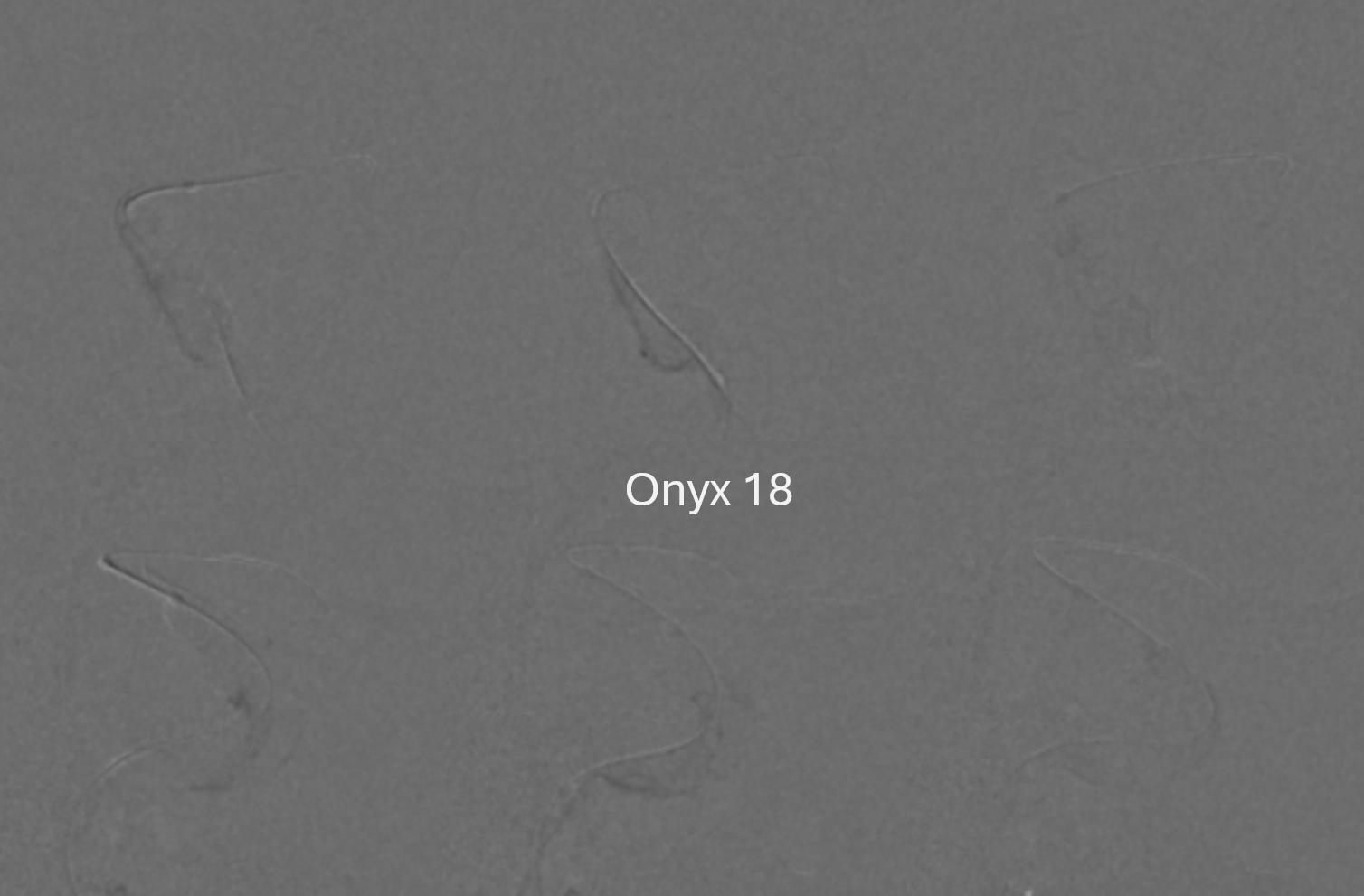
Glue or Onyx? Got good reasons for both. Went with Onyx 34. Clearly, some of it is in the carotid.
Interestingly, the Onyx stabilized the headway and allowed Eclipse to be brought up and inflated. More Onyx went mostly into the right areas — but some still went around the balloon inferiorly. Important to pull out headway with balloon inflated — rightmost images
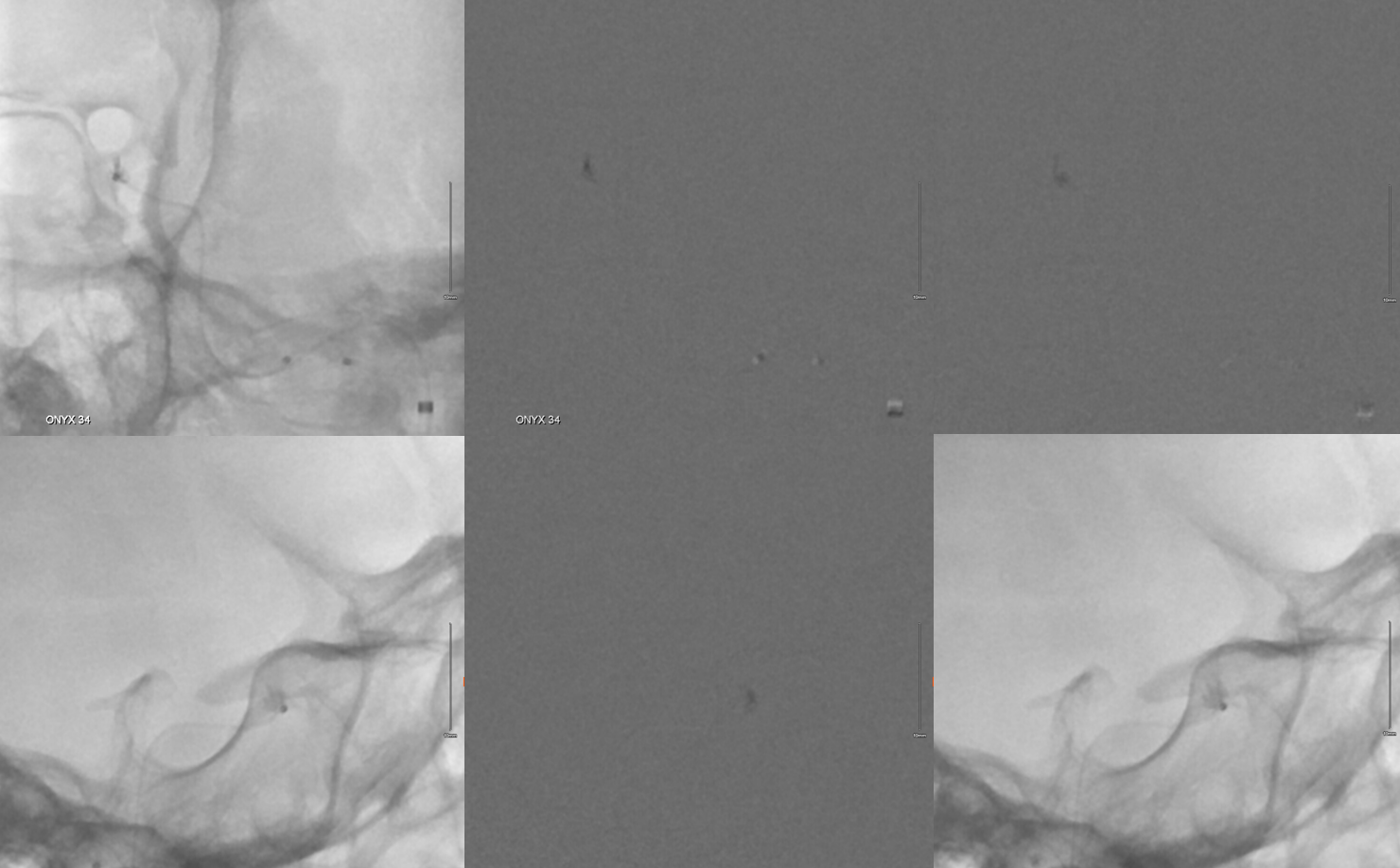
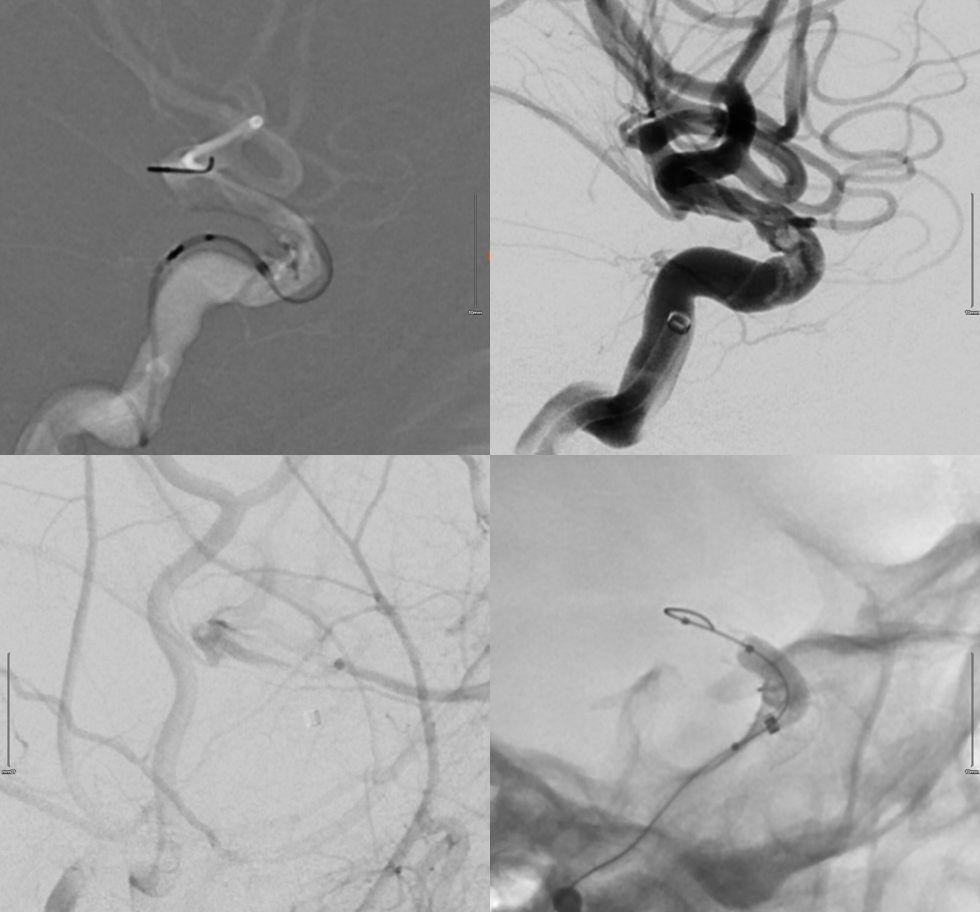
Not pretty… Clot already forming on the intravascular onyx. the ACA is backfilling through a small ACOM…
So, avoiding the stent was unavoidable… The cheese is eaten. Now must have bread also. Despite full heparin and integrilin load, the artery still almost closed. Who says Onyx is not thrombogenic — except during preop embo of a brain AVM 🙂
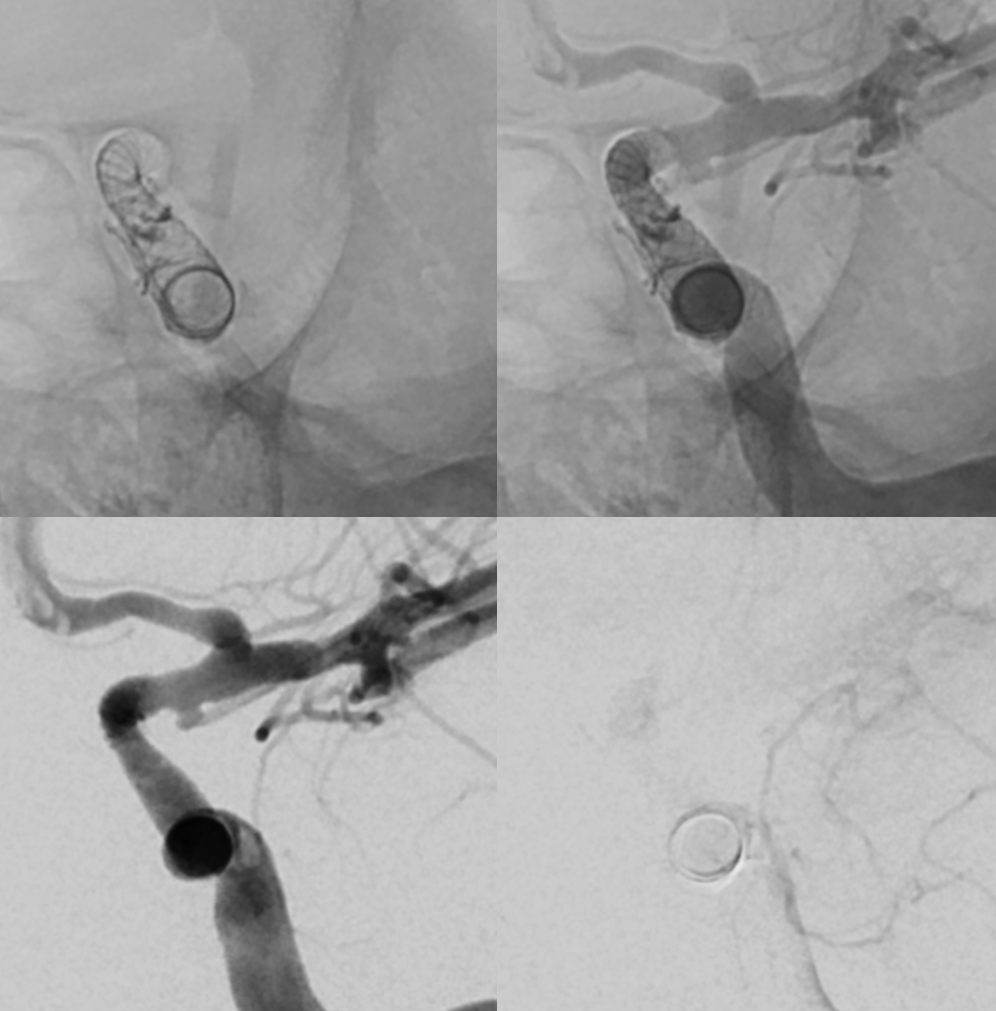
Things got a bit hectic here. First pipe (4.5×14, top left) did not want to open. After pulling it out, things seemed tolerable (top right). A few minutes later, the carotid almost closed (bottom left). A different Pipe (4.25×12) did better, followed by Scepter 4×10 balloon (bottom right). It was some work to open these pipes.
All well so far
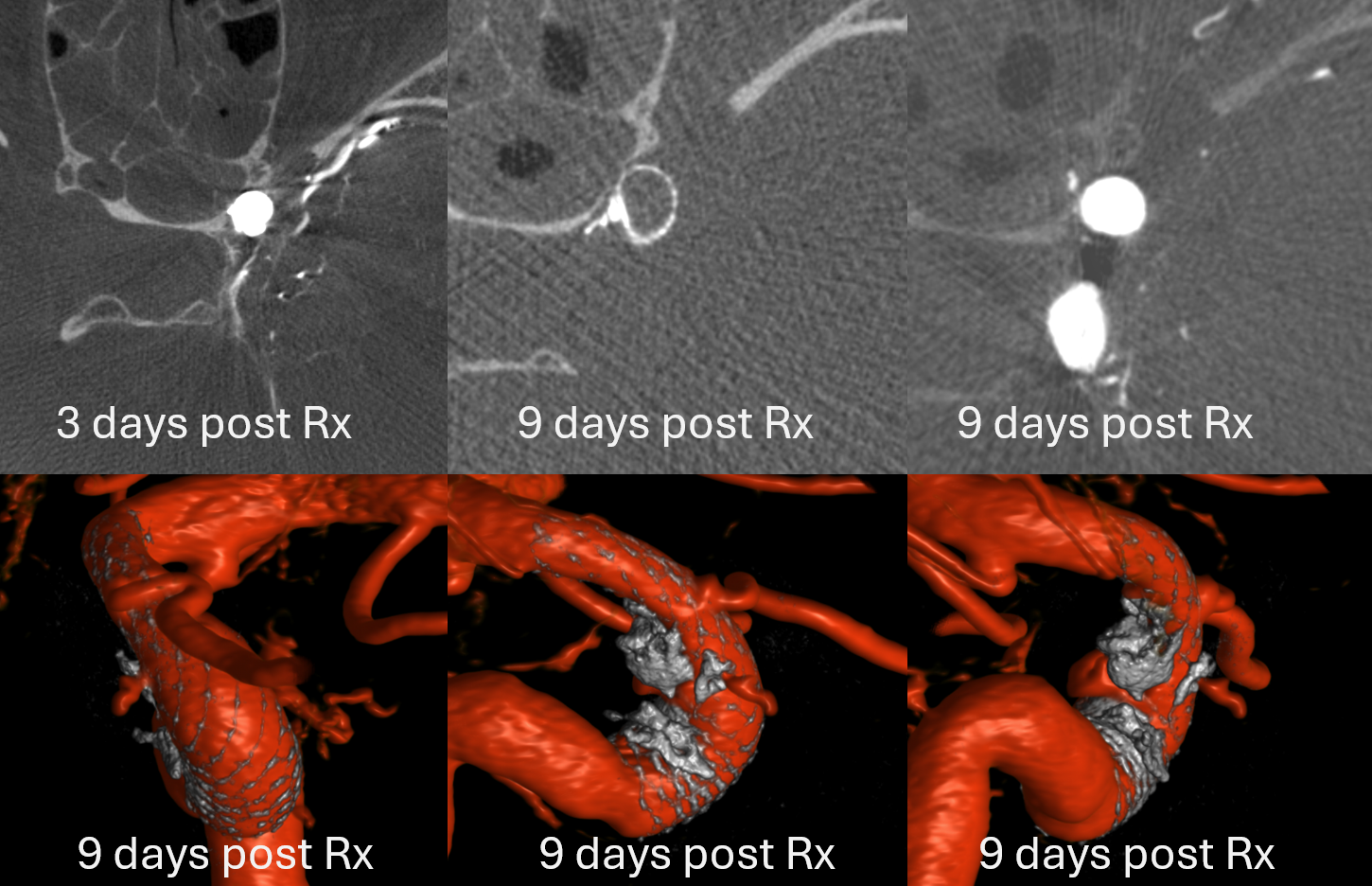
See that small dot in bottom row images — thats the residual tiny hole. Good news is that Onyx also closed the cavernous fistula. Hopefully.
Question — what about the right side?
WELL, THIS IS NOT THE ENDO OF STORY!
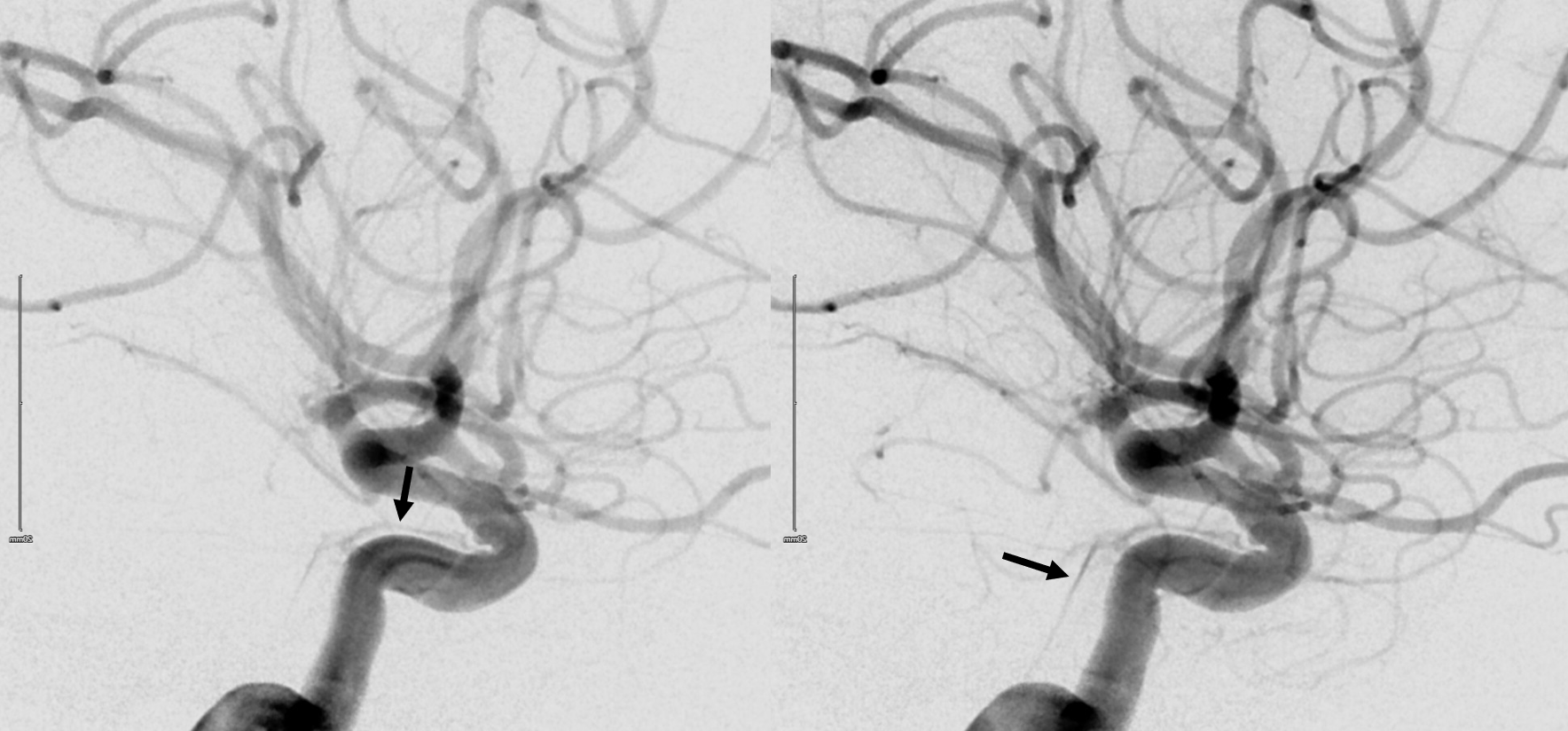
2D-DSA

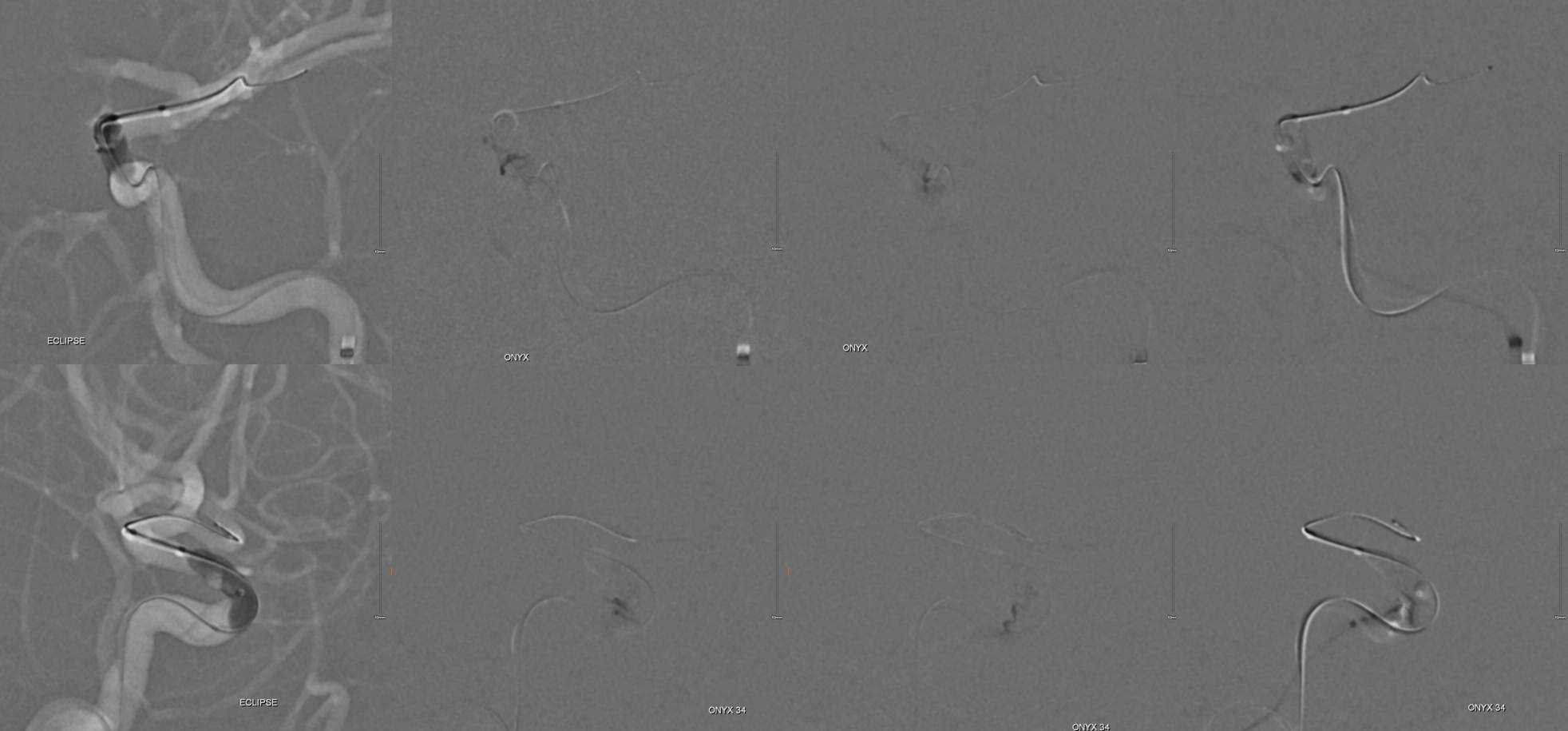
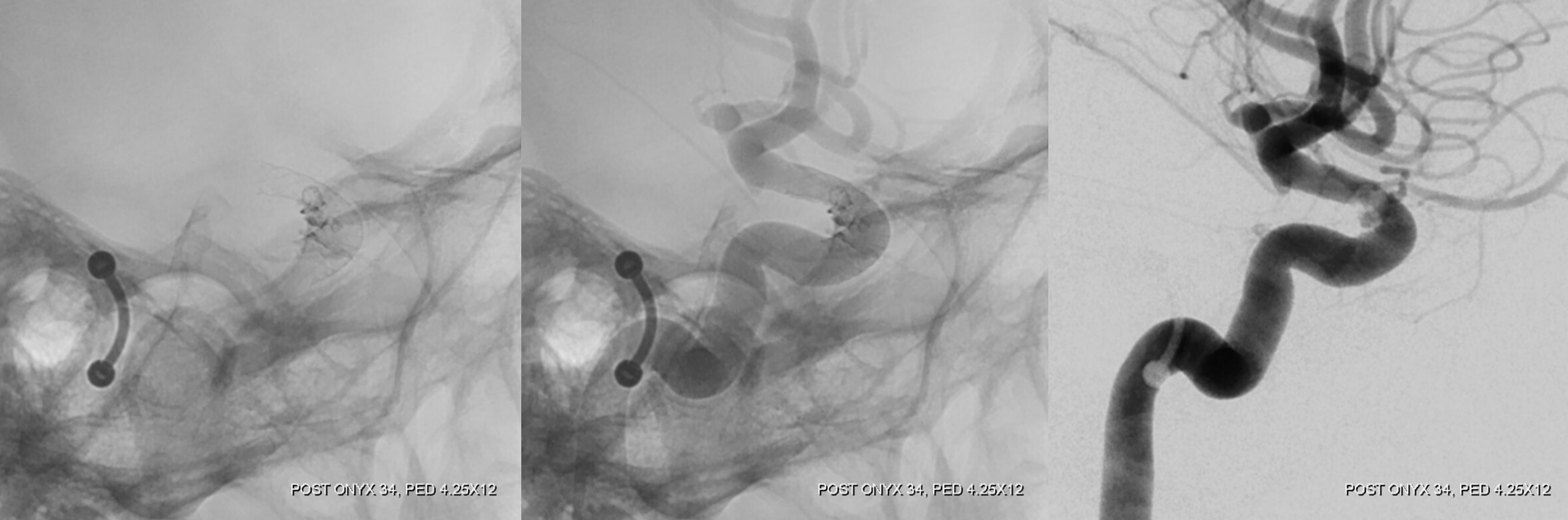
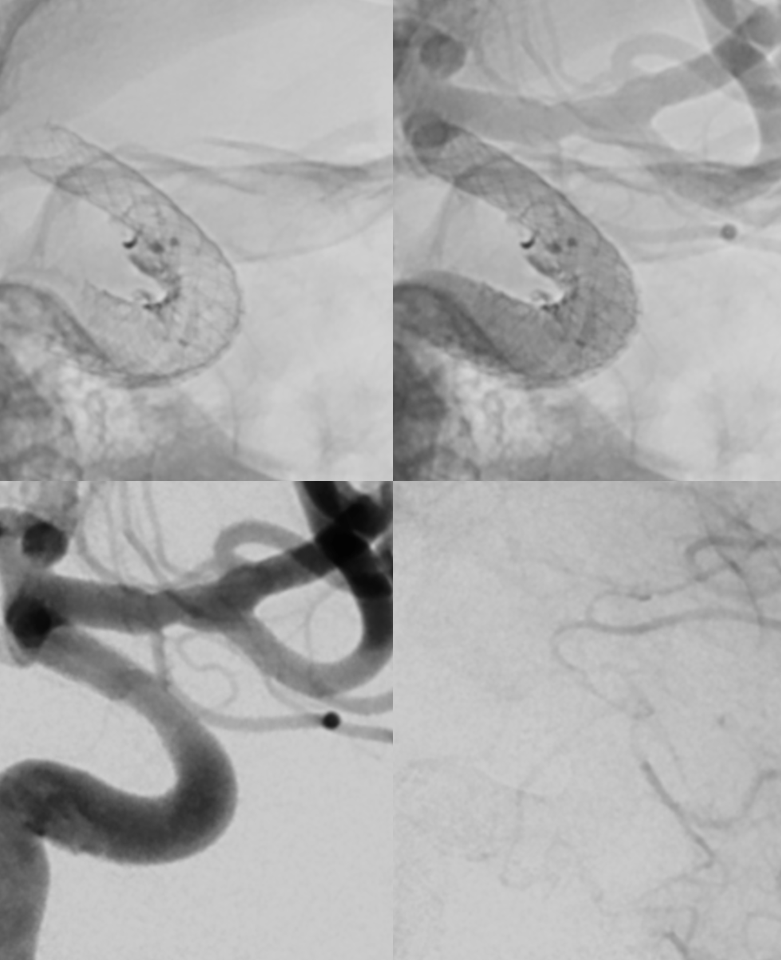
More sandwich… Headway Duo with Aristotle inside trapped against another Pipeline. It is critical that the tip of headway be as close to the hole as possible or it will not work. This only works because of the small space between the vessel wall, the hole, and the pipeline created by the microcatheter.
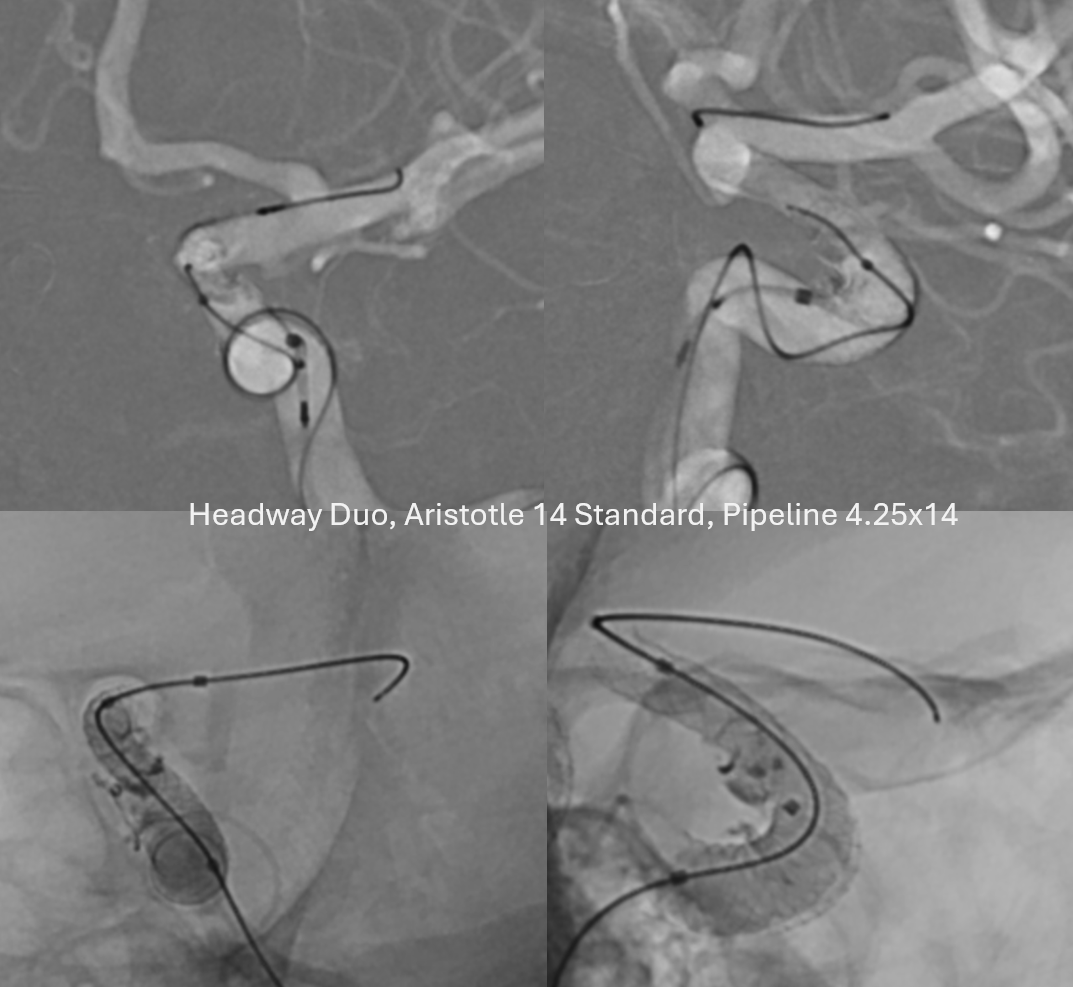
Test injection of the microcatheter is critical. The onyx will go wherever, and quickly, but if test contrast injection looks bad then its bad.

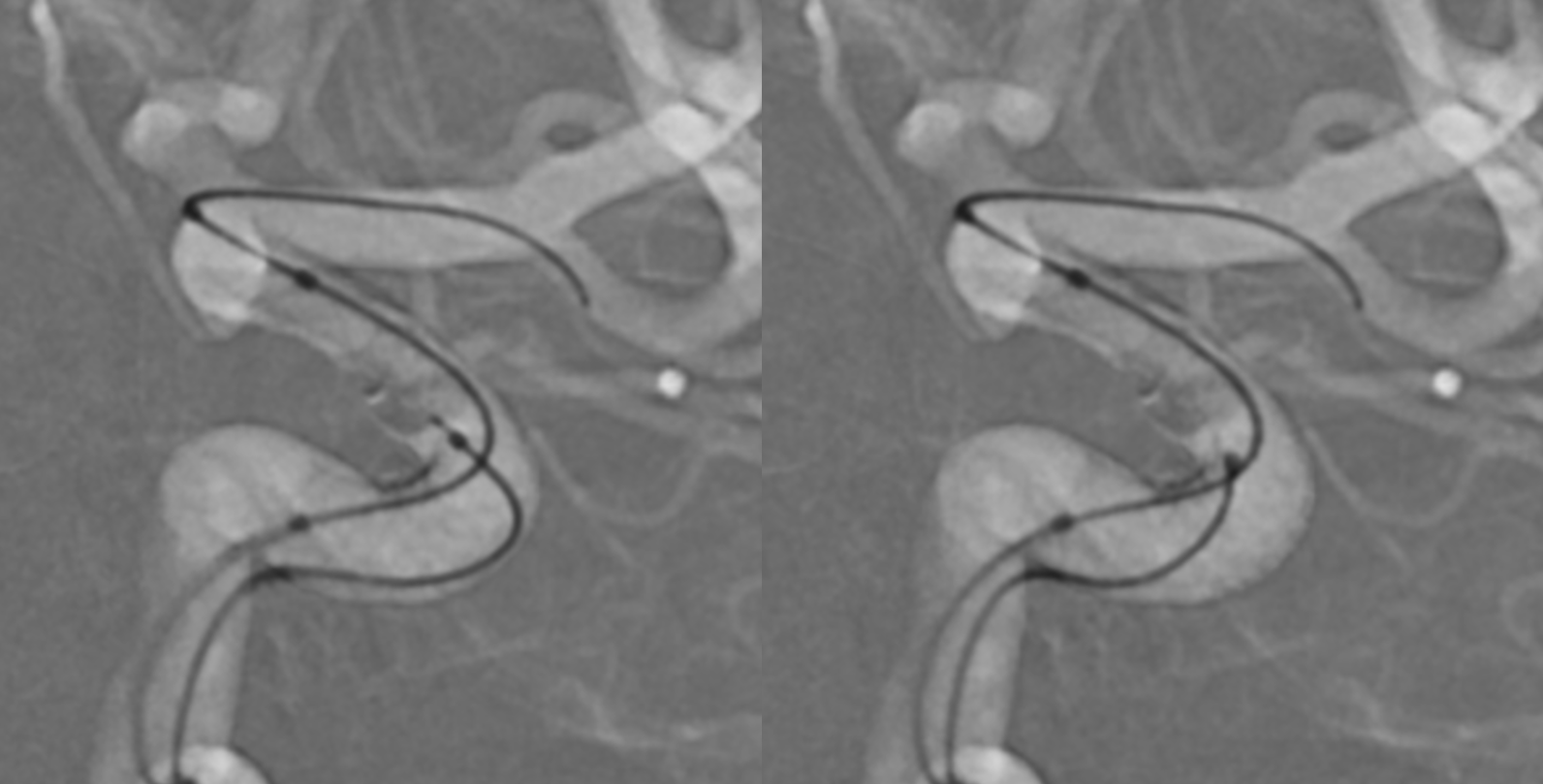
Pulling back the headway (wire re-introduced) is better
Onyx injection. We did not save the contrast injection before onyx and after repositioning unfortunately. it was opacifying the horizontal cavernous sinus — always there will be a leak around the balloon
Post drop another Pipe to be sure

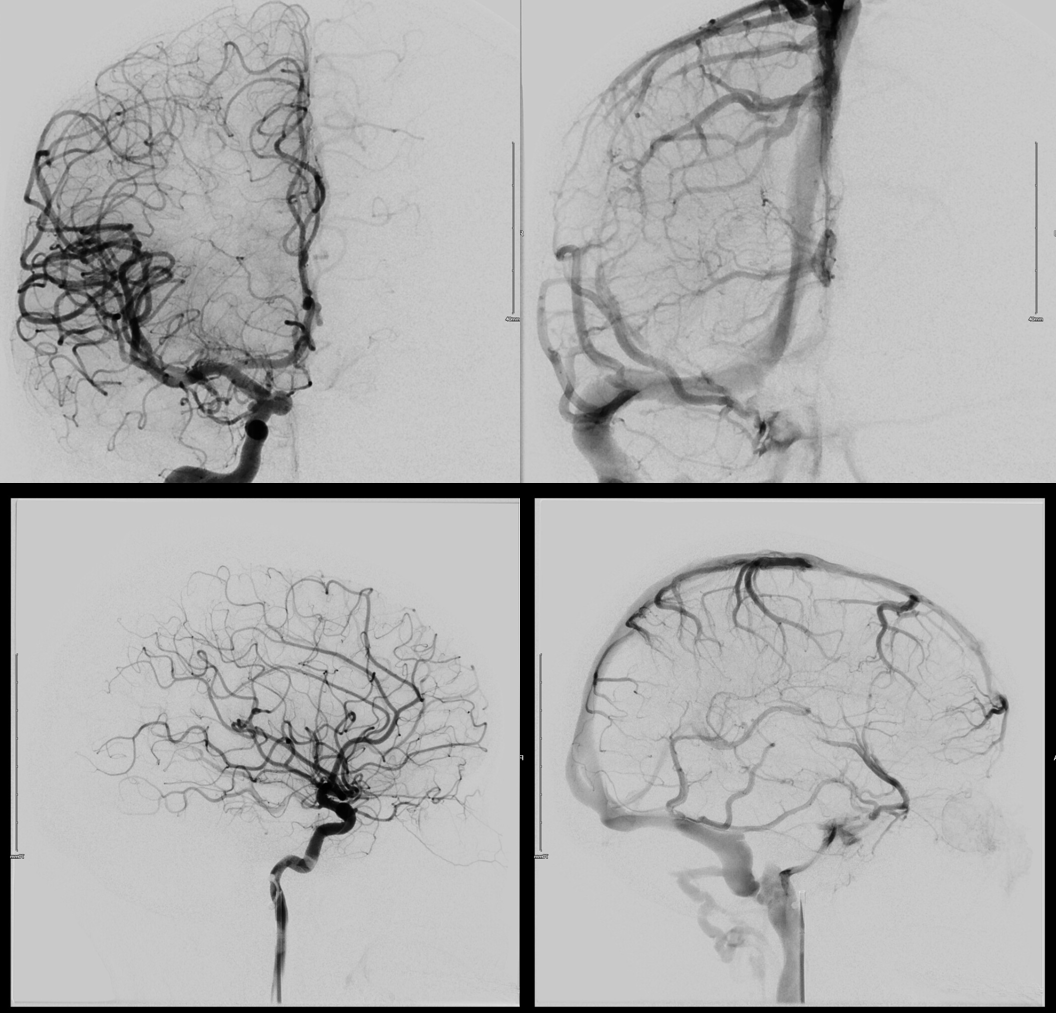
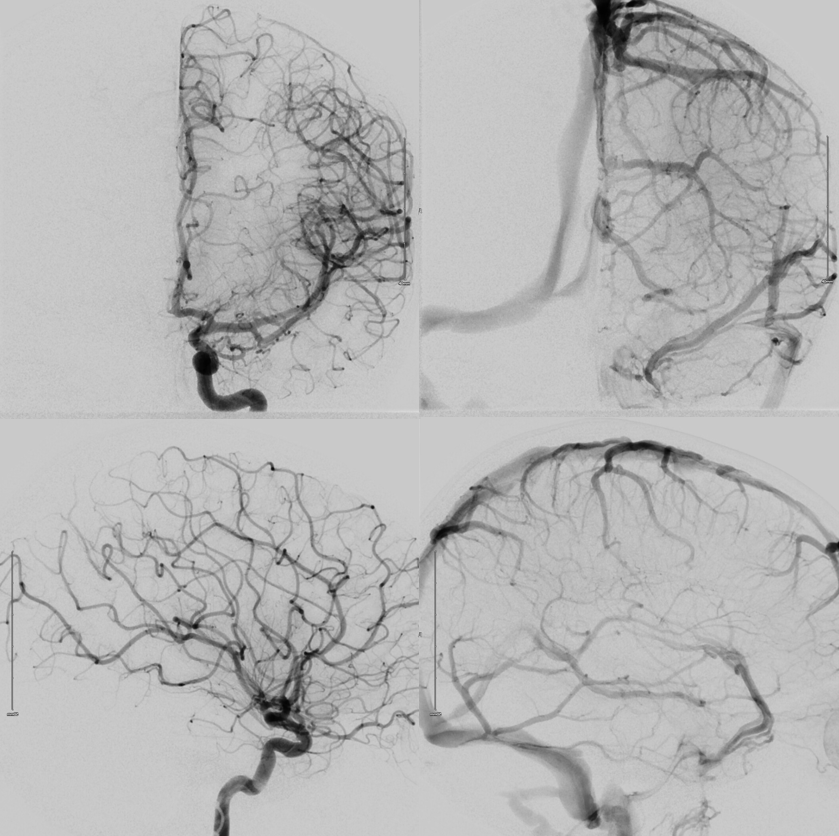
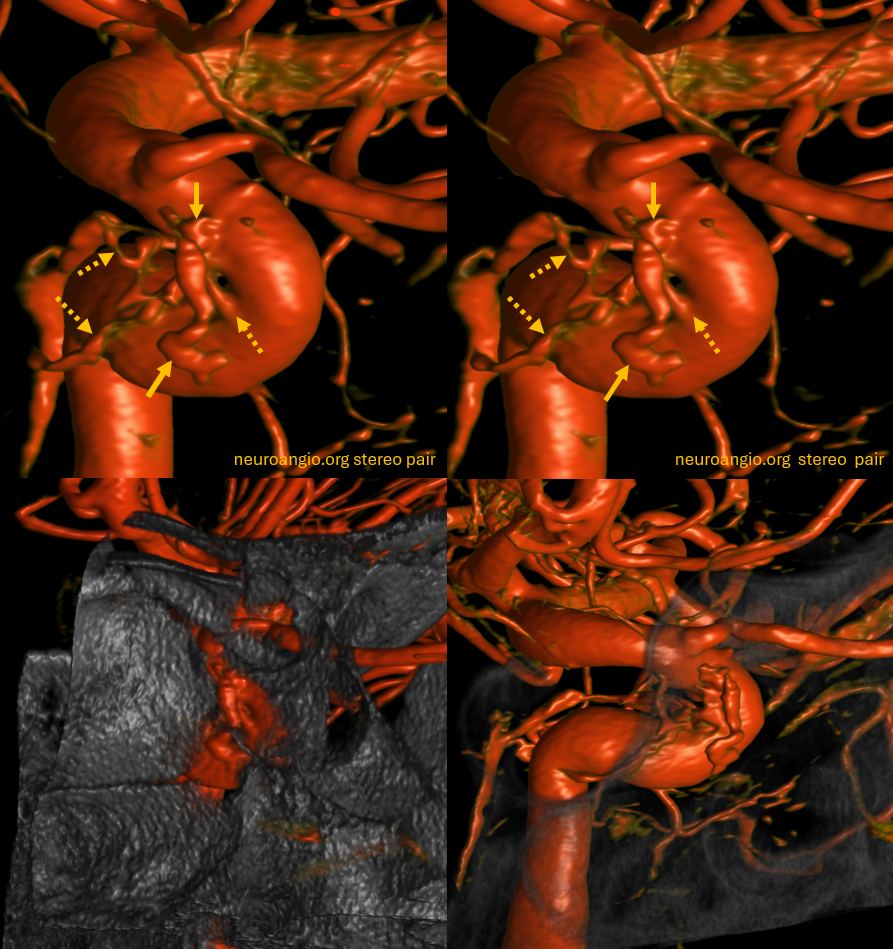
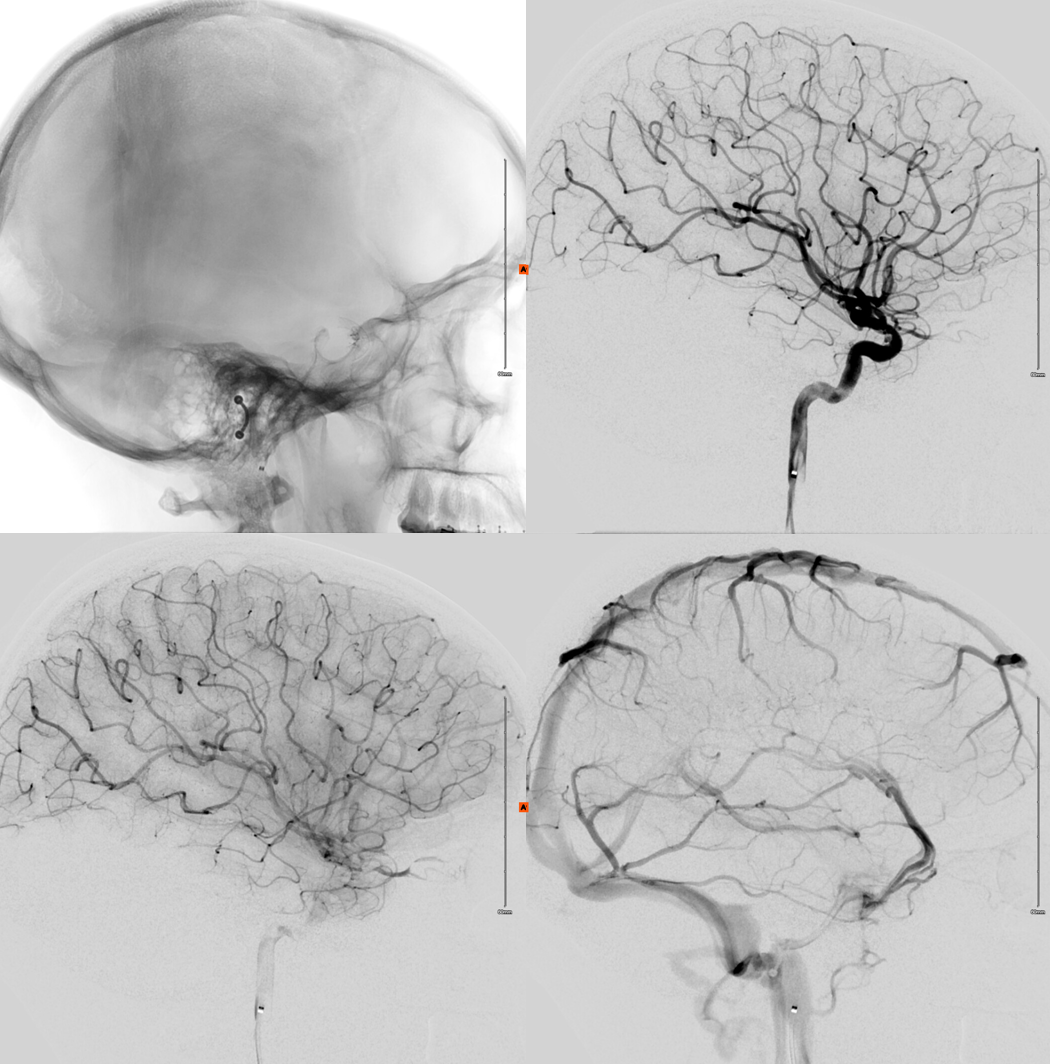
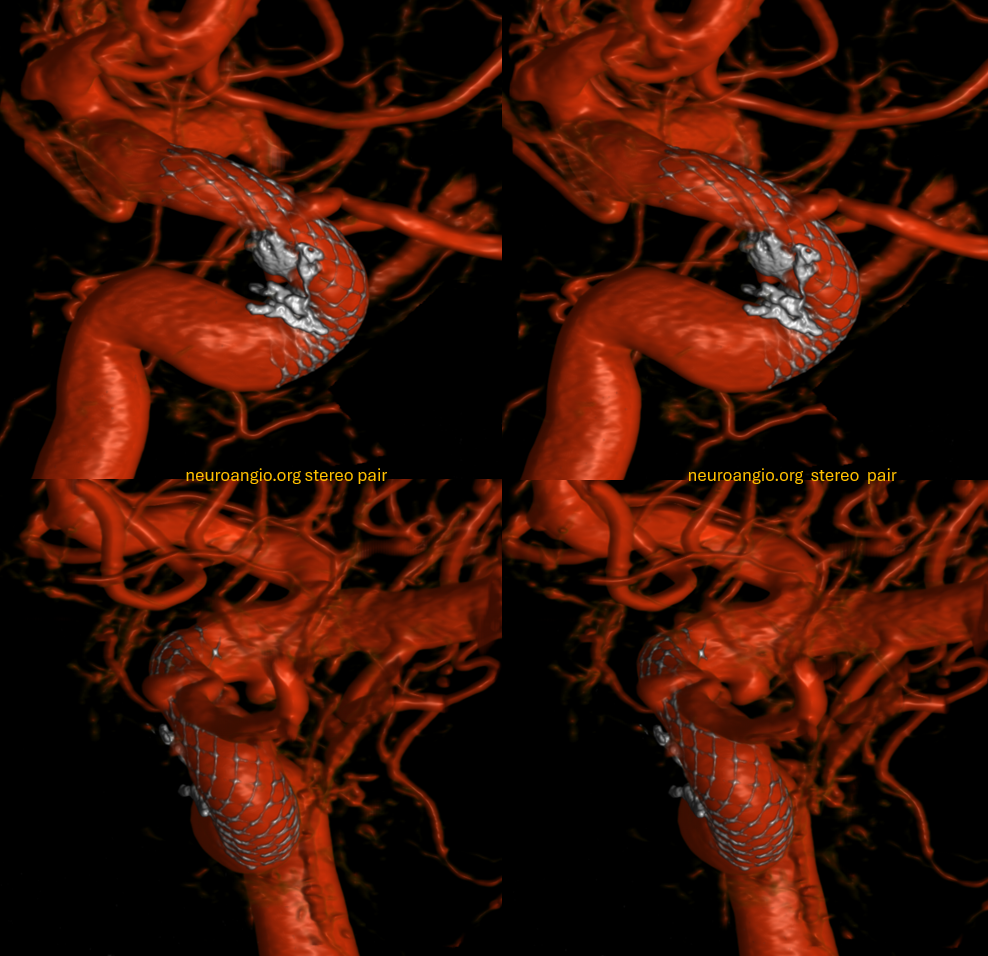
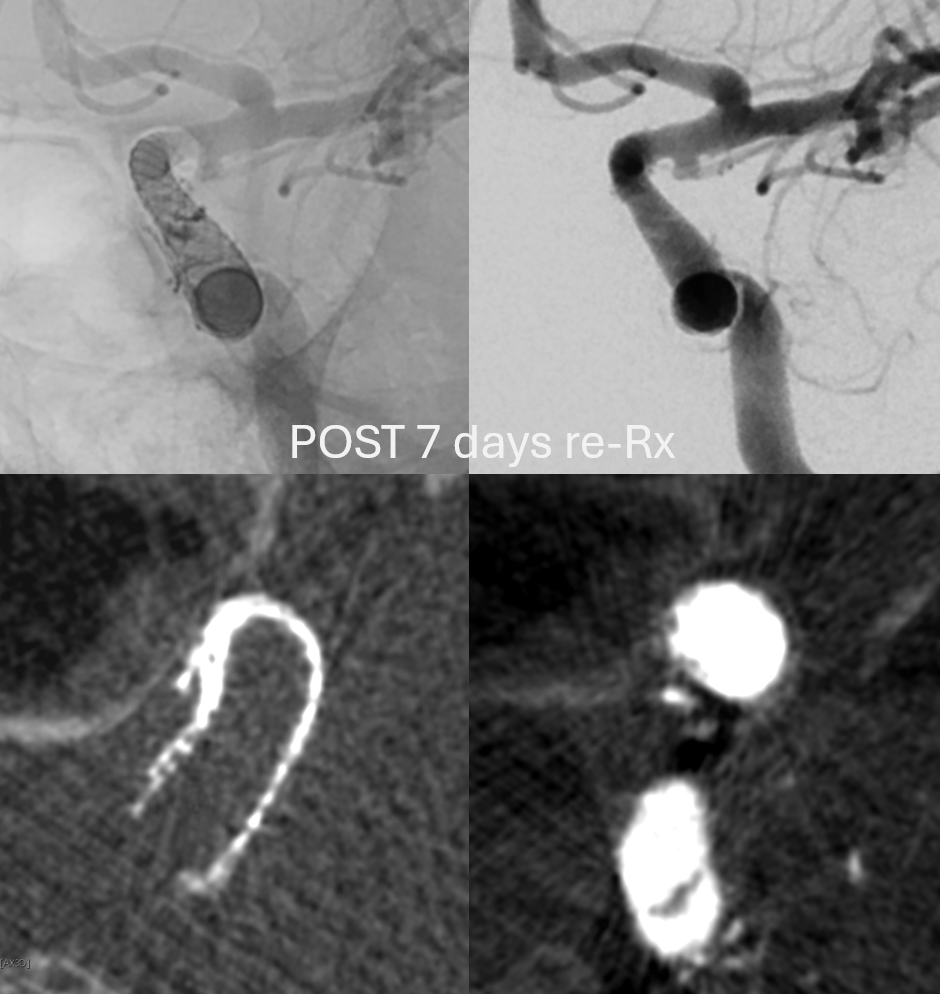
Top row are post retreatment stereos. Bottom left is before re-treatment. Bottom right is a fusion of pre and post — with additional in green
One week later, still holding up
What a saga — and we have not even talked about the right side…
In fact, there was a third shit sandwich to eat here also… but so far so good